
Abstract
Despite widespread usage in aging and health services, the concept of person-centeredness (PC) does not have a single, universal definition. This definitional challenge may be due, in part, to desired parsimony that oversimplifies the concept’s intrinsic complexity. To better understand the inherent breadth and depth of PC, 116 experts in health- and aging-related policy and practice participated in meetings to discuss PC as a concept, which led to a multilevel conceptualization of the term at the macro, meso, and micro levels. The focus, implementation, and challenges of PC were identified at these interrelated levels, creating a nuanced, contextual model. In addition, the model’s application to current measurement of PC is detailed, and recommendations are made for additional review and development to best measure PC at all levels. This innovative multilevel approach makes explicit the innately contextual nature of PC as a value-based concept, with application for policy, practice, and research.
• A contextual, multilevel conceptualization of person-centeredness (PC) that accounts for its macro, meso, and micro-level aspects. • The conceptualization is supported by existing literature and measures assessing person-centeredness.
• This conceptualization of person-centeredness allows interdisciplinary collaboration and coordination across policy, practice, and research. • Further review and implementation of this model and related measurement of the concept by researchers, practitioners, and policymakers are recommended.What This Paper Adds
Applications of Study Findings
Background
Nearly 30 years after the concept of person-centered care was introduced, there is still no single, agreed-upon definition of person-centeredness (PC) or person-centered care (Nolte et al., 2020). A 2016 systematic review of the topic found 15 definitions that included 17 principles within six domains (e.g., dignity, choice, and self-determination) (Kogan et al., 2016). In a recent systematic scoping review of the definitions being used in scholarly literature related to dementia, most papers referencing person-centered or patient-centered interventions did not define the term, and when they did, the definitions vary widely (Efird-Green et al., in review). The concept of PC is applied to numerous populations and services, including virtually all aspects of healthcare, complicating the definition further and creating even more terms for the concept (Fazio et al., 2018).
The multiple components of PC sometimes overlap in disparate definitions, but are not universal (Kogan et al., 2016), particularly in social and cultural contexts that are not Western and individualistic (Smith et al., 2022). Although a single definition may not be a reasonable goal given the values-based nature of the concept, an organizational structure that embraces the differences inherent in current definitions would allow a common understanding of PC and be beneficial to healthcare practitioners, policymakers, and consumers. Currently, much of the existing research conceptualizes PC as a single, unified construct and concentrates on person-centered care practices, thereby overlooking the personal, organizational, and societal contexts that influence how PC is perceived and experienced. A common, nuanced understanding of the concept could improve operationalization, implementation, and measurement/assessment of PC across a variety of settings and populations, thus making the concept less esoteric and more actionable (Kogan et al., 2016).
One such organizational structure is the multilevel sociological analysis framework, which has been utilized and adapted in a variety of social science fields including public health, social work, sociology, and political science and proposes three levels to understand the application and impact of social problems and interventions: the micro, meso, and macro levels (Pyyhtinen, 2017; Serpa & Ferreira, 2019; Wiley, 1988). These levels are not isolated from one another; rather, the multilevel elements of a concept, policy, or intervention are interrelated, and when applied to a concept or phenomenon, a multilevel perspective allows for a more complex, nuanced definition and implementation that holds space for multiple understandings and experiences (Pyyhtinen, 2017).
In healthcare research, this framework has been applied in a variety of contexts, including studies of value (Beirao et al., 2017) and quality (Wiig et al., 2014) in health service systems; understanding health policy implementation (Caldwell & Mays, 2012) and the roles of institutions in healthcare inequality (Gkiouleka et al., 2018); as well as in interpreting the results of patient-reported outcome measures (Sawatzky et al., 2021) and the implications of big data in healthcare (Kuziemsky et al., 2018). However, this framework has never explicitly been applied to the concept of PC; indeed, the struggle to universally define PC is perhaps due to a desire to simplify this complex concept into a single sentence. For example, defining PC as only relevant in certain populations (e.g., dementia- or aging-related care) deemphasizes the importance of PC across all health and service settings; similarly, defining it through values alone (e.g., dignity or empowerment) limits actionable implementation and does not recognize value differences across settings or cultures. A multilevel conceptualization of PC could incorporate the “richness and messiness of the world” (Pyyhtinen, 2017, 302), as well as the value- and context-based nature of the concept, while still providing a structure through which person-centered practice, policy, and research can be understood and evaluated. To that end, this project was conducted to create a more nuanced conceptualization of PC based on the multilevel sociological analysis framework.
Methods
As part of a larger project to understand PC and its application to systems, the workforce, and technology, meetings were held with 116 diverse experts in health and aging. Of the 116 experts, 37 participated in virtual meetings of four to eight people and included researchers, practitioners, policymakers, advocates, and direct care providers in long-term and healthcare. An additional virtual meeting included 10 members of the Alzheimer’s Association Early-Stage Advisory group. Finally, three in-person meetings were held with 12 care partners in an assisted living community; 16 attendees at the Center for Innovation Conference; and 41 members of the Alzheimer’s Association Dementia Care Provider Roundtable.
All meetings included prompts developed a priori by the project team that asked about participants’ definitions of PC, and three of the meetings specifically focused on the concept of PC. For example, participants were asked: • What comes to mind when you think of being person-centered, not just in terms of care, but in terms of society in general? • What are the key elements of PC? Where are the fuzzy edges? • How should issues of race, class, inequality, and privilege be taken into consideration as part of attempts to be person-centered?
The meetings were 60 to 90 minutes in duration and were recorded and transcribed. Feedback from these discussions was then organized into a multilevel conceptualization of PC, using the traditional sociological levels of analysis (micro, meso, and macro), that holds space for nuance while still allowing for a common understanding that can be used at all levels of policy, practice, and research. Given the project’s goals, participant feedback was organized in an inductive manner, with constructs identified by the project teams, and the sociological framework was applied post-hoc to these constructs by the authorial team. In addition, a literature search was conducted after feedback was compiled to identify illustrative measures of PC, in part to examine whether the multilevel conceptualization is present in the PC-related measurement, as well as to understand if and how the focus, recommendations for implementation, and challenges identified by participants may already be being measured across systems, cultures, organizations, communities, individuals, and families. These measures were categorized depending on their audience/users and item content (e.g., organizational self-assessment versus individuals’ assessment of care quality). System-level assessments were defined as macro; organizational as meso; and individual as micro, in keeping with the overall sociological framework.
Results
Participants talked about PC in a way that fit within a multilevel model and addressed three topics: its • At the macro level—meaning systems and cultures—there is a focus on core values, the influence of privilege and oppression, and how PC is implemented—or not—in systems and cultures. • On the meso level—organizations and communities—there is a focus on organizational responsibility, the applicability of PC to various communities, and the importance of relationships. • On the micro level—individuals and families—PC is focused on care, including individualization and personalization, the importance of care partners/family, and the challenges of PC in context. Multilevel model of person-centeredness, including the focus, implementation, and challenges of each interrelated level
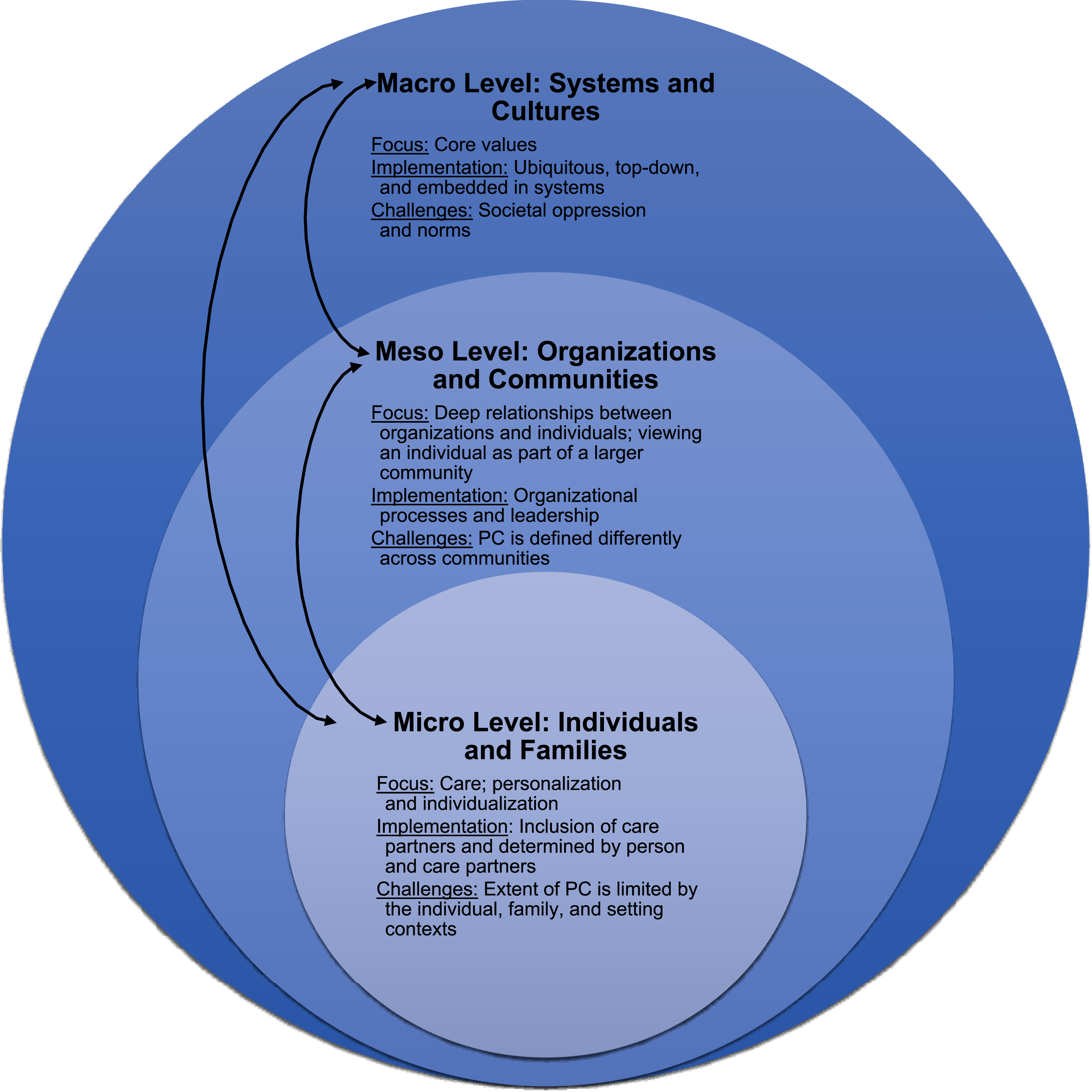
Each of these levels and the related focus, implementation, and challenges are detailed in the material that follows.
The Macro Level: Cultures and Systems
Focus, Implementation, and Challenges of the Macro Level of PC: Systems and Cultures
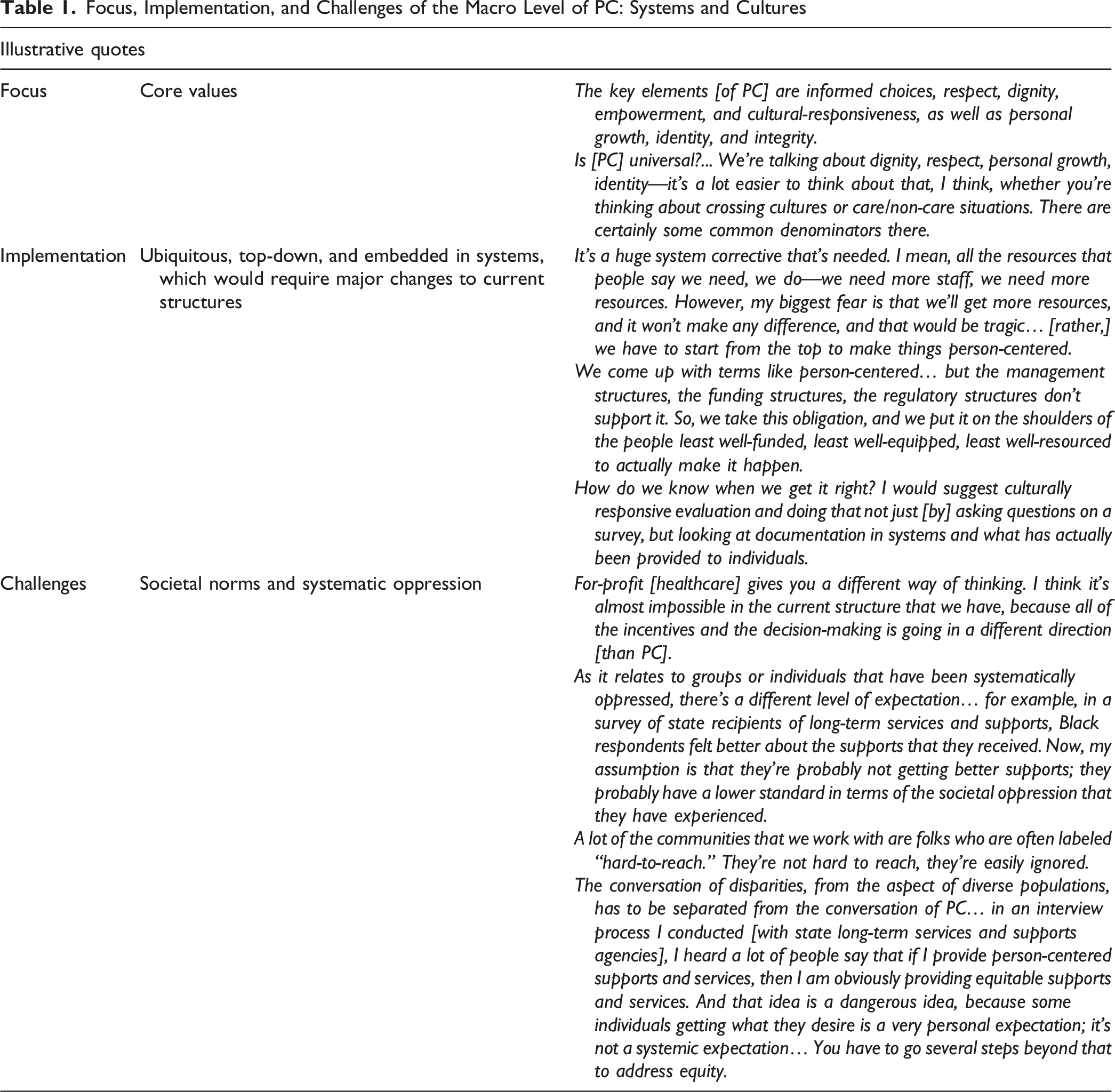
In remarking on the challenges of PC at the macro level, respondents noted that the reality of a values-based shift in industry- and system-wide practices is complicated. In fact, the very nature of the for-profit American healthcare system, which relies on the creation of profit and complex funding mechanisms to survive, is antithetical to the idea of PC; it currently motivates organizational and policy leaders to prioritize efficiency and one-size-fits-all solutions to increase profitability, as one participant stated: “For-profit [healthcare] gives you a different way of thinking. I think it’s almost impossible in the current structure that we have, because all of the incentives and the decision-making is going in a different direction [than PC].” Another macro-level consideration for the concept of PC is that it must recognize and address issues of privilege and oppression at a societal level. For example, satisfaction data, which are often how PC is measured, can be skewed by the impact of oppression for groups that have systematically been denied access to PC programs and practices: “In a survey of state recipients of long-term services and supports, Black respondents felt better about the supports that they received. Now, my assumption is that they are probably not getting better supports; they probably have a lower standard in terms of the societal oppression that they have experienced.”
In relation to challenges, PC must be implemented inclusively, particularly for “hard-to-reach” and underserved groups such as those who do not speak English as a first language: “[Communities are] not hard to reach, they are easily ignored… We don’t want to pay for language access, or we don’t want to meet them where they’re at, in rural areas or on reservations, we don’t want to go there.” PC requires more than just good intentions and a focus on the individual; it needs to be designed equitably and co-created with diverse populations “with any number of intersections around their identities.” However, the implementation of PC or its core values should not be mistaken for societal equity; participants identified that as a “dangerous” overreach of the core concept. For example, “We might say that an individual navigated a service well, but then we might miss big-picture discrimination, or big-picture obstacles and barriers for folks around how certain people are accessing services.” Because of the historical oppression of individuals with diverse identities and the longevity of inequity in American society, addressing disparities requires more work than the implementation of PC in various systems: “Some individuals getting what they desire is a very personal expectation; it is not a systemic expectation… You have to go several steps beyond that to address equity.”
The Meso Level: Organizations and Communities
Focus, Implementation, and Challenges of the Meso Level of PC: Organizations and Communities
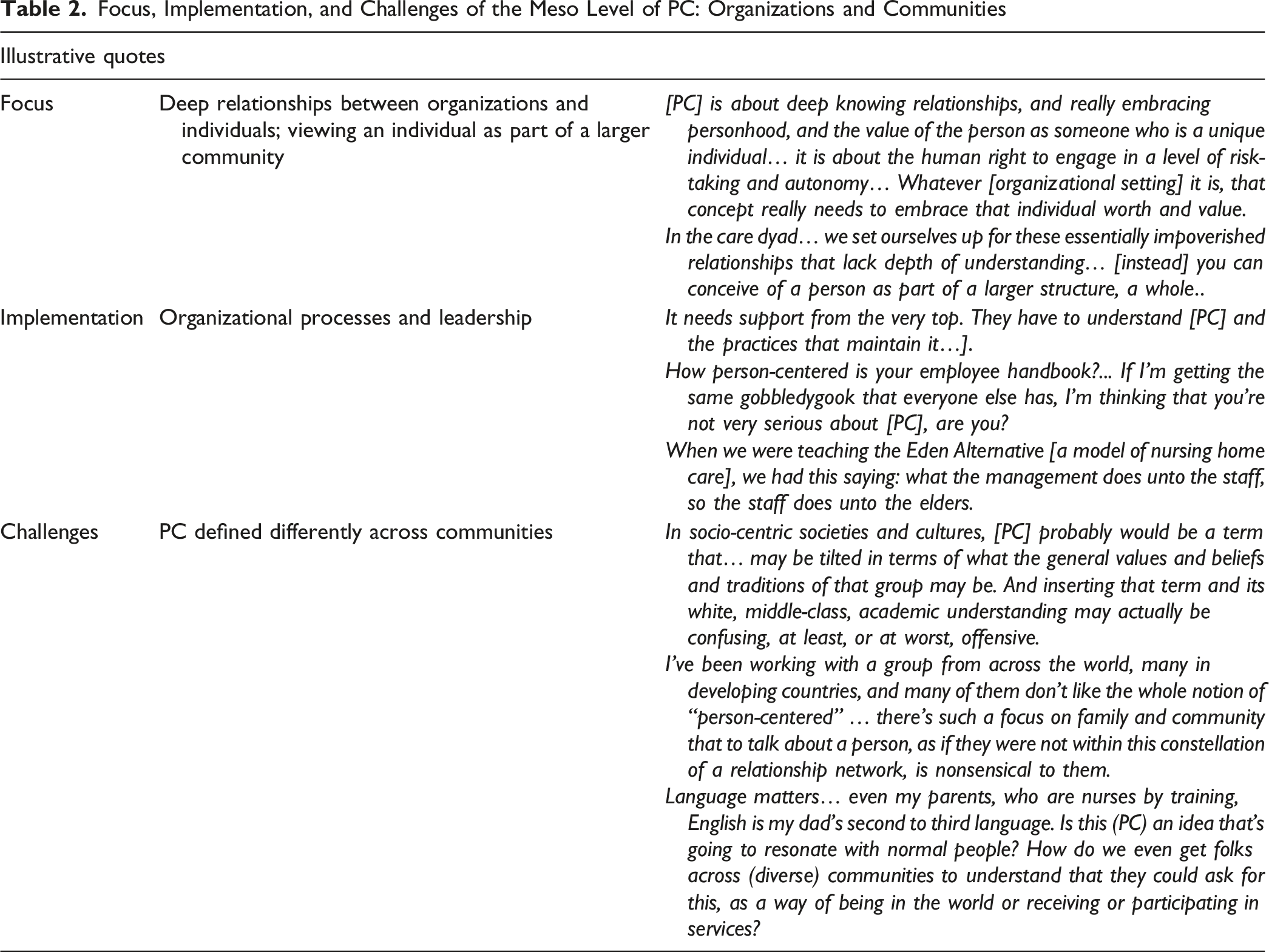
To implement PC on the meso level, respondents stated that organizations must consciously embed it into their internal processes and practices (e.g., staff culture) rather than solely client-focused functions; for example, “How person-centered is your employee handbook?... If I’m getting the same gobbledygook that everyone else has, I’m thinking that you’re not very serious about [PC], are you?” Additionally, organizational leaders must understand the concept and support its implementation: “It needs support from the very top. They have to understand [PC] and the practices that maintain it.” Changing internal processes requires an organizational culture shift and dedicated leadership—“What are you doing to create cultures of belonging? And where is leadership in really modeling that?”—not just by a single champion, but by the entire management structure of the organization. The extent to which PC is embedded into an organization impacts its core functions; for example, how staff in a long-term care setting treat their residents (“what the management does unto the staff, so the staff does unto the elders”), or how ethical dilemmas are solved (“those are tough decisions, and you can’t just knee-jerk… you need a process to solve problems that honor values and respect that person’s right to make a choice”).
Participants identified a meso-level challenge of PC: that communities may have disparate understandings of the concept. The term, or some of its core values, may not universally resonate in non-individualistic communities, both within the US and globally. For example, one participant stated that “I’ve been working with a group from across the world, many in developing countries, and many of them don’t like the whole notion of ‘person-centered’… there’s such a focus on family and community that to talk about a person, as if they were not within this constellation of a relationship network, is nonsensical to them,” and another said that “inserting that term and its white, middle-class, academic understanding [into socio-centric communities] may actually be confusing, at least, or at worst, offensive.” These value-based differences must be addressed through cultural adaptation and translation of PC. An inability to effectively do so could affect access to person-centered services and care: “Language matters… is this [PC] an idea that’s going to resonate with normal people? How do we even get folks across [diverse] communities to understand that they could ask for, as a way of being in the world or receiving or participating in services?”
The Micro Level: Individuals and Families
Focus, Implementation, and Challenges of the Micro Level of PC: Individuals and Families
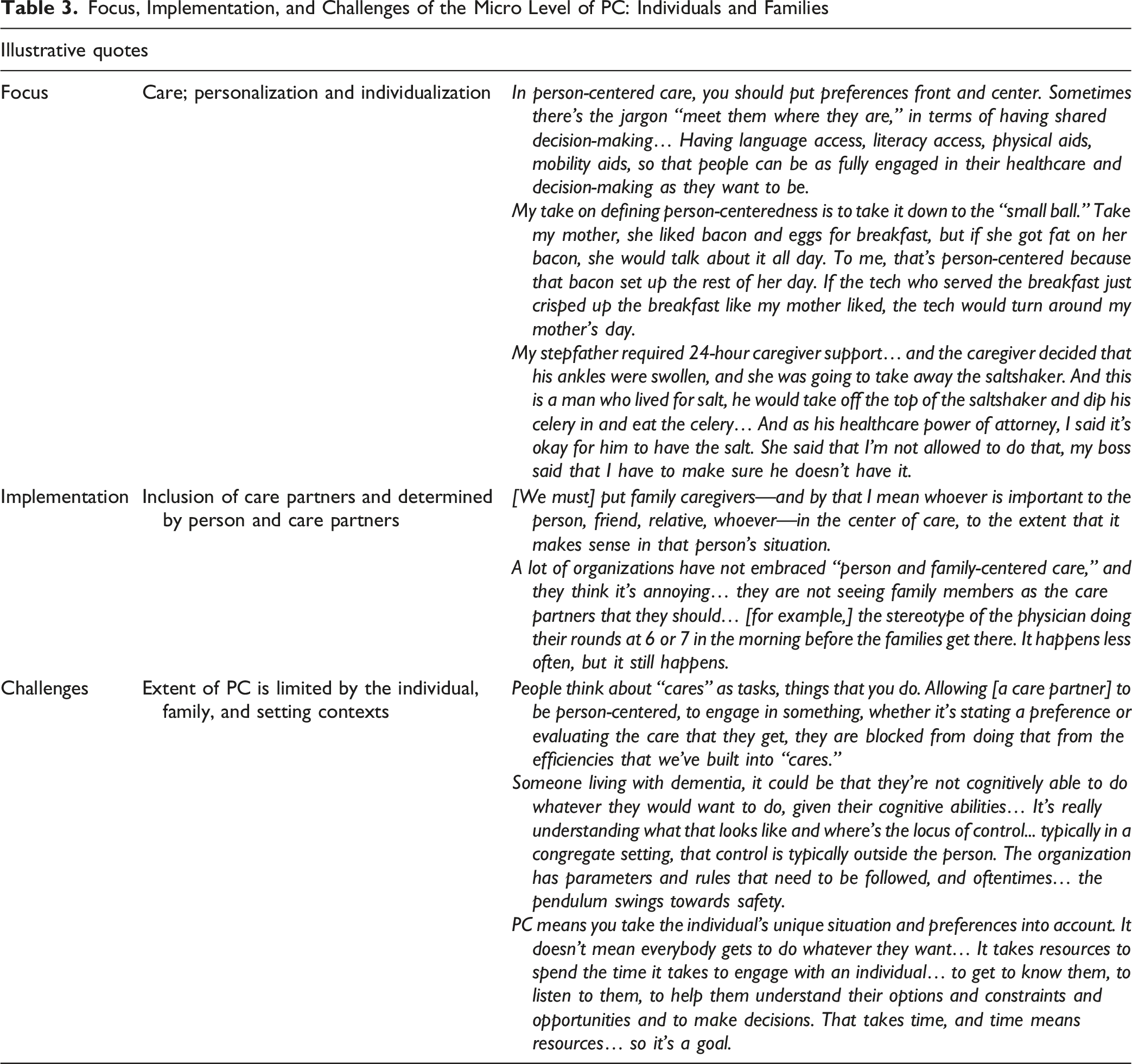
Participants also insisted that PC should consider the role of families, which may be family, friends, or others involved in a person’s care: “[We must] put family caregivers—and by that I mean whoever is important to the person, friend, relative, whoever—in the center of care, to the extent that it makes sense in that person’s situation.” Some participants identified person- and family-centered care as an analogous term for person-centered care. Unfortunately, families may not be regarded as key partners by all healthcare providers, despite their importance to the shared decision-making and care processes: “A lot of [care] organizations have not embraced ‘person and family-centered care’, and they think it’s annoying… they are not seeing family members as the care partners that they should… [for example,] the stereotype of the physician doing their rounds at 6 or 7 in the morning before the families get there.”
On the other hand, PC can and sometimes must be limited by the care context. For example, in long-term care settings, efficient, task-oriented “cares” may limit PC—“People think about ‘cares’ as tasks, things that you do… Allowing someone to be person-centered, to engage in something, whether it’s stating a preference or evaluating the care that they get, they are blocked from doing that from the efficiencies that we’ve built into ‘cares.’” In addition, there are limitations to PC for individuals who live with cognitive change or in congregate settings, which may prioritize safety and liability over personal choice. One participant stated that “Someone living with dementia, it could be that they’re not cognitively able to do whatever they would want to do, given their cognitive abilities… where’s the locus of control... in a congregate setting, that control is typically outside the person. The organization has parameters and rules that need to be followed, and oftentimes… the pendulum swings towards safety.” Finally, resources are often a challenge at the micro level. Time, money, and capacity all affect how an individual’s preferences can be expressed and carried out by caregivers. Thus, PC may be a goal, rather than a guarantee: “It takes resources to spend the time it takes to engage with an individual… to get to know them, to listen to them, to help them understand their options and constraints and opportunities and to make decisions. That takes time, and time means resources… so it’s a goal.”
Multilevel Measurement of PC
Examples of Multilevel Measurement in PC
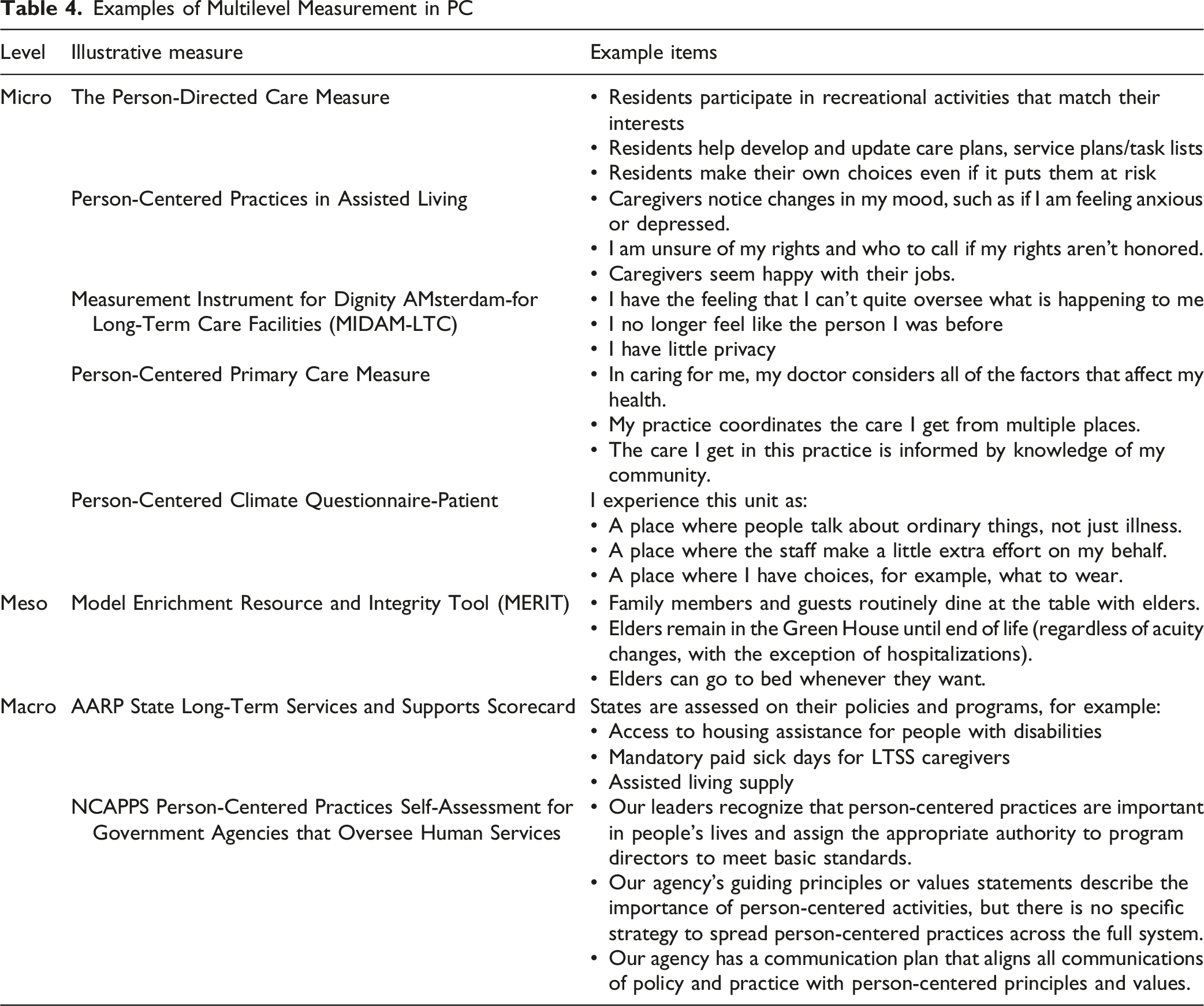
At the micro level, there are a variety of tools to measure aspects of individual person-centered care, including the Person-Directed Care Measure (White et al., 2008); the Person-Centered Practices in Assisted Living (Zimmerman et al., 2015); the Measurement Instrument for Dignity AMsterdam-for Long-Term Care Facilities (Oosterveld-Vlug et al., 2014); the Person-Centered Primary Care Measure (Etz et al., 2019); the Person-Centered Climate Questionnaire-Patient (Edvardsson et al., 2009), and many others. These and other instruments ask individuals, including service recipients, family members, and organizational staff, their opinions of their care and environment with the purpose of evaluating and improving that care and environment. In this way, these measures are micro, in that they are focused on the experience of an individual but aim to impact the implementation of PC at the meso (organizational) level.
A person-centered organizational measure is the Green House Project’s Model Enrichment Resource and Integrity Tool (MERIT), developed with the Calvin University Center for Social Research (Green House Project, 2023). This measure is completed by organizational leaders in order to evaluate organizational practices and policies for PC. Finally, at the macro level, the AARP State Long-Term Services and Supports Scorecard assesses systems, has an equity focus, and is based on a person- and family-centered approach (AARP, 2023); another example is the National Center on Advancing Person-Centered Practices and Systems (NCAPPS) Person-Centered Practices Self-Assessment for Government Agencies that Oversee Human Services (NCAPPS, 2022). Both of these measures are meant to be completed by the leadership of long-term services and supports departments at the local, state, or federal level to evaluate these systems’ implementation of PC.
It is apparent that there are limitations to measurement at the meso and macro levels, in that there are fewer available instruments available. Siloing PC into the micro level is common, and results from a focus on person-centered care rather than on person-centered organizations or systems (Leidner et al., 2021). In addition, there is a lack of commonality in assessed elements among the measures, both within and among framework levels. In a critical comparative review, Edvardsson and Innes (2010) found that most measures do not explicitly define their conceptual underpinnings, which makes comparing measures difficult. An updated systematic review and crosswalk of such measures to identify the most effective way to evaluate PC from a multilevel perspective, including via a multiscale assessment, could then allow evaluators to measure PC at each framework level simultaneously. One possible assessment strategy could be person-centered attainment scaling, which considers multilevel challenges to PC that result in inherent tensions (e.g., safety versus freedom, and superficial versus deep knowing) and its effect on the well-being of individuals in a variety of settings (Zimmerman et al., in review).
Discussion
PC is widely used but has no universal definition, which impedes research, the development of policies, and the implementation of practices. Based on discussion groups with 116 experts in aging and healthcare, a multilevel conceptualization of PC was evident, modeled using the three levels of sociological analysis: macro (systems and cultures); meso (organizations and communities); and micro (individuals and families). This conceptualization includes the term’s core values and foci—for example, personhood, dignity, deep knowing, and individualization based on preferences—as well as how those foci are implemented and their boundaries and challenges. This project, unique in its reach and focus, resulted in an innovative and nuanced model that could be applied to a variety of settings and fields at every sociological level. Of course, PC has innate tensions, such as community versus individual and policy compliance versus flexible decision-making; these and other tensions are reported in a related article, “The Need to Reconstruct ‘Person-Centeredness’ Based on Inherent Tensions” (Zimmerman et al., in review).
It is important to note that although the results of this project are organized and reported by each framework level, the model’s levels are interrelated as represented by the arrows in Figure 1, and participants often discussed multiple levels of PC within the same prompt response or meeting. For example, macro-level structures, actions, and challenges (e.g., regulation and funding) affect both meso (e.g., organizational priorities) and micro (care delivery) levels of PC implementation, and vice versa. This multilevel model, while preliminary, thus incorporates important context and interactions that are often missing in current research, practice, and policy definitions of PC.
In addition, the elements of PC proposed by participants are also present in the literature, supporting the multilevel model of PC as presented. At the macro level, the foundational values of PC, including personhood, dignity, and empowerment, are generally present in all cultures and are widely acknowledged as essential to conceptualizing PC (Fazio et al., 2018). The impact of oppression has been named as a challenge for implementation of PC across systems and cultures (Smith et al., 2022). In addition, for-profit healthcare systems limit the ability to systemically implement PC at a macro level, because organizational efficiency is often highly valued (Arnold et al., 2020). Creating systems that are person-centered therefore requires dramatic changes to both public and healthcare industry policy; making the delivery and financing of healthcare services, as well as regulatory structures, more person-centered is particularly important to achieving this goal (Leidner et al., 2021; WHO, 2013). In addition, greater public accountability from healthcare organizations and systems, including public reporting of performance measures to illustrate commitment to PC values and practices, could assist with the shift towards PC at the systemic level (WHO, 2013).
At the meso level, the importance of organizational investment in PC is common in best practice reports from expert organizations. For example, the National Center on Advancing Person-Centered Practices and Systems has developed recommendations for the creation of a person-centered organizational culture, including promoting learning; accountability and partnership; and the importance of leaders who invest in power with, rather than power over (NCAPPS, 2024). In addition, the meso-level challenge, disparate definitions, is present in the literature. The cultures that first elaborated the concept of PC, namely, Europe and the United States, are generally individualistic societies which comes with a particular set of values and priorities that is not universal, especially in more socio-centric or collectivistic cultures (i.e., those with a primary focus on the good of the family and community) (Arnold et al., 2020). Whether someone belongs to a collectivistic or individualistic culture influences provider-patient interactions, how illness is conceptualized, and how healthcare decisions are made (Armstrong & Swartzman, 2001); for example, families that live and make health decisions intergenerationally may have disagreements in values and beliefs about healthcare (Johnstone et al., 2016). Given these differences, the need for adaptation of person-centered practices for diverse communities is clear and has been shown to improve health outcomes in advance care planning discussions (Johnstone & Kanitsaki, 2009) and hospitalizations and end-of-life care (Johnstone et al., 2016).
At the micro level, the role of informal care partners, such as family members, in aging and health services is well-established. Family caregivers have consistently been shown to be helpful in promoting person-centered care, including acute care and hospitalization, long-term and home care, and palliative care (James et al., 2009; Thomas et al., 2002; Ward-Griffin et al., 2012). Their integration into shared decision-making with healthcare providers and professional caregivers, without superseding the individual’s wishes, is crucial to the implementation of person-centered practices on an interpersonal level (Boltz, 2012). In addition, the limitations of person-centered care in context are supported by the literature. Efforts to integrate individual choices and preferences into care despite contextual challenges is an ongoing topic of academic research, as well as national and organizational policy for healthcare settings (Bangerter et al., 2017; Leidner et al., 2021). For example, the Rothschild Care Planning Process for Resident Choice to address negotiated risk is one way to approach one of the challenges of PC in care contexts (Behrens et al., 2018). The inherent tensions in PC—for example, community benefit versus individual benefit, or efficiency versus individualization—frequently play out at the micro level, though the tensions are present in the macro and meso contexts in which an individual or family resides (Zimmerman et al., in review).
While this project provides an innovative multilevel conceptualization of PC, there are some limitations. Despite the engagement of a wide swath of experts and providers, some perspectives were inevitably missed. In addition, because of the preliminary nature of this research, the resulting model, though well-established in the literature, has not previously been made explicit. Therefore, examples of its use are limited, and it requires further consideration and evaluation by researchers, policymakers, practitioners, and consumers. However, support in the literature for the aspects of PC present in each of the three levels, as well as measures specific to each level, strengthen the model.
Conclusion
This project leveraged the opinions and expertise of 116 specialists in aging policy and practice to identify a multilevel conceptualization of PC. Their insight of the macro, meso, and micro levels produced a nuanced understanding of PC practices in a variety of settings and contexts, which could aid the development of measures and assessment tools and guide conversations about PC implementation, particularly at the meso and macro levels where PC is more difficult to achieve. A variety of strategies, including the creation of multilevel measures that evaluate systems, cultures, organizations, communities, and individuals’ and families’ experiences, are needed to improve PC at all sociological levels. In addition, research is indicated to better understand the interrelationship between levels and nuances across different populations.
Footnotes
Acknowledgements
The authors thank the meeting participants, including Maria Aranda, PhD, D. Pearl Barnett, MPA, Alice Bonner PhD, RN, Barbara Bowers, PhD, RN, Rebecca Bratsch, MSW, Eric Carlson, JD, Peter Chamberlain, SM, Tony Chicotel, JD, MPP, Laci Cornelison, MS, David Farrell, MSW, LNHA, Colleen Galambos, PhD, Christian Goodwin, MPH, David Grabowski, PhD, Kari Gray, Holly Harmon, RN, MBA, LNHA, Chris Herman, MSW, LCSW, Mauro Hernandez, PhD, Juliet Holt Klinger, MA, Harriet Komisar, PhD, Tamara Konetzka PhD, Bill Lamb, MSW, MPA, David Lindeman, PhD, Jeff McSpadden, Laura Mosqueda, MD, Arif Nazir, MD, Sherry Perry, Lauren Pongan, MA, Lori Porter, Marilyn Rantz, PhD, RN, Ronen Rozenblum, PhD, MPH, Susan Ryan, MA, Robyn Stone, DrPH, Kim Strom, PhD, William Thomas, MD, Kenesha Wood, MSW, LRT/CTRS, Jack York, Gina Zimmermann, MPS, members of the Dementia Care Provider Roundtable, participants of the Center for Innovation 2023 annual conference, and staff of Brightview Senior Living.
Ethical Considerations
The information presented in this paper was compiled from recorded group meetings rather than a systematic investigation and so did not meet the Code of Federal Regulations (CFR) definition of research; therefore, IRB approval was not required.
Author Contributions
Lea Efird-Green, MSW, MPA—lead author, concept, methodology, initial draft of article, final revision, and review of article.
Sheryl Zimmerman, PhD—concept, methodology, and review of article.
Sam Fazio, PhD—concept and review of article.
Philip D. Sloane, MD, MPH—concept, methodology, and review of article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Aging, grant R24AG065185.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.