
Abstract
• Isolation caused by the pandemic led older adults to reduce their physical activity levels. • Reduced physical activity was associated with worse cognitive and neuropsychiatric symptoms among older adults. • Changes in physical activity levels varied based on age and income.
• Community programs that promote accessible physical activity opportunities among older adults are needed. • Understanding the relationship between physical activity and the psychological and cognitive well-being of older adults is crucial for healthcare systems worldwide. • Given that older adults with self-reported low and middle income and those 55–65 years old reported less physical activity, directed initiatives to encourage physical activity in these groups can be helpful.What this paper adds
Applications of study findings
Introduction
In March 2020, the World Health Organization (WHO) declared the novel Coronavirus disease (COVID-19) outbreak a global pandemic (Cucinotta & Vanelli, 2020). In response, governmental authorities implemented restrictions that increased social isolation and reduced mobility, altering people’s daily routines, including changes in physical activity engagement and mood (Sepúlveda-Loyola et al., 2020). In fact, studies reported a decrease in physical activity levels in older adults and an increase in fatigue and sedentary behaviors since the onset of the COVID-19 pandemic (Amanzio et al., 2021; Ding et al., 2021).
These changes in behavior will likely have long-term impacts on brain health as low physical activity levels have negative implications for physical and mental health, cognition, and overall well-being (Sutton et al., 2022). In particular, physical inactivity in older adults has been associated with a greater risk of frailty, psychological distress (e.g., greater symptoms of depression and anxiety), premature mortality, worse quality of life, and increased risk for Alzheimer’s disease and related dementias (Arrieta et al., 2018; Creese et al., 2021; Horder et al., 2018). Intervention studies have shown that increasing exercise and physical activity levels can significantly improve cognition and reduce cardiovascular disease and other risk factors for dementia (Fiuza-Luces et al., 2018). Engaging in regular physical activity has also been associated with improved mental health, including greater resilience, positive affect, and lower depression (Carriedo et al., 2020).
Within the context of the COVID-19 pandemic, some studies have suggested that there is a relationship between government measures that were placed to reduce contagion rates and worse physical activity levels, mental health, physical health, and overall well-being outcomes in the general population (Gama de Matos et al., 2020). For example, precautionary isolation measures have been associated with increased rates of noncommunicable diseases-related behavioral risk factors, such as cardiovascular diseases, cancers, and diabetes (Musa et al., 2023) and increased emotional distress (Ammar et al., 2020). Other studies have also reported decreased mental well-being, sleep quality, and total physical activity energy expenditure levels in older adults in relation to COVID-19 lockdown and a sedentary lifestyle (Trabelsi et al., 2021). Consistent with these findings, a study conducted in Iran showed that physically active adults 18 years or older reported less severe anxiety than inactive adults during the pandemic and better emotional, psychological, and social well-being (Akbari et al., 2021).
Notably, it has been suggested that demographic and other individual differences may have influenced how the pandemic impacted people’s behaviors and mental health. For instance, one study reported that identifying as a woman and being retired were independently associated with worsening depressive symptoms during physical isolation while not being in full-time employment was associated with worse anxiety symptoms compared to being employed full-time (Creese et al., 2021). Similarly, it has been reported that the pandemic disproportionately negatively impacted low-income older adults as they exhibited worse mental and physical health (Bergeron et al., 2021).
It has been well established that engaging in physical activity is associated with better health outcomes in older adults (Posadzki et al., 2020). However, less is known about changes in physical activity induced by physical isolation during the COVID-19 pandemic, and its relationship with psychological well-being (e.g., anxiety and depression symptoms), and subjective cognitive decline in older adults. The latter has also been associated with objective cognitive decline and neurodegeneration (Jessen et al., 2020). Moreover, there is limited information about how physical activity levels during the early phase of the pandemic may have changed based on sociodemographic factors, such as age, sex/gender, income level, and employment status.
Enhancing our knowledge in this area can improve our understanding of the potential effects of physical and social isolation, which is known to be prevalent in older adults (Huang et al., 2023), on cognitive functioning and well-being during public, global health crises such as COVID-19. It can also help elucidate whether changes in physical activity levels could help counteract some of the potentially deleterious effects of physical and social isolation on cognitive functioning and psychological well-being during unexpected events such as public health crises. Additionally, this work may help identify sociodemographic characteristics that may place people at greater risk for reducing physical activity levels during unprecedented times.
The current study had three main aims. First, we examined physical activity changes in older adults living in the United States (US) between May and October 2020, and 3 months later. We then investigated whether changes in physical activity at baseline and the 3-month follow-up related to subjective cognitive decline (at baseline and the 3-month follow-up) and symptoms of depression and anxiety (at the 3-month follow-up). We hypothesized that older adults who maintained or increased their physical activity during this period would report fewer cognitive difficulties and fewer symptoms of depression and anxiety than those who reduced their physical activity or did not engage in physical activity. We also evaluated if participants had differences in physical activity changes based on age, sex assigned at birth, income level, and employment status. We hypothesized that those from higher-income households, men, those employed, and younger participants would report increasing or maintaining their physical activity. These variables were selected as these have been shown to be associated with health outcomes during the pandemic in several populations from outside the United States (Amatori et al., 2020; Cheval et al., 2021; García-Fernández et al., 2020).
Materials and Methods
Participants and Procedures
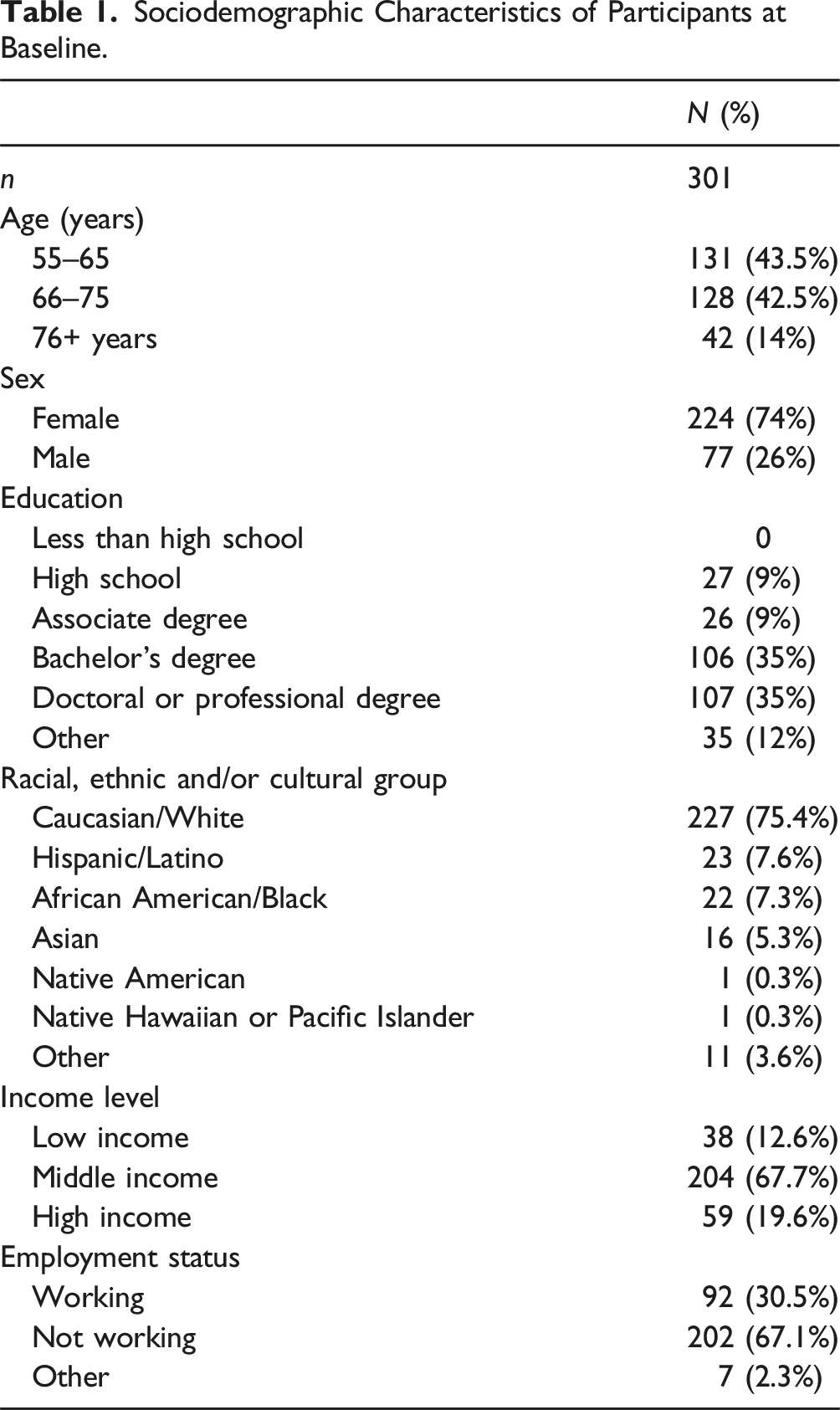
Our study presents data from an international effort titled “The Impact of COVID-19 on Well-being and Cognition in Older Ethnically Diverse Individuals” launched in May 2020. The study reports data from a non-probabilistic sample selected based on convenience. Participants completed a baseline online survey in either English, Spanish, or Portuguese using Research Electronic Data Capture (REDCap) between May and October 2020. They then completed the survey three and six months after baseline. Specifically, they completed a sociodemographic questionnaire and self-reported measures of subjective cognitive decline, anxiety, and depression symptoms. The sociodemographic questionnaire included information such as age, sex, income level, and employment status. Participants were grouped into one of the following three age groups: 55–65, 66–75, and 76+ years. Ethnicity and race were assessed with the following question: “How do you identify racially, ethnically, and/or culturally?” The response options were Caucasian/White, African American/Black, Asian, Hispanic/Latino, Native American, Native Hawaiian or Pacific Islander, or Other. Income was assessed with the question, “What category best describes your yearly household income?” and participants could answer “low income,” “middle income,” or “high income.”
We report data from 301 people. Inclusion criteria for this study included being 55 years or older and residing in the United States. Further, we only included participants who completed all baseline and 3-month follow-up measures and excluded those with only baseline data. Data from the 6-month follow-up was not included given that less than 100 people completed all questionnaires at this time.
Participants were recruited using flyers on social media through the Alzheimer’s Association (but participants could not be Alzheimer’s patients), researchers’ contacts, virtual meetings, and word-of-mouth.
All the data supporting this study’s findings are available on request from the co-corresponding author (Y.T.Q.) All research materials are available.
Standard Protocol Approvals, Registrations, and Participant Consents
The study was carried out in accordance with the latest version of the Declaration of Helsinki. The study was approved by the institutional ethics review board of Massachusetts General Hospital in Boston, Massachusetts (IRB protocol number: 2020P001131). All participants provided online informed consent before completing the survey.
Measures
Everyday Cognition (ECog) Scale
The total score of the ECog (Farias et al., 2008) was used to measure subjective cognitive decline
Epidemic-Pandemic Impact Inventory (EPII)
Changes in physical activity were measured with the EPII (Grasso et al., 2020). This instrument measures different changes in daily living associated with the pandemic, parting from the question, “Since the coronavirus disease pandemic began, what has changed for you or your family?” The questionnaire is divided into different sections, and two of them are “physical health problems” and “positive change.” The “physical health problems” includes the statement “less physical activity or exercise,” while the “positive change” section includes the “increase in exercise or physical activity” statement. Participants could answer “yes (me)” if the statement applied to them, “yes (person in home)” if the statement applied to someone else in their home, “no” if the statement did not impact them, and “N/A” if the statement did not apply to them or someone in their home. Participants could choose “yes (me)” and “yes (person in home)” if the statement was true for both the participant and other person in their home. We only included the answers that only pertained to the person completing the survey (i.e., “yes (me))” and not another person as the mental health measures and the ECog are self-reported.
The answers about physical activity or exercise changes were grouped into “less physical activity or exercise,” “increase in exercise or physical activity,” and “same activity level/no change.” The latter included participants who denied both engaging in “less physical activity or exercise” and an “increase in exercise or physical activity,” as this indicates they did not increase or decrease their levels of physical activity or exercise. We verified that no participant had responded contradictorily by selecting that they had increased and decreased their physical activity. No person answered “yes” to both statements.
Center for Epidemiological Studies-Depression Scale Revised (CES-D-R-10)
Depressive symptomatology was measured with the CES-D-R-10 (Björgvinsson et al., 2013), a self-report measure of symptoms of depression experienced over the past week. It has 10 items, and answers range from 0 (rarely or none of the time) to 3 (all of the time). A total score is calculated by adding all items for a maximum score of 30. This measure was only administered at the 3-month follow-up and not at baseline.
Generalized Anxiety Disorder Assessment (GAD-7)
Anxiety symptoms were measured using the GAD-7 (Löwe et al., 2008). It comprises seven items, and answers range from 0 (not at all) to 3 (nearly every day). A total score is calculated by adding all items for a maximum score of 21. This measure was only administered at follow-up and not baseline.
Statistical Analyses
All statistical analyses were conducted using SPSS Statistics, version 28.0.0.0 (Armonk, NY: IBM Corp). We calculated descriptive statistics for the sample. All analyses were conducted in the whole sample at baseline and at the 3-month follow-up. We conducted one-way analysis of variance (ANOVA) tests to examine if there were differences in subjective cognitive decline (ECog), anxiety symptoms (GAD-7), and depressive symptoms (CES-D-R-10) based on physical activity levels (i.e., “less active,” “more active,” and “no change”). Post hoc Tukey’s multiple comparisons tests were conducted to account for multiple comparisons. Since the GAD-7 and CES-D-R-10 scales were unavailable at baseline, the ANOVA tests for these scales were only completed for the 3-month follow-up. We also conducted chi-square tests to calculate group differences in categorical variables based on physical activity changes, including income level, sex, employment status, and age. We used Bonferroni correction to correct for multiple comparisons.
Results
Sociodemographic Characteristics of Participants at Baseline.
Maintenance of Physical Activity during the Pandemic
At baseline, 60% of participants reported engaging in less physical activity than before the pandemic, 25% reported that they had been doing more physical activity than before the pandemic, and 15% said they were doing the same amount of physical activity as before the pandemic (Figure 1(a)). During the 3-month follow-up, 58% of participants reported doing less physical activity than before the pandemic, 19% indicated that they were engaging in more physical activity than before the pandemic, and 23% stated that they were doing the same physical activity as before the pandemic (Figure 1(b)). Changes in physical activity at baseline and 3-month follow-up. (a) Number and percentage of people who reported less, more, or no change in physical activity at baseline, and (b) at the 3-month follow-up.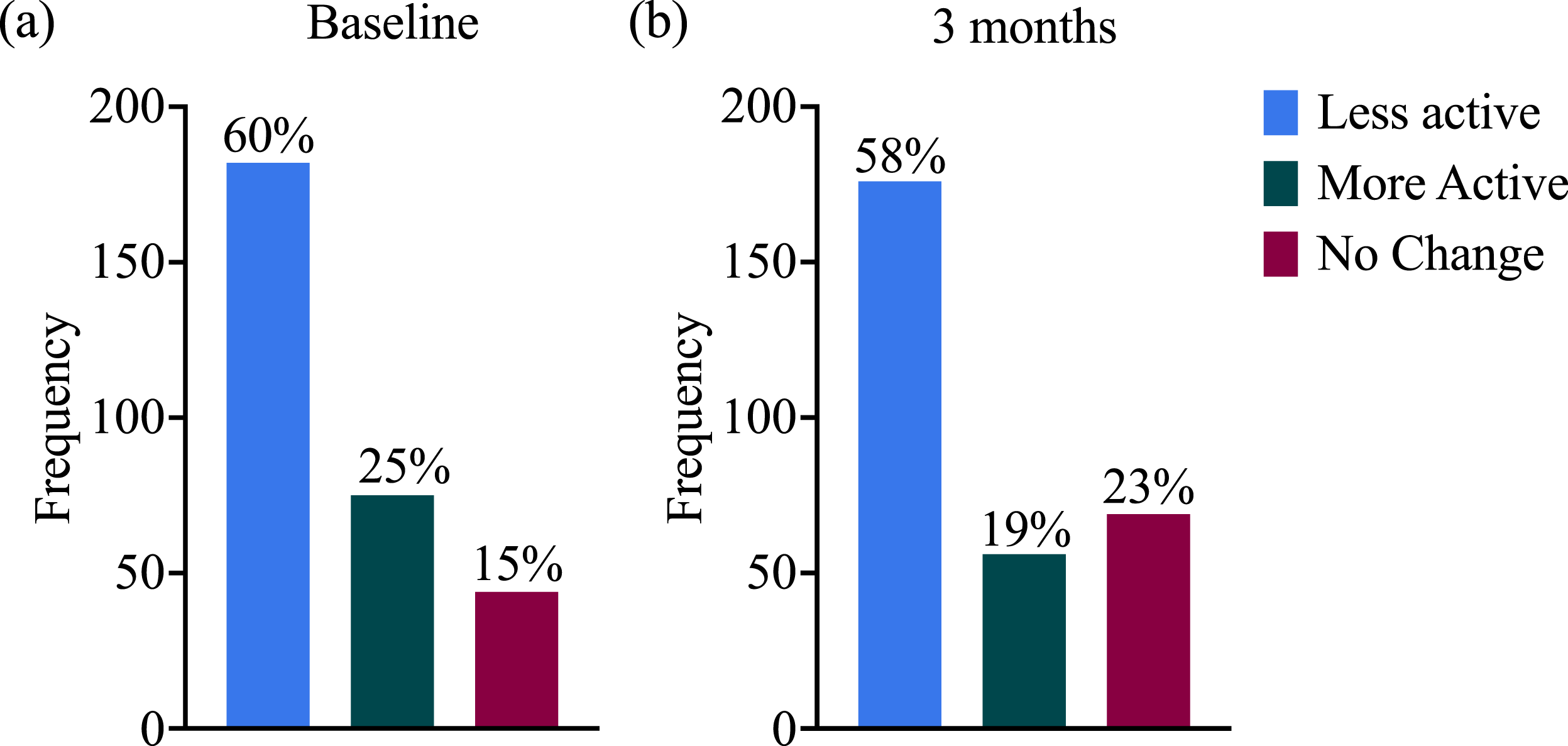
Maintenance of Physical Activity, Cognitive Concerns, and Mental Health Symptoms
There were significant differences in ECog scores between physical activity maintenance groups at baseline (F (2, 298) = 5.75, p < .01). Post hoc Tukey’s multiple comparisons test showed that those who increased their physical activity levels had lower ECog scores (i.e., better subjective cognitive functioning) compared to those who reduced their physical activity levels (p < .01; 7.07 [95% C.I. = 1.75, 12.40]). There were no differences between the increased or maintained physical activity groups (p = .88), or between less active and maintained physical activity groups (p = .11; 95% C.I. [−0.94, 12.11]) (Figure 2(a)). At the 3-month follow-up, there were also significant differences in ECog scores between the different physical activity groups (F (2, 298) = 4.88, p < .01). At the 3-month follow-up, the participants who reported reducing their physical activity levels reported higher ECog scores (i.e., worse subjective cognitive decline) compared to those who maintained their physical activity levels (p = .02; 5.89 [95% C.I. = 0.78, 11.01]) (Figure 2(b)). Differences in ECog scores, anxiety, and depression symptoms. (a) Differences in ECog scores between individuals who reported less, more, or no change in physical activity at baseline, and (b) at the 3-month follow-up. (c) Differences in GAD-7 scores between individuals who reported less, more, or no change in physical activity at the 3-month follow. (d) Differences in CES-D-R-10 scores between individuals who reported less, more, or no change in physical activity at the 3-month follow. It is important to clarify that figures C and D reach below 0 because of the kernel density estimates, but the lowest possible value is 0 for both measures (GAD-7 and CES-D-R-10). All graphs show the means and standard deviation. *p 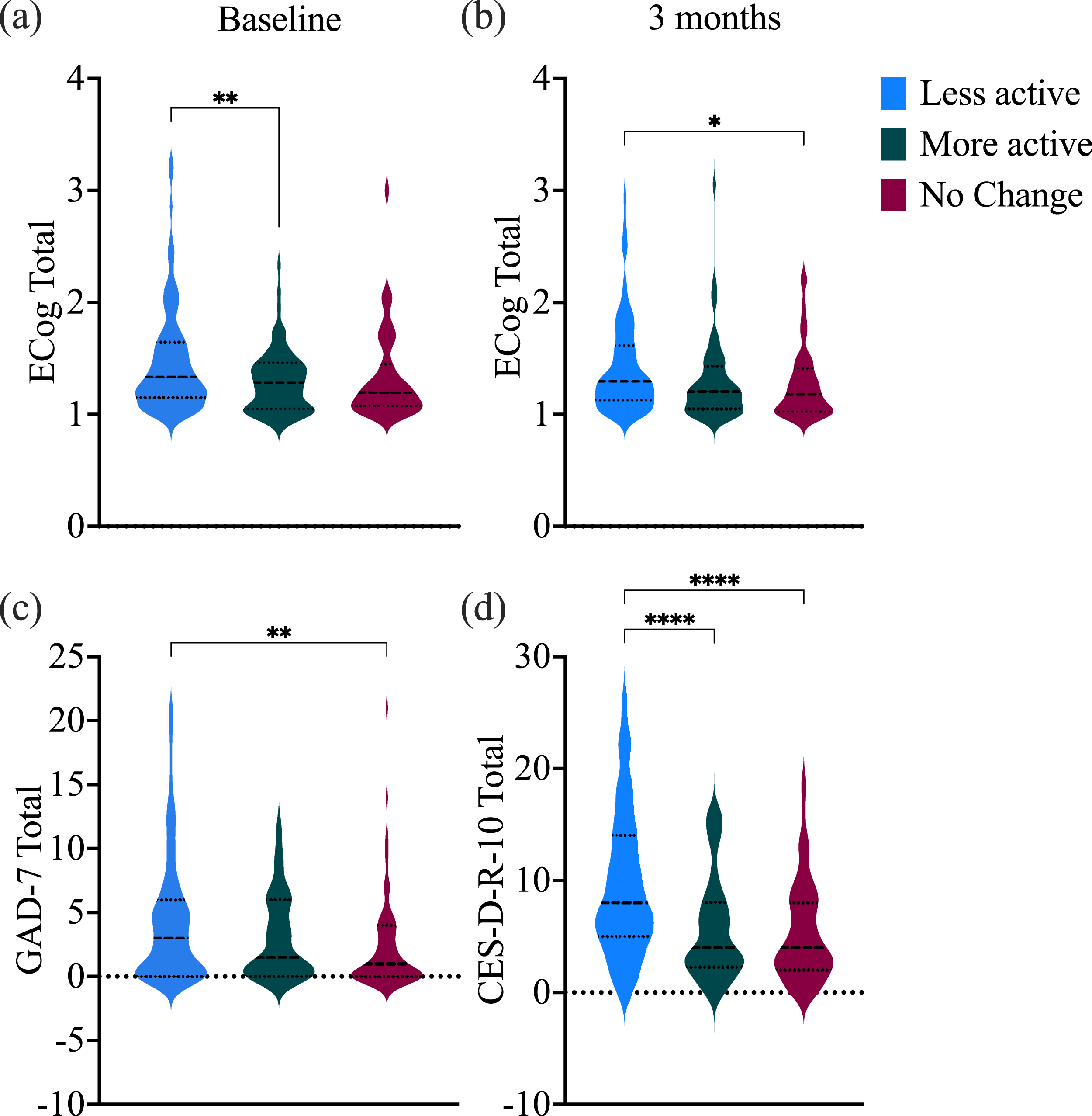
We then examined differences in mental health symptoms at the 3-month follow-up. There were significant differences in anxiety symptoms between physical activity levels (F (2, 298) = 5.89, p < .01). Participants who reported no change in physical activity level reported fewer anxiety symptoms than the ones who reported having reduced physical activity levels (p < .01; 2.03 [95% C.I. = 0.56, 3.52). There were no significant differences in anxiety symptoms between those who reported increased physical activity levels and the ones who reported less (p = .14; 95% C.I. = [−0.30, 2.89]) and between those that reported increased physical activity levels and the participants that reported having the same activity level as before the pandemic (p = .62; 95% C.I. = [−2.61, 1.13]) (Figure 2(c)).
Regarding depression symptoms, there were also significant differences between physical activity levels at the 3-month follow-up (F (2, 298) = 18.30, p < .0001). Participants who reported having reduced their physical activity levels during the pandemic reported greater depressive symptoms than those who maintained them (p < .0001; 4.19 [95% C.I. = 2.27, 6.11]) or increased their physical activity levels (p < .0001; 3.87 [95% C.I. = 1.81, 5.95]). There were no significant differences in depressive symptoms between the participants who had the same physical activity level and the ones who reported being more active than before the pandemic (p = .95; 95% C.I. = [−2.74, 2.11]) (Figure 2(d)).
Sociodemographic Variables and Physical Activity
There were significant differences in physical activity levels based on income and age, but not based on sex or employment status. At baseline, there were significant differences between low-income and high-income earners, with a greater proportion of high-income earners reporting that they engaged in more physical activity during the pandemic (X2 (1, N = 82) = 4.78, p = .03) (Figure 3(a)). This difference between the low-income and high-income earners remained at the 3-month follow-up (X2 (1, N = 70) = 7.59, p < .01) (Figure 3(b)). At the 3-month follow-up, a significant difference between middle-income participants and high-income participants was also observed, with middle-income earners reporting being less active than high-income earners (X2 (1, N = 206) = 8.92, p < .01) (Figure 3(b)). Differences in physical activity levels based on income and age. (a) Differences in the number of people who reported less, more, or no change in physical activity stratified by income at baseline and (b) 3-month follow-up. (c) Differences in the number of people who reported less, more, or no change in physical activity stratified by age at the 3-month follow-up.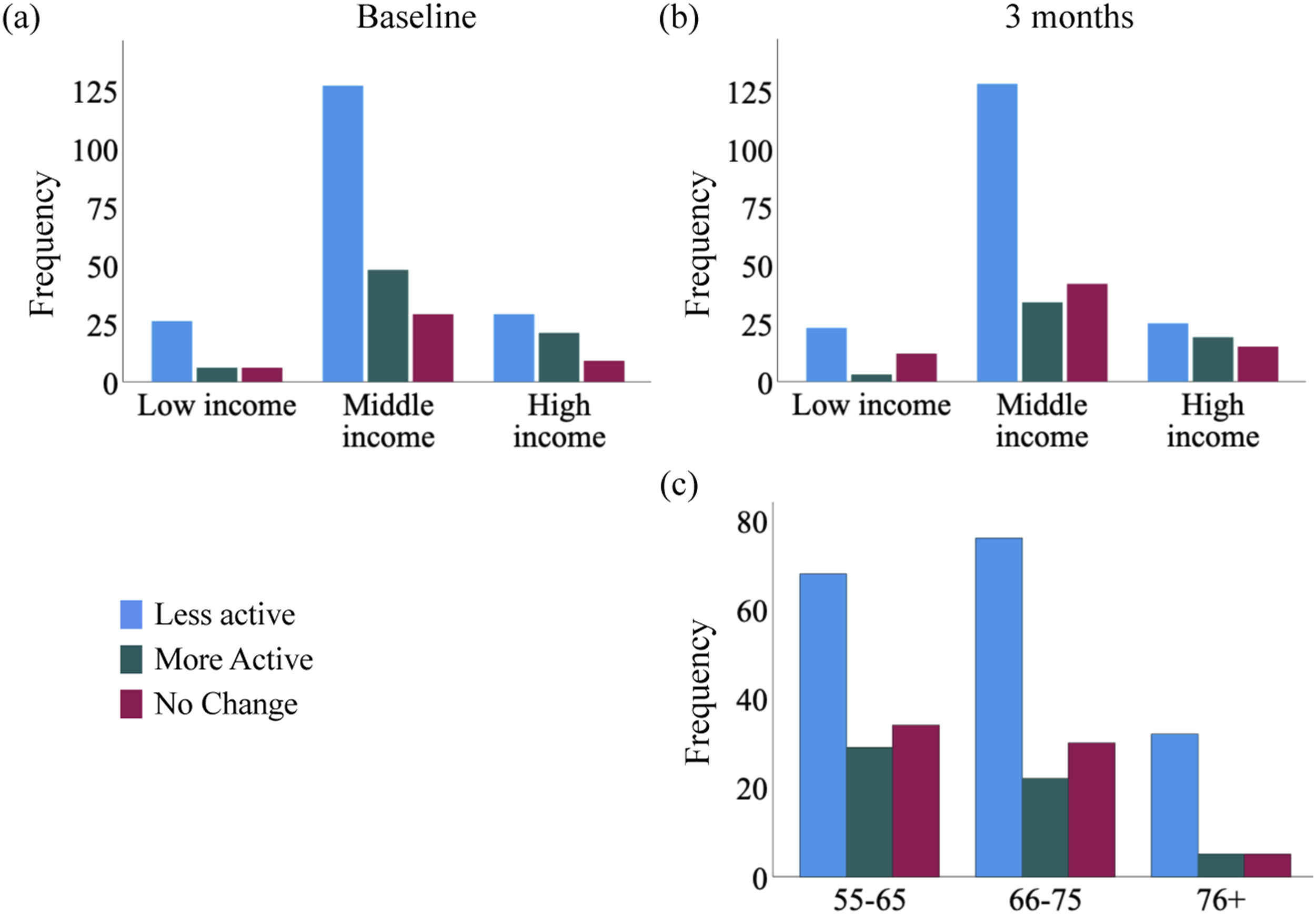
At the 3-month follow-up, the 55–65 age group reported being significantly less active than the 76+ group (X2 (1, N = 139) = 5.28, p = .02) (Figure 3(c)). There were no significant differences with the other age groups. Physical activity levels did not differ between males and females or part-time versus full-time employment.
Discussion
This study investigated whether there were self-reported changes in physical activity in older adults residing in the US during the first months of the COVID-19 pandemic in 2020, when strict social distancing mandates were in place. Specifically, we investigated whether changes in physical activity during the COVID-19 pandemic were associated with subjective cognitive decline, anxiety, and depression over a 3-month period, as well as whether changes in physical activity varied based on age, sex, income level, and employment status.
Our findings showed that most older adults reported a decrease in their physical activity (60% during baseline and 58% at the 3-month follow-up), and fewer participants reported having increased (25% during baseline, 19% at the 3-month follow-up) or maintained the same physical activity levels as before the pandemic (15% during baseline, 23% at the 3-month follow-up). These findings are consistent with other studies that included participants from France, Switzerland, and Italy (Cheval et al., 2021; Maugeri et al., 2020). Overall, a decrease in physical activity level was associated with greater subjective cognitive decline, as well as greater symptoms of anxiety and depression.
There were also significant differences in physical activity levels based on income (during baseline and the 3-month follow-up) and age, but not on sex or employment status. Higher-income earners reported engaging in more physical activity than before the pandemic in comparison with low- and middle-income earners. Further, participants between the ages of 55–65 years reported being less active compared to before the pandemic than the ones who were 76+ years old. Altogether, these findings show that reduced physical activity is associated with greater cognitive concerns and psychological distress, and that changes in physical activity may vary by age and income level during physical and social isolation.
Older adults often report feeling more socially isolated compared to when they were younger, which was likely exacerbated by the COVID-19 pandemic (Boden et al., 2021). As social creatures, isolation often has deleterious effects on health and overall well-being (Hammig, 2019). For instance, social isolation and loneliness during the pandemic have been associated with greater subjective cognitive decline in older adults (Pluim et al., 2023). The current study suggests that the isolation imposed by the COVID-19 pandemic also led to reductions in physical activity in most older adults, which was associated with worse mental and cognitive health. However, the deleterious effects of reduced physical activity extend beyond mental health and cognition. For instance, studies have shown that people who are physically inactive are at a greater risk for falls, cancer, cardiovascular disease, dementia, low-grade systemic inflammation, and obesity (Burini et al., 2020; Kerr et al., 2017; Warren et al., 2010; Yan et al., 2020). As such, behavioral changes associated with the COVID-19 pandemic may be a threat to healthy aging and psychological well-being. More research is needed to understand the long-term consequences of having reduced physical activity during the pandemic.
It is likely that increasing physical activity can lead to improvements in mental and cognitive health. However, it may be the case that rather than lower physical activity leading to greater cognitive concerns and neuropsychiatric symptoms, those with greater neuropsychiatric symptoms were more likely to reduce their physical activity levels (Steinmo et al., 2014). This would suggest that greater efforts to improve mental health could result in a more physically active lifestyle.
Some limitations of the study must be acknowledged. First, self-reported data may introduce recall bias and social desirability bias. In our study, all data was self-reported and we had no objective measures of physical activity, cognitive functioning, or medical and clinical data about participants that may have limited their physical activity levels. Also, since income level was self-reported through broad categories (low, middle, high, etc.), participants may have used different criteria to determine how to identify their socioeconomic status, making it difficult to know how uniform this self-identification is. We also did not have data quantifying how much time participants spent engaging in different types of physical activity (e.g., aerobic and strength training). In addition, we cannot infer causality from the existing data. Future studies should also consider the recruitment and retention of a more sociodemographically diverse sample (Blumenthal et al., 2020). Lastly, it would be important to understand which individual and environmental factors beyond age and income level (e.g., access to recreation space, personal motivation, and medical advice) allowed individuals to maintain their physical activity levels.
However, our study also has multiple strengths. We were able to evaluate several variables of interest longitudinally. Having multiple points allowed us to consider how physical activity levels and cognitive concerns may have changed over time and how sociodemographic variables related to physical activity engagement. We also used validated scales of subjective cognitive concerns, depression, and anxiety. Lastly, the size of our sample is also a strength of our study.
Altogether, the COVID-19 pandemic has had detrimental impacts on people’s physical and mental health. Almost four years after, we have learned that the COVID-19 pandemic has had immediate and long-term health consequences, including greater sleep disturbances, difficulties accessing healthcare services, reduced quality of life, and increased loneliness in older adults (Bailey et al., 2021; Lebrasseur et al., 2021). It is important to consider how our results and those of others could extrapolate to other challenging periods that require confinement and lifestyle changes. This knowledge can prepare us, individually and collectively, for future similar events to the COVID-19 pandemic that result in isolation.
Our study has broader practical implications as social confinement or isolation continues to be prevalent in older adults, particularly after the pandemic. Attention must be given to lifestyle factors that could be implemented rapidly, such as at-home physical activity interventions that can improve quality of life, cognitive function, and overall well-being. Online physical activity programs may also be considered and promoted. Similarly, public health systems could create programs specifically targeted to the older adult population that would consider their social and physical needs. This way, older adults may be more motivated to engage in physical activity programs, given that their other important needs are also being met. In addition, civic centers, spiritual and religious groups, community initiatives, and Area Agencies on Aging, among others, could be valuable sources of support, resources, education, and activities to promote greater well-being in the older adult population. Further, our study supports the evidence that income could be a limiting factor for older adults to stay active physically (Yang et al., 2023). Thus, increasing access to physical activity and mental health programs that are free or low-cost, as well as accessible transportation to them, could help modify unhealthy behaviors and be protective for overall health, better cognition, and emotional functioning.
Footnotes
Acknowledgments
We thank all participants for contributing their time to this study and their commitment to it.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Yakeel Quiroz serves as a consultant for Biogen. All other co-authors have no conflicting interests to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (NIH) [grant number 5T32HL007901-23]; National Institute on Aging (NIA) [grant numbers K23AG 061276, R01 AG054671, R01 AG074302, R01 AG068183, R01 AG067428, R01 AG056466, R01 AG080469, and K99AG073452]; National Research Service Award (NRSA) support from the NIH NIA [grant number F31AG06215801 A]; Alzheimer’s Association [grant numbers 2019A00585 and AACSFD-21-853089]; BrightFocus Foundation [grant number A2021142S]; and National Institute on Aging (NIA) pilot project from the Center for Aging in Diverse Communities [grant numbers UCSF 2P30AG015272-21, 3P30AG062421-01S1, R01AG066823-01A1, and 5P30AG062421-03].
Institution of the Review Committee
The study was approved by the institutional ethics review board of Massachusetts General Hospital in Boston, Massachusetts (IRB protocol number: 2020P001131).