
Abstract
This study investigated family caregivers’ willingness to utilize institutional care under South Korea’s Long-Term Care Insurance. Using data drawn from 1,369 family caregivers (including spouses and adult children) in the 2019 Korean Long-Term Care Survey, logistic regression analyses were conducted to identify factors associated with institutional care intentions. Results showed that 72% of family caregivers favor institutional care, with adult children and children-in-law being twice as likely to do so as spouses. Willingness to utilize institutional care was significantly higher among non-coresiding caregivers than those coresiding, whereas caregiver gender had no significant effect. Interaction analyses confirmed that the impact of coresidence remains consistent across different relationship types. These findings suggest that coresidence status, rather than kinship alone, shapes caregiving trajectories. The study underscores the need for nuanced long-term care policies, prioritizing burnout prevention for coresiding caregivers and enhancing case management for non-coresiding families to ensure care continuity.
• Adult children and children-in-law are twice as likely as spouse caregivers to favor institutional transitions, reflecting a shift toward long-term feasibility over traditional caregiving norms. • Coresidence status, rather than kinship ties alone, emerges as the most powerful structural factor in determining family caregivers’ willingness to utilize institutional care. • Contrary to traditional Confucian expectations, caregiver gender shows no significant effect on institutional care intentions, suggesting that care decisions are increasingly driven by practical constraints rather than gendered roles.
• Compared with non-coresiding caregivers, coresiding caregivers remained less likely to favor institutional care despite a higher caregiving burden, indicating that coresidence functions as a powerful commitment mechanism. • Policy frameworks must shift from uniform service delivery to nuanced approaches, prioritizing burnout prevention (respite care) for coresiding caregivers and care coordination (case management) for non-coresiding families.What This Paper Adds
Applications of Study Findings
Introduction
As populations rapidly age, the care of older adults has emerged as a critical concern for both families and society. The establishment of Long-Term Care Insurance (LTCI) systems has institutionalized a distinction between in-home and residential care, thereby broadening access to formal services. Despite the expansion of these systems, however, scholarly debate remains limited regarding the optimal timing, location, and delegation of responsibility for caring for older adults (Gitlin & Wolff, 2012; Wolff et al., 2018). Consequently, families often face considerable ambiguity at key decision points, such as identifying who assumes responsibility, determining when to seek assistance, and navigating the coordination between formal and family care. Less attention has been paid to how caregiving intentions are shaped within families, particularly in cultural contexts where traditional caregiving norms are undergoing rapid transformation.
Filial piety and family-based care remain culturally salient in Korea, but these norms are increasingly challenged by demographic shifts—changing gender roles, living arrangements, and the expansion of formal care services (Chon et al., 2024; Ministry of Health and Welfare, 2024). This growing tension between cultural expectations and socioeconomic realities often leads to intra-family negotiation and conflict over care responsibility and quality (Kwak et al., 2012; Lee, 2024; Wang & Youderian, 2025). As a result, caregiving decisions are driven less by normative obligation and more by practical constraints and individual willingness.
Yet, how this shift toward individual willingness translates into care transitions remains underexplored. In particular, the extent to which caregivers’ willingness to use institutional care shapes transitions from home-based care—net of structural factors such as financial resources and access to services—has not been clearly established. Prior research has largely emphasized structural determinants (Bolster-Foucault et al., 2024; Gaugler et al., 2007) or examined family characteristics retrospectively (Gaugler et al., 2007; Wolff et al., 2018), leaving the proactive role of caregivers’ intentions underexamined.
Second, little is known about how spouses and adult children differentially influence care transitions. Existing studies focus primarily on caregiving burden (Liu, 2021) or general attitudes toward elder care (Fenton et al., 2022; Pinquart & Sörensen, 2011), offering limited insight into how these roles shape transition decisions (Gitlin & Wolff, 2012; Verbakel et al., 2024).
Third, the role of coresidence remains insufficiently examined. Although coresiding caregivers often bear greater responsibility and hold more influence in care arrangements (Kim & Lim-Soh, 2024; Pezzin et al., 2015), coresidence has rarely been incorporated as a key contextual factor in shaping willingness to use institutional care.
Addressing these gaps, this study examined the differences in family caregivers’ willingness to utilize institutional care, focusing on how such intentions are linked to kinship ties and living arrangements. Specifically, we analyzed (a) the individual and contextual factors associated with caregivers’ inclinations toward institutional care in anticipation of health deterioration among older adults currently receiving home-based services; and (b) differences in this inclination between spouses and adult children, with a particular focus on the interaction between kinship ties and coresidence status.
Caregiving Trajectories in the Long-Term Care Insurance (LTCI) Context
The implementation of Korea’s Long-Term Care Insurance (LTCI) system formalized the distinction between in-home and institutional care. Consistent with a strong preference for “aging in place,” most older adults receive care at home (Jung & Kim, 2024; Wiles et al., 2012); currently, 80% of LTCI recipients use home-based services, compared to 20% in institutional care (Ministry of Health and Welfare, 2025).
Despite its benefits for recipient well-being, in-home care places substantial demands on family caregivers (Hensly et al., 2021; Kim et al., 2017). With LTCI services typically limited to about 3 hours per day, families must provide the remaining care, often resulting in significant physical and emotional strain (Cha et al., 2023). Although institutional care can alleviate this burden through round-the-clock support, it introduces trade-offs, including psychological adjustment and higher costs (Hébert et al., 2001).
Caregiving arrangements in Korea are also shifting. The vast majority of older adult households now comprise those living alone (32.8%) or with a spouse only (55.2%; Ministry of Health and Welfare, 2024), while the traditional pathway of moving into an adult child’s home is declining (Kim, 2007). Instead, older adults increasingly rely on spouses or formal services (Cha et al., 2022), suggesting a shift toward more direct transitions from home-based to institutional care, bypassing coresidence with adult children (Chon et al., 2024; Jung & Kim, 2024).
Kinship Ties, Gender, and Willingness to Utilize Institutional Care
Prior research indicates that preferences for care settings are shaped by kinship ties and gendered caregiving norms (Abel & Nelson, 1990; Kim et al., 2017; Liu, 2021; Rodrigues et al., 2023; Ueno, 1999). Spouses and adult children differ in their orientation toward institutional care (Freedman et al., 2014; Liu, 2021). Despite heavier caregiving burdens, spousal caregivers tend to favor home-based care to preserve emotional closeness and marital continuity (Pinquart & Sörensen, 2011), although transitions may occur abruptly due to their own age-related limitations (Wong et al., 2019).
Adult children, by contrast, assess care arrangements in terms of long-term feasibility, balancing caregiving with work and family demands (Kwak et al., 2012; Wang & Youderian, 2025). Consequently, they show a greater propensity to rely on formal or institutional care (Firgo et al., 2020; Savundranayagam et al., 2011). These differences highlight how kinship roles shape decisions to outsource care and navigate institutional transitions.
These patterns are further embedded in gendered expectations. Caregiving remains highly feminized, with women—wives, daughters, and daughters-in-law—providing the bulk of hands-on care, particularly in East Asian contexts (Carr & Utz, 2020; Grigoryeva, 2014; Lee, 2024; Ueno, 1999). Accordingly, scholars argue that “aging in place” tends to be more sustainable when daughters, rather than sons, assume primary caregiving roles (Firgo et al., 2020; Rodrigues et al., 2023).
Coresidence and Bargaining Power in Care Transitions
Traditionally, research has presupposed a coresidential model in which a spouse or adult child lives with the older adult to provide continuous, hands-on care (Labbas & Stanfors, 2023; Ma & Wen, 2016). However, as more older adults live independently, caregiving increasingly occurs across separate households or over long distances (Falzarano et al., 2022; Van der Pers et al., 2014). Coresiding caregivers typically provide intensive physical care, whereas non-coresiding or distance caregivers, often living more than an hour away, focus on coordinating care, monitoring, and providing financial support (Cagle & Munn, 2012; Labbas & Stanfors, 2023; Michielin & Mulder, 2007; Oh & Lee, 2025).
These distinct roles likely shape caregiving trajectories through different lenses. From a unitary household perspective, coresidence reflects family-level utility maximization, with care allocated based on opportunity costs in market and domestic labor (Gershuny & Robinson, 1988; Ma & Wen, 2016). In contrast, a bargaining perspective emphasizes negotiation; non-coresiding adult children may compensate for limited direct care with financial support, while coresiding caregivers gain greater influence over care arrangements and anticipate future reciprocity (Pezzin et al., 2015; Takagi & Silverstein, 2011). Building on these frameworks, this study examines whether coresidence shapes caregivers’ willingness to use institutional care, shedding light on how families navigate care transitions in contemporary Korea.
Methods
Data and Sample
This study utilized data from the 2019 Long-Term Care Survey (LTCS), a nationally representative survey conducted every 3 years by the National Health Insurance Service (NHIS) in South Korea. The LTCS provides comprehensive information on the living conditions, service utilization, and caregiving arrangements of older adults enrolled in the national Long-Term Care Insurance (LTCI) system, as well as the characteristics and experiences of their family caregivers (Kim et al., 2024).
The 2019 LTCS employed a two-stage stratified cluster sampling design to ensure national representativeness across regions and service types (Statistics Korea, 2020). Data were collected through structured, in-person interviews conducted by trained interviewers using standardized questionnaires.
The original dataset included responses from over 6,000 older adults receiving long-term care services and their caregivers (N = 5,606), who were identified as being most knowledgeable about care arrangements. For the present analysis, the sample was initially restricted to LTCI beneficiaries receiving home-based services (n = 2,749). To focus specifically on the perspectives of immediate family caregivers, we excluded cases where the survey was completed by the care recipient (n = 1,137), formal caregivers (n = 176), or extended kin (e.g., grandchildren or other relatives; n = 49). After further excluding cases with missing demographic information (n = 18), the final analytic sample consisted of 1,369 family caregivers (comprising 395 spouses and 974 adult children/children-in-law).
Measures
Willingness to Utilize Institutional Care
Caregivers’ willingness to utilize institutional care was assessed using the following item: “Would you consider placing the care recipient in a long-term care institution if their health condition were to deteriorate further?” Responses were dichotomized for the analyses (0 = willing to continue care at home, 1 = willing to utilize institutional care). This binary classification facilitates a clear distinction between caregivers committed to home-based care and those considering institutional transitions as a potential alternative in response to declining recipient health.
Care Recipient Characteristics
To capture the demographic and care-need profiles of the older adults, we included the care recipient’s gender (0 = male, 1 = female) and age (1 = 60–64 to 7 = 90+), marital status (0 = non-widowed, 1 = widowed), household type (0 = live with others, 1 = living alone), and residential location (0 = rural or small town, 1 = metropolitan area). The LTCI grade, ranging from 1 (most severe physical restriction) to 6 (mild physical and cognitive restriction), served as a proxy for the recipient’s functional limitations. Dementia diagnosis was included as a binary variable (0 = no diagnosis, 1 = diagnosed) to account for cognitive impairment. Furthermore, the frequency of hospitalization (i.e., annual number of admissions; range = 0–3) was utilized as an indicator of the care recipient’s overall health stability and medical needs.
Caregiver Characteristics
The caregiver relationship to the care recipient, originally recorded in detailed categories (e.g., spouse, son, daughter, and daughter-in-law), was recoded into three categories for analysis: (1) spouse, (2) adult child (son or daughter), and (3) child-in-law. The coresidence status was categorized into a binary variable (0 = coresiding, 1 = non-coresiding).
Regarding caregiver demographics, gender was coded as a binary variable (0 = male, 1 = female) and age was treated as a continuous variable (in years). Employment status indicated whether the caregiver was currently working (0 = not employed, 1 = employed). We also included whether the caregiver held a care worker certificate as a proxy for formal caregiving expertise. The monthly household income was measured on a 7-point ordinal scale (1 = less than 1,000,000 KRW to 7 = 6,000,000 KRW or more).
Care Contexts
To capture the threshold where caregiving becomes unsustainable during health declines, we measured both perceived burden and formal service utilization. Subjective caregiving burden was assessed across five domains: (a) emotional toll, (b) activities of daily living (ADL)-related toll, (c) instrumental activities of daily living (IADL)-related toll, (d) housework-related toll, and (e) financial strain. Each domain was rated on a 5-point Likert scale (1 = not at all burdensome to 5 = very burdensome), where a higher score indicates a greater perceived burden. Additionally, the monthly hours of formal care services, including service-visits to daycare and short-term respite care, were log-transformed to normalize the right-skewed distribution of the raw data.
Analytic Procedure
Data were collected using a stratified sampling design, with sampling weights applied to ensure representativeness. The analysis proceeded in three steps. First, descriptive statistics summarized sample characteristics across caregiver relationship types (spouse, adult child, and child-in-law) and coresidence status (categorized as coresiding vs. non-coresiding).
Second, logistic regression models estimated predictors of willingness to use institutional care, incorporating care recipient characteristics (e.g., demographics and health), caregiver characteristics (e.g., relationship, living arrangement, and socioeconomic factors), and care context variables (e.g., caregiving burden and formal service use).
Third, subgroup analyses examined the interaction between relationship type and coresidence by estimating adjusted odds ratios (AORs) for the resulting five caregiver groups, using coresiding spouses as the reference. To further isolate coresidence effects among adult children, models were re-estimated with coresiding adult children as the reference group.
Results
Descriptive Statistics of Study Variables by Caregivers’ Relationship Type
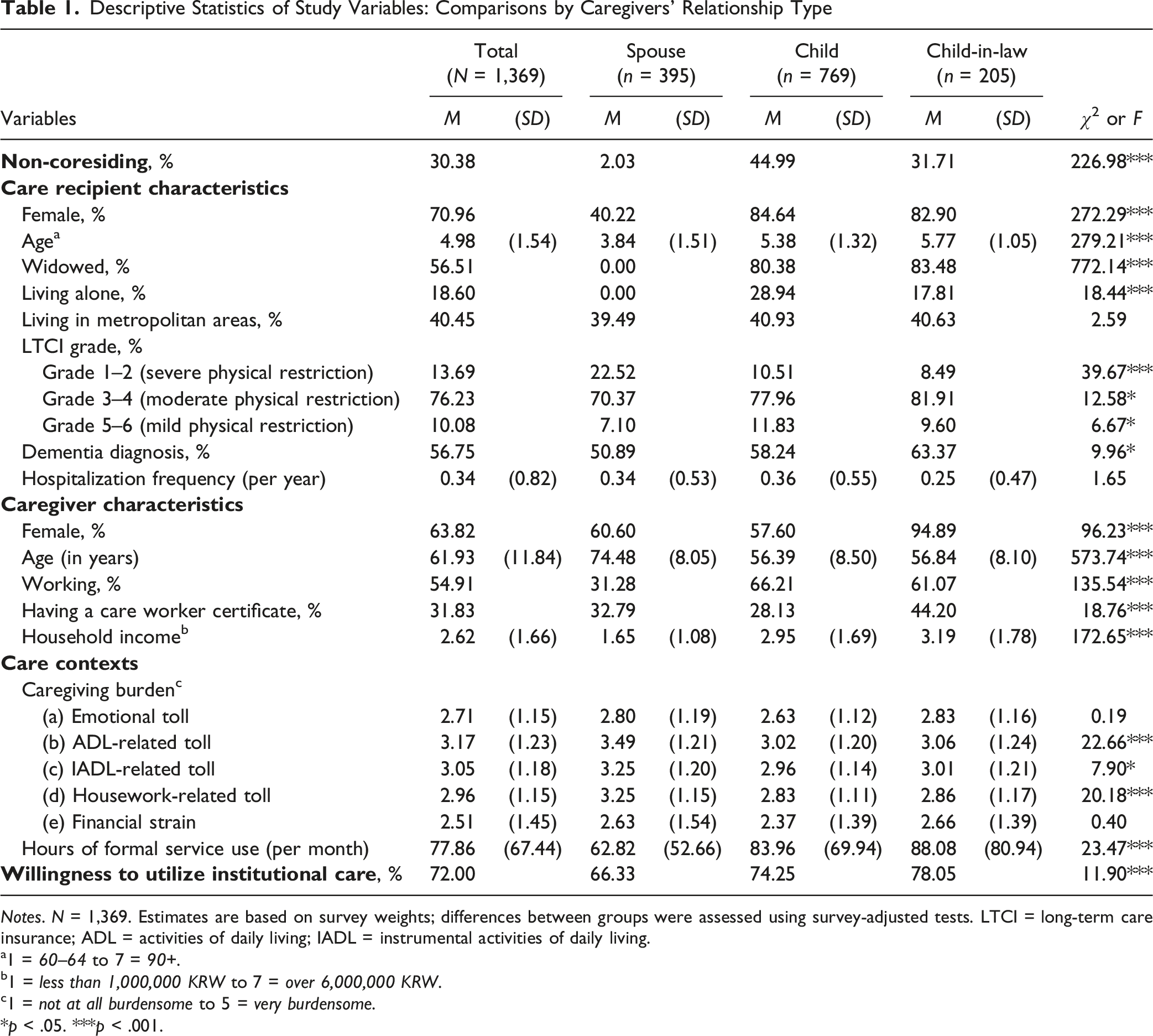
Descriptive Statistics of Study Variables: Comparisons by Caregivers’ Relationship Type
Notes. N = 1,369. Estimates are based on survey weights; differences between groups were assessed using survey-adjusted tests. LTCI = long-term care insurance; ADL = activities of daily living; IADL = instrumental activities of daily living.
a1 = 60–64 to 7 = 90+.
b1 = less than 1,000,000 KRW to 7 = over 6,000,000 KRW.
c1 = not at all burdensome to 5 = very burdensome.
*p < .05. ***p < .001.
Care recipient profiles also differed across groups. The majority of care recipients (71%) were female. Among spousal caregivers, care was more often provided by wives to husbands, as only 40% of recipients were wives. The average age category of care recipients was 4.98, which corresponds to the 80–84 age category. On average, recipients cared for by spouses were younger (age category = 3.84) compared to those cared for by adult children (age category = 5.38) or children-in-law (age category = 5.77). Approximately 40% of recipients resided in metropolitan areas. Overall, 19% of care recipients lived alone; this proportion was higher among those cared for by adult children (29%), compared to those cared for by children-in-law (18%).
Health profiles of recipients further distinguished the groups. Recipients cared for by spouses (23%) were more likely to present severe physical restrictions (Grades 1–2), compared to those cared for by adult children (11%) or children-in-law (8%). In contrast, adult children and children-in-law were more frequently involved in care for recipients with moderate (Grades 3–4) to mild (Grades 5–6) physical restrictions than spouse caregivers. Furthermore, while over half of all care recipients (57%) had a dementia diagnosis, the prevalence was significantly higher among those cared for by adult children (58%) or children-in-law (63%) than among those cared for by spouses (51%).
Caregivers were predominantly female (64%); 61% of spouses, 58% of adult children, and 95% of children-in-law were female. The mean age of caregivers was 61.93 years (SD = 11.84), with spouses being significantly older than the other two groups. Employment rates were highest among adult children (66%) and children-in-law (61%), whereas only 31% of spouses were active in the labor market. Nearly one-third (32%) of caregivers held a care worker certificate, with children-in-law showing a slightly higher prevalence (44%). The mean household income was 2.62 (SD = 1.66), with children-in-law reporting the highest income and spouses reporting the lowest.
Consistent with these differences, spouses reported the highest burden for ADL (M = 3.49), IADL (M = 3.25), and housework (M = 3.25). The emotional toll and financial strain were similar across groups. In contrast, formal service use (hours per month) followed the opposite pattern, with the highest utilization among children-in-law (M = 88.08 hours) and the lowest among spouses (M = 62.82 hours).
When asked about caregivers’ willingness to utilize institutional care in the event of worsening health of the care recipient, a significant majority of caregivers (72%) expressed a preference for institutional care, while 28% preferred continuing in-home care. This willingness was lower among spouses (66%) than among adult children (74%) and children-in-law (78%).
Descriptive Statistics of Study Variables by Caregivers’ Coresidence Status
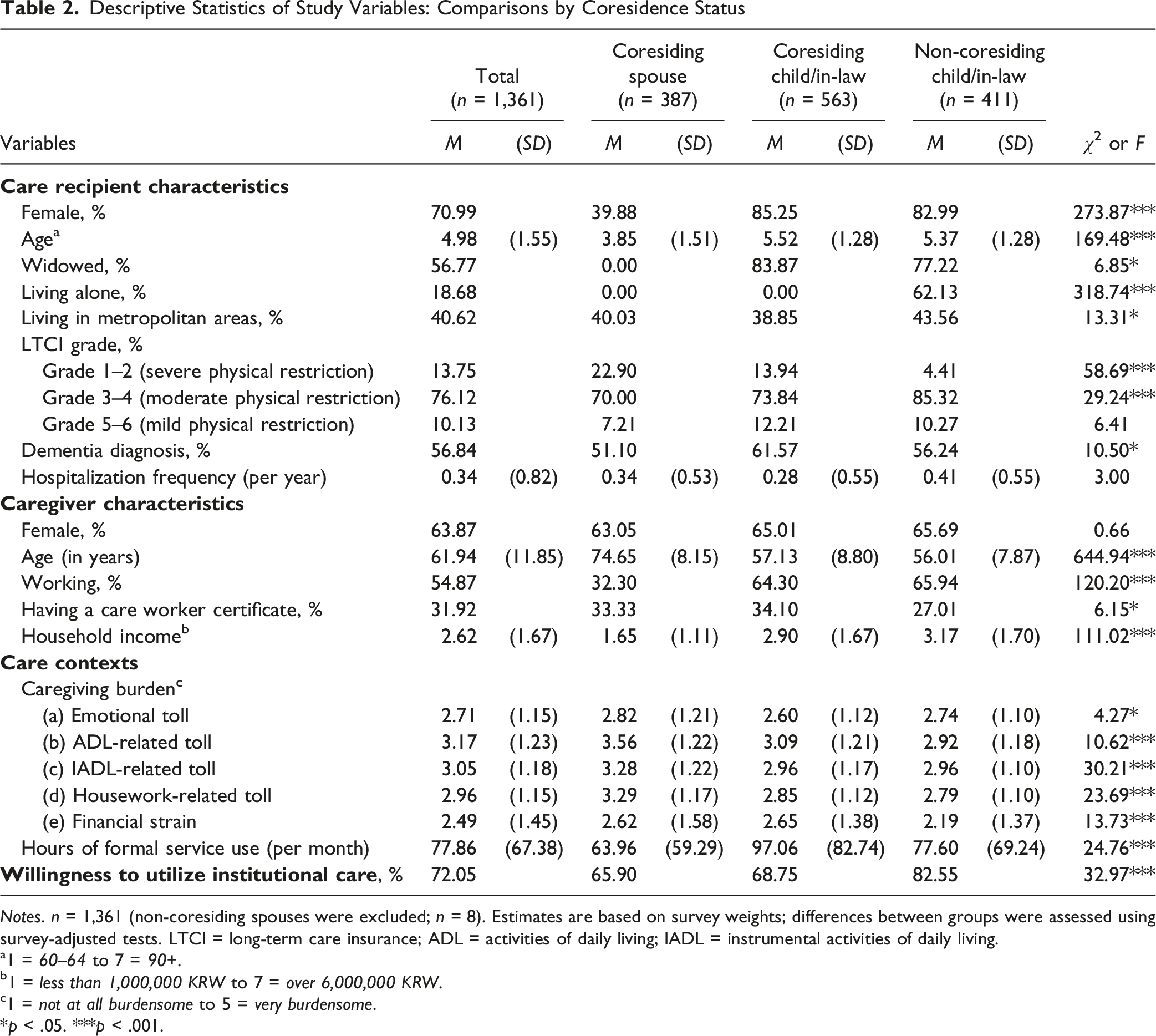
Descriptive Statistics of Study Variables: Comparisons by Coresidence Status
Notes. n = 1,361 (non-coresiding spouses were excluded; n = 8). Estimates are based on survey weights; differences between groups were assessed using survey-adjusted tests. LTCI = long-term care insurance; ADL = activities of daily living; IADL = instrumental activities of daily living.
a1 = 60–64 to 7 = 90+.
b1 = less than 1,000,000 KRW to 7 = over 6,000,000 KRW.
c1 = not at all burdensome to 5 = very burdensome.
*p < .05. ***p < .001.
Caregivers’ sociodemographic characteristics also differed by coresidence status. Non-coresiding caregivers were generally younger and more likely to be employed than their coresiding counterparts. Caregiving expertise varied, with care worker certificates held by 34% of coresiding children/children-in-law, 33% of spouses, and 27% of non-coresiding caregivers. Household income followed a clear gradient; non-coresiding caregivers reported the highest household income, while coresiding spouses reported the lowest. Coresiding caregivers, particularly spouses, reported the highest levels of burden across domains, including emotional, ADL, IADL, housework, and financial domains, while non-coresiding caregivers reported relatively lower burden levels.
Predictors of Caregivers’ Willingness to Utilize Institutional Care
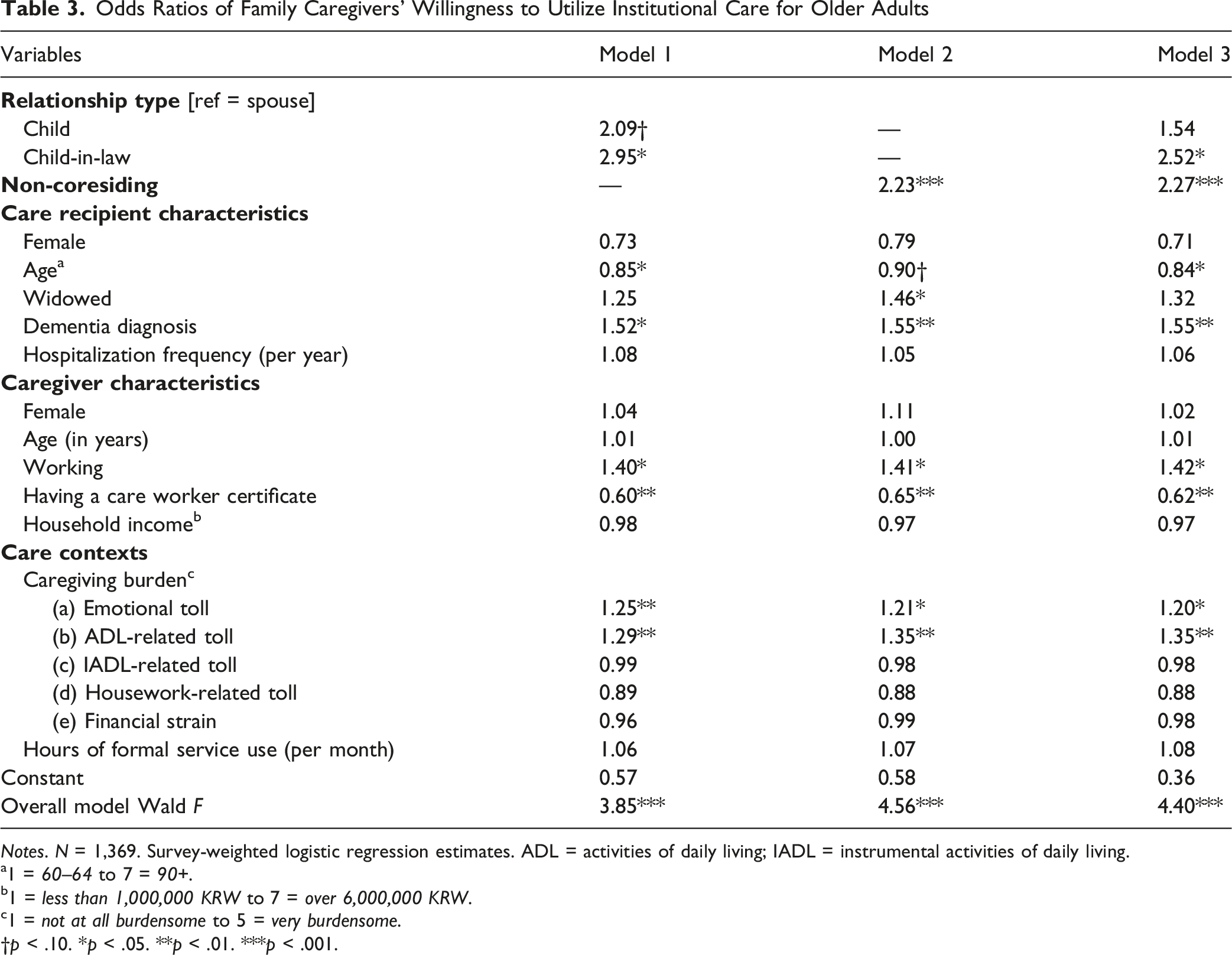
Odds Ratios of Family Caregivers’ Willingness to Utilize Institutional Care for Older Adults
Notes. N = 1,369. Survey-weighted logistic regression estimates. ADL = activities of daily living; IADL = instrumental activities of daily living.
a1 = 60–64 to 7 = 90+.
b1 = less than 1,000,000 KRW to 7 = over 6,000,000 KRW.
c1 = not at all burdensome to 5 = very burdensome.
†p < .10. *p < .05. **p < .01. ***p < .001.
Among care recipient characteristics, dementia diagnosis emerged as a robust predictor of higher willingness to utilize institutional care (OR = 1.52–1.55). Older age in the recipient was associated with lower odds of considering institutionalization (OR = 0.84–0.90). Widowhood was associated with a higher willingness only in Model 2 (OR = 1.46, p = .048), but this effect did not reach statistical significance in other models. Notably, recipient gender and hospitalization frequency did not show statistically significant associations with caregivers’ willingness to utilize institutional care.
Among caregiver’s characteristics, employed caregivers showed higher odds of considering placing the care recipient in an institution (OR = 1.40–1.42). However, if the caregiver held a care worker certificate, the chances of considering the institutional care were significantly lower (OR = 0.60–0.65). Across the models, perceiving a greater emotional toll (OR = 1.20–1.25) or ADL-related toll (OR = 1.29–1.35) was also associated with a higher likelihood for considering institutional care.
Interactions Between Relationship Type and Coresidence Status
Figure 1a illustrates the interaction effects between caregiver relationship and coresidence status on the willingness to utilize institutional care. Using coresiding spousal caregivers as the reference group (OR = 1.00), the analysis revealed stark disparities across adult child and in-law caregiver subgroups, excluding the non-residing spouse group. Non-coresiding adult children were nearly three times more likely to express willingness to utilize institutional care (AOR = 3.18, p < .001), whereas their coresiding counterparts did not differ significantly from the reference group (AOR = 1.45, p = .36). The most pronounced effect was observed among non-coresiding children-in-law, whose odds of endorsing institutional care were more than seven times higher than those of coresiding spouses (AOR = 7.19, p < .001). Although coresiding children-in-law also showed a higher propensity for institutional care (AOR = 2.15, p = .090), this association did not reach statistical significance. Adjusted Odds Ratios of Family Caregivers’ Willingness to Utilize Institutional Care for Older Adults: Comparisons by Caregivers’ Relationship Type and Coresidence Status. a. Reference = coresiding spouse; N = 1,369. b. Reference = coresiding child; n = 974 (excluding 395 spouses). Notes. Survey-weighted logistic regression estimates. ***p < .001.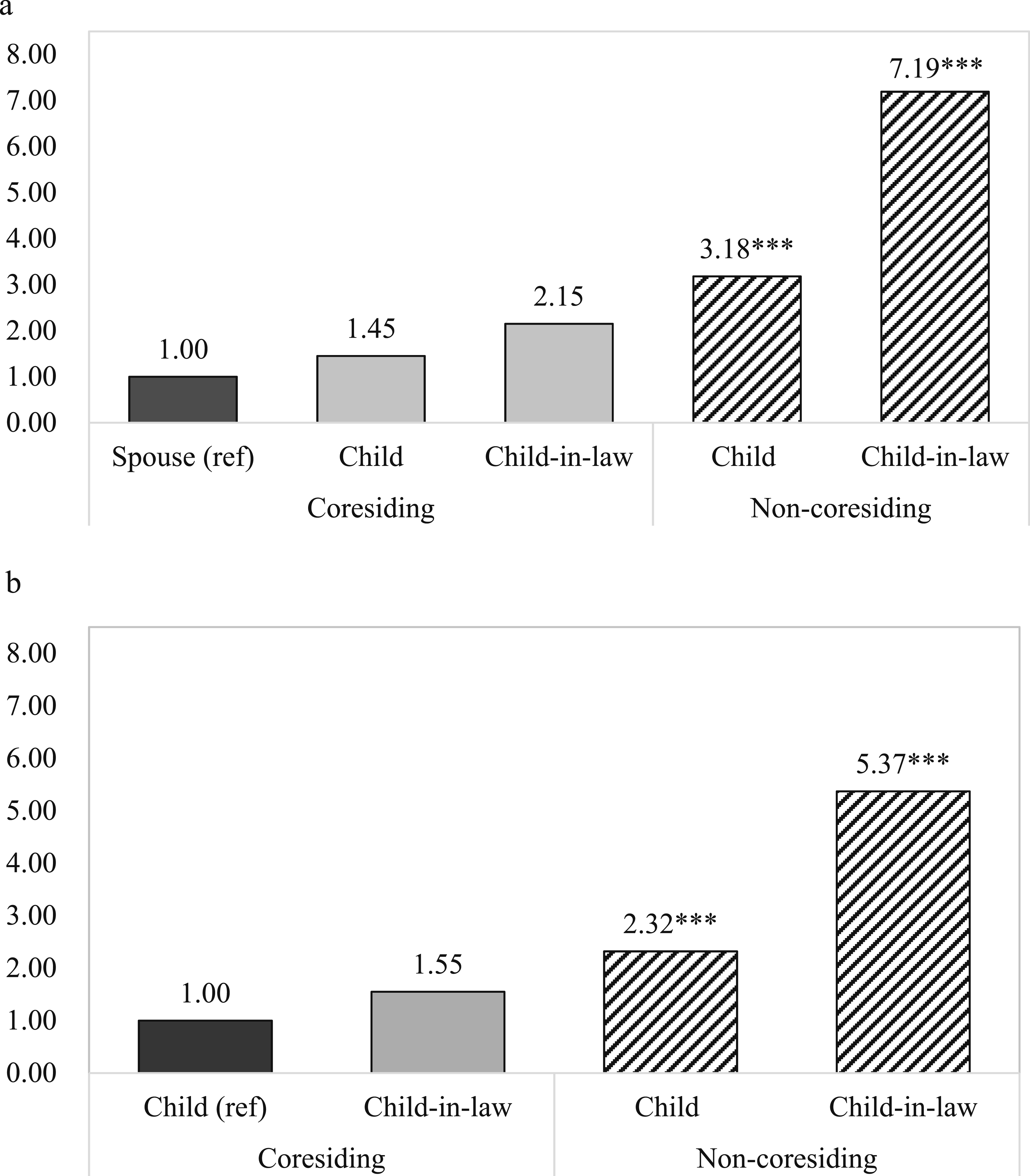
Figure 1b further examines these dynamics by using coresiding adult children as the reference group (OR = 1.00) to isolate the effect of coresidence status within the adult-child generation. The results demonstrate that non-coresiding adult children were more than twice as likely to express willingness to utilize institutional care, compared to their coresiding counterparts (AOR = 2.32, p < .001). In contrast, non-coresiding children-in-law exhibited the highest odds of willingness to utilize institutional care (AOR = 5.37, p < .001), whereas coresiding children-in-law did not differ significantly from coresiding adult children (AOR = 1.55, p = .095).
Discussion
This study investigated the complex interplay between living arrangements and kinship ties in shaping family caregivers’ willingness to utilize institutional care under South Korea’s LTCI. Our findings indicate a distinct demographic and structural divide in caregiving arrangements: spousal care is predominantly coresidential and concentrated on severe physical limitations, whereas nearly half of adult children provide care across separate households, frequently in response to cognitive impairments. The multivariate analyses demonstrated that non-coresiding adult children were more than twice as likely to favor institutional care as their coresiding counterparts, regardless of whether the adult children were biological or children-in-law. This suggests that the challenges of long-distance caregiving may outweigh traditional gender roles or economic capacity, indicating that the feasibility of “aging in place” is increasingly shaped by the spatial organization of the family. However, our measure does not capture meaningful variation in distance, and future research with more precise measures is needed.
A central contribution of this study is to highlight the salience of the spatial context of caregiving (i.e., how care occurs) rather than the caregiver-recipient relationship (i.e., who provides care). Prior research has emphasized gender and kinship, particularly the contrast between spousal devotion and filial obligation (Firgo et al., 2020; Ueno, 1999; Wong et al., 2019). In contrast to prior studies, where female caregivers often comprise over 90% of the sample, our data include a substantial proportion of male caregivers (37%), enabling a more balanced gender comparison. Within this context, we find that when situational constraints are comparable, such as living apart, preferences for institutionalization converge across gender. This pattern suggests that the observed lack of gender differences is driven more by the caregiving context than by sample composition. In turn, these findings call into question the assumption that women (wives or daughters) are inherently more committed to sustaining in-home care (Grigoryeva, 2014; Ueno, 1999).
Specifically, coresidence acts as a powerful commitment mechanism, particularly for adult children. Coresiding adult children, including children-in-law, showed a stronger preference for continuing in-home care, displaying a pattern similar to that of spouse caregivers. Notably, this preference persists despite higher reported levels of burden. In our sample, care recipients receive 3-hour in-home visiting care or have access to day care services. Within this context, sharing a household may foster a sense of obligation (e.g., “co-destiny”) that sustains home-based care. This dynamic may override individual demographic factors often emphasized in caregiving research. Although emotional and ADL-related toll increased willingness to utilize institutional care, their effects did not surpass the robust influence of coresidence. This suggests that coresidence status serves as a primary lens through which burden is interpreted. Coresiding caregivers may develop deeper emotional ties, which can shift their perspective from burden perception to empathetic understanding (Liu, 2021; Rodrigues et al., 2023; Wong et al., 2019). As a result, institutionalization may be viewed as a “last resort,” even under substantial caregiving demands.
In contrast, non-coresiding adult children, who are more likely to be employed, tend to treat caregiving as a distinct responsibility rather than an embedded part of daily life. From a household economic perspective (Gershuny & Robinson, 1988), they are more likely to prioritize labor market participation, making sustained involvement in intensive care less feasible. Holding a care worker certificate may partially offset this constraint by allowing caregivers to combine paid caregiving with employment, thereby reducing the opportunity costs of involvement. However, even after controlling for certification, non-coresiding adult children remained more likely to consider institutional care, suggesting that employment-related constraints are not fully mitigated. As care needs intensify, institutional care may therefore emerge as a more practical alternative than restructuring daily life to accommodate coresidence or intensive home-based care (Verbakel et al., 2024). This pattern aligns with intra-family bargaining frameworks emphasizing unequal caregiving responsibilities and decision-making power (Pezzin et al., 2015). Our findings extend this perspective by showing that coresidence structures these dynamics, with coresiding caregivers more likely to sustain in-home care and non-coresiding members more likely to favor institutional solutions.
Several limitations warrant consideration. First, the cross-sectional design limits causal interpretation, as residential proximity may reflect a strategic response to evolving care needs rather than a fixed determinant (Reyes & Shang, 2024). Longitudinal research is needed to capture these dynamic transitions. Second, the data do not distinguish between primary and secondary caregivers. Although the survey identified the most knowledgeable family member, it remains unclear whether this individual was the primary caregiver, and the extent of support from other family members could not be assessed. As such, differences in caregiving intensity and duration may shape willingness to utilize institutional care in ways not captured in our analysis. Third, non-coresiding spousal caregivers were excluded from subgroup analyses due to a small sample size, which may limit generalizability. Finally, the data do not allow for variation in residential proximity among non-coresiding caregivers; future research should move beyond a binary distinction to better capture distance-related differences.
Conclusion and Implications
As demographic shifts increasingly place adult children at a distance from their aging parents, caregiving is becoming more spatially dispersed. Non-coresiding children, particularly those engaged in the labor market, are more likely to view institutional care as a necessary and acceptable option as care needs intensify. When caregiving must be balanced with employment across households, the sustainability of “aging in place” may be undermined. Despite the expansion of formal services, caregiving responsibilities remain heavily concentrated among coresiding family members, especially spouses and coresiding children or children-in-law, who bear substantial physical and emotional burdens.
Our findings underscore the need for long-term care policies and community-based care frameworks that better reflect the diverse living arrangements of older adults. Current policy frameworks often prioritize older adults living alone, focusing on social isolation and service provision, while implicitly assuming that those living with family (e.g., spouse or adult children) have adequate support. As a result, coresiding households are frequently excluded from targeted policy attention, despite the significant burden on family caregivers. Moreover, there is limited policy guidance on how to support residential transitions when the health of coresiding older adults declines. Coresiding family members should therefore not be treated as “natural” providers, but as critical care resources requiring targeted support to prevent burnout (Van der Pers et al., 2014). Incorporating living arrangements into care planning will be essential for responding to the evolving realities of aging in Korea.
Footnotes
Ethical Consideraion
Institutional Review Board at Dongduk Women’s University approved this study as exempts from review (DDWU2510-01).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the research grant of The University of Suwon in 2024 (U2024-0147).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The current study drew on data from the 2019 Korean Long-Term Care Surveys, which are publicly available on the website of Microdata Integrated Service (![]() ). The data we used for analysis and our analytic methods are described in detail in the text, and will be made available to other researchers upon request. This study did not involve clinical trials and was not pre-registered.
). The data we used for analysis and our analytic methods are described in detail in the text, and will be made available to other researchers upon request. This study did not involve clinical trials and was not pre-registered.