
Abstract
This study examined psychosocial factors associated with help-seeking intentions if and when a family member developed Alzheimer’s disease (AD) among American Indian populations, focusing on gender differences. Guided by Andersen’s behavioral model of health service use, predisposing, enabling, and need factors were considered as potential sources for AD help-seeking intentions. Multivariate regression analyses were conducted on a sample of 226 American Indian adults residing in South Dakota. Subjective norms and family support were positively associated with help-seeking intentions for both men and women. Gender differences emerged. American Indian women were more likely than men to intend to seek help for a family member with AD if the need arose, while self-confidence in completing medical forms was positively associated with help-seeking intentions among American Indian men only. Identifying common and gender-specific AD intervention strategies can promote timely help-seeking and improve treatment outcomes in American Indian communities.
Keywords
• To the best of our knowledge, this is the first study of American Indian populations to provide insights into gender differences in help-seeking intentions for family members with AD and psychosocial factors underlying these intentions. • Gender is a crucial factor in seeking AD-related healthcare services for families with AD among American Indian adults.
• The findings can inform the development of both general and gender-specific AD preventions, caregiving support services, and interventions that address gaps in dementia care in American Indian communities. • AD-related healthcare services for American Indian adults should be tailored to address gender differences, Indigenous cultural beliefs and norms, and facilitators and barriers to utilizing dementia care among these populations.What This Paper Adds
Applications of Study Findings
Introduction
Dementia refers to a group of symptoms affecting memory, behaviors, and cognitive functioning, and social abilities that interfere with one’s daily life (Alzheimer’s Association, 2019). Alzheimer’s disease (AD) is the leading cause of dementia, constituting 60–80% of total dementia cases, and is the most rapidly increasing cause of death globally
Among American Indian (AI) populations, AD is significantly underdiagnosed and underreported (Garvey et al., 2011). As of 2021, AIs constitute about 9.7 million people across 574 federally recognized tribes in the U.S. (Indian Country Today, 2022). While AI communities are diverse, they share elevated rates of AD risk factors, including limited physical activity, low socioeconomic status, hypertension, type 2 diabetes, obesity, smoking, and high cholesterol (Anstey et al., 2011; Marden et al., 2017; Ronnemaa et al., 2011; Wilson et al., 2013). Shifting demographics have made AD more prevalent in AI communities than in the past. In the 1970s, 4.8% of the AI population was aged 65 or older; today, 15% is aged 65 or older. With increasing life expectancy, the number of AIs living with AD is expected to quadruple by 2050 (Apostolou et al., 2024).
Despite these projections and heightened risks, little attention is paid to AD healthcare service utilization in AI populations (Jervis & Manson, 2002). While help-seeking for AD healthcare services is critical for early diagnosis, improves the identification of at-risk individuals, and leads to better outcomes (Galvin et al., 2008), research indicates that AIs often underutilize conventional healthcare services (Hartmann & Gone, 2012), posing a critical barrier to early detection and adequate treatment. Given that help-seeking intention is an important precursor of actual healthcare use (Galvin et al., 2008), promoting help-seeking intentions is essential. To address this gap, the current study applies Andersen’s (1995) behavioral model of health service use—one of the most widely used help-seeking frameworks—which categorizes multilevel factors influencing healthcare use into predisposing, need, and enabling factors (Holde et al., 2018; Jiang et al., 2020; Lee et al., 2020).
Women are disproportionately affected by AD, both as patients and caregivers. They account for 70% of AD caregiving and face higher rates of disability-adjusted life years and mortality from dementia (World Health Organization, 2024). Women are also more likely than men to seek help when facing stressful events (Mo & Mak, 2009; National Alliance for Caregiving & Alzheimer’s Association, 2017). Gender disparities in caregiving often reflect gender role socialization and women’s historically greater involvement in family responsibilities, despite growing female labor-market participation and increased male involvement in caregiving (Barzallo et al., 2024). Demographic patterns contribute as well—women tend to live longer and are more likely to assume caregiving for spouses or relatives. However, little is known about factors influencing AIs’ intentions to seek AD-related healthcare and how these may be similar or differ by gender. A better understanding of common and gender-specific factors that influence AD help-seeking intentions in AI populations can guide targeted interventions to improve early diagnosis, screening, and prognosis.
Alzheimer’s Disease Among American Indians
AD studies among racial/ethnic minority populations are largely lacking, particularly with AIs (Suchy-Dicey et al., 2024). However, existing work in AI populations offers useful baseline evidence of high levels of AD in this group
Factors Associated With Help-Seeking for Alzheimer’s Disease Among American Indians
While limited, research findings consistently indicate a complex interplay of individual, cultural, and structural factors that affect AIs’ intentions to seek AD-related healthcare services (Sehar et al., 2023). These often include low socioeconomic status, limited knowledge about AD, logistic factors (e.g., inadequate health insurance, geographic isolation, transportation), traditional health beliefs and stigma, and systematic/structural inequities (e.g., limited access to specialized care, unmet healthcare needs, mistrust of healthcare systems) (Griffin-Pierce et al., 2008; Lewis et al., 2021). Attitudes and perceptions play a pivotal role in healthcare service engagement for AD. Allick and Bogic (2024) explored perceptions of cognitive decline among AI and Alaska Native elders. Roughly 75% of respondents believed cognitive decline was an inevitable part of aging. AI and Alaska Natives’ reluctance to frame memory loss as a medical issue, rather than a normal part of aging, reflects a potential barrier to seeking preventive care or intervention leading to delayed diagnosis and treatment for AD. Crouch et al. (2023) indicated that stigma is one of the most influential factors influencing AI’s reluctance to seek services for AD and related dementias.
Gender Differences in Caregiving and Help-Seeking for Alzheimer’s Disease
The gender gap in AD help-seeking behaviors is pronounced and shaped by traditional gender roles and stigmas surrounding the disease in general populations (Barzallo et al., 2024; Sharma et al., 2016). Research on AD-related stigma reveals that both men and women may experience shame or reluctance to seek care due to societal misunderstandings of the disease (Gove et al., 2016). However, women, often in caregiving roles, are more likely to seek formal help, reflecting their openness and active engagement in caregiving tasks. In contrast, men often delay seeking medical attention for loved ones or themselves, influenced by stigma and cultural barriers tied to AD (Goetz et al., 2023). These gendered patterns align with broader trends in caregiving and health service utilization. Women, as both caregivers and recipients of care, engage more actively with healthcare systems, while men’s caregiving roles and help-seeking behaviors are often constrained by cultural expectations of self-reliance and emotional suppression. Although AI caregivers may share common challenges with other caregiving populations, such as heightened stress and financial strain, AI women are likely to be disproportionately affected by AD caregiving roles compared with women in general (Sehar et al., 2023). This is partly due to their higher likelihood of assuming caregiving responsibilities, influenced by cultural values that emphasize family dependence (Jervis & Manson, 2002), as well as limited access to community support (Strachan & Buchwald, 2023). More research is needed to explore gender variations within AI populations.
Theoretical Framework and Hypotheses
For this study, we used the behavioral model of health service use as a conceptual framework (Andersen, 1995). The model provides a theoretical structure to conceptualize health service access and use. This model helps identify a range of key factors that facilitate or impede a person’s use of health service, categorizing them into three main constructs: predisposing, need, and enabling factors. Predisposing factors refer to individual-level characteristics, such as demographics and social structure, which influence an individual’s likelihood of using health services. These are often operationalized through proxy variables, such as age. Need factors are one’s perceptions or assessment of their healthcare needs, which motivate people to seek care. These factors include personal health concerns, as well as broader influences, such as social norms and cultural acceptance, that would indicate the need for service use. Enabling factors include both individual and community level resources that assist people to access healthcare services (e.g., financial resources, social support).
In applying the model to AI populations, it is recommended that the unique situational, social, and cultural factors specific to these communities be addressed (Lee et al., 2020). The core principles of AI wellness and healing are deeply rooted in ancient traditions revolving around harmony and balance between body (physical), mind (mental and emotional), and spirit (spiritual) (Koithan & Farrell, 2010; Napoli, 2002). In their holistic approach to wellness, AIs may seek natural remedies to improve health, encompassing a wide range of interrelated behaviors, such as use of herbal medicine, sweat lodges, and energy work and sound healing (e.g., drumming and chanting). Research has shown that many Indigenous individuals prefer traditional healing practices over conventional biomedical healthcare, despite considerable variations among tribes and regions (Gone & Trimble, 2012; Walls et al., 2006). Traditional wellness approaches may not deter using Western medical services, but rather the two complement each other (Baines, 2012; Buchwald et al., 2000), which may, in turn, increase professional help-seeking.
Guided by Andersen’s (1995) behavioral model of health service use, this study examined three sets of psychosocial factors (predisposing, need, and enabling) associated with AIs’ intentions to seek healthcare for family members with AD if the need should arise, focusing on gender differences. We targeted the AI general public, exploring the intention of men and women to seek AD-related care for a family member, to understand broader community perspectives on AD help-seeking. We hypothesized that: • Hypothesis 1: AI women would score higher on help-seeking intentions for family with AD than AI men. • Hypothesis 2: Gender differences would exist in how three sets of psychosocial factors are associated with help-seeking intentions for family with AD: (1) predisposing factor (age), (2) need factors (cultural orientation, perceived stigma, and subjective norms), and (3) enabling factors (self-confidence in completing medical forms, family support, and dementia knowledge).
Methods
Sample and Data Collection
This study was undertaken with the guidance of a Community Advisory Board, consisting of AI community elders, healthcare service professionals, and AI researchers. The Community Advisory Board members engaged early in the research process and guided all aspects of study, including the initial planning, development, implementation, and dissemination of research findings. They initially met during the planning phase, and then met quarterly to provide input and community perspectives, assist in recruitment strategies, and ensure cultural and local relevance. The Community Advisory Board members received $50 compensation.
We used a cross-sectional, paper-based survey of AIs aged 18 years or older living in South Dakota, including Sioux Falls, Vermillion, and Brookings, where large, regular Indigenous celebrations attract participants from diverse AI tribes. Participants were recruited using a convenience sampling strategy through a variety of recruiting sources including three powwows (regular celebrations of AI culture and heritage across diverse Indigenous nations), AI churches, other religious organizations, social service centers, referrals, and word of mouth between March and April in 2022. Inclusion criteria for study participation included: (1) self-identified AI men and women, (2) 18 years of age or older, (3) born/raised in tribal areas or reside in South Dakota, and (4) demonstration of sufficient cognitive ability to understand and complete the survey (determined by the Short Portable Mental Status Questionnaire). South Dakota is home to nine tribes (South Dakota Department of Tribal Relations, 2025), making it a valuable setting for region-specific research. This allows for the collection of data that is locally and regionally relevant and also broad enough to capture diverse perspectives within the AI population. Individuals who were interested in participating in the study directly contacted the principal investigator (first author). A total of 250 AI adults participated in the survey. Twenty-four participants who had more than 10% of missing data were excluded, leading to a final sample of 226 AI adults.
Institutional Review Board approval was obtained prior to data collection from the principal investigator’s university. A survey was scheduled and conducted at the participants’ preferred locations (e.g., participants’ home, researcher’s office, conference room in powwows). Prior to the survey, all participants provided signed informed consent. The self-administered survey took approximately 20–30 minutes to complete. Each participant completed the survey individually and received a $13 gift card for participating.
Measures
Dependent Variable
Help-Seeking Intentions for Family With AD
The help-seeking intention for family with AD, in the event that a family member becomes ill with AD, was measured using a three-item scale adapted from the Help-Seeking Intention Scale (Mo & Mak, 2009), which was developed with reference to the Ajzen’s (2002) guidelines for constructing a theory of planned behavior questionnaire. Mo and Mak’s original Help-Seeking Intention Scale assessed individuals’ intentions to seek mental health care was used with a Chinese sample in Hong Kong. For our study, we modified the scale by replacing the term “mental health service” with “AD healthcare service professionals” and by reframing the questions to focus on seeking care for a family member in the event they become ill with AD. The three-item questions include: “I intend to seek healthcare service professionals for my family with AD (including primary care physicians and AD specialists)” “I will try to seek healthcare service professionals for my family member with AD” and “I plan to seek healthcare service professionals for my family member with AD.” The items were measured by a four-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree), where higher scores indicated stronger intentions to seek AD healthcare services. The total score of the three items was calculated, yielding a range from three to 12. The internal consistency reliability for the scale was high with the present sample (Cronbach’s alpha = 0.88).
Independent Variables
Predisposing Factors
Age
Participants’ age was measured in years.
Need Factors
Cultural orientation
A single item asked, “How much do you identify with your own tribal traditions?” The original response options (0 = “not at all,” 1 = “little,” 2 = “some,” and 3 = “a lot”) were dichotomized to reflect whether participants culturally identified as “at least partially Indigenous” (1) or “not Indigenous” (0).
Perceived stigma
We used a 10-item STIG-MA Scale (Piver et al., 2013) to assess perceived stigma against AD. The questions examined several dimensions of perceived stigma: reluctance to disclose illness, fear of exclusion, courtesy stigma, and fear of loss of family support. The question “If you were suffering from Alzheimer’s disease….” initiated the exploration of feelings of participants. Sample items include: “Would you rather people do not know about your disease?” and “Do you think others would avoid you because of the disease?” The 10-items were measured by a four-point scale ranging from 0 (no) to 3 (yes) with lower scores indicating lower perceived stigma. The negatively worded items were reverse-coded. The total summed score for the 10-items ranged from 0 to 30. The internal consistency reliability for the scale was 0.79 with the present sample.
Subjective norms
Subjective norms were measured using two questions adapted from the Subjective Norms Scale (Mo & Mak, 2009), which was developed in accordance with Ajzen’s (2002) guidelines for developing theory of planned behavior-based questionnaires. The original Mo and Mak scale assesses one’s perceptions and expected behaviors that are important to people regarding mental health service use. In this study, we modified the scale to focus on “AD healthcare service use.” The modified questions in the present study asked about participants’ planning about care in the event that their family member(s) become ill with AD. The questions include: “Most people who are important to me think that I should consult with healthcare service for my family member with AD” and “Most people who are important to me will seek AD healthcare service if they are in need.” Responses were recorded on a four-point Likert scale, ranging from 1 (strongly disagree) to 4 (strongly agree), with higher scores indicating more positive perceptions of social norms around seeking AD care. The total summed score for the two items ranged from 2 to 8. The internal consistency reliability of this measure was 0.70.
Enabling Factors
Self-confidence in completing medical forms
To assess AI participants’ perceived self-confidence in seeking AD healthcare services, they were asked to rate an investigator-generated single item on a five-point Likert scale: “How confident are you filling out medical forms by yourself?” (0 = not at all, 4 = extremely). Higher scores reflected a greater level of self-confidence in completing medical forms.
Family support
The Multidimensional Scale of Perceived Social Support (Zimet et al., 1988) was used to assess the perceived level of social support with family. The original scale includes 12 items which cover three dimensions: family, friends, and significant others. We used four questions to assess a family support domain (e.g., “My family really tries to help me,” and “I get the emotional help and support I need from my family.”). The scale had a four-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). A total score was computed by summing the four items. Overall scores ranged from 4 to 16 with higher scores representing higher levels of family support. The internal consistency reliability of this measure was high with the present sample (Cronbach’s alpha = 0.93).
Dementia knowledge
The 10-item Dementia Knowledge Subscale was used to measure dementia knowledge, which is a subscale of the 20-item Dementia Attitudes Scale (O’Connor & McFadden, 2010). The Subscale of Dementia Knowledge assesses participants’ knowledge and beliefs regarding the capabilities of individuals with dementia and asked questions, such as “People with AD can enjoy life,” “It is possible to enjoy interacting with people with AD,” and “People with AD can feel when others are kind to them.” Response options were scored on a seven-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Summative scores were computed, ranging from 10 to 70, indicating higher scores reflecting greater dementia knowledge. The Cronbach’s alpha of the scale was 0.91 in the present study.
Analytic Strategy
Our strategy was organized in three parts. First, descriptive statistics summarized the sample characteristics by gender. Second, we used chi-square to examine associations between key variables and independent samples t-tests to assess differences in key variables between males and females. Third, we conducted linear regression analyses to examine the associations between predisposing, need, and enabling factors and help-seeking intentions for AD healthcare using the total sample (Model 1) and then by gender (Model 2 and Model 3). No multicollinearity problems were observed among the independent variables since variance inflation factor (VIF) scores were all below 1.29 (Mertler & Vannatta, 2002). This study used IBM SPSS Statistics version 28 for data analyses.
Results
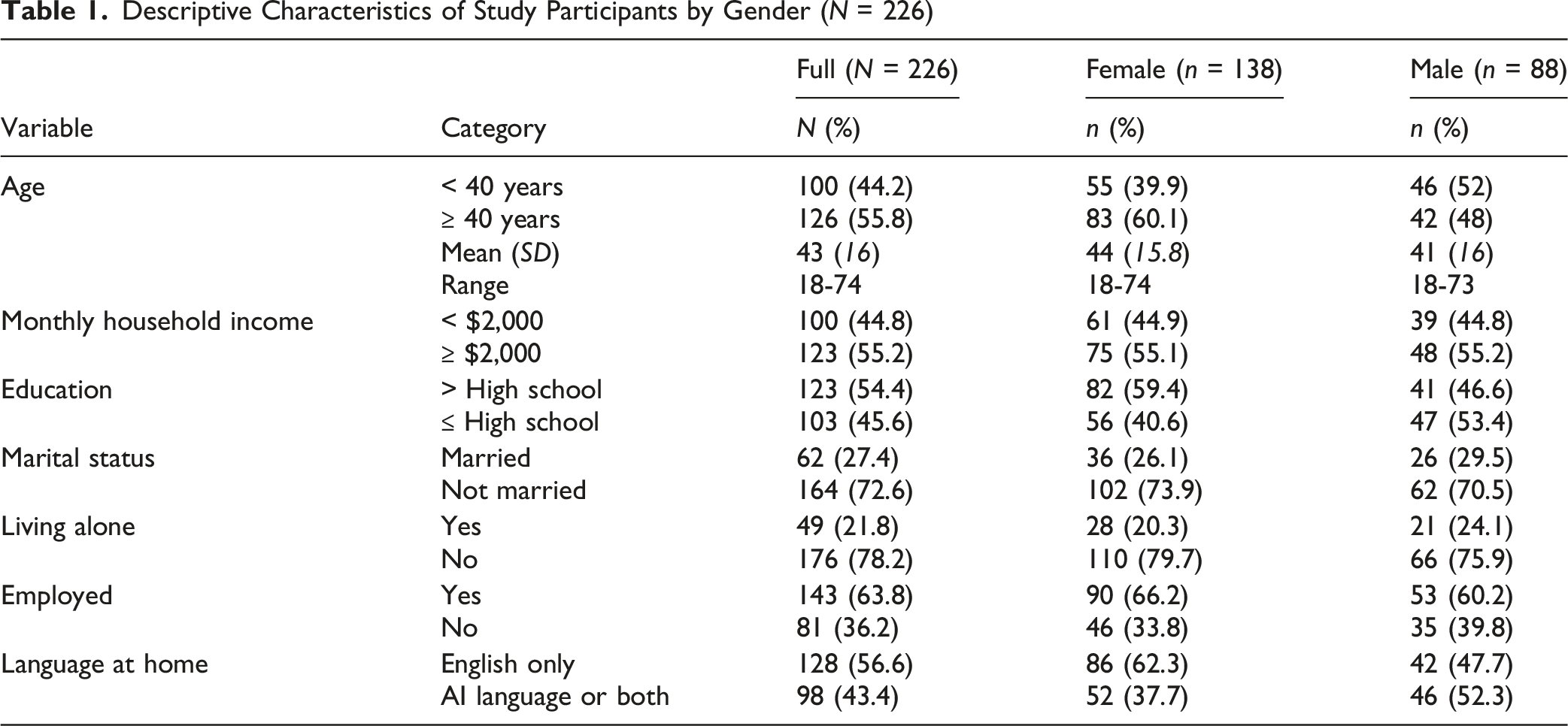
Sample Characteristics
Descriptive Characteristics of Study Participants by Gender (N = 226)
Group Differences Among Key Variables
Group Differences/Percentages of Key Study Variables (N = 226)
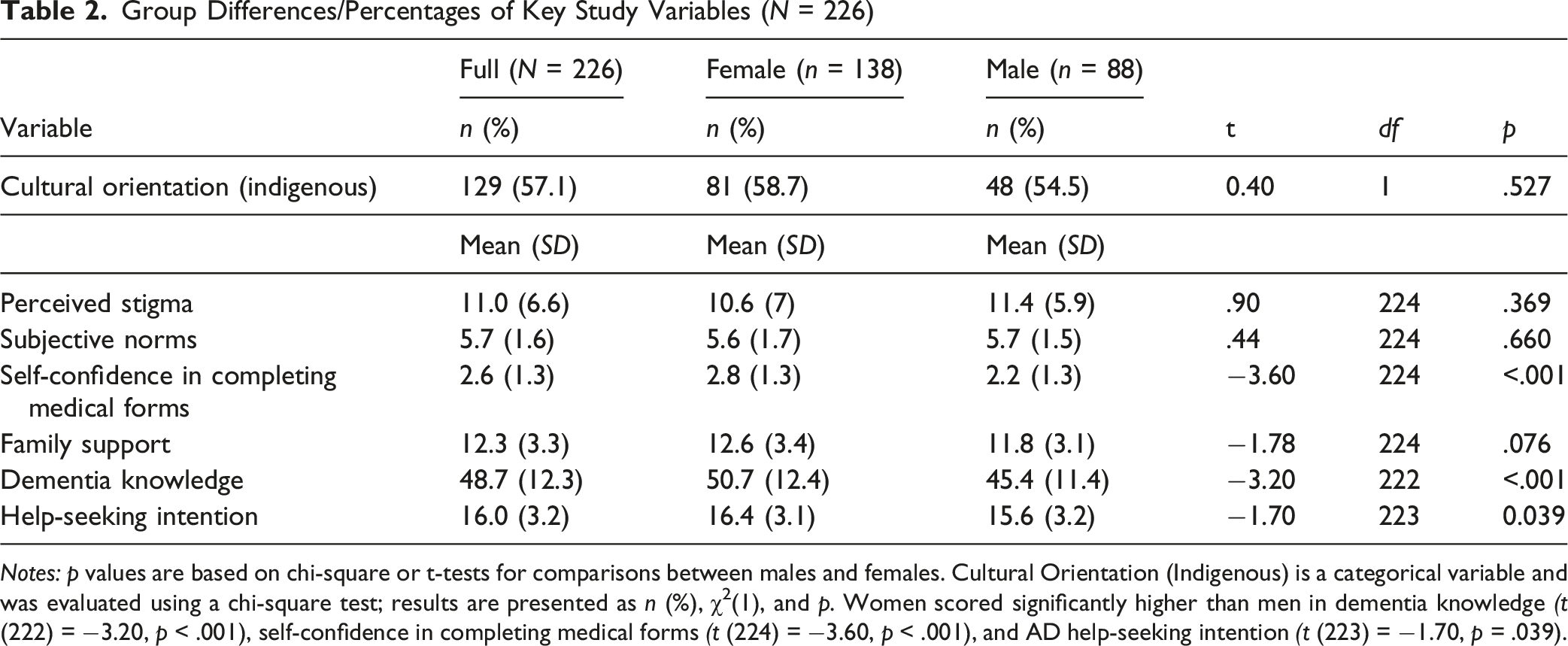
Notes: p values are based on chi-square or t-tests for comparisons between males and females. Cultural Orientation (Indigenous) is a categorical variable and was evaluated using a chi-square test; results are presented as n (%), χ2(1), and p. Women scored significantly higher than men in dementia knowledge (t (222) = −3.20, p < .001), self-confidence in completing medical forms (t (224) = −3.60, p < .001), and AD help-seeking intention (t (223) = −1.70, p = .039).
Linear Regression Analyses
Linear Regression Analyses of Help-Seeking Intentions for Family with Alzheimer’s Disease by Gender (N = 226)
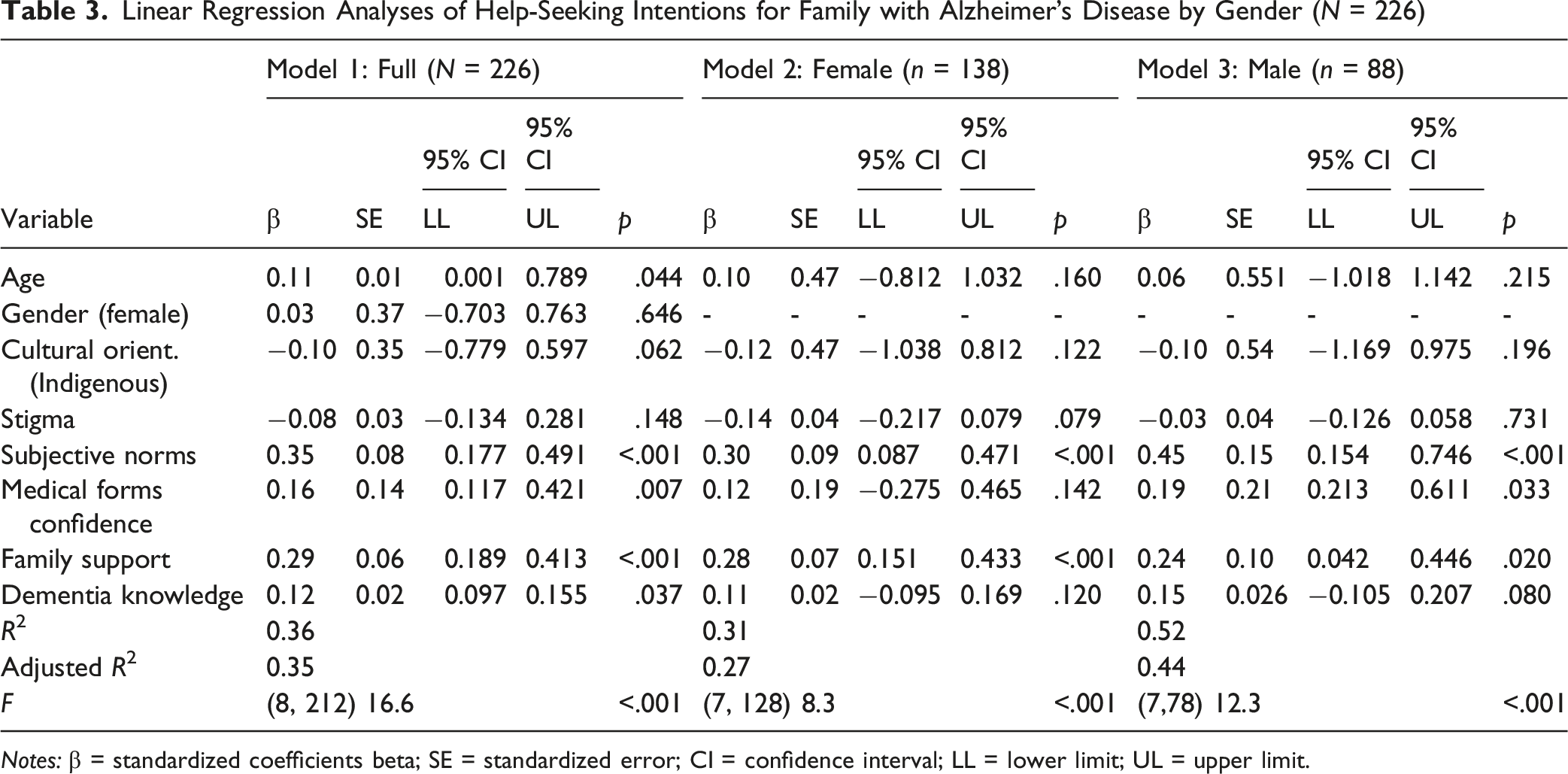
Notes: β = standardized coefficients beta; SE = standardized error; CI = confidence interval; LL = lower limit; UL = upper limit.
Discussion
Drawing on a sample of 226 AI adults aged 18 years and older residing in South Dakota, this study is among the first to assess help-seeking intentions when family member(s) become ill with AD. The focus of the study explores potential gender differences in help-seeking intentions, acknowledging the well-established consensus on the gendered role expectations and demands for family caregiving that women are more likely than men to provide caregiving for persons with AD (World Health Organization, 2024). Using the behavioral model of health service use (Andersen, 1995), we examined the associations between help-seeking intentions and predisposing (age), need (cultural orientation, perceived stigma, and subjective norms), and enabling factors (self-confidence in completing medical forms, family support, and dementia knowledge).
Gender Differences in Help-Seeking Intentions for Family With Alzheimer’s Disease
Confirming Hypothesis 1, AI women were found to score higher on help-seeking intentions for family with AD than AI men. Women were also likely to have higher dementia knowledge and greater self-confidence in completing medical forms. The average score of current AI participants on AD knowledge was moderate (48.7 out of 70), with women scoring 50.7 and men scoring 45.4. This finding is in line with prior studies that reported moderate levels of AD knowledge among AI adults (Jernigan et al., 2020). These gender differences may be attributed to the higher educational levels of AI women compared to men in our sample. It is also possible that since women are more likely than men to assume caregiving roles, knowledge of AD and available resources may naturally be transmitted via in-group social bonds.
Help-Seeking Intentions for Family With Alzheimer’s Disease and Associated Psychosocial Factors
Confirming Hypothesis 2, one of the most notable findings of the current study is that the intention to seek help for family members with AD was associated with several psychosocial factors. Moreover, the relationships among variables differed significantly across genders. Andersen’s behavioral model of health service use proved useful in examining factors associated with help-seeking intentions. Need (subjective norms) and enabling factors (family support and self-confidence completing medical forms) were significantly associated with help-seeking intentions, whereas the single non-modifiable factor, age, was not, for both women and men. Future research should examine a broader range of non-modifiable factors—such as tribal affiliation and family history of AD—to better understand their influence on help-seeking intentions for AD care.
Specifically, subjective norms emerged as a key factor associated with help-seeking intentions for both AI men and women. AI adults who believed that important others would support seeking care were more likely to intend to seek help. This finding aligns with prior research showing that sociocultural values shape attitudes toward elder caregiving, including U.S.-based Indigenous populations (Browne et al., 2017), U.S. Latino and other minority groups (Vila-Castelar et al., 2022), and Korean Americans, where subjective norms are linked to attitudes toward seeking AD care (Casado et al., 2018).
AI communities often rely on shared caregiving responsibilities and strong tribal and communal ties (Goins et al., 2011). Family caregiving is especially prevalent, with an estimated 16–17% of people providing care for family, relatives, or friends, driven by cultural values emphasizing family dependency. While family caregiving is common in non-Hispanic Whites, Hispanics, and Blacks (Vila-Castelar et al., 2022), limited resources and inadequate healthcare services in many tribal and rural areas increase the reliance on family caregiving (Jervis & Manson, 2002). In these sociocultural contexts, values, such as interpersonal relatedness, reciprocity, and tight kinship bond, heavily influence health behaviors and decisions (Jervis et al., 2010). Individuals frequently base care decisions on the perceived expectations of family and close community members. Our findings underscore a critical role of significant others in shaping health behavioral intentions, personal choices, and actions. Future interventions should account for the strength of group norms and community attitudes when addressing AD healthcare use among AI adults. A culturally grounded qualitative understanding of how subjective norms affect AI adults’ help-seeking decisions is essential to inform both clinical practice and health education efforts.
As hypothesized, family support proved to be a significant factor associated with AD help-seeking intentions for AI men and women alike. The importance of family and social support in health and mental health outcomes for AI populations, including cancer, quality of life, and help-seeking attitudes, is highlighted in several studies (e.g., Lee et al., 2020; Manson, 2000). For instance, Manson (2000) emphasized the centrality of family and community in treatment, identifying these as critical factors influencing mental health services use in AI populations. Our study reinforces the assertion that the greater the family support perceived by AI men and women, the stronger their intentions to seek healthcare for AD. Family-focused interventions could offer a valuable alternative to individually-focused approaches, as highlighted by Roh et al. (2024).
Another finding of our study is the identification of a gender-specific factor—self- confidence in completing medical forms—which was significantly positively associated with help-seeking intentions for AI men. Prior studies have highlighted self-efficacy—one’s confidence in their ability to perform specific tasks—as the most important requisite for behavioral change, affecting the amount of effort and level of performance given by an individual (Galvin et al., 2008). The results of this study appear to be in line with these findings. Interestingly, no significant associations emerged in AI women. In our sample, AI men had lower levels of education, dementia knowledge, self-confidence in filling out medical forms, and intentions for seeking AD care. It is possible that as AI men gain greater confidence in completing medical forms, they develop greater overall confidence in seeking healthcare and may have more experience with healthcare problems, which may translate into a stronger inclination to pursue AD care. Future studies should more deeply explore the effects of self-confidence on help-seeking intentions, with particular attention to gender differences and a broad range of self-efficacy measures.
Limitations of the Study
Several limitations of the present study should be acknowledged. First, the cross-sectional nature of the analyses requires caution in drawing causal inferences about the findings. Second, due to the use of convenience sampling of AI adults in South Dakota, the findings of this study should not be generalized to a larger population. For example, our sample was recruited from various traditional powwows, religious organizations, and social service centers, all of which may attract individuals who are more physically active and socially engaged. As such, the findings do not represent AI adults in other geographical regions or groups, such as individuals who may face greater physical or cognitive limitations. Another limitation of the study pertains to a single indicator of self-confidence with filling out medical forms, which may not adequately reflect AI adult’s overall confidence in seeking AD healthcare. In addition, the use of non-psychometrically validated measures—such as those that were modified or developed by the research team—may impact the internal validity and statistical conclusion validity of the study. Finally, the modest sample size, particularly for the regression model involving only male participants (n = 88), increases susceptibility to Type II error due to low statistical power.
Conclusion
With increasing life expectancy in AI communities, the prevalence of AD is expected to rise. This study addresses a key knowledge gap by examining gender differences in AD help-seeking intentions and psychosocial factors underlying these intentions in AI populations—an area largely unexplored. Notably, compared with AI women, AI men demonstrated lower dementia knowledge and were less likely to seek care for family members with AD. These results highlight the need for gender-specific, culturally tailored strategies. Educational and prevention efforts should address gender-related risk factors (e.g., cardiovascular health), improve AD knowledge, and promote early screening and care-seeking. For instance, programs emphasizing brain health, AD symptoms and consequences, and the benefits of early assessment and treatment may increase AD awareness and encourage early diagnosis and treatment.
Interventions should target key influences, such as subjective norms, family support, and self-confidence in help-seeking. Future research, particularly in partnership with tribes, should explore regional and cultural variation and identify barriers and facilitators to help-seeking. Health initiatives that incorporate unique sociocultural norms and Indigenous health beliefs regarding AD are a critical first step toward developing culturally relevant, targeted, community-based interventions for AI populations.
Footnotes
Acknowledgments
We acknowledge that this project was supported by the U.S. Department of Education, Higher Education Emergency Relief Fund, which funds San Francisco State University. Research reported in this publication was partially supported by the Dakota Cancer Collaborative on Translational Activity (DaCCoTA) Scholars Award, which is supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number U54GM128729 and the National Institute on Aging of the National Institutes of Health under Award Number P30AG059295. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the U.S. Department of Education. The authors wish to thank the stakeholders and all study team members who collaborated to offer their time and expertise on this project, as well as the study participants for their valuable input.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the San Francisco State University Institutional Review Board (IRB Number 2022-059).
Consent to Participate
No information that could be used to identify study participants is presented in this article. Informed consent was obtained from all individual participants included in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge that this project was supported by the U.S. Department of Education, Higher Education Emergency Relief Fund, which funds San Francisco State University. Research reported in this publication was partially supported by the Dakota Cancer Collaborative on Translational Activity (DaCCoTA) Scholars Award, which is supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number U54GM128729 and the National Institute on Aging of the National Institutes of Health under Award Number P30AG059295
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Our data, analytic methods, and materials can be made available to other researchers for replication purposes upon request and can be obtained by contacting the corresponding author at