
Abstract
This study aims to examine the trajectory of older adults’ cognitive function over time and identify its predictors. Based on the model of neuroplasticity and cognitive reserve, participants’ general characteristics as well as their physical, mental, and social factors were included as predictors of cognitive function. A latent growth model analysis was used to examine the trajectory of cognitive function and its predictors. The analysis of the unconditional model revealed that older adults’ cognitive function significantly decreased over time. The rate of cognitive decline was significantly related with age, current smoking status, depression scores, number of social activities, time spent in group cognitive activities, and number of individual cognitive activities. The findings identified predictors affecting initial cognitive function and the rate of cognitive decline in older adults. The rate of cognitive decline varies widely among individuals. Identifying these differences is essential for effectively tailoring interventions that address individual needs.
Keywords
• Factors influencing initial cognitive function and changes in the cognitive function of older adults were identified. • Among modifiable health factors, current smoking accelerates cognitive decline. • The higher the depression score, the slower the cognitive decline. • Stimulating activities which were performed individually or in group were both effective in alleviating cognitive decline.
• This study could serve as a foundation for preparing strategies suitable for the various physical and psychological characteristics of older adults. • Tailoring interventions to an individual’s risk profile, including age, depression scores, and current engagement in cognitive activities, can enhance their effectiveness. • The findings of this study could contribute to the preparation of intervention strategies for maintaining cognitive function in older adults in clinical and academic fields.What this paper adds
Applications of study findings
Introduction
Cognitive decline is common in older age, often progressing subtly over several years (Montine et al., 2021). Maintaining a high level of cognitive function is crucial for tasks such as integrating sensory and motor information and performing daily activities (Bahureksa et al., 2016; Taylor et al., 2019). Literature indicates that cognitive decline correlates with poor physical function such as slow gait and low balancing ability (Demnitz et al., 2016; Taylor et al., 2019). Previous research has also linked impaired cognitive function in older adults to an increased risk of falls. The repeated falls of older adults can lead not only to physical injuries but also to death and a loss of independence (Montero-Odasso & Speechley, 2018). Moreover, subjective cognitive decline is one of the major risk factors for the development of dementia, and the onset of dementia can influence disability, activities of daily living, independence, and mortality in older adults (Pike et al., 2022). Cognitive function changes over time, and while addressing the current cognitive abilities of older adults is important, it is equally crucial to prepare for the future to prevent significant cognitive decline. To achieve this, it is necessary to examine how cognitive function in older adults changes over several years and identify the factors that influence these changes.
According to the model of neuroplasticity and cognitive reserve (Vance & Crowe, 2006), cognitive reserve can be influenced by six domains: modifiable health factors, education, social support, positive affect, stimulating activities, and cognitive training (Vance & Crowe, 2006). Firstly, modifiable health factors encompass specific medical conditions, nutritional habits, physical activities, and alcohol consumption. Evidence indicates that conditions such as diabetes, hypertension, and pulmonary disease are associated with cognitive decline (Taylor et al., 2020; Vance & Crowe, 2006). Secondly, education is one of the most important predictors of cognitive reserve in older adults (Clouston et al., 2020; Vance & Crowe, 2006). A higher educational level has been linked to a reduced risk of dementia. Thirdly, increased social interaction is correlated with greater neuroplasticity. Larger social networks and socially integrated lifestyles have been found to decrease the risk of dementia in older adults (Fratiglioni et al., 2004; Vance & Crowe, 2006). Furthermore, previous literature has suggested that positive affect could serve as retrieval cues from positive material, thereby facilitating cognitive organization (Isen et al., 1987). Likewise negative affect and depressive symptoms are particularly linked to cognitive decline. Lastly, both engaging in active leisure pursuits and participating in cognitive training activities are associated with improved cognitive function (Vance & Crowe, 2006).
Previous studies have examined the correlation between cognitive function and various variables, identifying specific characteristics associated with individuals’ cognitive function. It was found several factors were related to cognitive function, including age, gender, income level, education, physical activity, chronic diseases, smoking, depression, leisure activities, and emotional support (Chen & Chang, 2016; Jia et al., 2020; Tsai & Chang, 2019). In particular, one study found association between older age, male gender, low educational attainment, and diabetes (Griffiths et al., 2020). However, when cognitive function was measured twice over a 4-year period, no significant decline was observed (Li & Hsu, 2015). It was speculated that the limited number of measures used may have hindered the detection of cognitive changes over time.
While it is important to address cognitive function at a single point in time, sequentially assessing cognitive function across multiple time points is crucial for understanding the magnitude and direction of change. In particular, investigating changes based on results from cognitive assessments conducted over an extended period can aid in identifying changes that may have been overlooked in previous studies. Therefore, there is a need to comprehensively assess cognitive function by conducting multiple assessments over an extended period. Thus, the purpose of this study was to explore the trajectory of cognitive function changes over an 8-year period and to identify the predictors of cognitive decline using data from a national-level panel survey.
Methods
Study Design and Data Sources
This study conducted a secondary data analysis using national panel data called Korean Longitudinal Study of Ageing (KLoSA) which was surveyed by the Korea Employment Information Service (KEIS, 2015). The longitudinal panel survey commenced in 2006, sampling adults aged 45 or older in Korea. The panel study is conducted biennially, with the latest data released in 2020. All the data are accessible online for researchers.
For this study, data from 2012 to 2020 were utilized. In 2012, out of 4134 older adults aged 65 or older included in the dataset, a total of 2445 participants with complete cognitive function data for all five time points over the 8-year period were selected for analysis. There were missing values for a total of four items: one for the number of chronic diseases, 96 for BMI, 735 education level, and 19 for depression scores. Missing data for the selected participants were imputed using expectation maximization (EM) method and full information maximum likelihood (FIML) method (Cheung, 2007).
Measures
Cognitive Function
The cognitive function, a dependent variable of this study, was measured using a modified version Mini-Mental State Examination (MMSE) measurement scale (Folstein et al., 1975; Kang et al., 1997). This scale measures cognitive function of an individual in the domains of orientation, registration, attention, calculation, recall, language, and visual construction. The total score of the scale ranges from 0 to 30 points, with lower scores indicating lower cognitive function (Folstein et al., 1975).
Study Variables
Health Factors and Education
Age, gender, and educational level were included as participants’ characteristics. Educational level was divided into two categories: less than college education or college graduation and above, based on participants’ final academic background. First, health factors included the number of chronic diseases, smoking experience, drinking experience, body mass index (BMI), and regular exercise at least once a week. The participation in regular exercise was assessed through a single question asking whether the individual engages in physical activity at least once a week, with responses provided as either “yes” or “no.”
The number of chronic diseases refers to the count of diseases diagnosed among the following five: hypertension, diabetes, chronic pulmonary diseases, cardiovascular diseases, and neurovascular diseases. These diseases have been reported in previous studies as being related to cognitive function (Wang et al., 2022). Regarding smoking experience, the study participants were classified as current smokers if they were currently smoking, past smokers if they had smoked more than five packs in their lives, and non-smokers if they had smoked less than that or not at all. The participants who still drink alcohol were classified as current drinkers, those who used to drink but have stopped as past drinkers, and those who have never drunken alcohol as non-drinkers.
Negative Affect
Depression was measured as affect of the participants using 10 questions of the Korean version of Anderson form CES-D (Center for Epidemiologic Studies Depression) scale (Radloff, 1977). A value of 1 was given for positive answers and 0 for negative answers with a total score within 0–10 points. A higher score means that participants have more depressive symptoms. The Cronbach’s alpha of the CES-D was 0.822 (Bae et al., 2020).
Social Participation
Social participation refers to the types and number of social activities that participants engaged in. The types of activities included religious gatherings, social gatherings, leisure/culture/sports-related organizations, alumni/hometown/family gatherings, volunteering, and political parties/citizens’ organizations/interest groups. The participation status for six different types of activities, without any limitation of specified participation duration, was surveyed, with a score range of 0–6.
Cognitively Stimulating Activities
Lastly, stimulating activities refer to cognitively stimulating activities in which the participants engaged either in groups or individually. Group cognitive activity was measured by the total time spent in a community center, borough office, welfare center, or club that offered formal programs for hobbies, entertainment, or education for competency development, or volunteering per one month during the past year. Individual cognitive activity was measured by the number of times participants watched movies, performances, concerts, exhibitions, or sports games over one year. The group cognitive activities were assessed through three questions regarding the time spent participating in the previously mentioned three types of activities, with the score range being 0 to 96. Individual cognitive activities were examined through a single question, with the score range being 0 to 30.
Statistical Analysis
Descriptive statistics were used to analyze the baseline characteristics of the participants surveyed in 2012, the first time point used for this study. An unconditional model analysis of the latent growth model (LGM) was then performed to confirm the trajectory of changes in participants’ cognitive function, the average rate of change, and individual differences in changes using data collected at five time points from 2012 to 2020 over the 8-year period. Additionally, a conditional model analysis was conducted by adding covariates to determine which factors affect the initial value and rate of change in cognitive function in older adults.
To verify the model, the goodness of fit for each model was checked during data analysis. Besides the CMIN/df value (chi-square test value), other indices used included the Normed Fit Index (NFI), Tucker–Lewis Index (TLI), Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), and Akaike Information Criterion (AIC). A model is considered suitable if the CMIN/df value is less than 3, the CFI and TLI values are more than 0.9, and the RMSEA value is less than 0.08, with a lower AIC value indicating a better fit (Hu & Bentler, 1999; Jung & Kim, 2020). However, the chi-square test is sensitive to sample size (Bentler & Bonett, 1980) and may not be suitable if the sample size is too large. Therefore, the goodness of fit was evaluated based on the NFI, TLI, CFI, RMSEA, and AIC values, and the best model was selected.
For descriptive statistics, IBM SPSS Statistics 26.0 (IBM Corp, Armonk, NY, USA) was used, and the latent growth model analysis was conducted using IBM SPSS Amos 29.0 (IBM Corp, Armonk, NY, USA).
Ethical Approval
The data used in this study is derived from a national survey, and since anonymized data was obtained from a national agency, individual participant consent was not required. Prior to conducting the data analysis, ethical review and approval were obtained from the institutional review board, and the analysis was carried out based on this approval.
Results
Demographic Characteristics
Demographic Characteristics (N = 2445).
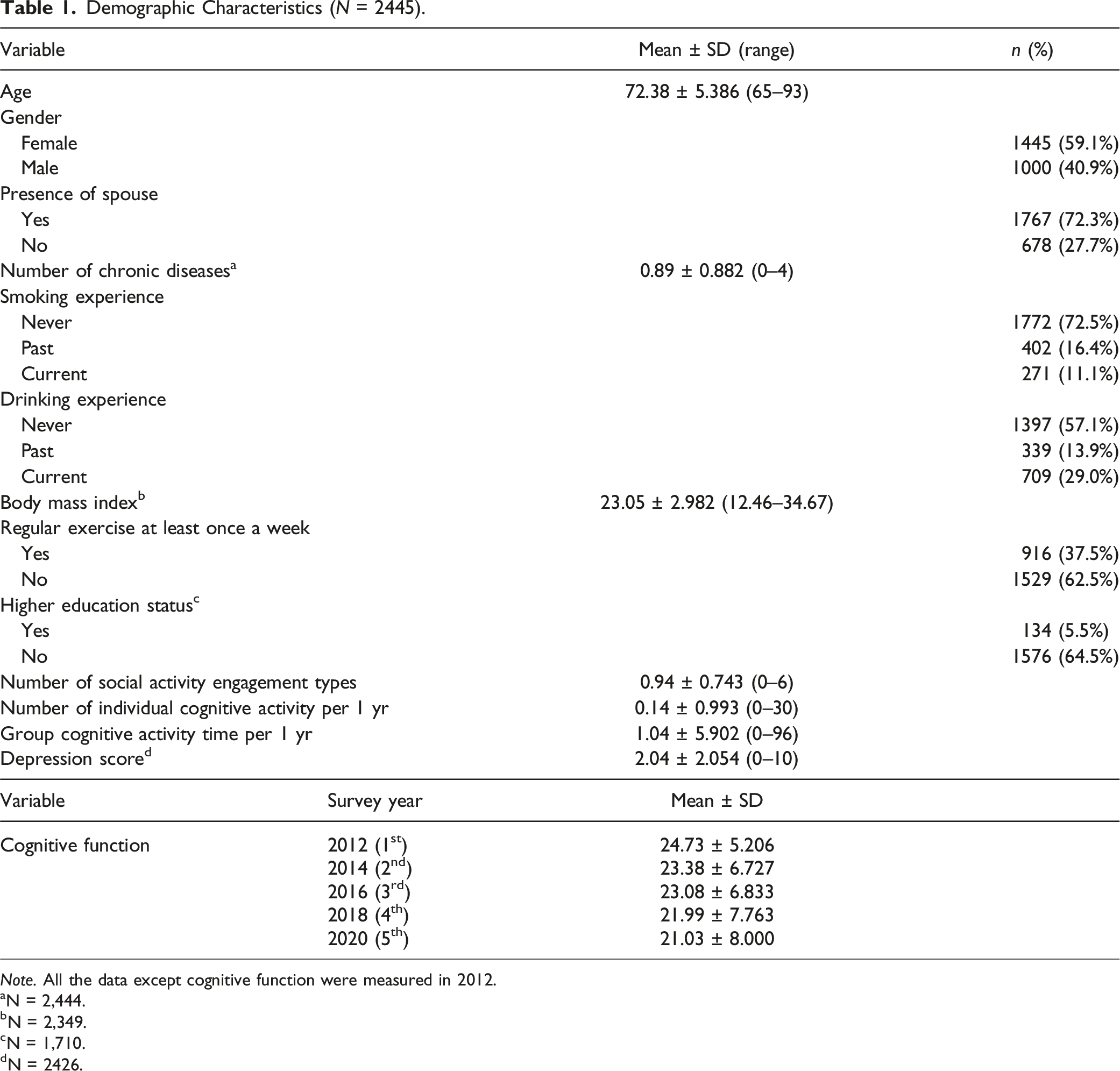
Note. All the data except cognitive function were measured in 2012.
aN = 2,444.
bN = 2,349.
cN = 1,710.
dN = 2426.
Cognitive Trajectory
Goodness-of-Fit Statistics for the Estimated Unconditioned Models.
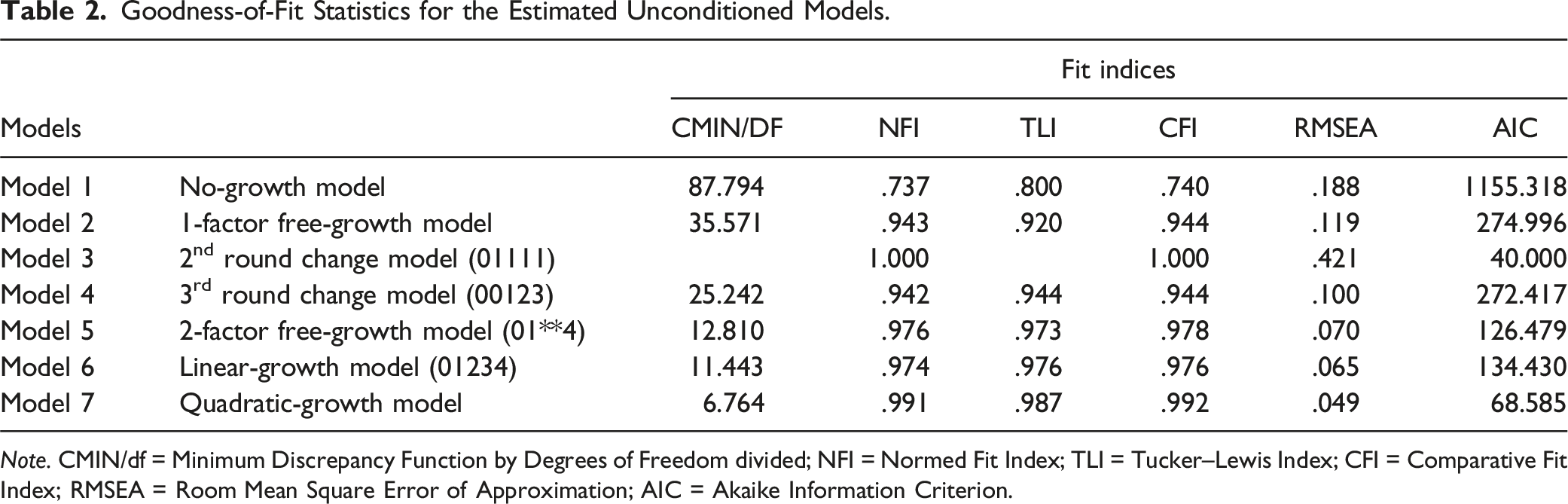
Note. CMIN/df = Minimum Discrepancy Function by Degrees of Freedom divided; NFI = Normed Fit Index; TLI = Tucker–Lewis Index; CFI = Comparative Fit Index; RMSEA = Room Mean Square Error of Approximation; AIC = Akaike Information Criterion.
Means and Variance of the Intercept and the Slope of Model 6.

Predictors of Cognitive Function
Estimates of the Conditioned Model.
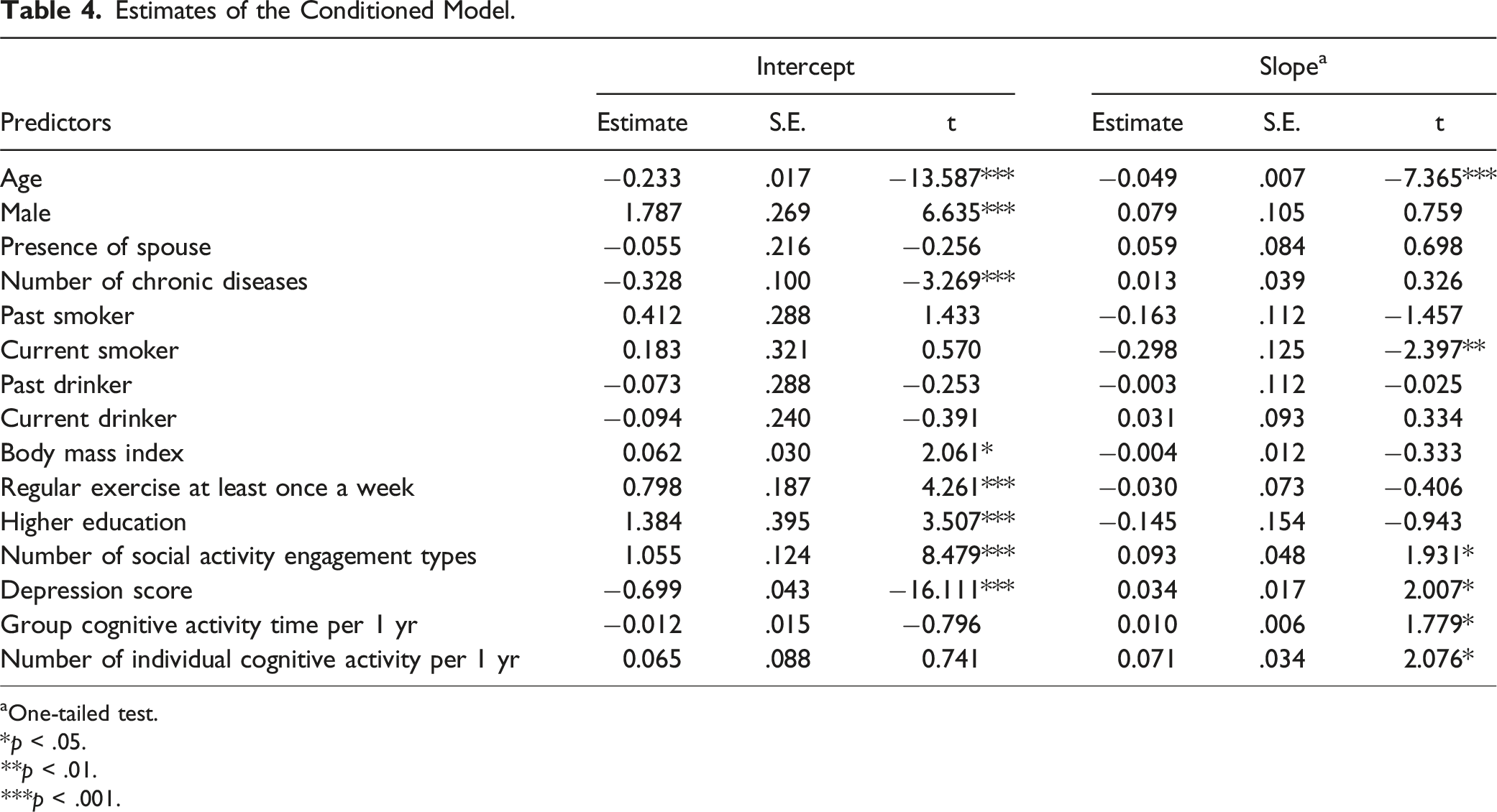
aOne-tailed test.
*p < .05.
**p < .01.
***p < .001.
Initial cognitive function was significantly influenced by age, gender, number of chronic diseases, BMI, regular exercise, higher education, number of social activities, and depression scores. Specifically, older age predicts a lower initial cognitive function (p < .001), being male is associated with a higher initial cognitive function (p < .001), and a higher number of chronic diseases predict a lower initial cognitive function (p < .001). Higher BMI (p < .05), regular exercise (p < .001), higher education (p < .001), and more social activities (p < .001) predict higher initial cognitive function, while higher depression scores predict lower initial cognitive function (p < .001). Factors such as having a spouse, past and current smoking and drinking status, time spent on group cognitive activities, and the number of individual cognitive activities did not significantly affect initial cognitive function. The rate of cognitive decline was significantly influenced by age, current smoking status, social activity engagement, depression scores, group cognitive activities, and individual cognitive activities. Older age (p < .001) and current smoking status (p < .01) predict a faster decline in cognitive function, while more social activities (p < .05), higher depression scores (p < .05), time spent on group cognitive activities (p < .05), and more individual cognitive activities (p < .05) predict a slower decline. Gender, having a spouse, number of chronic diseases, past smoking status, past and current drinking status, BMI, regular exercise, and higher education did not significantly affect the rate of cognitive change.
Discussion
The findings of this study confirmed that older adults’ cognitive function decreased over time and that individual differences existed in these declining trends. As reported in several studies, cognitive function normally shows a declining trend with aging (McQuail et al., 2015; Murman, 2015). This trend was also observed in this study, which showed that older adults’ cognitive function consistently declined over time. Previous research has shown that older adults’ cognitive function is associated with physical performance, activities of daily living, and quality of life, all of which have a significant impact on older adults’ lives (Pan et al., 2015; Vance & Crowe, 2006; Wang et al., 2022).
In this study, the participants had higher initial cognitive function if they were younger, were male, had fewer chronic diseases, exercised regularly, were highly educated, participated in more social activities, and were less depressed. These findings are consistent with previous studies. Research has shown that hypertension, heart failure, and chronic pulmonary diseases, which cause changes in brain structure, are related to cognitive decline (Xie & Xie, 2019; Zuo & Wu, 2022). Evidence indicated that continuous and currently maintained exercise habits are associated with better cognitive function (Tsai & Chang, 2019), while physical inactivity is linked to cognitive decline (De la Rosa et al., 2020). Additionally, education levels have been found to correlate with cognitive function and a lower risk of developing dementia in the future (Lövdén et al., 2020). Depression has also been associated with cognitive decline, with depressed older adults being about 22% more likely to suffer cognitive impairment than those who are not depressed (Muhammad & Meher, 2021).
Regular exercise significantly predicted initial cognitive function but did not slow cognitive decline in this study. Despite this, regular exercise has been shown to enhance cognitive ability, mitigate cognitive aging, and potentially lower the risk of Alzheimer’s disease and other dementias (Kennedy et al., 2017). Previous research has indicated that physical exercise can increase the brain’s gray matter and improve neuroplasticity (Mandolesi et al., 2018). In other words, engaging in physical activity may serve as a protective factor against neurodegeneration and help prevent age-related cognitive decline (Mandolesi et al., 2018). Among various forms of exercise, aerobic exercise has been highlighted as particularly beneficial (Paillard, 2015), especially when performed over an extended period and at moderate to high intensity, with moderate duration, as single-session exercises are considered to have minimal effects (Mandolesi et al., 2018). In this study, the focus on whether participants engaged in exercise at least once a week did not provide information on the specific amount of exercise, types of activities, or duration of the sessions. Therefore, it is important to avoid definitively concluding that regular exercise cannot prevent cognitive decline based solely on this data. Notably, this study addresses whether the exercise conducted in the early stages can predict subsequent cognitive decline. To confirm this more accurately, diverse information regarding exercise, in addition to the mere frequency of participation, is necessary.
This study found that higher age, current smoking, number of social engagement types, depression level, group cognitive activity, and individual cognitive activity affect changes in cognitive function in older adults over time. Specifically, older adults showed greater cognitive decline if they smoked, were less depressed, and did not participate in cognitive activities. Previous studies have shown that nicotine affects acetylcholine receptors in the brain, impacting cognitive function (Amini et al., 2021; Chen & Chang, 2016). Additionally, smoking has been reported to reduce cognitive reserve. One study indicated that baseline smokers were more likely to show cognitive decline compared to non-smokers (Amini et al., 2021).
Previous studies have shown that leisure activities are related to cognitive function, and similar results were confirmed in this study. Another study found that leisure activities were related to spatial ability and memory performance (Hassing, 2020), and participation in stimulating cognitive activities was associated with a lower incidence of Alzheimer’s disease (Kim et al., 2020; Vance & Crowe, 2006). Furthermore, board gaming was found to be effective in improving cognitive functions such as attention, concentration, and memory. Handwriting also improved cognitive function, whereas activities such as reading and cooking did not show significant effects (Iizuka et al., 2019). According to prior studies, the impact of activities on cognitive function varies depending on the type of activity (Kim et al., 2020). Therefore, while the duration or frequency of engaging in stimulating activities is important, the type of activity can also significantly influence cognitive function. Notably, the results of this study indicate that both individual and group cognitive activities positively affect the reduction of cognitive decline. Thus, it is necessary to encourage older adults to engage in both small and large stimulating activities for the preservation of their cognitive function.
However, the relationship between depression and cognitive function in this study was inconsistent with previous research, which reported that more depressed participants experienced a significantly steeper decline in cognitive function (Formánek et al., 2020; Zhu et al., 2022). In this study, older adults with higher depression scores had lower initial cognitive function, but their cognitive function decreased relatively less over time. The initial score aligns with the results of previous studies (Scult et al., 2017; Teles & Shi, 2021), but the slope shows a different pattern. In another prior study examining the relationship between changes in depressive symptoms and cognitive function, it was reported that consistently high depressive symptoms and increasing depressive symptoms were associated with a faster rate of cognitive decline (Yin, John, & Cadar, 2024). Conversely, when depressive symptoms improved, the rate of cognitive decline was less steep. In this study, the analysis was based on initial depression scores, which presents a challenge in assessing how these scores change over time. Additionally, the average depression score in this study was low, approximately 2 out of 10, suggesting that the depression levels were not sufficiently high to significantly promote cognitive decline. Therefore, caution is warranted in interpreting the results of this study, and further research is needed to clarify the relationship between depressive symptoms and cognitive function.
When the factors affecting initial cognitive function in this study are classified based on the model of neuroplasticity and cognitive reserve (Vance & Crowe, 2006), it is evident that modifiable health factors, education, social support, and positive affect influence initial cognitive function. Improving health-related factors, such as reducing the prevalence of chronic diseases and promoting regular exercise, positively affects current cognitive function in older adults. In particular, participation in stimulating activities has little effect on current cognitive function, but it significantly affects changes in cognitive function over time. It is important to allow older adults to participate in stimulating activities which slow down cognitive decline and help them maintain higher cognitive function over time. Creating an environment where they feel socially supported and experience more positive affect can help preserve cognitive function. It is necessary for local communities and various social organizations to offer classes related to various activities that can be performed in groups or individually, making it easier for older adults to participate. Given the steady decline over time, it is necessary to establish various social and policy measures to support these efforts.
Because this study included only participants who completed cognitive function data for all five time points over the 8-year period, the findings need to be interpreted with caution. When comparing the data of 1869 individuals excluded due to missing values with that of 2445 individuals, it was found that those with missing values had lower initial MMSE scores, were older, participated less in group activities, had a higher number of chronic diseases, had lower BMI scores, and had higher depression scores. Additionally, they spent less time in group activities, had a higher proportion of men, and a higher proportion of women, and were less likely to engage in regular exercise.
This suggests a limitation in that individuals with lower initial cognitive function and those more vulnerable to cognitive decline may have been excluded from the analysis in this study. Various reasons could contribute to participant dropout, including refusal to participate, as well as factors such as death and worsening health conditions. Therefore, it is possible that these vulnerable individuals did not participate in subsequent data collection due to health deterioration, highlighting a limitation of the latent growth model analysis method, which cannot utilize the data of excluded participants. However, the data of the 2445 individuals included in this study show that their initial MMSE scores were distributed within the range of 0–30. This indicates that while some vulnerable individuals were excluded, the study still included participants with a diverse range of cognitive function levels. To address this, future research should consider including data with missing values in the analysis.
Due to the nature of secondary data analysis, there are also other limitations that the study participants were selected through convenience sampling and it is hard to choose the scale which is fit to the study. Participants who completed cognitive function assessments over five waves may not be representative of the general older population, potentially introducing bias into the results. Additionally, the study was limited to an 8-year period, which may not capture the full trajectory of cognitive decline in older adults. In the data used in this study, validated tools such as the MMSE and CES-D were employed to assess participants, while other items were surveyed using single questions. This may pose challenges in comprehensively addressing specific aspects of certain items. Therefore, using validated measurement tools for the assessment would be beneficial. Future research should employ longer follow-up periods and theory-driven frameworks to better understand the complex interaction of health, social, and psychological factors in cognitive aging using reliable scales.
Conclusions
The results of this study provided insights into predictors affecting initial cognitive function and the rate of cognitive decline in older adults. The rate of cognitive decline in older adults varies widely among individuals. The findings can serve as a basis for developing strategies tailored to the conditions of older adults. Appropriate education and interventions can be offered according to individuals’ physical, psychological, social characteristics, and lifestyle. Furthermore, it is critical to increase social and cognitive activities, which have been found to positively affect older adults’ cognitive function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2023R1A2C1006362).