
Abstract
Guided by the Rowe and Kahn model, the current study examined the longitudinal association of objective and subjective components of successful aging (SA) with individuals’ life satisfaction and level of optimism across adulthood aiming to validate the related scanty existing research. Data were from waves 2 and 3 (2004–14) of the Midlife in the United States (MIDUS) study. Using structural equation modeling, we examined (N = 2,040) whether subjective life satisfaction (wave 2) has any effect on a composite measure of SA (wave 3) while controlling for baseline sociodemographic and health factors. We also examined the mediation effects of optimism in the above associations. Findings revealed that life satisfaction has a significant positive effect on SA; also, this effect is bidirectional. Further, high optimism positively mediated the bidirectional association between life satisfaction and SA. This study identified life satisfaction and optimism as having potentially positive impacts on achieving SA in middle-aged and older adults.
Keywords
• The current study expands prior work by examining the association of individuals’ life satisfaction with objective and subjective components of successful aging. • The findings revealed that life satisfaction has a positive and bidirectional effect on successful aging in US middle-aged and older adults. • Further, high optimism positively mediated the bidirectional association between life satisfaction and successful aging.
• While successful aging is often examined in relation to various risk/protective factors in late life, this study identified some psychosocial factors as having potentially positive impacts on achieving successful aging across adulthood. • These findings have direct practical applications, whereby promotion of social interaction and encouragement of optimistic views of life may guide health care professionals to promote successful aging in their middle-aged and older clients. • Future research should consider ways to examine successful aging as a composite objective/subjective measure to more finely examine aspects of individuals’ well-being.What this paper adds
Applications of study findings
Introduction
Researchers have described successful aging (SA) from different perspectives; these theoretical frameworks include either objective or subjective evaluations or both (Cosco et al., 2013; Pruchno et al., 2010; Zhang et al., 2018). For example, Depp and Jeste (2006) have reported 29 separate definitions of SA. However, a comprehensive definition of SA should incorporate biopsychosocial measures; instead of only biomedical ones (Jeste et al., 2010). While defining SA, on the one hand, most Western definitions describe freedom from disease and disability (Jeste et al., 2010); on the other hand, non-Western literature mostly focuses on adaptation, meaningfulness, connection, acknowledgment, and spirituality (Lamb, 2014).
One of the most well-known theories of SA was proposed by Rowe and Kahn (1997), emphasizing a combination of three objective criteria, that is, low probability of disease and disability, high cognitive and physical functioning, and active engagement with life (Chen et al., 2020; Fasoro et al., 2023; Manierre, 2019; Zhang et al., 2018). Although the theory focuses on late adulthood, critics note that it fails to capture social relationships and late-life developmental processes by entirely focusing on late adulthood as a static point to assess an individual’s “successful aging,” ignoring dynamic perspectives in later life (Stowe & Cooney, 2015). For example, research has documented that cognitive functioning, such as concentration, visual and verbal memory, attention and processing speed, language, executive function, spatial and/or psychomotor ability show long-term decline with age in adulthood (Yang et al., 2020).
Jeste and colleagues (2010) found chronological age as an objective predictor of SA. In other words, those who attain long life may successfully control many age-related disorders. In this context, some scholars found Rowe and Kahn’s theory a useful framework for examining longevity (Paulson et al., 2011). However, many others do not consider the theory to be useful regarding longevity (Nosraty et al., 2019). This is because, for some scholars, longevity is a relative term that considers the life expectancy of individuals of a specific country or population, while for others, it is an absolute term related to the maximum human lifespan (Aiello et al., 2016). Paulson and colleagues (2011) found that the oldest women in their study had fewer cerebrovascular problems, better cognitive performance, and a lower level of depressive symptoms. The study also revealed that both SA and longevity were associated with lower levels of depression and higher cognitive function (Paulson et al., 2011). Paulson et al. interpreted Rowe and Kahn’s conceptualization of SA from the context of overall quality of life, that is, adding life to years, not adding years to life while sick. They found that a rapid decline in physical and cognitive functions is closely associated with mortality while higher functioning is associated with longevity. In fact, Rowe and Kahn (2015) also considered age an under-emphasized factor in their earlier framework and argued that society should consider older adults’ life trajectories including their life experiences as resources.
Previous studies also found SA to be related to many factors, such as gender, marital status, workability, practicing healthy activities, social interaction, and strong religious beliefs (Kim, 2023; Pruchno et al., 2010). For example, in a meta-analysis, Depp and Jeste (2006) found that nearly half of the reviewed longitudinal studies report that women were more likely to experience SA than men. However, most of these findings emphasize the role of socio-behavioral factors. While objective components (e.g., physical activity) are easier to assess, subjective evaluation (e.g., social relations, positive outlook) depends on the personality and psychological adaptability of the specific person (Bhattacharyya et al., 2023). Although Rowe and Kahn’s (1997) earlier model did not include subjective perceptions of well-being as determinants of SA, they acknowledged the necessity of considering subjective components of SA in their more recent essay “Successful aging 2.0,” which refines the original model to more actively take into account structural constraints (Rowe & Kahn, 2015).
Indeed, research has documented that although physical functionality is an important factor to age successfully, at an advanced age, psychosocial determinants are more realistic indicators of SA than physical health only (Zhang et al., 2018). For example, the concept of interpersonal relationship is not limited to the nuclear family, merely including parents and their biological children. Siblings, aunts and uncles, cousins, grandparents, unmarried, step-relatives, and adopted cohabitants can all be considered part of a family. Moreover, friends and neighbors are also important parts of one’s social environment. In other words, an extended multi-generational family along with neighbors constitutes the horizontal (siblings, cousins, and so on), vertical (grandparents, parents, children, and so on), and complex social relationships that exist between individuals sharing the same environment and with whom they interact daily (Scott Crapo & Bradford, 2021). Therefore, maintaining social relationships is integral for active engagement with life. Further, a recent scoping review found that apart from physical activity and basic aspects of well-being, satisfaction with life and optimistic outlook are also important for SA; however, the findings did not determine longevity to be a primary component of SA (Bhattacharyya et al., 2023).
In this context, Diener differentiated between cognitive-evaluative and affective components of subjective well-being; the affective component refers to the experience of positive and negative affect and the cognitive-evaluative component refers to overall subjective judgments of life circumstances, that is, life satisfaction (Diener et al., 2002; Karataş et al., 2021). Recent literature emphasizes life satisfaction as a good indicator of older adults’ quality of life, and thus, a good predictor of SA (Torregrosa-Ruiz et al., 2021). Many older adults experience a sense of life satisfaction even after multiple losses as they age (Torregrosa-Ruiz et al., 2021). Life satisfaction can be accomplished through social support (Lee et al., 2020), through happiness, positive outlook, and purpose in life (Karataş et al., 2021), and through good physical and psychological health behavior and practices (Karataş et al., 2021). Research also has found that older adults, who have high level of perception of SA, also have a high level of life satisfaction (Kars Fertelli & Deliktas, 2020). Regarding maintaining a positive outlook, optimism is a more trait-like and thus relatively stable psychological attribute eliciting an individual’s hope of expecting good things to happen and is considered a facet of positive psychological well-being (Ferguson & Goodwin, 2010). In this context, dispositional optimism (Scheier & Carver, 1985) considers optimism as a positive factor toward achieving future goals and objectives. This theory considers that optimism helps individuals to achieve positive consequences in life, but individuals with pessimistic thoughts put the least effort into achieving their goals because they believe their efforts will be of no avail, leading to stress and more dissatisfaction (Molero et al., 2022). Prior research has revealed that an optimistic outlook is correlated with better physical and psychological outcomes compared to a pessimistic one (Conversano et al., 2010), and thus, it might be a meaningful predictor of both life satisfaction and SA. Indeed, some recent studies proposed optimism as an important construct in understanding SA (Carver & Buchanan, 2016; Nakamura et al., 2022); optimism has been associated with life satisfaction and both have similar beneficial effects on individuals’ health (Carver & Buchanan, 2016).
From the perspective of the current study, the Rowe and Kahn’s “SA 2.0” model provides an appropriate theoretical framework to incorporate multidimensional biopsychosocial factors. Despite having some under-emphasized areas, this model prominently acknowledges life course perspectives and to this date remains the most widely applied model of SA. Following Rowe and Kahn, this study views SA as a composite measure based on three criteria that include high cognitive and physical functioning, low level of disease and disability, and active engagement with life; it considers successful agers as those with higher scores in cognition, with minimal difficulties in performing physical activities, free of multiple chronic conditions, and maintaining active engagement with life. Previous research has extensively studied various concepts of SA; however, little is documented, to date, about the longitudinal associations of SA measures with life satisfaction of middle-aged and older adults in a nationally representative sample (Kars Fertelli & Deliktas, 2020), and how this association is influenced by level of optimism. The current study therefore expands prior work by examining the association of individuals’ prior subjective life satisfaction with objective and subjective components of SA (and vice versa), and by evaluating whether high level of optimism has any role in mediating these associations. This study was designed to extend contributions to the earlier literature in this area using data from a large longitudinal sample of middle-aged and older adults in the US while controlling for well-documented correlates of SA, including sociodemographic and health factors. We hypothesized that (i) individuals’ prior subjective life satisfaction has a positive effect on achieving SA, and also, SA positively impacts individuals’ life satisfaction, and (ii) high level of optimism mediates these associations.
Method
Data
The current study used data from the Midlife in the United States (MIDUS) survey, a nationally representative longitudinal study spanning 20 years. MIDUS was initiated in 1995–1996 (wave 1), with 7,108 English-speaking participants aged 24–75 years; participants in the contiguous US states were recruited through random digit dialing (Lachman et al., 2014). Follow-up waves 2 and 3 were conducted, respectively, in 2004–05 with 75% of the eligible original respondents in wave 1 (N = 4,963), and in 2013–14 with 77% of eligible (N = 3,294) wave 2 participants (Lachman et al., 2014).
Study Sample
In the current study, we included data from 2,040 individuals who participated in waves 2 and 3 (2004–2014) and had no missing observations.
Measures and Procedure
Dependent Variable
In keeping with the Rowe and Kahn model, we used a composite measure of SA as the dependent variable in our study. To obtain a multidimensional SA score, we considered cognitive and physical functions, engagement with life, and chronic conditions as follows.
To evaluate cognitive function, MIDUS used the Brief Test of Adult Cognition by Telephone (BTACT) (Lachman et al., 2014), which assesses participants’ cognitive performances through seven cognitive tests, including two measures of episodic memory (immediate and delayed free recall of 15 words), inductive reasoning (measured by number series completion), category verbal fluency (measured by verbal ability and fluency in 60 seconds), working memory span (measured by backward digit span), processing speed (measured by 30-Second and Counting Task, or 30-SACT), and attention switching and inhibitory control (measured by Stop and Go Switch Task, or SGST, calculating reaction times) (Lachman et al., 2014). Results of factor analyses for cognitive tests in MIDUS were reported by Lachman and colleagues (2014). MIDUS standardized the cognitive test scores (mean [M] = 0; standard deviation [SD] = 1) and a higher z-score indicated higher cognitive functioning. In the current analysis, we considered the nearest integer value of the mean-central score as the cutoff and categorized cognitive function as higher (=1 for score >0) and lower (=0 for score 0≤).
For evaluating physical function, participants were asked, through a functional status questionnaire, whether they had difficulty (i.e., functional limitations) in instrumental activities of daily living (IADL, which included activities of daily living [ADL] and some other activities, such as lifting or carrying groceries, climbing several flights of stairs, bending, kneeling, or stooping, walking more than 1 mile or walking several blocks, or moderate activities [e.g., bowling, vacuuming]). The responses in MIDUS were coded in four categories from 1 = a lot to 4 = not at all, and scales were constructed by calculating a composite score from the mean of all the reverse-coded values of the items in each scale with higher scores indicating more functional limitations. In the current analysis, following LaPlante (2010), physical function was represented using a combined IADL/ADL scale. We considered the nearest integer value of the composite mean-central score as the cutoff and categorized physical function as higher (=1 for score <2) or lower (=0 for score ≥2).
In the US, more than half of all older adults and nearly three-fourth of Medicare beneficiaries are living with multimorbidity, that is, concurrently having 2 or more diseases (Jindai et al., 2016). Therefore, to evaluate chronic conditions, we categorized participants dichotomously to indicate whether they were free from multiple (≥2) chronic conditions (1 = yes, 0 = no), as suggested in the earlier literature (Jindai et al., 2016). The conditions included high blood pressure, stroke, heart problems, high cholesterol, diabetes, cancer, lung problem, ulcer, anxiety/depression, and aches/joint stiffness in the past 12 months.
To evaluate engagement with life, we considered the MIDUS variable “Positive Relations with Others,” a 7-item scale in the SAQ; we categorized participants using a dichotomous code. The sample questions included whether, “Most people see me as loving and affectionate” (R), “Maintaining close relationships has been difficult and frustrating for me,” “I often feel lonely because I have few close friends with whom to share my concerns,” and “I enjoy personal and mutual conversations with family members and friends” (R). Response options ranged from 1 (strongly agree) to 7 (strongly disagree); some items (indicated as “R”) were reverse-coded. The “Positive Relations with Others” score is constructed in MIDUS by calculating the sum of the values of the items in each scale (score range 14–49); higher values indicate an individual’s higher engagement with life. In MIDUS, scores were considered missing if participants answered fewer than four scale items. For the current analyses, we considered the nearest integer value of the mean-central score as the cutoff and categorized engagement with life as higher (scores > 31 coded with a [1]) or lower (=0 for score ≤ 31).
In the current analysis, we constructed a composite score for SA using sum of the binary values of cognitive and physical function, chronic conditions, and engagement with life (score range 0–4); higher values indicate an individual’s higher level of SA across the 4 domains of SA.
Key Independent Variable
We used life satisfaction as the key independent variable. The life satisfaction score is based on a 5-item SAQ; for each item, MIDUS asked the participants to rate their life based on overall, work, health, relationship with spouse/partner, and relationship with children (Prenda & Lachman, 2001). Responses were coded from zero (the worst possible) to 10 (the best possible). First, MIDUS averaged the scores for the relationship with spouse/partner and relationship with children to create one item. Then, this score was used along with the remaining three items (life overall, work, health) to calculate an overall (average) mean score; higher scores reflecting better overall life satisfaction. Next, MIDUS computed the score for cases that have valid values for at least one item on the scale (score range 1–10). The score for the life satisfaction was not calculated for cases with no valid item and was identified as missing data. For the current analyses, we considered the average (mean) score provided in MIDUS for the entire range of responses on life satisfaction.
Mediator Variable
We used individuals’ level of optimism as the mediator variable in our analysis. For level of optimism, we considered the variable “Overall Optimism,” a 6-item scale in the SAQ in MIDUS. The scale combined the 3 “optimism” items (sample question: whether “In uncertain times, I usually expect the best,” “I’m always optimistic about my future,” and “I expect more good things to happen to me than bad.”) and the 3 “pessimism” (sample question: whether “I rarely count on good things happening to me”) items, using the Life Orientation Test-Revised (LOT-R) as described by Scheier and colleagues (1994). Response options ranged from 1 (a lot agree) to 5 (a lot disagree); items were reverse-coded so that higher scores represent higher levels of optimism (score range 6–30). The optimism score was considered missing if participants answered fewer than three scale items. In the current analyses, we considered the average (mean) score provided in MIDUS for the entire range of responses on overall optimism.
Covariates
We used six sociodemographic factors as covariates: age, gender, race, marital status, education, and employment. Age was split into two categories: Older adults (≥65 = 1) and middle-aged (<65 = 0). Gender (0 = male, 1 = female) was a binary variable, and Race (1 = White, 2 = Black, 3 = other) was measured in three categories; in contrast, marital status (1 = married, 2 = separated/divorced, 3 = widowed, 4 = never married) and educational level (1 = no/some school, 2 = high school graduate/in college, 3 = graduated from college, 4 = having master’s/professional degree) were measured in four categories. Employment status was measured in five categories (1 = currently working, 2 = self-employed, 3 = retired, 4 = unemployed, 5 = other). We included other variables related to health behavior that included tobacco and alcohol use (1 = regular tobacco/alcohol user, zero otherwise).
Statistical Analysis
Demographic Characteristics of Adults in MIDUS Wave 3 (N = 2,040).
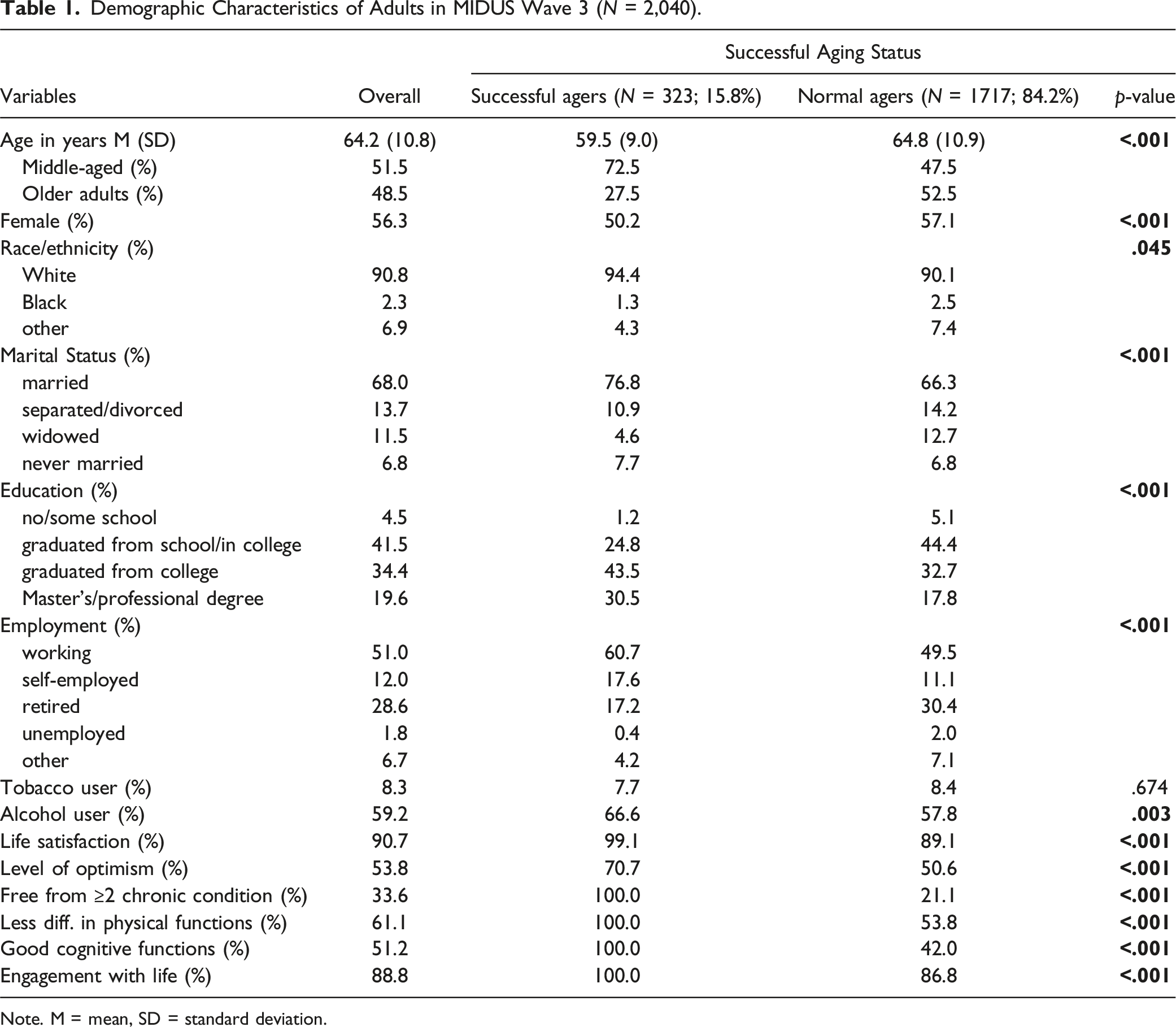
Note. M = mean, SD = standard deviation.
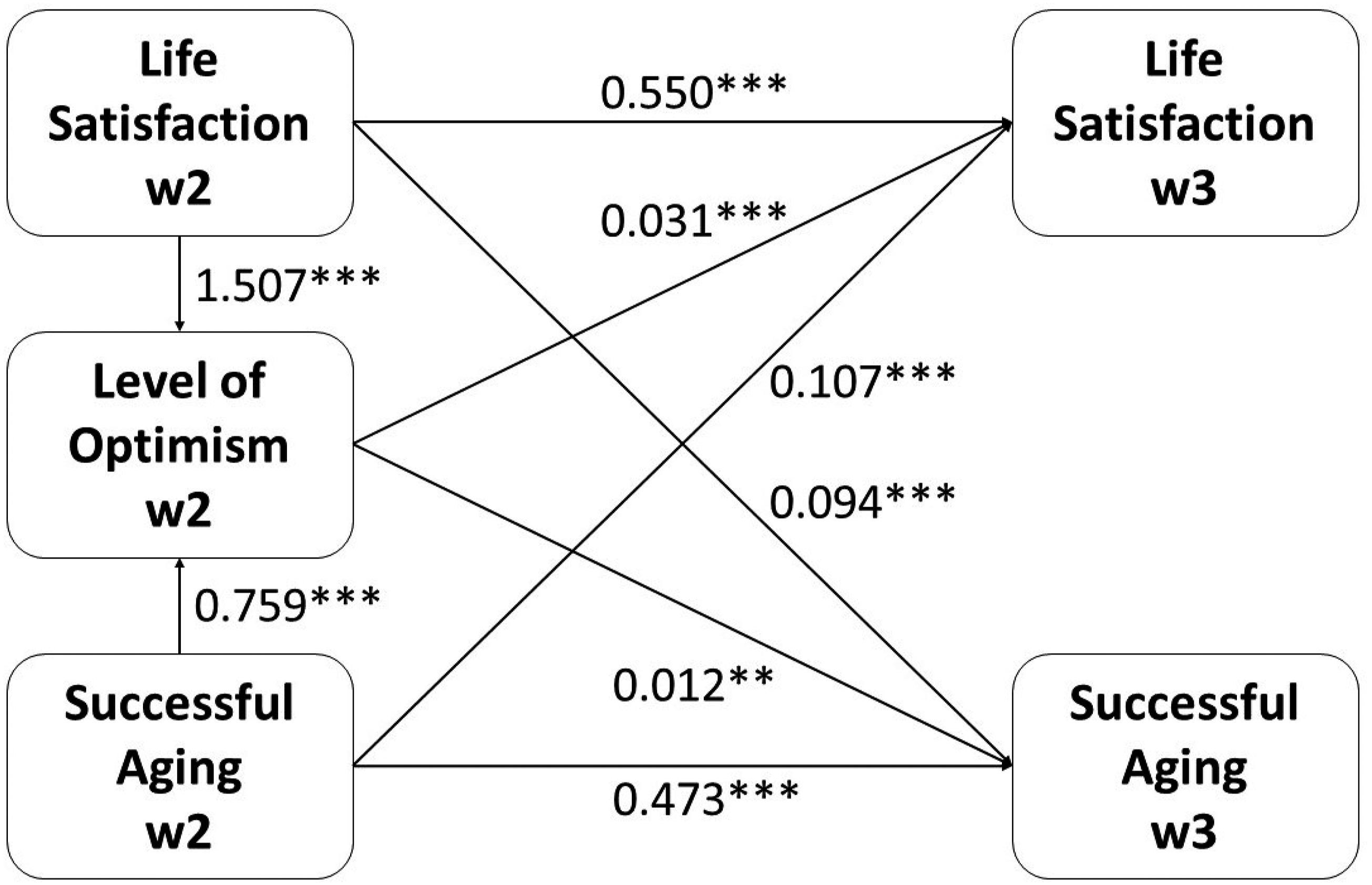
Structural equation models showing mediation effects of level of optimism on the association between life satisfaction and successful aging in mid and later life (N = 2,040; Model goodness of fit criteria: CFI = 0.966, RMSEA = 0.050, and SRMR = 0.008). Note. w2 = wave 2. w3 = wave 3. Covariates were included in each of the SEM equations; however, effects of covariates not shown in the diagram. ***p < .001; **p < .01; *p < .05.
Results
Correlations Between the Variables (i.e., Life Satisfaction, Optimism, and Indicators of Well-being) (N = 2,040).
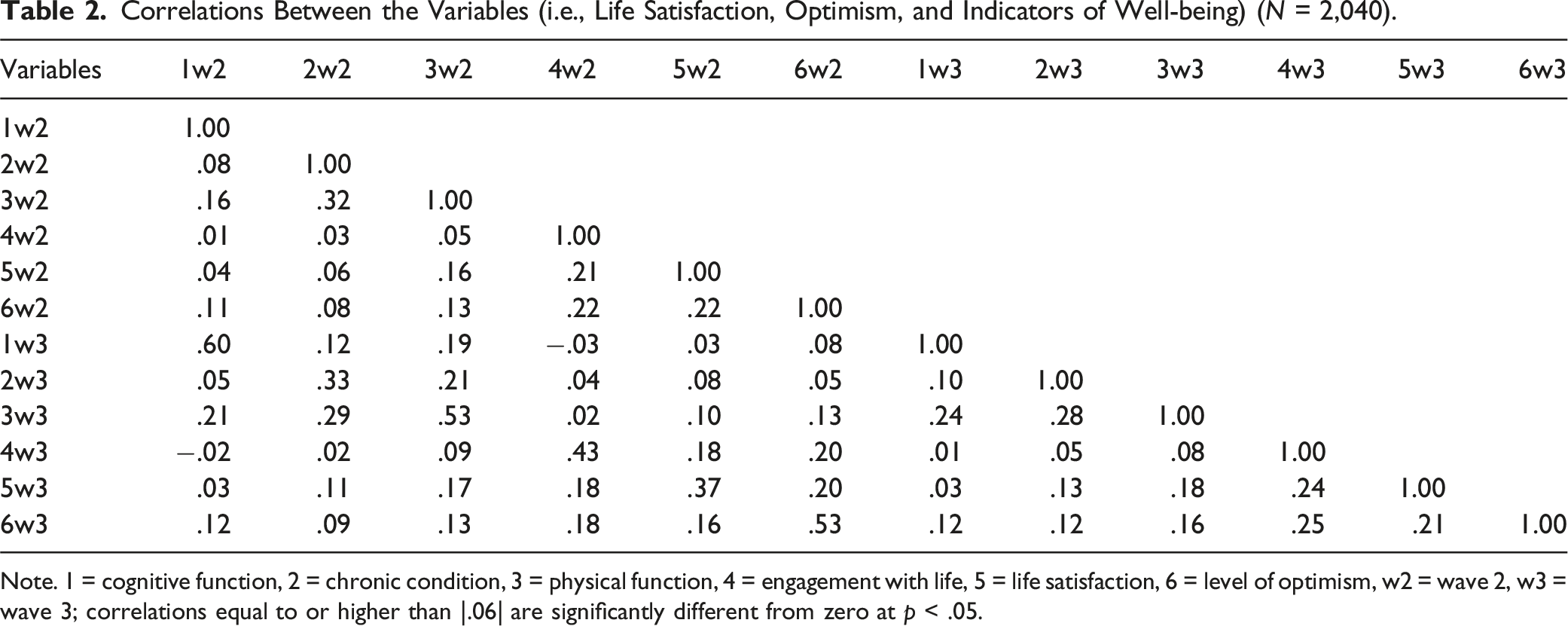
Note. 1 = cognitive function, 2 = chronic condition, 3 = physical function, 4 = engagement with life, 5 = life satisfaction, 6 = level of optimism, w2 = wave 2, w3 = wave 3; correlations equal to or higher than |.06| are significantly different from zero at p < .05.
Structural Equation Model Showing Mediating Roles of Levels of Optimism in the Association Between Life Satisfaction and Successful Aging in mid and Later Life Over 10 Years, Controlling for Covariates (n = 2,040).
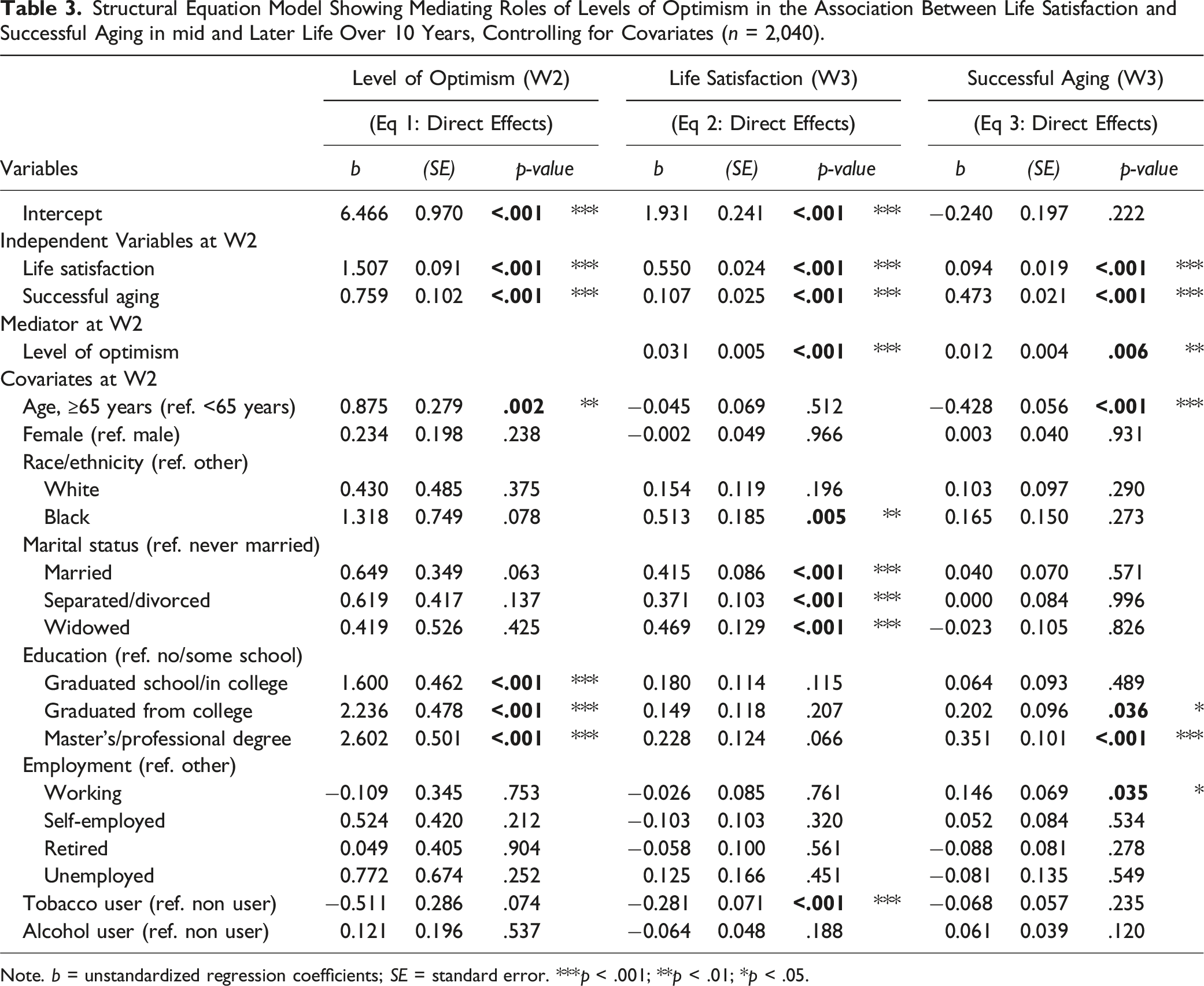
Note. b = unstandardized regression coefficients; SE = standard error. ***p < .001; **p < .01; *p < .05.
In Figure 1, we report results from the SEM regression model after controlling for sociodemographic and health factors. It shows the mediation effects of level of optimism in the associations between life satisfaction and SA. The model fit the data well (CFI = 0.966, RMSEA = 0.050, and SRMR = 0.008). In addition to the direct effect of life satisfaction on SA (and vice versa), the coefficient estimates for the mediating total indirect effects revealed that a high level of optimism has positive significant effects on the bidirectional associations between life satisfaction and SA.
In the mediation analyses to examine whether high level of optimism mediates the above associations, after controlling for covariates and prior level SA, for SA (W3), the total effect of life satisfaction (W2), .113, is the effect we would find if there was no mediator in our analysis; it is significant with a z of 6.20. The direct effect of life satisfaction is .094, which, while still significant (z = 4.87), is smaller than the total effect (see Supplemental Table 1). The indirect effect of life satisfaction that passes through high level of optimism is .019 and statistically significant. The findings revealed that the proportion of the total effect that is mediated through optimism is almost .17; the ratio of the indirect effect to the direct effect is about .20, and finally, the total effect is about 1.20 times the direct effect. We therefore conclude that high level of optimism mediates the relationship between life satisfaction (W2) and SA (W3). On the other hand, for life satisfaction (W3), the total effect of SA (W2) is .130; it is the effect we would find if there was no mediator in our model. It is significant with a z of 5.17. The direct effect of SA is .107, which, while still significant (z = 4.22), is smaller than the total effect (see Supplemental Table 1). The indirect effect of SA that passes through high level of optimism is .024, and statistically significant. The findings revealed that the proportion of the total effect that is mediated through optimism is almost .18. The ratio of the indirect effect to the direct effect is about .22; finally, the total effect is about 1.22 times the direct effect. Therefore, we conclude that high level of optimism mediates the relationship between SA (W2) and Life satisfaction (W3).
Discussion
Physical and cognitive functions, low morbidity, and engagement with life are three primary aspects of SA. Guided by Rowe and Kahn’s model, the multidimensional perspective of SA examines various aspects of individuals’ satisfaction with life and interpersonal experiences. The current study extended earlier research in a couple of ways: first, by examining how individuals’ prior satisfaction with life is bidirectionally associated with SA as a composite measure, and second, by examining how individuals’ level of optimism mediates this association between life satisfaction and SA.
In support of our first hypothesis, the current study revealed that prior life satisfaction has a potentially positive impact in achieving SA in MIDUS middle-aged and older adult populations. This finding is consistent with previous literature indicating that life satisfaction operationalized as one’s attitude toward life, such as eating habits, choice of food, self-actualization, and desires, impacts SA (Cherry et al., 2013; Yalcinoz-Baysal et al., 2020). Further, corroborating earlier literature, our result also supports that SA has a direct positive impact on individuals’ life satisfaction (Torregrosa-Ruiz et al., 2021). Regarding our second hypothesis, findings from our analysis corroborate the earlier literature showing an optimistic outlook, such as thinking about the potentials of the rest of their lives instead of focusing on deficits and losses, positively affects SA (Chen et al., 2020). Again, consistent with our findings, research has also shown that older adults feel better when sharing their experiences and stories with others, such as grandchildren making the dining atmosphere more enjoyable or an emotional conversation with close others sitting around a table helping them cope with various life stressors (Chen et al., 2020; Yalcinoz-Baysal et al., 2020).
We operationally defined SA as a combination of physical, mental, and social factors, with a connection to well-being that is mediated through personality (optimism). In this context, another theory of SA (Jeste et al., 2010) acknowledges two fundamental components of SA, objective and subjective, may diverge; the former as measurable physical and mental factors, and the latter as adaptation within society and purpose in life. For example, Strawbridge and colleagues (2002) found that more than half of the research participants considered themselves successful agers by self-ratings, while less than a fifth met the objective criteria.
Although some earlier research found that longevity is not an essential component of SA (Bhattacharyya et al., 2023), our findings on covariates indicate that age (older adults compared to middle-aged) is negatively associated with SA, which is in line with a few other research studies (Yalcinoz-Baysal et al., 2020). Relatedly, it is already evidenced that successful agers care more about overall quality of life, not the lifespan only (Wahl, 2020). Also, contrary to earlier research (Lang et al., 2013), we found that older adults are more optimistic. According to our SA criteria, women were less likely to be categorized as successful agers than men, which is opposite the earlier findings (Depp & Jeste, 2006). However, this difference is no longer significant after controlling for additional variables. Further, corroborating earlier research, the current findings suggest that successful agers have more educational attainment (Cosco et al., 2013). The current findings also suggest that one of the factors that affects SA was employment status. This result is consistent with the results of other studies conducted on SA whereby working people consider themselves as successful agers (Kars Fertelli & Deliktas, 2020).
In sum, SA appears to be a multidimensional concept that may help guide individuals to age well; it is an accomplishment that is mostly reflected in one’s quality of life (Zhang et al., 2018). Although Rowe and Kahn’s original theory (1997) was grounded on three interrelated factors largely based on objective measurements, many suggest that it needs to include subjective measures (Pruchno et al., 2010; Rowe & Kahn, 2015; Zhang et al., 2018). The current study was designed to incorporate both, because in addition to more objectifiable criteria, we considered positive relations with others an indicator engagement with life, thus an indicator of SA. Relatedly, while we did not examine associations between different indicators of SA, other studies have found these associations; for example, increased social engagement has a beneficial effect on cognitive functioning among older adults (Krueger et al., 2009). Previous research also found that social engagement was significantly associated with higher levels of life satisfaction among older adults (Chu & Koo, 2023). Further, physical activity undoubtedly increases cognitive functioning among older adults (Bhattacharyya et al., 2022). Also, preserved cognitive functioning is essential for older adults to remain active and healthy (Hertzog et al., 2008). These factors, in turn, help older adults to lead an independent lifestyle and stay socially involved, thus serving to reduce loneliness, boredom, and helplessness.
Limitations
The main strength of the current study is its large sample size; however, it has some limitations. For example, as MIDUS did not screen the participants for cognitive impairment at baseline, we were unable to determine the neurocognitive status of the participants in our sample. Another limitation is related to recall bias because responses were collected retrospectively. For example, participants were asked to report health conditions experienced in the last 12 months. Therefore, the current negative association between age and SA may be a measurement issue with more older adults having cognitive impairment, greater levels of comorbidity, and less socialization. Also, the racial make-up of this study sample is predominantly White, inducing generalizability concerns, and future research should include a representative number of African Americans, Hispanics, and Asians. Further, given limited guidance from the literature, we applied deviation from the mean-central value to identify cutoff values for categories of SA. Additionally, our definition of chronic conditions as “free of multiple chronic conditions,” is consistent with the literature but nonetheless somewhat restrictive. We only considered those conditions included in MIDUS; obesity, hearing, and vision defects were important omissions. Although we considered body mass index (BMI) as a covariate and found that the results were unaltered (see Supplemental table 2). Further, multimorbidity (≥2 chronic conditions) is common among older adults in the US and MIDUS data does not provide information on whether chronic conditions were effectively managed with medications. Moreover, there are disagreements in the earlier literature regarding using binary versus nonbinary measures of SA − both regarding conceptualization and to establish an empirical foundation for measurement choices (Manierre, 2019). Our study adds to this existing literature by combining several binary measures of SA. Finally, although we used two latest available MIDUS waves, information in MIDUS is dated and may not be entirely representative of health and economic conditions that middle-aged and older adults face in current times.
Conclusions
While SA is often examined in relation to various risk/protective factors in late life, this study identified that life satisfaction and high level of optimism have a potentially positive impact on achieving SA in middle-aged and older adults. These findings have direct practical applications, whereby promotion of an optimistic outlook on life via positive psychology interventions may guide healthcare professionals to facilitate SA in their middle-aged and older clients. Psychological treatment has been shown to improve optimism (Malouff & Schutte, 2017). Relatedly, it should also be considered that more optimistic individuals often engage themselves in more meaningful activities, such as mentoring grandparents, and healthier behaviors, such as exercising, on the basis of their better physical and cognitive health and their sense that they can do the job (Roth et al., 2009). This self-selection bias could be a potential confound because it may make them perform better than less optimistic individuals in some specific cognitive/physical dimensions (Roth et al., 2015). These findings could also direct family caregivers and policymakers in preparing action plans accordingly. Further, while capturing engagement with life we mostly considered social aspects of engagement but did not address many vocational and avocational engagement activities. Therefore, future research should consider ways to examine SA as a composite objective/subjective measure filling these gaps to more robustly examine aspects of individuals’ well-being attributes, such as life satisfaction.
Supplemental Material
Supplemental Material - The Role of Life Satisfaction and Optimism for Successful Aging in Mid and Late Life
Supplemental Material for The Role of Life Satisfaction and Optimism for Successful Aging in Mid and Late Life in Kallol Kumar Bhattacharyya, Victor Molinari, Debasree Das Gupta, and Gizem Hueluer in Journal of Applied Gerontology
Footnotes
Acknowledgments
We acknowledge support from the Alzheimer’s Disease and Dementia Research Center at Utah State University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.