
Abstract
Person-centeredness is generally viewed at the interpersonal level of one-on-one interactions, but broader systemic components affect these interactions. Individuals (micro level) are embedded institutions (meso level) which are embedded in society (macro level), all of which affect person-centeredness. This special article draws on five discussion groups with diverse participants to better understand person-centeredness in a systemic context. Insight indicated four key issues inherent in person-centeredness: that it varies based on the system; that principles from one system can be applied to another; that limits on person-centeredness are necessary for system success; and that the amount of person-centeredness within a system is dependent upon resources, resulting in societal inequities. These insights are integrated to provide implications for practice, policy, and research related to healthcare and long-term care for older adults.
• An elucidation of how understanding the functioning of one system can promote understanding of the functioning of another system • New insights of four key issues related to person-centeredness in healthcare and long-term care for older adults
• Suggestions of how to promote person-centeredness in long-term care in recognition of its systemic nature • Future research into person-centeredness recognizing long-term care as a complex adaptive systemWhat this paper adds
Applications of study findings
Person-centeredness has become a catchword of quality health care in general (National Academies, 2018) and particularly of geriatric medicine and long-term care (American Geriatrics Society, 2016; Tellis-Nayak, 2007). Generally speaking, the concept involves focusing on the person as an individual, knowing them holistically, and meeting their needs and preferences (American Senior Communities, 2018). However, despite its frequent use in the literature surrounding care, the term “person-centered” lacks an agreed-upon definition and generally accepted key parameters and measurement principles (Efird-Green, under review).
This research began by conducting a search of the academic and gray literature for definitions of person-centeredness. These included statements and discussions from a variety of online sources (American Senior Communities, 2018; Center for Medicare and Medicaid Services, 2025; Code of Federal Regulations, 2024; Washington DC Department of Disability Services, 2025) and publications that addressed the topic (American Geriatrics Society, 2016; Brocato, 2009; Kitwood, 1997; Rogers et al., 2013;). After the literature review was completed, a think-tank of researchers associated with LINC-AD, an interdisciplinary consortium funded by the National Institute on Aging with a focus on improving care and outcomes for people living with dementia, met to discuss results of the literature review and to propose next steps. They agreed that the concept of person-centeredness needed refinement and proposed an effort to investigate it from multiple perspectives. This paper reports results of the activities related to person-centeredness from a systemic perspective.
The conceptual framework was Jonathan Turner’s Macro-Micro-Meso theory, which is referenced and displayed in Figure 1 (Collins, 2021). For example, in the context of long-term care for older adults, the interpersonal level reflects the daily interactions between care providers and residents in a nursing home (micro); which are influenced by the policies of that nursing home (meso); as well as by the societal issues related to the nursing home as it is situated within the larger US healthcare system (macro); see Figure 1. More so, the embedded levels of micro, meso, and macro relate to all systems and are not exclusive to health care; they are similarly applicable to areas ranging from government to business to education (Artemova et al., 2021; Kunze, 2013; Nisar, 2021; Veech, 2004). By way of illustration, one-on-one interactions between instructors and students (micro) are embedded within the practices and policies of a given school (meso), and also within the practices and policies across school systems, and the state and national organizations that regulate and oversee educational programs (macro). However, the general promotion of person-centeredness tends to gloss over the nuances of its expression within a systemic context, and understanding these nuances may inform the concept in relation to the well-being of older adults. Levels in Long-Term Care Systems Relevant to Person-Centeredness: Interpersonal (micro), Institutional (meso), and Societal (macro)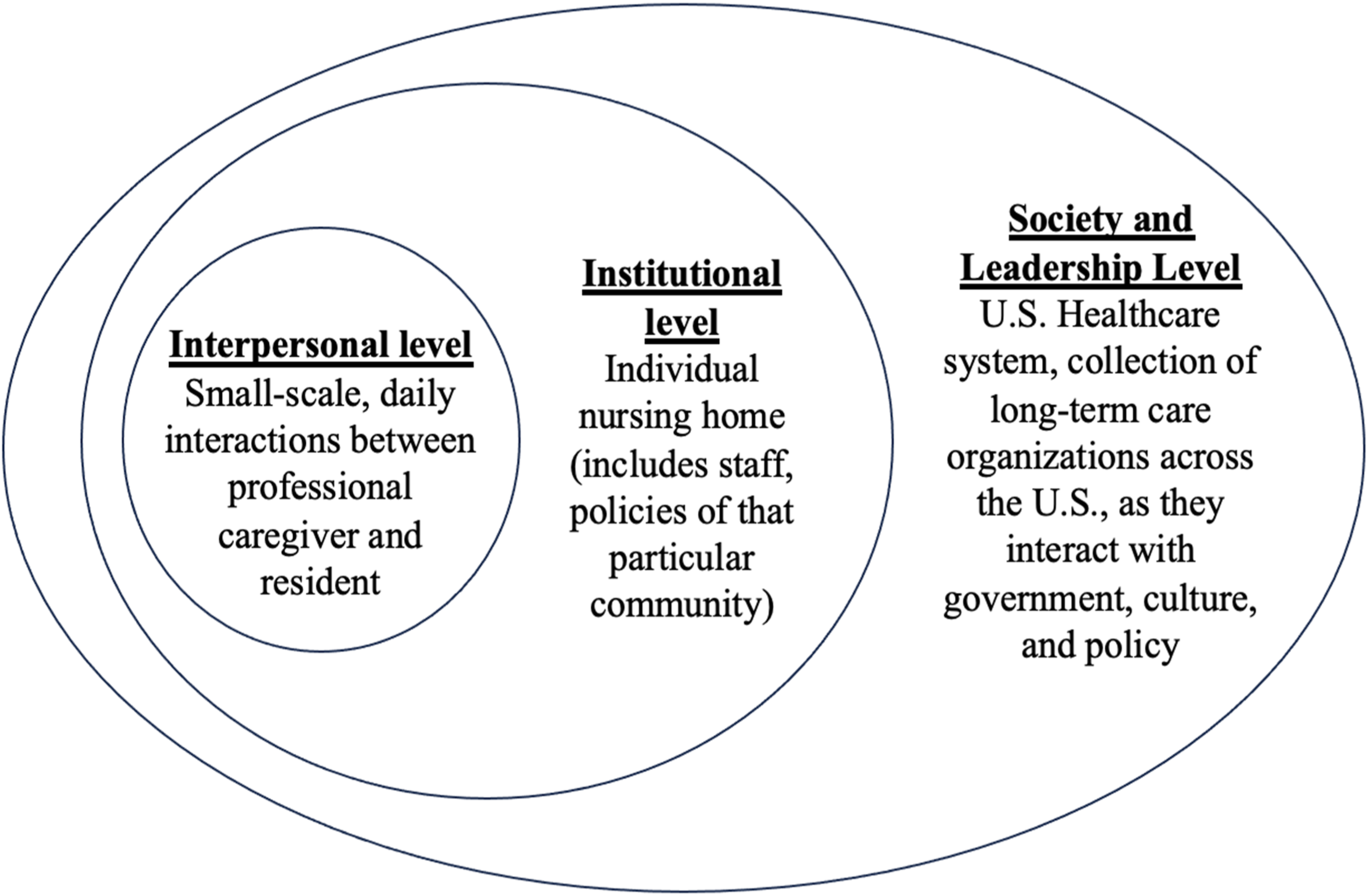
To understand the concept of person-centeredness from the perspective of systems, and how different systems may inform the expression and expectations of person-centeredness, three face-to-face meetings were held, which included staff working in a senior living community; members of the Alzheimer’s Association Dementia Care Provider Roundtable; and attendees of the Center for Innovation 2023 annual conference. In addition, two virtual Zoom meetings included diverse national experts were held, composed of an attorney with extensive experience in long-term care, a professor of health policy, a professor of ethics and social work, long-term care policy researchers, a physician leader in long-term care, a leader in nursing and rehabilitation policy, and a social worker with national expertise in policy and advocacy pertaining to older adults.
Each discussion began with this introduction: We’re here to talk about what it means to be person-centered. People have used the term person-centered as though it’s a simple concept, but we’re coming to realize that person-centeredness isn’t as straightforward as it may seem. Today we’d like to discuss person-centeredness not to arrive at a definition, but to understand it more broadly. In today’s discussion, we want to focus on person-centeredness within formal systems—educational systems, workplace systems, governmental systems, and health care systems.
For each of the above systems (educational, workplace, government, and health care), two questions were asked: (1) What’s an example of a person-centered situation you’ve experienced or know of? (2) What’s an example of a non-person-centered situation you’ve experienced or know of? Additional questions asked (3) To what extent can person-centeredness exist in a for-profit environment? (4) How can an organization effectively provide oversight of the person-centeredness of its services? And (5) Can and should person-centeredness be mandated by an organization? If so, how can that be done effectively and efficiently?
Meetings were audio-recorded and transcribed. Each had a project member assigned as a note-taker, who produced a summary within 24 hours, which was subsequently reviewed and edited by the project team. An exploratory thematic analysis was conducted, with materials analyzed by the study team using a qualitative iterative process. Themes were developed by group consensus and further refined by project team members so as to incorporate input from all project components.
This special article presents the four key observations emanating from the group meetings, shedding light on how person-centeredness can be understood from the systemic perspective, particularly in relation to long-term care for older adults.
Systemic Issues Inherent in Person-Centeredness
Group discussion elucidated insights inherent in person-centeredness based in part on the differences to which they are exhibited within different systems. Overall, it was considered that the most person-centeredness is expected in hospitality, followed by healthcare, education, government, and businesses that produce material goods. Based on the discussion, group meetings identified four issues inherent in person-centeredness: that it varies based on the system; that principles from one system can be applied to another; that limits on person-centeredness are necessary for system success; and that the amount of person-centeredness within a system is dependent upon resources, resulting in societal inequities. Each issue is elaborated below, with related quotes.
The Goals and Manifestation of Person-Centeredness Vary Depending on the Scale of the System, an Individual’s Role within the System, and the Hierarchical Nature of the System
Person-centeredness can be considered within virtually all types of systems, but the parameters and goals of person-centeredness within systems may vary depending on issues such as the numbers of people receiving services (scale); whether the individual is paying for a service or receiving payment for their efforts (role); and inherent managerial and organizational structures that either minimize or emphasize a person’s autonomy (hierarchy).
Considering the matter of scale—the number of people receiving services—person-centeredness is more likely in systems where services are provided in dyads and small groups, compared to larger settings in which the needs of the group take priority when services intend to meet the needs of the greatest number of people. Moreso, as illustrated in the examples below, the extent of person-centeredness can vary in the same type of system. “In healthcare, it's usually a dyad, right? It’s us and our provider, therefore the emphasis on me as a person matters. As opposed to congregate settings, such as a classroom or a workplace, where it has to be the good of the individual as well as the good of the group.” “I’m thinking of going through preparation for joint replacement, and they tried to do the education in a group setting … some people didn’t drive, some people were 90, some people were 50 … there was a lot that didn’t matter to many of us. That’s why healthcare [should be person-centered] because so much of it is personal, delivered to us one-on-one as opposed to as part of some cohort.”
In addition, the expectation of person-centeredness in systems tends to be vary depending on the individual’s role within a system—being more expected when the person is receiving a service and less expected when the person is the one providing the service. More pointedly, there is less expectation for person-centeredness towards employees because workplace goals are largely for the employee to provide value to the organization, as opposed to what might be expected if one was the person paying for services. One group member noted “Another thing…is distinguishing the goal of the system. You’re showing up to work—you’re not paying for that. They’re paying you, and so it’s not about providing a value to you necessarily.” Still, systems vary in their proclivity for person-centeredness toward their employees. It is particularly hindered in institutions that are hierarchical and define their outcomes as deliverables, as reported in these two examples. “I have this image of a factory being very hierarchical. You’re working on this assembly line and you’re told what to do. And if you have an opinion, [you’re told] ‘shut up and keep working’.” “When I bagged groceries … you were told what to do. And if you said ‘oh, we could do this faster, we could do this better’ - [you’re told] ‘thanks for that but keep bagging groceries’. You’re not given a voice….You don’t have control or autonomy over what you’re doing. You’re just a cog in the machine.”
On the other hand, some systems are more sensitive to person-centeredness in relation to their employees, manifested by the extent of discretion and autonomy allowed to the worker. “When we did the evaluation at Greenhouse [a model of nursing home care], the person at the center of everything was still the [nursing home] resident, but these staff members who had been marginalized in a lot of settings actually were given a lot more voice and autonomy there.” At the employee level, person-centeredness can be experienced as listening to and respecting the opinions of workers; one cafeteria worker said: “We [a cafeteria staff member working in a senior living community] have influence. We can let [the dining service supervisor] know how we think about things—he asks us a lot of questions. He’s very hands-on with us. If there’s anything we can work on, he’ll let us know, and we try to fix it. And sometimes we get it the first time and sometimes we don’t. But it’s a friendly reminder, and it’s personal—it’s person-centered. It’s not like ‘this is your job’ and that’s it. He’s a little bit more with us.”
Principles of Person-Centeredness within One System Can Apply to Another; Most Notably, Applying Principles of the Hospitality Industry to Healthcare and Long-Term Care Organizations
The hospitality industry, known for its “customer is always right” attitude, is obligated to provide personalized services for paying customers. As one participant stated, “We’re the customer. We’re paying, and if it’s not person-centered, we’ll go somewhere else where we’ll feel person-centered.” In fact, some group members noted that person-centeredness is synonymous with hospitality. One said, “We’ve overthought [person-centeredness] so much we’ve gone away from basic customer service” and another noted: “Go back to the basic foundation of customer service…If I’m a vegan, don’t give me meat—that’s not what I want or need. Or if I’m in a hotel and I don’t want to be on the 11 th floor… they’re going to try to adapt to what my needs are... and it really is person-centered.”
The idea of systems serving “customers” extends beyond restaurants and hotels to other systems where one is paying for a service. In this sense, healthcare and long-term care are also based on the customer model where individuals pay for services; therefore, there is an expectation of person-centeredness, most especially when the cost is directly out-of-pocket. Assisted living, for example, was initially developed with a strong hospitality emphasis, to provide a contrast to the institutional structure of nursing homes—and notably, assisted living is largely a private pay model, whereas nursing home care is largely publicly funded and not considered to have a hospitality focus. A staff member working in the senior living community noted “Each [resident] here has a different state of mind … They’re always going to be right. …If they get mad at you, just take it. Don’t go against them. Just say ‘yes, okay, you’re right’. Do what they want, it’s all about giving what they want.” Other examples on the senior living setting included ensuring that pescatarian residents have fish options at two meals a day, serving onions according to resident preferences, and having budget flexibility to allow kitchen staff to be creative in food purchases; in fact, some group members described the ideal long-term care worker as caring about people in a manner similar to workers in the hospitality industry.
Some Limits on Person-Centeredness are Necessary for System Success
Even when person-centeredness is presumably inherent in the goal of a system, there are times when return on investment, financial stability, policies, and safety place limits on person-centered practices. For example, it may not be safe to allow a long-term care resident to take medications exactly as they would like (such as taking all medications in the morning), as in “I think every interaction has to have person-centered in it, but it might not be an absolute 100% of what the patient really wanted, because if we’ll start giving what patients really want, or what the families really want, we could actually be harming them and we’re not going to do that.”
Person-centeredness can also be limited by policies that have the intention of achieving other necessary goals; one group member described competing goals as follows: “It’s competing goods, right? It’s the dilemma—because there are things we value: meeting the needs and assets of the individual—the reasons to be person-centered—and yet we also value consistency, equity, efficiency, return on investment.” At the same time, group members recognized that systems may have flexibility to accommodate person-centered practices, such as making atypical food purchases for dining services: “You just have to think about it logically, honestly. I mean, don’t go $5,000 over budget…So a lot of times the servers will talk to me and one of the requests they’ll get is ice cream sandwiches or certain types of foods, and maybe it’s not in our business model for buying, but we can find ways around that still help them out and find compromises.”
The Extent of Person-Centeredness is Dependent on Resources, in which Case Inequities Hinder Person-Centeredness
As noted in the preceding quote, the ability of a system to be person-centered is restricted by resources, including money and time. When asked about what limits their ability to meet food requests of senior living community residents, one staff member responded, “It’s the time and preparation that it takes to [address resident requests]. We’ve had to reduce some of that to be able to make the rest of the residents happy.”
The limitations to person-centeredness are evident across systems, with this example pertaining to government systems. “If you file a complaint with the department of health in almost any state right now, you are not going to get a personal response. No one is going to answer the phone; you’re not going to get a letter; and when you eventually get a letter a year from now, it’s not a personal letter…The system is not set up to promote person-centered interactions and responses, and some of that is just size and ability and funding and all the things that we know.”
In contrast, individuals paying for concierge medicine are typically able to receive personalized, readily accessible care, because they pay a premium for it. “Concierge medicine is an example of something that’s very person-centered. It’s a high-end model that these individuals can call their doctor when they want. ‘I want to come in today and I want to do this’. Whether that’s a good thing for their health, that’s separate, but it’s very much about the individual.” What this example displays is that person-centeredness is a commodity that in some instances can be purchased, and which is not available to all.
Because person-centeredness is bound by resources, person-centeredness in systems exists in the context of social barriers and resource inequities. “I think about it like informed consent, in that people have autonomy, people have self-determination but you can’t self-determine when there are no resources. I mean, someone may want to stay at home, but if there are no resources to support that… that seems like that’s part of the rub.”
Conclusions and Implications for Practice, Policy, and Research
There exist numerous types of systems, each including interpersonal (micro), institutional (meso), and societal (macro) levels relevant to person-centeredness. Comments from diverse individuals participating in group meetings identified four central topics related to person-centeredness by discussing similarities and differences within the systems: that goals and manifestations of person-centeredness vary across system type; that principles from one system can be applied to another, especially the hospitality industry that can inform healthcare and long-term care; that some limits on person-centeredness are necessary for system success; and that the availability of resources exert influence on the ability of a system to be person-centered, resulting in societal inequities in person-centeredness.
Expectations of person-centeredness vary depending on the type of system: in general, it was thought that most person-centeredness is expected in businesses related to hospitality, followed by healthcare, education, government, and businesses that produce material goods. This variation was thought to largely reflect the extent to which dyads and small groups are a focus of the system’s mission. Within all systems, however, opportunities exist to apply and augment principles of person-centeredness, including for the workers—for example, by promoting worker autonomy and fostering a culture wherein their voices are valued and contribute to decision-making (Zimmerman et al., 2014). These principles of management are reflected in literature describing the person-centered approach taken by organizations in the automobile and hotel industries toward employees (Hashimoto, 2021; Veech, 2004;), and that are especially relevant to industries that experience high employee turnover, such as the hospitality industry (Liu & Cho, 2011). Applying these person-centered practices toward employees in long-term care organizations may similarly help address high staff turnover and the quality of care provision (Castle & Engberg, 2005). Other research suggests that staff empowerment practices, such as flattened administrative hierarchies and involving staff in programming and management decision-making contribute to staff retention (Berridge et al., 2018; Zimmerman, 2024) for review). One area of person-centeredness not discussed in the group meetings but that also contributes to retention of direct care aides is having opportunities for advancement (Berridge et al., 2018), which is clearly person-centered.
The hospitality industry centers around providing personalized services for customers; similarly, healthcare systems, including long-term care settings, are customer-based, and so principles and applications of person-centeredness borrowed from the hospitality industry may be useful to make healthcare more person-centered. However, structural barriers to person-centeredness exist in healthcare systems, such as a culture of paternalism, high levels of regulation, and depersonalization of patients (Eisenberg, 1997). More so, some authors assert there are key differences between customer service and care, in that customer service is more scripted and detached than patient care; patients are by definition more vulnerability than customers; and patients often seek care because they have no choice while customers can choose to make purchases (Torpie, 2014). Consequently, literature emphasizes the importance of training employees in customer service principles, promoting team building among staff, and defining standards of service (Howard, 1999) as well as application of policies such as providing a customer service handbook for staff, pursuing outside consulting to improve customer service relations, and encouraging staff participation in activities regarding customer relations (Cheng et al., 2005). Thus, the literature provides considerable support for highlighting the importance of customer service as a first step in quality, person-centered care, which may increase person-centeredness in healthcare and long-term care for older adults.
Even in the best of circumstances, however, some limits on person-centeredness are necessary for system success. For example, an institution may value efficiency, standardization, and return on investment, but these values may translate into policies which in effect result in a system that does not leave much room for individual discretion. Therefore, in a conflict between organization and individual values, a balance is necessary, allowing for person-centeredness while preserving the values central to organizational stability. For example, a nursing home resident may wish to spend time outdoors, but would prefer to do so in front of the building rather than on the patio designated for time outside, putting himself at risk of injury or wandering without supervision; to address this and similar issues, tools such as the Rothschild Person-Centered Care Planning process have been developed to facilitate collaborative decision-making between long-term care residents, families, and professional care staff (Behrens et al., 2018), and others have more recently been recommended (Zimmerman & Cohen, 2010).
In addition, it is helpful to recognize that healthcare systems are complex adaptive systems composed of numerous independent individuals who interact in a nonlinear manner and in which one systemic element may need to adapt to accommodate changes in other parts of the system (Martin, 2018; Zimmerman, Moczygemba, Sloane, & Fazio, under review). Thus, policies that impact interpersonal interactions would need modification to change care at the person-level, lest policies that preserve the goals of one level impede desired activities at other levels. An area of future research would be exploring the concept of complex adaptive systems specifically in the context of person-centeredness.
Person-centeredness provided in human services is limited by finite resources such as staff availability and funds. Given these limitations, direction of resources toward one activity or output and away from others reflects values and priorities of that organization and serves as a limiting factor to person-centeredness—as illustrated by studies finding that lower staffing ratios in long-term care are associated with worse resident outcomes (Harrington et al., 2020). If money is a limiting factor for person-centeredness, it follows that an increase in reimbursement will allow for more person-centered care; however, this relationship is not straightforward (Grabowski, 2001), as it is complicated by factors such as resident case-mix and may be circumvented by profit-making incentives (Harrington et al., 2020; National Academies, 2022; O’Neill et al., 2003). Therefore, while resource limitations are an important issue in care—and particularly in long-term care—governmental and corporate policies, and differences in business models, must be taken into consideration when promoting person-centered care.
Finally, for a system to be truly person-centered, it must account for the person in the context of their identity and life experience, and adjust for systemic inequities of society. Addressing these issues is challenging. Factors such as cultural values may impact the care a person receives (Johnstone et al., 2016); expectations for communication style may vary between individualistic and collectivist cultures (Armstrong & Swartzman, 2001); and decision-making processes may not emphasize the person who is the consumer of care (Johnstone et al., 2016; McLaughlin & Braun, 1998). Linguistic diversity is another component of identity that must be considered in person-centeredness; when not accommodated, language difference can become a barrier resulting in incomplete communication and preferences not being met (Eriksson & Hjelm, 2022). Tools must be translated into multiple languages, as has been done in the case of cognitive testing instruments (Khan et al., 2022; Steis & Schrauf, 2009), but individuals who speak the language must be available to communicate effectively. Indeed, so challenging are these issues that some researchers have called for reimagining the concept of personhood itself, asserting that the current model of person-centered care does not account for power dynamics, oppression, and limited agency accorded to certain groups in society (Smith et al., 2022).
The insights generated from the discussion groups reported in this paper raise numerous considerations about the complex natures of systems in relation to person-centeredness, but the number of participants and organizations they represent were limited; thus, there was much convergence of opinions and perspectives, but the limited number of sessions precluded certainty of data saturation, and so the insights are meant to promote further dialogue and research. Importantly, the discussions identified issues especially relevant to long-term care for older adults, and may be applied to better consider how to meet individual residents’ needs and preferences within the resource limitations that exist in such systems. Furthermore, the insights have implications for policymaking and creating training guidelines for care staff, so that person-centeredness may be more effectively integrated into the way that both residents and staff are approached. Much additional research is needed, including a greater variety of perspectives relevant to the topic to provide additional insights into the systemic components of person-centeredness, and how they might be addressed to further person-centeredness in healthcare and long-term care.
Footnotes
Acknowledgments
The authors thank the meeting participants, including Alice Bonner PhD, RN; Eric Carlson, JD; Tony Chicotel, JD, MPP; David Grabowski, PhD; Chris Herman, MSW, LCSW; Tamara Konetzka PhD; Arif Nazir, MD; Robyn Stone, DrPH; Kim Strom, PhD; Gina Zimmermann, MPS; members of the Dementia Care Provider Roundtable; participants of the Center for Innovation 2023 annual conference; and staff of a senior living community in Maryland.
Ethical Considerations
The information presented in this paper was compiled from recorded group meetings rather than a systematic investigation, and so did not meet the Code of Federal Regulations (CFR) definition of research; therefore, IRB approval was not required.
Author Contributions
All authors made a significant contribution to the concept of the paper; participated in drafting the article or revised it critically for important intellectual content; approved the final version of the article for publication; and agreed to be accountable for all aspects of the work and resolve any issues related to its accuracy or integrity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging of the National Institutes of Health under Award Number T35AG038047 and R24AG065185. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
The information presented in this paper was compiled from recorded group meetings rather than a systematic investigation, and so did not meet the Code of Federal Regulations (CFR) definition of research; therefore, IRB approval was not required.