
Abstract
Use of technology is widespread in healthcare, and although much has been written about innovative technology in support of older adults, little research focuses on whether technology facilitates person-centeredness—the ability to serve individuals’ interest, values, goals, and needs. Using person-centeredness as a framework, we solicited input regarding technology’s potential to maximize quality of life based on discussions with care providers and experts in technology design and aging-related healthcare. Discussion identified that technology can facilitate or impede person-centeredness depending on its adaptability and implementation. Further, co-design with older adults, caregivers, family members, and clinicians is considered critical to eliciting person-centered goals from the end-user, meaning that technology designers should involve these groups in all phases of design. Importantly, it was also noted that inequity in access based on income, location, and race/ethnicity prevents technology from reaching many older adults; therefore, person-centeredness in technology must address this issue.
• An overview of whether, when, and how technology for older adults is person-centered. • Application of co-design principles to technology for older adults to ensure that products are person-centered. • How issues of access prevent technology from being person-centered for a significant proportion of the older adult population.
• Nursing homes, assisted living communities, and other environments that care for older adults should thoughtfully consider staff training before implementing a new technology for the care of older adults. • Further research on how health technology assessments can prioritize person-centered technology is warranted. • Government should be attentive to older adults who are without broadband access and work to increase access and provide skills training on technology and its potential to enrich their lives.What this paper adds to existing literature
Applications of study findings to gerontological practice, policy, and/or research
Introduction
Technology has transformed the healthcare industry over the last half-century. Advancements such as ventilators, dialysis machines, magnetic resonance imaging scanners, artificial heart valves, and implanted defibrillators have directly improved the diagnosis, treatment, and prognoses of many illnesses (Thimbleby, 2013). Communication and record-keeping have become computerized; use of electronic medical records (EMRs) and decision support tools has become widespread (Morris et al., 2021); and medical informatics has emerged as an entirely new field (Evans, 2016). Indeed, technology has had immeasurable impact on healthcare, with a net public health benefit.
Use of technology in healthcare is not, however, without its drawbacks. One example is the widespread introduction and use of EMR systems, which has increased administrative burden placed on healthcare professionals, contributed to physician burnout (Kroth et al., 2019), and raised security concerns for patients (Basil et al., 2022)), all with only limited demonstration of improvement in care quality (Graber et al., 2017).
Of particular concern is whether technology can meet individualized goals and provide true person-centered support to individuals, or whether it detracts from person-centeredness. Increasingly, technology is being used to supplement and at times to replace personal contact in care settings—a situation that poses significant risk of reducing person-centeredness by eliminating the one-on-one interaction upon which person-centeredness depends (Dyb et al., 2021). Examples include robots for socialization (Trainum et al., 2023) and safety devices that use cameras and artificial intelligence systems to identify falls (Potter et al., 2016; Zimmerman, Xiong, & Netscher, 2024). Furthermore, new technologies tend to be disseminated when they automate repetitive tasks and lower production costs, a process that requires standardization and mass production, which means that technologies that standardize will always receive more investment and attention than those that provide customized attention to a given person (Thimbleby, 2013).
The scientific literature, while replete with studies about innovative technologies, has rarely examined them using a lens of person-centeredness, which emphasizes how the technology serves an individual’s interests, values, goals of care, and needs (American Geriatrics Society, 2016). Therefore, it is worth evaluating whether and to what extent new technologies enhance or inhibit person-centeredness, and whether they are being implemented in ways that promote person-centered care and a person-centered lifestyle for persons residing in independent living settings and those in long-term care.
Therefore, to better understand the relationship between technology and person-centeredness in care of older persons, we conducted two on-site discussion with providers of dementia and long-term care services for older adults, and two virtual meetings with experts in the field. Drawing from these sources, this special article discusses the ability of technology to both facilitate and limit person-centeredness and provides suggestions for how technology should be designed by engineers, implemented by organizations, and used by individuals to maximize its person-centeredness.
For this special article, technology is defined as any digital or physical tool that is used in care settings for persons who are older or disabled; that is not routinely used in daily life outside of care settings; and that requires special skills to implement. A book, for example, is technically a tool but does not meet this definition because it requires no special skills to utilize. On the other hand, an “app” (i.e., computer application) used to communicate care issues between caregivers meets this definition because it is digital and its use requires specialized understanding and training.
Participants in one on-site discussion group involved two interviews with 12 staff from a continuing-care retirement community, to elicit opinions about technology designed for care of older adults; participants included a nurse, two resident assistants, four dining staff, and five medical technicians. The second on-site discussion group was conducted at the Alzheimer’s Association Dementia Care Provider Roundtable, with 30 individuals representing a range of settings including assisted living, nursing homes, and home and community-based services; participants included certified nursing assistants, nursing directors, and directors of both for-profit and not-for-profit settings.
In addition, we conducted two 90- to 120-minute virtual discussion groups with diverse experts with experience in technology design and evaluation for older persons, and in aging-related health and function. Members were selected by a combination of literature searches and networking, so as to include individuals from diverse locations with a variety of perspectives. Participants included four principals in technology companies that featured products targeted toward seniors, three researchers/academics, and two advocates working in areas related to improving care and equity for older persons.
The first group included: • the state chair of a non-profit advocacy organization for long-term care residents; • a nursing professor with extensive experience in practice and research in long-term care; • a leading scientist devoted to healthcare technology research and evaluation; and • the principal in a company that developed and is marketing a technology platform for persons with dementia.
The second group included: • the principal of a company distributing an electronic device to detect falls; • a staff member from an advocacy organization working for digital equity; • the founder of an electronic engagement platform for older adults; • the co-founder of a music platform for personalized engagement of older adults; and • a gerontologist/health services researcher who promotes and evaluates new technologies for older adults.
The meeting facilitator provided general questions for discussion, but the questions did not restrict the discussion. The introduction noted many uses of technology, such as related to safety and security, social communication, care and support, social engagement, work-related communication, and artificial intelligence. Discussion addressed technologies that were considered especially person-centered (and not person-centered) in any of these areas; whether there were limits or guidance as to how technology should be used in relation to person-centeredness, and solicited suggestions regarding areas where novel technologies would be especially beneficial.
Discussion identified four key issues related to technology in the context of person-centeredness: technology can both facilitate and impede person-centeredness; all stages of technology development should incorporate potential users; advanced design and implementation planning should focus on ease of use and adoption; and implementation in a manner that reduces racial, geographic, and income-related disparities is an ongoing challenge. Each issue is discussed below, with representative quotes for illustration.
Technology Can Both Facilitate and Impede Person-Centeredness
To be person-centered, technology must be a “tool that can bring engagement or make life easier or more successful.” In so doing, a person-centered technology should enable older adults to achieve goals that they have set for their lives, including goals such as extending life, optimizing function and experiences, or symptom relief. Furthermore, principles of engagement, adaptability, and meeting the individual’s needs must be met for a technology to be person-centered.
Participants reported that many widely used technologies have limited potential to be person-centered, especially when they are difficult to implement in a person-centered manner, are not adaptable, or offer limited options for use. For example, care planning templates that provide limited choices are not person-centered when their inherent rigidity impairs the user’s best effort to match the output to the user’s needs. Furthermore, it was felt that to be person-centered, technology requires personal interaction, and so many technologies have limited potential to be person-centered. As one participant noted “A content platform in and of itself doesn’t know who it’s delivering content to. It’s up to the person using the platform to ‘person-center’ it… (and it) has to be (made) person-centered by some other person making sure that the right content or the right application or solution is getting to the right person.”
One nuance of this issue is whether technology must be used by the individual it is serving or whether enhancing caregiver function can be considered in the context of person-centeredness. Some participants felt that if a technology focused on improving caregiving workflow, it was not person-centered because the older adult is not engaged or having their needs met by this utilization. On the other hand, some argued that when a technology increases a caregiver’s efficiency, it allows the caregiver more time to engage directly with the older adult on a human level, thereby making the technology inherently person-centered.
In this context, some technology used by caregivers can indirectly promote an older person’s autonomy. For example, security technologies such as automatic stove turn-offs, tracking devices, and surveillance cameras, when used by family caregivers who live elsewhere, have the potential to promote autonomy and aging in place. Consider an older woman who lives alone and is increasingly forgetful. Her son, who lives in another city, worries about his mother’s safety if she continues living alone. In this scenario, devices that permit the son to monitor his mother, lock her door, and turn off her stove from his cellular phone “prolong the time that seniors can age in place, which is often considered the gold standard for autonomy.” However, from another vantage point, such devices can be viewed as intrusive and therefore as interfering with autonomy.
Designing Technologies in a Person-Centered Manner Requires Participation of Potential Users, Including, as Appropriate, Older Adults, Caregivers, and Clinicians in Every Stage of Development
Participants noted that technology is often designed without direct user involvement. They emphasized that disconnects often develop between the intentions of the engineers who design technology and their target populations. Therefore, from the earliest stages of target use identification and prototype development, designers of new and/or modified products should involve potential users (older adults, clinicians, and caregivers, as appropriate), because that involvement will help identify needs to address and anticipate problems in usability and implementation.
A case in point is the fact that many technologies are created out of curiosity without clarity on the problem and/or users to target. In such situations, the driving force behind product development is the developers’ personal belief in the “rightness” of the idea. This process results in a technology being developed and then going “in search of users,” rather than identifying a problem first and designing technology to fill the existing need. One participant described it thusly: “I’ve got one hell of a hammer. Now, where’s the nail that’s going to be right to fit?”
The solution to this potential mismatch is to engage older adults, and as appropriate their caregivers and clinicians, from the beginning. This process of involving intended users at all stages of product development assures that the focus of the process will be end-user goals and needs, which can vary across individuals and frequently diverge markedly from the often-naïve opinions of the engineers who are designing the product. As one participant noted, “Technology often assumes that everyone wants to be on the wellness or optimal health path, which may not be in the person’s goals. Not enough time is spent on the front side of tech development thinking about whether a person wants it or not.”
Particularly valuable, according to several participants, are interdisciplinary teams that include all potentially relevant users as well as developers. Such groups are better able to focus on a meaningful problem which if addressed by an innovative technology could significantly improve care or quality of life, and on designing the product that will be useful to and accepted by target users. This process itself is person-centered because it is “centered on the real person and their real goals and their real needs in a practical, operational way.”
The last stage of development is evaluation of the technology. Overwhelming, participants strongly felt that outcome measurement must focus on the outcomes related to the person’s experience. Specifically, “Outcomes have to be patient-centered outcomes such as patient surveys, prompts, patient activation measure...the qualitative part brings in the patient’s perspectives.” In response, another panelist noted that there is little incentive in measuring these outcomes because “the person’s experience as an outcome is not what gets paid and it’s not (considered) the return on investment that matters to people who are writing the checks for the technology.” This discussion highlights a critical obstacle to ensuring person-centered outcome measures are used for evaluating technology; they are often not tied to financial return.
In Advanced Design and Implementation Planning, Ease of Use and Adoption of a New Technology Should Be at the Forefront
In older adult populations, adoption and use of technological innovations is often lower than in the general population. Products with a steep learning curve are often accompanied by user frustration, leading to abandonment of the technology without exploring its potential to improve the individual’s life. One participant noted that many older adults prefer using tablets with styluses over smart phones because the tablet and stylus mimics the pen and paper model with which they are already familiar; relatedly, uptake of tablet-based technologies tends to be greater than that of smartphone-based products. Insights such as these help developers design products away from general, often youth-focused, models, to better target the older adult population.
Ease of use is also important in design of products for caregivers in home and long-term care settings. These individuals often juggle numerous tasks and demands, so they are unable to invest a large amount of time in learning or using a new technology. Therefore, ease of access, simplicity of use, and modest training needs are important for adoption. One participant said this about a technology that he believed had exciting potential: “A lot of people were just afraid to take on a new task because they were overloaded. Training (on the technology) is investment of time even though, if the tech is done right, it should save you time and give you all kinds of benefits.” Therefore, even if a technology were to markedly improve staff’s ability to care, its potential would not be realized unless it fits readily into work flow, is easy to learn, and is easy to use.
Early interest from users is critical to adoption of a new technology, which depends on the product being easy to learn and perceived as helpful; these outcomes can be promoted by including end-users in all stages of the design process. Clinicians should also be involved, as they play a crucial leadership role in care settings. As one participant said: “(A) tech may look great in theory but in reality it doesn’t work, because there is no buy-in from clinicians”—illustrating that more than one user is often needed for a technology to be adopted.
Indeed, how the technology is received by the intended user is thought to be the crux of its ability to fulfill the goal of achieving person-centeredness. Older adults need to feel empowered to use the technology in a way that enhances their life, and staff and clinicians need to be able to train quickly and perceive that the technology will add value, not burden, to their work. In terms of reception from caregivers, technology should supplement the personal relationship, not replace it. If technology can aid completion of simple caregiver tasks, it can free time for staff to address more complex needs, including meaningful interactions with the older person.
Implementation of New Technologies in a Manner That Reduces Racial, Geographic, and Income-Related Disparities Is an Ongoing Challenge
Repeatedly, the concept of equity arose when implementation was discussed by participants, particularly around long-term care settings. They noted marked differences in resources and infrastructure among care settings, ranging from resource-poor rural or inner-city settings to highly resourced, private pay-dominant, often suburban settings. This wide range of resource availability by geography and payment sources was known to be associated with disparities along racial lines, with Black and other minority older persons often being concentrated in a few low-resourced settings.
As such, the range of settings where target users live must be considered in technology implementation. For example, a participant who has experience working with resource-poor nursing homes and assisted living communities stated that many high-tech “solutions” are simply not possible in communities that are already struggling to carry out basic tasks: “The things I’ve seen in assisted living don’t come close to the solutions [other panelists] talked about. For example, these facilities don’t even have a license for Music and Memory, so staff try to replicate it in other ways.”
A related issue is that, although the world is increasingly dependent on the internet, many residents and staff in home and long-term care settings remain cut off from reliable Wi-Fi access, either entirely or having it available only in certain areas such as an office and day room but not bedrooms. Participants agreed that Wi-Fi access remains a principal issue and is key to bringing rural and “lower-end” urban settings into the modern era, where they can reap the benefits of new technologies. Otherwise, technology will only reach the wealthier communities and further exacerbate disparities.
There are multiple strategies to increase digital access, but equity is dependent on public policy. As one participant commented, “as much as private sector and large companies and wonderful startups or smaller companies have done, high quality internet access is still a public policy issue.” To that end, some panelists suggested municipal Wi-Fi programs and/or pressuring departments on aging to prioritize digital access for older adults.
A widespread problem, particularly with data-driven technology, is that many long-term care communities do not have sufficient staff to utilize data generated by electronic systems. In such settings, implementing technology into a system that cannot act on it will have no net benefit and may instead strain limited human resources. Comments about this issue include “if there is no caregiver support to address needs identified from the technology to improve health, there is no net benefit” and “we need to get people available to act on tech.”
From an equity perspective, simple devices are often more person-centered because they are easier to distribute widely. For example, an inexpensive handheld speech amplification device, such as can be purchased at an electronics store, if made available for use by any visitor who enters a long-term care community, may well improve interaction better than more sophisticated devices such as hearing aids. Thus, a focus on simple technologies might improve person-centeredness both at the individual and the community level, thereby reducing disparities based on income and resources.
Conclusions and Implications for Practice, Policy, and Research
Consideration of the insights from discussion groups on the interface between technology and person-centeredness identified both challenges and opportunities. A key observation of these discussions is that technology can serve as either a barrier or facilitator of person-centeredness depending on what it does and how it is used. Other observations focus on conceptualization, development, roll-out, and application, stressing that this continuum must involve older adults, direct care staff, clinicians, and—if appropriate—families. If done properly, resulting innovations are more likely to be person-centered and more easily adopted into the busy routine of care provision. A final observation involved consideration of the possibility that technology may promote care disparities, as resources are needed to adopt and maintain most innovations; therefore, policy makers and regulators must both encourage development of simple, inexpensive solutions to problems and foster their dissemination into low-resourced settings. The literature supports all four of these observations.
Involving Users in Design
Figure 1 provides a simple framework to engage populations in the design process from brainstorming to evaluation; the emphasis is the continued inclusion of users in all stages of the design process. However, people working in technology development often lack awareness and guidance on how to achieve input, and more specifically, on how to ensure that development itself is conducted in a person-centered manner. The American Geriatrics Society defines person-centeredness as occurring when the “individual’s values and preferences are elicited and, once expressed, guide all aspects of their health care, supporting their realistic health and life goals” (American Geriatrics Society, 2016). Following this dictum in the design process can help achieve the goals in development and dissemination of new technologies. Some technology designers are already following this principle; for example, designers of an innovation for ophthalmology care—the field of medicine with the highest proportion of patients aged 65 and older (American Association of Retired Persons, 2021)—visited hospitals and studied the workflow to assure that a new design facilitated the needs of the end-users (Rezhepp, 2022). Similarly, such principles can be applied to design of technology for older adults, if designers meet with older adults, family members, caregivers, and clinicians to ascertain needs and wants. Furthermore, engaging users in the evaluation process is one solution to designing value-based measurements that ensure that technology is actually augmenting the lives of older adults. Framework for Engaging Older Adults, Family Members, Staff Caregivers, and Clinicians in the Design of Technology to Promote Person-Centeredness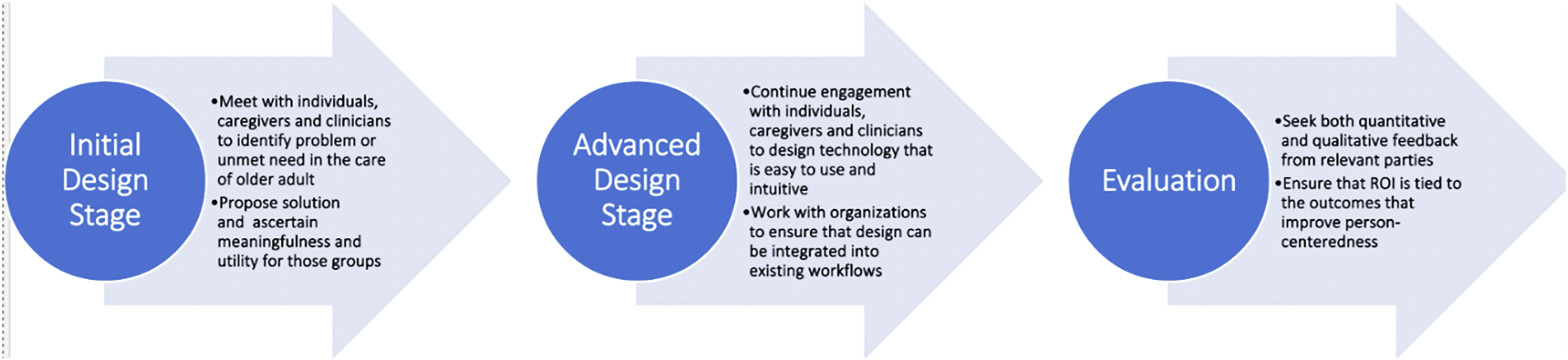
The heterogeneity of older persons is another reason that knowing the target user is crucial. For example, walking aides such as canes and walkers reduce falls in cognitively intact individuals but increase the risk in persons with cognitive impairment, most likely because of overload from the cognitive demands of the devices combined with increase in confidence and therefore in adventurousness (Pellfolk et al., 2009), highlighting the need to consider subpopulations and specific impairments rather than expecting one-size-fits-all solutions. An additional issue is that goals of living and care vary among older persons. One participant emphasized that technology developers often assume that everyone is on a path to improvement or well-being, whereas there are three trajectories of health or well-being—recovery/improvement, maintenance, or decline (Godfrey & Townsend, 2008; Murray et al., 2005). People designing technologies are advised to recognize needs in these three areas and be adaptable to these varying goals based on the user desires.
Challenges to broader inclusion are that expanded, group processes add cost and time. Therefore, companies, designers, and investors need to be convinced of the value of collaborative design processes, and so promoting established principle of good design referred to as co-design (Ollevier et al., 2020)—which asserts that older adults have a more positive view of technology if they are engaged in the design process and if they participate in training that is suited to their needs—could bridge this gap. Applying co-design to seniors is relatively new, so further study is warranted on barriers in this population, as well as its facilitators and impacts (Sumner et al., 2021).
Return on Investment and Value-Based Measures
Another major issue identified by participants is that technology designers tend to focus more on making money and reinvesting it rather than serving the needs of users (Thimbleby, 2013). A relevant parallel is that healthcare payments continue to be determined mostly by a fee-for-service model rather than a value-based model (Ray & Kusumoto, 2016). There is growing awareness that pure economics is not adequate to evaluate health technology, and value-based evaluations are beginning to be considered (Angelis & Kanavos, 2016). However, developing person-centered quality measures is challenging for many reasons, including difficulty establishing causal links between a specific technology and a given health outcome (McGlynn & Asch, 1998), and designing research that overcomes methodologic complexities in the heterogeneous older adult population (Brownie & Nancarrow, 2013). However, developing person-centered quality measures relevant to the goals of older adults represents an opportunity to standardize the process of designing and evaluating technology.
Not all types of technology are regulated to the same extent, and so health-related devices that undergo more rigorous evaluation can be a fruitful starting point for discussion about evaluation metrics. Often, however, health technologies are vaguely defined, such as by the European commission which defines health technology as “medicinal products, medical equipment for diagnostic and treatment, prevention methods” (European Commission, 2024). Thus, one step toward better measurement would be for health technology regulators to develop a framework to define and assess the value of health technology by (1) defining measures that can assess health benefits for patients, (2) developing scientific guidance for industry, and (3) promoting health insurance coverage of health technology (Henshall et al., 2013).
A major problem in the United States is that there is no single agency that acts as a health technology assessment organization; currently, momentum is building again for federal agencies to take charge of health technology assessment, rather than private sector evaluators (Luce & Cohen, 2009), which increases opportunity for including value-based measurements in the evaluation of technology designed for older adults. The Centers for Medicare and Medicaid Services (CMS), some argue, has taken on this role unofficially, such as by creating evidence requirements for coverage of medical devices; although this fragmentation of authority presents a challenge that reflects the fragmented healthcare system in the United States, suggestions have been provided to better ensure that CMS is able to meet its new role (Neumann & Tunis, 2023).
Interaction Between Care Providers and Technology
Another consideration noted by participants is understanding how caregivers will interact with a new technology and how the technology will alter or enhance the relationship between the older adult and the caregiver. Often family and staff caregivers welcome the help afforded by technology (Gibson et al., 2015), but some worry that their human relationships will be replaced by technology (Olesen et al., 2023).
Reinforcing the perspective of the discussion group members, a review of 46 studies found that staff training is often inadequate in the roll-out of new technologies, which may be a factor in the mixed evidence regarding whether health technology implementation increased staff productivity, as well as the lack of evidence that technology implementation improves quality of care or health outcomes (Ko et al., 2018). This issue is particularly critical because staff are regularly overburdened by work demands, and so technology must improve outcomes and not increase staff burden if it is to be valuable; one such technology is passive lighting systems to reduce falls among long-term care residents, which do not require staff involvement (Zimmerman, Sloane, et al., 2024).
Another consideration noted by our participants is how a new technology will affect relationships between older adults and caregivers. Theoretically, involving technology to aid in basic needs should free staff to spend more time developing strong relationships, but this assumption has often not been borne out in reality (Corbyn, 2021). Therefore, careful consideration of technology’s impact on this core relationship should be at the forefront of research and product evaluation and roll-out, and reassurance may be required—such as reflected in a study wherein nurses assumed a new technology would deteriorate their relationship with patients, whereas they found that it actually enhanced their relationship (Olesen et al., 2023).
Making Technology More Equitable
Another key area of concern for virtually all participants was whether technology can be person-centered for all older adults given equity issues, because without equity of access and use, technology cannot achieve the goal of being person-centered. Thus, the fact that technology is inaccessible to seniors and caregivers in settings that are low-resourced and/or disadvantaged by geography, race, or income is an equity issue. Currently, 42% of Americans over 65 do not have wired broadband connection compared to 27% of adults aged 18–64 (American Association of Retired Persons, 2021). In addition to age, strong predictors of low internet adaptivity include education less than a high school degree, income less than $25,000, Black and Latino race, poor health, female gender, and residence in rural area (American Association of Retired Persons, 2021). It is critical, therefore, to consider these as well as cost-related factors to make technology use more equitable for older adults and the communities in which they live (American Association of Retired Persons, 2021).
The Broadband, Equity, Access and Deployment (BEAD) Program—signed into law in November 2021—will provide funding to states to expand internet access and technology education (de Wit, 2023). In implementing this program, state agencies should ensure that older adults are targeted for internet connectivity by focusing on the areas that have high rates of age-based disparities in internet availability. Further, merely increasing internet access is not sufficient, because while many seniors are open to and actively engaging with technology, others are hesitant—for example, only 61% of older adults over 65 own a smartphone compared to 85% of the general population (Pew Research Center, 2021). The fact older adults who embraced technology during the COVID-19 pandemic felt less isolated and maintained social connections compared to those who did not (Zapletal et al., 2023) illustrates the importance of technology outreach, promotion, and education to older adults (American Association of Retired Persons, 2021).
In sum, the insights from the discussion groups highlight the need for technology to be designed and made available in ways that support the mission of achieving person-centered goals of care and lifestyle for older adults. Technology design needs to involve users and recognize unique needs that vary between subpopulations of older adults; it should complement and supplement care relationships without diminishing them; and systemic problems that discourage person-centered technology must be overcome (e.g., fee-for-service payment model, the digital divide, and lack of support for staff training on new technologies). Policy changes encouraging digital equity and health technology assessment show the most promise in changing the landscape into one with a person-centered focus. Concurrent with policy changes, technology designers are advised to focus on simple devices that do not require internet access, are easy to learn to implement, and involve users throughout the design process. As such, there are many opportunities to shift focus to person-centered technology, if public policy and private companies follow suit.
Footnotes
Acknowledgements
The authors thank the meeting participants, including Peter Chamberlain, SM, Kari Gray, Juliet Holt Klinger, MA, Bill Lamb, MSW, MPA, David Lindeman, PhD, Jeff McSpadden, Marilyn Rantz, PhD, RN, Ronen Rozenblum, PhD, MPH, Jack York, members of the Dementia Care Provider Roundtable, participants of the Center for Innovation 2023 annual conference, and staff of a senior living community.
Ethical Considerations
The information presented in this paper was compiled from recorded group meetings rather than a systematic investigation, and so did not meet the Code of Federal Regulations (CFR) definition of research; therefore, IRB approval was not required.
Author Contributions
All authors made a significant contribution to the concept of the paper; participated in drafting the article or revised it critically for important intellectual content; approved the final version of the article for publication; and agreed to be accountable for all aspects of the work and resolve any issues related to its accuracy or integrity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging of the National Institutes of Health under Award Numbers T35AG038047 and R24AG065185. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.