
Abstract
Person-centeredness has been championed as a key principle of quality healthcare, but its application to the fourth aim of quality healthcare—workplace quality for the persons providing care—has received little attention. Drawing on notes and transcripts from four facilitated discussion groups with a total of 31 purposively selected participants, ranging from direct care workers to organizational leaders and academics working in aging, this special article describes insights gained about person-centeredness as it applies to the caregiving workforce. Three key issues emerged: person-centeredness varies by care setting due to differences in organization and client/patient needs; person-centeredness is not considered standard care; and person-centeredness consists of an interplay between leadership and care providers. A consistent point across all three issues is of variation, which can be addressed in part by identifying and addressing barriers at the individual and setting level to person-centered care.
• Perspectives of person-centeredness in geriatric care from diverse direct care workers, clinicians, and organizational leaders • Comparisons of person-centered care across settings that provide care for older adults
• Concepts identify barriers that can be addressed to change organizational structures and care practices to promote person-centered care • Making care more person-centered may improve the work life of health care providersWhat This Paper Adds
Applications of Study Findings
Worldwide demographic shifts are causing healthcare systems to focus more on persons who are older and have chronic and disabling conditions. In the US, the coming decades will see the population aged 65 and older—who already disproportionately use health care services—grow nearly 50% faster than those aged 25–65 (Congressional Budget Office, 2023). The rapid expansion of the older population will result in an increasing demand for and shortage of workers, particularly those in aging services and long-term care (Health Resources & Service Administration, 2024). COVID-19 complicated staffing shortages even more, as long-term care services lost proportionately more workers than hospitals and still are struggling to recover (American Health Care Association/National Center for Assisted Living, 2022; Telesford et al., 2023). Shortages and related issues increase worker burnout and lessen satisfaction, resulting in reduced performance, absenteeism, and exit from the workforce (Chatterjee, 2022; Richert & Zucchero, 2023).
Throughout the health care industry, efforts are underway to identify more effective ways to improve population health, enhance the care experience, and decrease cost per capita—an approach known as the Triple Aim (Berwick et al., 2008), which recognizes person-centeredness as a central tenet to achieve these goals (Cohen et al., 2022). In fact, the concept of person-centeredness has been widely applied across healthcare, highlighting the need for care providers to cultivate relationships with patients to best identify and meet their care preferences (Tieu et al., 2022). Until recently, the well-being of the care provider in achieving the Triple Aim was not fully recognized, but in recognition of increasing provider shortages and burnout, the goal to achieve quality health care has added a fourth aim: improving the work life of health care providers (Bodenheimer & Sinsky, 2014; Feeley, 2017; Mate, 2022).
The link between quality patient outcomes and satisfied, high-functioning healthcare staff is well documented (Bragge et al., 2025). Yet, reported rates of staff depression and high levels of stress, anxiety, and burnout are reported throughout health systems worldwide (Bragge et al., 2025; Sloane et al., 2024; Vracevic et al., 2025). For example, a recent study of over 300 certified nursing assistants (CNAs) across multiple states found that, to deal with work-related stress, many used maladaptive strategies such as emotional isolation, leaving or avoiding work, or smoking cigarettes (Sloane et al., 2024).
Because it is now recognized that care providers are paramont to achieving quality, person-centered care, healthcare systems are advised to be more supportive toward workers, especially those who are critical to addressing coming demographic changes, including nurses, CNAs, and other direct care workers. Consequently, person-centeredness has begun to be applied to the experience of workers as well as that of patients in settings such as hospitals and long-term care systems (Celano et al., 2022; Pereira et al., 2024).
Unfortunately, implementation of person-centeredness in healthcare presents challenges for both those receiving care and those providing care. Issues such as the balance between patient safety and independence, and when to restrict person-centered practices due to safety concerns, have been challenging to resolve (Brownie & Nancarrow, 2013; Simmons et al., 2016; Zimmerman et al., in press), and at times create dissonance between healthcare workers and the settings in which they work (Myers et al., 2018). Further complicating the matter is that the reality of providing person-centered care can reinforce inequities due to issues such as cultural, racial, and socioeconomic differences between providers and patients, and between providers and their supervisors (Roets-Merken et al., 2016; Smith et al., 2022; Syed et al., in press).
Indeed, person-centeredness is now a key principle of quality healthcare, but its application to the fourth aim of quality healthcare—the persons providing that care—has received little attention. To address the relative dearth of literature understanding how providers who care for older adults conceive of person-centeredness oriented to their own well-being, we conducted a series of discussion groups to better understand the core values and concepts of person-centeredness in relation to care settings and care providers. Through the conduct of discussion groups with four groups of diverse providers from a variety of settings, this special article present new insights related to person-centeredness as perceived by the workforce caring for older adults.
Design and Methods
Initially, a search was conducted of the peer-reviewed and gray literature, including a focus on the healthcare workforce. The PubMed search engine was used to query peer-reviewed sources; an internet search engine (Google) was utilized to identify gray literature. Search terms for person-centeredness included “person centered care,” “person directed care,” “individualized care,” or “personalized care.” Search terms related to the workforce included “caregiver,” “worker,” “administration,” “direct care worker,” “provider,” and related terms. Sources were limited to the past 20 years. The review was presented to the steering committee of LINC-AD (Leveraging an Interdisciplinary Consortium to Improve Care and Outcomes for Persons Living with Alzheimer’s and Dementia), a national network convened by the Alzheimer’s Association. Based on the literature, the steering committee identified four summative topics for in-depth exploration: definition of person-centeredness, person-centeredness from a systemic perspective, person-centeredness and technology, and person-centeredness in relation to care and the healthcare workforce. This paper reports the results related to person-centeredness and the workforce.
We employed a series of two meetings with long-term care staff and two facilitated think tank discussions with national experts in the summer of 2022 to explore perspectives on person-centeredness as it relates to the healthcare workforce and to identify factors that facilitate or impede the implementation of person-centered practices. Each lasted 90–120 minutes and was facilitated by a trained moderator, with a separate project team member assigned as note-taker. The two in-person meetings included: (a) 11 staff members (including nursing, direct care, and dining staff) from a Maryland assisted living community, and (b) 10 members of the Alzheimer’s Association Dementia Care Provider Roundtable. Participants for the virtual sessions were selected through literature review and professional networking to ensure representation from diverse disciplinary and professional backgrounds. Virtual think tank participants included: • A senior policy maker and administrator of a state center on aging • The owner of a health care management company focusing on assisted living • A professor of geriatrics • A certified nursing assistant (CNA) active nationally in health care advocacy • A licensed nursing home administrator who is active in public policy • A social worker who works at a county department on aging and formerly worked in adult day services • A national advocate for direct care workers in nursing homes • An experienced nursing home administrator now working in policy for a national health care organization • A doctoral student with experience working as a nursing assistant in home health and in conducting health systems research • A social worker and former nursing home activity director
The discussion facilitator was provided a series of open-ended questions to stimulate discussion. The questions included prompts such as “How does the concept of person-centeredness relate to you in your work? How does it apply to health care workers in general and in your setting? Does person-centered care need to be taught? What kind of care is easiest/hardest to deliver in a person-centered way? What does administrative support for person-centered care look like?” The semi-structured question framework was used flexibly, allowing participants to introduce additional topics and perspectives beyond prepared questions.
All meetings were audio-recorded and transcribed verbatim. For each session, the designated note-taker prepared a written summary within 24 hours, which was subsequently reviewed and revised by the project team to ensure accuracy and completeness.
An exploratory thematic analysis was conducted, with materials analyzed by the study team using a qualitative iterative process. Concepts were elaborated by group consensus and refined iteratively to incorporate perspectives across all project components and participant groups. For this report, representative quotations were selected from the transcripts to illustrate each concept. Quotations were chosen based on their ability to capture perspectives expressed by multiple participants.
Issues Identified
Overall, discussion elucidated three key concepts: person-centeredness varies by care setting due to differences in organization and client/patient needs; person-centeredness is not considered standard care; and person-centeredness variably consists of an interplay between leadership and care providers. Each topic is presented with illustrative quotes in the material that follows.
Person-Centeredness Varies by Care Setting due to Differences in Organization and Client/Patient Needs
Through the course of discussion, participants noted that person-centeredness differed based upon the setting in which care was delivered. At one extreme, home care was considered to have successfully implemented person-centered concepts into its operations because it is structured on one-to-one interactions, but at the same time, home health agencies struggle with barriers to person-centeredness common to other care settings, including lack of staff continuity and adherence to protocol-driven care. However, a participant noted that one-on-one interactions can in part overcome such barriers: “Regardless of what’s in that care plan, the caregivers have the ability to shift the procedure and documentation to match the care plan while making the care really more valuable and more person-centered” (former home health aide). At the other extreme, acute care hospitals were considered to be least person-centered, as they treat high acuity conditions and are especially time-bound in their approach to care; the goal of hospital care is to treat and discharge patients efficiently, leading to shorter interactions and more procedural care, which is what patients have come to expect. “Hospitals are not expected to be home. We understand that [when] we check into a hospital, we are giving this nebulous group of people control over our bodies” (former home health aide).
Person-Centeredness is Not Considered Standard Care
To be sure, participants recounted events that conveyed person-centered care, including “CNAs [certified nursing assistants] go out of their way to accommodate residents in ways they don’t necessarily have to. I know a lot of times…you have residents who can’t afford to go to the beauty shop every week, but they want their hair done. So, the CNAs buy the rollers, bring them in … roll their hair, and then they dry it and fix it and comb it up for [the residents] every week .. [they] take their time to do that” (nursing home CNA). As noted though, person-centeredness was not necessarily considered standard care, as per the comment that CNAs “go out of their way.” Such an approach can extend to non-nursing staff as well: This is our full-time job, but their full-time life. And so because of that, you have to kind of connect with them. Whenever I do have time, I make the time. That’s going a little bit above and beyond” (assisted living dining services staff). Another noted that “Person-centered care doesn’t mean that you get everything you want, when you want, how you want it, and I want it now kind of a thing. It’s about living in the community” (professor of geriatrics). Further, it was recognized that staffing realities themselves challenge the provision of person-centered care. “There are some people who are just not going to be good at person-centered care. There are some people who just shouldn’t be in those roles [as frontline caregivers], and I think the staffing crisis we see has tied a lot of [leadership’s] hands with that. If there’s a warm body with the right certification, pat them on the back and get them in there” (former home health CNA).
Person-Centeredness Variably Consists of an Interplay Between Leadership and Care Providers
There was debate among participants regarding whether ownership itself influences whether or not organizations have person-centered practices; instead, the general consensus was that the issue is not so much about ownership at the corporate level but about leadership at the individual setting. “We’d be hard pressed to find a nursing home corporation that can point to ten of their nursing homes and say ‘look we replicated the [company] culture exactly in each one’, because it’s never been achieved…I wouldn’t say the ownership type creates the …[quality]; I would say the DON [Director of Nursing] and administrator do” (licensed nursing home administrator).
At the same time, direct care workers did not universally embrace that supportive leadership was necessary to provide person-centered care. “I can be person-centered whether my facility is or not. As a CNA, I can approach every one of my residents as a person” (CNA leader and advocate). Similarly, staff reported instances when leaders espoused quality care but did not carry through in practice. “My administrator would get up and say, ‘it’s all about quality now...’ [Meanwhile,] I’ve had a broken wheel on the shower chair for a month….and I’m thinking, ‘oh great! It’s all about the residents now. It’s all about quality.’ I rush up to the office, as a shower aide, and I say, ‘Can I get that new shower chair?’ And he goes, ‘No; it isn’t in the budget” (CNA leader and advocate).
Discussion
Person-centeredness has become increasingly championed as a key principle of quality healthcare; however, its application to the fourth aim of quality healthcare—the persons providing that care—has received little attention. This paper describes a series of discussions related to person-centeredness based on the perspectives of those who oversee or provide that care. Through these discussions, three observations emerged: person-centeredness varies by care setting due to differences in organization and client/patient needs; person-centeredness is not considered standard care; and person-centeredness variably consists of an interplay between leadership and care providers. The commonality across these observations is the variability of person-centeredness in geriatric care.
Person-Centeredness Across Different Care Settings
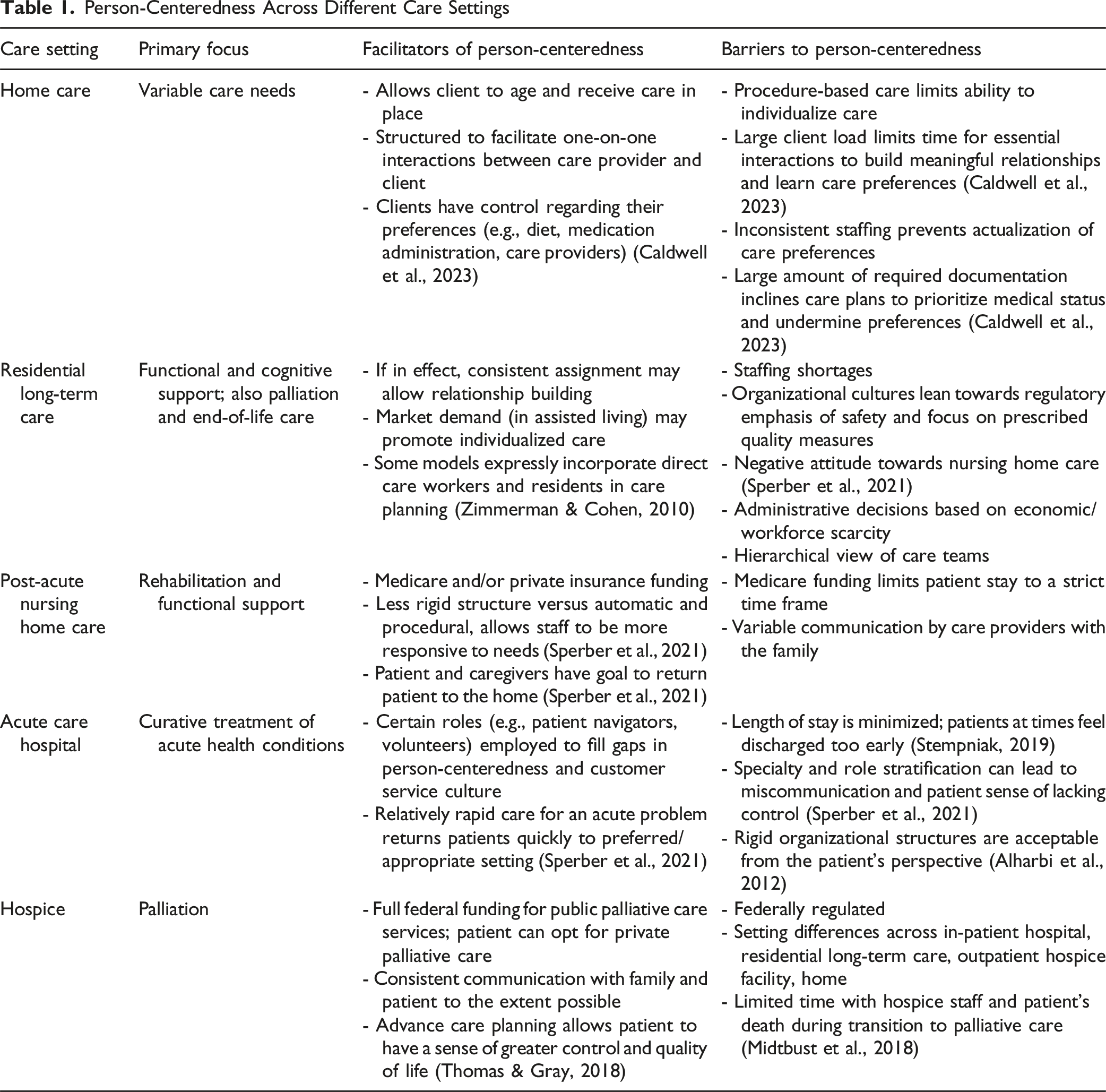
Another clear although disappointing finding was that person-centeredness is rarely the standard of care. In provision of home and community-based services, for example, barriers to person-centeredness include a medicalized care planning process that often marginalizes both the patient and the direct care provider, language and racial differences, and lack of coordination between multiple providers (Caldwell et al., 2023; McPherson et al., 2024). In long-term care settings, barriers to staff performing with person-centeredness exist at the person-level, team-level, and organizational level (Backman et al., 2024), and institutional realities such as staffing shortages, financial limitations, and even the survey/certification process itself work to limit person-centeredness (Travers et al., 2022).
Despite the many limitations, staff have innumerable options to provide person-centeredness in daily interactions, ranging from encouraging a nursing home resident to select their clothes for the day, to providing preferred food, to providing care for activities of daily living in a way that is sensitive to preferred practices (Sloane et al., 2004; Zimmerman et al., 2020). Given the many barriers, however, person-centeredness involves building relationships that go beyond standard care models so as to develop more person-centered trust and understanding between the individual and care provider (Bishop et al., 2008; Kelly et al., 2019). However, not all providers find it easy to build meaningful relationships with their patients/residents/clients; traits associated with those who are most successful include strong interpersonal skills, working holistically, belief in shared decision-making, authentic engagement styles, and flexibility (Vareta et al., 2023); so identifying effective teaching and supervisory structures to enhance such skills, and applying them to person-centeredness, may be indicated (Roets-Merken et al., 2016).
A large and expanding body of literature indicates that high staff turnover and low job satisfaction are improved by organizational changes that support and encourage staff to be person-centered (Austrom et al., 2016; Bishop et al., 2008; Brooker, 2003; McCormack & McCance, 2006). However, participants in the discussion groups noted that encouragement of person-centeredness by healthcare leaders and managers is not consistent, in part because of concerns meeting quality indicators that ostensibly run counter to person-centeredness. Management style is critical as well; evidence indicates consensus-driven leadership—a style that embodies person-centeredness by soliciting and acting on employee input, as opposed to more authoritarian approaches, is associated with higher quality care, increased staff satisfaction, and lower staff turnover (Castle & Decker, 2011; Donoghue & Castle, 2009). Another component of person-centered administrative practice is to provide time and flexibility for care workers to develop relationships and tailor care, because delivering care that is flexible and relationship-focused is a prime source of satisfaction among care providers (Kelly et al., 2019; Myers et al., 2018; Rodríguez-Martín et al., 2013).
Implications for Practice, Policy, and Research
Person-centeredness, as a desirable key element of health care quality, depends on high-performing, satisfied care providers; and viewing person-centeredness from the perspective of caregivers identifies several elements that must be considered and addressed. For one thing, the optimal degree and essential components of person-centeredness will differ depending on the setting. In addition, efforts to improve person-centeredness should consider patient-level, team-level, and organizational factors, identifying both barriers and facilitators to improvement. Finally, because person-centeredness is rarely considered standard care, its promotion needs conscious and ongoing education and quality-improvement efforts that aim to increase support for person-centeredness at the organizational level, foster such traits as interpersonal skills and flexibility among staff, and improve the overall worker experience.
Finally, we note that the observations emanating from our discussion groups are but the beginning of a conversation to better understand and promote person-centeredness in geriatric care by those individuals responsible for the care. The commonality across the observations can enable frank discussion about the root cause of the variability, especially if it is examined in the context of a “just culture” that balances accountability for individuals and the organization as a whole to improve care (Boysen, 2013).
Footnotes
Acknowledgments
The authors thank the meeting participants, including Rebecca Bratsch, MSW, Laci Cornelison, MS, David Farrell, MSW, LNHA, Christian Goodwin, MPH, Holly Harmon, RN, MBA, LNHA, Mauro Hernandez, PhD, Laura Mosqueda, MD, Sherry Perry, Lori Porter, Kenesha Wood, MSW, LRT/CTRS, members of the Dementia Care Provider Roundtable, and staff of a senior living community.
Ethical Considerations
The information presented in this paper was compiled from recorded group meetings rather than a systematic investigation, and so did not meet the Code of Federal Regulations (CFR) definition of research; therefore, IRB approval was not required.
Author Contributions
All authors made a significant contribution to the concept of the paper; participated in drafting the article or revised it critically for important intellectual content; approved the final version of the article for publication; and agreed to be accountable for all aspects of the work and resolve any issues related to its accuracy or integrity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging, grant R24AG065185, T35AG038047.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.