
Abstract
While technology holds great promise for promoting independent living, older adults still encounter challenges with technology adoption. The current study identified classes of technology users among older adults and examined associations between technology user class and individual characteristics. The Technology Assessment Procedure method was utilized. Participants (N = 187, ages 65–92) were presented with technologies spanning domains of transportation, leisure, health, and new learning, and rated various measures related to technology adoption. Two user groups, “open to technology” and “reluctant to technology,” were identified. The “reluctant to technology” group, indicated needing more help with new technologies, had less confidence using technology, perceived greater losses associated with aging, and reported less technology experience. In contrast, the “open to technology” group showed higher levels of crystallized intelligence, greater openness to experience, and lower perceptions of aging-related loss. Interventions promoting technology adoption should focus on boosting technology-efficacy, confidence, and accessibility of technology applications.
• Cluster analyses identified two classes of users (“open to technology” and “reluctant to technology”) with respect to adoption of technology related to aging in place within a diverse sample of older adults. • Findings identified factors important to technology adoption beyond demographic variables. • Compared to the “open to technology” group, those in the “reluctant to technology” groups higher perceptions of loss with aging and lower crystalized intelligence scores and less technology experience. A person’s sense of their capacity to utilize and adapt to technology may be undermined by the internalization of negative stereotypes of age-related losses and cognitive abilities.
• Findings provide insight into interventions that can help older adults successfully adopt technologies that can foster independent aging. This is relevant for current and future generations of older adults who will inevitably confront the need to adopt unfamiliar technologies. • Interventions should promote technology self-efficacy and confidence to support older adults’ adoption of technology related to aging in place. • Interventions to foster technology adoption should address factors beyond the demographic factors to target modifiable factors such as self-ageism.What this paper adds
Applications of study findings
Background and Objectives
Technology to Support Older Adults Aging in Place
According to the Center for Disease Control and Prevention (CDC), aging in place refers to “the ability to live in one’s own home and community safely, independently, and comfortably, regardless of age, income, or ability level” (Center for Disease Control and Prevention, 2017). Key components to support older adults aging in place include activities of independent living (e.g., transportation), communication, social connectivity, and access to healthcare (National Institute on Aging at NIH, n.d). Technologies such as mobile phone applications, the internet, or other types (e.g., smart-home, robots) of technology have shown great potential in supporting older adults’ independent living (e.g., Peek et al., 2016). For example, a mobile app intervention utilizing Lyft to provide transportation to older adults resulted in improvements in quality of life and increased social engagement with the community (Saxon et al., 2019). Technology-based social applications have also been shown to increase communication and social connectivity among older adults (Barbosa Neves et al., 2019; Czaja et al., 2018). Moreover, telehealth applications and mHealth interventions designed for older adults are effective in patient self-management and many health-related outcomes (e.g., quality of life, physical activity, chronic disease) (Kruse et al., 2020; Markert et al., 2021; Rasche et al., 2018). While technology holds promise in fostering independent living, older adults still face barriers to adopting technology with a lower rate of technology use compared to younger adults (Berkowsky et al., 2017; Levine et al., 2016; Wilson et al., 2021). Thus, it is important to examine factors to promote equitable adoption of technologies related to aging in place among older adults.
Digital Divide in the Context of Aging in Place
The digital divide refers to the gap between those who use and have access to technologies (e.g., internet, smartphone) and those who do not (Cohron, 2015). Older cohorts, households with less annual income, those with less education, those who live in rural locations, and people with worse health conditions (e.g., disabilities) often lack access to technology or use technology less compared to their counterparts (Elena-Bucea et al., 2021; Fang et al., 2019; Lustria et al., 2011). The digital divide related to aging in place is caused by factors such as financial constraints, geographic disparity (e.g., rural), technology literacy, physical and cognitive impairments, and negative perceptions of technology (Fang et al., 2019; Levine et al., 2016). While older adults have been increasingly using technology over the past decade (Faverio, 2022), older adults with less technological experience face a steeper learning curve compared to younger adults. The digital divide is still prominent and widens the gap in health disparities among vulnerable populations, particularly older adult cohorts and those in lower-income communities. This was clearly evidenced in the COVID-19 pandemic when reliance on digital tools for health-related activities and communication vastly increased (Lai & Widmar, 2021; Litchfield et al., 2021) and there were differences in access and use among “at risk” older populations. Moreover, other consequences of digital divide that affect aging in place include reduced independence due to lack of support for daily activities, increased social isolation and loneliness, decreased quality of life, and barriers to accessing essential services related to independent living (e.g., transportation, access to healthcare, social programs) (Fang et al., 2019; Levine et al., 2016).
Technology Adoption Models
Several models exist that outline the factors that impact technology adoption. The Technology Acceptance Model (TAM) posits perceived usefulness, perceived ease of use, and attitude toward using technology as three factors that determine technology acceptance among users (Davis et al., 1989). The Unified Theory of Acceptance and Use of Technology (UTAUT) model identified facilitating conditions, social influence, effort expectancy, and performance expectancy as four factors that influence people’s intention to adopt technology (Venkatesh et al., 2003). Moreover, UTAUT also highlighted demographic characteristics such as age and gender as moderators in technology adoption (Venkatesh et al., 2003). However, the TAM and UTAUT models were not initially developed for older adults but rather targeted younger adults such as students or users in workplace settings. The Senior Technology Acceptance Model (STAM) was developed based on the TAM and UTAUT framework to understand technology adoption among older adults by adding age-related health and ability characteristics (Chen & Chan, 2014). However, this model did not focus on factors that may influence older adults’ willingness to adopt new and unfamiliar technologies related to aging in place. The current study extends existing models to identify additional factors that are related to the adoption of new technologies related to aging in place (e.g., transportation, telehealth, communication), such as willingness to adopt, perceived value, perceived effort, help, confidence, privacy concerns, and quality of life.
Other Factors Related to Technology Adoption
Beyond demographics, individual differences in abilities such as intelligence (crystallized or fluid), problem-solving, comprehension, and reasoning, as well as individual differences in personality traits such as perceptions of aging (loss or gain) or openness to new experience may also relate to technology adoption. Studies have shown that older adults with less cognitive abilities, such as fluid and crystallized intelligence or comprehension skills were less likely to adopt technology (e.g., Czaja et al., 2018; Mitzner et al., 2019; Nori et al., 2020). Moreover, older adults with greater perceptions that aging is associated with loss often face barriers to technology adoption due to the negative self-stereotypes of aging and self-perceptions of lack of ability to adopt and use technology (Low et al., 2021). Research has also revealed that people with more openness to experience are more likely to rate technology as useful and easier to use (Mitzner et al., 2016). However, past studies and existing technology adoption models often focused on broader technology use and adoption (e.g., email, internet) rather than technologies in the context of aging in place (Choi & DiNitto, 2013; Choi et al., 2022; Hunsaker & Hargittai, 2018). The current study extends these models by incorporating non-demographic factors (e.g., individual differences), providing a more nuanced understanding of technology adoption in the context of aging in place. Our approach is also unique as it focuses specifically on examining differences within an older cohort, providing insights that are directly applicable to this demographic and can guide the development of tailored interventions aimed at enhancing the quality of life for older adults.
Objectives
The purpose of the current study was to expand our understanding of factors influencing the adoption of technology related to aging in place among older adults. Ultimately the findings will help identify the development of more efficacious interventions or technologies to support older adults to age independently. A unique aspect of this study was to contribute further to existing models of technology adoption by using cluster analysis techniques to examine variations in use within an older adult population. Cluster analysis was chosen due to the size and depth of the available data, and provided a different way of exploring and highlighting the diverse profiles of how older adults view technology related to aging in place. This methodology allows for the identification of distinct groups based on shared characteristics, by sorting the population into groups who share a similar pattern of experiences across multiple variables. This offers a comprehensive understanding of technology patterns among older adults. Cluster analysis also provides an effective way to segment the population, making it possible to identify the specific needs and preferences of different subgroups. Thus, this approach afforded us an opportunity to provide a more nuanced view of adoption technology related to aging in place and identifying common barriers to adoption, ultimately informing the development of more personalized and effective intervention and support strategies. The study objectives were to (1) identify different types of users based on ratings of willingness to adopt different types of technology related to aging in place (e.g., transportation, telehealth) using cluster analysis; (2) characterize each cluster by demographic (age, education, income, and self-rated health) and individual differences variables (objective abilities, subjective perceptions of ability, and personality traits); and (3) explore whether cluster membership and individual differences predicted technology experiences.
This study extended previous research and made several unique contributions to the literature. First, participants with no prior experience with the targeted technologies were provided with a detailed walkthrough of the various types of technology (see Moxley et al., 2022). This differed from past studies that often used surveys or questionnaires and asked participants to retrospectively recall their experience with technologies (Gell et al., 2015; Hunsaker & Hargittai, 2018; Quinn, 2010). Second, past studies often compared users who were already familiar with the technology with those who had no prior exposure to the technology, which may include many confounding factors (Choi & DiNitto, 2013; Duplaga, 2021; Hunsaker & Hargittai, 2018). Participants of the current study were all newly exposed to each type of technology related to aging in place. Third, differing from past studies that examined individual factors related to decisions about technology adoption among older adults (Berkowsky et al., 2017; Czaja et al., 2006; Moxley et al., 2022), the current study identified cluster groups within older adults and analyzed the characteristics of the cluster groupings. Fourth, past studies often focused on general technology use and adoption (e.g., email, internet) (Choi & DiNitto, 2013; Choi et al., 2022; Hunsaker & Hargittai, 2018). The current study adds to the literature by focusing on the adoption of technology related to aging in place within a diverse population of older adults.
Research Design and Methods
The study was approved by the University’s Institutional Review Boards (approval #1808019538). Written informed consent was obtained from each participant before the study. The current study constitutes a secondary analysis of an experimental study examining older adults’ technology adoption. Detailed methods of the original study are reported in the paper by (Moxley et al., 2022).
Participants
Participants were recruited (2017–2019) from two large East Coast cities in the US through local media advertisements, older adult community service agencies, and participant registries. Inclusion criteria included age 65 years or older, able to read and understand English at the sixth-grade level, able to hear with or without correction as evidenced by their ability to hear and respond to queries appropriately during the telephone screening, a vision of at least 20/70 with or without correction, and able to write or use a keyboard, mouse or a laptop computer. Participants were non-cognitively impaired as assessed by the Telephone Interview for Cognitive Status (TICS) and defined by a cutoff score adjusted for age and education (e.g., for people between 70 and 79 years of age. A minimal score of 29 was required for those with less than a high school education, and a minimal score of 31 was required for those with at least a high school education) (Lopez & Kuller, 2010). Further, participants could not have prior experience with any of the five technologies presented in the study. Participants were compensated $40 for participation and reimbursed for parking or transportation expenses upon study completion.
Participants (N = 187) ages ranged from 65 to 92 (M = 74.1, SD = 6.3). About 80% (78%) of the sample were women, 84% had at least some college education, 83% were retired, and 90% self-reported good health. The sample was ethnically/racially diverse with 21% of the sample identified as Hispanic and 36% identified as Black or African American (See Moxley et al., 2022 for a full descriptive of the sample).
Procedure
The current study utilized a modified version of the Technology Assessment Procedure (TAP), a mixed-method data collection technique (Berkowsky et al., 2017), where groups of 2–4 participants were given PowerPoint presentations about five technologies in a randomized order. The five technologies were Lyft (a ride-sharing app), eCareCompanion (a telehealth app to share health information with care team and track health tasks), Curious.com (a website with lessons on a variety of topics), InteliChart (a patient portal with medical charts and appointments/other healthcare-related management), and Fittle (a fitness app with a social support component). The current analyses did not include the Fittle app given that the focus was on technologies that directly facilitate independent living for older adults. After each presentation, participants rated the technology on criteria related to the adoption of that technology. They were allowed to ask clarification questions about each technology but were not permitted to discuss the technologies amongst themselves. Then, participants completed additional instruments to complement the ratings. The current study focused on the quantitative data derived from the study.
Measures
Technology ratings for each technology included criteria that measured participants’ willingness to adopt (“How willing are you to take up the technology and start using it?”), perceived value (“How would you rate the importance or value”), perceived effort (“How much effort do you think you would have to put into learning and mastering”), help with technology (“How much help would you need from family and friends to learn and master”), confidence in using technology (“How confident are you that you have the ability to learn and master”), concerns about privacy (“How worried or concerned are you about privacy and trust issues”), and quality of life (“How much can the technology just presented to you help improve your quality of life”). Each criterion used a 9-point Likert scale (1 being not at all, 5 being some, and 9 being a lot). All scores were coded such that higher values indicated higher ratings of the criteria.
The demographic measures included age, education, income, and self-reported health (Likert scale rating from 1 = “poor” to 5 = “excellent”). Other measures included measures of objective abilities (crystallized and fluid reasoning), assessed by the Shipley Vocabulary test (Zachary & Shipley, 1986); subjective ratings of crystallized (summed across 3 items: vocabulary, comprehension, and numeric ability) and fluid intelligence (summed across 4 items: memory, learning ability, applying new knowledge, and problem-solving and reasoning) based on a 9-point scale (1 = very low ability; 9 = very high ability) (adapted from Ackerman & Wolman, 2007); and personality traits (perceptions of aging—loss or gain) (Kaspar et al., 2019), and openness to experience (Gosling et al., 2003). Technology experience was measured by summing responses to questions regarding use (1) or non-use (0) of a desktop computer, laptop, smartphone, tablet, and internet or email. Scores ranged from 0 to 5. Higher scores indicated higher values for all measures.
Statistical Analyses
The missing data was trivial (0.3% of the data were missing), so list-wise deletion was used for all the analyses. Two-step cluster analyses were conducted in SPSS, in which each technology rating for each technology type was used to create the clusters. This procedure comprises two steps. In the first step, a pre-clustering method is used to identify and store summary features of the data that are in dense regions (multiple data points being close to each other in values). The second step involves applying a hierarchical clustering algorithm to cluster those dense regions and using a model selection criteria to the different cluster number solutions to select a single solution (Chiu et al., 2001). The method is computationally efficient, can be used for continuous or categorical data, and also provides information on the variables that were most important in the cluster classifications, as classified by the “Importance” score, which is a relative measure that examines the extent each item contributed to the cluster creation (Tkaczynski, 2017).
Hierarchical logistic regression was then used to predict cluster membership by entering each set of regressions separately and jointly with the subsequent sets of variables: demographic variables (age, education, income, and self-reported health), objective ability measures (crystallized and fluid intelligence), subjective rating of abilities (self-assessed cognitive abilities), and personality traits (openness to experience, perception of loss in aging, and perception of gain in aging). Finally, the interaction effects of cluster membership with factors such as crystallized intelligence, perception of loss in aging, and openness to experience were tested using regression to predict technology experience. Given that technology experience was not distributed normally, we conducted a Jaekel–Hettmansperger–McKean (Hettmansperger & McKean, 1998) test using the “rfit” module in R (Kloke & McKean, 2024) to conduct non-parametric regressions for models with technology experience as an outcome. All of the models were multivariate models, and we only interpreted individual parameters if the model was significant.
Results
Cluster Analysis
The results of the cluster analyses indicated a 2-cluster solution, which identified two types of users. The cluster cohesion and separation were assessed by Silhouette (S) which measures how similar an item is to its own cluster compared to the other clusters, which indicated a fair cluster fit (S = .3). Figure 1 depicts the cluster membership criteria ratings for the identified clusters based on the importance scores (Figure 1). Cluster 1 included 51% (95/187) of the participants described as “reluctant to technology.” Cluster 2 included 49% (92/187) of the participants labeled as “open to technology.” Compared to participants labeled “open to technology,” “reluctant to technology” participants indicated needing more help using all the technology and reported less confidence with technology, particularly telehealth-related technology such as eCareCompanion and IntelliChart. They were also less willing to adopt technology and reported less perceived value of technology and more perceived effort to use technology and more privacy concerns. All results reported were statistically significant at p < .001 level. Cluster membership criteria rating ranked from most importance (Left) to less important (Right).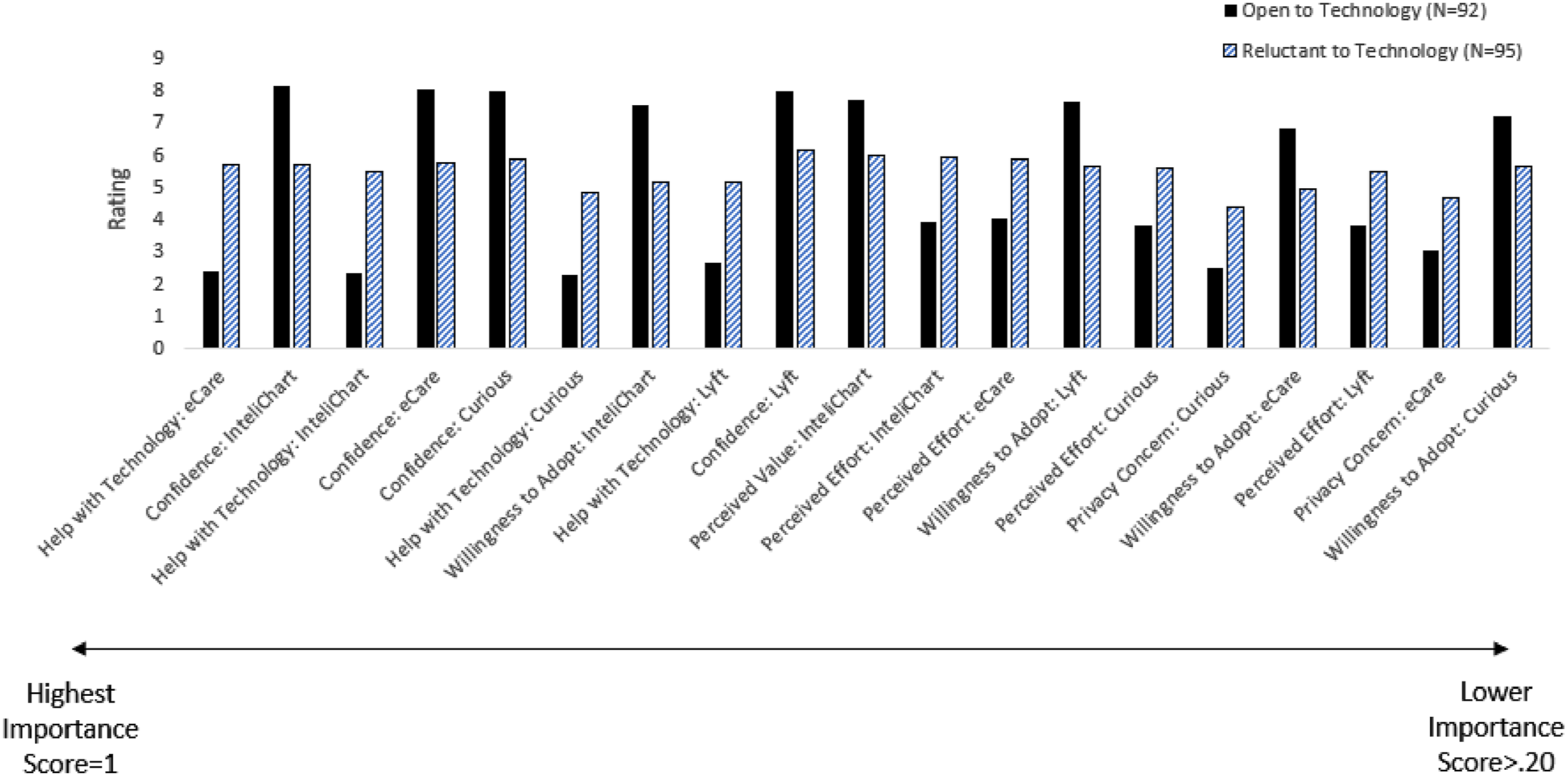
Variables Associated With the Clusters
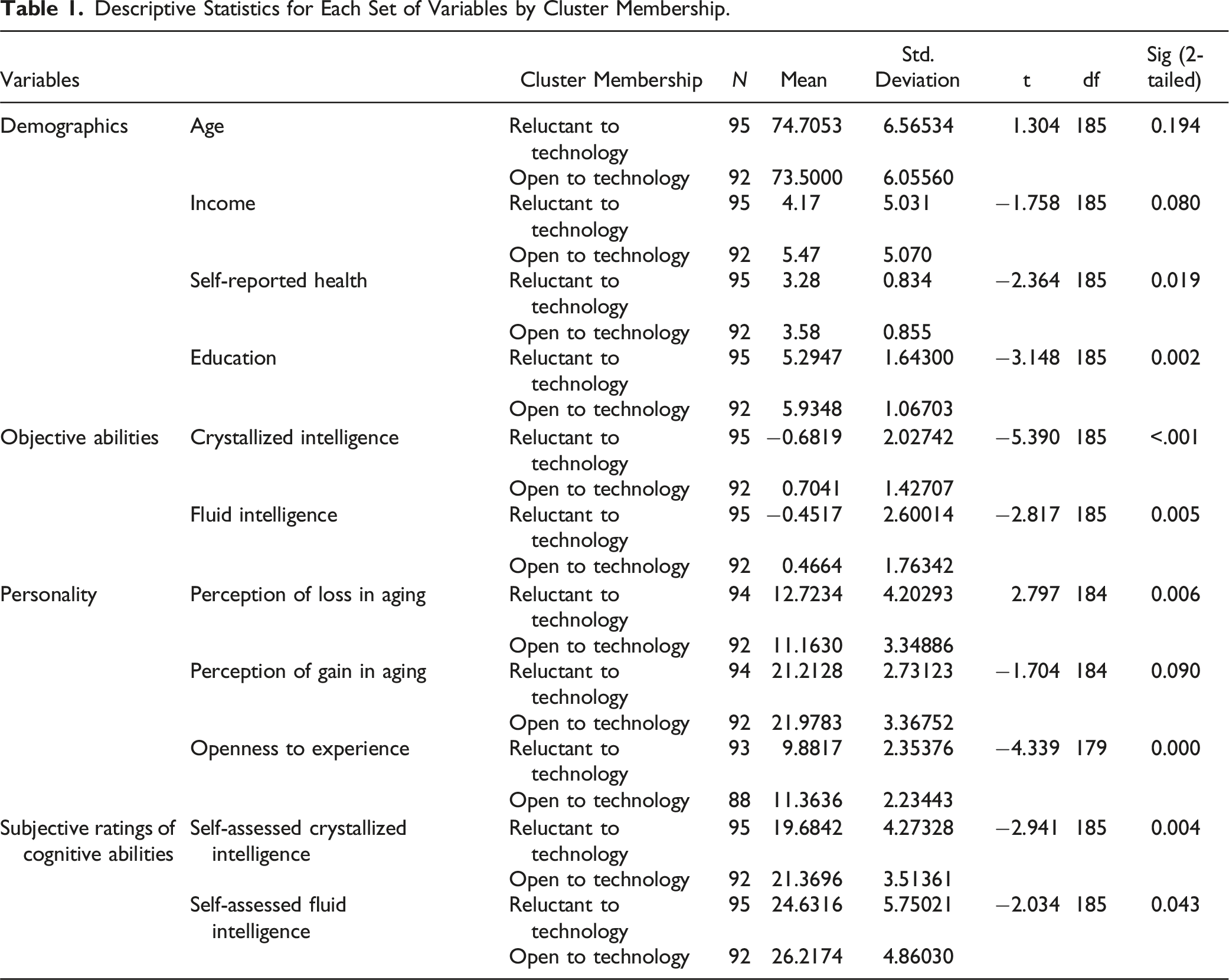
Descriptive Statistics for Each Set of Variables by Cluster Membership.
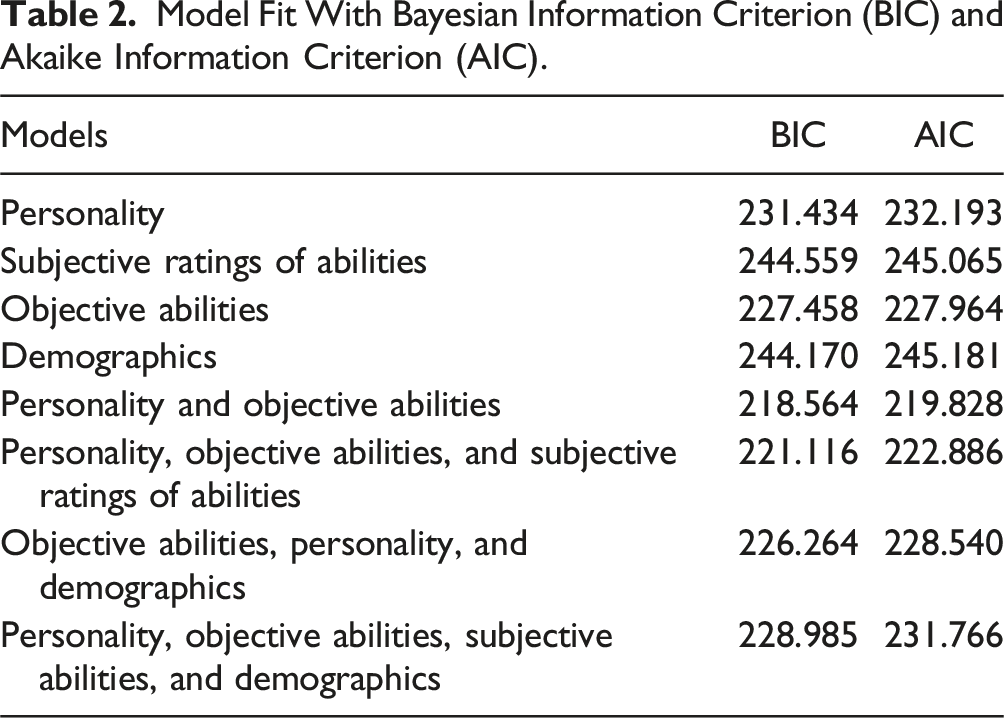
Model Fit With Bayesian Information Criterion (BIC) and Akaike Information Criterion (AIC).
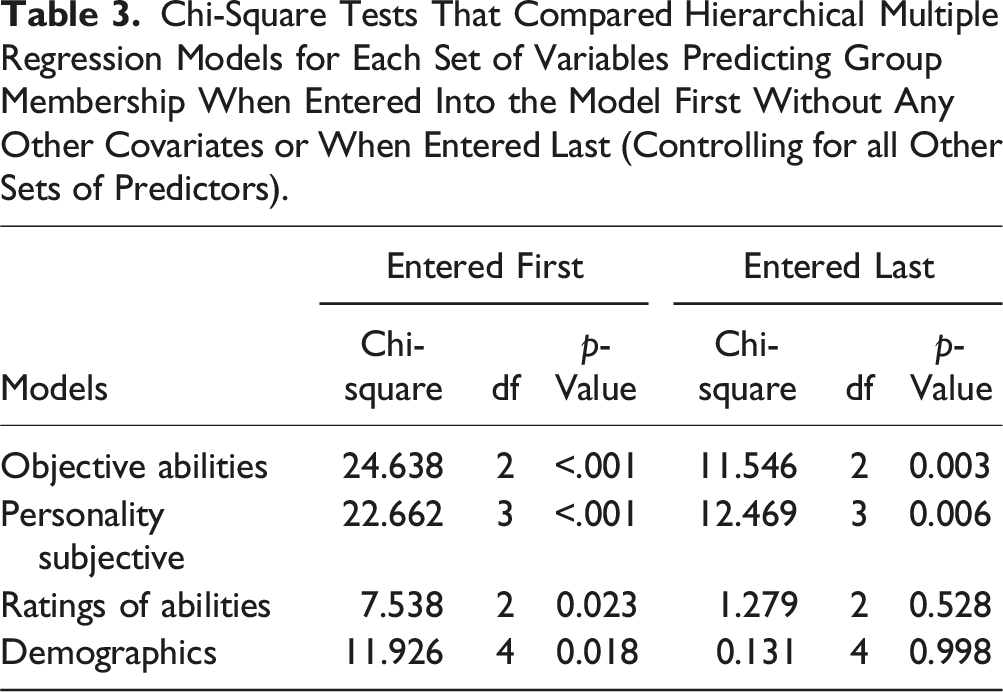
Chi-Square Tests That Compared Hierarchical Multiple Regression Models for Each Set of Variables Predicting Group Membership When Entered Into the Model First Without Any Other Covariates or When Entered Last (Controlling for all Other Sets of Predictors).
Predictors of Technology Experience
Given that crystallized intelligence, perceptions of loss in aging, and openness to experience predicted cluster membership, it was also of interest to examine whether these measures predicted technology experience. Results of the Jaekel–Hettmansperger–McKean test showed that cluster membership predicted technology experience (Β = .52, t = 3.45, p < .001), such that the “open to technology” group had more technology experience compared to the “reluctant to technology” group. A significant interaction effect was found for cluster membership and perceptions of age-related losses (Β = .13, t = 3.49, p < .001) (Figure 2(a)), such that for those in the “reluctant to technology” group, greater perceptions of age-related losses predicted less technology experience (Β = −.09, t = −4.13, p < .001), but this relationship was not present among those who were in the “open to technology” group (Β = .04, t = 1.23, p = .22). A significant interaction was also found for cluster membership and crystalized intelligence, (Β = −.31, t = −3.68, p < .001) (Figure 2(b)), such that among those in the “reluctant to technology” group, higher crystalized intelligence predicted more technology experience (Β = .42, t = 8.61, p < .001), but again this relationship was not observed in the “open to technology” group (Β = .11, t = 1.53, p = .13). There were no significant interactions for cluster membership by openness to experience (Β = −.02, t = −.41, p = .68) with respect to technology experience (Model Summary: R-Square = .26, p < .001). Interaction effects predicting technology experience. Note. Those in the “reluctant to technology” group with more loss related to perception of aging (a) and less crystallized intelligence (b) demonstrated less technology experience while loss related to perception of aging and crystallized intelligence did not predict technology experience for the “open to technology” group.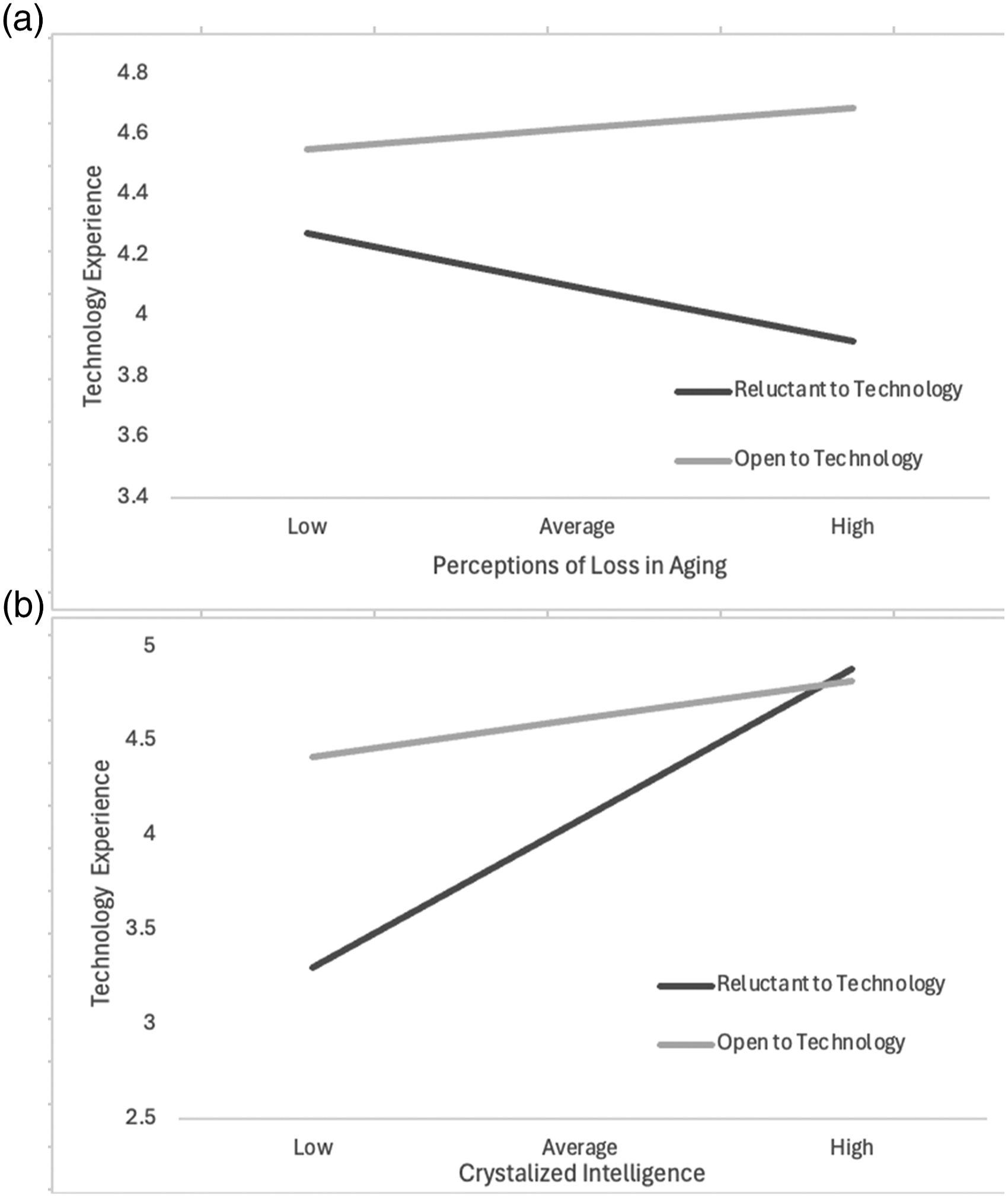
Discussion and Implications
The present study adds to existing technology adoption models (TAM, UTAUT, and STAM) by identifying additional user characteristics important to the adoption of technology related to aging in place within a diverse sample of older adults. In addition, in contrast to assessing factors related to technology adoption based on user’s retrospective recall of their experiences with a familiar technology, the data from this study is unique in that it was based on participants’ concurrent perspectives on new and unfamiliar technologies related to aging in place.
The findings, based on the ratings of the novel technologies, identified two clusters of technology users: those that were “reluctant to technology” and those that were “open to technology.” The “open to technology” group rated high confidence in using technology and a willingness to adopt the novel technologies related to aging in place, whereas the “reluctant to technology” group rated needing more help using technology and reported less confidence with technology, particularly telehealth-related technologies. Compared to the “open to technology” group, the “reluctant to technology” group also reported less perceived value and more perceived effort and privacy concerns in using technology related to aging in place. This result is consistent with the TAM model that suggests the importance of perceived value and ease of use as factors that determine technology adoption and added to the model by revealing that the attitude towards new and unfamiliar technology is directly related to one’s confidence, perceived effort, and privacy concerns. Understanding both user groups informs the design and development of future technologies and interventions to promote technology adoption. Developers should prioritize ease of use and highlight the potential value of technology with respect to daily living, as these are critical factors influencing adoption among older people. Technologies can also be designed with adaptive features that cater to both individuals within both clusters. For example, telehealth platforms could offer basic interfaces for novices and advanced features for more experienced users.
These findings identified some of the barriers to older adults adopting technology related to aging in place and provide insights into interventions that can help older adults, particularly those who are “reluctant to technology,” successfully adopt technologies that can foster aging independently. Consequences of being reluctant to new technologies related to aging in place include remaining in the digital divide and not having access to the potential benefits of these technologies with respect to quality of life. Furthermore, people who are reluctant to adopt technology are at disadvantages as resources access, particularly resources essential to aging in place, are being continuously moved to online platforms (e.g., Social Security, Medicare). This is also relevant for future generations of older adults who will inevitably confront the need to adopt unfamiliar technologies. The findings can also inform policy and practice guidelines, encouraging the adoption of best practices for technology implementation in aging populations. These strategies should promote equitable access to technology, and ensure that all older adults, regardless of their initial attitudes towards technology, benefit from advancements in aging-in-place technologies.
Our findings suggest that telehealth-related technologies are especially challenging for the “reluctant to technology” group. This is likely due to barriers such as a lack of available technical support. In fact, findings show that the needs and abilities of older adults are not considered in many telehealth applications (Kruse et al., 2020; Wilson et al., 2021). This was particularly evident during the COVID-19 pandemic (Elimelech et al., 2022). Future technology interventions for aging in place should provide accessible training and technical support. An alternative approach such as employing simple interactive tutorials that involve hands-on use of the technology by leveraging artificial intelligence (AI) methods can assess user difficulties and offer assistance or guidance to users accordingly. AI applications can be used to adapt complex interfaces and provide personalized support, potentially making technology more accessible for those who struggle. Future research can also consider hybrid approaches that combine AI with human support, ensuring that interventions are inclusive and cater to the diverse preferences of older adults.
Consistent with the literature regarding the digital divide, worse self-reported health, and lower education predicted the “reluctant to technology” membership. However, it is worth noting that after adding these variables to the hierarchical logistic regression set, self-reported health and education were no longer significant predictors of cluster membership. This finding suggests that although demographics are important, it is essential to look beyond the demographic variables and examine other factors such as objective abilities and personality traits that may influence older adults’ willingness to adopt technology related to aging in place. It is crucial for interventions to also address these factors beyond the digital divide, particularly for older adults who are more vulnerable and experience more challenges in using technology.
Our findings complement other findings regarding the digital divide and the UTAUT model that focus on demographic differences such as age in technology adoption; our results indicate that demographic factors such as age and income, although important, were not the primary predictors of cluster membership. One explanation could be a cohort effect, as the current sample only included older adults 65 years or older, who were “digital immigrants” (people who started using technology as adults), whereas past studies tend to include cross-sectional comparisons, comparing, for example, older and younger adults (“digital natives” who grew up with technology) (Lüders & Gjevjon, 2017). Moreover, the sample was recruited from two large cities in the US, where the majority have access to technology given the continuous government and social service initiatives that promote technology use (Vogels, 2021).
Personality traits such as openness to experience and perceptions of loss with aging, as well as crystallized intelligence, predicted cluster membership. Consistent with past research, more openness to experiences and crystallized intelligence, and lower perception of loss in aging were associated with the “open to technology” cluster membership (Czaja et al., 2006; Kornadt et al., 2017; Mitzner et al., 2016). It is crucial to recognize that cognition is key to learning and interacting with new technology. If individuals with lower cognitive abilities are less likely to adopt technology, it may indicate that current designs related to aging in place are too complex. Simplifying designs to accommodate varying cognitive abilities can enhance accessibility and adoption. Intervention programs should be designed to dispel existing myths that older adults are unable to learn new technologies. These strategies should foster the development of technology self-efficacy and more positive attitude towards technology use. They should also reinforce that older adults are capable learners and willing to use technologies that have perceived value with respect to promoting independence. The findings also indicate that current technology adoption models, which often emphasize demographic factors, should be expanded to include personality traits, attitudinal variables related to technology, and cognitive abilities. Incorporating these variables can provide a more comprehensive understanding of the factors influencing technology use among older adults in the context of aging in place. Through inclusion of these variables, existing technology models can be refined to better predict and explain technology adoption behaviors in the context of aging in place among older adults.
Compared to the “open to technology” group, those in the “reluctant to technology” group had less technology experience, which further validates the cluster analysis results. Moreover, among those in the “reluctant to technology” group perceptions of age-related losses and crystalized intelligence were related to technology experience. A person’s sense of their capacity to utilize and adapt to technology may be undermined by the internalization of negative stereotypes of age-related loss (perception of loss in aging) and cognitive abilities, which could ultimately lower their confidence and self-efficacy in adopting new technology. Given that one cannot change people’s demographic characteristics such as age, these findings point to the importance of interventions to target modifiable and malleable factors such as self-ageism. Training programs should also be tailored to the cognitive abilities of older adults with simplified instructions, step-by-step guidance, and more hands-on practice, particularly for older adults who are reluctant to use technology. These findings also shed light on design considerations for technology developers. It is crucial to design user-friendly interfaces that reduce complexity and enhance user confidence, which can ultimately promote greater technology adoption. Moreover, policymakers and advocates should be aware of current barriers to adoption and promote the creation of supportive environments that encourage technology adoption among older adults to facilitate aging in place. This could, for example, include funding for community programs that offer technology training and support.
These findings enrich the literature by elucidating factors beyond those identified by existing models of technology adoption. Further, our focus was on new/unfamiliar technologies that support aging in place technology. The findings provide critical insights into the comprehensive technology experience of older adults. This approach ultimately contributes to a deeper understanding and more effective support for improving support systems for aging in place by identifying common barriers to technology adoption. The findings also inform the development of more tailored interventions to promote older adults’ technology adoption and sustained use.
Strengths and Limitations
The current study contributed to the literature in several ways. First, participants were provided with a detailed walkthrough of various types of technology related to aging in place in an experimental study. Second, unlike prior research, participants of the current study were all newly exposed to each type of technology and thus were subject to fewer confounding variables (Choi & DiNitto, 2013; Duplaga, 2021; Hunsaker & Hargittai, 2018). Third, the current study identified cluster groups based on participants’ technology ratings and characterized the clusters by individual differences beyond the digital divide. Fourth, the present study specifically targeted technology related to aging in place within a diverse sample of older adults. This can provide insight into how technology can best support older adults aging in place and the implications for interventions that can encourage more older adults to adopt technology related to aging in place. Finally, the current study contributes to existing models of technology adoption by using cluster analysis techniques to examine variations in technology use within an older adult population. This approach helps us further understand factors that predispose older adults to adopt new technologies related to aging in place. This in turn can help identify more targeted and effective interventions to support adoption of new technologies that support aging in place. Ultimately, this can enhance the quality of life and independence of older adults. This is particularly important as older adults continually need to confront and adapt to new technologies related to aging in place in an ever-evolving digital landscape.
Limitations of the present study included that participants were recruited from two large cities, and we did not include people from more rural regions. Given the existing wide gap in technology adoption between urban and rural areas (Vogels, 2021), future studies should be conducted across a variety of geographic locations including urban, suburban, and rural locations. Also, participants in the current study were only shown each type of technology and did not have a chance to use each technology, which may have influenced their willingness to adopt the technologies. Moreover, other technologies such as wearables, Virtual Reality, robotics, and artificial intelligence were not included in the present study. Future studies could consider having participants use various other types of technologies and examine whether willingness to adopt the technology changes after engagement with these technologies over time.
Conclusions
The goal of the present study was to further understand factors influencing the adoption of technology related to aging in place among older adults to better support older adults age independently. Two types of users (“open to technology” and “reluctant to technology”) were identified, in which the “reluctant to technology” group rated needing more help using technology and having less confidence with technology. In addition, the findings showed that higher crystallized intelligence, more openness to experience, and less perceptions of loss with aging predicted the “open to technology” cluster membership. Moreover, compared to the “open to technology” group, those in the “reluctant to technology” group that perceived greater loss with aging and less crystalized intelligence had less technology experience. These results call for interventions that could remediate digital inequities and promote technology adoption among those older adults that are reluctant to technology related to aging in place.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health; National Institute on Aging [P01 AG17211]. X.L. acknowledges support from a National Institute on Aging funded T32 Training Program in Behavioral Geriatrics [NIA T32 AG049666].
Institutional Review Board
The study was approved by the Institutional Review Boards of the University of Miami and Weill Cornell Medicine (approval #1808019538).