
Abstract
Background
Global aging trends indicate a substantial increase in the older population, alongside rising rates of chronic illness and greater care needs. Preventive health strategies are essential to mitigate healthcare costs and improve quality of life.
Objective
This study proposes a conceptual preventive health model for older adults by integrating the Theory of Planned Behavior with the Life Situation framework.
Methods
A cross-sectional study was conducted with 400 older adults enrolled at the Antalya Tazelenme University. Validity and reliability of data tool were assessed using exploratory factor analysis and Cronbach’s alpha; relationships among variables were examined using multiple linear regression.
Results
The LS dimensions significantly influenced the TPB components, which in turn predicted intentions and behaviors related to preventive health (R2 = 0.598).
Conclusion
The proposed
Keywords
• Integrates the Life Situation (LS) framework with the Theory of Planned Behavior (TPB) to specify how upstream living conditions shape preventive health intentions and behaviors in later life. • Provides empirical evidence (multiple regression) linking seven LS dimensions to attitudes, subjective norms, and perceived behavioral control, strengthening explanation of preventive health behavior. • Derives the Pro-Aging-Health Model as a concise conceptual map that translates validated LS and TPB determinants into a usable framework for prevention planning.
• Practice: Use LS-informed assessment (e.g., resources, participation, and support) alongside TPB targets (attitudes, norms, and control) to tailor preventive programs for older adults. • Policy: Support age-friendly prevention by strengthening social support, access to services, and opportunities for activity/learning that enable self-care and sustained healthy routines. • Research: Test the Pro-Aging-Health Model in diverse samples and evaluate interventions that modify LS conditions to determine downstream effects on TPB pathways and behavior change.What This Paper Adds
Applications of Study Findings
Introduction
Population aging is accelerating worldwide. By the late 2070s, the number of people aged 65 years and older is expected to reach 2.2 billion, exceeding the number of children under 18 (United Nations 2024). In the EU, the proportion of people aged 65+ is projected to reach 32.5% by 2100 (Eurostat, 2026), and in Türkiye the share of adults aged 65+ exceeded 10% for the first time in 2023 (Türkish Statistical Institute 2024). As longevity increases, chronic illness and care needs rise, particularly among adults aged 80 years and older with multimorbidity (Kanowski, 1991, p. 227; Tufan, 2017).
These trends intensify the need for effective prevention and health promotion to reduce avoidable morbidity and pressure on health systems—especially under conditions such as epidemics and disasters (World Health Organization [WHO], 2019) and persistent access barriers (Pan American Health Organization [PAHO], 2012). Governments and health systems therefore face a dual task: strengthening preventive and protective services while also supporting older adults in developing and sustaining health-promoting behaviors (Vlaev et al., 2016).
Research on health decision-making has drawn on Rational Choice Theory and related approaches (Bryan, 2018; Maziak & Ward, 2009; Owumi & Raji, 2013), as well as on the Theory of Planned Behavior (TPB), which has been widely used to design or evaluate interventions in chronic disease contexts (Paul et al., 2022, 2023). Understanding how older adults form intentions and translate them into preventive actions is therefore central for practitioners and policy makers seeking to address behavior-related health problems (Buetow, 2007; Vlaev et al., 2016).
Beyond individual choice, later-life health is shaped by social inequality and unequal access to services (2002). Gerontology therefore considers aging at both micro (individual) and macro (societal) levels (Amann, 1993, p. 100; Tufan, 2020). The Life Situation (LS) framework operationalizes this perspective by integrating individuals’ attitudes and behaviors with their objective living conditions (Tufan, 2020).
Although TPB helps explain preventive health intentions and behaviors through attitudes, subjective norms, and perceived behavioral control, it often leaves the upstream “life situation” conditions that shape these determinants under-specified in older populations. Contextual factors are frequently treated as background variables rather than as a coherent, multidimensional construct with clear intervention levers. Integrating TPB with the LS framework may therefore provide a more comprehensive explanation of preventive health behaviors in later life.
Building on this perspective, the purpose of this study is to develop and test a conceptual preventive health model for older adults by integrating the TPB with the LS framework. Specifically, we examine whether older adults’ LS conditions are associated with the TPB determinants—attitudes (A), subjective norms (SN), and perceived behavioral control (PBC)—and whether these determinants predict preventive health intention (Int) and, in turn, preventive health behavior (BE). (1) To test the TPB pathways linking A, SN and PBC to preventive health intention. (2) To examine how LS dimensions relate to the TPB determinants (A, SN, and PBC) and how preventive health intention translates into preventive health behavior within the integrated model.
The hypotheses of this study are stated below:
Older adults who believe they can protect their health through positive behaviors are more likely to intend to engage in such behaviors.
Older adults who perceive social approval for their behaviors are more likely to form intentions to protect their health.
Older adults who believe they can control their health-related behaviors are more likely to intend to protect their health.
Background
In this paper, we use health promotion and disease prevention in line with World Health Organization definitions: health promotion is “the process of enabling people to increase control over, and to improve, their health” (WHO, 1986, 1998), while disease prevention refers to population- and individual-based interventions (including primary prevention and early detection) aimed at reducing disease burden and associated risk factors (Kisling & Das, 2023). To align this public-health perspective with the TPB, we conceptualize older adults’ LS conditions as upstream influences that shape the TPB determinants—attitudes, subjective norms, and perceived behavioral control—that then drive preventive health intentions and behavior.
LS approaches human development as a multidimensional and multifaceted phenomenon within a broad framework that spans the entire life course from conception to death. In this context, LS is conceptualized as a complex structure consisting of seven dimensions with fluid boundaries between them (Naegele, 1998, p. 106). This study examines seven LS dimensions: (1) Asset and Income (AI), (2) Material Supply (MS), (3) Connection, Cooperation, and Activity (CCA), (4) Learning and Experience (LE), (5) Organization and Participation (OP), (6) Recreation and Refreshment (RR), and (7) Social Network and Support Resources (SNR).
TPB, emerging from developments in Rational Choice Theory, draws on D. Dulany’s “theory of propositional control” and on foundational attitude concepts introduced by H. Peak and G. J. Rosenberg. TPB defines behavioral intention as the outcome of three components: “Attitudes (A), Subjective Norms (SN), and Perceived Behavioral Control (PBC)” (Kunz, 1997, p. 184): (i) Attitudes (A) “refer to individuals’ personal evaluations, beliefs, and values regarding a specific behavior.” (ii) Subjective norms (SN) reflect individuals’ perceptions of social expectations and pressures related to performing a specific behavior. (iii) Perceived behavioral control (PBC) represents individuals’ perceptions of their ability to perform a behavior and manage potential barriers.”
TPB posits that an individual’s intention to perform a behavior is the strongest predictor of actual behavior. Individuals who have positive attitudes toward the action, who believe that society supports the action, and who believe they can personally control the action are more likely to have intention (Int) and behavior (BE) towards the action (Ajzen & Fishbein, 1980, pp. 42–43). The relative influence of A, SN, and PBC may vary depending on individual differences, personal preferences, and contextual factors. To account for this variability, LS dimensions that may influence TPB components were incorporated into the model based on recommendations in the literature (Hagger & Hamilton, 2024).
Method
Participants
The sample of this study consists of students aged 60 and older enrolled in different classes (1st, 2nd, 3rd, and 4th) at the Antalya Tazelenme University during the 2024–2025 academic year. A total 400 older adults agreed to participate in the study out of 740 students. The questionnaire, available in both online and printed formats, was administered either online or through face-to-face interviews, depending on participants’ preferences.
Procedure
The questionnaire, developed by integrating items designed for the GeroAtlas project (Tufan, 2007; Tufan et al., 2019), was first piloted with 20 individuals outside the study sample, and the data collection form was subsequently refined.
Measures
Based on the collected data, a conceptual model (Chandra Kafle, 2019) was designed. While the sociodemographic section consisted of mixed-type questions, the LS- and TPB-related sections used 5-point Likert-type (Reinert et al., 2021) items. Data on the living situation of older individuals were collected based on the LS dimensions (AI, MS, CCA, LE, OP, RR, and SNR).
Analytic Strategy
This descriptive, cross-sectional, and exploratory study presents a conceptual model of preventive health derived from the integration of LS and TPB (Figure 1). After examining the effects of LS dimensions on the TPB components (A, SN, and PBC), the effects of these components on intention (Int) and, subsequently, on behavior (BE) were investigated, as recommended in typical statistical analysis models for TPB-framed studies (Hankins et al., 2000). Study design and method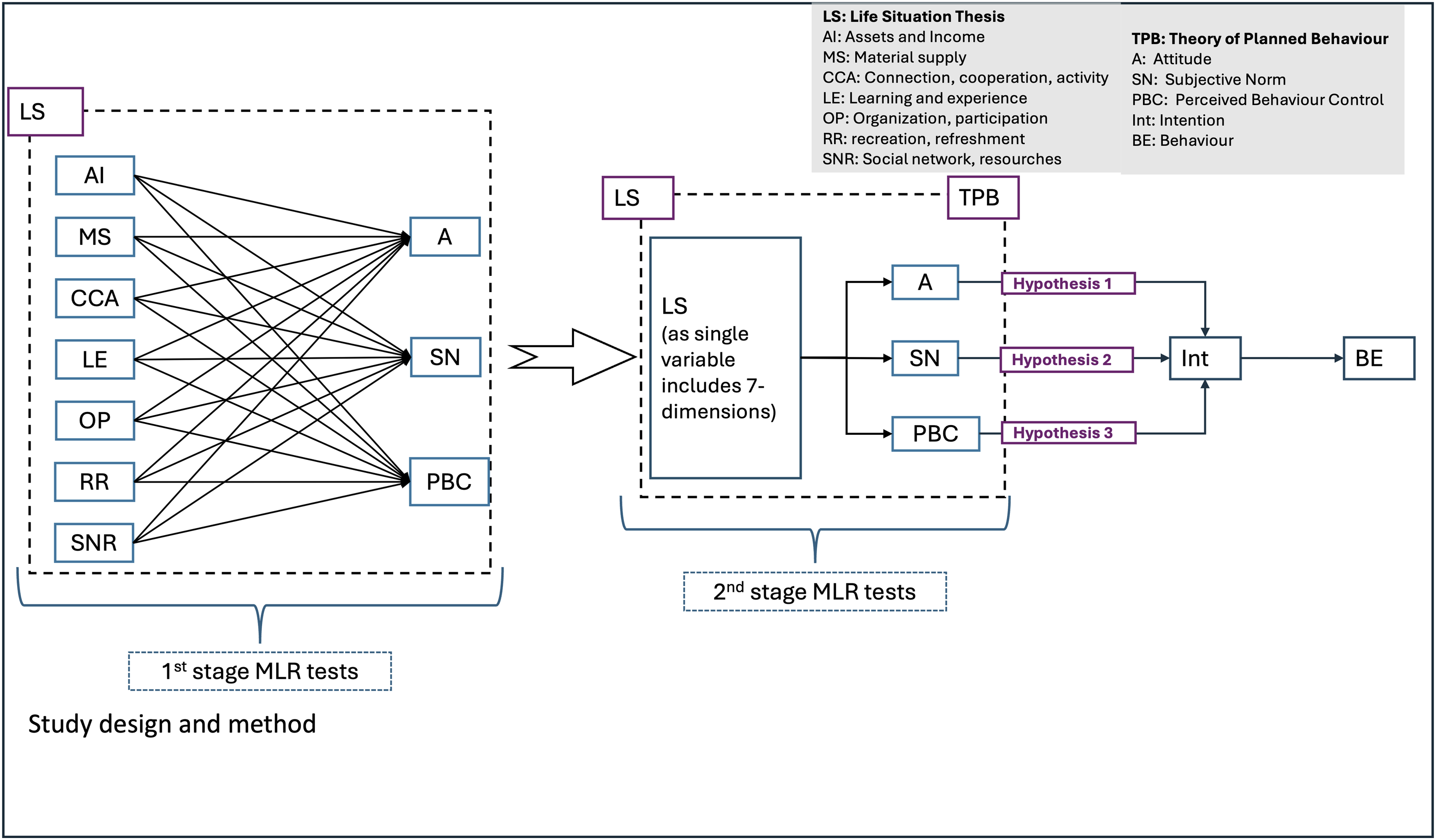
The study hypotheses and the relationships between LS and TPB components were tested using multiple linear regression (MLR). Descriptive, causal, and explanatory analyses were also conducted.
Data were analyzed using Microsoft Excel and SPSS version 17 (Statistical Package for Social Science for Personal Computers) PASW Statistics (version 17.0.3). Correlation and regression are statistical tools used to evaluate relationships between variables by estimating how changes in one variable relate to changes in another (Aneshensel, 2013, p. 4; Tabachnick & Fidell, 2013, p. 117). Exploratory factor analysis and Cronbach’s alpha reliability tests were applied to 79 TPB items and 69 LS items. Valid and reliable items were then carried forward to the MLR analyses.
Validity and Reliability of Tool
Because the data collection form was used for the first time in this study and included a large number of items, the LS dimensions and TPB components were subjected to validity and reliability testing.
Multidimensional data collection tools are commonly validated using exploratory factor analysis (EFA) to identify relationships among items within and across dimensions. Factor analysis clusters variables into common factors to uncover underlying constructs without specifying independent and dependent variables (Shrestha, 2021). In this study, EFA was used to determine whether items empirically corresponded to the TPB components or the LS dimensions. Items with loadings below 0.30 or cross-loadings on multiple factors were removed. Principal component analysis was used to highlight variation in the data and reveal clear patterns, and Varimax orthogonal rotation was applied to minimize the number of variables with high loadings within each factor. The Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity were applied. Following EFA, Cronbach’s alpha was calculated to assess internal reliability, consistent with prior research (Peterson, 1994; Liew & Noranini, 2017). Based on Taber’s (2018) classification, the Cronbach’s alpha coefficients indicated high or very high reliability for all components and dimensions.
In the TPB section of the questionnaire, data were collected using 80 items representing the components A, SN, PBC, Int, and BE. One item was removed because most participants did not answer it. The remaining 79 TPB items and 69 LS items were subjected to validity and reliability tests. After calculating mean scores for loaded items within each component or dimension, relationships were analyzed using MLR.
The Positive Response Rates and Validity and Reliability Test Results of Items Belonged to TPB Components
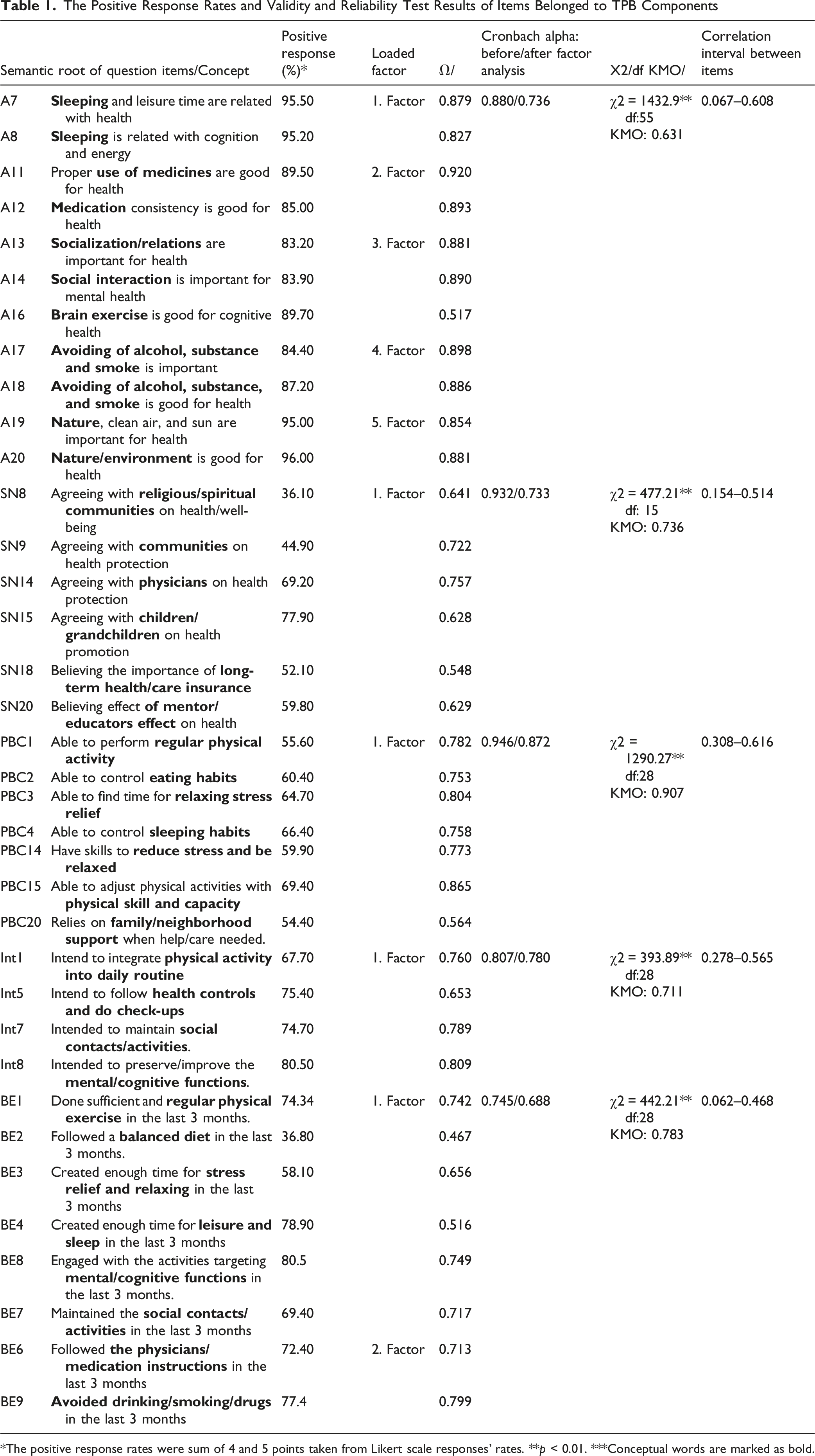
*The positive response rates were sum of 4 and 5 points taken from Likert scale responses’ rates. **p < 0.01. ***Conceptual words are marked as bold.
According to factor analysis results for the LS dimensions (AI, MS, CCA, LE, OP, RR, and SNR), all items loaded onto a single factor within each dimension, except for the AI dimension. Within the AI dimension, 8 of the 10 items loaded onto a single factor (KMO = 0.916; χ2 = 2186.34; p < 0.001) and Cronbach’s alpha was 0.924. Correlations among the eight items ranged from 0.120 to 0.568. In the other LS dimensions, items clustered within a single factor, with factor loadings above 0.70 in the first rotation. Cronbach’s alpha values were 0.924 (AI), 0.933 (MS), 0.933 (CCA), 0.927 (LE), 0.941 (OP), 0.956 (RR), and 0.935 (SNR).
Before the MLR analyses, mean scores were calculated for items assumed to be determinants of the TPB components (A, SN, PBC, Int, and BE). For multi-factored components and dimensions (Attitude and Behavior), factor-level means were calculated first and then aggregated to the component level. The MLR analyses examined: (a) relationships between TPB components (A, SN, and PBC) and LS dimensions and (b) relationships between TPB components (A, SN, and PBC) and Int and BE. • The relationships between TPB components (A, SN, and PBC) and LS dimensions • The relationship between TPB components: A, SN, PBC and Int, BE
Figure 2 shows the PERT (Program Evaluation Review Technique) diagram illustrating the statistical analysis process conducted throughout the study, including validity and reliability tests. Statistical model of the study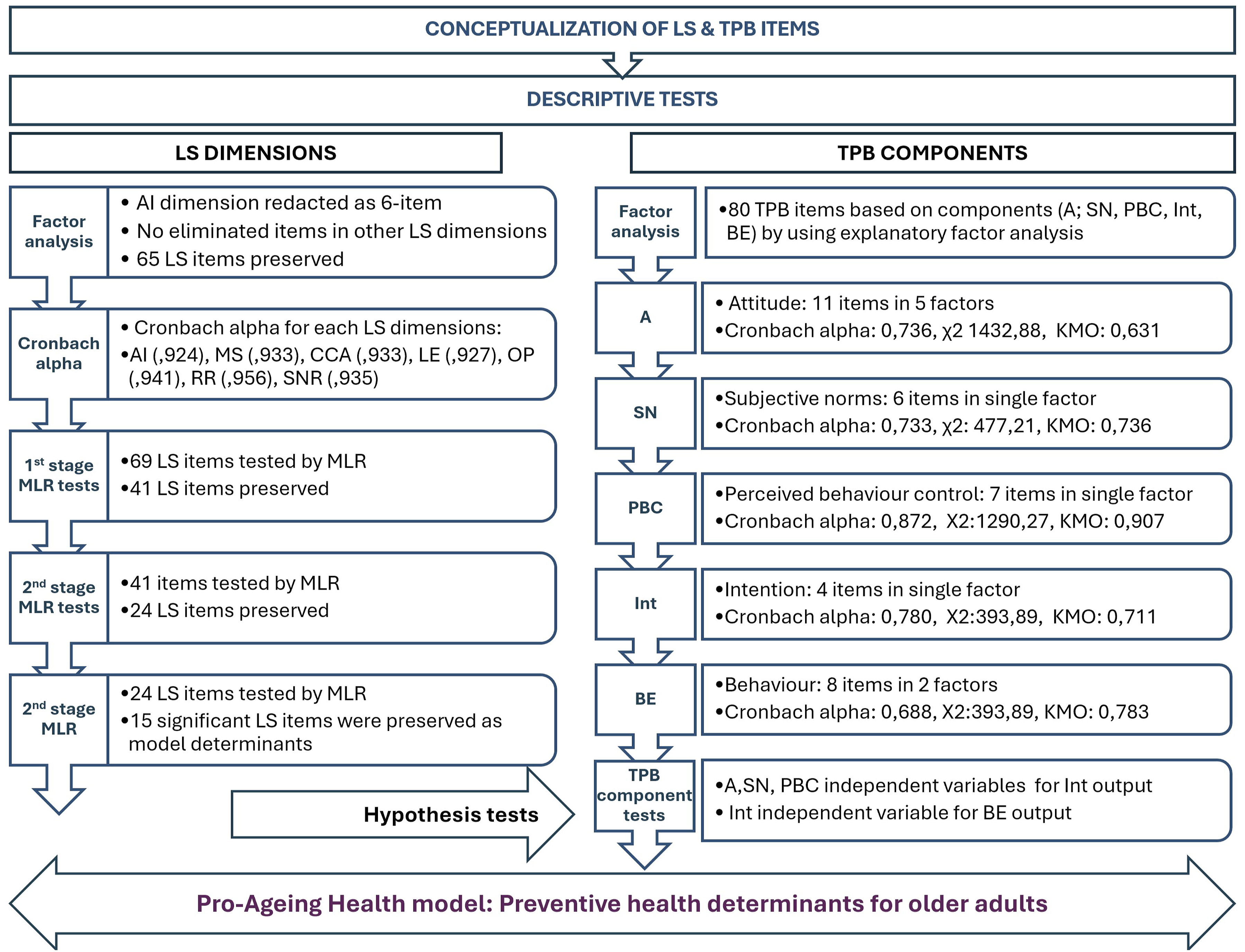
Based on the empirical findings, a conceptual preventive health model for older adults was developed. The model map (Figure 3) was created using the main concepts from questionnaire items, including 36 TPB items with sufficient factor loadings and 15 LS items associated with the TPB components. Conceptual map of preventive health for older adults: Pro-aging-health model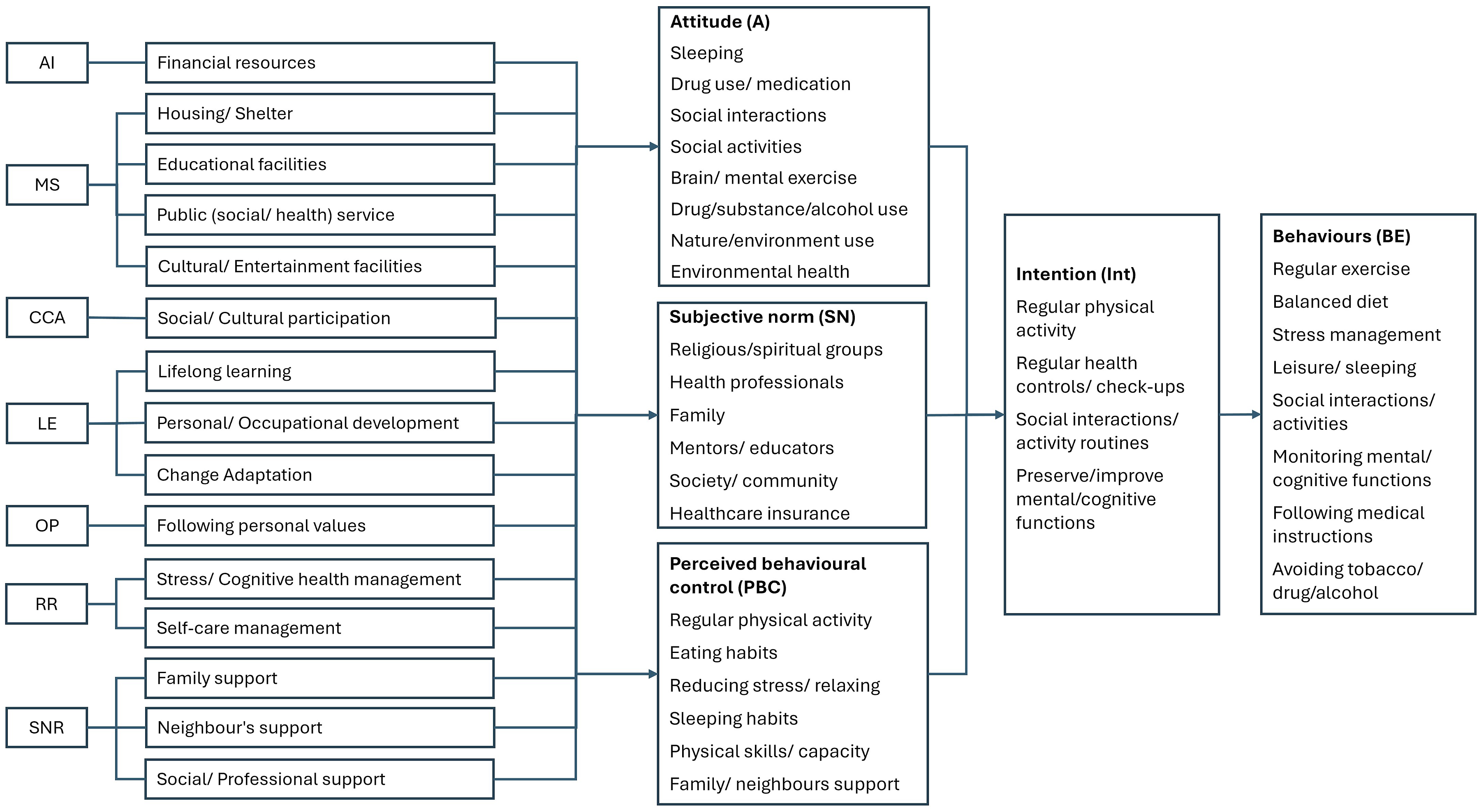
The concepts included in the conceptual map are keywords from questionnaire items assumed to explain the TPB components and LS dimensions: ⇨ TPB key concepts: Based on Factor analysis and Cronbach’s alpha tests were used to select items assumed to be predictors. ⇨ LS key concepts: The relationship between LS items, were subjected to dimensional validity and reliability tests in dimensional level. Then, the relation of items with TPB components (A, SN, and PBC) was examined in two stages by MLR, and the items selected are assumed to be predictors of LS.
Ethical Considerations
The research was conducted in accordance with the Declaration of Helsinki. Ethics approval (KAEK-675) was obtained from the Akdeniz University Faculty of Medicine Clinical Research Ethics Committee, and informed consent was obtained from participants. Permission was also obtained to use the questionnaire adapted from the GeroAtlas project (Tufan, 2007; Tufan et al., 2019).
Results
Sociodemographic Data Based on Gender
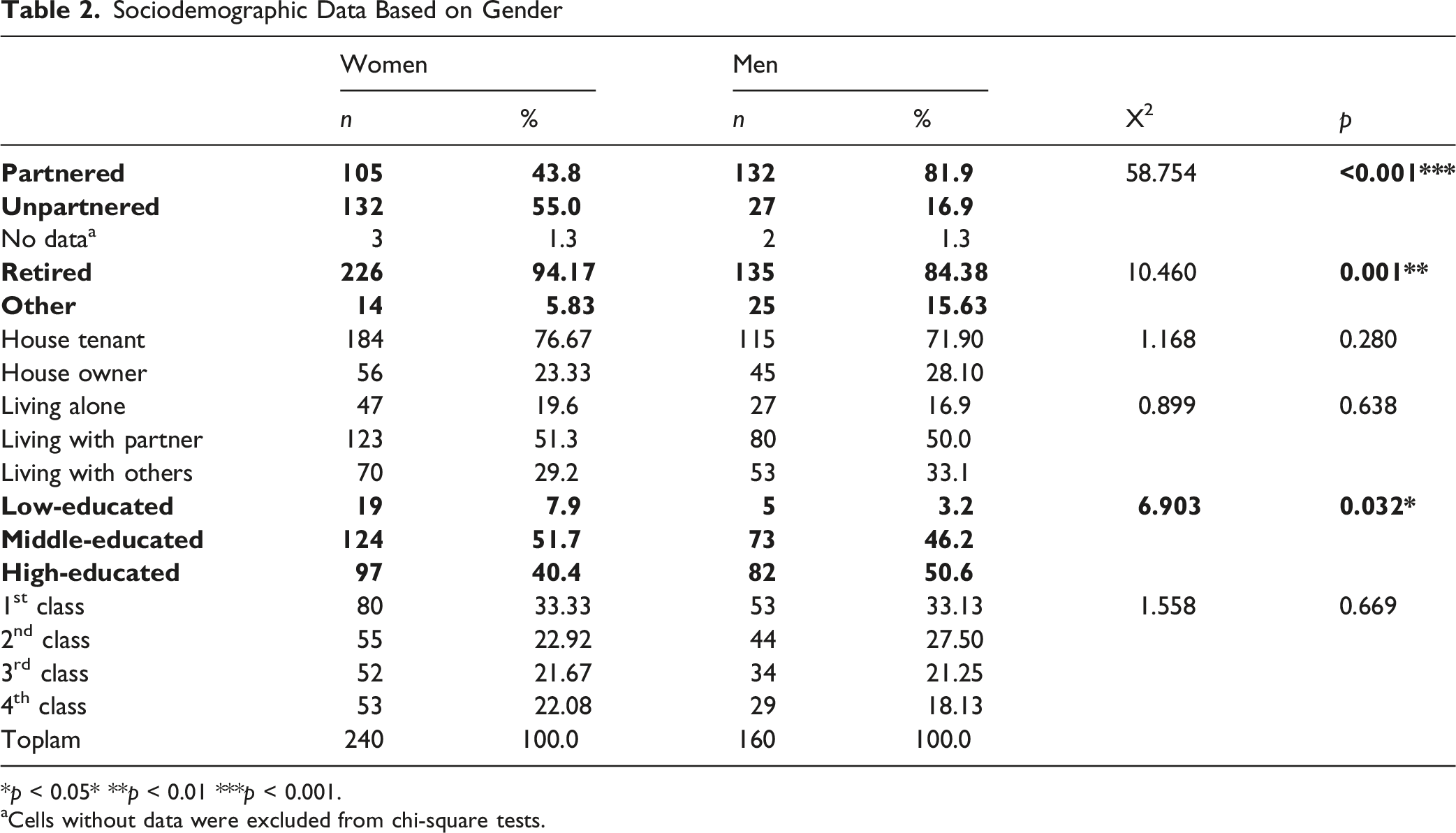
*p < 0.05* **p < 0.01 ***p < 0.001.
aCells without data were excluded from chi-square tests.
The relationships between the seven LS dimensions and the three TPB components (A, SN, and PBC) were examined using multiple linear regression (MLR). The explanatory power of the LS dimensions for each TPB component was determined. MLR analyses were conducted in two stages (Figure 1):
Examining the explanatory power of LS items as a 7-dimensional construct for each TPB component.
Examining the explanatory power of LS items as a single construct for each TPB component.
After the Stage 1 MLR tests, 23 LS items were identified as potential predictors of the TPB components. Appendix A presents the positive response rates, coefficients (B), adjusted R2 values, and variance values for these 23 items. In the Stage 2 analysis, 15 items were statistically significant determinants of the TPB components. These concepts are shown in bold Appendix A. and were incorporated into the “LS & TPB based preventive health model,” as they were assumed to explain the TPB components.
Relationships among the TPB components were examined using determinant items identified in Table 1. The relationships between older adults’ intentions (Int) related to preventive health and A, SN, and PBC were investigated. Correlation coefficients among A, SN, and PBC ranged from 0.50 to 0.515. For the MLR analysis, mean scores of the 24 TPB items were calculated first at the factor level (7 factors) and then at the component level (3 components). A (p = 0.003), SN (p = 0.019), and PBC (p < 0.001) significantly predicted the intention variable (R2 = 0.598) as shown in Appendix B.
All hypotheses were supported. Older adults’ A, SN, and PBC scores were associated with their intentions to engage in preventive health behaviors, including regular physical activity, routine health controls and check-ups, social contact and activities, and sustaining mental abilities and functions.
Older adults who expected doctors, educators, and the broader community to pay attention to their health, and those who believed that long-term healthcare insurance supports healthy living, reported higher intention scores (p < 0.025). Higher intention scores were also associated with having sufficient resources to incorporate regular physical activity into daily routines, maintaining eating and sleeping habits, having time and resources to relax and reduce stress, and receiving family and neighborhood support when help or care was needed. Additionally, all intention-related items significantly influenced preventive health behaviors (Table 1).
A Conceptual Map: Preventive Health Model for Older Adults
In this study, relationships between LS dimensions (AI, MS, CCA, LE, OP, RR, and SNR) and TPB components (A, SN, and PBC) were examined first, followed by an analysis of interrelationships among the TPB components. Through a two-stage regression process, 15 LS (Appendix A) items were identified as significant determinants, and 36 TPB items (Table 1) with sufficient factor loadings and internal reliability were confirmed as determinants of the TPB components. These items collectively form the foundation of the conceptual model.
Using key concepts derived from these validated items, a conceptual model was developed to illustrate how older adults’ life situations shape preventive health intentions and corresponding planned behaviors. The resulting model—the
Discussion
Concepts such as lifelong learning, change management, active aging, and social interaction in later life are closely linked to health service models for older adults. Preventive health, health promotion, and the organization of service delivery are also strongly associated with older adults’ health literacy. The sample in this study consisted of students aged 60 years and older from the “3rd Age University” (Antalya Tazelenme University), all of whom have adopted principles of lifelong learning. This sample profile should therefore be considered when interpreting the findings, evaluating the conceptual map, or refining the model.
According to 2024 population statistics for Türkiye, 55% of the national population is female, whereas 60% of participants in this study were women. The TÜİK database also reports that the proportion of married older men in Türkiye (84%) is higher than that of married older women (47%). Similarly, in this study, 82% of older men were married compared with 44% of older women. While labor force participation among older adults in Türkiye is 12.2%, only 4.25% of the sample was employed. Although the illiteracy rate among older adults is 12.5%, all participants in this study were literate. Finally, 8.7% of older adults in Türkiye have completed higher education, whereas this rate was 44.75% in the study sample. Consistent with national trends, men in the sample had higher educational levels than women.
The sample differs from the overall profile of older adults in Türkiye, particularly in education. However, as educational goals (Goal 3.4) of the Türkiye Healthy Aging Action Plan and Implementation Program are achieved, the older population may increasingly resemble this sample. Accordingly, the study may provide guidance based on projected trends for the Turkish population.
The findings indicate that older adults’ preventive health intentions (Int) and behaviors (BE) were determined by attitudes (A), subjective norms (SN), and perceived behavioral control (PBC). In other words, A, SN, and PBC were significant predictors of intention and subsequent behavior in preventive health activities in this sample (Appendix B).
The TPB is recognized for its simplicity and flexibility and for explaining substantial variation in intention and behavior through attitudes, subjective norms, and perceived behavioral control. Longitudinal and meta-analytic research by Hagger and colleagues (2022) suggests that although relationships among TPB components may evolve over time, the core components retain their explanatory power. The present findings likewise confirm the predictive strength of A, SN, and PBC in determining intention and subsequent behavior among older adults.
A systematic review by Ritchie et al. (2021) applying TPB to mammography screening reported explained variance ranging from 16% to 81%, with mean R2 values of 0.24 for screening behavior and 0.46 for intention. In the present study, intention included daily physical activity, attending health check-ups, maintaining social contact and activities, and preserving mental abilities and functions. These intention variables were predicted by A (β = 0.319), SN (β = 0.120), and PBC (β = 0.415), showing strong explanatory power (R2 = 0.598) (Table 2). This finding aligns with another study on COVID-19 vaccine decision-making, where a strong influence of SN was observed; participants reported that their vaccination decisions were influenced by social norms (Hossain et al., 2021; Shmueli, 2021). However, consistent with findings by Li et al. (2023) and Ritchie et al. (2021), the strong influence of PBC is also evident in the present study; moreover, the effect of A on Int is greater than that of SN (Appendix B).
Older adults’ preventive health intentions were associated with corresponding behaviors. Intentions related to daily physical activity, health check-ups, social engagement, and preserving mental abilities were linked to behaviors including regular exercise, balanced nutrition, stress reduction and relaxation, adequate sleep and rest, maintaining cognitive function, adhering to medical recommendations, taking medications regularly, and avoiding harmful substances during the previous 3 months (Appendix B).
In another TPB-framed study, intention was also significantly related to health-related behaviors (White et al., 2012). Across 58 studies, the effects of A, SN, and PBC on intention were consistently examined in relation to preventive health behaviors such as smoking, alcohol consumption, exercise, walking, dietary habits, and protection against infectious diseases (Godin & Kok, 1996). The present findings align with this evidence in terms of relationships among TPB components, even though path coefficients may differ.
In this study, 15 determinants related to older adults’ life situation (LS framework) influenced preventive health intentions and behaviors with high positive response rates (Appendix A). Investments individuals make in their own health earlier in life may reduce healthcare costs later (Ozkan, 2025), although various dynamics can affect older adults’ ability to make independent financial decisions (Strough et al., 2020). In the present study, participants indicated that using financial resources for personal priorities and needs was associated with intentions and behaviors related to maintaining health (Appendix A).
Consistent with prior research (Li & Woolrych, 2021), older adults’ satisfaction with housing and living conditions, educational institutions, social and healthcare infrastructure, and the availability of cultural and entertainment venues was associated with TPB components through the material supply (MS) dimension. Participation in cultural and social activities was also associated with TPB components through the connection, cooperation, and activity (CCA) dimension. Opportunities for personal growth and adaptability to new experiences were similarly related to preventive health intentions and behaviors through TPB components (A, SN, and PBC).
Personal values and beliefs are often maintained in later life; however, experiences may still lead to shifts in worldview (Hoogland, 2015). In this study, 63% of older adults reported adhering to their own values and beliefs, and integrating these into daily life was positively associated with preventive health intentions and behaviors within the TPB framework (Appendix A).
Maintaining cognitive vitality in later life is linked to effective stress management and sustained engagement in lifelong learning, and it also plays a role in managing chronic diseases (Fillit et al., 2002). In this study, stress regulation, mental health management, and self-care practices were identified as determinants influencing health-related intentions and behaviors within the recreation and refreshment (RR) dimension (Appendix A).
Family characteristics and neighborhood relationships influence mental, physical, and social well-being (Jiang & Liu, 2023). In this study, support from family, neighbors, and broader social and professional networks was positively associated with preventive health intentions and behaviors within the social network and support resources (SNR) dimension (Appendix A).
Integrating LS and TPB offers a unique contribution by treating life situation conditions as theory-driven upstream determinants of A, SN, and PBC; rather than as background covariates. This linkage helps translate behavioral mechanisms into concrete, modifiable social and structural levers, clarifying where gerontological interventions and policy can act to strengthen preventive health intentions and behaviors in later life.
Hovewer, this study has several limitations. Although the TPB framework was strengthened by incorporating LS dimensions to address unexplained variance, alternative theoretical models could also be applied. In addition, background factors such as personality, emotions, values, knowledge, stereotypes, and sociodemographic characteristics may influence TPB constructs and should be considered when interpreting the findings (Alhamad & Donyai, 2021). Our operationalization also treated preventive health as an umbrella outcome spanning both individual health behaviors (e.g., exercise, diet, sleep, and stress management) and use of preventive health services (e.g., routine controls/check-ups). While both can be conceptualized as planned actions within TPB, their determinants may differ in strength—for example, lifestyle behaviors may be more sensitive to motivational and knowledge-related beliefs (attitudes), whereas preventive service use may depend more strongly on perceived behavioral control and structural constraints captured by LS (e.g., financial resources, accessibility of services, and living conditions). Future studies should therefore test behavioral and service-use outcomes separately to identify potentially distinct pathways and intervention levers. Finally, the representativeness of the preventive health variables used (e.g., exercise, diet, screenings, and social relationships), as well as the cohort profile and study duration, may have affected the results.
Conclusion
The findings indicate that older adults’ life situation (LS) was significantly associated with attitudes (A), subjective norms (SN), and perceived behavioral control (PBC), which in turn shaped preventive health intentions (Int) and behaviors (BE). The results confirm that A, SN, and PBC are key determinants of preventive health intentions and actions, and all three hypotheses were supported.
Using EFA, TPB items were reduced to 36 items grouped under 10 factors (A = 5, SN = 1, PBC = 1, Intention = 1, Action = 2). LS items across seven dimensions were then analyzed through a two-stage MLR procedure to identify specific LS predictors of A, SN, and PBC. Fifteen LS items were identified as significant determinants (Appendix A). Together, these 36 TPB items (Table 1) and 15 LS items formed the basis for the conceptual framework named the
This paper is adapted from the corresponding author’s PhD thesis. The conceptual model developed in this study offers practical implications at both micro and macro levels and is expected to support older individuals, academic institutions, and stakeholders at local, national, and global levels.
Supplemental Material
Supplemental Material - Preventive Health Model for Older Adults: A Conceptual Map
Supplemental Material for Supplemental Material - Preventive Health Model for Older Adults: A Conceptual Map by Işıl Kaleli and İsmail Tufan in Journal of Applied Gerontology.
Supplemental Material
Supplemental Material - Preventive Health Model for Older Adults: A Conceptual Map
Supplemental Material for Supplemental Material - Preventive Health Model for Older Adults: A Conceptual Map by Işıl Kaleli and İsmail Tufan in Journal of Applied Gerontology.
Footnotes
Author Note
My sincere appreciation goes to Professor Ismail Tufan for his exceptional mentorship and continuous support. I extend my heartfelt gratitude to the students of Antalya Resfresment (Tazelenme) University who generously contributed their time and insights to this study.
Ethical Considerations
This research was approved by the Ethics Committee approval (KAEK-675) obtained from the Akdeniz University Faculty of Medicine Clinical Research Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This study constitutes a component of the corresponding author’s doctoral dissertation conducted within the Gerontology Department at Antalya Akdeniz University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.