
Abstract
The concept of person-centeredness (PC) is ubiquitous in health and supportive care regardless of recipients’ age and condition, which might suggest that the concept is clear, uniformly understood, and its provision straightforward; however, such is not the case. To more fully understand the concept and challenges inherent in applying PC overall and in the care of older adults, including persons with dementia and receiving long-term care, this special article draws on meetings held with 116 participants representing diverse perspectives and expertise. Six deeply rooted tensions were identified: community (public) versus individual (private); efficiency versus individualization; superficial knowing versus deep knowing; policy compliance versus flexible decision making; safety versus freedom; and expense versus investment. Given these pervasive tensions, full PC can never be achieved, and requires ongoing negotiation. Therefore, the concept of PC must be reconstructed, adopting a more nuanced and realistic approach to practice, policy, and research.
Keywords
• Identification of tensions inherent in person-centeredness (PC) • Potential strategies to negotiate PC • A realistic appraisal of the limitations of PC
• Encouragement to not espouse PC as a monolithic concept • Use of strategies to promote PC • Development of measurement tools and examining their ability to promote PCWhat this paper adds
Applications of study findings
The concept of person-centeredness (PC) has become ubiquitous in the provision of health and supportive care regardless of recipients’ age and condition. International organizations promote PC, including the United Nations General Assembly that declared 2021–2030 the Decade of Healthy Ageing, grounded in person-centered care as a pillar of the initiative (World Health Organization, 2022). In the U.S., the Institute of Medicine identifies PC as a goal for the 21st century (Institute of Medicine [US] Committee on Quality of Health Care in America, 2001) and the Centers for Medicare & Medicaid Services consider it key in government-funded services (CMS, 2023). Societies such as the American Geriatrics Society recognize PC as critical to quality care for older adults (The American Geriatrics Society Expert Panel on Person-Centered Care, 2016), and the Alzheimer’s Association grounds its Dementia Care Practice Recommendations in PC (Fazio et al., 2018). In addition, countless institutes and centers are dedicated to person-centered care (e.g., Institute for Patient and Family-Centered Care, n.d.; National Center on Advancing Person-Centered Practices and Systems, n.d.), and organizations regularly highlight it in their marketing materials (e.g., Brookdale Senior Living, n.d.).
The universal call for PC might suggest that the concept is clear, uniformly understood, and its provision straightforward, but such is far from the case. For one, disciplinary foci regarding PC differ: nursing stresses recognizing the person rather than the disease; psychology focuses on the relationship with the care provider; medicine underscores the importance of the person’s perspective as opposed to the provider’s perspective; and dementia care highlights the critical role of communication (Kitwood, 1998; Nolte et al., 2020). To be sure, common threads among definitions do exist—recognizing the person as an individual and the individual’s perspectives, and honoring the individual’s control and self-direction—but the bulk of the literature indicates that the concept is fuzzy, elusive, and poorly conceptualized (Scholl et al., 2014), resulting in potential confusion related to its operationalization (Byrne et al., 2020). Acknowledging these variations, a convincing case has been made that different definitions of PC may in fact be justified and necessary based on the care context, the care recipient, and ethical perspectives (Mitchell et al., 2022), which is supported by contradictions in PC when considering the needs of patient versus the needs of employees, standardization versus customization of care, and other areas (Meranius et al., 2020; Saunders et al., 2021; Vogus et al., 2020).
To more fully understand the concept and challenges inherent in PC overall and in relation to care for older adults including persons with dementia and receiving long-term care, this special article draws on recorded group meetings (60–120 min) held with 116 participants representing diverse perspectives and expertise. Eight were virtual meetings including 37 experts representing (non-mutually exclusive categories of) long-term care (n = 21), advocacy/policy (n = 14), healthcare (n = 11), academia/research (n = 13), direct care (n = 7), technology (n = 7), and law (n = 2). Experts were identified for inclusion based on a literature review of the topic areas, those known based on their national reputation, and those affiliated with key organizations central to the topic. An additional virtual meeting was held with members of the Alzheimer’s Association Early-Stage Advisory group (n = 10). In addition, three in-person meetings were held with the Alzheimer’s Association Dementia Care Provider Roundtable (n = 41), members attending the Center for Innovation Conference (n = 16), and care providers in an assisted living community (n = 12).
To elicit discussion across a range of topics, each meeting largely focused on one of four areas, with multiple topics areas often being discussed in any one meeting due to their interconnected nature. Topic areas addressed the concept of PC, the systemic perspective of PC, PC in relation to care and the workforce, and PC and technology. The topics were chosen by an expert research steering committee of the Leveraging an Interdisciplinary Consortium to Improve Care and Outcomes for Persons Living with Alzheimer’s and Dementia (LINC-AD) network to represent key and diverse issues related to PC in practice and policy. Sample questions for each topic are provided below; they helped launch but did not restrict the conversation. • The concept of PC: How are individual rights and societal good balanced? What elements of PC do and don’t transcend cultures? • The systemic perspective of PC: To what extent can PC exist in a market economy? How broadly does responsibility for PC extend? • PC in relation to care and the workforce: Are there limits to PC when there are cultural differences? What kind of care is most challenging to deliver in a person-centered way? • PC and technology: Can technology ever be completely person-centered? At what point does technology interfere with human rights?
Through an exploratory thematic analysis of session recordings, this special article presents six tensions identified by participants as inherent in PC, and related negotiation strategies. Based on the tensions, this paper reconstructs PC as a dynamic process, and calls for more nuanced use of the term itself. It posits that full PC can never be achieved and requires ongoing negotiation, as illustrated in the material to follow.
Tensions Inherent in Person-Centeredness and How to Negotiate Them
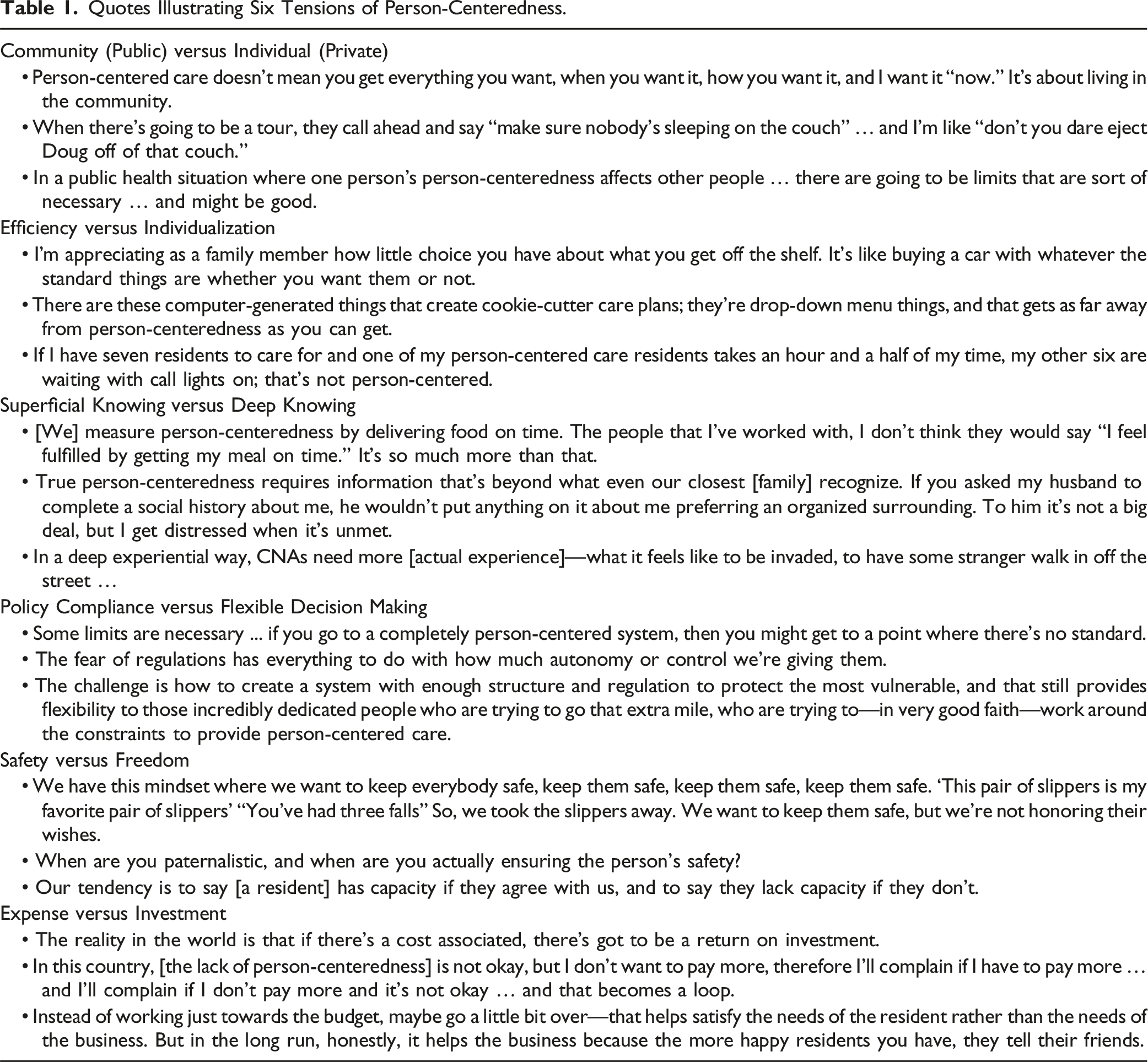
Figure 1 displays the six tensions identified as inherent in PC by the group members: community (public) versus individual (private); efficiency versus individualization; superficial knowing versus deep knowing; policy compliance versus flexible decision making; safety versus freedom; and expense versus investment. The figure displays each tension on a graphic akin to a dial, suggesting dynamic movement that can fluctuate between one or the other anchor of the tension based on purposeful action. Each tension is discussed below, incorporating literature that provides grounding and fleshes out strategies for negotiation. As will be evident, many examples relate to residential long-term care, largely reflecting the expertise of many of the meeting members—but the tensions by no means relate only to older adults, persons with dementia, or those who receive long-term care. Table 1 provides illustrative examples for each tension incorporated into the text that follows; additional examples can be found in Appendix A. Six tensions of person-centeredness. Quotes Illustrating Six Tensions of Person-Centeredness.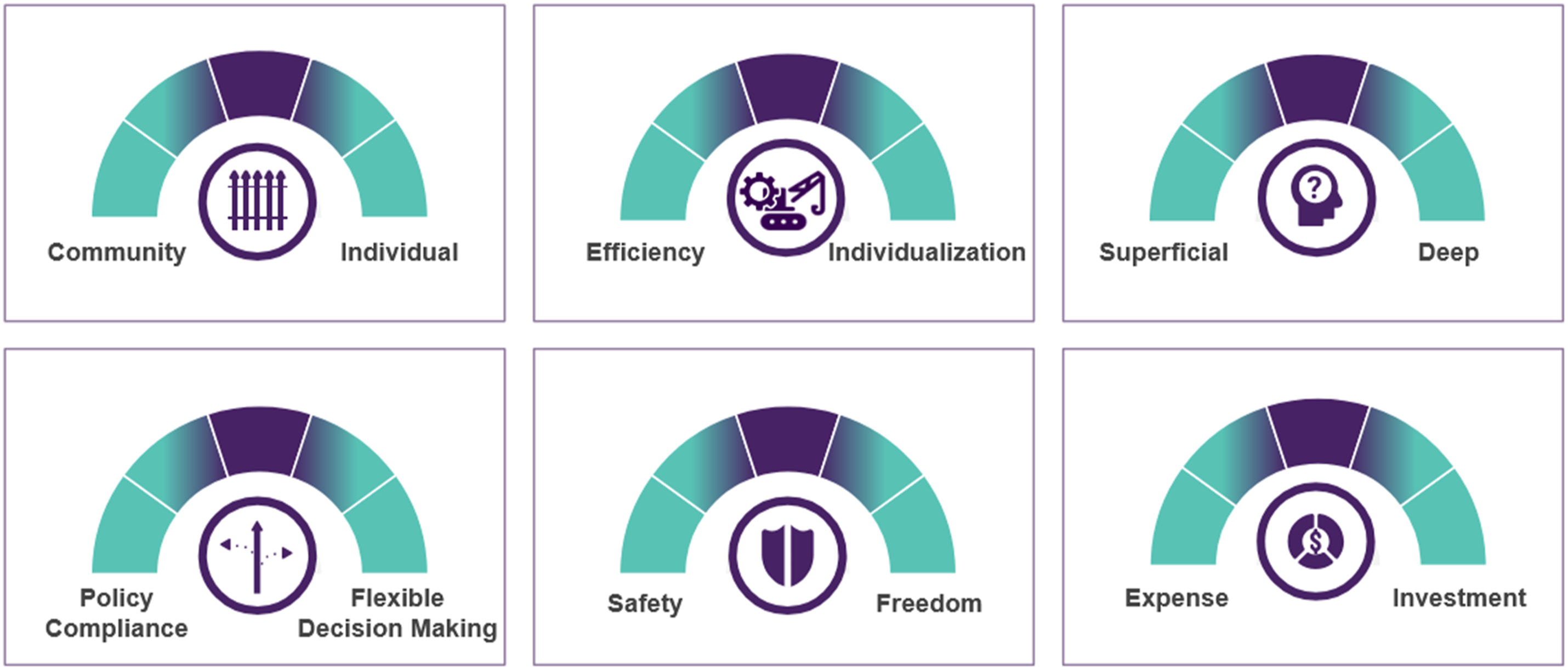
Community (Public) versus Individual (Private)
One of the most basic constructs regarding PC is that because man is a social animal, individuals must learn and live within the norms of society (Barkan, 2011), which set parameters for PC. One group member stated, “Person centered care doesn’t mean you get everything you want, when you want it, how you want it, and I want it ‘now’. It’s about living in the community.” At the same time, the balance between individual rights and group membership may be unclear, as illustrated in an anecdote shared by an assisted living staff member regarding a resident being banned from the public living room: “When there’s going to be a tour, they call ahead and say ‘make sure nobody’s sleeping on the couch’… and I’m like ‘don’t you dare eject Doug off of that couch’.” Supporting that perspective, others have noted that organizational policies themselves may run counter to individual preferences (Abbott et al., 2016), with the couch scenario being an apt example of the need to attend to occupancy even if it inhibits PC. A third quote similarly reflected the tension between community (public) versus individual (private), referencing actions during the COVID-19 pandemic that largely protected the public (Iaboni et al., 2020) at the expense of lockdowns and social distancing that disadvantaged individuals by causing isolation, anxiety, and depression (Rodrigues et al., 2021). “In a public health situation where one person’s person-centeredness affects other people … there are going to be limits that are sort of necessary … and might be good.” Negotiation: The tension between the community versus the individual is evident from the moment of birth, as children experience competing demands, boundary issues, and conflicts within their family (Broderick, 1993) and learn that focus on the individual has bounds. More so, the family system itself must be sound—and in the case above, so too must the long-term care organization striving to maintain occupancy and remain fiscally solvent. Negotiating the tension of community versus individual requires the two-fold process of recognizing conflict as a need to examine competing priorities, and promoting shared decision making when priorities conflict. Shared decision making is appropriate when multiple reasonable options as to a course of action exist, but is admittedly challenging when individual impact and community benefit are in conflict (van der Horst et al., 2023). Figure 2 illustrates how through negotiation, PC favoring “community” might move closer to the “individual” anchor, a concept that is applicable to all six tensions. Graphic depicting moving the dial of person-centeredness when negotiating tensions. Note: The graphic illustrates the tension of “community versus individual,” but is applicable to all tensions.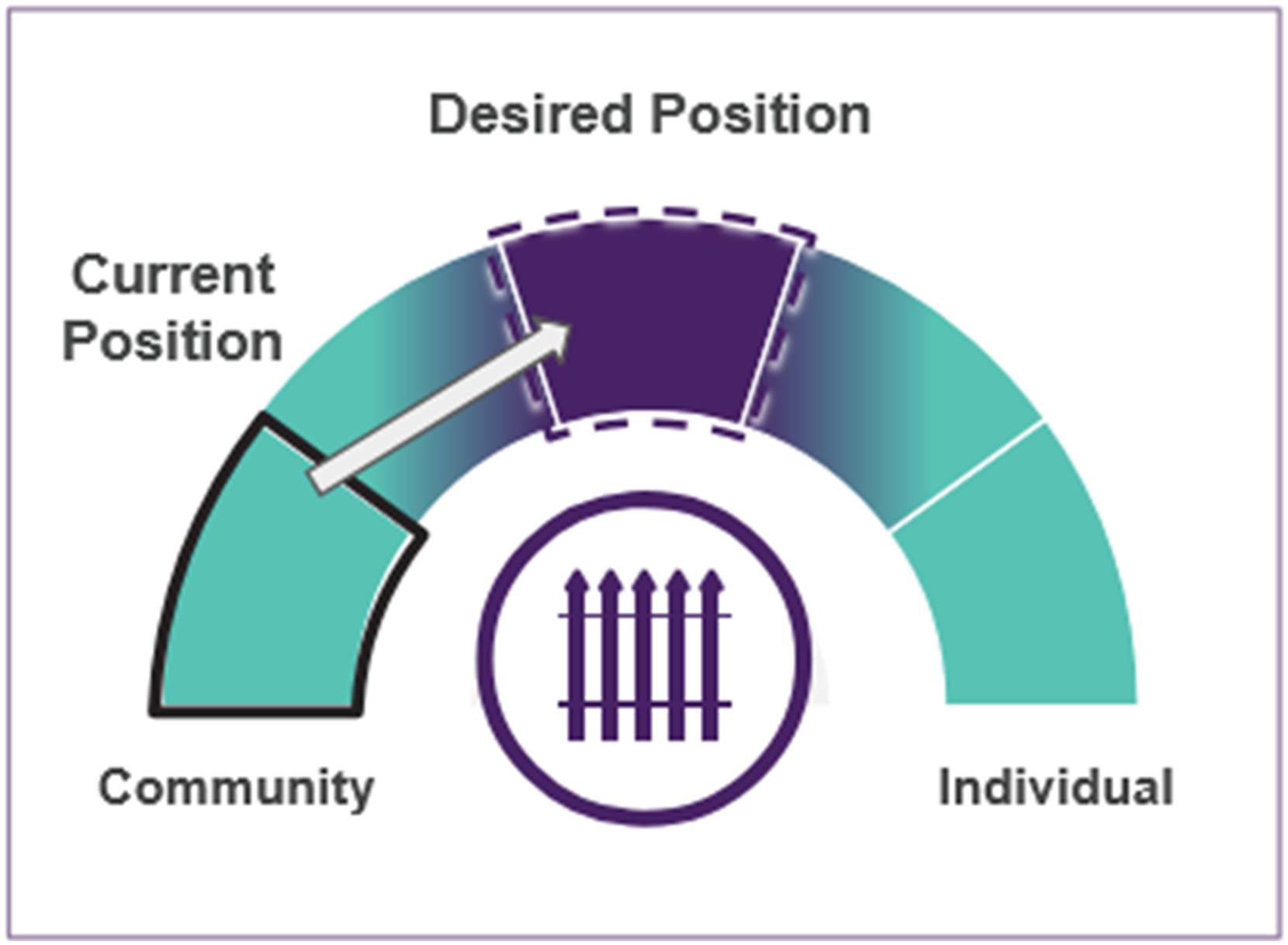
Efficiency versus Individualization
Standardization promotes efficiency and reduces errors (Vogus et al., 2020) but is antithetical to PC. A family member participant noted “I’m appreciating as a family member how little choice you have about what you get off the shelf. It’s like buying a car with whatever the standard things are whether you want them or not.” Technology-driven healthcare innovations have further promoted efficiency through standardization, as “There are these computer-generated things that create cookie-cutter care plans; they’re drop-down menu things, and that gets as far away from person-centeredness as you can get.” Further limiting individualization, person-centered practices come at a cost due to the time needed to train staff and the time required to provide them (Kales et al., 2019), and may have an adverse effect for the group: “If I have seven residents to care for and one of my person-centered care residents takes an hour and a half of my time, my other six are waiting with call lights on; that’s not person-centered.” This example displays not only the tension of efficiency versus individualization, but also its intersection with the tension of community versus individual. Negotiation: Efficiency refers to producing desired results with little or no waste of time or materials. In healthcare and other systems, the reality is that there is need to reduce cost and waste, while at the same time focusing on quality (Fraser et al., 2008). Efficiency is also pragmatic, and recognizes that not all settings can adopt all practices (Zimmerman et al., 2022)—including the technology in the quote above, which requires resources and technical capacity. Despite the parameters introduced by efficiency, it may in and of itself solve problems, such as by providing new and overworked staff (Pace et al., 2024) a menu of care options reflecting presumed best practices. Negotiating efficiency versus individualization calls for a purposeful evaluation of inputs and outputs (Culyer, 2018), which is helpful in the context of shared decision making.
Superficial Knowing versus Deep Knowing
Perhaps one of the most uninformed assumptions related to PC is that what is known about a person is what matters to them, yet many PC recommendations go no further than “knowing the person” (Osuoha et al., 2021). Participants recognized that such knowing may be too simplistic: “[We] measure person-centeredness by delivering food on time. The people that I’ve worked with, I don’t think they would say ‘I feel fulfilled by getting my meal on time’. It’s so much more than that.” Instead, consider that “True person-centeredness requires information that’s beyond what even our closest [family] recognize. If you asked my husband to complete a social history about me, he wouldn’t put anything on it about me preferring an organized surrounding. To him it’s not a big deal, but I get distressed when it’s unmet.” However, truly knowing someone requires a “critical mass” of shared experiences (Talbert, 2015), which is often challenging given racial and cultural differences between the individuals providing and receiving care (Wallace & Roth, 2024). “In a deep experiential way, CNAs [certified nursing assistants] need more [actual experience regarding]—what it feels like to be invaded, to have some stranger walk in off the street.” Negotiation: Almost 70 practices have been identified to promote culturally competent healthcare, ranging from using culturally and linguistically appropriate screening instruments to modifying the environment and methods of outreach to families and others (Handtke et al., 2019). Tools also exist to elicit choice in specific situations, such as related to goals of care in advanced dementia (Hanson et al., 2017) and to learn about an individual (e.g., the About Me Tool [University of North Carolina at Chapel Hill, n.d.]). Typically, asking “what matters to you” is done in relation to healthcare (Institute for Healthcare Improvement, 2022), but this negotiation strategy is recommended throughout the lifespan and in a broad context. Still, if due only to pragmatism, all tools solicit a limited range of preferences, so it is recommended that earlier in life individuals document what creates true meaning and share it with others.
Policy Compliance versus Flexible Decision Making
The need for policy compliance is especially evident in organizations that must adhere to external standards, ranging from the aviation industry that must assure traveler safety; to educational systems that must assure competency-based learning standards; to nursing homes that must assure a minimum level of care. One participant stated, “Some limits are necessary ... if you go to a completely person-centered system, then you might get to a point where there’s no standard.” At the same time, standards may impede PC: “The fear of regulations has everything to do with how much autonomy or control we’re giving them.” Thus, in a highly regulated setting such as long-term care, it is not surprising that staff have pointed to policies as barriers to impeding PC (Abbott et al., 2016; Engle et al., 2017). One participant suggested “The challenge is how to create a system with enough structure and regulation to protect the most vulnerable, and that still provides flexibility to those incredibly dedicated people who are trying to go that extra mile, who are trying to—in very good faith—work around the constraints to provide person-centered care.” However, implementing such an approach requires that the workforce be sufficient and competent to “work around” regulations. Negotiation: While policies do set parameters for care, there are instances wherein deeper probing finds sanctioned “work arounds”—such as altering policy-based medication approval and administration procedures to ensure meeting individuals’ immediate needs (Azad & King, 2008). In cases where policies seem to override personal practices, it may be advisable to solicit guidance from relevant organizational or regulatory authorities as to acceptable alternative care practices. More so, and recognizing that policies themselves are developed in response to need, numerous organizations are active in promoting related flexibility and change, including but not limited to the American Geriatrics Society (AGS, n.d.), the Post-Acute and Long-Term Care Medical Association (PALTmed, n.d.), the Alzheimer’s Association (Alzheimer’s Association, n.d.), and the National Association for Social Workers (NASW, n.d.); becoming active in these organizations may promote more PC policies.
Safety versus Freedom
Broadly speaking, policies exist to avoid negative outcomes—perhaps none more important than risks to safety. However, safety may come at the expense of freedom, a tension clearly identified by participants. “We have this mindset where we want to keep everybody safe, keep them safe, keep them safe, keep them safe. ‘This pair of slippers is my favorite pair of slippers’ ‘You’ve had three falls’. So, we took the slippers away. We want to keep them safe, but we’re not honoring their wishes.” A focus on falls is not surprising, given that more than 14 million older adults fall every year, constituting the leading cause of injury and death (Centers for Disease Control and Prevention, 2024). At the same time, the balance between safety and freedom, regardless the topic, is subjective—“When are you paternalistic, and when are you actually ensuring the person’s safety?”—and also, perhaps self-serving: “Our tendency is to say [a resident] has capacity if they agree with us, and to say they lack capacity if they don’t.” That subjectivity may be most important to address in negotiating the tension between safety versus freedom. Negotiation: Assuming individual preferences have been elicited, discussion can address how they differ from the preferred practices of the organization, after which shared decision making can ensue. However, such may be easier said than done, given different weightings of risk by those involved in shared decision making (Clarke et al., 2009). Negotiated risk agreements address this tension, and document recognition of risk based on preferred activities and acceptance of the related risk (Jenkens et al., 2006). However, use of these agreements is not straightforward, such as if an individual is cognitively impaired or the service provider is concerned about legal liability regardless of the agreement (Mitty & Flores, 2008). As another strategy, attention might be given to the adoption of a “culture of safety” which respects individual choice, promotes collaboration, embodies a blame-free environment, and displays organizational commitment (Agency for Healthcare Research and Quality, 2019). For individuals with impaired capacity, supported decision making—where a trusted family, friend, or other care partner collaborates to help the individual make informed choices involving pre-identified decision-making domains (Peterson et al., 2021)—offers a useful framework, helping to ensure that decisions regarding safety and freedom remain aligned with the person’s subjective values and preferences.
Expense versus Investment
There is no avoiding that PC requires resources for programming, training, assessment, care planning, and care provision (Tay et al., 2018). In a market economy where supply and demand drive production of goods and services, the business case is such that “The reality in the world is that if there’s a cost associated, there’s got to be a return on investment.” At the same time, consumers are driven by expectations and their own pocketbook (Kuşçu & Yozgat, 2019). “In this country, [the lack of person-centeredness] is not okay, but I don’t want to pay more, therefore I’ll complain if I have to pay more … and I’ll complain if I don’t pay more and it’s not okay … and that becomes a loop.” One participant suggested employing a risk-taking approach, which may not be feasible for many providers in the short run: “Instead of working just towards the budget, maybe go a little bit over—that helps satisfy the needs of the resident rather than the needs of the business. But in the long run, honestly, it helps the business because the more happy residents you have, they tell their friends.” Negotiation: A key example of return on investment is illustrated in the examination of the Green House Model of nursing home care, a PC model based on core values of real home, meaningful live, and empowered staff (Cohen et al., 2016). Compared to other types of nursing home care, residents in these nursing homes had fewer health care events, including hospital readmissions, which translated to decreases in Medicare spending (Zimmerman et al., 2016). Other support about cost savings also exist, such as from person-centered homes for patients with heart failure (Ekman et al., 2012; Sahlen et al., 2015). Admittedly though, not all person-centered approaches will have a monetary return on investment (Uittenbroek et al., 2018), meaning that the need to examine costs is important.
Conclusions and Implications for Practice, Policy, and Research
The concept of PC must be reconstructed, adopting a more nuanced and realistic approach to its incorporation in practice, policy, and research. Findings from group meetings of 116 participants representing diverse perspectives and expertise identified six deeply rooted tensions inherent in PC: community (public) versus individual (private); efficiency versus individualization; superficial knowing versus deep knowing; policy compliance versus flexible decision making; safety versus freedom; and expense versus investment. Because the tensions are pervasive, full PC cannot be achieved and requires ongoing negotiation. Negotiation strategies include but are not limited to shared decision making; evaluation of inputs and outputs; reflection of “what matters” early in life and beyond; a focus on health care; advocacy; negotiated risk; and assessment of return on investment.
The tensions exist across systems, and negotiation is rarely simple or straightforward—illustrated, for example, by “community versus individual” tensions in perspectives on issues ranging from gun ownership to vaccination requirements. In addition, tensions intersect, which further complicates negotiation, such as being required to wear seat belts (policy compliance vs. flexible decision making) that restrict autonomy (safety vs. freedom). Still, the presence of tensions and the challenge of negotiation are not meant to suggest that the concept of PC should be abandoned. Quite the contrary: PC deserves much more serious attention than has been accorded in words rather than action.
In situations where identified tensions restrict PC, the dial in Figure 2 could potentially be moved through assessment, determination and use of new care practices, goal setting, and measurement, allowing quantification of a current and desired state of PC. Goal-attainment scaling can inform this effort, given its focus on individualized outcome measurement and application across disciplines (Cheema et al., 2024); as such, it provides a sound launch pad to inform methodology and scoring for the development of person-centered attainment scaling (PC-AS). PC-AS could then be used to guide and evaluate new care practices and outcomes, and truly move the needle toward PC. For example, consider the situation of Mr. M, who has been a resident of an assisted living community for ten years. He has moderate Alzheimer’s disease and becomes agitated when staff enter his room to brush his teeth—a task that was added to Mr. M’s care plan by a software program that generates a checklist of care tasks based on diagnoses. The assisted living administrators track task completion and incorporate this information into staff annual performance reviews. The primary care partner is concerned that she may not receive her raise if she cannot complete tasks efficiently and so has grown frustrated; she has expressed her dissatisfaction to her supervisor, stating that she spends too much time with Mr. M and feels like “giving up” on him. Figure 3 identifies the tensions in this scenario, provides examples of relevant PC practices to address the tensions (e.g., person-centered employment practices [Zimmerman, 2024] or person-centered mouth care practices [Zimmerman et al., 2020]), and displays a simplified model using PC-AS principles to evaluate the effectiveness of the new care practices to increase PC. Case study illustrating navigating tensions of person-centeredness: Person-centered attainment scaling (PC-AS).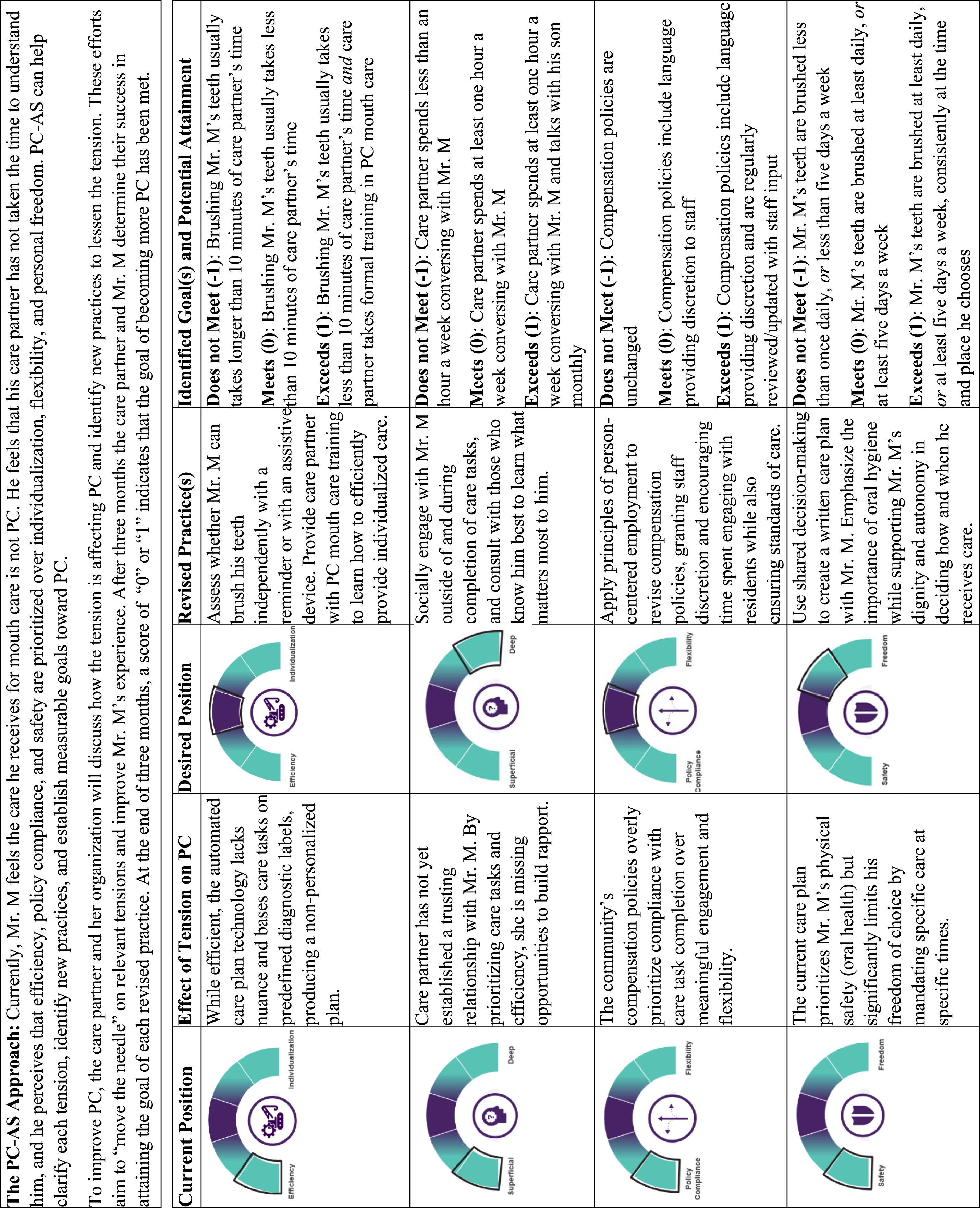
The six tensions related to PC are thus not only informative in understanding limits to PC, but also in identifying and promoting new practices to further PC. That said, it is not suggested that new practices will eradicate the tensions, because the tensions reflect the complexities of life. Instead, understanding the tensions and their dynamic nature may promote shared understanding and better balance the continuum of PC.
Supplemental Material
Supplemental Material - Legal Reforms and Outcomes of the Action of Police Institutions in Combating Violence Against Women: A Systematic Review Protocol
Supplemental Material for Legal Reforms and Outcomes of the Action of Police Institutions in Combating Violence Against Women: A Systematic Review Protocol by Sheryl Zimmerman, Walter Moczygemba, Philip D. Sloane, Sam Fazio in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors thank the meeting participants, including Maria Aranda, PhD, D. Pearl Barnett, MPA, Alice Bonner PhD, RN, Barbara Bowers, PhD, RN, Rebecca Bratsch, MSW, Eric Carlson, JD, Peter Chamberlain, SM, Tony Chicotel, JD, MPP, Laci Cornelison, MS, David Farrell, MSW, LNHA, Colleen Galambos, PhD, Christian Goodwin, MPH, David Grabowski, PhD, Kari Gray, Holly Harmon, RN, MBA, LNHA, Chris Herman, MSW, LCSW, Mauro Hernandez, PhD, Juliet Holt Klinger, MA, Harriet Komisar, PhD, Tamara Konetzka PhD, Bill Lamb, MSW, MPA, David Lindeman, PhD, Jeff McSpadden, Laura Mosqueda, MD, Arif Nazir, MD, Sherry Perry, Lauren Pongan, MA, Lori Porter, Marilyn Rantz, PhD, RN, Ronen Rozenblum, PhD, MPH, Susan Ryan, MA, Robyn Stone, DrPH, Kim Strom, PhD, William Thomas, MD, Kenesha Wood, MSW, LRT/CTRS, Jack York, Gina Zimmermann, MPS, members of the Dementia Care Provider Roundtable, participants of the Center for Innovation 2023 annual conference, and staff of Brightview Senior Living. Additional thanks are given to Maria Gutierrez, MBA, and Esha Solanki, BA for their contributions.
Author Contributions
Sheryl Zimmerman, PhD—lead author, concept, methodology, final revision and review of article.
Walter Moczygemba, MSW—initial draft of article, data interpretation, review of article.
Philip D. Sloane, MD, MPH—concept, methodology, review of article.
Sam Fazio, PhD—concept, review of article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Aging, grant R24AG065185.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.