
Abstract
Background
Chronic non-cancer pain (CNCP) disproportionately affects older adults, yet randomized trial evidence on psychosocial interventions in this population remains poorly characterized.
Objective
To map the randomized controlled trial (RCT) literature evaluating psychosocial interventions for CNCP in older adults.
Methods
Following Arksey and O'Malley, we searched four databases (1999–August 2024). Eligible studies were RCTs enrolling adults with mean age ≥60 years with CNCP, evaluating structured psychosocial interventions; headache and cancer pain were excluded. Two reviewers screened records. Of 7,394 studies, 49 met inclusion criteria.
Results
Trials mainly evaluated cognitive-behavioral therapy, self-management, acceptance and commitment therapy, and emotional awareness and expression therapy. Among trials specifying primary outcomes, pain intensity and physical function predominated. Psychosocial constructs were rarely primary endpoints. Adherence, fidelity, and adverse event reporting varied considerably.
Conclusions
Outcome prioritization is misaligned with the mechanisms of psychosocial interventions. Future RCTs should pre-register psychosocial outcome measures, standardize reporting, and recruit diverse samples.
Keywords
• Provides the first scoping review of randomized trials of psychosocial interventions for chronic non-cancer pain in adults ages ≥60, mapping modalities and methodological features. • Identifies key gaps in the existing literature: underreporting of psychosocial outcomes inconsistent adherence/fidelity/credibility and harms reporting, lengthy/complex dosing that limits feasibility, and underrepresentation of diverse populations.
• By mapping the existing literature on psychosocial approaches to chronic non-cancer pain in older adults, we have identified key areas that limit translation of these modalities into routine practice and provide the actionable groundwork for future studies • This study outlines the existing research on emerging modalities such as emotional awareness and expression therapy, positive affect-based treatments, acceptance and commitment therapy, and pain-reprocessing therapy and suggests that these novel treatments are promising and should be examined in future studies.What This Paper Adds
Applications of Study Findings
Introduction
The U.S. population continues to age, with adults aged 65 and older projected to reach almost 84 million by 2050 (Ortman et al., 2014). This demographic shift is expected to lead to an increase in the prevalence of chronic conditions, such as chronic non-cancer pain (CNCP), that disproportionately affect older adults (Dahlhamer et al., 2018). Chronic pain is commonly defined as pain lasting longer than 3 months (Treede et al., 2015), affects approximately 20% of Americans, and is associated with significant disability, reduced mobility, falls, depression, sleep impairment, and social isolation (Reid et al., 2015; Institute of Medicine [IOM], 2011; Yong et al., 2022). As a result, chronic pain poses a significant economic burden on society estimated at $560–635 billion dollars annually from medical expenditures and lost wages (IOM, 2011; Gaskin & Richard, 2012).
Managing chronic pain in older adults poses multiple challenges. Age-related physiological changes, sensory and cognitive deficits, polypharmacy, and multimorbidities increase the risks of adverse effects from pharmacologic and surgical treatments (Ali et al., 2018; Reid et al., 2015). Other barriers to pharmacological interventions include the ongoing opioid epidemic, clinicians’ concerns about the risks of adverse drug reactions, a limited evidence base to guide treatment decisions, and older adults’ attitudes towards pain and its treatment options (Haley & Saitz, 2020; Nelson et al., 2015; Reid et al., 2015).
The biopsychosocial model of pain has been widely adopted and frames pain as multi-dimensional, arising from a dynamic interaction between biological, social, and psychological factors. This framework has led to the development of the fear-avoidance model, which conceptualizes pain as a product of repeated catastrophic interpretations of acute pain as an uncontrollable, threatening event (Leeuw et al., 2007; Vlaeyen & Linton, 2000; Zale & Ditre, 2015). These maladaptive interpretations trigger fear and anxiety, reinforcing avoidance of physical activity, hypervigilance, and persistent pain.
Psychosocial interventions that target maladaptive cognitions and behaviors among older adults have become increasingly common (Meints & Edwards, 2018; Zale & Ditre, 2015). These interventions belong under the umbrella of non-pharmacological methods and include approaches such as cognitive-behavioral therapy (CBT), acceptance and commitment therapy (ACT), mindfulness, pain coping skills, and self-management programs (Broderick et al., 2014; Clarke et al., 2017; DeBar et al., 2021; Hausmann et al., 2018). Psychosocial interventions are defined as “interpersonal or informational activities, techniques, or strategies that target biological, behavioral, cognitive, emotional, interpersonal, social, or environmental factors with the aim of improving health functioning and well-being” (Committee on Developing Evidence-Based Standards for Psychosocial Interventions for Mental Disorders, Board on Health Sciences Policy, & Institute of Medicine, 2015, p. 31). While psychosocial interventions are a type of non-pharmacological method, they specifically utilize psychological and behavioral approaches, whereas non-pharmacological approaches encompass a broader category of treatments that can include physical, educational, or social approaches (e.g., low-level light therapy, massage, and hypnosis) (Hargett et al., 2022). Collectively, psychosocial interventions have demonstrated benefits in pain-related outcomes, but most evidence is derived from populations with mean ages under 60 (Hughes et al., 2017; Williams et al., 2020; Ye et al., 2024).
Several reviews have synthesized psychosocial interventions targeting chronic pain among older adults, yet important gaps remain. Prior reviews focus on interventions that involve one specific modality (e.g., CBT, mindfulness, and coping skills programs) (Keefe et al., 2013; Niknejad et al., 2018; Williams et al., 2020), online delivery platform (E-health and virtual reality) (De Lucia et al., 2024), or special population (e.g., individuals living with dementia) (Pu et al., 2019). A recent systematic review and meta-analysis provided effect size estimates for various non-pharmacological interventions for chronic pain among older adults but primarily analyzed well-established interventions (i.e., CBT, mindfulness, physical activity, and physical activity + CBT) (Leung et al., 2024). However, no studies to date have comprehensively summarized emerging intervention modalities, trial design features, or implementation characteristics, such as recruitment settings, interventionist type, intervention dose, and monitoring of adherence. Moreover, heterogeneity in outcome measures and limited reporting quality further hinder synthesis across studies. A scoping review that systematically maps these characteristics is needed to elucidate how non-pharmacological interventions for chronic pain among older adults are delivered and evaluated as well as to identify gaps that can inform future research and implementation efforts.
As such, we conducted a scoping review to systematically synthesize findings from existing randomized controlled trials of psychosocial interventions for CNCP in older adults and to identify key evidence gaps. Using the Arksey and O’Malley framework and including trials published through August 2024, this scoping review captures both established and understudied modalities, while characterizing (1) patient characteristics (e.g., age, gender, race/ethnicity, and pain type), (2) intervention characteristics (e.g., modality, mode of delivery, and dose/length), (3) outcome measures used to assess benefits and fidelity, (4) reported harms, and (5) other trial characteristics. This evidence map will inform future trials, implementation strategies, and progress towards standardized outcome reporting.
Methods
Approach
We conducted a scoping review using an interpretive scoping literature review methodology (Arksey & O’Malley, 2005). This framework outlines five stages: (1) identification of research questions, (2) identification of relevant studies, (3) selection of studies, (4) data extraction, and (5) gathering, analyzing, and reporting results.
Search Methods
We performed comprehensive searches to identify studies that assessed the effects of non-pharmacological interventions on CNCP in older adults. MEDLINE ALL (Ovid), Embase (Ovid), the Cochrane Library (Wiley), and APA PsycINFO (EBSCOhost) were searched on January 18, 2022. Search strategies were based upon those employed in a previous systematic review on non-pharmacological interventions (Niknejad et al., 2018). All databases were searched from 1999 and limited to articles in English. Results were imported into, and automatically deduplicated in, the Covidence systematic review software. Reference checking of included articles was conducted on September 29, 2022. The search was updated on August 6, 2024. Further details including the full search strategies for all sources are available in the Supplemental Material and at the Open Science Framework (Hickner, 2022).
Selection Criteria
Studies were eligible for inclusion if they met the following criteria: (1) article was published from 1999 through August 6th 2024, (2) published in English, (3) employed a randomized-controlled trial design (including comparative effectiveness RCT), (4) enrolled older adults as evidenced by a mean sample age of 60 years or greater, (5) enrolled patients with chronic pain: defined as either having ≥3 months of chronic pain (Treede et al., 2015) or a physician documented diagnosis of chronic pain, and (6) evaluated a psychosocial intervention for pain. Psychosocial interventions were eligible if they (1) included an explicit psychological/behavioral component targeting cognition, emotions, coping, or behavior and (2) were delivered as a structured program (e.g., CBT, ACT, problem solving, mindfulness, and pain self-management). We excluded purely physical/somatic modalities and education-only interventions without skills training or behavior-change content. We restricted inclusion to randomized-controlled trials to focus on interventions with at least preliminary efficacy testing and to align with evidence standards used in clinical guidelines for geriatric pain care. Combination therapies (e.g., medication with CBT) were also included. Interventions with any mode of delivery (in-person, online, group, or individual) were eligible for analysis. Studies that enrolled participants with pain due to headache or cancer were excluded, as these conditions have distinct underlying mechanisms and clinical management pathways. Including them would have introduced substantial heterogeneity outside the scope of CNCP in older adults.
Study Screening
After duplicate studies were removed, two independent reviewers screened titles and abstracts of the remaining studies. Articles that appeared to meet our inclusion criteria along with those that were unclear were retained for full-text screening. Disagreements and conflicts of the articles were resolved through team discussion or third-party adjudication.
Data Extraction and Synthesis
Four reviewers independently extracted data from each article into a Microsoft Excel spreadsheet. Extracted items included eligibility criteria (pain population, inclusion and exclusion criteria), study characteristics (study setting, recruitment setting, recruitment rate, number of subjects, determining if power calculation was provided), participant characteristics (total mean age, gender (% female per study), race and ethnicity, education level, intervention characteristics (intervention, who delivered the intervention, mode of delivery, group or in-person, determining if primary care providers were involved in the study, number and duration of treatment session, total intervention exposure), feasibility measures (adherence to intervention sessions, determination of homework assignment, adherence to homework exercises), process measures (determining if authors assessed for adverse events, measure of treatment credibility and fidelity, determining if the author specified primary outcomes), efficacy (primary, secondary, and non-specified outcomes, names of these outcome measures), and study measures (number of assessments and timing of assessments). We summarized study features descriptively and organized primary and secondary outcomes into domains. For studies with multiple primary and secondary outcomes, each outcome was categorized into domains. Primary outcomes were categorized into the following domains: pain intensity, pain interference, physical function, depressive symptoms, pain-related attitudes/beliefs, self-efficacy for managing pain, quality of life, and other. Secondary outcomes were categorized into the following domains: pain intensity, pain interference, physical function (self-report and performance-based), mood, anxiety, depressive symptoms, self-efficacy managing pain, pain-related attitudes/beliefs, catastrophizing beliefs, others (psychological), sleep, mindfulness, medication use, global change, fatigue, coping strategies, satisfaction, quality of life, and others. The “other” domain included outcomes that did not fit into the named domains and was not found in more than one study. Similarly, the “Other (psychological)” domain included psychological outcomes that did not fit into the named psychological domains and was not found in more than one study. We did not perform risk-of-bias assessment or meta-analysis, consistent with scoping review objectives. Of the data extracted, only select categories were reported.
Interrater Agreement
To estimate interrater agreement, one reviewer independently reviewed a random subsample of 20 articles abstracted by a second reviewer. The level of agreement was excellent as determined by a Pearson r correlation coefficient of 0.99 (for continuous variables) and substantial as evidenced by a kappa statistic of 0.79 for nominal and categorical variables.
Results
Study Characteristics and Design
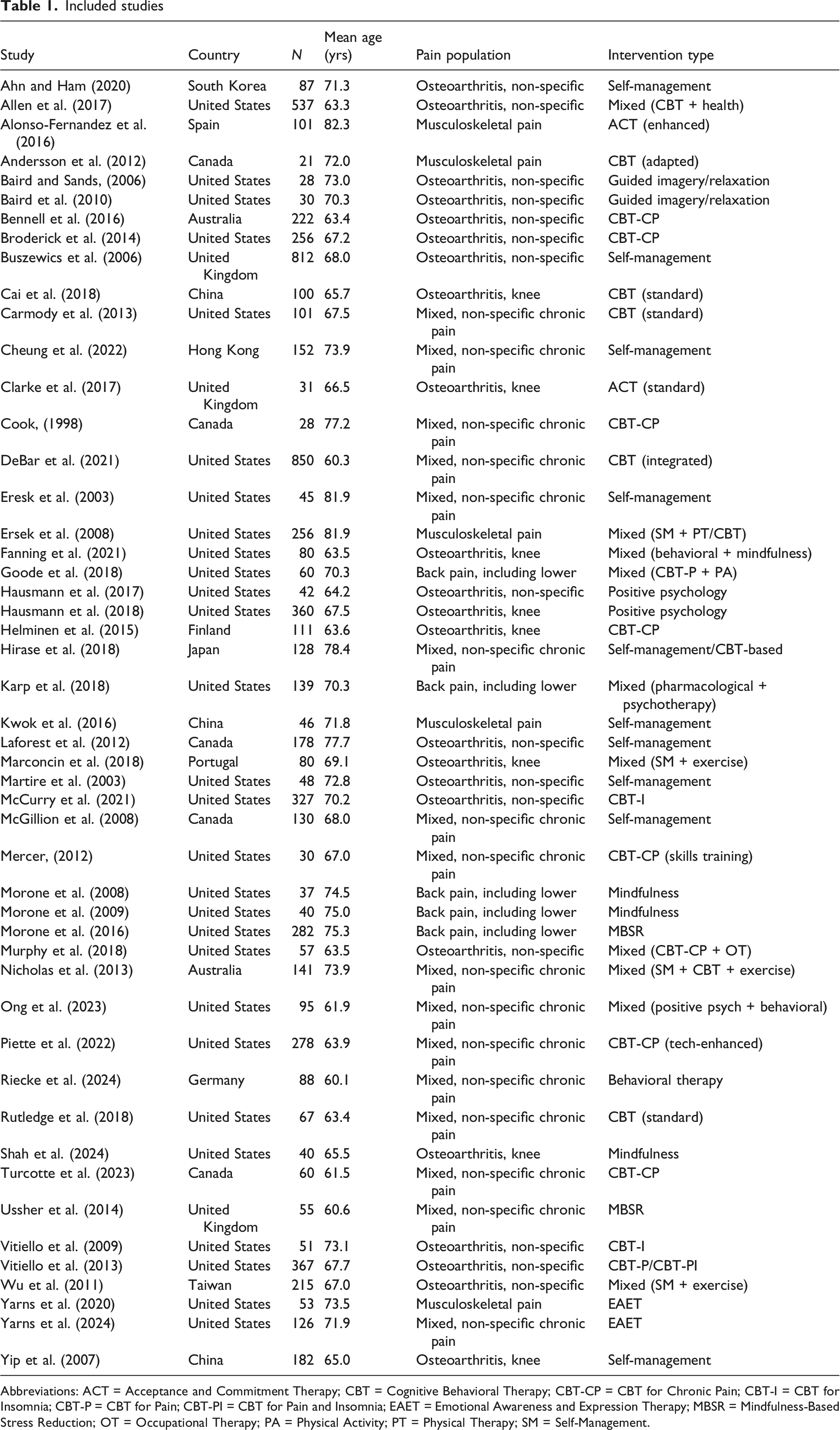
Figure 1 presents the PRISMA-ScR study flow diagram. Our search strategy generated 7,394 articles. After removing duplicates, the titles and abstracts of 4,226 unique articles were screened. A total of 564 articles underwent full-text review and of these 515 (91.3%) were excluded (reasons shown in Figure 1), leaving 49 articles that underwent full data extraction (Table 1; see Supplemental Table 1 additional information on included studies). PRISMA flow diagram Included studies Abbreviations: ACT = Acceptance and Commitment Therapy; CBT = Cognitive Behavioral Therapy; CBT-CP = CBT for Chronic Pain; CBT-I = CBT for Insomnia; CBT-P = CBT for Pain; CBT-PI = CBT for Pain and Insomnia; EAET = Emotional Awareness and Expression Therapy; MBSR = Mindfulness-Based Stress Reduction; OT = Occupational Therapy; PA = Physical Activity; PT = Physical Therapy; SM = Self-Management.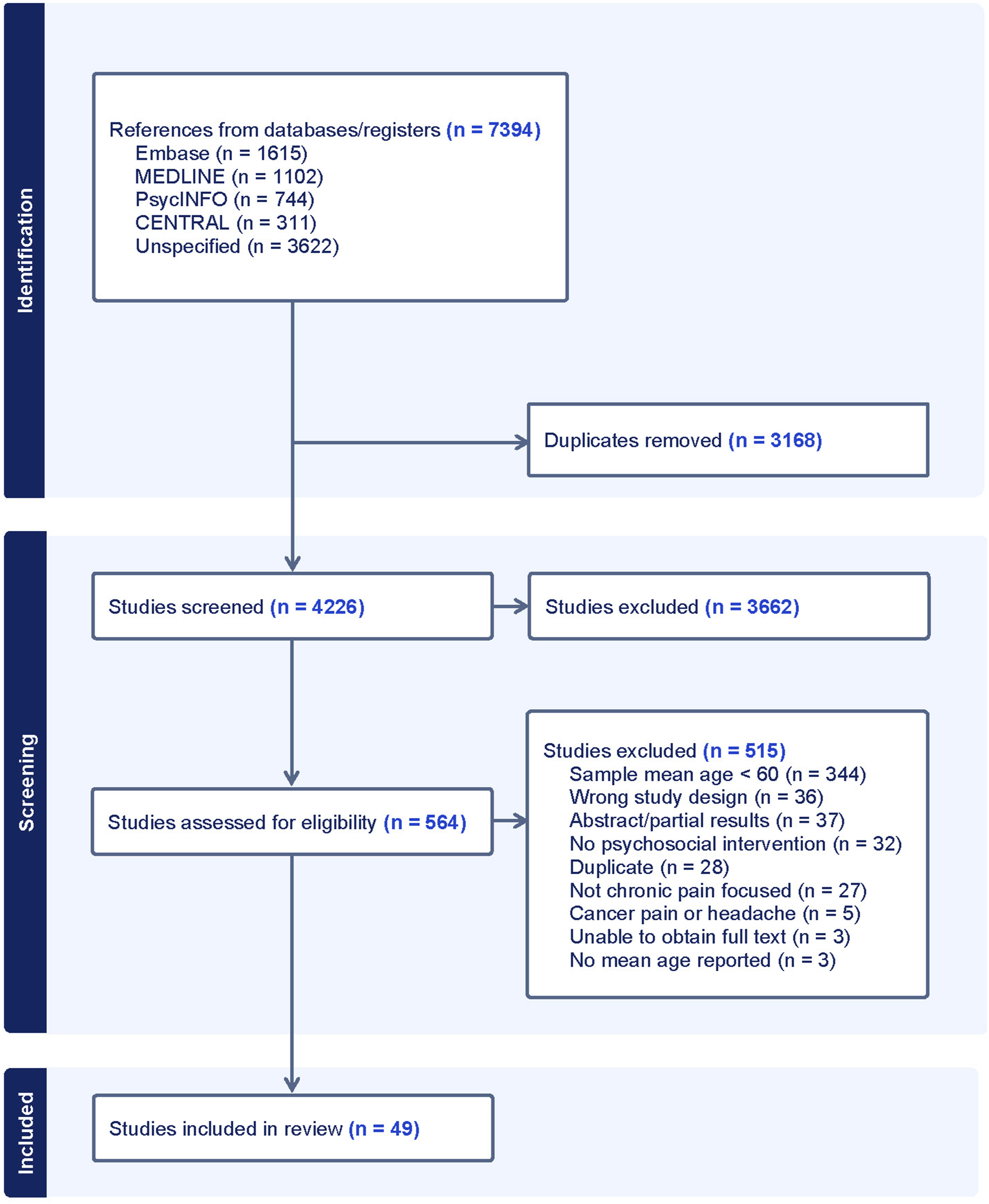
Summary of study characteristics of the included studies
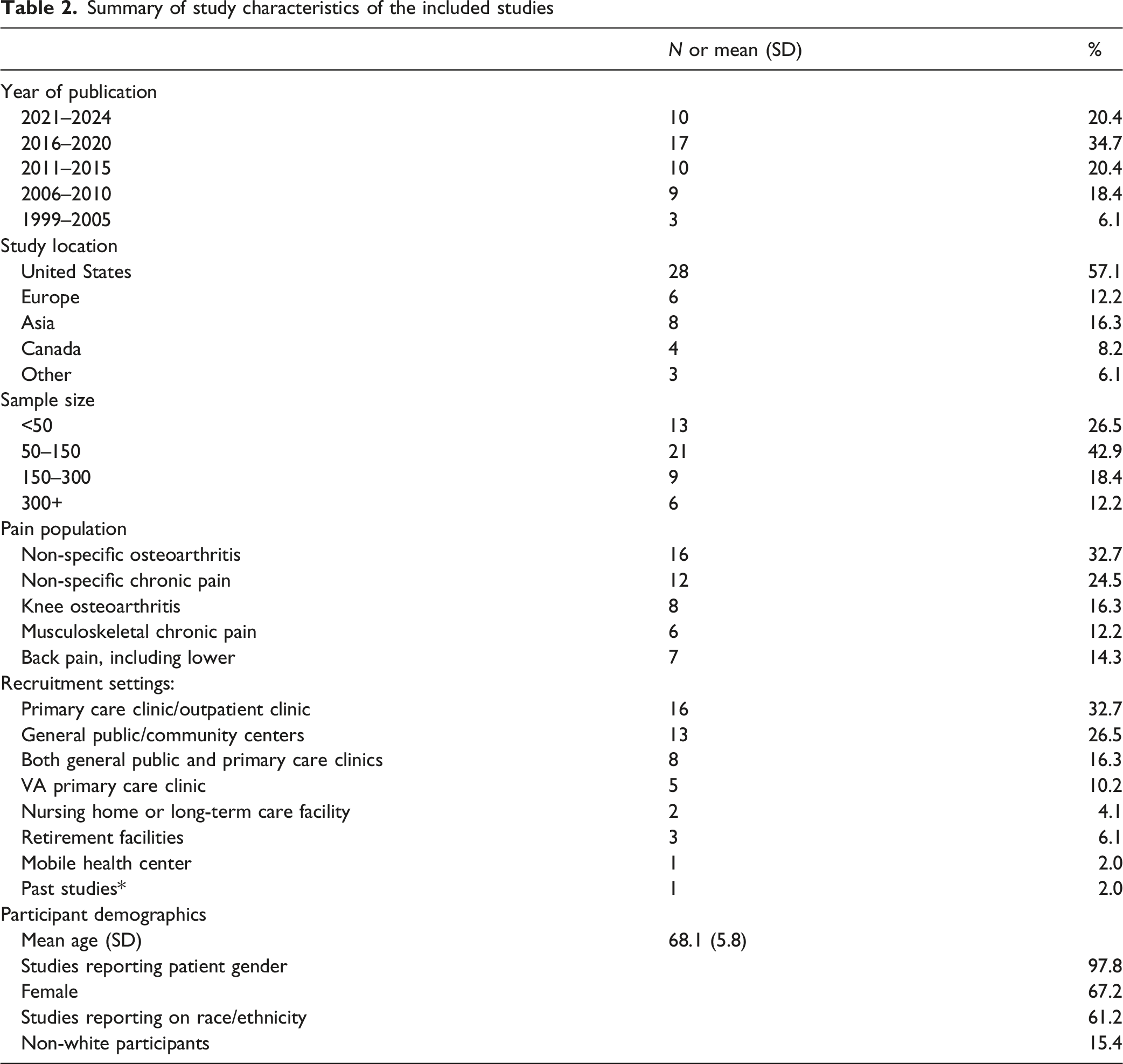
Across the analyzed studies, the mean (SD) participant age was 68.1 (5.8), and most participants were female (67.2%). Race/ethnicity was not reported in 38.8% of studies. Among the 61.2% of studies that did report race/ethnicity, the majority of participants were White (84.6%).
Intervention Types and Mode of Delivery
Summary of intervention characteristics of the included studies
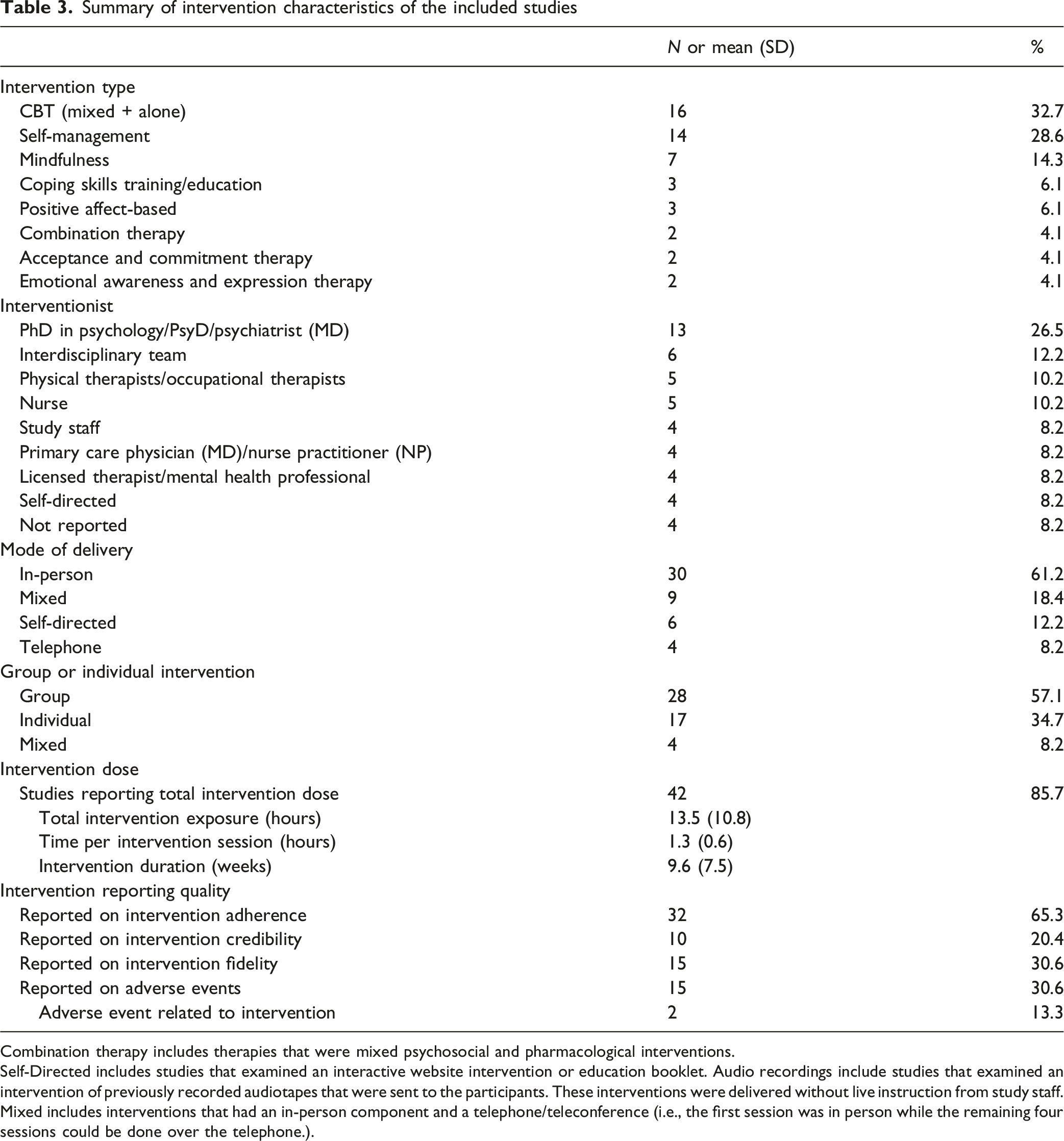
Combination therapy includes therapies that were mixed psychosocial and pharmacological interventions.
Self-Directed includes studies that examined an interactive website intervention or education booklet. Audio recordings include studies that examined an intervention of previously recorded audiotapes that were sent to the participants. These interventions were delivered without live instruction from study staff.
Mixed includes interventions that had an in-person component and a telephone/teleconference (i.e., the first session was in person while the remaining four sessions could be done over the telephone.).
Interventionists varied in the sample: Doctorate-level scientists in psychology (PhD or PsyD) or psychiatry (MD) were the most common (26.5%), followed by interdisciplinary teams (e.g., a psychologist and physical therapist; 12.2%). Most studies examined interventions delivered in-person (61.2%) while some used mixed formats (i.e., an initial in-person session followed by telephone sessions) or entirely self-directed (educational workbooks or online modules). One intervention tested a dynamic delivery model using AI-based monitoring to tailor participant support (Piette et al., 2022).
Intervention Dose
Most trials reported total intervention dose (85.7%). Across these studies, the mean (SD) total dose was 13.5 (10.8) hours delivered over 9.6 (7.5) weeks with considerable variability (range, 0.8–44.8 hours). A minority of trials (14.3%) did not report total dose. These studies typically used interactive websites, workbooks, or educational booklets.
Intervention Adherence, Credibility, Fidelity, and Monitoring for Possible Harms
Across the 49 trials, 65.3% recorded intervention adherence/attendance. 20.4% assessed perceived intervention credibility, and 30.6% reported conducting treatment fidelity assessments (most commonly by rating audio/video session recordings with standardized instruments). Possible harms were assessed in 30.6% of trials, of which 2 (13.3% of those that assessed harms; 4.1% overall) reported an adverse event related to the intervention.
Assessment Frequency
All trials conducted at least one short-term assessment (baseline to ≤13 weeks). Fewer than half (46.9%) conducted an additional assessment between 14 and 26 weeks; 18 (36.7%) assessed longer-term outcomes (27–52 weeks). Few trials (13.7%) assessed outcomes beyond 1 year (Figure 2). Assessment frequency of analyzed studies. For studies with multiple assessments, each assessment frequency was categorized. Week 0 refers to the start of the intervention and week 52 refers to 1 year after the start of the intervention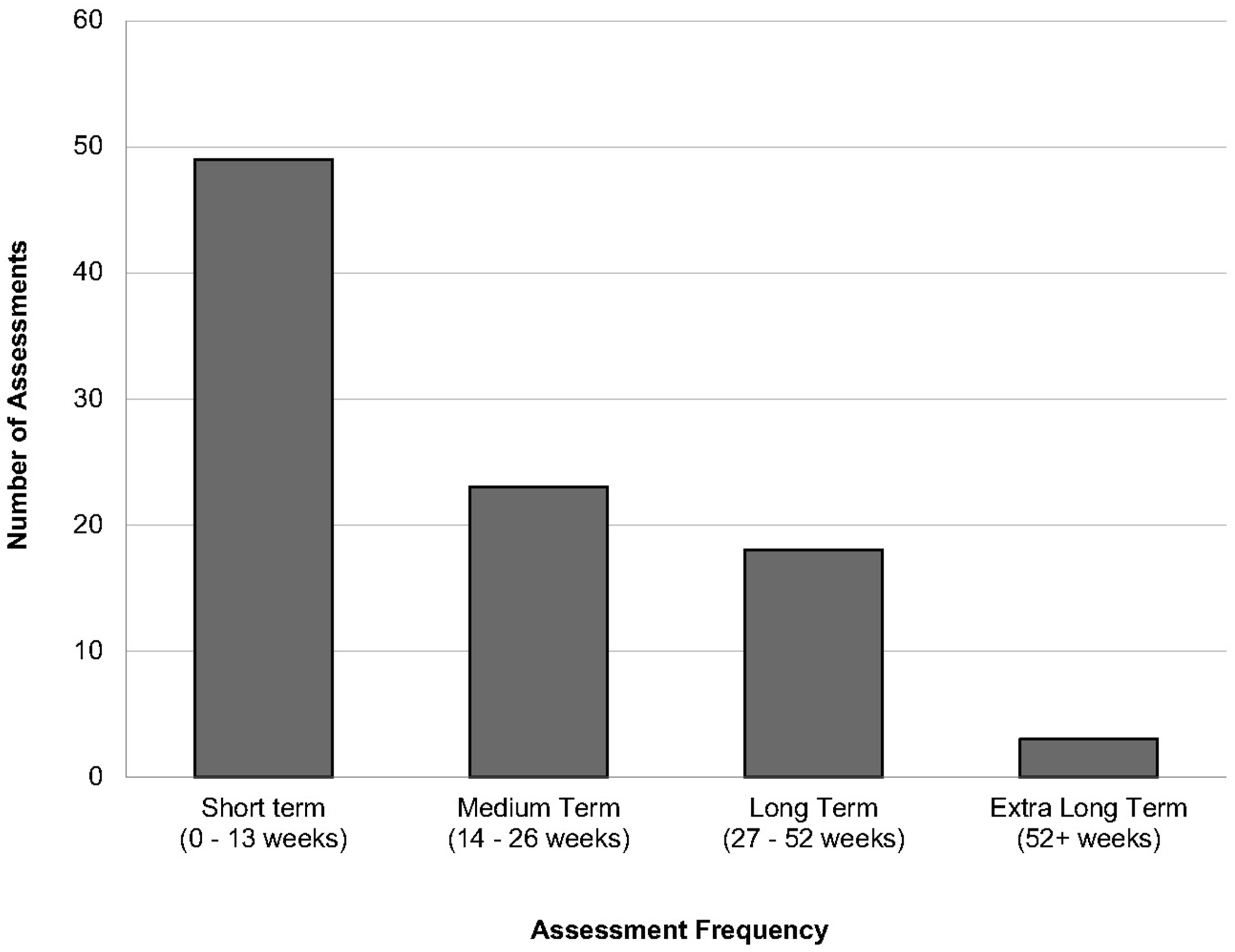
Primary and Secondary Outcomes
Among the 49 analyzed studies, 32 (65.3%) specified primary outcomes (Figure 3). Pain-related measures were the most common, with 16 (50.0%) evaluating pain intensity and 4 (12.5%) evaluating pain interference. Physical function was also frequently designated as a primary outcome, assessed by self-report in 12 studies (37.5%) and by performance-based measures in 2 (6.3%). Primary and secondary outcomes of the analyzed studies categorized by domain. “Other” category included outcomes that were not found in more than one study. Examples include outcomes that measured stiffness, miscellaneous pain behaviors, spousal emotional support, perceived quality of care, effective communication with physicians, and study acceptability/feasibility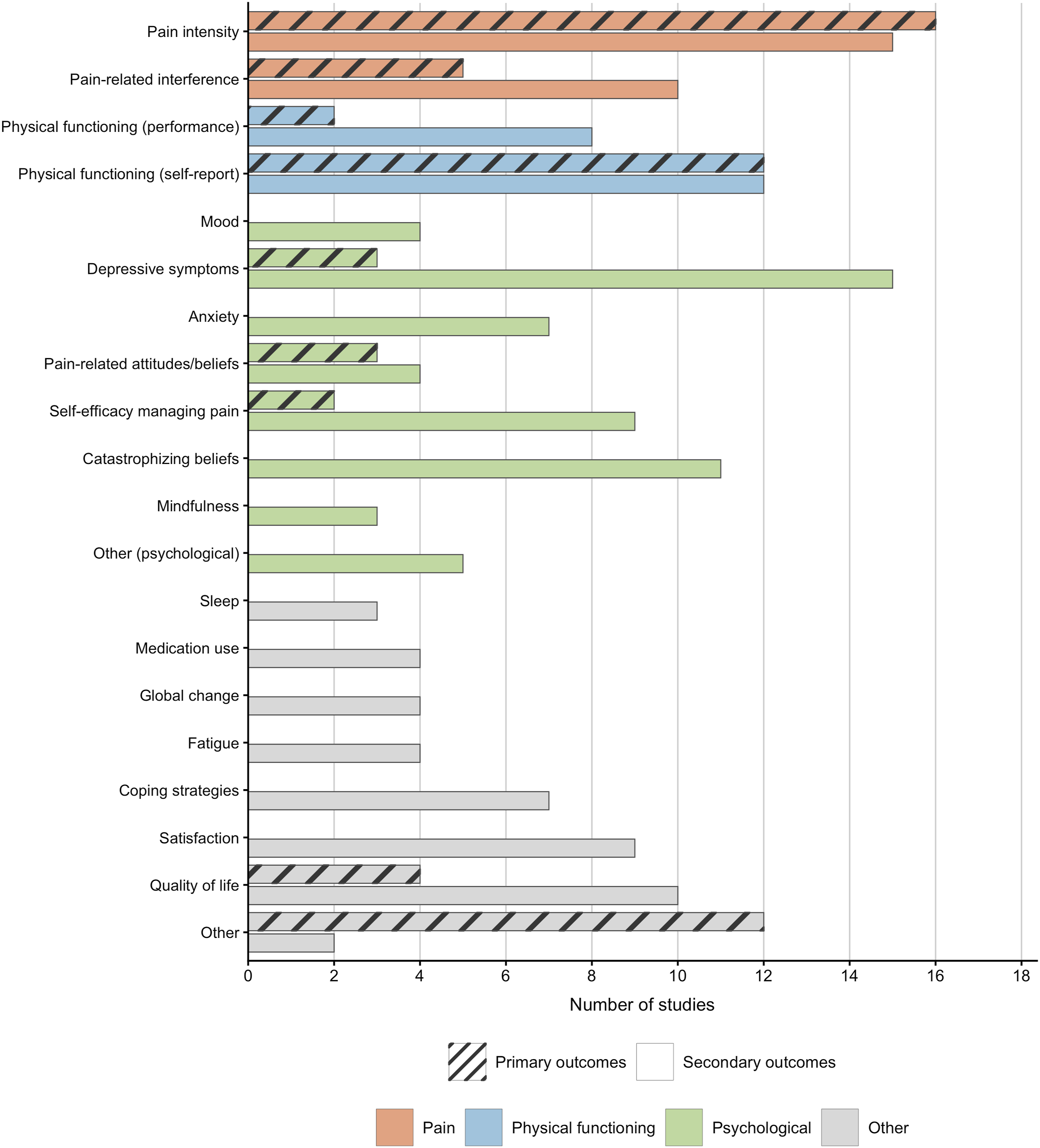
Psychological constructs were less frequently prioritized as primary outcomes. Three studies (9.4%) examined depressive symptoms, three (9.4%) examined pain-related beliefs, and two (6.3%) assessed self-efficacy for managing pain. Quality of life was designated as a primary outcome in four studies (12.5%). Thirteen studies (40.6%) reported diverse “other” primary outcomes, each represented in only a single trial. These included domains such as satisfaction, coping, sleep, catastrophizing, kinesiophobia, communication, and feasibility (see Figure 3).
In the same subset of 32 studies, secondary outcomes were categorized into 20 domains, including an “other” category (Figure 3). Pain-related measures were again the most common, with 15 studies (46.8%) evaluating pain intensity and 10 (31.3%) evaluating pain interference. Physical function was assessed by self-report in 12 studies (40.0%) and by performance-based measures in 8 (25.0%).
Psychological outcomes spanned multiple constructs. Depressive symptoms were the most common, assessed in 15 studies (50.0%), followed by catastrophizing beliefs in 11 (36.7%), self-efficacy in 9 (28.1%), coping strategies in 7 (21.9%), and pain-related beliefs in 4 (12.5%). Anxiety was assessed in seven studies (21.9%), mood in four (12.5%), mindfulness in three (9.4%), and other psychological outcomes in five (15.6%). Quality of life was assessed in 10 studies (31.3%). Additional outcomes included satisfaction in nine studies (28.1%), medication use in four (12.5%), fatigue in four (12.5%), global change in four (12.5%), and sleep in three (9.4%).
Compared with primary outcomes, psychological and psychosocial constructs were more frequently included as secondary endpoints, suggesting these domains are commonly measured but rarely prioritized.
The 17 studies that did not specify primary or secondary outcomes showed a more even distribution of measures across pain intensity, self-reported physical function, and psychological domains.
Discussion
Map of Evidence
This scoping review examined existing randomized trials of psychosocial interventions in older adults with chronic non-cancer pain. Among trials that specified primary outcomes (n = 32), pain intensity (53.1%) and self-reported physical function (37.5%) predominated, whereas psychological endpoints and pain interference were rarely designated as primary outcomes despite most interventions targeting cognitive and emotional processes such as psychological flexibility, coping, and emotional regulation. Psychological domains, particularly depressive symptoms (50%) and catastrophizing (36.7%), were commonly assessed as secondary outcomes. Sleep and quality-of-life measures were infrequently prioritized, and heterogeneity across instruments limited comparability. Additionally, 17 trials did not specify primary or secondary outcomes, further complicating interpretation. Samples were predominantly female but importantly race and ethnicity were frequently unreported. This underreporting limits interpretation and generalizability, highlighting the need for standardized reporting in all future trials. Brief, scalable formats and remote or hybrid delivery models may improve access for older adults who are limited by cognitive deficits, mobility, and transportation.
Comparison With Prior Reviews
The current scoping review extends this body of work by systematically characterizing 49 studies of psychosocial interventions for chronic pain among older adults with an emphasis on intervention design, implementation, and reporting practices. Compared with prior reviews that emphasized treatment efficacy or single-modality outcomes, our review provides a comprehensive mapping of intervention components, delivery contexts, and reporting rigor. Importantly, we found that reporting practices varied widely: intervention adherence was reported in 65.3% of studies, intervention credibility in 20.4%, fidelity in 30.6%, and adverse events in 30.6%. By identifying substantial heterogeneity and underreporting in key implementation domains, this work extends the literature beyond efficacy and offers insights into how, where, and by whom non-pharmacological interventions for chronic pain among older adults are delivered and evaluated.
Analysis of Outcome Prioritization
Although over half of all analyzed studies designated physical function as a primary outcome, few articulated a theoretical or empirical mechanism for how psychosocial interventions might improve physical function. One theory may be that these psychosocial interventions target constructs like behavioral activation, coping self-efficacy, psychological flexibility, and emotion regulation, which may support daily functioning in the presence of chronic pain. In contrast, relatively few psychosocial modalities mainly target reductions in pain perception. In geriatric care, where the primary goal is maintaining independence, functional gains are clinically meaningful irrespective of the continued nociceptive pain.
Despite psychosocial interventions being designed to target cognitive and emotional processes, psychological outcomes were rarely assessed as primary endpoints. Only a quarter of the studies examined psychological constructs (e.g., self-efficacy, pain-related attitudes/beliefs, or depression), and just three studies assessed depressive symptoms specifically. Most trials instead prioritized pain intensity and physical function. The limited prioritization of psychological primary outcomes restricts the ability to examine the mechanisms of change for pain management in an older adult population with complex and understudied needs.
Although infrequently assessed as primary outcomes, depressive symptoms were assessed as secondary outcomes in over half of the analyzed studies, potentially reflecting interest in the bidirectional relationship between chronic pain and mood disturbances. Given that there is strong evidence for this relationship, the limited prioritization of psychological endpoints represents a missed opportunity for further characterization of treatment effects (De la Rosa et al., 2024; Werneck et al., 2024). Pain catastrophizing was also frequently evaluated as a secondary outcome, particularly among CBT-based interventions. Prior evidence suggests that reductions in pain catastrophizing mediate improvements in pain intensity, functional status, and mood (Burns et al., 2021; Miró et al., 2018). Given its central role as a potential mechanism of change, pain catastrophizing should be consistently assessed in future CBT trials for older adults. More broadly, measuring constructs like pain catastrophizing, emotional regulation, and positive affect may improve the ability to detect mediators of treatment response and guide optimization for future psychosocial trials.
Further, very few studies examined sleep as a primary outcome or secondary outcome despite the well-established bidirectional link between chronic pain and sleep disturbances particularly in older adults (Griffin et al., 2021; Runge et al., 2024). Given age-specific changes in sleep patterns, future studies examining interventions for older adults with chronic pain should explore sleep duration and quality as potential mediators of pain reduction.
Delivery and Feasibility
For older adults, the value of psychosocial interventions is highly dependent on feasibility of delivery. Since COVID-19, delivery models for psychosocial interventions for pain have expanded to include more self-directed and internet-delivered formats. These approaches may enhance scalability and reduce personnel costs to deliver the intervention. CBT for chronic pain has been the most widely studied across both face-to-face and internet-based delivery methods; however, direct head-to-head trials comparing in-person versus internet-delivered CBT for chronic pain remain limited and should be prioritized. Older adults may face barriers to internet-delivered interventions such as digital literacy, cognitive capacity, and sensory impairments. As a result, research that incorporates caregiver support, hybrid models, and user-centered designs will be essential for effective and feasible interventions. Feasibility of psychosocial interventions for pain remains a key concern, given the long duration and intensity of many current intervention protocols. In this review, the average intervention dose was 13.5 hours (SD = 10.8) delivered over an average of 9.6 weeks (SD = 7.5). Developing and evaluating condensed interventions may enhance feasibility and patient adherence. For instance, Empowered Relief (ER), a single-session, 2-hour CBT-informed intervention, has demonstrated comparable outcomes on pain and related variables compared to an 8-session CBT protocol (Darnall et al., 2021, 2024). Further, older adults may face practical barriers, such as transportation, to completing multi-week protocols. Future trials should investigate condensed psychosocial interventions among older adults to enhance real-world feasibility and implementation.
Research Implications
This review found that evidence is currently concentrated on a few specific interventions, that is, CBT and self-management modalities. Promising alternative approaches such as ACT, EAET, and positive affect-based interventions remain understudied in older adults. These modalities should be tested in adequately powered, comparative-effectiveness trials against CBT, the current reference standard. Early trials for EAET in older adults have suggested advantages over CBT in several outcomes including pain intensity, mental health, and satisfaction (Yarns et al., 2024). In addition, pain reprocessing therapy (PRT) in middle-aged adults with chronic pain has shown promising large and durable reductions in pain intensity (Ashar et al., 2022, 2025). PRT and EAET may represent an emerging category of interventions that focus on recalibrating centralized pain processing beyond traditional coping-focused frameworks like CBT. The early positive findings of these novel psychosocial interventions for chronic pain, combined with the underrepresentation of therapies such as ACT in older populations (Hughes et al., 2017; Ye et al., 2024), justify targeted evaluation of these modalities in older adults.
Measurement and Reporting Recommendations
To improve interpretability and replication, trials should pre-register primary endpoints and power analyses, and routinely report adherence, treatment fidelity, and harms using CONSORT-SPI and TIDieR guidance for psychosocial interventions (Grant et al., 2019; CONSORT-SPI Group). Inconsistent reporting of adherence and fidelity limits the interpretability of null findings, as poor engagement could be misinterpreted as a lack of intervention efficacy. Among the studies that assessed treatment fidelity, most relied on researcher review of audio or video recordings of sessions using standardized rating instruments. Most studies also reported standardized interventionist training prior to trial initiation, which may have reduced delivery variability. However, without formal fidelity assessments, it remains difficult to isolate intervention effects from potential variability in delivery. This is particularly relevant in older adult trials where interventions often require adaptations for cognitive, sensory, and functional limitations. Fidelity monitoring is also important in diverse care settings, where cultural and contextual adaptations may be needed to maximize engagement.
Equity and Generalizability
Generalizability is limited by the underreporting of race and ethnicity and the limited percentage of non-white participants in the included studies. Studies have shown that Black, Indigenous, and People of Color (Boyd et al., 2024) are persistently underrepresented in US-based chronic pain trials. Cultural tailoring of interventions, intentional recruitment from diverse communities, and evaluation of intervention acceptability across cultural contexts should be prioritized to avoid exacerbating inequities in chronic pain care for older adults (Boyd et al., 2024; Janevic et al., 2022).
Strengths, Limitations, and Future Directions
Strengths include a prespecified approach, comprehensive multi-database search, duplicate screening and data charting, and a focus on randomized evidence. This scoping review has several limitations that warrant consideration. As a scoping review, we did not conduct formal risk of bias assessment and therefore did not report on intervention effectiveness or perform meta-analyses. The review was limited to published studies in English indexed in major databases. The review was restricted to randomized-controlled trial design, including randomized comparative efficacy clinical trial design, which may have excluded promising feasibility, single-armed, or implementation trials. Included studies demonstrated substantial heterogeneity which limited direct comparisons between interventions and precluded formal synthesis of effect sizes. Additionally, the lack of standardized outcome measures, particularly for psychological domains, made it difficult to determine which domains may function as mediators for pain reduction. Most included trials were also conducted under controlled conditions, often with trained interventionists in small group or individual formats.
Future directions include conducting pragmatic trials in diverse healthcare systems and community settings to assess implementation feasibility in the older adult population. Finally, the lack of racial and ethnic diversity across the reviewed studies raises important questions about the equity of psychosocial pain interventions. Without intentional recruitment of diverse older adults and cultural adaptations, future psychosocial intervention development risks exacerbating existing disparities in chronic pain care.
Conclusion
This review highlights both the progress and limitations of current research on psychosocial interventions for chronic pain in older adults. Of the studies that met the criteria for this review, the most commonly reported primary outcomes were related to perceptions of pain, such as pain intensity and management, and physical functioning. Psychological constructs, such as depressive symptoms and self-efficacy, were seldom reported as primary outcomes. The most commonly implemented intervention was CBT. Future studies in this population should prioritize emerging therapies such as ACT, EAET, positive affect-based interventions, and PRT. Aligning primary outcomes with intervention mechanisms, standardizing reporting of adherence, fidelity, and adverse events, evaluating brief, scalable formats, and diversifying samples will strengthen the evidence base and help advance the standard of care for older adults with chronic pain.
Supplemental Material
Supplemental Material - Psychosocial Interventions for Chronic Non-Cancer Pain Among Older Adults: A Scoping Review
Supplemental Material for Psychosocial Interventions for Chronic Non-Cancer Pain Among Older Adults: A Scoping Review by Ethan L. Low, Sidney L. Gibson, Keya B. Patel, Andy Hickner, Mubarak O. Sanni, Clara J. Scher, and M. Cary Reid in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors thank Ms Elizabeth Edmund; Ms Emma Hemmings, MA; Mr Olaniyi Olaleye; and Mr Erik Siu of the Samuel J. Wood Library for their assistance in obtaining full text of studies.
Ethical Considerations
Ethical approval was not required.
Author Contributions
Ethan L. Low: Conceptualization (equal); methodology (equal); data extraction (equal); writing—original draft (lead); formal analysis (lead); data curation (lead); visualization (lead); writing—review and editing (equal). Sidney L. Gibson: Data extraction (equal); formal analysis (supporting); data curation (supporting); writing—original draft (supporting); writing—review and editing (equal). Keya B. Patel: Data extraction (equal); visualization (supporting); data curation (supporting); writing—original draft (supporting); writing—review and editing (equal). Andy Hickner: Methodology (equal); data extraction (supporting); data curation (equal); writing—original draft (supporting); writing—review and editing (supporting). Mubarak O. Sanni: Data extraction (supporting); formal analysis (supporting); writing—review and editing (supporting). Clara Scher: Conceptualization (equal); methodology (equal); data extraction (supporting); writing—original draft (supporting); writing—review and editing (equal). M. Cary Reid: Conceptualization (equal); methodology (equal); data extraction (equal); writing—original draft (supporting); writing—review and editing (equal).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by grants from the National Institute on Aging (K24AG053462, P30 AG02284).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No new data was created in this scoping review. All data summarized are derived from previously published studies cited in the article. The data-extraction codebook and any additional materials are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.