
Abstract
Sleep disturbances create adverse cognitive and health outcomes for people living with dementia (PLwD). Approximately 19% to 44% of PLwD in the community experience sleep disturbances, but to date, no systematic review has focused primarily on interventions developed for community-dwelling populations (Livingston et al., 2024; Koren et al., 2023; Wong & Lovier, 2023). This systematic review builds on a Cochrane Systematic Review (Wilfling et al., 2023) that evaluated all non-pharmacological interventions to help address poor sleep in PLwD. The current review builds on the Wilfling et al. (2023) review but focuses only on studies published from 2022 through 2024 and only RCT studies for community-dwelling PLwD experiencing sleep disturbances. Six studies met the inclusion criteria. Photo/light interventions and activity-based interventions had mixed outcomes, preventing any firm conclusions about effectiveness. Dyadic-based multi-component interventions may be effective for treating sleep in PLwD in the community.
Keywords
• The current review is the only identified systematic review that collects and evaluates non-pharmacological interventions specifically for community-dwelling PLwD experiencing sleep disturbances. • This systematic review provides an update to a Cochrane Review by Wilfling et al. (2023) to create a comprehensive collection of high-quality non-pharmacological interventions to treat sleep disturbances in community-dwelling PLwD.
• Sleep disturbances have an overall negative impact on PLwD and Caregivers. Therefore, providers working with this population need to assess the effects of sleep disturbances on the quality of life and burden of care for both the PLwD and the Caregivers. • This review highlights the need for future research to focus on replicating non-pharmacological interventions for addressing sleep disturbances in PLwD, utilizing similar methods and assessment tools.What This Paper Adds
Applications of Study Findings
Introduction
Globally, over 78 million people are projected to have a dementia diagnosis by 2030 (Shin, 2022). An estimated 25–38% of persons living with dementia (PLwD) experience poor sleep (Aryankhesal et al., 2024) with approximately 19%–44% being community-dwelling (Livingston et al., 2024; Koren et al., 2023; Wong & Lovier, 2023). Poor sleep, or sleep disturbances, are connected to the deterioration of dementia symptoms, increased caregiver burden (Cipriani et al., 2015; Gibson et al., 2014), increased risk of institutionalization (Wennberg et al., 2017; Cipriani et al., 2015; Benca et al., 2022), increased mortality risk (Beydoun et al., 2024; Cipriani et al., 2015), and poor Quality of Life (QoL) (Benca et al., 2022; Nikmat et al., 2015). Current research supports the effectiveness of non-pharmacological interventions (NPIs) for managing sleep disturbances in PLwD, as they carry a lower risk of adverse events compared to medications (Huong et al., 2024). No systematic review has specifically focused on NPIs for this community-dwelling population. Instead, most reviews combine intervention settings, making the identification of community interventions difficult. The goal of this systematic review is to address this gap in two ways. First, it will update a Cochrane Systematic Review by Wilfling et al. (2023), which evaluated NPIs for PLwD experiencing sleep disturbances, regardless of the setting. Second, this current review will focus on NPIs specifically for community-dwelling PLwD experiencing sleep disturbances.
Sleep Disturbances Among PLwD
Sleep disturbances are often categorized into three main groups: daytime napping, sleep disruptions, and sleep disorders (Wennberg et al., 2017; Sidani et al., 2022). Frequent daytime and long-duration napping are distinct types of sleep disorders that impact sleep by disrupting the sleep cycle and are associated with decreased cognitive functioning (Gibson et al., 2014; Kitamura et al., 2021; Liu et al., 2022). Sleep disruptions include delayed sleep onset, sleep fragmentation at night, nighttime wandering, nightmares, or nighttime behavioral problems (Gibson et al., 2014). These disruptive sleep behaviors are the most common in sleep research for PLwD and are most impactful for caregivers. The final group of sleep disturbances includes sleep disorders like obstructive sleep apnea, as well as illnesses that affect sleep, like chronic obstructive pulmonary disease (Wennberg et al., 2017; Gibson et al., 2014). Oxygen, CPAP, and BIPAP are used to treat sleep disorders by ensuring adequate air flow. The devices improve issues linked to sleep disorders, but the pressure generated by the machines can create sleep disturbances like delayed sleep or sleep fragmentation (Brown et al., 2024). No matter the category, all sleep disturbances increase the risk of adverse health outcomes for PLwD and Caregiver. For example, sleep disturbances are linked to cardiovascular disease, depression, anxiety, decrease in cognitive performance (Chaput et al., 2020), and increased risk of falls (Lach et al., 2017).
Impact of Sleep Disturbances Among PLwD
Sleep disturbances in PLwD increase the burden of care, which negatively impacts both the PLwD and caregiver quality of life (QoL) (Jing et al., 2016; Mao et al., 2025). Research has identified the risk of institutionalization and mortality risk increases as the burden of care for PLwD increases (Björkstedt et al., 2023; Brodaty et al., 2014; Luppa et al., 2008; Eska et al., 2013). Sleep disturbances may not directly increase the risks but can act as a mediating variable that increases risk. Recently, Beydoun et al. (2024) identified mortality for PLwD increased by 7% when sleep disturbances were present for PLwD.
Sleep disturbances can negatively impact caregivers. Informal caregivers of PLwD with sleep disturbances reported poor sleep quality and higher rates of sleep disturbances (Almutairi & Zauszniewski, 2022). Caregivers also reported an increase in anxiety, depression, and fatigue, which increased the perception of the burden of care (Almutairi & Zauszniewski, 2022; Gibson et al., 2023). In a qualitative study by Gibson et al. (2023), caregivers reported they wished they had prioritized sleep when providing care. However, the thematic feelings of being “on high alert day and night” and being “unsure of sleep” prevented them from sleeping added to their sense of anxiety and fatigue (Gibson et al., 2023, p. 1044). A mixed-method study by Yamaguchi et al. (2024) found that chronic stress caused by sleep disruptions physically changed the sleep patterns of caregivers and decreased their sleep quality. Overall, poor sleep by the caregiver and care recipients impacts the dyad by increasing the burden of care, which affects QoL, institutionalization, and risk of mortality. Caregivers who experience increased stress from sleep disruptions created by PLwD had higher risk of mortality over a 4-year period than non-caregivers (Cipriani et al., 2015).
Treating Sleep Disturbances
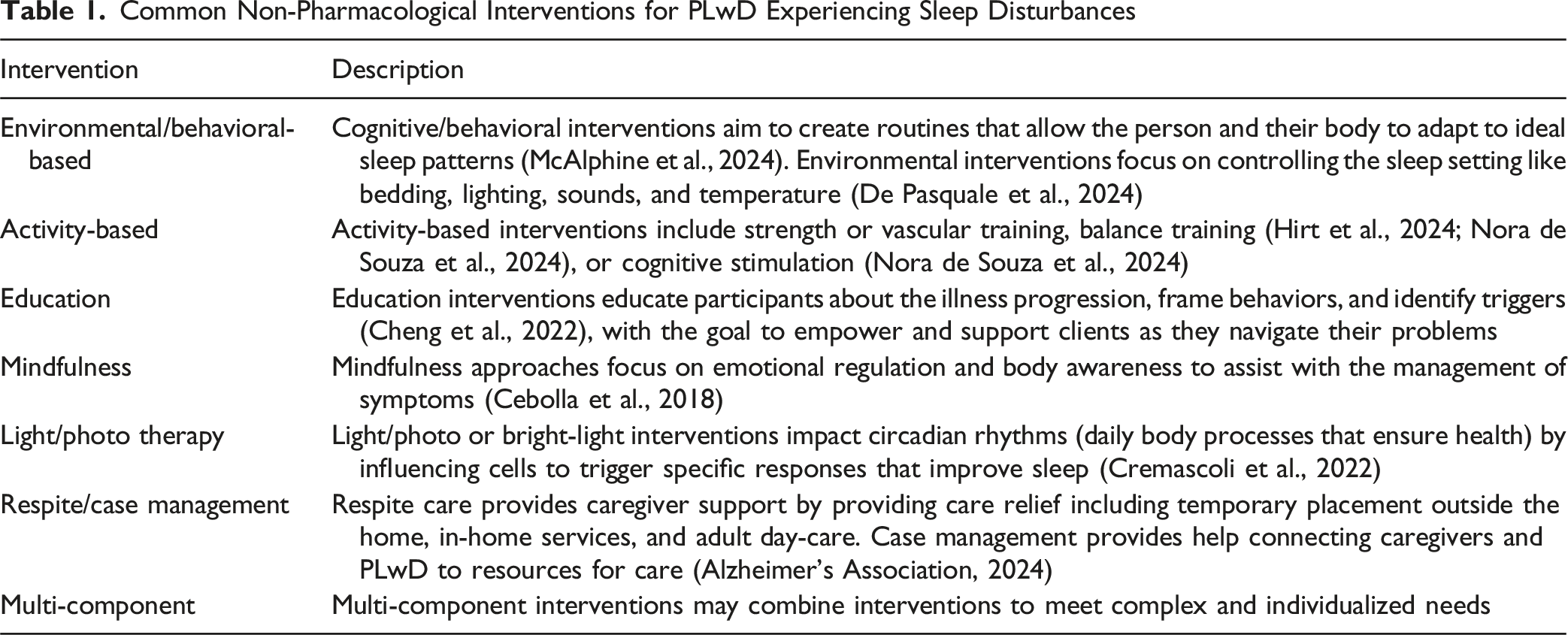
Common Non-Pharmacological Interventions for PLwD Experiencing Sleep Disturbances
Project Rationale and Aims
Research into NPIs for PLwD experiencing sleep disturbances has increased in recent years as researchers work develop alternatives to medications that carry a higher risk of adverse outcomes (Cipriani et al., 2015). NPIs have shown a positive effect on treatment; however, a gap in the literature exists between interventions developed with institutional-dwelling populations and with community-dwelling populations. Evidence-based practice indicates that the population demographics used to develop an intervention are an important consideration when selecting interventions for use (Stewart et al., 2018). Systematic reviews are excellent tools for intervention summary and evaluation, however, they may emphasis the methods and outcomes of interventions more than context and demographic information evidence-based providers need to select interventions (Munthe-Kaas et al., 2020; Tricco et al., 2016).
From 2020 to 2024, 24 systematic reviews were published that evaluated sleep interventions for PLwD, with 22 of these studies focusing on participants living in institutions or having little distinction between settings. One study stood out by the details provided about the review of interventions for PLWD in the community as well as institutional setting that allows readers to identify intervention setting. Wilfling et al. (2023) conducted a Cochrane Systematic Review of NPI for PLwD experiencing sleep disturbances. The reviewers provided separate, detailed analyses of each included study, as well as a combined analysis of the interventions. Building upon Wilfling et al. (2023), this review will replicate the exact search but focus on interventions for community-dwelling populations. The goal of this research is to collect and evaluate all interventions for sleep disturbances for PLwD in the community.
Methods
This systematic review addresses the population, intervention, comparison, and outcome (PICO) question: How effective are non-pharmacological interventions, compared to control groups, in improving sleep outcomes for persons living with dementia in the community who experience sleep disturbances? The current systematic review builds on the Cochrane Systematic Review by Wilfling et al. (2023) and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.
Search Strategy
Wilfling et al. (2023) conducted a systematic review of NPIs for PLwD experiencing sleep disturbances. Their most recent search concluded in January 2022 but did not have any date limitations. The current review is an update Wilfling et al. (2023) review in two ways: (1) It updates the studies published after January 2022 through October 2024 and (2) it focuses on community-based interventions only. Following the same search strategy as Wilfling et al. (2023), an updated search for NPI studies for PLwD experience sleep disturbances was conducted in October 2024 for all studies published after January 2022. Additionally, community-based studies in Wilfling et al. (2023) review were extracted and included in the current search to provide a comprehensive review of community-based interventions for PLwD experiencing sleep disturbances. The studies identified by Wilfling et al. (2023) dates ranged from 2005 to 2016.
Modifications to the present search included adding search terms (communit* OR House OR Home OR dyad) as limiters to help focus results on community-based studies (see Appendix A for full search terms). To ensure that the added search terms did not create a variance in methods from Wilfling et al. (2023), the authors conducted an initial search with no publication date limits to verify whether the search still identified the same articles. After confirming that search methods were consistent, the review team conducted the primary search. The search included the following databases: PsycINFO, CINAHL, Medline, Embase (OVIDSP), Web of Science, Central (Cochrane Library), ClinicalTrials.gov, and ICTRP. See Appendix A for a list of full search terms and databases used.
Criteria for Inclusion
Identified studies met inclusion if they met the PICO defined criteria: (1) any age person living with a diagnosis of dementia or subtype confirmed by a medical provider or medical records; (2) had a sleep problem at baseline based on any subjective measure; (3) more than 80% of participants had a dementia diagnosis; (4) featured a non-pharmacological sleep intervention to improve physiological sleep in PLWD; (5) had a comparator group; (6) primary sleep outcome measured by a standard objective measure (i.e., actigraphy, instrument/scale, repeated direct observation) or standard subjective measure (i.e., PSQI, CPSQI, and SDI); (7) in a community-based setting (i.e., home, apartment); and (8) study was RCT design.
Studies were excluded when: (1) subjective diagnosis of dementia or subjective/objective diagnosis of mild cognitive impairment; (2) no objective standard measure of sleep outcome; (3) sleep was not an intended primary outcome of the study; (4) intervention was institutionally based (i.e., person resides in a licensed care facility like nursing homes, assisted living, long term care home); (5) intervention outcome measured for impact on the caregiver; (6) no comparator group; (7) study was not RCT design; or (8) involved a medication-only intervention.
Study Selection
All studies were extracted into Endnote, linked with abstracts, grouped by data source, and then formatted for Excel. Once extracted into Excel, articles were deduplicated, and three authors were involved in title review, abstract review, and final article review for inclusion. All three authors discussed any disagreements about inclusion or exclusion until an agreement was reached.
Quality Assessment
The Cochrane Risk-of-Bias 2 (RoB2) tool for randomized trials was used to evaluate the quality of the studies risk of bias based on the Intent-to-Treat principle (Higgins et al., 2024). Cochrane recommends the tool to evaluate the risk of bias from randomization, deviations from the intervention, missing outcome data, measurement of the outcome, and selection of the reported results. All three researchers independently evaluated the included studies to determine the risk of bias. All three authors discussed any disagreement until an agreement was reached. All studies that met inclusion criteria were included in this review regardless of risk of bias assessment outcome.
Data Extraction
Studies that met inclusion criteria were grouped in a standardized table, including (1) author(s) last name and date; (2) intervention setting; (3) description of the intervention; (4) study design; and (5) observed outcomes. Studies were additionally analyzed using the RoB2 Risk of Bias assessment tool recommended by Cochrane.
Results
The primary search identified 1,009 articles. After deduplication, title and abstract screening, 47 articles met for full-text review. Two articles met the inclusion criteria based on the updated search, and the other four were identified and extracted from Wilfling et al. (2023). A total of six articles met the inclusion criteria for this review. Studies that did not meet inclusion criteria did not meet due to a lack of a community setting, the study being unrelated to sleep, or a study design that was not a randomized controlled trial (RCT) (Figure 1). (PRISMA) Flow diagram for study selection. **All records were excluded by human reviewers. Figure 1. Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram for study selection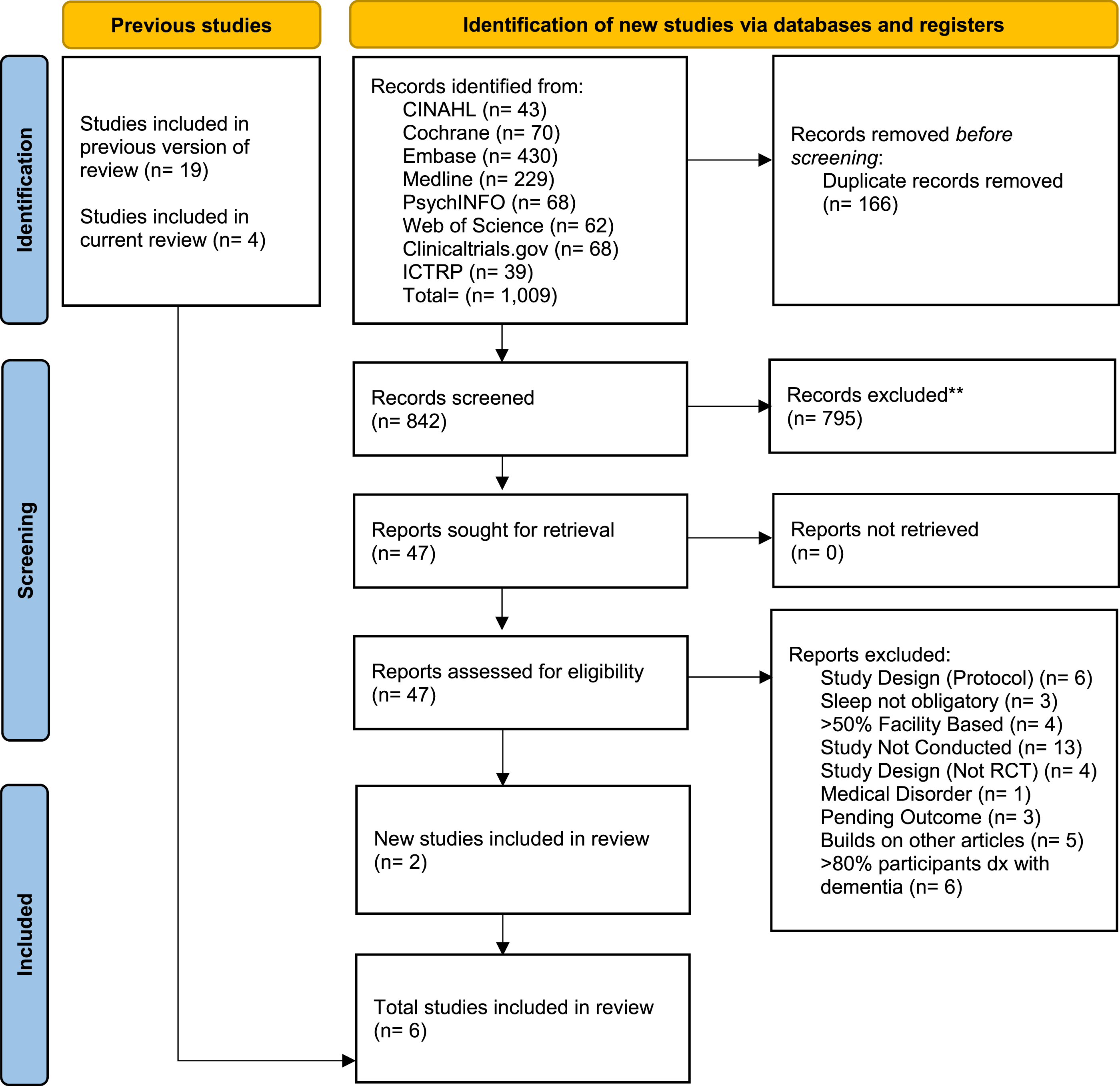
Participant Description
Overall, a total of 629 participants were included collectively for all studies before randomization; the average study sample size was 104.8 ± 140.1, with a range of participants from 15 (Lin et al., 2022) to 377 (Rapaport et al., 2024). Three studies were conducted in the US (McCurry et al., 2005, 2011; Sloane et al., 2015); one was conducted in China (Chan et al., 2016); one was conducted in the UK (Rapaport et al., 2024); and one was conducted in Taiwan (Lin et al., 2022). The study publication dates ranged from 2005 (McCurray et al., 2005) to 2024 (Rapaport et al., 2024). The average age in years for the treatment group was 79.8, ranging from 78.4 (Chan et al., 2016) to 82.2 (McCurry et al., 2011). An estimated 36.8% ± 17.8% of intervention participants were male, and 85.9% ± 6.7% were White/non-Hispanic. Two studies did not include information on race or ethnicity (Chan et al., 2016; Lin et al., 2022). The average age of the control group was 79.6, with a range of 77.3 (Lin et al., 2022) to 82.2 (Chan et al., 2016). An estimated 42.1% ± 12.1% of participants were male, and 81.8% ± 7.7% were white/non-Hispanic.
Study Design
Assessment of Included Studies
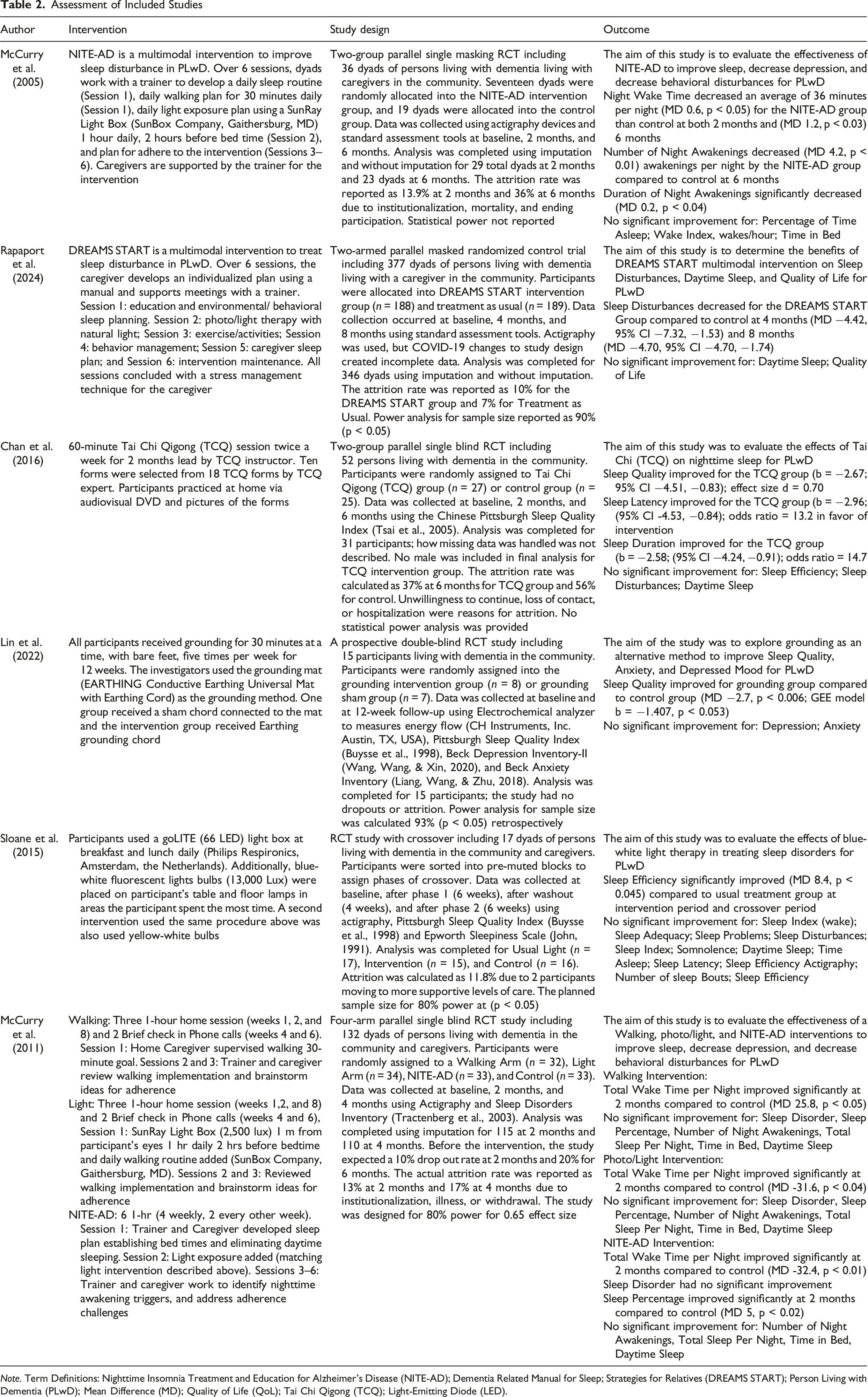
Note. Term Definitions: Nighttime Insomnia Treatment and Education for Alzheimer’s Disease (NITE-AD); Dementia Related Manual for Sleep; Strategies for Relatives (DREAMS START); Person Living with Dementia (PLwD); Mean Difference (MD); Quality of Life (QoL); Tai Chi Qigong (TCQ); Light-Emitting Diode (LED).
All studies used a Randomized Control Trial (RCT) design. The most common RCT design included a two- or three-arm parallel design with masking in which participants were not aware if they were assigned to intervention or treatment as usual group (Chan et al., 2016; McCurry et al., 2005, 2011; Rapaport et al., 2024). Only one study used double-blinding where researchers and participants were not aware of the intervention and control group (Lin et al., 2022), and one study used a crossover design which all participants received the intervention at either the first study period or the second (Sloane et al., 2015). Actigraphy was the primary data collection tool in three studies (McCurry et al., 2005, 2011; Sloane et al., 2015). One study planned to use actigraphy but was not able to ensure that the protocol was followed correctly, so the collected data were not reported (Rapaport et al., 2024). Only two studies did not attempt to use actigraphy as the primary objective data collection tool (Chan et al., 2016; Lin et al., 2022); these studies used a standard assessment tool completed by objective assessors.
All studies included a standard assessment tool either as a primary measure (Chan et al., 2016; Lin et al., 2022) or as a concurrent measure (McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015). The PSQI (Buysse et al., 1998) was the most common standard assessment tool (Chan et al., 2016; Lin et al., 2022; McCurry et al., 2005; Sloane et al., 2015), followed by the Epworth Sleepiness Scale (ESS) (Johns, 1991) used in three studies (McCurry et al., 2005; Rapaport et al., 2024; Sloane et al., 2015), and the SDI (Tractenberg et al., 2003) used in two studies (McCurry et al., 2011; Rapaport et al., 2024). All standard assessment tools reported good internal consistency, with an alpha coefficient greater than or equal to 0.69 and strong concurrent validity compared to Actigraphy measures (Spira et al., 2011; Beaudreau et al., 2012; Hjetland et al., 2020).
Interventions and Outcomes
Details about the interventions and outcomes are in Table 2. Interventions are grouped into three thematic categories for analysis: Photo/light interventions (McCurry et al., 2011; Sloane et al., 2015), activity-based interventions (Chan et al., 2016; Lin et al., 2022; McCurry et al., 2011), or multi-component interventions (McCurry et al., 2005, 2011; Rapaport et al., 2024). The goal for all studies was to test interventions aimed at improving sleep for community-dwelling PLwD experiencing sleep disturbances. Intervention implementation was structured differently depending on the study. Only four studies required active participation by caregivers in the intervention (McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015).
Photo/Light Interventions
Two studies tested photo/light interventions (McCurry et al., 2011; Sloane et al., 2015). Sloane et al. (2015) evaluated the effects of blue-white (13,000K) or yellow-white (2,700K) lamps installed around the home by a study coordinator. Participants used a goLITE P2 lightbox (Philips Respironics, Amsterdam, the Netherlands) for direct light exposure at breakfast and lunch. The intervention by McCurry et al. (2011) provided 2,500 Lux of direct photo/light exposure using a SunRay lightbox (SunBox Company, Gaithersburg, MD), 1 m from participants’ faces, for 1 hour daily, 2 hours before bed. The intervention team provided support for caregivers via three sessions. Caregivers developed plans to increase participant adherence to a daily routine that included 1 hour of use of the SunRay box (SunBox Company, Gaithersburg, MD).
Sloane et al. (2015) reported improvement in sleep efficiency during the first intervention period, with continued improvement through the crossover period, as measured by the PSQI, but not by actigraphy. No other measured categories of sleep reported improvement from the intervention. McCurry et al. (2011) reported a decrease in time awake per actigraphy at 2 months but not at 6 months and no improvement in any sleep categories according to subjective measures. No other measured categories of sleep reported improvement from the intervention. Overall, each study reported improvement in at least one domain of sleep measured, although not all. No concurrent agreement between measures within the studies confirmed outcome findings. Sloane et al. (2015) reported improvement with the PSQI, but concurrent actigraphy measures did not demonstrate improvement. McCurry et al. (2011) reported improvement according to actigraphy; however, the concurrent standard assessment tool did not identify improvement. Mixed results for photo/light Interventions are consistent with current research findings.
Activity-Based Interventions
Three studies reported the effects of activity-based interventions (Chan et al., 2016; Lin et al., 2022; McCurry et al., 2011) on sleep. In the study by Chan et al. (2016), participants were taught 10 modified Tai Chi forms to practice for 60 minutes twice a week over a period of 2 months by a master instructor-led Tai Chi session. Between sessions, participants were given video resources to practice at home on their own. Lin et al. (2022) studied an intervention that provided 30 minutes of chair-based grounding activities five times a week. The chairs were on grounding mats, connected by grounding wires. Grounding is the concept of energy transfer between the body and the Earth, which can enhance wellness. The study by McCurry et al. (2011) evaluated an activity-based intervention using a goal of 30 minutes walking daily. Support was provided to caregivers via three sessions to develop adherence plans and troubleshoot any issues.
Two activity-based interventions out of the three used a similar analysis approach. Both Chan et al. (2016) and Lin et al. (2022) employed the PSQI to measure outcomes and used regression analysis to analyze the findings. Chan et al. (2016) reported improvements in sleep quality, sleep latency, and sleep duration according to the Chinese Pittsburgh Sleep Quality Index (CPSQI) (Tsai et al., 2005); actigraphy measurements were not used. Lin et al. (2022) reported improved sleep quality at 12 weeks, as measured by the PSQI; however, actigraphy was not used. McCurry et al. (2011) reported that walking decreased time awake compared to the control group at 2 months, as measured by actigraphy, but not at 6 months. The concurrent SDI measure noted no improvements in sleep.
The activity-based interventions included two studies that did not require active participation by caregivers in the intervention (Chan et al., 2016; Lin et al., 2022). Rather than interventions taking place in the home, the Tai Chi (Chan et al., 2016) and Grounding (Lin et al., 2022) interventions required participants to attend sessions at a community location. Lin et al. (2022) and Chan et al. (2016) reported positive outcomes; however, Lin et al. (2022) used post-hoc power analysis to determine the effect, and Chan et al. (2016) reported a high attrition rate (37% for the intervention group and 56% for the control group). Both Lin et al. (2022) and Chan et al. (2016) also had small sample sizes of (n = 8) and (n = 17) completing the interventions, respectively. For generalizability, the studies by Chan et al. (2016) and Lin et al. (2022) may be limited.
Multi-Component Interventions
Three studies reported multi-component interventions (McCurry et al., 2005, 2011; Rapaport et al., 2024) that included environmental/ behavioral sleep routines, education, light exposure, caregiver support, and exercise, delivered through a progression of in-person sessions. McCurry et al. (2005) and later McCurry et al. (2011) implemented the intervention NITE-AD. NITE-AD provides education, training, and support for PLwD and Caregivers over a series of six sessions. The first session, led by a trainer, focuses on establishing sleep routines, identifies triggers that impact sleep, and starts a 30-minute daily walking program. Session two, led by a trainer, reviewed any issues that had developed from the previous session and implemented a daily photo/light intervention. The photo/light intervention uses 2,500 Lux of direct photo/light exposure, using a SunRay Lightbox (SunBox Company, Gaithersburg, MD) 1 m from the participants’ faces, for 1 hour daily, two hours before bedtime. Sessions 3–6, led by a trainer, followed up on the previous session to address adherence to treatment and barriers.
Rapaport et al. (2024) developed a multi-component manual-based intervention called DREAMS START. The program includes a six-session manual-based approach that helps caregivers, and PLwD develops individualized care plans for sleep. All sessions feature stress management activities and review discussions from earlier sessions. The first session included education about dementia, sleep, and plan development for environmental/ behavioral sleep routines. Session 2 included education and planning for natural light exposure and stress management. Session 3 developed a plan for the activity. Session 4 reviewed managing behavior problems. Session 5 reviewed and planned for caregiver sleep. Session six reviewed what is working and plans for future adherence to the individualized plan.
NITE-AD and DREAMS START interventions reported improved sleep for participants during the first measure period. The NITE-AD intervention (McCurry et al., 2005, 2011) reported a decrease in time awake at night per actigraphy at 2 months. McCurry et al. (2005) reported an improvement of 5% in sleep percentage at 2 months, a decrease in time awake at night of 42 minutes at 6 months, and a decrease in the number of night awakenings at 6 months. McCurry et al. (2011) did not report significance for any category at 6 months but did report improved sleep percentage and decreased wake time per night at 2 months. Neither McCurry et al. (2005) nor McCurry et al. (2011) reported improvement in the NITE-AD intervention for any sleep category based on the SDI standard assessment tool; all findings were based on actigraphy.
Rapaport et al. (2024) (DREAMS START) reported a significant decrease in sleep disturbances according to Sleep Disorder Inventory (SDI) at both 4 and 8 months but did not report actigraphy data due to concerns about the appropriateness of device utilization. Unlike McCurry et al. (2005) and McCurry et al. (2011), Rapaport et al. (2024) did not report subcategories of sleep disturbances for their measure, only the overall scores, making cross-comparison difficult. DREAMS START also reported no improvement in sleep for Epworth Sleepiness Scale (ESS), Neuropsychiatric Inventory, or Dementia Quality of Life (QoL) measures. Much like the photo/light Interventions, the two studies identified improvements in sleep but used separate measures and lacked concurrent validation based on multiple measures. Unique to this group of studies, the NITE-AD intervention reported replication of sleep improvement across two different studies of the same interventions. DREAMS START had the largest sample size (n = 377) with attrition rates for intervention and control group of 10% or less at any collection period, increasing the likelihood of generalizable findings.
Caregiver Satisfaction
Only four studies reported evaluated caregiver satisfaction with the intervention (McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015). Two studies used the Zarit Burden Interview (Zarit et al., 1980), which is a standardized assessment tool used to measure caregiver emotional, physical, and social well-being (Rapaport et al., 2024; Sloane et al., 2015), while two studies did not specify the assessment tool used (McCurry et al., 2005, 2011). Rapaport et al. (2024) and Sloane et al. (2015) reported low to moderate caregiver burden when implementing the intervention, but there was no statistical difference in scores between the intervention and control groups. These findings suggest that the interventions did not increase caregiver burden beyond that of the control condition. McCurry et al. (2005) and McCurry et al. (2011) both reported that caregivers would recommend the intervention program to friends, that they benefited from the program, and that the program added more burden compared to treatment as usual.
Risk of Bias Evaluation
Randomization
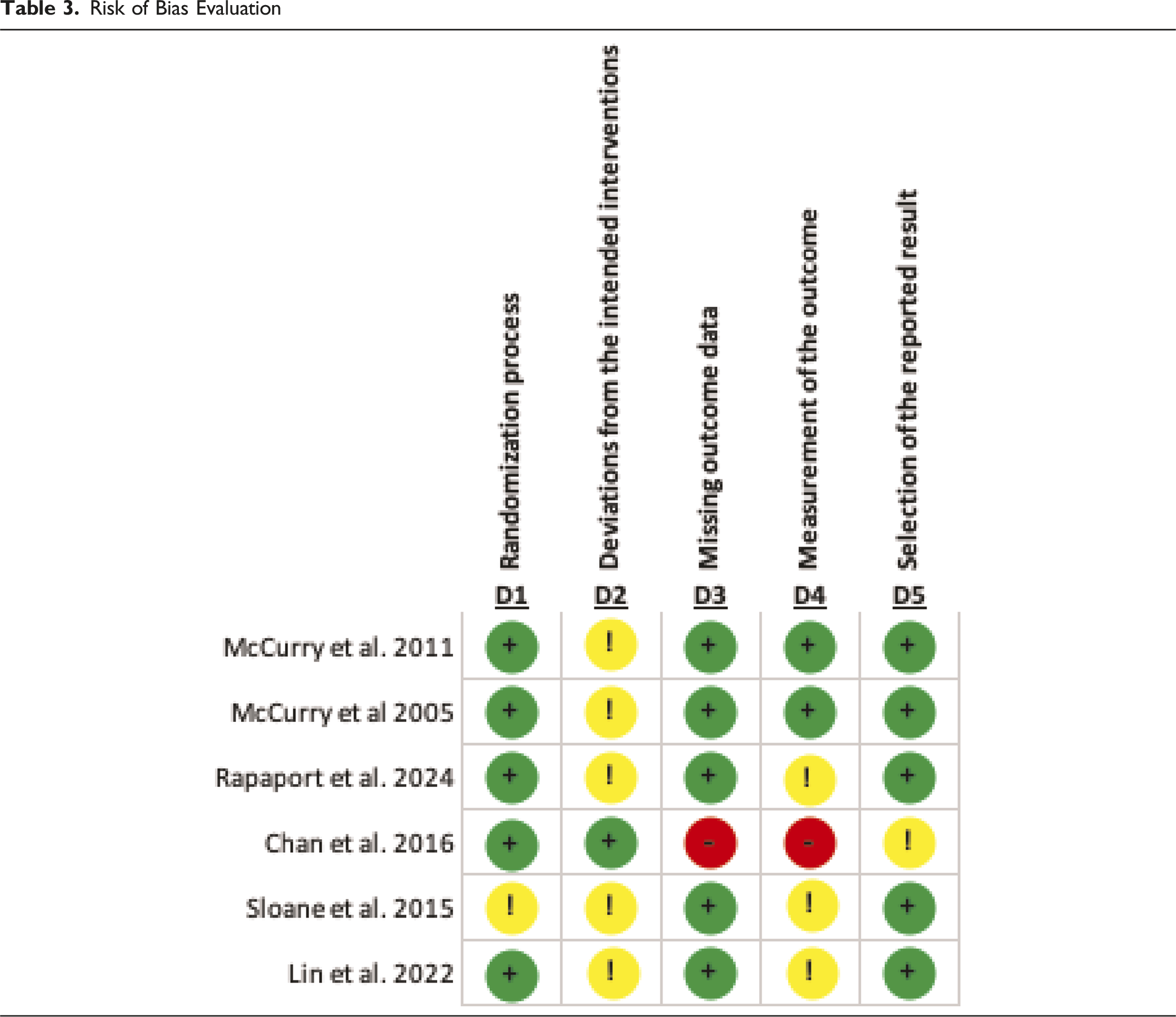
Risk of Bias Evaluation
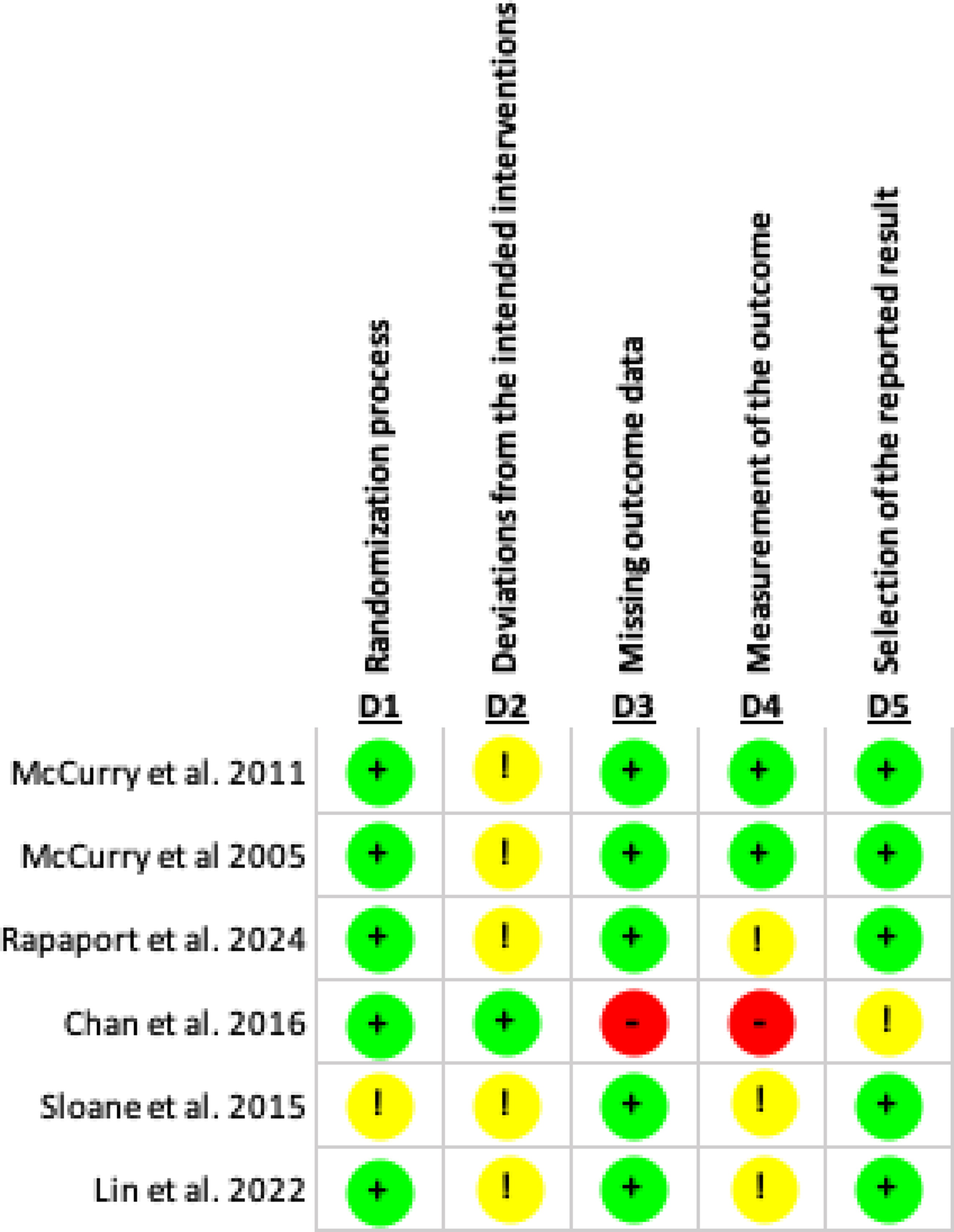
Deviations from the Intended Interventions
Five studies raised concerns for bias due to deviations from the intended interventions, and one study raised a low risk of bias. Chan et al. (2016) had a low risk of bias because the intervention design controlled for accidental exposure to the Tai Chi intervention, as participants were required to practice both at home and in the studio. All other studies raised concerns about bias because they carried a risk of additional uncontrolled exposure to the intervention outside the intended period (McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015). For example, the activity-based intervention that utilized Grounding (Lin et al., 2022) had little control over grounding that may occur outside of the intervention when participants walked around. Photo/light and multi-component interventions had no control over additional light exposure outside of the interventions (McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015). Two studies also had concerns for deviations due to study design. Rapaport et al. (2024) had to modify intervention delivery methods from in-person to remote due to COVID-19 pandemic restrictions. Sloane et al. (2015) used a crossover design, which creates some concern because both groups received treatment at different times.
Missing Outcome Data
Five studies had a low risk of bias due to missing outcome data, acknowledgment of attrition, and comparing calculations based on imputations with missing data (Lin et al., 2022; McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015). One study had a high risk of bias due to missing outcomes, as the attrition rate at the final data collection point (6 months) was high, resulting in a substantial amount of missing data (Chan et al., 2016). At the 6-month final collection period, the attrition rate was 56% for the control group and 27% for the intervention group.
Measuring the Outcome
Two studies had a low risk of bias because they measured the outcome using objective measures, such as actigraphy (McCurry et al., 2005, 2011). Three studies raised concerns about bias because the primary data collection used standard assessment tools administered by assessors but still introduced a risk of bias (Lin et al., 2022; Rapaport et al., 2024), or the crossover nature of the intervention introduced a risk of bias due to knowledge of when the intervention took place (Sloane et al., 2015). One study had a high risk of bias because the method of data collection used the PSQI by unmasked or blinded observers. Additionally, the study design for the control group introduced a high risk of error in unmasking because they would be aware that they were not undergoing Tai Chi training (Chan et al., 2016).
Selection of the Reported Result
Five studies have a low risk of bias in selecting reported information because they used the expected measures and analysis as designed (Lin et al., 2022; McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015). The most common analysis was the mean difference (McCurry et al., 2005, 2011; Rapaport et al., 2024; Sloane et al., 2015), followed by generalized estimating equations (GEE) regression analysis (Chan et al., 2016; Lin et al., 2022). One study raised concerns about bias due to the analysis unexpectedly providing a narrow sub-group analysis, which increases the risk of selection bias in outcome reporting (Chan et al., 2016).
Discussion
The results of the current systematic review of 6 RCT intervention studies, designed to help provide relief for community-dwelling PLwD experiencing poor sleep, demonstrated mixed results and indicated the need for further research. The systematic review updated a previous systematic review (Wilfling et al., 2023) but limited the reviewed studies to the community-dwelling PLwD population. While intervention outcomes were mixed, the approach of this review helps evidence-based providers identify interventions for the community making the research more accessible.
This review reports no firm conclusions about the effectiveness of photo/light interventions or activity-based interventions in reducing sleep disturbance due to differences in the assessment tools and methods used in the studies. Studies included in this review were required to have used standard assessment tools and an RCT design. Each study used standard assessment tools; however, only two studies reported positive impacts on sleep using the same measurement tool. For example, Lin et al. (2022) and Chan et al. (2016) both reported positive impacts for activity-based interventions using the PSQI. However, both studies had small sample sizes and an increased risk of bias. In the photo/light themes, McCurry et al. (2011) and Sloane et al. (2015) both reported using actigraphy, but only the study by McCurry et al. (2011) reported positive outcomes using actigraphy. Additionally, McCurry et al. (2011) employed a parallel arm RCT, whereas Sloane et al. (2015) used a crossover design, limiting cross-comparison.
The difference in assessment procedure and study design limits the determination of the effectiveness of interventions as a theme. Replication of methods or interventions in current studies should be considered for future research to help strengthen the effectiveness of the findings and determine when interventions are most effective, as well as which populations benefit most. Other systematic reviews also report mixed findings for photo/light interventions. The systematic review by Mitolo et al. (2019) reviewed photo/light interventions and was inconclusive for the effects of photo/light interventions, while Zang et al. (2023) reported positive effects of photo/light interventions for institutionalized PLwD but not for community-dwelling. Further research is needed to draw firm conclusions about the effectiveness of interventions.
Multi-component interventions employed a unique approach by focusing on the caregiver-care recipient dyad for intervention implementation. These interventions included multiple approaches, such as environmental/ behavioral sleep routines, education, light exposure, caregiver support, and exercise, delivered through a progression of in-person sessions. The caregivers were taught the intervention components one session at a time by trainers (McCurry et al., 2011; Rappaport et al., 2024). The trainers taught the caregivers about the illness and worked with the dyads to develop intervention implementation and adherence plans for success. This approach integrates with daily routines and provides the development of practical caregiving skills in addition to the intervention itself. Trainers taught the dyads to address real-world issues in a support-direct method. Dyadic interventions in the community may help increase resiliency within the dyads, thereby decreasing caregiver burden and improving QoL (Balvert et al., 2024).
The multi-component intervention group did not find similar findings using the same assessment tools; however, the strength of this category was the use of replication and larger sample sizes. The NITE AD researchers replicated, in two different RCTs that took place 6 years apart, the NITE AD, both with positive impacts on sleep. McCurry et al. (2005) and McCurry et al. (2011) both studied the impacts of NITE AD using similar methods and reported similar positive findings, helping strengthen the intervention’s generalizability. The DREAM START intervention had a large sample size (n > 300), strengthening the power and generalizability of the study findings. The robust study designs and sample sizes enhance confidence in the effectiveness of the interventions in reducing sleep disturbances.
Caregiver burden is a significant risk factor for institutionalization and poorer QoL for PLwD (Benca et al., 2022; Nikmat et al., 2015; Gibson & Gander, 2020). Of the six studies in this review, only four reported on caregiver burden. The findings regarding caregiver burden were mixed. Some caregivers reported an increased burden implementing the intervention based on direct interventions (McCurry et al., 2005, 2011). Two studies compared the perception of the burden of care for the intervention group with that of the control group, reporting no difference (Rappaport et al., 2024; Sloane et al., 2015). One possible explanation for these outcomes is that the overall burden of care for PLwD experiencing sleep disturbances is more challenging in general. Future studies should assess the potential impact of the study or intervention on caregiver burden and its effects on the results.
Limitations
Despite strategies to enhance rigor of this review (e.g., multiple reviewers), there are limitations to this study. Most notably, there were a small number of studies identified and many of the reviewed studies had a moderate to high risk of bias because the risk of external factors influencing the intervention effect. Finally, no study evaluated the impacts of the interventions on the progression of dementia; rather, outcomes are based on QoL. Future research is needed to understand what the interventions are directly impacting. It should be noted that all of these studies involved vulnerable populations, people with cognitive impairments, and therefore all of the studies reviewed involved ethical and methodological challenges that may have impacted the findings.
Conclusions
Growing evidence supports the use of NPI for treating sleep disturbances in PLwD; however, the effectiveness of interventions remains inconclusive. Multi-Component dyadic interventions, such as NITE AD and DREAMS START, have more evidence supporting their effectiveness for community-dwelling populations than other intervention themes. Further research is needed, along with replication of the interventions identified in this review, to increase confidence in its effectiveness. Future research also needs to compare intervention effectiveness across community and institutionalized settings. Dementia is a complex illness that has far-reaching impacts on the person with the illness and their families. Continued research and support are necessary to assist all those affected.
Supplemental Material
Supplemental Material - Evaluation of Non-Pharmacological Interventions for Community-Dwelling Individuals With Dementia Experiencing Sleep Disturbances: An Updated Systematic Review
Supplemental Material for Evaluation of Non-Pharmacological Interventions for Community-Dwelling Individuals With Dementia Experiencing Sleep Disturbances: An Updated Systematic Review by Patton Childers, Nicole Ruggiano, Ellen L. Brown
Footnotes
Ethical Considerations
Not Applicable for Review.
Consent to Participate
Not Applicable for Review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.