
Abstract
Everyday technologies, like smartphones, might improve care of persons living with Alzheimer’s disease and related dementias (PLWADRD) and reduce burden among care partners. However, care partners often report inadequate technical skills for using technology-based strategies. To address this need, we developed a manualized behavioral intervention called Technology Assistance in Dementia (Tech-AiD). We gathered feedback on the intervention concept from invested partners (10 care partners and 10 healthcare professionals) in a multimethod study. Quantitative results suggested very high intervention acceptability (4.55/5), appropriateness (4.36/5), and feasibility (4.11/5). Qualitative responses indicated a willingness to participate in Tech-AiD if available, described the program as a good fit for the needs of persons living with ADRD and care partners, and suggested that Tech-AiD’s delivery format was convenient. Qualitative responses also included specific suggestions to improve Tech-AiD (e.g., creation of a technology helpline, booster sessions). Results provide evidence of Tech-AiD’s readiness for a pilot trial.
• There are few evidence-based interventions to improve technology-based strategy use in the care of persons living with Alzheimer’s disease and related dementias (PWLADRD). • We conducted a multimethod study to evaluate invested partner perceptions of a novel behavioral intervention, Technology Assistance in Dementia (Tech-AiD). • Healthcare professionals and care partners to PWLADRD rated the planned intervention highly on measures of feasibility, acceptability, and appropriateness.
• Results support readiness of Tech-AiD for a pilot trial. • If proven feasible and efficacious in clinical trials, Tech-AiD would offer clinicians an empirically supported approach to improving technology-based strategy use in ADRD care. • Results also highlight the importance of focusing on accessibility and personalization in technology-based interventions.What this paper adds
Application of study findings
Introduction
Care partners to persons living with Alzheimer’s disease and related dementias (PLWADRD) may use technology-based strategies (e.g., video calls for social participation, wearable devices for location tracking, online portals for healthcare communication) to reduce burden and improve care (Fabricatore et al., 2020; Kiselica et al., 2024). While promising, technology-based strategies are not used frequently by care partners (Benge et al., 2020) and come with costs, complexity, and privacy and security concerns (Mikula et al., 2024).
As a solution, we developed an intervention to expand and optimize use of technology-based care strategies in ADRD care called Technology Assistance in Dementia or Tech-AiD (Figure 1; ANONYMIZED). Tech-AiD is a manualized treatment, consisting of a 5-week (one, two-hour session per week) program delivered by an occupational or behavioral health professional to empower PLWADRD and care partners to use technology-based strategies to meet personalized goals. Novel interventions, like Tech-AiD, need to be developed with input from invested partners who may deliver or participate in interventions (Harrison et al., 2020). Thus, we assessed care partner and healthcare professional perceptions of Tech-AiD’s acceptability, appropriateness, and feasibility to assess readiness for a pilot trial (Boyle et al., 2022; Proctor et al., 2011; Weiner et al., 2017). Visual depiction of the Technology Assistance in Dementia (Tech-AiD) intervention.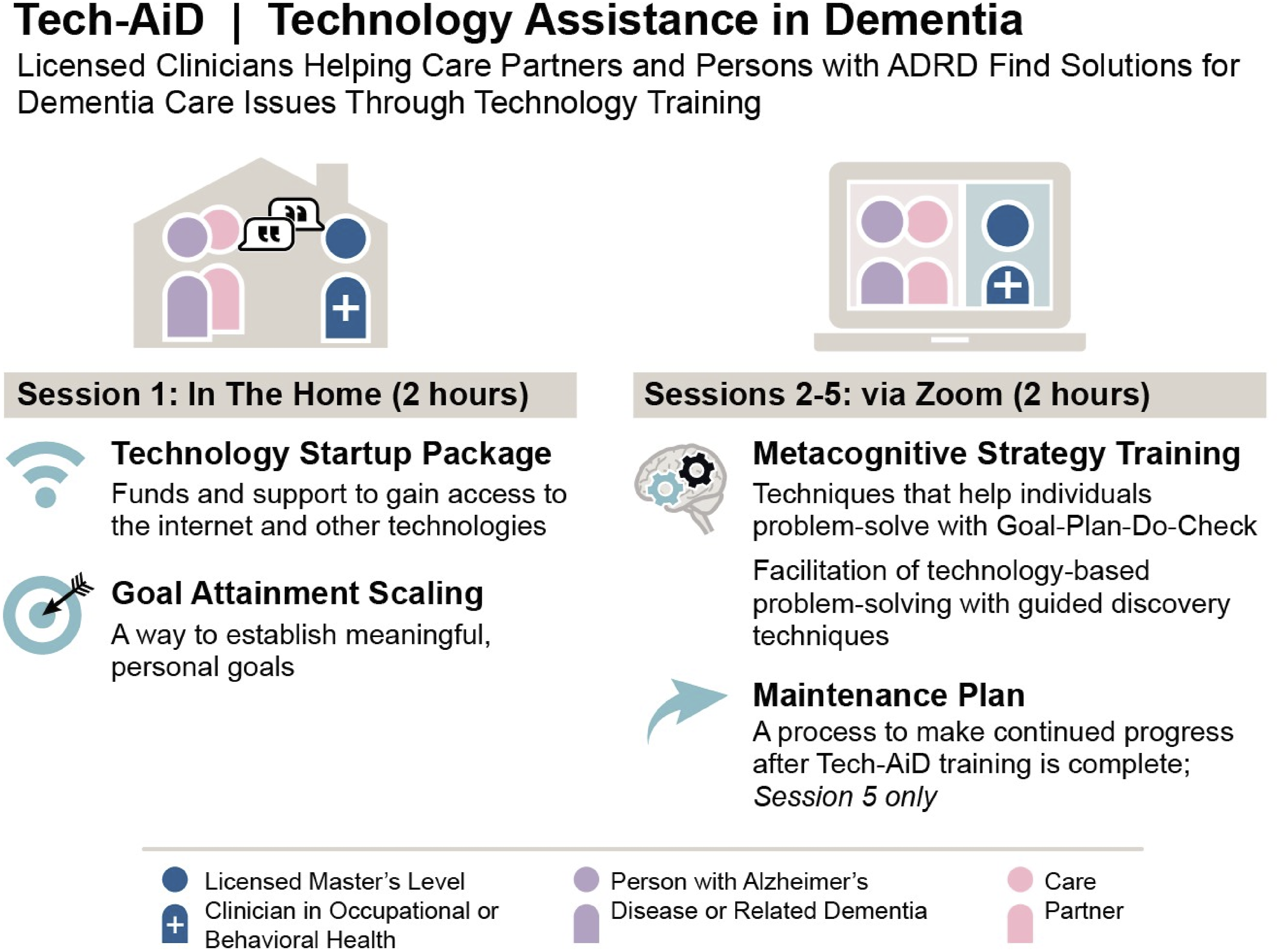
Methods
Study Procedures
We conducted a multimethod study in which participants 1) completed a demographic survey via Qualtrics; 2) reviewed a 10-min presentation describing Tech-AiD; 3) completed a knowledge check quiz with feedback for incorrect responses; and 4) participated in recorded semi-structured interviews (M = 56.50 minutes, SD = 13.33). Data collection was offered in person or via Zoom; all participants except for one care partner opted for Zoom. Participants received a $100 gift card. The research was granted exempt status by an IRB.
Participants
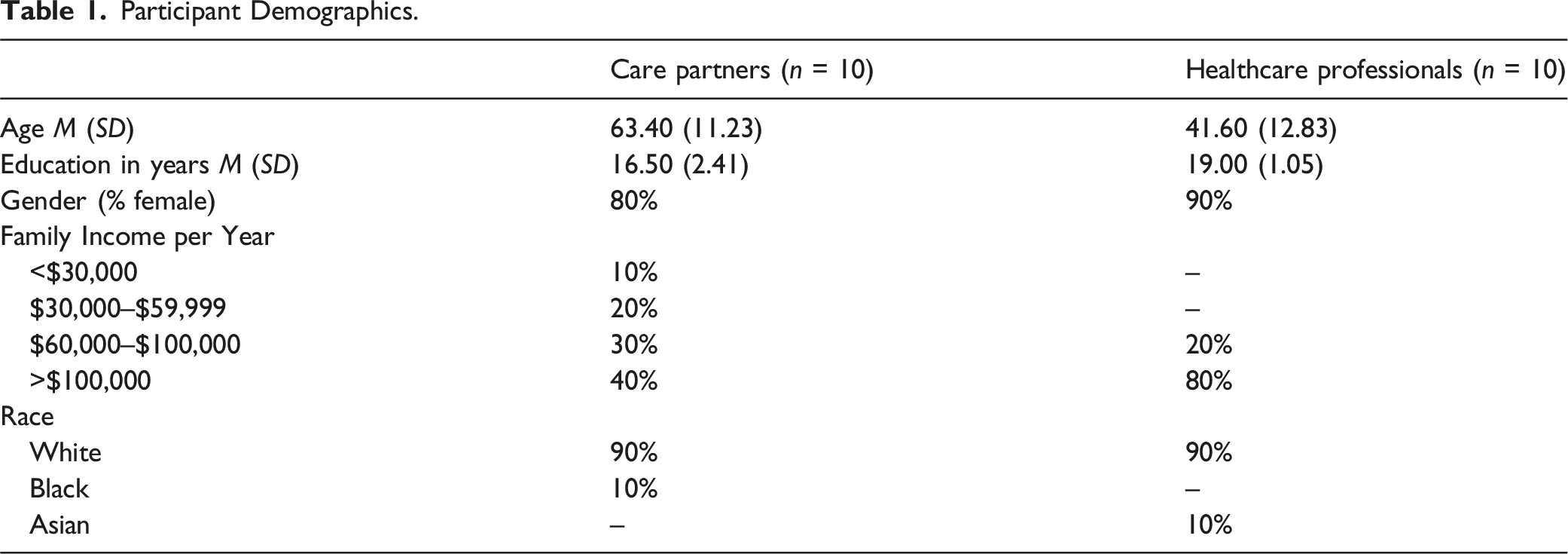
Participant Demographics.
Intervention Description
Participants viewed a 10-min presentation about Tech-AiD delivered by research staff following a script (supplemental materials). Tech-AiD is delivered to care dyads (PLWADRD and care partner) by a licensed clinician. The first session occurs in the home and includes a technology startup package (internet connected device with data plan). In this session, dyads also set individualized goals using Goal Attainment Scaling (Turner-Stokes, 2009). In sessions 2–4, the clinician utilizes metacognitive strategy training principles (Cicerone et al., 2019; Dawson et al., 2017) in the context of applying technology-based strategies towards individualized goals. Finally, in session 5, participants develop a maintenance plan to sustain progress.
Qualitative Interviews
Interviews inquired about acceptability, appropriateness, and feasibility of Tech-AiD (Weiner et al., 2017). In addition, we evaluated other aspects of Tech-AiD relevant to implementation (Baier et al., 2019), including the interventionist’s qualifications, the delivery method, session intensity and frequency, and session content.
Quantitative Measures
Knowledge Check
Nine multiple choice items assessed participants’ understanding of Tech-AiD. Participants correctly answered 85% (SD = 12.63%) on average and were provided with feedback for incorrect responses.
Implementation Readiness Measures
Implementation readiness measures (Weiner et al., 2017) included the Acceptability of Intervention Measure (AIM), Intervention Appropriateness Measure (IAM), and Feasibility of Intervention Measure (FIM). Each instrument includes four items rated on a five-point scale (1 = completely disagree; 5 = completely agree), and responses are averaged to obtain a total score. They had good to excellent internal consistency in this sample (AIM α = .90; IAM α = .97; FIM α = .81).
Specific Aspects of the Intervention
Interventionist
Participants responded to the following prompt using a five-point scale (1 = completely disagree; 5 = completely agree): “Individualized sessions with a licensed clinician are necessary for persons with dementia and their care partners to learn to use technology-based strategies.”
Delivery Setting
Participants responded to the following prompts using a five-point scale (1 = completely disagree; 5 = completely agree): “Having the first session in the home is a good idea”; “Having subsequent sessions over Zoom is a good idea.”
Session Frequency
Participants stated how often Tech-AiD sessions should occur: every day, twice per week, once per week, every other week, or once per month.
Session Length
Participants were asked how long Tech-AiD sessions should last: 30 minutes, 1 hour, or 2 hours.
Number of Sessions
Participants Specified the Ideal number of Sessions for Tech-AiD.
Tech-AiD Content
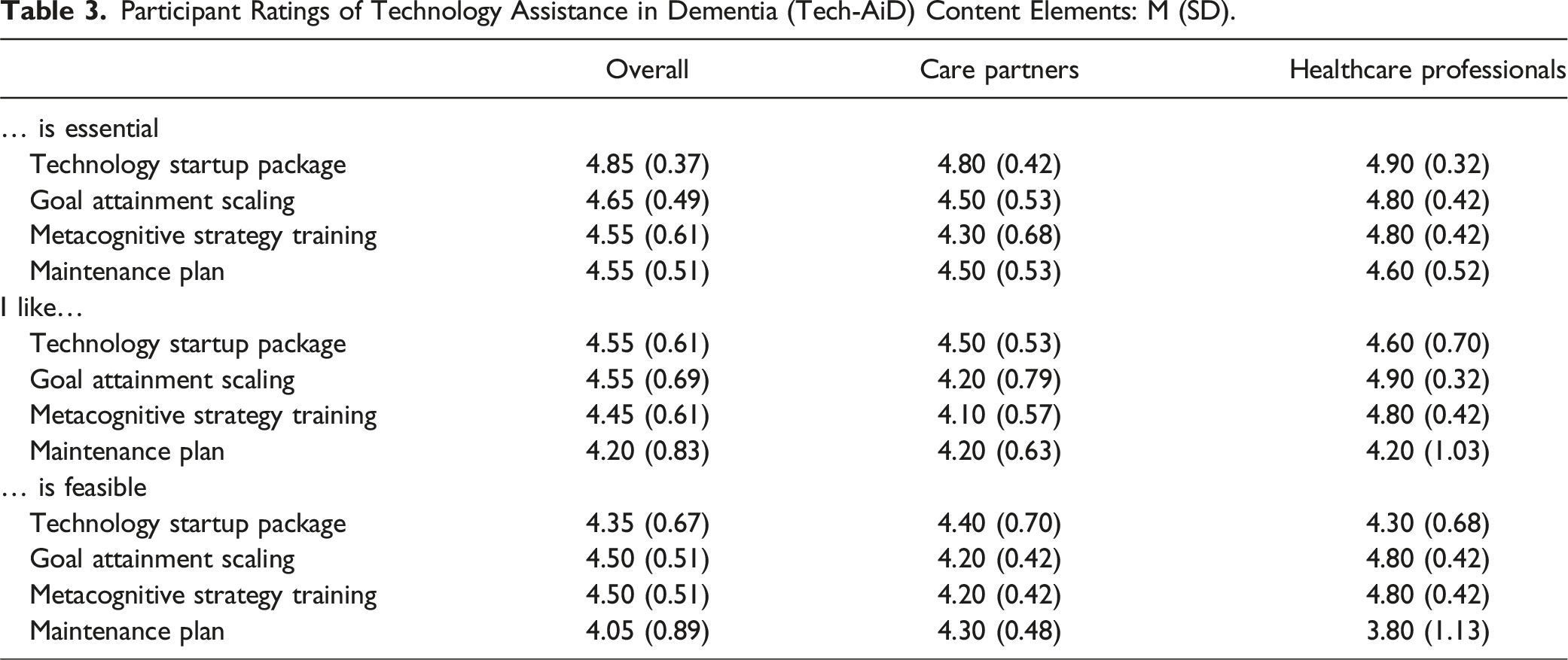
Tech-AiD sessions include four key elements: 1) a technology startup package; 2) individualized goal setting using Goal Attainment Scaling; 3) use of metacognitive strategy training principles to promote independent application of technology-based strategies; and 4) development of a maintenance plan to sustain progress. For each element, we asked participants whether they 1) liked it, 2) thought it was essential, and 3) thought it was feasible. They responded using a five-point scale (1 = completely disagree; 5 = completely agree).
Data Analyses
Quantitative Analyses and go-no-go Criteria
We summarized quantitative results using descriptive statistics and graphs. We operationalized a priori go-no-go criteria for whether results provided evidence to proceed with a pilot trial: A “go” result was defined by average AIM, IAM, and FIM scores >3. These criteria were based on agreeable responses to the AIM, IAM, and FIM measures, since 3 = a neutral response.
Qualitative Analyses
We transcribed audio recordings and analyzed transcripts using deductive qualitative analysis (Fife & Gossner, 2024). Deductive qualitative analysis is appropriate when researchers seek to ascertain whether qualitative data fit with an established framework; in this case, the framework was intervention implementation readiness focused on acceptability, appropriateness, and feasibility (Weiner et al., 2017). Development of a codebook started with these three codes, with additional iterative development of codes and subcodes based on analysis of the data until no new codes emerged. Three coders participated in coding with discrepancies resolved via consensus discussion. In the results, we describe the number of units of analysis that related to Tech-AiD’s acceptability, appropriateness, and feasibility and whether they were coded as positive, neutral/mixed, or negative. Additionally, we used subcodes to identify themes related to acceptability, appropriateness, and feasibility, as well as to understand the qualitative reasoning behind participants’ quantitative responses regarding specific aspects of Tech-AiD.
Results
Tech-AiD Implementation Readiness
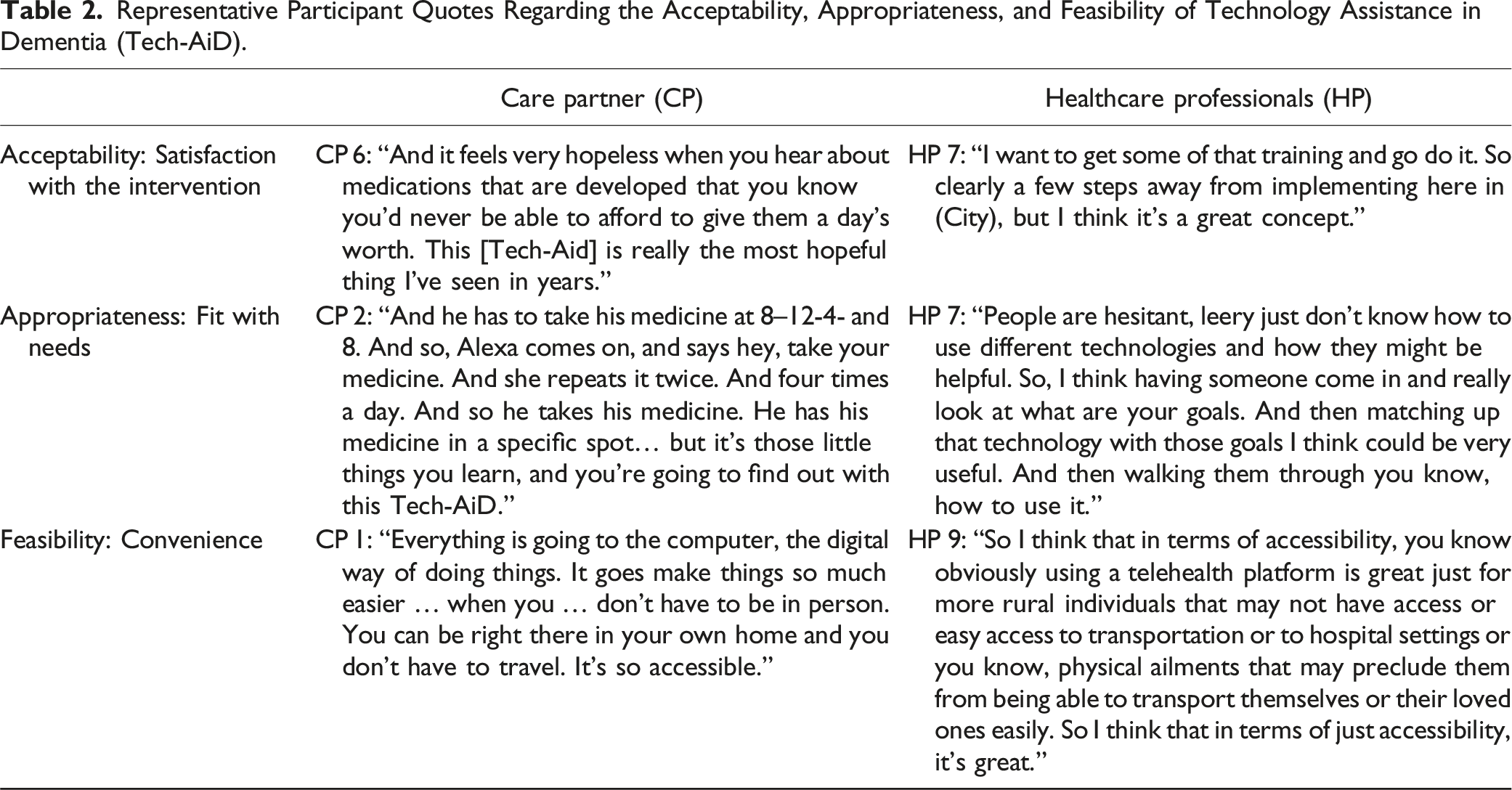
Participants indicated (Figure 2) they found Tech-AiD to be highly acceptable (overall M = 4.55, SD = 0.60; CP M = 4.28, SD = 0.70; HP M = 4.83, SD = 0.31), appropriate (overall M = 4.36, SD = 0.62; CP M = 4.05, SD = 0.61; HP M = 4.68, SD = 0.47), and feasible (overall M = 4.11, SD = 0.50, CP M = 3.98, SD = 0.40, HP M = 4.25, SD = 0.58). The majority of qualitative responses (Supplemental Figure) regarding acceptability (91.30%), appropriateness (73.46%), and feasibility (56.14%) were positive. See Table 2 for interview excerpts. Positive responses regarding acceptability reflected satisfaction with Tech-AiD and willingness to participate in it. Positive responses relevant to appropriateness centered on the perceived fit of the intervention for the needs of the care dyad or the provider. Finally, qualitative responses regarding feasibility focused on the convenience of Tech-AiD. Density plot of average scores for Tech-AiD on the Acceptability of Intervention Measure, Intervention Appropriateness Measure, and Feasibility of Intervention Measure. The dotted line indicates a neither agree nor disagree response; scores above this line indicate agreement that the intervention is acceptable, appropriate, or feasible. Representative Participant Quotes Regarding the Acceptability, Appropriateness, and Feasibility of Technology Assistance in Dementia (Tech-AiD).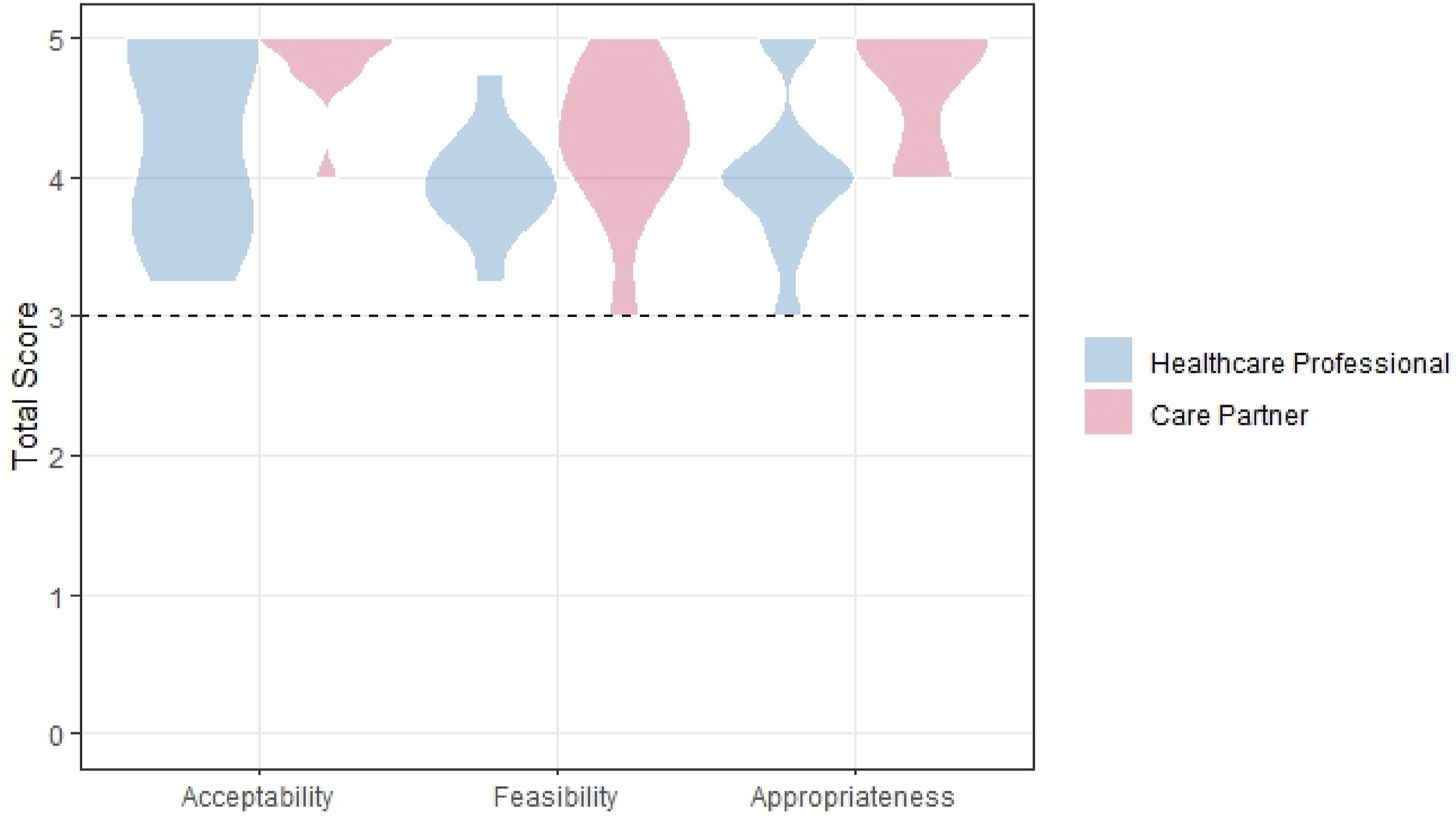
Neutral/mixed comments were somewhat common regarding Tech-AiD’s feasibility (39.47%). The most common concern regarding feasibility was how participants might be supported to use technologies outside of sessions, and a suggestion to improve feasibility was to add a technology helpline: CP 8: “Are we able to pick up the phone and call somebody for the technical advice that we need or do we have to wait till the session?”
Specific Aspects of Tech-AiD
Interventionist
Participants largely agreed that a licensed clinician should deliver the intervention (overall M = 4.25, SD = 1.12; CP M = 4.10, SD = 1.29; HP M = 4.40, SD = 0.97). Qualitative responses suggested that the involvement of a qualified HP was necessary given the complexity of ADRD: HP 4: “And I really think that when it comes to dementia, it needs to be a clinician. It needs to be somebody who understands cognition and brain changes and has training. … I really feel like having a licensed clinician is necessary.”
Delivery Setting
There was near complete agreement that an initial in-home session was a positive aspect of Tech-AiD (overall M = 4.80, SD = 0.41; CP M = 4.80, SD = 0.42; HP M = 4.80, SD = 0.42). Participants described this option as more convenient for care dyads and noted that it could provide actionable information for HPs. HP 2: “Any time you have an in person visit in someone’s home, A) it makes them feel like you care, and B) you get a good sense of what their abilities are in their home. You can work with that environment, and how its set up, or you can help them set it up a different way.”
There was somewhat less enthusiasm for holding subsequent sessions over Zoom, though Zoom sessions were still rated positively (overall M = 3.90, SD = 0.92; CP M = 4.00, SD = 1.15; HP M = 3.80, SD = 0.63). Qualitative responses described Zoom as convenient, though concern was expressed about difficulty using Zoom among PLWADRD: CP 7: “[Zoom is] More Convenient for Everybody.” HP 6: “[Zoom] can also be overwhelming and off-putting, and so I think that some people won’t want to participate.”
Session Frequency
A sizable majority of participants indicated that the ideal session frequency for Tech-AiD would be once per week (overall = 75%; CP = 80%; HP = 70%). A once per week session frequency was described as balanced: HP 8: “I think once a week is … doable for a lot of people and … it’s… hard for them … to have … multiple times a week. But then like, every other week they may like, forget or … need more like immediate like assistance with stuff. So like, I think once a week is a good like happy medium.”
Session Length
A majority of participants indicated that the ideal session length for Tech-AiD would be 1 hour (overall = 65%; CP = 60%; HP = 70%). One hour was described as long enough to cover material without encountering boredom or distraction. CP 6: “30 minutes—you just barely feel like … you can ask your questions and make sure you’re grasping everything. More than an hour, I think is … too much time.”
Number of Sessions
On average, participants described the ideal number of sessions for Tech-AiD as 6 (overall M = 6.40, SD = 2.39; CP M = 6.40, SD = 2.99; HP M = 6.40, SD = 1.78). This ideal number seemed to reflect a desire to add a booster session to the five-session structure. HP 4: “I just feel like you … need to have that follow up, in order to just have that check in with yourself and make sure everything is going [well].”
Tech-AiD Content
Participant Ratings of Technology Assistance in Dementia (Tech-AiD) Content Elements: M (SD).
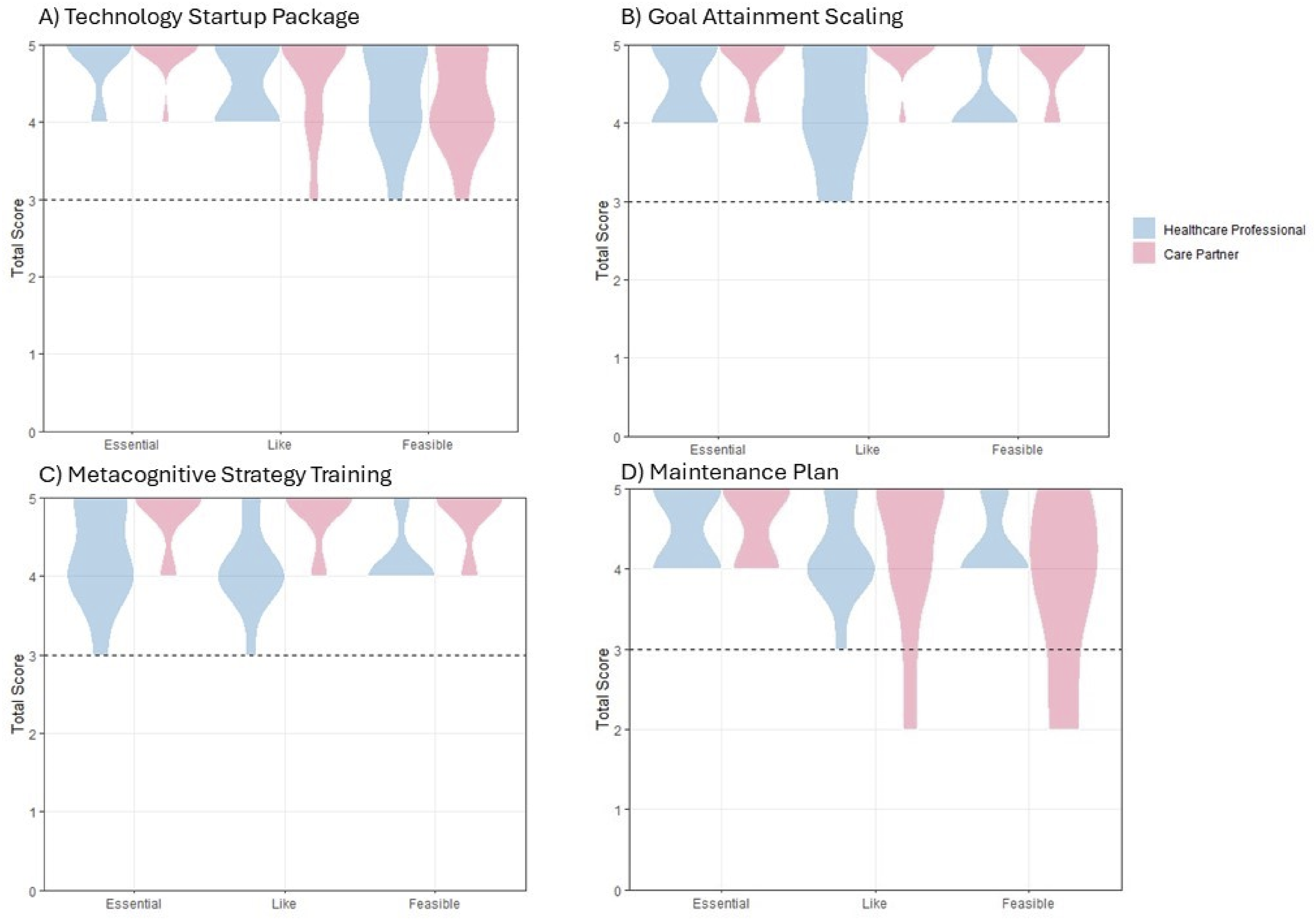
Density plots of average scores for each element Tech-AiD: (a) the Technology Startup Package; (b) Goal Attainment Scaling; (c) Metacognitive Strategy Training; and (d) the Maintenance Plan. Participants rated the elements on whether they were essential, whether they liked the element, and whether they thought the element was feasible. The dotted line indicates a neither agree nor disagree response; scores above this line indicate agreement that the element is essential, well liked, or feasible.
Discussion
Tech-AiD Implementation Readiness
19/20 (Figure 2) participants rated the intervention >3 on all implementation readiness measures, meeting our a priori criteria for proceeding with a pilot trial. Further, the majority (56.14–91.30%) of qualitative comments were positive toward Tech-AiD (supplemental figure). High ratings for acceptability reflected satisfaction with Tech-AiD and a willingness to participate, consistent with the Technology Acceptance Model (Venkatesh et al., 2012). Positive responses regarding appropriateness appeared driven by a perception that Tech-AiD would fit the needs of care partners and PLWADRD, consistent with findings that PLWADRD and care partners prefer individualized care (Gibson et al., 2015). Finally, strong feasibility ratings indicated that Tech-AiD participation would be convenient, overcoming logistical barriers to treatment (e.g., distance). A frequent suggestion to improve feasibility was to add a technology helpline. Key lessons learned from this research for technology-focused behavioral interventions include the importance of meeting the needs of care dyads, individualizing treatment, and providing as needed support.
Specific Aspects of Tech-AiD
Interventionist
Participants expressed agreement that Tech-AiD should be delivered by a licensed clinician (4.25/5), driven by a belief that the complexity of helping a PLWADRD requires specialty training. Research supports this assumption: Individuals receiving dementia-specific care tend to have better outcomes than those receiving non-specialty care (Orth et al., 2023).
Delivery Setting
Participants expressed near complete agreement that having the initial session of Tech-AiD in the home was a good idea (4.8/5). This findings fits with the stated preferences of PLWADRD, who feel that home-based services better meet their daily needs (Hoel et al., 2021). There was somewhat less enthusiasm about holding subsequent sessions over Zoom, though Zoom sessions were still rated favorably on average (3.9/5). Studies show good feasibility and acceptability of telehealth approaches among PLWADRD (Yi et al., 2021).
Session Frequency, Duration, and Number
A sizable majority (75%) of participants agreed that weekly sessions were appropriate and provided a balance, allowing adequate time to practice skills, while preserving recall of previous sessions. Next, most participants (65%) reported that one-hour sessions would be ideal. One hour was perceived by participants as allowing enough time for coverage of material without inducing boredom or distraction. Finally, participants reported that six sessions would fit with their ideal treatment length. This perception was rooted in a liking of our five-session framework with an added booster session.
Tech-AiD Content
Participants reacted favorably to all four content elements of Tech-AiD (Table 2, supplemental table, Figure 3). First, the technology startup package was reported to offset a main barrier to use of technologies in ADRD care—financial costs (Mikula et al., 2024). Second, Goal Attainment Scaling was thought to be important for individualizing the intervention and tracking goal progress, which has been missed in prior technology-based ADRD interventions (Boyle et al., 2022). Third, metacognitive strategy training was rated as essential for acquiring technology skills and applying them to ADRD care, consistent with the importance of technology training (Werner et al., 2022). Finally, the maintenance plan was described as a way to preserve progress following intervention completion.
Limitations and Future Directions
Findings from this study must be interpreted in light of certain limitations. First, it should be noted that we assessed participant perceptions of the intervention based on a description, and a future pilot trial is necessary. Second, we focused on the viewpoints of care partners and healthcare professionals, and it will be important to ascertain perceptions and experiences with Tech-AiD among PLWADRD. Finally, our sample overrepresented White women, and future work should gather feedback on Tech-AiD from a more racially and gender diverse sample. Even considering these limitations, the results provide strong support for Tech-AiD’s readiness for a pilot trial.
Supplemental Material
Supplemental Material - Invested Partner Feedback on Technology Assistance in Dementia (Tech-AiD)
Supplemental Material for Invested Partner Feedback on Technology Assistance in Dementia (Tech-AiD) by Andrew M. Kiselica, Greta Hermann, Sawyer Harmon, Megan Gilligan, Rylea Ranum, Anna Boone, Timothy Wolf, Alan Stevens, Renato F. L. Azevedo, Jenay Beer, and Jared Benge in Journal of Applied Gerontology
Footnotes
Acknowledgments
We would like to acknowledge the support of a proposal illustrator, Samantha Bosland, for assistance with one of the figures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a career development award from the National Institute on Aging of the National Institutes of Health award Number [U54AG063546], which funds National Institute on Aging’s Imbedded Pragmatic Alzheimer’s and AD-Related Dementias Clinical Trials Collaboratory. Additional support was provided by the National Institute of Health grant number [AG082783]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Statement
Data Availability Statement
Deidentified data will be shared with others upon reasonable request to the first author.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.