
Abstract
The literature does not adequately examine the relationship between cardiovascular disease (CVD) and risk in handgrip strength (HGS) among community-dwelling older adults in India. The study aimed to investigate this relationship, considering sociodemographic, lifestyle, and clinical variables. A cross-sectional study involving 31,001 individuals aged ≥60 assessed HGS in kilograms using a handheld Smedley Hand Dynamometer and self-reported CVD status. Participants were classified into two groups: with (n = 2291) and without CVD (n = 28,710). Multivariate logistic regression analyses revealed a significant odds ratio (OR) of HGS among older adults with CVD, adjusted for age, gender, education, marital status, place of residence (sociodemographic), alcohol consumption, smoking, activity, body mass index (lifestyle), hypertension, diabetes, and chronic bone/joint diseases (clinical) (right-handed: OR = 1.23, 95% confidence interval [CI] = 1.09–1.38; left-handed: OR = 1.16, 95% CI = 1.04–1.30). CVD is associated with an increased risk of reduced HGS in older Indians, underscoring that improving HGS may help reduce death rates in this population.
• CVD is a significant cause of death in India. • There is a lack of research on the association between CVD and HGS risk in older adults, particularly among community-dwelling older Indians. • After analyzing data from 31,001 people ≥60 years old, we found that community-dwelling older Indians are more likely to have reduced HGS if they have CVD, especially men and those with chronic bone or joint illness, diabetes, low physical activity levels, and rural residence.
• The study findings emphasize the importance of enhancing HGS to decrease mortality rates among community-dwelling older Indians with CVD and other comorbidities. • The study findings also emphasize the value of encouraging physical activity, particularly in older Indian people with CVD. • Policies should consider using HGS as a vital health indicator to reduce CVD death rates in this population.What this paper adds
Applications of study findings
Introduction
Cardiovascular diseases (CVD) are a major cause of mortality, affecting over 30% of deaths worldwide (Roth et al., 2020). In India, its impact is particularly pronounced among older adults, who endure a rising burden of this disease (Kundu & Kundu, 2022). The CVD crisis in India is exacerbated by aging, obesity, poor diabetes management, smoking, and higher vascular susceptibility (India State-Level Disease Burden Initiative, 2018; Kalra et al., 2023; Koya et al., 2023; Kundu & Kundu, 2022). Although handgrip strength (HGS) has an inverse relationship with CVD, aging was found to be substantially linked to a higher risk of decreasing HGS, particularly among older men in India (Zhuo et al., 2022).
Evidence suggests that the prevalence of CVD increases as HGS decreases; a 5-kilogram (kg) decrease in HGS is associated with a 1.21-fold increase in CVD incidence (Wu et al., 2017). However, most of the data come from observational studies, which are limited in their ability to conclusively prove causality because of the possibility of residual confounding and reverse causation. A previous study (Xu & Hao, 2017) showed a causal connection between higher HGS and lower coronary artery disease (CAD) risk. However, the study’s findings were still limited because it solely examined the relationship between HGS and CAD and selected two single-nucleotide polymorphisms as instrumental factors. A recent study (Zhuo et al., 2022) revealed that HGS was not substantially linked with hypertension, stroke, or heart failure. However, it was associated with myocardial infarction (MI) and CAD. Additionally, studies indicate that low HGS in hypertensive individuals is linked to the highest risk of CVD, CVD mortality, and all-cause mortality (Celis-Morales et al., 2018; Leong et al., 2015; Liu et al., 2021).
Since HGS is a well-known indicator (Lee, 2021), the most direct and valid objective measure of muscle strength (Muollo et al., 2022; Rantanen et al., 2002), and health outcomes (Soysal et al., 2021), it serves as a crucial tool for assessing overall health in older adults. HGS is particularly useful in developing countries like India due to its predictive accuracy, non-invasive nature, cost-effectiveness, and portability. Moreover, HGS recently has garnered increasing attention as a useful predictor of CVD risk (Li et al., 2023; Liu et al., 2021). A recent comprehensive review also summarized that HGS could be a significant indicator of health (Vaishya et al., 2024). A recent study (Shim & Yoo, 2020) also specifically found that for every kg rise in HGS, the 10-year risk of CVD was 1.68 times lower.
However, no research has examined the relationship between the presence of CVD and HGS in older adults, specifically among community-dwelling older Indians (Ramirez-Velez et al., 2021; Soysal et al., 2021). Given this gap in the literature, the present study aimed to examine the relationship between the presence of CVD and HGS in community-dwelling older adults in India, encompassing sociodemographic, lifestyle, and clinical factors. The study hypothesized that the presence of CVD would be associated with an increased risk of reduced HGS in older Indians with CVD than those without CVD. Understanding the relationship between CVD and reduced HGS in older Indians may highlight the importance of improving HGS to reduce mortality rates in this demographic.
Methods
Data Source
Secondary data analyses were conducted using data from the 2017–2018 Longitudinal Ageing Study in India (LASI, Wave 1) (Perianayagam et al., 2022). While LASI is designed to be longitudinal, data collection for the second wave is still ongoing. Currently, only wave 1 baseline data are available. LASI is a comprehensive survey representing the entire nation, encompassing more than 72,000 individuals aged 45 and older from all states and union territories (UTs) of India. The primary aim of the LASI survey is to investigate the health and socioeconomic conditions of older Indians. The survey involved three-stage sampling in rural areas and a four-stage approach in urban areas in all states and UTs of India. Primary sampling units (PSUs) were selected in the first stage, villages and wards were chosen within the PSUs in the second stage, and households were chosen from selected villages in the third stage. However, a randomly selected census enumeration block was used to choose households from urban areas in the final stage. The survey utilized advanced technology, computer-assisted interviews, and personal biomarkers to reduce errors and improve data entry, with high response rates of 87% varying by 96% in Nagaland and 74% in Chandigarh (Basu, 2022).
Participants
In our study, we focus on older adults aged 60 years and older. Older adults were defined as aligning with India’s demographic context and policy standards (Sujaya, 2000), which differ from the Western benchmark of 65 years. Given the lower life expectancy, earlier onset of health issues, and higher chronic disease burden, as well as government policies that recognize 60 as the threshold for senior citizenship (Meenai, 2021), this definition is more appropriate for the Indian population (Mandi et al., 2023). After excluding persons under the age of 60 (n = 40,899), both dominant handedness (n = 299), and missing data (n = 81), the final sample size for this study was 31,001 persons. Participants were classified into two groups: 2291 individuals with CVD and 28,710 without CVD.
Handgrip Strength
HGS measurements were conducted utilizing Smedley’s hand dynamometer. The procedure involved adjusting the device for both the respondent’s dominant right and non-dominant left hands. Participants were positioned with their right forearm at the elbow of the upper arm, maintaining the upper arm close to the body. They were then instructed to exert firm pressure on the dynamometer three times with each hand for a brief interval. Subsequently, the highest recorded value in kgs of the six trials was selected.
Cardiovascular Diseases
The independent variable in this study indicated the presence of CVD, which includes stroke, chronic heart disease, and hypertension. Respondents self-reported CVD in response to the question, “Has any health professional ever diagnosed you with chronic conditions or diseases such as stroke, hypertension (high blood pressure), or chronic heart disease?” Chronic heart diseases also include CAD (a heart attack or MI), congestive heart failure, or other chronic heart problems. Those who reported one or more such conditions were classified as having CVD and those without any conditions comprised the reference group. Similar questionnaires were employed in recent research to evaluate the above conditions (Ahmed et al., 2023).
Covariates
Age was measured as a continuous variable. Gender was dichotomized into men and women. The level of education was classified into less than primary school (standard 1–4), primary school (standard 4–7), middle school (standard 8–9), secondary/senior secondary/diploma, and graduate/professional degree/post-graduates. Marital status was classified as married, widowed/separated/divorced, and never married. The self-reported questions were used to assess place of residence, engagement in activity, alcohol consumption, tobacco consumption, and comorbidities, such as hypertension, diabetes, and joint/bone disease status. The place of residence was categorized into rural and urban areas. An engagement in activity was classified into daily/weekly and monthly/never. BMI was measured in kg/m2.
Statistical Analysis
The Shapiro-Wilk test was used to determine whether the data distribution was normal. Descriptive statistics, such as the mean and standard deviation (SD) were used for continuous data, whereas the count (%) was used for categorical variables. The significant difference between the groups was determined using an independent student t-test for mean values and a chi-square test for frequencies.
The multivariate logistic regression was used to investigate the relationship between CVD (independent categorical variable) and the likelihood of HGS risk (dependent continuous variable). The analysis was modified into two models to account for sociodemographic (such as age, gender, education, marital status, and place of residence), lifestyle (such as alcohol consumption, smoking, activity, and BMI), and clinical factors such as hypertension, diabetes, and chronic bone or joint diseases. Model 1 adjusted with sociodemographic factors. Model 2 adjusted for all sociodemographic, lifestyle, and clinical factors. The data were presented using the odds ratio (OR) and 95% confidence interval (CI). To assess multicollinearity, the variance inflation factor was employed. SAS, version 9.4 was used for all analyses (SAS Institute, Inc, Cary, NC). Each analysis was considered significant if the p-value was less than .05.
Results
The flow of the study participants through LASI has been shown in Figure 1. Of 72,250 participants, 31,001 (42.9%) individual data were used in the analysis after 41,249 (57.1%) were excluded. The data were excluded from the study due to age of less than 60, both handedness and lack of data. Flowchart of the study participants through LASI. λOlder adults with CVD. ηOlder adults without CVD.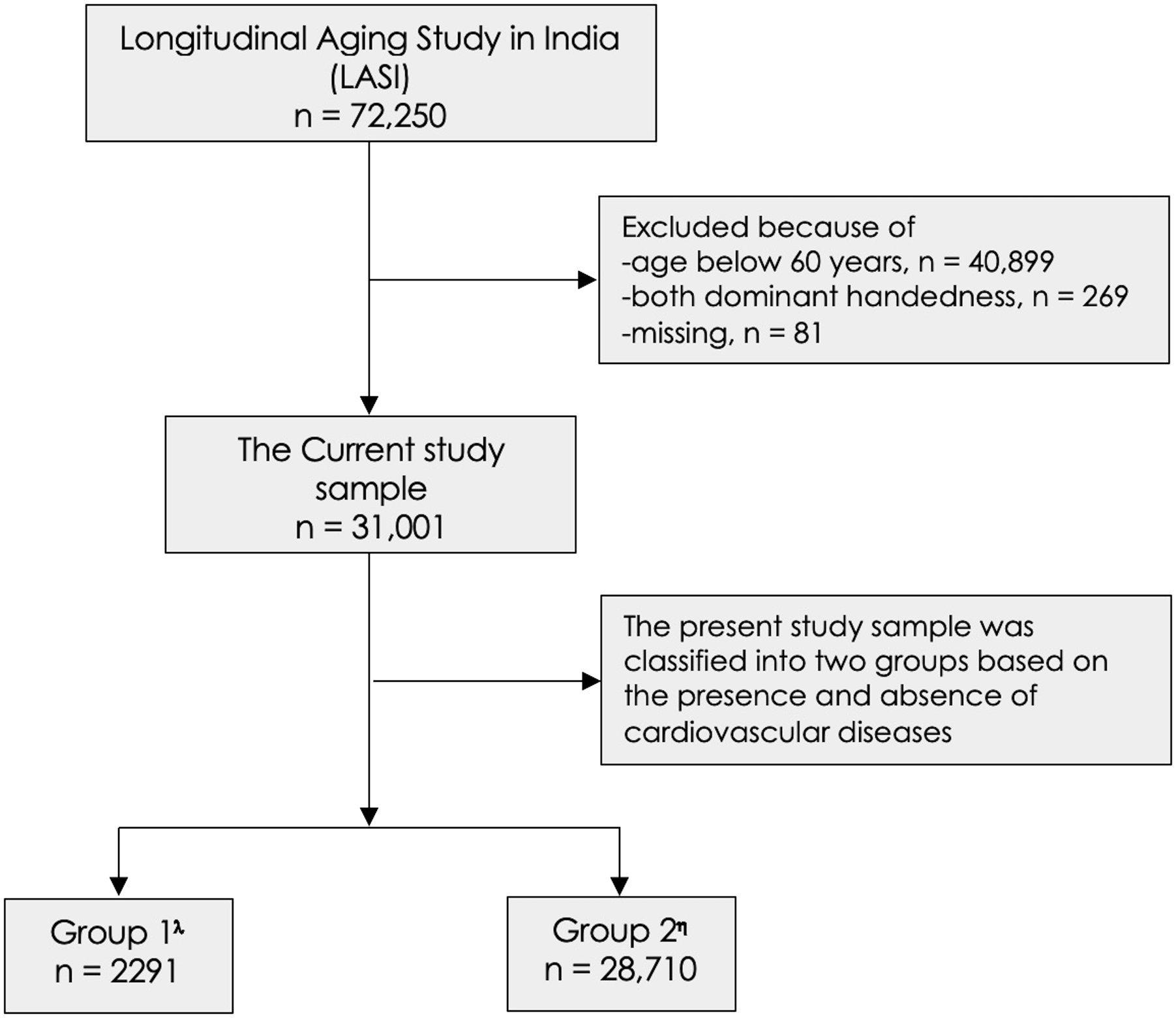
Characteristics of the Study Participants.
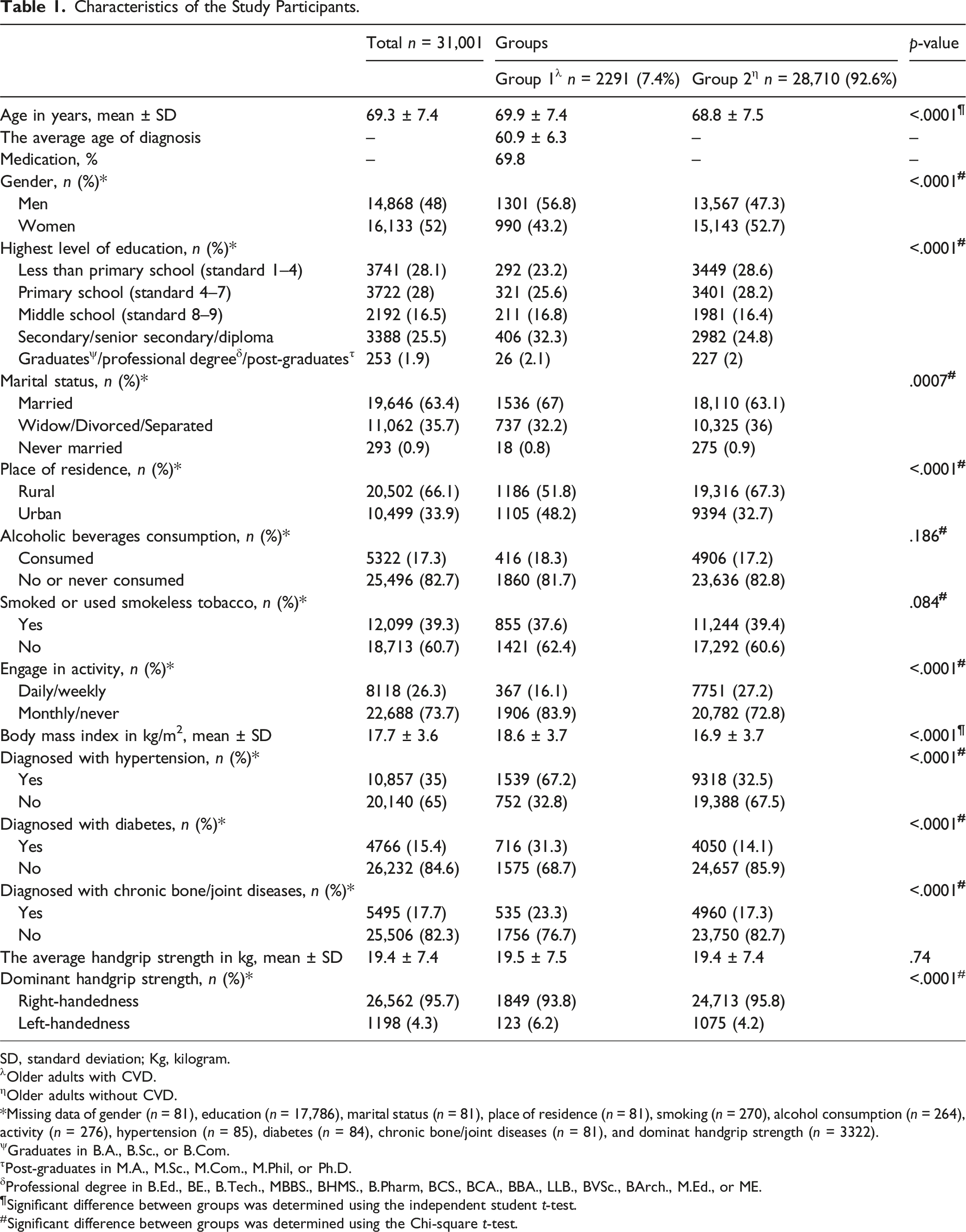
SD, standard deviation; Kg, kilogram.
λOlder adults with CVD.
ηOlder adults without CVD.
*Missing data of gender (n = 81), education (n = 17,786), marital status (n = 81), place of residence (n = 81), smoking (n = 270), alcohol consumption (n = 264), activity (n = 276), hypertension (n = 85), diabetes (n = 84), chronic bone/joint diseases (n = 81), and dominat handgrip strength (n = 3322).
ψGraduates in B.A., B.Sc., or B.Com.
τPost-graduates in M.A., M.Sc., M.Com., M.Phil, or Ph.D.
δProfessional degree in B.Ed., BE., B.Tech., MBBS., BHMS., B.Pharm, BCS., BCA., BBA., LLB., BVSc., BArch., M.Ed., or ME.
¶Significant difference between groups was determined using the independent student t-test.
#Significant difference between groups was determined using the Chi-square t-test.
Association Between the Presence of Cardiovascular Diseases and Handgrip Strength Risk.
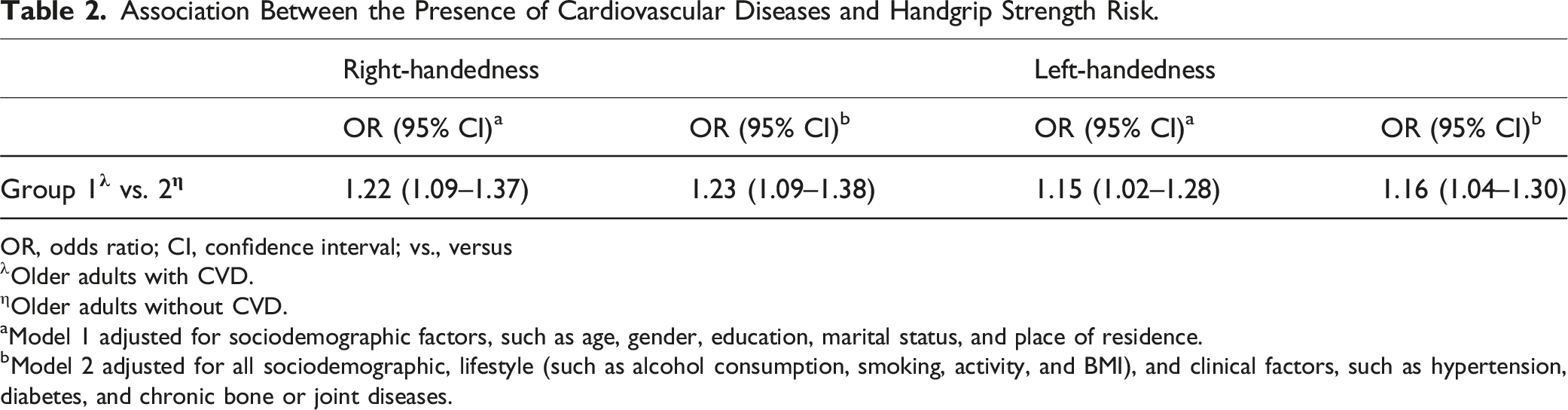
OR, odds ratio; CI, confidence interval; vs., versus
λOlder adults with CVD.
ηOlder adults without CVD.
aModel 1 adjusted for sociodemographic factors, such as age, gender, education, marital status, and place of residence.
bModel 2 adjusted for all sociodemographic, lifestyle (such as alcohol consumption, smoking, activity, and BMI), and clinical factors, such as hypertension, diabetes, and chronic bone or joint diseases.
Discussion
This study examined the association between the presence of CVD and HGS among community-dwelling older Indians. Findings showed that the presence of CVD was significantly associated with an increased risk of reduced HGS in this population, even after controlling for sociodemographic, lifestyle, and clinical factors. These findings consistently demonstrate a higher risk of reduced HGS in this population among those with CVD compared to those without it.
The association between CVD and HGS risk has not been explored in prior research, particularly among older community-dwelling Indians. Nonetheless, several studies (Ramirez-Velez et al., 2021; Shim & Yoo, 2020; Soysal et al., 2021; Vaishya et al., 2024) have examined the relationship between HGS and the onset of CVD. The current study is supported by earlier studies (Heiland et al., 2019; Jin et al., 2017), which found that leading an unhealthy lifestyle exacerbates the negative effects of CVD on physical health. It is reasonable to assume that CVD itself may directly contribute to muscle weakness, even when accounting for sociodemographic factors.
Several mechanisms support the idea that cardiovascular diseases such as atherosclerosis can lead to plaque accumulation in the arteries, narrowing and hardening them, decreasing muscle blood supply, and resulting in muscular weakening (Uchida et al., 2020). Sarcopenia, or muscular atrophy, is a condition diagnosed with HGS because of decreased physical activity and can be brought on by heart failure, stroke, or severe coronary artery disease (Coats et al., 2017; Fielding et al., 2011). Peripheral neuropathy, which results in hand weakness, tingling, or numbness, and chronic inflammation, which causes muscular weakness and loss of function, are two conditions that several CVDs can cause (Koshikawa et al., 2020; Tuttle et al., 2020). Furthermore, although older people often tolerate beta-blockers well, these drugs can occasionally cause muscle weakness or weariness (Cojocariu et al., 2021), which might further impair HGS.
Our findings showed that older adults with CVD have a higher risk of reduced HGS due to factors such as age, chronic conditions, and lifestyle challenges. Older Indians living in rural areas, smoking, and having low physical activity endured a higher HGS risk. People with diabetes and chronic bone or joint disease also reported a higher risk of reduced HGS. A possible reason for this may be that growing older is associated with decreased muscle mass and sarcopenia, which can be further exacerbated by chronic conditions such as CVD (Damluji et al., 2023). Furthermore, living in rural settings may make it more difficult to acquire services that promote health and medical care (Banerjee, 2021; Basu, 2022), which could worsen the adverse effects of CVD.
Our study is the first within the Indian context to examine the associations between the presence of CVD and HGS among community-dwelling older adults. Our findings are relevant to the practices and policies affecting Indian older people living in the community. Improved muscle strength with aging is associated with favorable changes in CVD biomarkers, such as waist circumference, high-density lipoprotein cholesterol, triglycerides, and blood pressure (Kim et al., 2020). As such, HGS has been recommended as a new vital indicator of health (Celis-Morales et al., 2018; Vaishya et al., 2024). However, its usefulness differs depending on gender and age (Taylor et al., 2024). High levels of education, physical activity, and good aging can all aid in CVD management (van Oort et al., 2021). In particular, there is a basic connection between physical activity and public health, as evidenced by its benefits for musculoskeletal health, healthy aging, the prevention of chronic diseases, and all-cause mortality (Herrmann et al., 2024; Lavie et al., 2024). These advantages emphasize the value of encouraging physical activity, particularly for older Indians who have CVD. Further research, relying on longitudinal data, is needed to understand the mechanisms underlying the link between CVD and HGS in this population, considering sociocultural, lifestyle, and clinical factors.
Limitations
First, the cross-sectional nature of our study limits the ability to conclude causality or sequencing of events. Longitudinal research is needed to track changes in HGS alongside changes in CVD status, enabling a better understanding of how these factors influence each other over time. Multiple waves of data would provide opportunities to explore the temporal relationships between CVD onset and declines in HGS, variability in their progression, and potential intervention points. Second, although HGS is commonly used to evaluate muscle strength, future research should contemplate integrating alternative measures of muscle function, like the chair rise test, to offer a more thorough assessment. Third, future research replicating our study should extend it by exploring pathways that connect CVD to HGS in Indian older adults. Lastly, the main focus of this study was on the association between CVD and HGS, but the models’ inability to account for neurological and cerebrovascular disorders may have attenuated estimates. Future studies should explore the impact of these circumstances on HGS, particularly in the Indian context. Investigating these interactions could clarify whether the associations are unique to cardiovascular health or part of a broader spectrum of age-related health outcomes, contributing to a more comprehensive understanding of HGS as a biomarker of overall health and aging.
Conclusions
Our study found that CVD is significantly associated with higher odds of low HGS among community-dwelling older adults in India. This association underscores the importance of HGS as a practical marker for physical function decline in individuals with CVD. The results are important for applied gerontology and clinical practice because they suggest that interventions that build muscle strength, like physical therapy or customized exercise programs, might help lessen the bad effects of CVD on health. Regular HGS assessments may help identify those at greater risk for physical deterioration, allowing for timely and targeted interventions to improve functional outcomes and enhance the quality of life in older adults. Further research should focus on developing strategies to enhance HGS among older adults with CVD, which could improve health outcomes and reduce mortality within this population, especially in developing countries like India.
Footnotes
Acknowledgments
The authors would like to extend their sincere appreciation to the Researchers Supporting Project Number (RSPD2024R1094), King Saud University, Riyadh, Saudi Arabia for funding this project.
Author Contributions
V.V. substantially contributed to the conceptualization, data analysis, writing – original draft preparation, and comprehensive review & editing. M.P. contributed significantly to the conceptualization, interpretation of the results, writing – original draft preparation, comprehensive review & editing. All authors have given final approval for the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Researchers Supporting Project Number (RSPD2024R1094), King Saud University, Riyadh, Saudi Arabia.