
Abstract
Annually, approximately 16% of adults aged 60 and older are victims of abuse in community settings. A critical first step toward effectively intervening and reducing the prevalence of elder abuse is to better understand the current state of knowledge, beliefs, and practices. This qualitative descriptive study explored the perceptions of US frontline community workers regarding elder abuse through focus groups and interviews conducted in the spring and summer of 2021. Participants represented various aging and victim services (n = 9), healthcare (n = 7), and law enforcement (n = 8). Thematic data analysis led to the emergence of three major themes in our data: societal influence, individual circumstances, and nature of abuse. Our findings point out several directions in which researchers and policymakers can begin moving the field forward. These include the need to focus on prevention strategies as well as the need to reduce ageist beliefs and attitudes.
• A deeper understanding of the current landscape surrounding abuse of older adults in community settings. • Evidence of ageism at multiple levels that inhibits effective response and prevention of elder abuse.
• Findings strongly point to the need to address ageism as an elder abuse prevention strategy. • Findings align with and support the World Health Organization’s recommendation to align policies and systems to optimize greater health and well-being for older adults.What this paper adds
Applications of study findings
Elder abuse is any intentional or negligent act that harms or increases risk of harm to older adults (National Center for Injury Prevention and Control, 2021), often committed by trusted individuals (U.S. Centers for Disease Control and Prevention, 2024). There are many forms of elder abuse, including physical, sexual, psychological, financial, neglect, and self-neglect (U.S. Centers for Disease Control and Prevention, 2024). Multiple forms of abuse can simultaneously co-occur (U.S. Centers for Disease Control and Prevention, 2024). Pre-pandemic, about 16% of older adults globally experienced abuse annually (Yon et al., 2017), rising to 21% annually post-pandemic (Chang & Levy, 2021). For each known case of elder abuse, as many as 24 cases are never reported (Lachs & Berman, 2011). Older adults who have experienced abuse are at risk of premature mortality (Yunus et al., 2019), multi-morbidity (Yunus et al., 2019), anxiety and depression (Acierno et al., 2017; Wong & Waite, 2017), poor functional health (Wong & Waite, 2017), hospitalization (Dong & Simon, 2013), feeling a sense of loneliness (Wong & Waite, 2017), and being placed in a long-term care facility (Lachs et al., 2002). Early recognition and effective response play key roles in reducing the occurrence and impact of elder abuse.
Research indicates that healthcare workers lack confidence and competence in recognizing elder abuse across various clinical settings (Braaten & Malmedal, 2017; Daly & Coffey, 2010; Gonzalez et al., 2016; Rosen et al., 2016, 2018). Contributing factors include lack of training (Gonzalez et al., 2016; Rosen et al., 2018) and insufficient knowledge of elder abuse (Braaten & Malmedal, 2017; Daly & Coffey, 2010; Rosen et al., 2016, 2018), as well as challenges to reporting elder abuse (Gonzalez et al., 2016). For example, a recent qualitative study revealed that radiologists reported having very little or no training in elder abuse detection and that these professionals never reported a suspected case despite believing they had encountered elder abuse (Rosen et al., 2016). Similarly, a sample of emergency department providers reported not routinely assessing for elder abuse (Rosen et al., 2018). These same providers reported overlooking abuse for various reasons, including a poor understanding of what constitutes elder abuse, inadequate training, challenges in distinguishing between mistreatment and standard age-related functional status, distrust of histories provided by older patients, and an absence of clear protocols to follow when elder abuse is suspected (Rosen et al., 2018).
As the world’s population ages, elder abuse is expected to rise (World Health Organization, 2022), posing significant costs and challenges despite decades of warning. Prioritizing the safety of older adults is a global priority, as highlighted by the United Nations’ call for re-evaluation and realignment of policies and programs to optimize quality of life and safety (United Nations Department of Economic and Social Affairs, Population Division, 2022). Unlike much of the research on elder abuse, our study delved into elder abuse in community-based settings to shed light on how various frontline workers respond to elder abuse individually and collaboratively. Thus, we conducted a qualitative descriptive study to answer the following research question: what is the current knowledge of abuse and beliefs about current practices and effectiveness of recognition and response, among central Virginia’s frontline community workforce?
Methods
Participants
Participants (n = 25) working with older adults in various settings were recruited through purposive sampling to take part in either a semi-structured focus group. Representatives from aging and victim services (n = 9), healthcare (n = 7), and law enforcement (n = 9) who worked in central Virginia in either an urban (n = 13), suburban (n = 9), or rural setting (n = 3) participated in this study. There was no prior acquaintance between study participants.
Procedures
All study procedures were approved by the Institutional Review Board of the researchers’ university (IRB Protocol: HM20020135). Participants were recruited online; electronic fliers were distributed through email listservs and advertised on social media. The three fields targeted for recruitment in the study—aging and victim services, law enforcement, and healthcare—were chosen because they are commonly included as members of multidisciplinary teams (MDTs) and are well-poised to interact with and recognize elder abuse in community settings. Interested participants contacted the project manager, who coordinated the scheduling of focus groups and interviews. The project manager then gave interested participants an information sheet detailing the purpose of the study as well as gathered informed consent from participants before adding them to the schedule of focus groups. Participants did not receive compensation for participating in the study. Five focus groups took place with three to five participants present. Two focus groups were scheduled to have three or more participants present but only one participant was able to attend. Three other participants were the only ones to sign up for their focus group timeslot; they were not available to join larger focus group sessions but were eager to participate. These five individuals were all interviewed one-on-one using the same semi-structured protocol.
All focus groups and interviews were conducted in the spring and summer of 2021 by the same researcher (AR) to ensure consistency across conversations. The questions began by asking participants to broadly consider and define what it means to be old and to be abused before moving specifically toward questions regarding their discipline’s role in response to abuse and what they believe other disciplines’ role is. Participants were also asked to comment on their experiences collaborating with other disciplines to respond to elder abuse. The full semi-structured protocol is in Appendix A. Given that we asked participants to discuss their experiences and perspectives in other disciplines, disciplines were not mixed during focus groups to ensure participants felt comfortable speaking openly about their experiences. All focus groups and interviews took place on teleconferencing software and were recorded; conversations ranged in length from 30 to 75 min. Audio-only recordings were sent to a third-party service for transcription.
Data Analysis
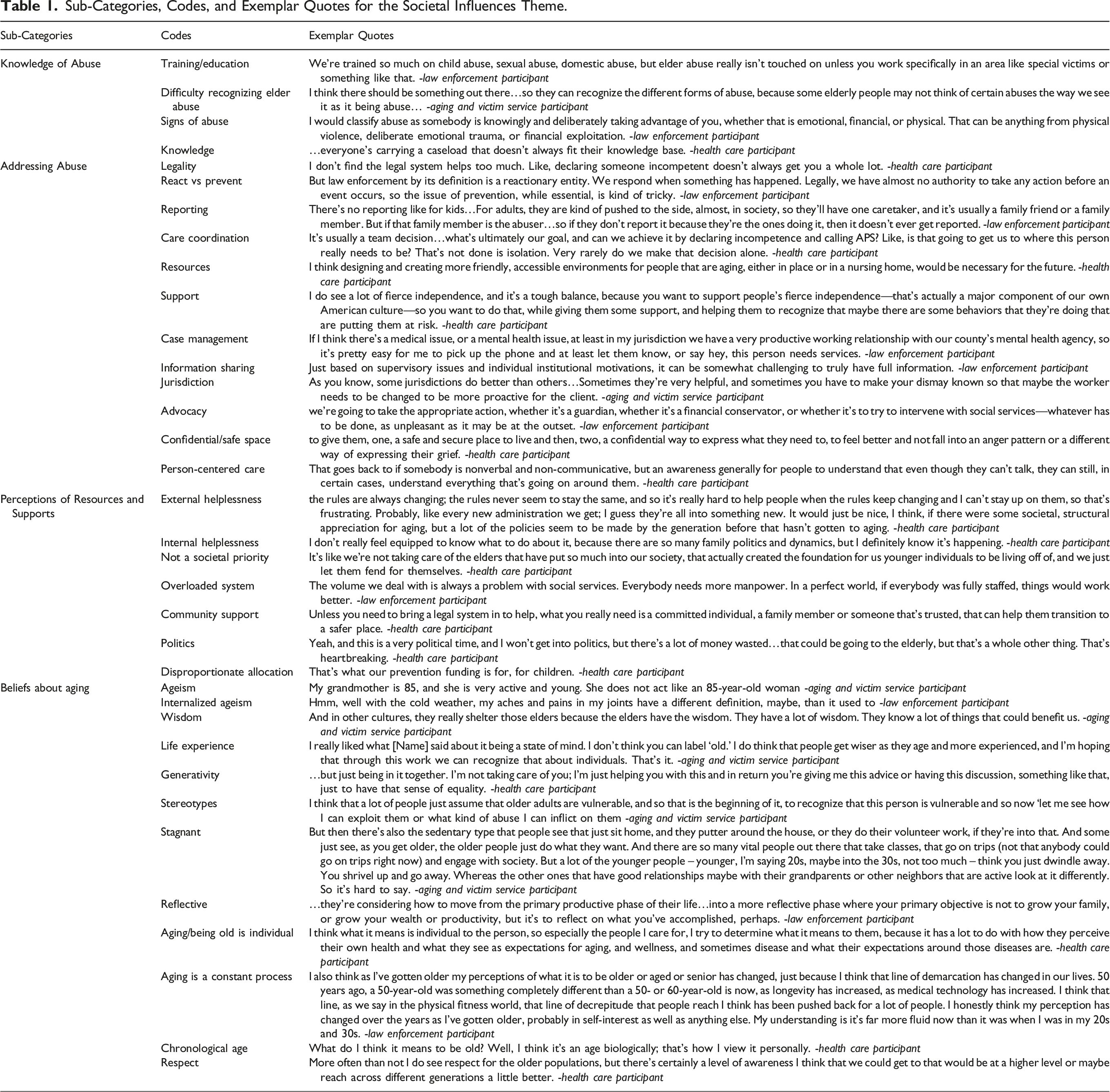
Sub-Categories, Codes, and Exemplar Quotes for the Societal Influences Theme.
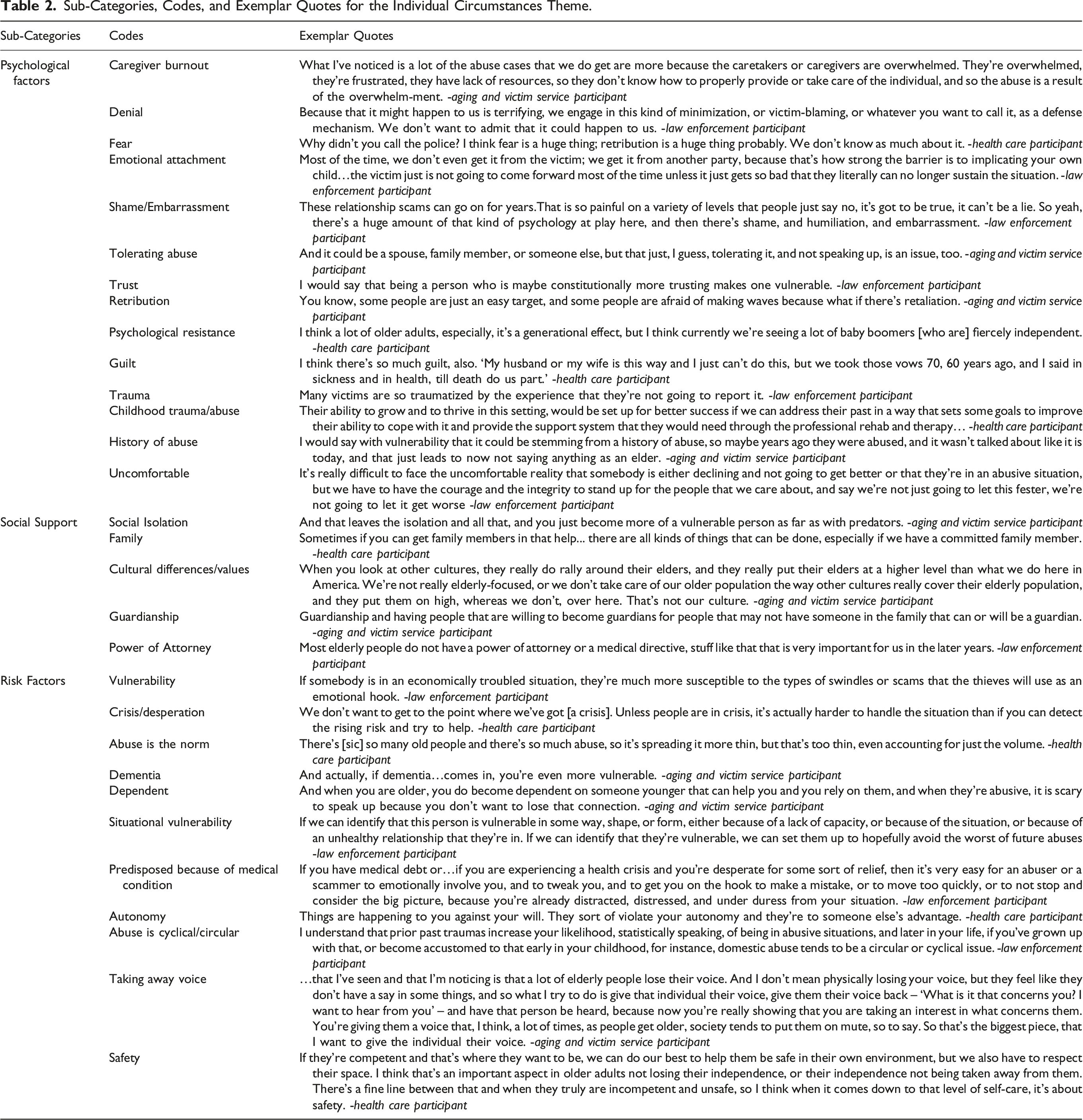
Sub-Categories, Codes, and Exemplar Quotes for the Individual Circumstances Theme.
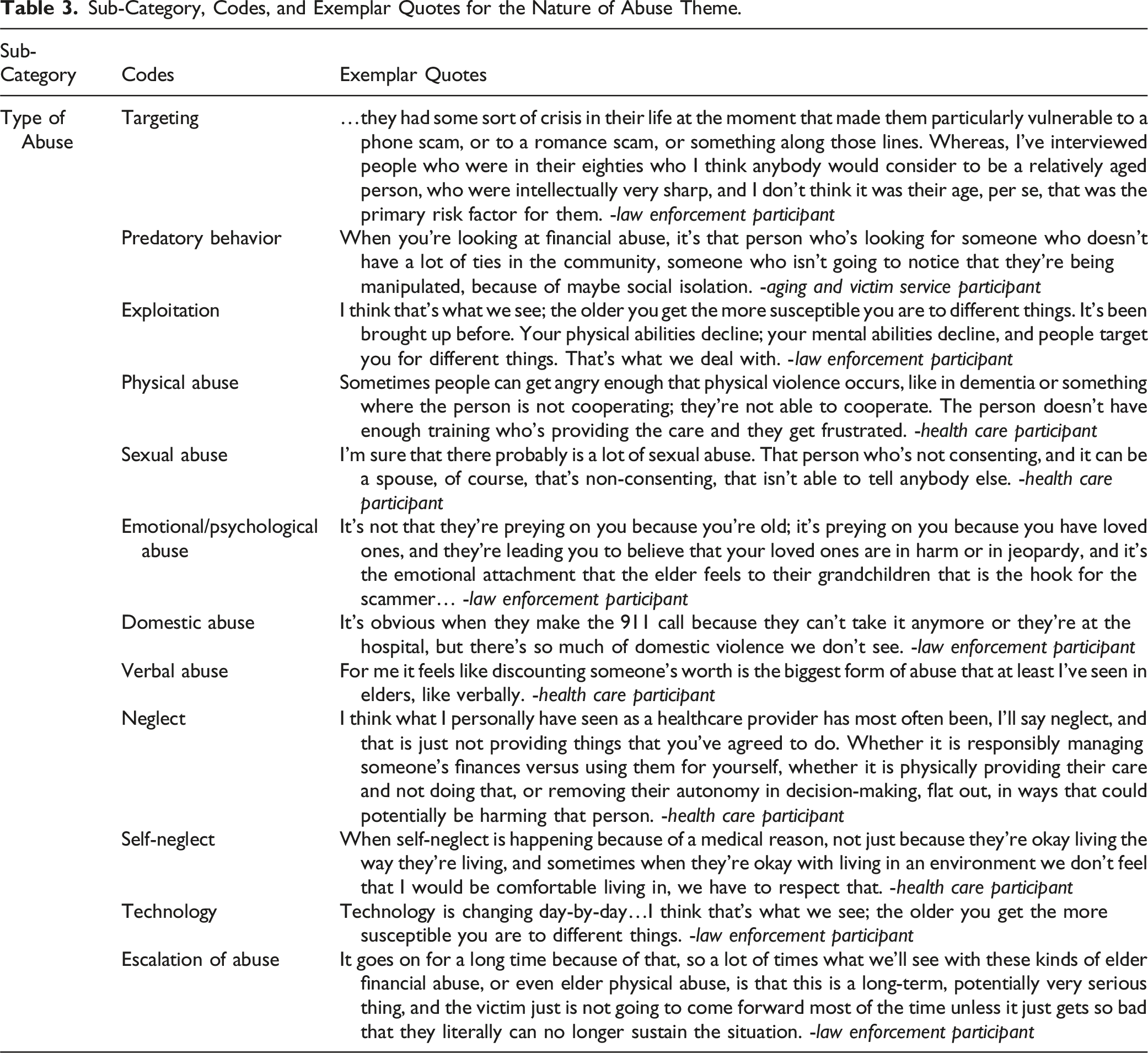
Sub-Category, Codes, and Exemplar Quotes for the Nature of Abuse Theme.
Results
Three major themes emerged from the data: societal influences, individual circumstances, and nature of abuse. Codes, sub-categories, themes, and exemplar quotes are in Tables 1 through 3.
Societal Influences
The societal influences theme consisted of four sub-categories: knowledge of abuse, addressing abuse, perceptions of resources and supports, and beliefs about aging.
Knowledge of Abuse
The sub-category knowledge of abuse included codes focused broadly on knowledge and education. In some instances, participants talked about abuse not being emphasized in their formal training. For example, one healthcare participant noted: I did a master’s in hospital administration and that never came up.
Participants also discussed feeling unprepared to recognize abuse. Often, this was coupled with the need for greater public awareness of what constitutes abuse, such as in the following quote: We want to prevent it, but we have to educate…we also need to start going into senior centers or church groups to get that out there… because there’ve been times when I’ve talked to someone that didn’t realize they were being abusive… that education to prevent it I think is huge. (Healthcare participant)
All of our participants believed greater awareness of what abuse is and how to recognize it is necessary for mitigating elder abuse. They also expressed willingness to take part in training to become better equipped to do this themselves.
Addressing Abuse
The second sub-category, addressing abuse, represented challenges within the current systems for addressing elder abuse. For instance, the processes for reporting abuse are often barriers, as captured below by a healthcare participant: …the rules never seem to stay the same and so it’s really hard to help people when the rules keep changing and I can’t stay up on them…
Another healthcare participant shared that making the decision to report can be difficult, saying: We spend a lot of time agonizing about whether or not APS [adult protective services] should be called.
Some participants expressed concerns about follow-up and case management. One law enforcement participant illustrated this, saying: With that agency [Adult Protective Services; APS], with social services overall, normally they’re understaffed and overworked, have a heavy caseload…So when we call other agencies… the response is so delayed at times…you’ll call and they won’t call you back for another two hours…
Other participants discussed how legality and jurisdiction often make case management challenging. For instance, a law enforcement participant described working with other community partners saying: Generally speaking…our first calls are typically to financial institutions, mental health clinicians sometimes… and department of social services…None of those work for law enforcement, so I can’t tell them what to do.
This perceived lack of linkage between various community systems and agencies was shared by other participants, as evidence by the following statement: …I’ve been in the field for a long time… it would just be nice to see a linking of the systems so that advocates and people actually working in the field know who they can turn to for certain types of assistance. (Aging and victim service participant)
Another law enforcement participant discussed how a more connected infrastructure would better serve older adults, saying: …Many hands lighten the load, so the more interconnection and intercommunication between all the players that end up interacting with seniors and to make sure that they get the law enforcement assistance or the APS [adult protective services] assistance.
In addition to better connecting systems involved with elders, our participants discussed challenges posed by a system structured around response rather than prevention of abuse. This observation is captured by the following participants’ statements: Unless people are in crisis, it's actually harder to handle the situation than if you can detect the rising risk and try to help…I often find that we are seeing the rising risk and can see what’s going to happen… and we’ll call them, and nothing happens, like they can’t do anything. (Healthcare participant)
A law enforcement participant commented on the lack of funding for responding to elder abuse saying: …it’s almost like they need to see the cases [of elder abuse] to justify providing more money. So instead of it being a, “Hey, let’s give you the funding to prevent these things from happening,” it’s, “Okay once we have enough cases, then we can justify giving you the money.” And that’s totally backwards.
Similarly, another law enforcement participant elaborated on “things they catch too late” saying: When…all the money is gone…when they show up to the hospital with malnutrition or they have a break…”Well, she fell.” She fell three months ago, too. “You’ve got to be more careful. How is the house set up?” Those are things we catch late.
Our participants all seem to believe that better systems and structures for recognizing and preventing elder abuse from happening is crucial to more efficient response.
Perceptions of Resources and Supports
The third category within the social influences theme offered some insight about how participants view the current structures and policies for addressing elder abuse. For example, many participants described pitfalls of the current system, indicating the existing systems and policies leave them feeling as if they are unable to have a positive impact, which this healthcare participant quote expresses: …I can think of one example where the person got the help they needed…But most of the time I don’t see a real change in the circumstances, except that I now have no relationship with the person that this happened to. [Laughs] Maybe it’s that we didn’t know when was the right time. Like I said, I don’t remember it being a part of my training as a health professional on when you should call…Maybe there’s just limitations of what can be accomplished through that route… I felt like the situation was actually worse afterwards.
Participants also believed that abuse of older adults is not a societal priority and that this contributes to an ineffective and inefficient structure for responding to elder abuse including, but not limited to, overloaded systems and insufficient resources. This is evidenced by the following healthcare participant quote: … every new administration we get… they’re all into something new. It would just be nice… if there were some societal, structural appreciation for aging, but a lot of the policies seem to be made by the generation before that hasn’t gotten to aging.
In other instances, participants feel as though they do not have the resources they need to properly advocate for older adults, saying: …it makes me feel like I don’t have the appropriate support I need to advocate for these individuals. (Aging and victim service participant)
Other participants discussed what they feel is “societal blindness” to aging, saying: …I think there’s some societal blindness to issues around aging...Issues around aging are so twisted up, because people just don’t want to deal with it…it seems possible that this area of our society is just kind of ignored because oh, Grandma’s in a home and these are just the sort of things that happen to old people…There have been elected officials who have made public statements that we should write off our elderly. Yikes. Can you imagine a statement like that made about any other population…? It would be staggering. (Law enforcement participant)
Other participants seemed to believe that the current structure and inadequate resources within it is more than mere “societal blindness” but is actually due to a lack of value on older adults, illustrated by this aging and victim service participant: It makes me feel that there’s little value on older adults…And so that just makes me feel like they’re saying, Well, they’ve lived their life. They don’t need anybody to advocate. They’re not going to be here much longer anyway.
In addition to commenting on society’s beliefs about aging, many participants also commented on various beliefs individuals have about aging and how that contributes to an overall, societal de-valuing of older adults.
Beliefs About Aging
Codes aligning with the sub-category beliefs about aging, illustrated the range of beliefs individuals have about aging, with the most prominent code being ageism. Within our data, ageism was both explicitly expressed as well as described as a symptom of our society. Explicit ageism was expressed as excuses to explain away instances of elder abuse or blame victims for their own abuse and neglect. Examples of ageism being explicitly expressed included the following: …and it doesn’t have to be physical or abusive but could be more like neglect, like, “I don’t have time to go get your groceries or take you to the doctor. So be it. Deal with it,” you know. And usually, the seniors aren’t really proactive. They just lie back and accept whatever. (Aging and victim service provider)
Some of the instances of explicit ageism that were expressed stereotypes applied to older adults, such as the following statement made by a healthcare professional: It’s an older person, so we expect them to be incapacitated in some ways. Like they should be dependent on this other person and…Well, what do you expect? Sure, they smell like urine and they’re not caring for themselves, but they’re old and that’s how it goes. These are sort of an acceptance of things in an older person that you wouldn’t accept in a younger one.
Participants discussed many other stereotypes of older adults that exist in our society, including stereotypes such as older adults don’t like to use the internet or computers, that they tend to live life more “slowly” than young people, that “boomers are fiercely independent,” and that they are more vulnerable. Participants also recounted how ageism can lead professionals to miss or explain away forensic indicators of abuse. One law enforcement participant shared the following story regarding stereotypes present in society: …we get a lot of…calls, where something will start in the emergency room…The ER will report something…They make a report, it comes to us, we investigate it. Then we talk to the next doctor, the specialist, and the specialist is like, “you know, for their age and their mobility, it’s a completely normal injury”…there’s a disconnect between intake and the specialists.
Overall, our participants seem keenly aware that our society’s ageist beliefs and attitudes contribute to a perpetuation of and dismissal of elder abuse.
Individual Circumstances
Three sub-categories comprised the second major theme of individual circumstances: psychological factors, social support, and risk factors.
Psychological Factors
Codes aligning with the psychological factors sub-category represented various psychological and emotional reasons an individual might tolerate, commit, or excuse abuse. Caregiver burnout was frequently discussed as an excuse for abusing an older adult, as evidenced by the following statement: …what I also see or what I’ve noticed is a lot of the abuse cases that we do get are more because the caretakers or caregivers are overwhelmed. They’re overwhelmed, they’re frustrated, and they have lack of resources, so they don’t know how to properly provide or take care of the individual, and so the abuse is a result of the overwhelm-ment. (Aging and victim service participant)
Childhood trauma or other histories of abuse were also discussed as reasons abuse may be normalized or tolerated. Other reasons given for toleration of abuse included fear, emotional attachment, shame, guilt, and retribution; most participants had stories they could tell about why someone had struggled to seek help when they were experiencing abuse, such as in the following example: Domestic abuse is always messy… and I think with elder abuse it’s especially bad, because what if it’s a child that’s taking advantage of you—your own child… So if you’re an elder and your adult child is taking advantage of you, imagine the psychological resistance to coming forward with that report. (Law enforcement participant)
Apart from struggling with emotional abuse, particularly when loved ones are the perpetrator of abuse, many participants discussed the difficulty of admitting to one’s self that they have been taken advantage of, such as in the following law enforcement quote: When you talk about the embarrassment and the humiliation… But the extreme cognitive dissonance of admitting to yourself yep, I got taken in and now I’m on the hook for a lot of money is really painful. People will tend to just double down.
Our participants discussed a number of incidents they have encountered in their work where older adults were struggling, both emotionally and psychologically, to accept what was happening to them was actually abuse committed by either loved ones or by strangers.
Social Support
Codes aligning with the second sub-category in the individual circumstances theme captured the role of a person’s various social supports in abuse. Family was discussed a great deal, both as a means of social support as well as a source of perpetrators of abuse. Some participants commented on cultural differences in familial care of older adults with comments such as: …we really see a vast cultural difference in families that will stay together in a community and families that feel that they must put their loved ones in a nursing facility. (Aging and victim service participant)
Being isolated from family was also discussed as a reason why elders might experience abuse or why abuse may go undetected for so long. Some participants reflected about elders in their own family and wondered how things might be different if they weren’t involved in caring for them, such as the following aging and victim service participant’s reflections of their own father: The other thing I’d like to mention here is maybe self-neglect as people get older. I take food to my father…My sister is able…to order his welding supplies and anything else that he needs. But I think it would be a different situation if he did not have us…I think he would be a bit neglectful…
Overall, our participants viewed social networks as both an opportunity for protection against abuse and neglect as well as a potential gateway for abuse and neglect to occur.
Risk Factors
The final sub-category in the individual circumstances theme, risk factors, highlighted traits that make older adults vulnerable to abuse. For example, many participants said older adults are vulnerable simply because they are old. Being in a crisis or state of desperation was mentioned as being both a risk factor for an older adult becoming a victim of abuse as well as something that might make a perpetrator more likely to commit abuse, such as in this quote: I would say that anytime that you’re emotionally involved…in some sort of desperate circumstances… and you’re desperate for some…relief, then it’s very easy for an abuser…to get you on the hook to make a mistake…because you’re already…under duress from your situation. (Law enforcement participant)
Other risk factors included living with dementia, being dependent, having certain medical conditions, lacking autonomy, or the fact that society seems to take away the voice and autonomy of older adults.
Nature of Abuse
Only one sub-category—Types of Abuse—emerged in the nature of abuse theme though 12 individual codes aligned with this theme. These codes focused on what abuse actually looks like. Many participants discussed targeting and “romance scams” when talking about elder abuse. Technology was frequently mentioned as a modality for committing abuse. Others described situations in which domestic or verbal abuse was taking place or neglect on the part of a caregiver or the older adult themselves. Many participants listed various types of abuse they were familiar with or frequently encountered in their field, such as the following participants’ reflections: I think it can look like a lot of things. Doing things against your will...It could be mental in not allowing you decision-making…It could be injury. It could also just be neglect, not caring for someone that you’ve accepted obligation to care for…It could even be financial, exploitation… I think of…different kinds of ways it could manifest.
Similarly, several participants also reflected on the type of abuse they most encountered through their work. Our participants appeared to have experienced or dealt with most forms of abuse as a professional.
Discussion
Our purpose was to gain understanding of the knowledge of abuse and beliefs about current practices among Virginia’s frontline workforce. Three major themes emerged from our data: societal influences, individual circumstances, and nature of abuse.
Within the
Within the second major theme,
The third theme,
Though not a stand-alone theme, ageism was present within our data across several themes and sub-categories. Ageism is the prejudice or discrimination against people based on age (Butler, 1969) that can be expressed implicitly or explicitly (de Paula Couto & Wentura, 2017; Levy & Banaji, 2002). Our participants expressed a strong belief that older adults are not valued by society. It is possible that society-at-large does not intentionally deny resources and services that support the safety of older adults but, instead, is the result of their collective implicit and negative bias toward older adults. Explicit ageism was also present in our data through several instances of ageist beliefs and stereotypes being expressed such as the belief that older adults are vulnerable, are frail, and smell of urine.
Our findings support and expand current research on elder abuse and, specifically, support the utility of the AIM and ecological systems models for identifying risk factors at multiple levels in an older adults’ environment and not just risk factors of the older adult themselves may. Though our findings suggest that ageism’s role in abuse is prominent, more research is needed to uncover the theoretical and empirical relationships between ageism and elder abuse. Future efforts should also seek to use the AIM and ecological systems models to identify opportunities for preventing elder abuse from occurring. Finally, this work points to the need for more interconnected, resource- and knowledge-rich agencies, policies, structures, and systems to effectively intervene and reduce the prevalence of elder abuse.
Implications
Our findings suggest that a critical step toward safeguarding older adults is to reduce ageist attitudes and beliefs held by individuals within the community. These findings align with The World Health Organization (2022), which recommends combating ageism as the top priority for addressing elder abuse worldwide. We also heard a call to invest in training and education from our participants. Future research on elder abuse should focus on the development and evaluation of more evidence-based training for our frontline personnel as well as older adults and caregivers of older adults. With increased knowledge, those best positioned to intervene when abuse occurs can do so more effectively, efficiently, and confidently. Providing similar education and training opportunities to the general population also serves as a means for safeguarding older adults. The more our society knows what abuse is, how to report it, and effective strategies for prevention, intervention, and treatment, the more likely that instances of elder abuse will be reduced.
Limitations and Conclusion
This study focused on frontline workers located in central Virginia, limiting the generalizability of our findings to similar demographics in other states or countries. Areas with more resources and robust social support available to older adults, such as municipalities that have active multidisciplinary teams (MDTs) for elder abuse response, might not have the same difficulties working across disciplines and agencies discussed by our participants (e.g., DePrince et al., 2019). The COVID-19 pandemic limited participant recruitment and availability, particularly frontline healthcare workers, due to increased workloads and staff shortages. This resulted in several focus group sessions where only one participant was able to attend. These participants were eager to participate and share their insight and valued the study topic. We wanted their voices to be included in the study and did not remove them from data analysis. Having to conduct focus groups via teleconferencing software also posed challenges recruiting from rural areas where broadband access is more limited. Knowing the conversations were recorded might have deterred some individuals from being completely honest in conversations about such sensitive topics. Finally, we did not collect additional demographic information about our participants, further limiting generalizability. Despite these limitations, our findings are consistent with other literature on elder abuse recognition. Moreover, our findings set the stage for future research and advocacy efforts that will ultimately be effective in reducing the prevalence of elder abuse.
Supplemental Material
Supplemental Material - An Exploration of the Knowledge and Current Practices of Frontline Workers Regarding Elder Abuse
Supplemental Material for An Exploration of the Knowledge and Current Practices of Frontline Workers Regarding Elder Abuse by Sarah A. Marrs, Miranda Yelvington, Annie Rhodes, Courtney O’Hara, Catherine MacDonald, and Tracey Gendron in Journal of Applied Gerontology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Virginia Commonwealth University Presidential Research Quest Foundation.
IRB Protocol Numbers
HM20020135.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.