
Abstract
Amid a global aging trend, particularly notable in the U.S., there is a growing focus on achieving enhanced longevity and well-being. We evaluated the association between lifestyle factors (sleep, diet, and healthy lifestyle index) and COVID-19 infection in an older adult population in San Bernardino and Riverside counties in Southern California, the United States. A sample of 380 older adults ≥75 years old were surveyed cross-sectionally and self-reported lifestyle behaviors and COVID-19 infection. The results revealed that half the participants reported COVID-19 infection. Participants who slept less than 7 hours or more than 8 hours/night had higher odds of COVID-19 infection than those who slept 7–8 hours/night (OR = 1.62, 95% CI: 1.03, 2.55). Healthy lifestyle behaviors were significantly associated with reduced COVID-19 infection (OR = 0.61, 95% CI: 0.40, 0.92). In conclusion, adequate sleep and healthy lifestyle behaviors may be protective against COVID-19 infection among older adults and should be investigated further.
• This paper offers evidence that potentially links healthy lifestyle behaviors to reduced COVID-19 infection in older adults. • Healthy lifestyle factors are crucial and contribute to lower infection rates and potentially protect against COVID-19 diagnosis and other similar virus-induced pandemics.
• Adopting healthy lifestyle practices can predict better health, longevity, and functioning, as well as reduce COVID-19 infection rates. • Interventions targeting lifestyle improvements among older adults, particularly concerning the repercussions of COVID-19, are imperative.What this paper adds
Applications of study findings
Introduction
With a large share of the global population aging, especially in the United States (U.S.), there is increased interest in living healthier and longer. Protective factors such as physical activity, diet, smoking cessation, and midday naps are a few of the secrets to long life (Panagiotakos et al., 2011; Trichopoulou, 2004). However, the COVID-19 pandemic has adversely impacted overall health and longevity, with the United States experiencing a decrease in life expectancy since the start of the pandemic (Andrasfay & Goldman, 2022). Therefore, it remains unclear how protective lifestyle factors may be in promoting longevity in the face of the COVID-19 pandemic.
A growing body of evidence worldwide has uncovered several regions in which the lifestyles of subpopulations have been associated with enhanced longevity (Buettner & Skemp, 2016). Globally, five key communities—Sardinia (Italy), Nicoya (Costa Rica), Okinawa (Japan), Ikaria (Greece), and Loma Linda, California (U.S.)—have been identified as Blue Zones or longevity hotspots where members live healthier and longer. It has been observed in different studies around the globe that people living in a Blue Zone area have a high life expectancy (Huang & Mark Jacquez, 2017; Legrand et al., 2019, 2021; Pes et al., 2021) and are ten times more likely to reach 100 years old (Buettner & Skemp, 2016). This study centered on investigating three distinct factors, namely, sleep, diet, and lifestyle behaviors in the Loma Linda Blue Zone.
Sleep
Research from various scholars has highlighted the importance of moderate sleep on the quality of life among older adults (Azri et al., 2016; Du et al., 2021; Stone & Xiao, 2018; Turner et al., 2017). Studies among older populations around the world have yielded similar results; regardless of the method used to measure sleep (e.g., different types of survey questions, sleep logs, and wrist actigraphy), both insufficient and excessive sleep durations are consistently linked to inferior concurrent health outcomes (Cappuccio et al., 2010; Chattu et al., 2018; Lauderdale et al., 2016; Ren et al., 2020; Sabia et al., 2022). The COVID-19 pandemic has directly affected sleep due to the resulting social isolation, home confinement, anxiety, fear of infection, stress, and economic uncertainties associated with the pandemic. These factors can cause circadian disruption and contribute to developing or continuing insomnia. In addition, based on previous research on other viral respiratory diseases, indirect evidence suggests that sleep disturbances can lead to immunological imbalances, which may increase the risk of infection (Bocek et al., 2023; Ibarra-Coronado et al., 2015; G. N. Pires et al., 2021). It is, therefore, plausible that a similar relationship may exist between sleep disturbances and COVID-19 (Pires et al., 2021).
Diet
Diet is a key component of the immune system. For the body to effectively fight infections, a proper diet is recommended. The crucial roles of micronutrients, including vitamins and trace elements, are well-established in innate and adaptive immune responses. Maintaining micronutrient homeostasis is vital for supporting a healthy immune system (Wintergerst et al., 2007). Micronutrient deficiencies have been shown to impair immunity to disease, while supplementation can enhance immunity to viral infections (Jayawardena et al., 2020). A deficiency in vitamin D, for instance, has been linked to weakened immune responses and a heightened risk of systemic infections (Bouillon et al., 2019). A vegan diet produced the healthiest levels of diet-related biomarkers, including carotenoids, isoflavones, enterolactone, saturated and polyunsaturated fatty acids, and vitamins, compared to other diet patterns, according to the Adventist Health Study-2 (AHS-2) (Butler et al., 2008; Miles et al., 2019). There are numerous reasons why individuals may opt for a vegan diet, including its health benefits, such as enhancing immunity and lowering the risk of certain illnesses like heart disease, diabetes, and some cancers (Glick-Bauer & Yeh, 2014). Recent scientific findings indicate that incorporating more plant-based foods in one’s diet, such as increasing vegetable intake, may reduce the incidence of chronic viral diseases, including hepatitis viruses, and lower the likelihood of developing severe COVID-19 (Wong et al., 2022). Results from a study done at Loma Linda University showed higher COVID-19 hospitalization rates for those who ate a high-protein and low-vegetable based diet (Reis et al., 2022).
COVID-19 Impact
All three lifestyle factors—sleep, diet, and physical activity—play an important role in longevity and may be even more important in promoting health and well-being during the COVID-19 pandemic. Emerging research studies are beginning to shed light on the relationship between lifestyle and health during the COVID-19 pandemic (Ahmadi et al., 2021; Cervera-Martínez et al., 2021; Tavakol et al., 2023; van der Werf et al., 2021). However, research is limited on the potential relationship between COVID-19 and healthy lifestyle practices, particularly in older adult populations. More research is needed to narrow the existing gap in the literature on how these factors are related to COVID-19 among this particular population. Thus, the purpose of this study is to assess the potential association between lifestyle factors and COVID-19 infection among older adults.
Methods
Study Design
This study evaluated the potential association between lifestyle factors (particularly sleep, diet, and a healthy lifestyle index) on COVID-19 infection in an older adult population in San Bernardino and Riverside counties in Southern California. This cross-sectional study was conducted at the Loma Linda University Office of Preventive Care, retirement homes, senior centers, community clinics, assisted living facilities, and churches in both counties between July 2021 and March 2023. The inclusion criteria included English speaking, 75 years of age or older, and residing in either San Bernardino or Riverside County in California, U.S.; the exclusion criteria included incomplete surveys and participants younger than 75 years of age. Participants responded to surveys through either a physical medium in the form of a paper survey or a verbal medium via a phone interview. A total of 394 individuals were initially enrolled as participants; however, 14 individuals were disqualified from the study due to not meeting the age criterion of 75 years or above and/or because of incomplete paper surveys. Therefore, the final sample size for the analysis consisted of 380 individuals at the end of the data collection phase.
Variables, Instrumentation, and Measurement
The survey collected information about sleep, dietary patterns, and lifestyle factors to construct the lifestyle index, demographic variables (i.e., gender, age, marital status, annual income, education level, and race/ethnicity), and COVID-19 infection.
Independent Variables (Sleep, Diet, and Healthy Lifestyle Index)
Independent/exposure variables include sleep, diet, and lifestyle factors included in the lifestyle index (based on responses to questions pertaining to diet, physical activity, alcohol consumption, smoking status, body mass index [BMI], and sleep duration).
To measure sleep, participants were asked: “On average, how many hours do you sleep each night?” Diet was assessed by the following question: “How do you classify yourself based on your usual dietary intake?” as defined in the AHS-2 (Butler et al., 2008). The possible answers included the following: non-vegetarian (eat all meats and animal products), semi-vegetarian (eat meats but 1 to 3 times per month), lacto-ovo vegetarian (no meat and fish but eat eggs and dairy), pesco-vegetarian (never eat meats but eat fish, eggs, and dairy), and vegan (never eat any animal product). In our study, we classified participants’ dietary patterns into two categories: vegetarians and non-vegetarians. The vegetarians’ group comprised individuals following a vegan, pesco-vegetarian, or lacto-ovo vegetarian diet, while the non-vegetarians’ group included individuals following a semi-vegetarian or non-vegetarian diet, given that the number of participants for each of these dietary patterns was less than 70.
Definition of the Healthy Lifestyle Index Score (HLIS).
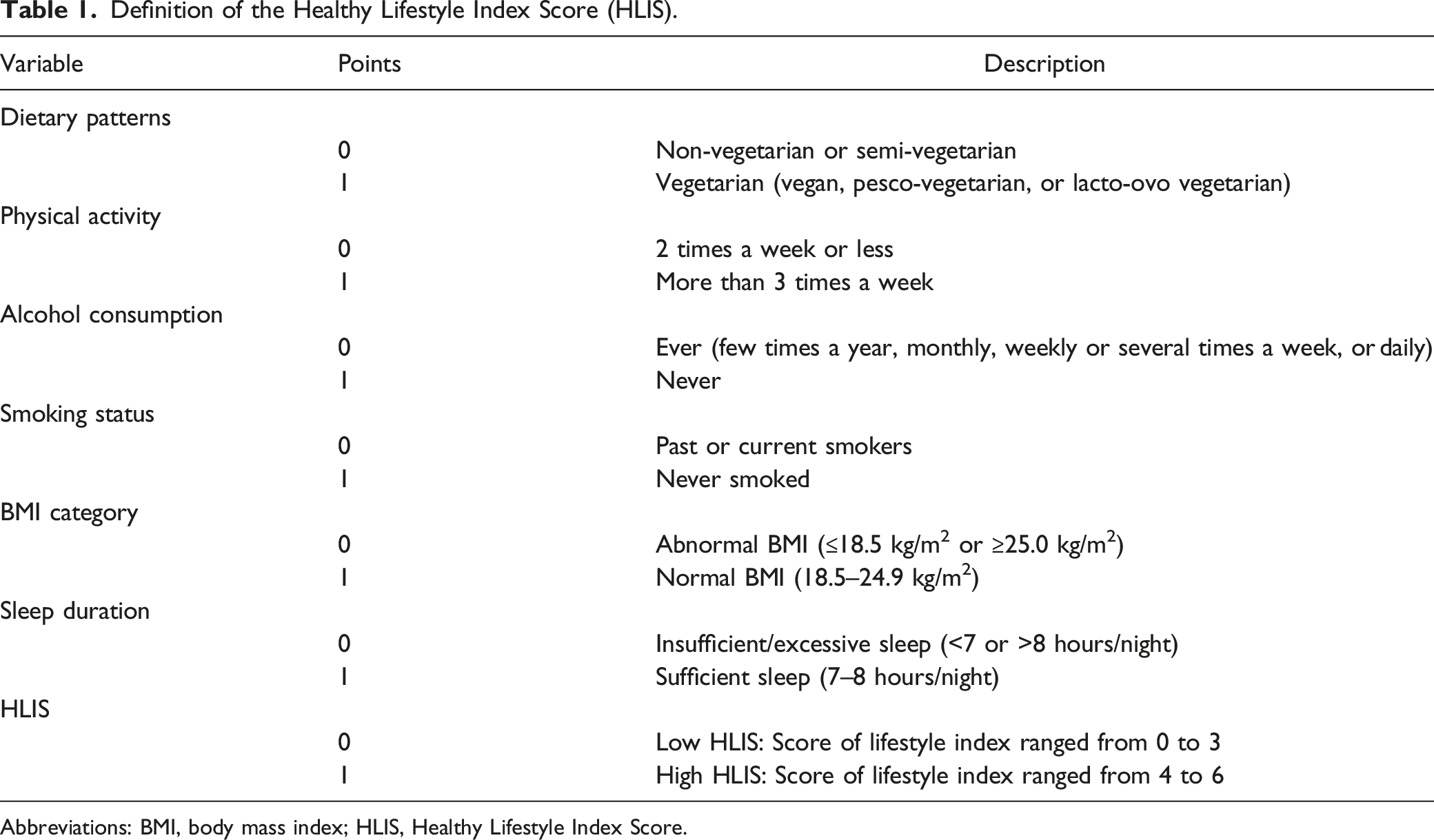
Abbreviations: BMI, body mass index; HLIS, Healthy Lifestyle Index Score.
Outcome Variable (COVID-19)
The dependent variable was the self-reported diagnosis of COVID-19, which was analyzed as a dichotomous variable and involved a yes/no response to the question, “Since 2019, have you had an infection with COVID-19?” Potential confounding variables were also collected from the survey, including demographics, COVID-19 vaccination status, number of daily medications taken, and comorbidities.
Ethical Considerations
Prior to commencing the study, all participants received comprehensive information about the nature of the study and provided their verbal assent to the informed consent to participate. The questionnaire was anonymous to protect their privacy. The survey collected was approved by the University Institutional Review Board (IRB#5210280), and the study was conducted with all the ethics and safety concerns.
Statistical Analysis
SAS software (version 9.4; SAS Institute, Inc., Cary, NC, USA) was used to perform the analyses of the study. Statistical hypotheses were tested using p < .05 as the level of statistical significance for univariate analyses, and 95% confidence intervals (CIs) were used for regression analyses.
Descriptive statistics for demographic and health characteristics in the study population were reported as counts with valid percentages for categorical variables. Pearson chi-square (χ2) was performed to evaluate the associations between categorical demographic characteristics, health characteristics, and COVID-19 infection after assessing the assumptions of these statistical tests.
A logistic regression model was used to evaluate the potential association between lifestyle factors and COVID-19 diagnosis, and potential confounding variables were added to the multivariable model with odds ratios (ORs) and 95% confidence intervals (CIs) reported. The variables included in the crude model were sleep, diet, and the HLIS as the main independent variables, adjusted for age. For the full model, we further adjusted for other demographics, including age, gender, marital status, race, and education level, as well as COVID-19 vaccination. The models were examined for 10% change in the primary variables (Greenland, 1989) in the presence of comorbidities (e.g., diabetes, hypertension, obesity, heart disease, arthritis, kidney disease, lung disease, liver disease, cancer, asthma, and/or sleep apnea) and the number of daily medications taken, and it was determined that they did not serve as significant confounding variables; thus, they were excluded from the final model. Confounding variables were evaluated by conducting preliminary analyses (i.e., univariate analysis) to identify any variables that were significantly associated with the dependent variable. Any variables found to be significant (p < .05) in the univariate analysis were included in the final model.
Results
Characteristics of the Survey Respondents by COVID-19 Cases versus Non-cases (n = 380).
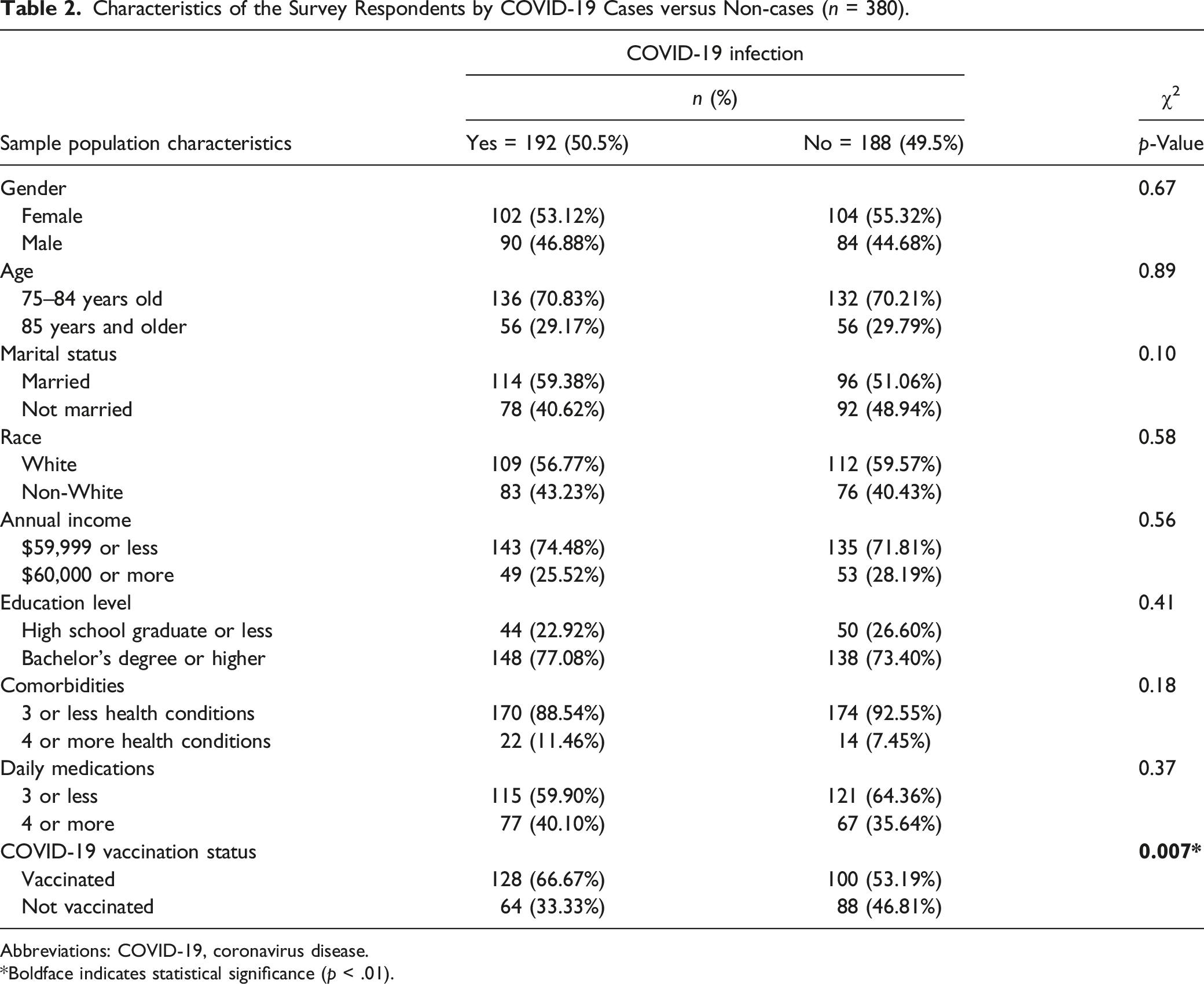
Abbreviations: COVID-19, coronavirus disease.
*Boldface indicates statistical significance (p < .01).
Components of the Healthy Lifestyle Index Score (HLIS) by COVID-19 Cases versus Non-cases (n = 380).
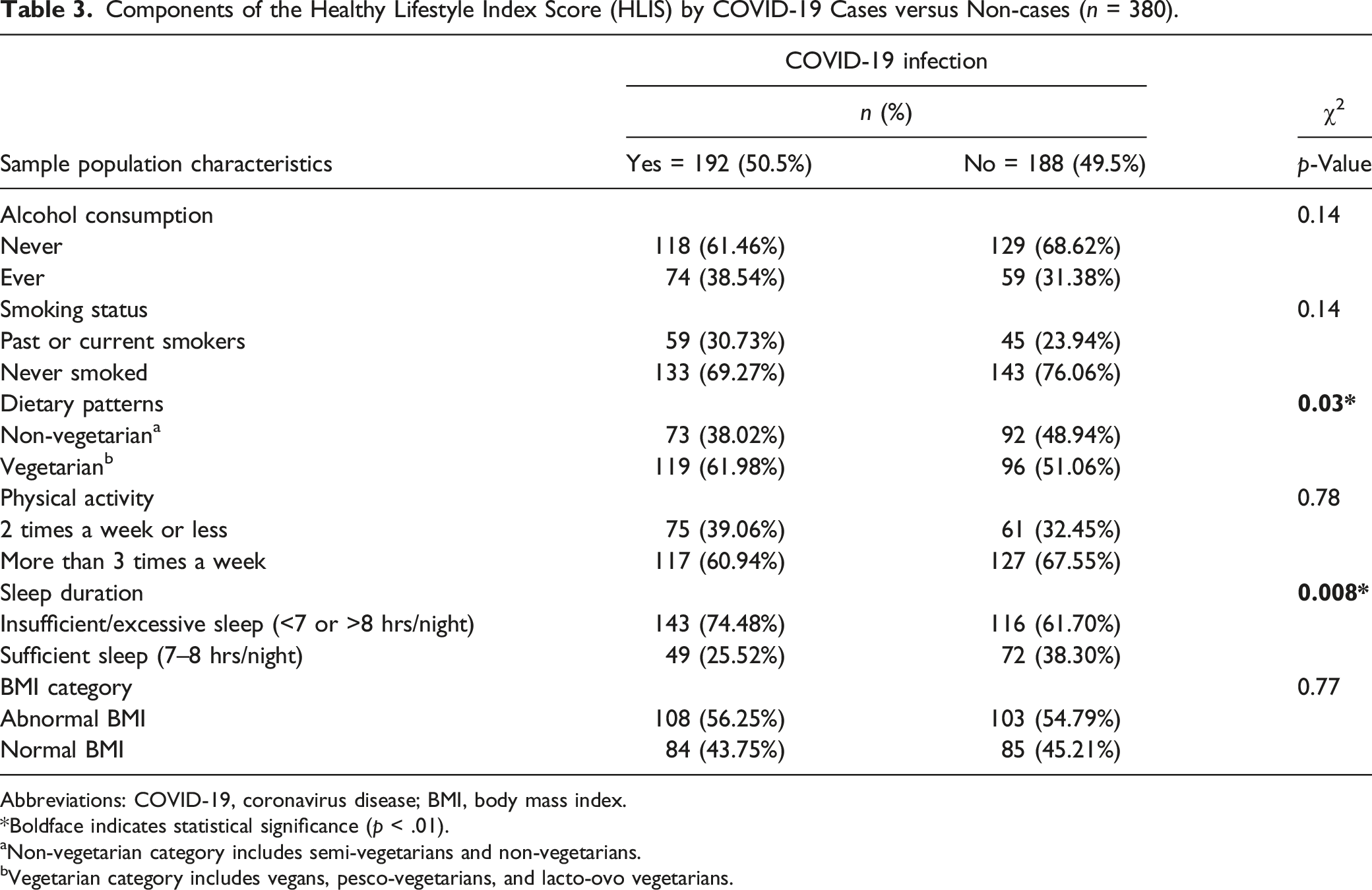
Abbreviations: COVID-19, coronavirus disease; BMI, body mass index.
*Boldface indicates statistical significance (p < .01).
aNon-vegetarian category includes semi-vegetarians and non-vegetarians.
bVegetarian category includes vegans, pesco-vegetarians, and lacto-ovo vegetarians.
Multivariable Adjusted Odds Ratios (ORs) for the Association Between Lifestyle Factors a and COVID-19 Infection.
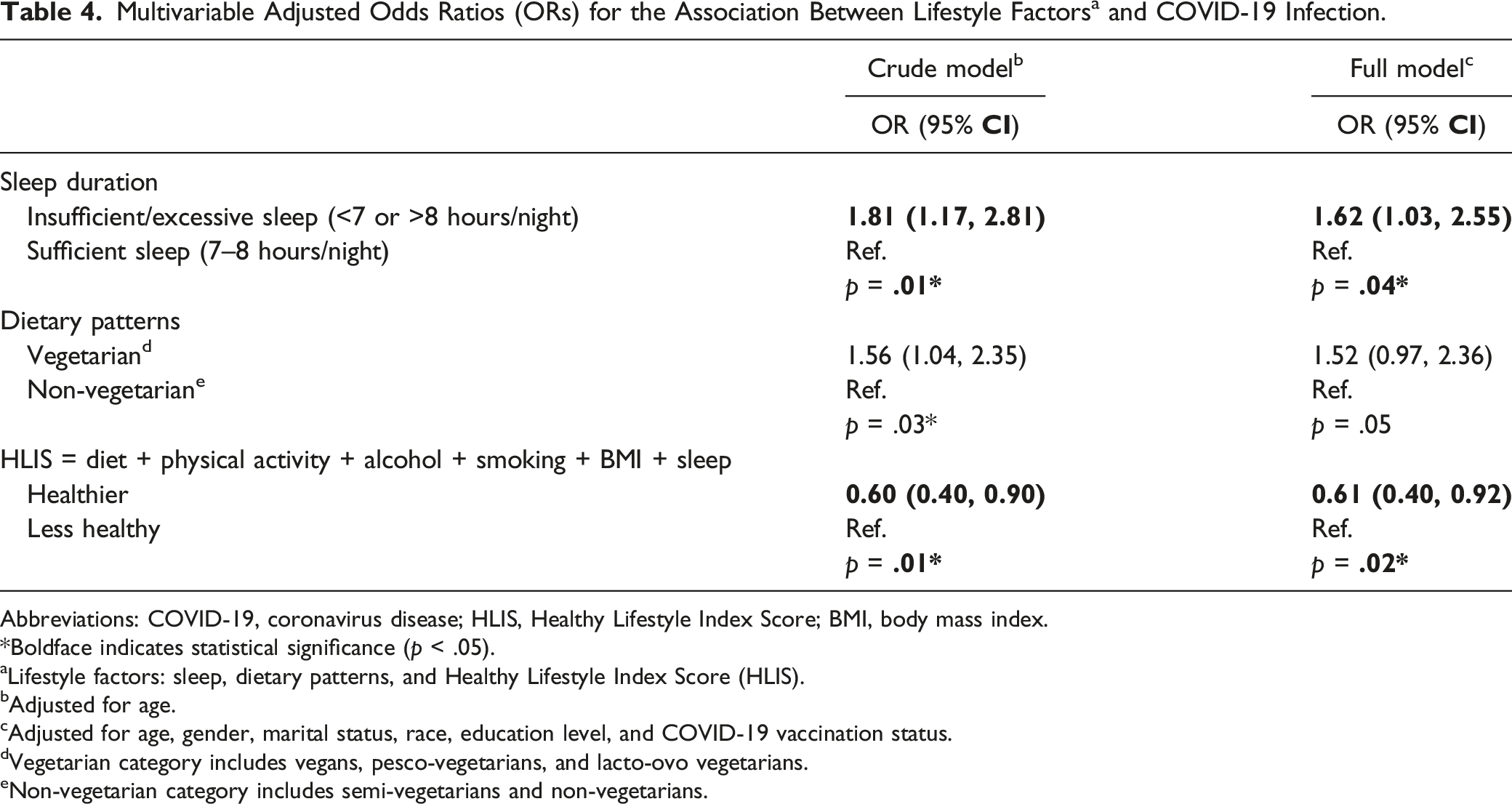
Abbreviations: COVID-19, coronavirus disease; HLIS, Healthy Lifestyle Index Score; BMI, body mass index.
*Boldface indicates statistical significance (p < .05).
aLifestyle factors: sleep, dietary patterns, and Healthy Lifestyle Index Score (HLIS).
bAdjusted for age.
cAdjusted for age, gender, marital status, race, education level, and COVID-19 vaccination status.
dVegetarian category includes vegans, pesco-vegetarians, and lacto-ovo vegetarians.
eNon-vegetarian category includes semi-vegetarians and non-vegetarians.
Discussion
Our study aimed to evaluate the potential association between lifestyle factors (with emphasis on sleep, diet, and healthy lifestyle index) and COVID-19 infection in an older adult population. We found an association between sleep duration and COVID-19 infection; our findings were consistent with previous studies conducted by other researchers (Becker, 2022; Neculicioiu et al., 2022; Pires et al., 2021). In our cross-sectional study, insufficient or excessive sleep (<7 or >8 hours/night) was associated with higher odds of reporting COVID-19 infection (62% increase, p = .04). Our study found that approximately 75% of the participants who did not sleep for 7–8 hours per night reported infection with COVID-19; therefore, individuals reporting insufficient sleep may exhibit increased susceptibility to the COVID-19 virus.
Sleep may play a crucial role in determining COVID-19 infection rates, as participants who reported less sleep time had a higher risk of contracting the virus. Poor sleep quality and negative attitude towards the pandemic may increase the risk of COVID-19 infection, and long-term outcomes of COVID-19 may be negatively impacted by poor sleep quality (Kantor et al., 2022). Another study found that the impact of COVID-19 on sleep quality displays significant variations among populations and is contingent on the baseline sleep quality before the pandemic (Kocevska et al., 2020). Al-Ajlouni, et al., (2020) found that increased self-reported levels of anxiety or depression exhibited a significant correlation with deteriorating sleep health outcomes, potentially explained by the complex connection between mental health and sleep health. The mechanism by which depression influences sleep is believed to involve the attenuation of deep, slow-wave sleep combined with an escalation in the nocturnal arousal (Al-Ajlouni et al., 2020). Another study found that insomnia and sleep duration are potential risk factors for increased COVID-19 susceptibility. Relieving insomnia and maintaining normal sleep duration may be a powerful measure to reduce COVID-19 infection (Peng et al., 2022).
Ren, et al., (2020) found that sleep durations lasting more than 8 hours or less than 6 hours have been associated with higher all-cause mortality rates among older populations. The authors observed that sleep duration affects mortality rates among the Chinese older adult population, with a mean age of 89 years; moderate duration of sleep was defined as sleeping 7–8 hours per night (Ren et al., 2020). Sleep has been found to possess immune-supportive functions, while impairments to the immune-inflammatory system may serve as a plausible mechanism that mediates the harmful health effects associated with sleep deprivation. Specifically, such impairments may play a role in the increased risk and adverse outcomes of chronic diseases, including infections, cardiovascular disease, metabolic disorders, autoimmune diseases, neurodevelopmental disorders, and cancer (Garbarino et al., 2021). Generally, the relationship between sleep and immunity has important clinical implications for maintaining good health in our rapidly changing society. Specifically, promoting sleep health and targeting sleep to improve or therapeutically manage the inflammatory response can have significant benefits. In the era of preventive medicine, this approach may lead to addressing sleep as a lifestyle factor, along with diet and physical activity, to improve overall public health.
Our study found no significant association for dietary patterns on reported COVID-19 diagnosis. Therefore, it may be practical to utilize more specifics on dietary intake as a means of examining health outcomes for future studies, rather than relying solely on overall dietary patterns (Bailey, 2021). The immune system can be positively or negatively influenced by the nutritional status of an individual, which can affect the course of infectious diseases and associated inflammatory processes. Malnutrition is known to increase the susceptibility of disadvantaged populations and older adults to COVID-19 infections, resulting in more severe clinical symptoms and outcomes (Rodriguez-Leyva & Pierce, 2021). Although a healthy diet or nutraceutical supplementation may influence the infectivity rates and severity of clinical symptoms associated with coronavirus infection, it is unlikely to fully prevent strong viral transmission. The impact of vitamin D and zinc status on viral transmission and clinical symptoms in COVID-19 patients is not yet well understood and requires further investigation (Rodriguez-Leyva & Pierce, 2021). Previous research on the interactions between nutrition and other viral diseases can help generate hypotheses related to COVID-19. However, the literature on this topic is inconsistent, and studies taken in isolation may lead to rumors and misguided attempts to prevent or cure COVID-19. In light of the established influence of malnutrition on the immune system, implementing public health measures to alleviate micronutrient deficiencies, undernutrition, and overnutrition is imperative. This necessitates leveraging the insights gained from other viral illnesses (James et al., 2021).
The incidence of infection with COVID-19 can potentially be mitigated by adopting healthy lifestyle behaviors. The results of this study suggest that participants who maintain a healthy lifestyle may potentially be less likely to contract COVID-19. Wang et al., (2023) have documented that individual lifestyle factors, such as obesity, smoking, unhealthy eating habits, and poor sleep quality, increase the risk of long-term COVID symptoms or hinder recovery from COVID-19. The prospective cohort study suggested that adherence to a healthy lifestyle considerably reduces the risk of developing post-COVID conditions (PCCs) in individuals subsequently infected with COVID-19. If the established association is causal, maintaining a healthy weight and adequate sleep duration may have the greatest potential for preventing PCC among healthy lifestyle factors (Wang et al., 2023). In general, people exposed to a healthy lifestyle, such as healthier dietary patterns and increased physical activity, may have a lower risk for associated severity of COVID-19 infection (Tavakol et al., 2023). Healthy lifestyle practices, such as maintaining a desirable BMI, abstaining from smoking, eating a healthy diet, moderate or no alcohol consumption, participating in regular exercise, and getting adequate sleep, have been shown to confer protection against inflammation (Hamer et al., 2020). Additionally, healthy lifestyle practices have been shown to predict better health, longevity, and functioning, as well as reduce COVID-19 infection rates (Diener & Chan, 2011; Formanek et al., 2020; Kokko & Feldt, 2018; Wang et al., 2023). The degree of adherence to multiple healthy lifestyle practices is directly correlated with less severe symptoms of COVID-19 and lower mortality due to infectious diseases, including COVID-19, in a dose-dependent manner (Ahmadi et al., 2021; Hamer et al., 2020; Wang et al., 2023).
The present study has several strengths and limitations that merit discussion. One of the strengths is that the study population was selected from the general population of two counties in Southern California, U.S., enhancing the generalizability of the findings for those 75 years or older. Additionally, the age bracket selected for our study is distinct, given the significance of age in relation to susceptibility to COVID-19 infection. Another notable strength is the presence of a substantial proportion of participants in both the sufficient sleep and insufficient or excessive sleep groups, facilitating the evaluation of the potential correlation between this variable and COVID-19 infection.
Limitations
The impact of the COVID-19 pandemic was a significant limitation of this study, as it hindered the researchers’ ability to reach out to some potential participants, particularly during the initial phase of the study in 2021. The pandemic also resulted in a longer study duration than initially anticipated. Moreover, due to the cross-sectional nature of our study, we were unable to establish causality or address risks. Additionally, selecting a sample from a large and heterogeneous population can introduce sampling bias, while misclassification due to recall bias is another potential limitation. Having our data collected from two counties may not be typical of all 58 counties in CA which restricts the external validity. Therefore, our sample may not have a fully representative collection of the older adults (75 years and older) in CA. Evaluating sleep quality rather than duration posed challenges, given that individuals might lack awareness unless informed by others, introducing another limitation to the study. Lastly, the self-reported nature of the data may also be prone to bias, as people may selectively remember events (telescoping), attribute outcomes to their actions or external factors, or exaggerate the importance of events. These limitations could lead to systematic bias in the study findings.
Conclusion
In summary, this study offers evidence that potentially links healthy lifestyle behaviors to reduced COVID-19 infection in individuals 75 years of age and older. While the timeline of data collection (July 2021 to March 2023) only partly accounts for population differences, a healthy lifestyle and adequate sleep duration are crucial factors that contribute to lower infection rates and potentially protect against COVID-19 diagnosis and other similar virus-induced pandemics. Moreover, our study highlights the need for further research to investigate the relationship between diet intake, such as consumption of fruits, vegetables, fibers, and sweetened products (beyond dietary patterns), and the risk of COVID-19 infection. These findings will provide valuable insights for designing future studies to elucidate the potential impact of diet on the susceptibility and severity of COVID-19. Additionally, further research is necessary to investigate whether these positive lifestyle behaviors remain protective factors against infectious diseases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the author(s) used the Writefull tool in order to make suggestions to help improve the quality of the writing. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
IRB Protocol/Human Subjects Approval Numbers
The survey collected was approved by the Loma Linda University Institutional Review Board (IRB# 5210280), and the study was conducted with all the ethics and safety concerns. All participants received comprehensive information about the nature of the study and provided their verbal assent to the informed consent to participate beforehand.