
Abstract
Alzheimer’s disease and related dementias (ADRD) pose a substantial caregiving burden in the United States, yet efforts to improve caregiver well-being have seen mixed results. We ask whether an app-based intervention (N = 143) to prioritize caregiver respite can substantially improve the caregiving experience, and whether these benefits are moderated by (1) caregiver demographics and (2) conditions of the caregiving situation (such as baseline impairment). Constructing curvilinear growth models to assess changes over a 20-week period, we find significant improvements in the positive aspects of caregiving (PAC). Greater benefits accrue to women, lower-income households, caregivers with a college degree, and caregivers who provide ≥80% of care to their family member. No differences in PAC growth are detected for care recipient memory and behavior problems, caregiver age, or caregiver race. We conclude that efforts to improve caregiver well-being may be especially effective for disadvantaged groups, with the notable exception of educational attainment.
• An online app designed to improve caregiver respite brought significant increases in the positive aspects of caregiving (PAC). • These benefits were larger for disadvantaged groups (with some exceptions).
• “Positive aspects of caregiving” (PAC) is an important and understudied caregiver outcome which is potentially modifiable by TLC, a respite-focused online-delivered intervention. • TLC should be considered a potentially effective intervention to support caregivers—especially those who are most disadvantaged. Targeted delivery to such individuals may provide an effective means of caregiver support. • Future evaluation research should prioritize measurement of PAC and adopt study designs that allow for the exploration of which caregiver characteristics and caregiving circumstances may modify an intervention’s effect.What this paper adds
Applications of the study findings
The number of Americans with cognitive impairments will rise sharply in the coming decades (Hale et al., 2020), imposing a substantial burden on family and other informal caregivers. Scholars have raised concerns about the poor mental health of dementia caregivers, documenting high rates of depression and burnout (Cheng, 2017). While interventions to improve caregiver well-being have proliferated in recent years, effect sizes are small and results are generally mixed (Walter & Pinquart, 2020).
One reason for these findings is that caregiving is not a uniform experience: caregiver characteristics such as age, gender, and race are linked to distinct mental health challenges (Dilworth et al., 2020; Hengelaar et al., 2023; Xiong et al., 2020), while the stresses of caregiving also differ wildly by the circumstances of the caregiving role—stages of disease, prior experience with the care recipient, and more (Choi et al., 2024). Consequently, the efficacy of interventions varies greatly across caregiver subgroups (e.g., Lee et al., 2010). For example, middle-aged caregivers may experience greater stress than older caregivers, in part because they are more likely to balance caregiving with employment (DePasquale et al., 2018; Schulz et al., 2020). Women may benefit more from caregiver interventions than men, given their greater propensity to engage in supportive services and self-help practices (Sagar-Ouriaghli et al., 2019). And, caregivers in different circumstances may need different forms of assistance, for example, practical skills-training versus socio-emotional support (Gaughler et al., 2017). The heterogeneity of the caregiving population and the complexities of the caregiving situation require that scholars explicitly investigate for whom their interventions are most effective.
Though much of the intervention literature has focused on caregiver burden, researchers are increasingly turning their attention to measurement and understanding of the positive aspects of caregiving (PAC; Quinn & Toms, 2019; Lee & Li, 2022). Interventions that emphasize these aspects have been linked to long-term improvements in the caregiving experience (Cheng et al., 2020). Such improvements are not limited to the caregivers themselves: Crucially, people who feel they benefit from caregiving may confer lower mortality risk on their own care recipients (Pristavec & Luth, 2020). Thus, identifying interventions that maintain or improve PAC may be essential in determining the types of support needed for caregivers to continue fulfilling their invaluable role in the delivery of long-term care (Reinhard et al., 2023).
One specific intervention target in which prior efforts have not always been successful is that of respite, or time away from caregiving (Whitmore et al., 2023). While respite is among the most requested sources of support among caregivers (Van Exel et al., 2008), caregivers often report anxiety about their time away from the care recipient and frustration that they have “wasted” precious free time (Lund et al., 2009; Utz et al., 2012; Zarit et al., 2017). Given that respite is highly desired, but its benefits often elusive, scholars have called for the development of more effective respite-focused interventions to support caregivers (Kirk and Summers, 2020; Rose et al., 2015).
In this brief report, we describe a novel intervention designed to improve respite time among caregivers, an online app called Time for Living and Caring (TLC; Utz, Caserta, et al., 2023). We examine the efficacy of the TLC intervention on changes in PAC over a 20-week period. Following previous calls to capture the diversity and complexity of caregiving experiences (Pristavec & Luth, 2020; Whitmore & Swanson, 2024), we test how the effects of this intervention differ by caregiver characteristics (sociodemographics) and conditions of the caregiving situation (e.g., degree of impairment). Results may inform future efforts to develop targeted interventions for caregiver well-being, and may also provide evidence about which segments of the older population may benefit from technology-delivered interventions—an increasingly common way to administer caregiver support (Egan et al., 2018; Etxeberria et al., 2021; Pleasant et al., 2020).
Methods
Data
Time for Living and Caring (TLC) is a self-administered, technology-driven intervention (app or website) that encourages dementia caregivers to make better use of their respite time by setting and evaluating their respite time-use (Utz, Caserta, et al., 2023). During an initial assessment, participants brainstorm activities they may have abandoned due to their caregiving duties and create a “wish list” of activities to prioritize during their upcoming respite. Over a 16-week period, participants are guided through simple, repetitive goal-setting and goal-review exercises where they (1) set weekly goals for respite using a calendar, (2) make a plan to address potential barriers to success, (3) evaluate whether they achieved their weekly goals and how satisfied they were with their actual respite time-use, and (4) receive access to virtual coaching (i.e., automated prompting and links) to maximize the effectiveness of their respite time—whether that time is extensive or very limited. In addition, every four weeks, respondents answer survey questions about their overall mental health, caregiver burden, and positive aspects of caregiving. Data are plotted on an interactive dashboard, intended to help raise caregivers’ self-awareness about the value and benefit of respite for their overall well-being. Final data collection occurs at week 20, four weeks after participants lose access to the TLC app (i.e., 16-week intervention exposure).
The TLC app was co-created with input from a community advisory board comprising caregivers, service providers, and community health workers and cultural leaders (Utz, Terrill, & Thompson, 2023). As detailed in prior publications, the app was found to be both feasible and usable as an internet-delivered intervention for older adults (Thompson et al., 2025) and potentially effective in improving caregivers’ perceived levels of anxiety and satisfaction with their respite time-use (Iacob et al., 2024). Further details can be found through Clinical Trials.gov (NCT-03689179) and NIH reporter (R01-AG061946). De-identified data from the TLC study are archived and publicly available through the Hive Data Repository at the University of Utah (doi:10.7278/S50d-2rgg-4549). And, a version of the TLC intervention is now freely available for public use (www.tlc-respite.com).
Measures
While TLC was designed to improve a variety of psychosocial measures, the key outcome in this brief report is the Positive Aspects of Caregiving (PAC) scale (Tarlow et al., 2004). The nine-item scale asks respondents to what extent caregiving has made them feel useful, needed, appreciated, and more. To test for heterogenous treatment effects of the intervention, we examine four caregiver characteristics: age in years, race (0 = nonwhite, 1 = white), gender (0 = Male, 1 = Female), household income (0 = < $50,000; 1 = $50,000+), and education (0 = no bachelor’s degree, 1 = bachelor’s degree or higher). Many of these measures have been dichotomized to maximize statistical power. We also examine two conditions of the caregiving situation: the Memory and Behavior Problem Checklist (MBPC), a measure of impairment assessed by the caregiver at baseline (Zarit & Zarit, 1982), and the percent of total care provided by the respondent as primary caregiver (0 = less than 80%, 1 = 80% or more). Finally, because half of the caregivers received the complete TLC app at baseline, while others waited to “unlock” certain features at week 8, we include an indicator for the study design group (0 = Immediate, 1 = Delayed); this is not an essential feature of the brief report, nor was it a significant moderator of PAC, yet we include it to adjust for any potential effects associated with the randomized study design (see Iacob et al., 2024; Utz, Caserta, et al., 2023 for further information).
Analytic Strategy
Analyses were conducted using Stata 18. Prior to hypothesis testing, empty and unconditional growth of PAC were assessed using multilevel modeling. We tested both linear and curvilinear growth parameters to determine the best fit for the longitudinal data, and we included a random intercept and random slope to allow for differences in baseline PAC and PAC growth, respectively. For the primary analysis, interactions were included as fixed effects to identify possible differences in initial PAC values or changes over time across subgroups. In cases where trajectories differed across moderators, post hoc analysis assessed between-group differences using simple slope analysis and visual representation of the interaction effect. Robust standard errors helped to mitigate potential heteroscedasticity over time (Huang et al., 2023).
We used Little’s (1988) missing completely at random (MCAR) test to examine patterns of missingness in our sample. After controlling for study design group (see above), data were missing at random (MAR; χ2 (90) = 80.73, p = .74). Therefore, we proceeded with listwise deletion (N = 24 dropped) but included the group indicator to correct for potential nonresponse bias. The analytic sample comprised 143 respondents.
Results
Descriptive Statistics and Unconditional Growth in PAC
Descriptive Statistics and Bivariate Correlations at Baseline (N = 143).
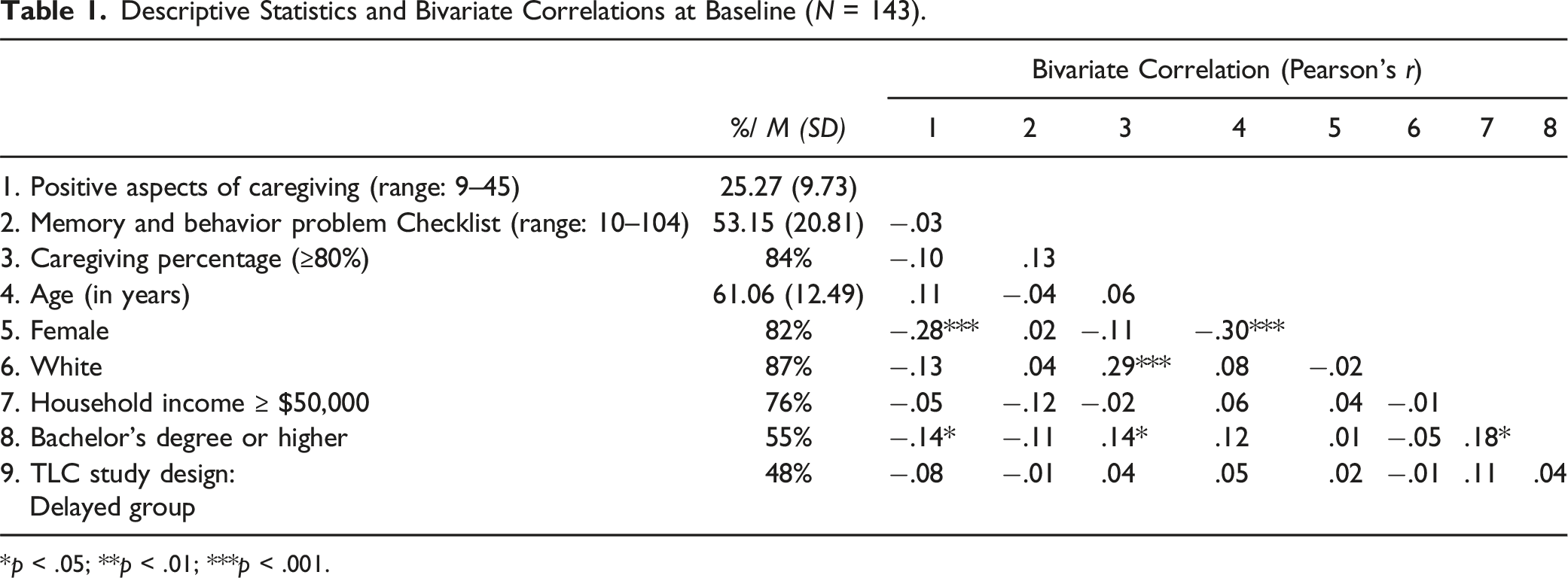
*p < .05; **p < .01; ***p < .001.
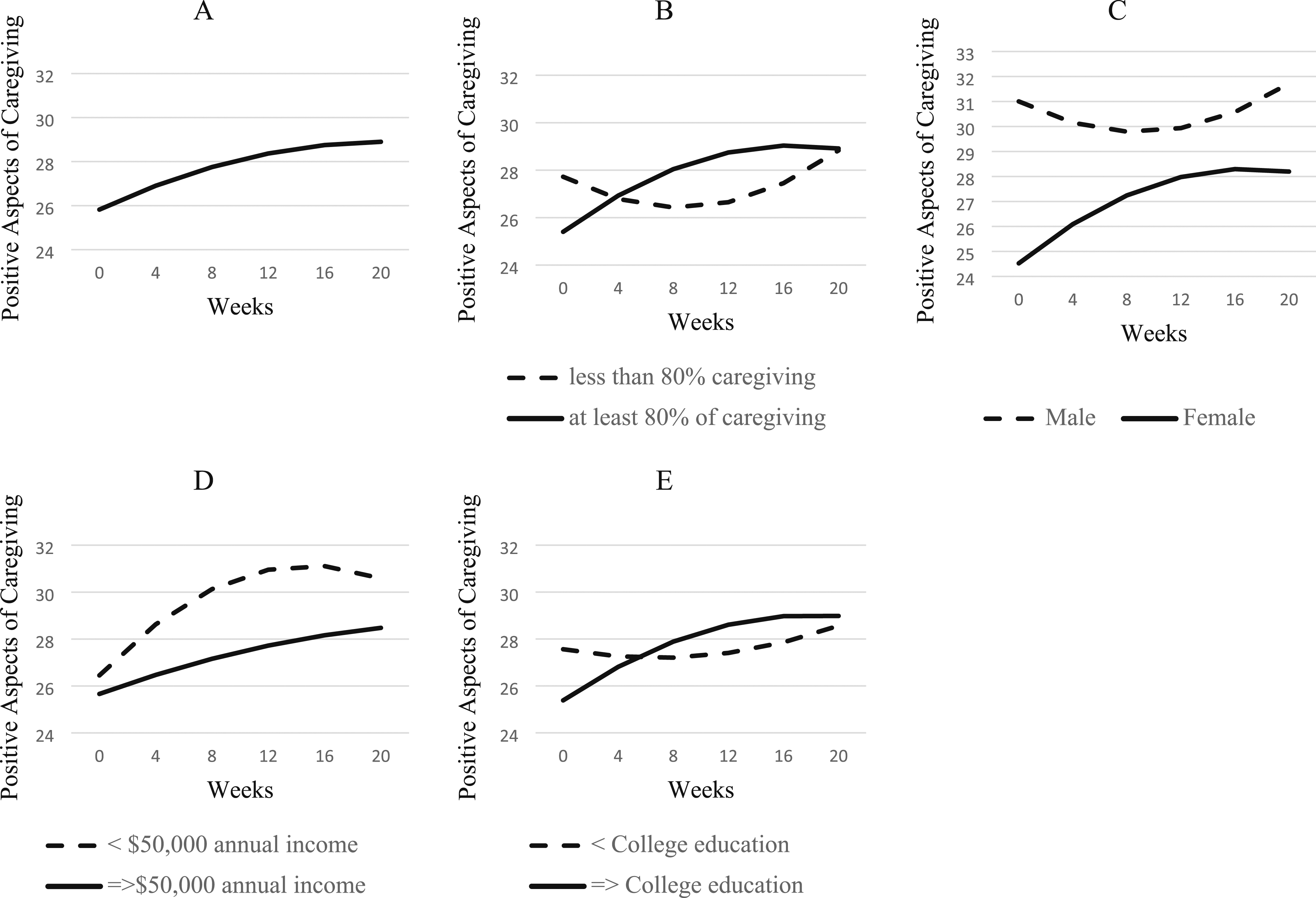
Unconditional growth model and simple slopes of moderators. Panel A shows overall growth, Panel B shows moderation by percentage of caregiving provided by the respondent, Panel C shows moderation by respondent gender, Panel D shows moderation by household income, and Panel E shows moderation by respondent educational attainment.
Moderators of PAC Growth
Multilevel Growth Model Estimating Individual Differences in Initial PAC and Trajectories in PAC (N = 143).
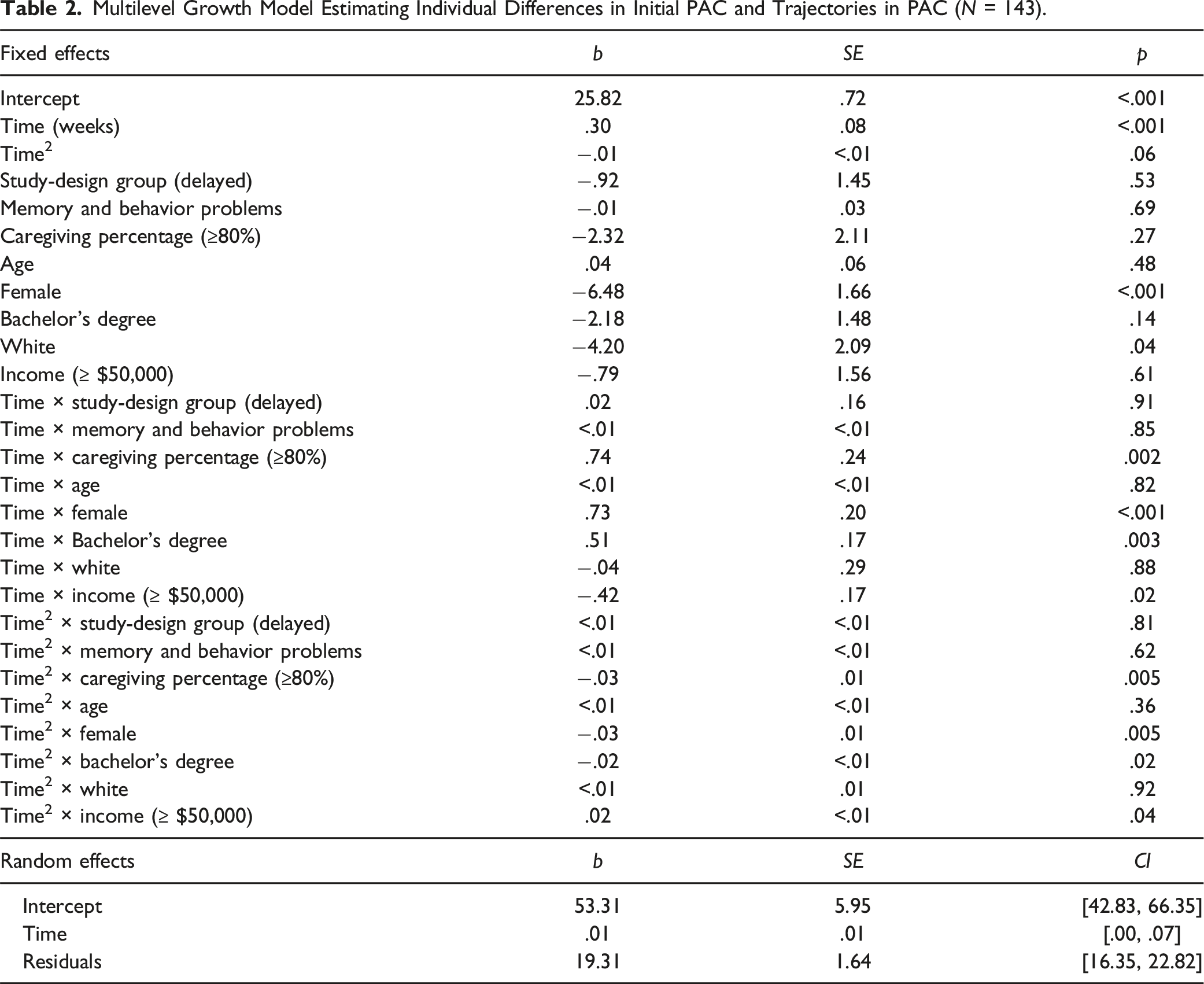
Figure 1(b) demonstrates that caregivers who provided at least 80% of the care to their family member experienced significant increases in PAC each week (b = .45, p < .001), whereas caregivers who provided less than 80% didn’t experience significant changes (b = −.30, p = .16). Women reported significantly lower PAC at baseline than men, but as Figure 1(c) shows, women experienced significant increases in PAC over time (b = .46, p < .001) while men did not (b = −0.27, p = .12). Figure 1(d) demonstrates that caregivers with a household income less than $50,000 annually experienced stronger PAC gains each week (b = .65, p < .001) compared to those who made at least $50,000 (b = .23, p < .05). Figure 1(e) indicates that participants with a college degree experienced improvements in PAC each week (b = .55, p < .001) while participants without a college degree did not (b = .04, p = .77). While there were no racial differences in growth trajectories, caregivers identifying as white reported significantly lower PAC at the initial assessment (b = −4.20, p < .05). Finally, there were no differences in initial PAC or PAC trajectories based on caregivers’ age or care recipients’ memory and behavior problems.
Discussion
We sought to examine whether trajectories in the positive aspects of caregiving (PAC) were moderated by caregiver characteristics or by conditions of the caregiving situation. Significant growth in PAC was observed among women (but not men), caregivers with a bachelor’s degree (but not those without), and individuals performing at least 80% of the caregiving (but not those performing less). Caregivers with a household income below $50,000 reported a greater increase in PAC than those at or above $50,000, but both groups showed some benefit in response to the intervention. Neither caregiver age or race, nor the severity of the care recipients’ dementia symptoms, modified the intervention’s effect on PAC.
Why did female, lower-income, and college-educated caregivers report greater increases in PAC after using the TLC app? These patterns may have conflicting explanations, but likely center on these groups’ positionality within the American social hierarchy. On the one hand, disadvantaged caregivers may benefit the most from an intervention such as TLC because they have the greatest need or the most to gain: For example, women may find greater need for respite because they have been socialized to provide the lion’s share of caregiving and to do so without support or complaint (Calarco, 2024). Similarly, lower-income households likely face greater time pressure (Roxburgh, 2004) and might find disproportionate benefit from increasing and improving their use of respite. On the other hand, more privileged caregivers, such as those with higher education, may benefit most from an intervention because they have the psychological skills or prior experience to take greatest advantage of it (Mirowsky & Ross, 2003). Prior research and theory have suggested that the introduction of new interventions or technologies is associated with greater health improvements in socially advantaged groups (Clouston & Link, 2021; Pleasant et al., 2020). In this case, caregivers with a college education may find a self-administered, app-delivered intervention less daunting. Alternatively, higher education may impose its own time pressures on caregivers due to greater work–life imbalances; this is especially true in women, for whom (as we have seen in this study) a respite intervention may be especially salutary (Roxburgh, 2002; Schieman et al., 2006).
While primary caregivers (i.e., participants who provided at least 80% of caregiving) benefited more from the intervention—consistent with our prior observations about time pressure—caregivers with more impaired care recipients (greater memory and behavior problems) did not disproportionately benefit from the intervention. While this is somewhat surprising, our findings are supported by previous work: Robison et al. (2009), for example, observed that “care receiver memory problems” were not associated with caregiver health or well-being, adjusting for income and other factors. More puzzling is the null finding for age: because younger Americans often balance caregiving with full-time employment, we might expect them to benefit more from a respite-based intervention (Pearlin & Aneshensel, 1994; Whitmore et al., 2023). It is worth noting that in our preliminary analyses—which modeled linear but not quadratic time—younger caregivers indeed showed greater PAC growth than older caregivers, though the effect was modest.
On the whole, these findings suggest that disadvantaged groups (women, lower-income caregivers, and those with a greater share of caregiving duties) may benefit most from an intervention designed to improve their respite time. Yet, disproportionate benefits also accrue to caregivers with a college degree. Though this may appear contradictory, it is consistent with the broader literature: Both the capacity to take advantage of respite and to find meaning in caregiving are likely molded by the “social and economic conditions” through which resources are unequally conferred (Meyer et al., 2022; Pearlin & Bierman, 2013).
Because the TLC intervention is fully self-administered and technology-delivered, these findings may also be identifying the types of caregivers for whom a technology-delivered intervention may be most feasible or effective. Previous research using the TLC sample (mean age = 61) found that although computer proficiency varied by age and affected how one engaged with the app itself (as expected), neither proficiency nor age determined the benefits of the intervention (Thompson et al., 2025). Taken together, these results suggest that older adults are receptive to using and can benefit from technology-delivered support interventions. Such approaches are increasingly seen as a viable alternative to traditional (e.g., in-person) interventions (Petrovic & Gaggioli, 2020).
Improving the positive aspects of caregiving is essential to the well-being of caregivers, and may have important implications for care recipients, as well. It may not always be feasible to ease the burdens that caregivers face, but interventions can still focus on “increasing perceived benefit when reducing burden is not possible” (Pristavec & Luth, 2020, p. 2204). By understanding the conditions under which positive aspects of caregiving can be strengthened, and the subgroups that most benefit from technologies designed for this purpose, we can more effectively target the delivery of our interventions to maximize the well-being of caregivers and those in their care.
Footnotes
Acknowledgments
Our study team acknowledges the support of our dedicated Community Advisory Board members who guided the redevelopment of the original TLC intervention into an app and who assisted us with recruitment and dissemination efforts. We also acknowledge the initial work and mentorship of Drs. Dale Lund and Michael Caserta, who were key in conceptualizing the TLC intervention model overall.
Author Contributions
M. E. Coleman planned the study, supervised the data analysis, and co-wrote the paper. D. A. Godfrey performed statistical analyses and wrote the analytic strategy and results. A. Thompson helped to revise the manuscript. C. Sparks contributed to data collection. R. L. Utz served as P. I. for the project and helped to plan the study and revise the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NIA R01-AG061946.