
Abstract
Background
Prior studies on marital satisfaction and health rarely consider whether improvements and declines have asymmetric effects. This study examined asymmetric associations between changes in marital satisfaction and frailty among older adults.
Methods
Data came from 4,833 married adults aged 65+ in the Korean Longitudinal Study of Aging. Frailty was assessed using a 41-item deficit-accumulation frailty index (0–100). Asymmetric fixed effects models distinguished the effects of increases versus decreases in marital satisfaction. Unconditional quantile regression within a fixed effects framework examined heterogeneity across the frailty distribution.
Results
Declines in marital satisfaction were associated with larger increases in frailty than the reductions linked to comparable improvements. Among women, associations were largely symmetric. Among men, declines in marital satisfaction were strongly associated with higher frailty, whereas improvements showed limited protective effects, particularly at mid-to-upper frailty levels.
Conclusion
These findings highlight gendered and asymmetric health consequences of marital relationships in later life.
• Introduces an asymmetric perspective by revealing that declines in marital satisfaction were associated with nearly three times larger increases in frailty (β = 0.074) than the reductions associated with comparable improvements (β = −0.028; Wald test, p < .001). • Reveals gender-specific asymmetry, by showing that the detrimental impact of declining marital satisfaction is particularly pronounced among older men (β = 0.085, p < .001), whereas no significant asymmetry was found among women. • Identifies distributional heterogeneity, by documenting that asymmetric effects among men are strongest at higher levels of frailty (β = 0.065 at the 80th percentile), highlighting vulnerability clustering within already at-risk groups.
• In contexts characterized by strong family-centered care structures (e.g., South Korea), incorporate routine assessment of marital/relationship quality into frailty risk screening, particularly for older men and those already exhibiting moderate frailty. • Design couple-based or relational support interventions within aging and community health programs to prevent frailty progression linked to relational deterioration. • Encourage life-course and distribution-sensitive modeling approaches that account for relational dynamics, gender differences, and asymmetric health effects when examining social determinants of aging.What This Paper Adds
Applications of Study Findings
Introduction
Marital relationships represent one of the most enduring and influential social ties in later life, a period characterized by the contraction of social networks and increasing reliance on emotionally meaningful relationships. According to socioemotional selectivity theory, older adults selectively invest in close ties that provide emotional fulfillment, often prioritizing spouses over more peripheral social connections (Carstensen, 1992; Carstensen et al., 1999). As a result, spouses frequently serve as primary sources of emotional support, companionship, and instrumental assistance in later adulthood, rendering the subjective quality of the marital relationship particularly salient for health and functional aging (Cornwell & Waite, 2009; J. Kim & Hwang, 2024). Reflecting this shift, a substantial body of research has moved beyond marital status to emphasize qualitative dimensions of marriage, demonstrating that marital satisfaction and relationship quality are closely linked to a wide range of health outcomes, including physical health, psychological well-being, and mortality risk among older adults (Lawrence et al., 2019; Liu et al., 2021; Robles et al., 2014). This growing focus on relationship quality is especially relevant in the context of population aging, where preserving functional capacity and resilience has become a central public health priority.
Frailty has emerged as a key indicator of health and functional decline in older adulthood, capturing the cumulative burden of physiological deficits across multiple domains, such as physical functioning, cognitive status, and chronic disease burden (Fried et al., 2001; Rockwood & Mitnitski, 2007). Unlike single disease outcomes, frailty reflects overall vulnerability to stressors and a reduced capacity to maintain physiological homeostasis, making it particularly well suited for examining how social and relational contexts shape aging trajectories (Clegg et al., 2013). A growing literature suggests that psychosocial resources—including social support, emotional well-being, and relationship quality—are closely linked to frailty risk and progression, underscoring the role of social environments in buffering age-related decline (Gale et al., 2018; Hoogendijk et al., 2019; Mehrabi et al., 2024). Given the significance of marital relationships in later life, examining the association between marital satisfaction and frailty offers important insight into the social determinants of functional aging and the ways in which close interpersonal relationships may contribute to resilience or vulnerability in old age (J. Kim et al., 2025).
Several interrelated mechanisms may link marital satisfaction to frailty in later life. High-quality marital relationships can promote health by reducing chronic stress exposure and enhancing emotional regulation, whereas marital strain may activate prolonged stress responses that accelerate physiological dysregulation across multiple systems (Kiecolt-Glaser & Newton, 2001; Umberson et al., 2010). Supportive marriages may also facilitate healthier behaviors through mutual monitoring, encouragement of medical adherence, and coordinated health-promoting routines, while distressed relationships may undermine such behaviors and contribute to maladaptive coping strategies (DiMatteo, 2004; Robles et al., 2014). In addition, spouses often play a central role in providing instrumental assistance, compensating for functional limitations (J. Kim & Kwon, 2024), and buffering the impact of age-related health shocks, thereby influencing the accumulation of deficits that characterize frailty (Cornwell & Waite, 2009; Hoogendijk et al., 2019). Psychological pathways are also salient, as marital dissatisfaction has been linked to depressive symptoms, loneliness, and diminished sense of purpose, all of which are independently associated with increased frailty risk (Andrew & Keefe, 2014; Gale et al., 2018). Through these psychosocial, behavioral, and stress-related pathways, the quality of marital relationships may shape trajectories of functional decline and vulnerability in later life.
The health implications of marital satisfaction may exhibit asymmetric effects, where declines in relationship quality exert stronger effects on health deterioration than improvements confer protective benefits. From a stress process perspective, deteriorations in marital satisfaction may represent salient stressors that trigger acute or chronic psychological distress, disrupt emotional regulation, and intensify physiological wear and tear, thereby accelerating the accumulation of deficits that characterize frailty (Kiecolt-Glaser & Newton, 2001; Pearlin et al., 2005). In contrast, increases in marital satisfaction may yield more modest health gains, particularly in later life when physiological reserve is already diminished and opportunities for recovery are constrained. This asymmetry is consistent with broader evidence of loss aversion and negativity bias in health processes, whereby adverse social experiences exert disproportionately larger effects than positive experiences of comparable magnitude (Baumeister et al., 2001; Taylor, 1991). Moreover, declines in marital satisfaction may undermine existing support structures and coping resources that older adults rely on to manage functional limitations, whereas improvements may primarily reinforce already established patterns of support (Thoits, 2011). However, most prior studies rely on conventional regression approaches that implicitly impose symmetry, thereby overlooking the possibility that declines and improvements in marital satisfaction have unequal health consequences.
These asymmetric processes are likely to unfold differently for women and men, given long-standing gender differences in marital roles, emotional labor, and dependence on spousal relationships in later life (Park & Kim, 2025; Waite & Gallagher, 2001). Prior research suggests that women tend to maintain broader emotional coping resources and social support networks beyond the marital relationship, whereas men are more likely to rely heavily on their spouse as their primary source of emotional support, companionship, and health-related assistance (Thoits, 2011; Umberson et al., 2010). As a result, declines in marital quality may represent a particularly salient stressor for men, disrupting key sources of emotional regulation and instrumental support that are closely tied to daily functioning and health maintenance in older adulthood (Kiecolt-Glaser & Newton, 2001; Pearlin et al., 2005). In contrast, women may experience both improvements and deteriorations in marital satisfaction as meaningful but comparatively balanced influences on health, given their greater capacity to draw on alternative support systems and adaptive coping strategies (Taylor et al., 2000; Thoits, 2011). Based on these gendered patterns, we hypothesize that decreases in marital satisfaction may exert disproportionately stronger effects on frailty among men than among women, whereas improvements may yield no significant differences across genders.
Furthermore, these gendered dynamics may further depend on individuals’ position within the frailty distribution, reflecting heterogeneity in physiological reserve and coping capacity in later life (Fried et al., 2001; Rockwood & Mitnitski, 2007). Frailty is inherently a cumulative and stratified process, and individuals at higher levels of frailty may be more sensitive to psychosocial stressors that disrupt emotional stability and daily functioning (Clegg et al., 2013; Gale et al., 2018). In this context, declines in marital satisfaction may exert increasingly deleterious effects among more frail individuals, particularly when spousal relationships serve as a primary source of emotional regulation and instrumental support (Cornwell & Waite, 2009; Kiecolt-Glaser & Newton, 2001). Gendered patterns in social dependence further suggest that this vulnerability may be more pronounced for men, who tend to rely more heavily on their spouse as their central support figure in later life (Antonucci & Akiyama, 1987; Umberson et al., 2010). As frailty increases and alternative coping resources become more limited, deteriorations in marital quality may therefore accelerate functional decline among men, whereas improvements in marital satisfaction may yield more modest health gains (Pearlin et al., 2005).
Building on this literature, the present study examines the association between marital satisfaction and frailty in later life using longitudinal data from a nationally representative sample of older adults in South Korea. We move beyond prior work in three key ways. First, rather than focusing solely on average associations, we assess whether changes in marital satisfaction are differentially related to frailty when marital satisfaction increases versus decreases, allowing for potential asymmetry in their health consequences. Second, we examine gender differences in these associations, recognizing that marital roles, support dynamics, and health vulnerability may operate differently for women and men in older adulthood. Third, we investigate whether these relationships vary across the frailty distribution by applying unconditional quantile regression within an asymmetric fixed effects framework, thereby capturing heterogeneity that may be obscured in mean-based models. Together, this approach provides a more nuanced understanding of how marital satisfaction shapes functional aging and contributes to the broader literature on social relationships and health in later life.
Methods
Data
The data for this study are drawn from the Korean Longitudinal Study of Ageing (KLoSA), a nationally representative panel survey of community-dwelling adults aged 45 and older in South Korea. Initiated in 2006, KLoSA has been administered biennially to capture detailed information on respondents’ socioeconomic circumstances, physical and mental health, employment, family structure, and other factors relevant to aging. The sampling frame was derived from enumeration districts defined in the Population and Housing Census conducted by Statistics Korea. Participants were selected using a multi-stage stratified probability sampling design that accounted for both housing type (apartment vs. non-apartment housing) and geographic context (urban vs. rural areas), ensuring representativeness of the older Korean population.
The present study utilizes longitudinal data spanning 12 years, from Wave 1 (2006) through Wave 7 (2018). Among the 18,897 person-wave observations across seven waves for respondents aged 65 or older and currently married, 392 observations with missing values on control variables were excluded, yielding a final sample of 18,505 observations. This represents approximately 2% of the total observations, well below the 5% rate that Schafer (1999) identified as inconsequential for bias, and substantially lower than the 10–20% threshold at which listwise deletion has been shown to produce meaningful bias in regression estimates (Newman, 2014). Because KLoSA is an unbalanced panel, the resulting analytic sample consisted of 4,833 unique individuals (2,153 women and 2,680 men). All respondents provided informed consent at the time of data collection, and KLoSA data are fully anonymized before public release. As this study relied exclusively on secondary analysis of publicly accessible data, it was exempt from ethical approval.
Measures
Dependent Variable
The frailty index was constructed using 41 indicators spanning seven domains, following established operationalizations in prior studies (Fan et al., 2020; Pérez-Zepeda et al., 2021). Items were selected based on a deficit prevalence exceeding 1% and coverage of seven health domains (Searle et al., 2008), further validated by Baek and Min (2022) who constructed a frailty index using the identical item configuration and the same dataset. These domains include self-rated health, physical condition, mental status, cognitive function, limitations in activities of daily living (ADL), limitations in instrumental activities of daily living (IADL), and chronic diseases. Self-rated health was coded on a 0–1 continuum (excellent = 0, very good = 0.25, good = 0.5, fair = 0.75, poor = 1). Physical condition measures—such as grip strength—were dichotomized using sex-specific cutoffs (men: 28.6; women: 16.4), with values above the threshold coded as 0 and those below coded as 1 (Yoo et al., 2017). Body Mass Index (BMI) was also dichotomized, with underweight status (BMI < 18.5) coded as 1 (Li et al., 2020). Mental status was evaluated using the CESD-10, with response options transformed to values between 0 and 1 (rarely/never = 0; some of the time = 0.33; occasionally = 0.66; all of the time = 1) (Irwin et al., 1999). Cognitive functioning was assessed using the Korean Mini-Mental State Examination (K-MMSE), with each component scaled to range from 0 to 1 in accordance with prior coding schemes (Oh et al., 2010). Functional limitations in ADL (e.g., dressing, hygiene, bathing) and IADL (e.g., meal preparation, housework, laundry) were coded as 0 (able), 0.5 (requires assistance), or 1 (unable), based on validated Korean versions of the instruments (Won et al., 2002). The chronic disease domain captured the presence of seven physician-diagnosed conditions—hypertension, diabetes, chronic lung disease, heart disease, stroke, arthritis, and urinary incontinence—as well as regular use of prescribed medications, with all items dichotomized (no = 0; yes = 1). The frailty index was calculated as the mean of the 41 deficit variables multiplied by 100 for interpretability, yielding a 0–100 frailty score. It produces a continuous score reflecting the proportion of age-related health deficits present for each respondent. Detailed descriptions of the items within each domain are available in Table S1 of the online supplementary file.
Independent Variable
Marital satisfaction was measured with a single-item indicator based on the question, “In general, how satisfied are you with your marriage?” (Choi, 2021). Participants rated their satisfaction on a 0–100 scale in 10-point increments, with higher values reflecting greater levels of marital satisfaction. Single-item measures have demonstrated criterion validity comparable to multi-item scales (Riviere & Sinclair, 2023), and predictive utility across health-related outcomes in prior KLoSA studies (Y. Kim, 2021; Min et al., 2020). Because zero is not a substantively meaningful value on this scale, marital satisfaction was entered into all models as a continuous variable on its original 0–100 metric, without mean-centering or standardization; coefficients therefore reflect the change in the 0–100 frailty index associated with a one-point increase in marital satisfaction.
Control Variable
A comprehensive set of covariates was incorporated to account for potential confounding influences: socioeconomic factors (educational attainment, income, homeownership, and employment) to capture material resources that shape both relational quality and health, household characteristics (number of children, household size) to account for variation in informal support availability, and regional covariates to adjust for geographic differences in healthcare access and social infrastructure. Among these factors, time-invariant characteristics included gender, educational attainment (elementary or less, middle school, high school, and college or higher), and the number of children (treated as fixed given the negligible likelihood of change among adults aged 65 and older). Time-varying covariates comprised age, household size (which may change as adult children leave the household), logged household income, homeownership status (owner-occupied vs. privately rented housing), current economic activity (whether the respondent was engaged in economically active employment), and region of residence, categorized as large city, small city, and rural area.
Statistical Analysis
To examine the association between marital satisfaction and frailty, we first estimated pooled ordinary least squares (OLS) models of the following form

To address this concern, we next employed standard fixed effects (FE) models, which exploit within-person variation to control for unobserved time-invariant confounders. The FE specification is given by:

Standard FE models, however, impose a symmetry assumption, implying that increases and decreases in marital satisfaction exert effects of equal magnitude but opposite sign. To relax this assumption, we estimated asymmetric fixed effects models that allow the effects of increases and decreases in marital satisfaction to differ. Specifically, marital satisfaction was decomposed into positive and negative changes



Finally, to explore heterogeneity in the association between marital satisfaction and frailty across the frailty distribution, we estimated unconditional quantile regression (UQR) models within the asymmetric FE framework (Borgen, 2016). This approach yields consistent estimates of covariate effects at different quantiles of the unconditional outcome distribution. To estimate UQR, we replaced the outcome variable in the regression model with the recentered influence function (RIF) (Firpo et al., 2009)

We estimated UQR models separately for the total sample and for women and men, rather than via gender interactions, so as not to impose common covariate effects across groups. Models were fitted at deciles from the 10th through the 90th percentile of the unconditional frailty distribution. The 10th and 90th percentiles were excluded from the main table because the small number of person-waves with frailty values in these tails yielded unstable RIF-regression estimates. To aid interpretation, Table S2 in the online supplementary file reports the values of the frailty index that correspond to the 20th, 40th, 60th, and 80th percentiles of its unconditional distribution (separately for the total sample, women, and men), providing a descriptive anchor for the quantile-specific UQR coefficients.
All analyses were conducted in Stata 18.0 (StataCorp, College Station, TX). Pooled OLS, symmetric FE, and asymmetric FE models were estimated using the reg and xtreg commands with individual fixed effects and cluster-robust standard errors at the person level. Unconditional quantile regressions were estimated using the user-written xtrifreg command (Borgen, 2016), which implements the recentered influence function approach within a two-way fixed effects framework. Tests of asymmetry (H0: β+ = −β-) were conducted using Stata’s test postestimation command. Diagnostic checks based on the pooled OLS specification indicated no evidence of problematic multicollinearity (all variance inflation factors were at or below 3.3, well within the conventional threshold of 10; the correlation between cumulative increases and cumulative decreases in marital satisfaction was 0.51) or undue leverage (maximum leverage statistic = 0.007, with only 1.4% of observations exceeding the conventional 2k/N threshold).
Results
Descriptive Statistics, Korean Longitudinal Study of Ageing (KLoSA), 2006
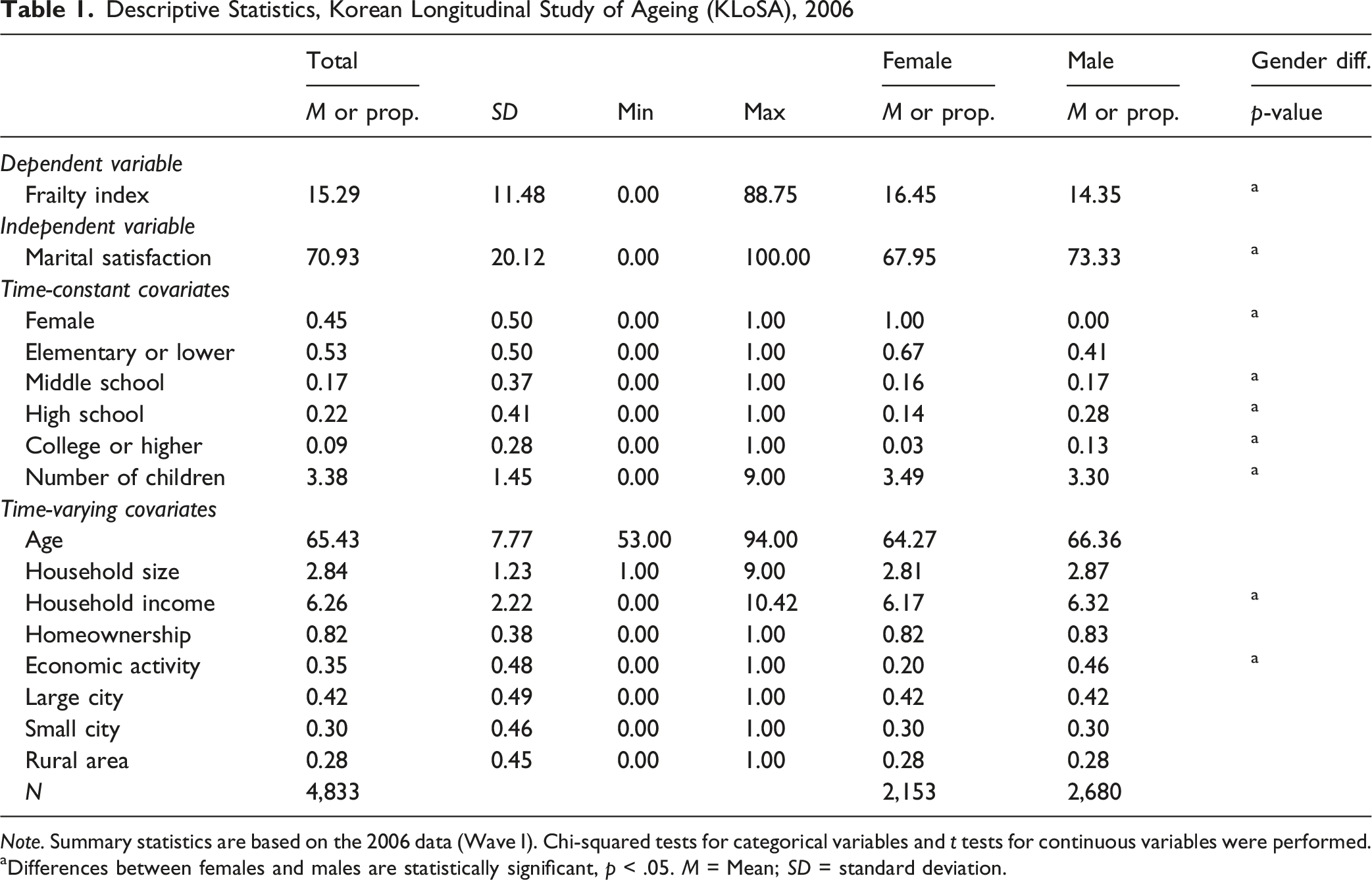
Note. Summary statistics are based on the 2006 data (Wave I). Chi-squared tests for categorical variables and t tests for continuous variables were performed.
aDifferences between females and males are statistically significant, p < .05. M = Mean; SD = standard deviation.
Table S3 in the online supplementary file reports between- and within-person standard deviations of the frailty index, marital satisfaction, and the cumulative increase and decrease terms in the analytic sample. The table shows that within-person variation accounts for approximately 47% of the total variance in marital satisfaction (within SD = 11.91 on a 0–100 scale) and approximately 29% of the total variance in the frailty index (within SD = 6.83). These figures confirm that KLoSA provides substantial within-person variation on both the exposure and the outcome across the seven waves, supporting the value of the FE and asymmetric FE specifications.
The Association Between Marital Satisfaction and Frailty
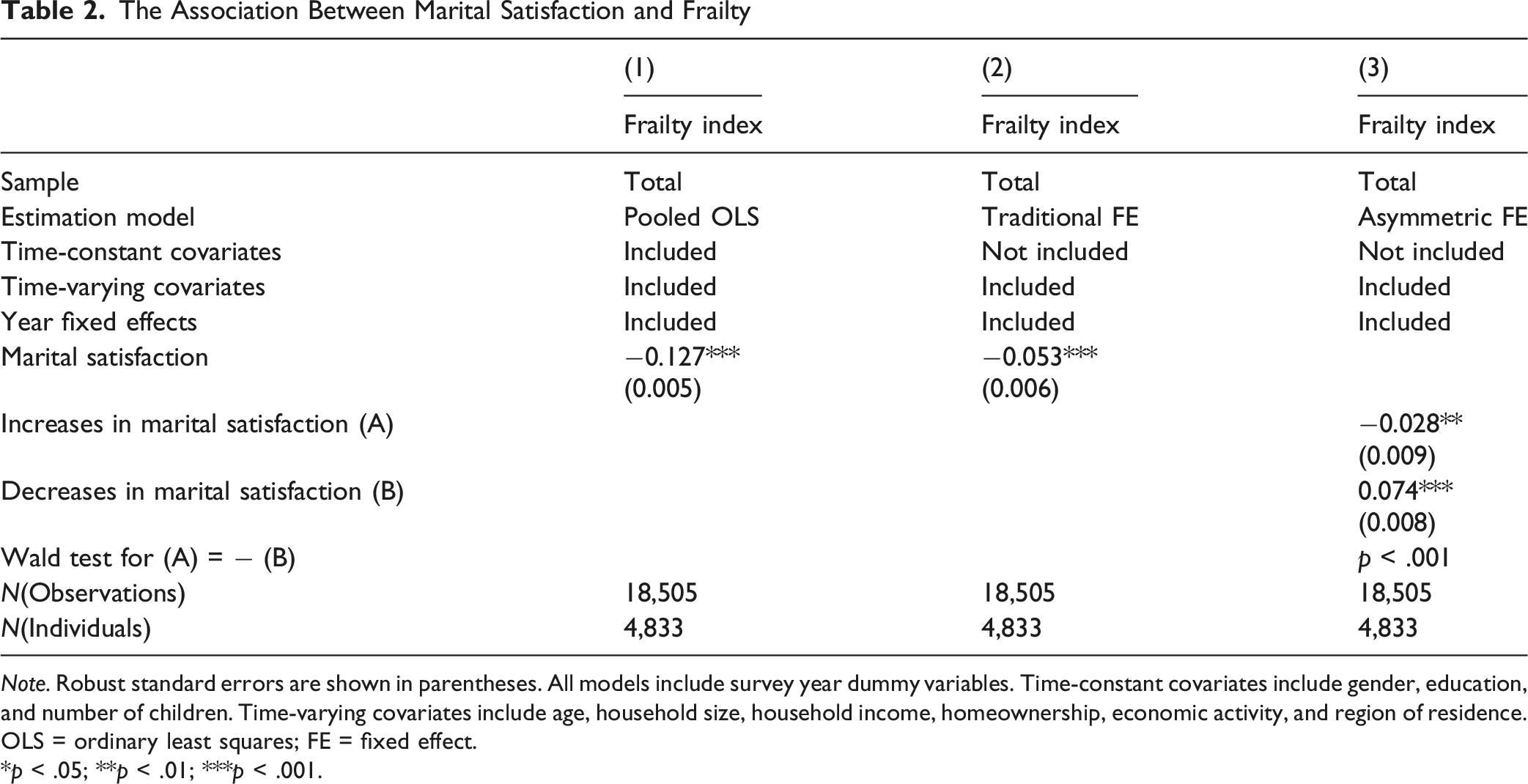
Note. Robust standard errors are shown in parentheses. All models include survey year dummy variables. Time-constant covariates include gender, education, and number of children. Time-varying covariates include age, household size, household income, homeownership, economic activity, and region of residence. OLS = ordinary least squares; FE = fixed effect.
*p < .05; **p < .01; ***p < .001.
The Association Between Marital Satisfaction and Frailty, by Gender
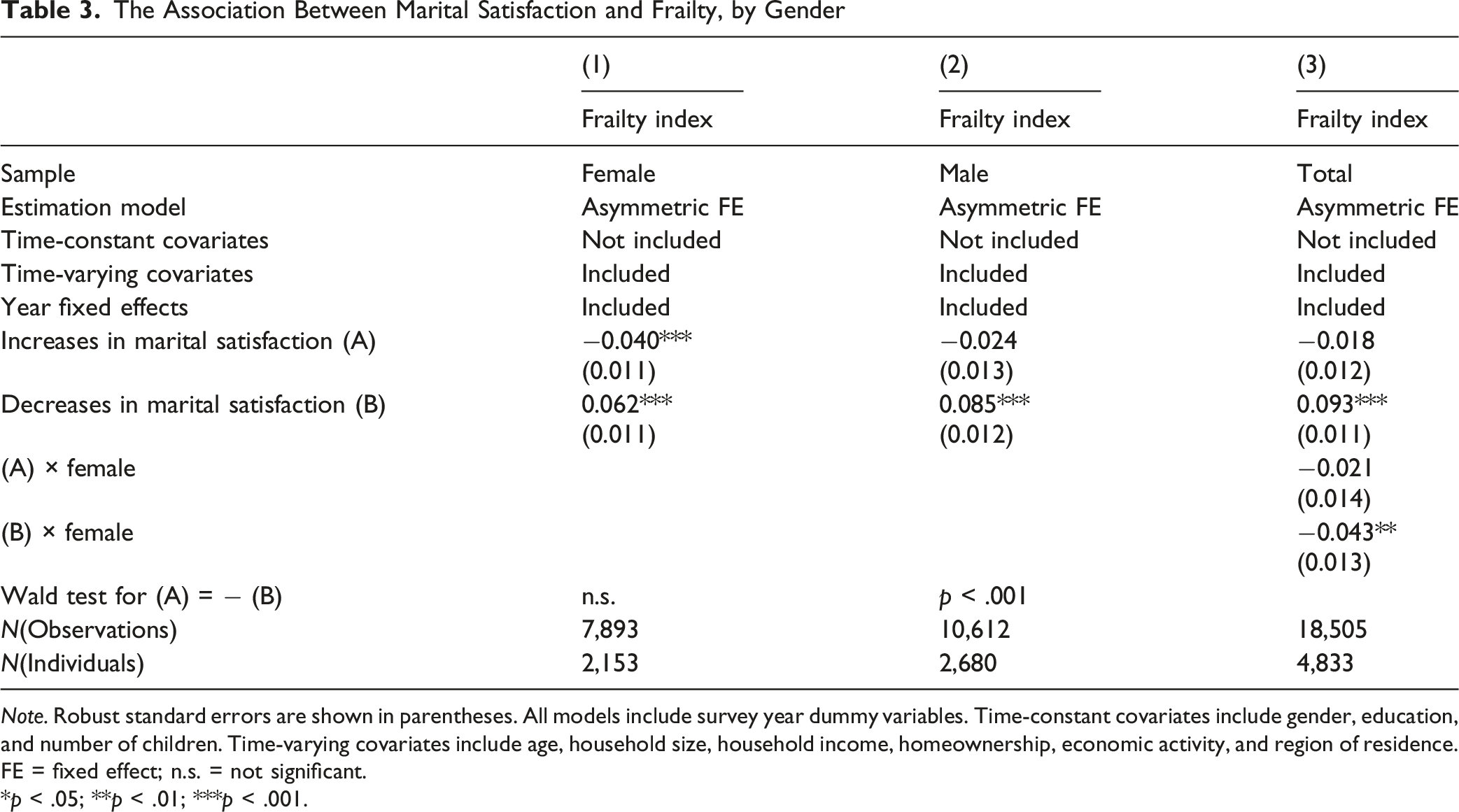
Note. Robust standard errors are shown in parentheses. All models include survey year dummy variables. Time-constant covariates include gender, education, and number of children. Time-varying covariates include age, household size, household income, homeownership, economic activity, and region of residence. FE = fixed effect; n.s. = not significant.
*p < .05; **p < .01; ***p < .001.
Unconditional Quantile Regression Models of the association Between Marital Satisfaction and Frailty

Note. Robust standard errors are shown in parentheses. All models include survey year dummy variables. Time-constant covariates include gender, education, and number of children. Time-varying covariates include age, household size, household income, homeownership, economic activity, and region of residence. FE = fixed effect; n.s. = not significant.
*p < .05; **p < .01; ***p < .001.
Figure 1 presents UQR estimates of the association between changes in marital satisfaction and frailty across the frailty distribution, shown separately for women and men. Among women, both increases and decreases in marital satisfaction are significantly associated with frailty across most quantiles, with increases linked to lower frailty and decreases linked to higher frailty; these associations remain relatively stable across the distribution. Consistent with this pattern, none of the asymmetry tests reached statistical significance at the 0.05 level, indicating no evidence that the effects of increases and decreases differ in magnitude among women. In contrast, the male panel reveals pronounced asymmetry across much of the frailty distribution. Decreases in marital satisfaction are strongly and increasingly associated with higher frailty at higher quantiles, whereas increases in marital satisfaction exhibit comparatively smaller and sometimes statistically insignificant associations. The asymmetry tests are statistically significant across a wide range of mid-to-upper quantiles, providing clear evidence that declines in marital satisfaction are substantially more detrimental for men than comparable improvements are protective. Unconditional quantile regression estimates of the association between marital satisfaction and frailty, by gender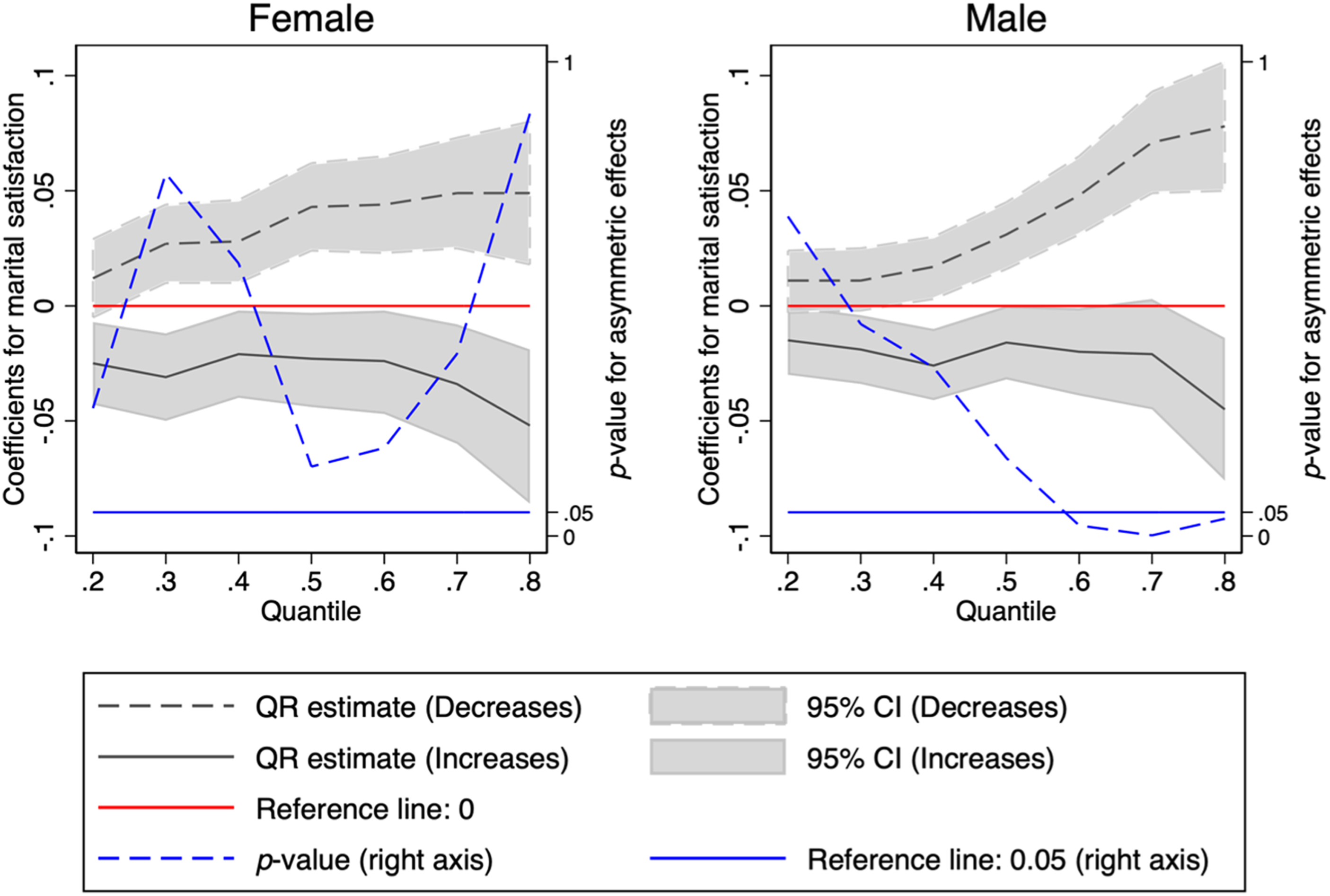
Discussion
The present study sought to examine whether changes in marital satisfaction are associated with frailty in later life and whether these associations are symmetric. While previous research has consistently shown that higher marital satisfaction is associated with better health and functional outcomes (Lawrence et al., 2019; Robles et al., 2014), most studies have implicitly assumed that improvements and deteriorations in relationship quality exert effects of comparable magnitude in opposite directions. Our findings challenge this assumption, as decreases in marital satisfaction (β = 0.074) were associated with approximately 2.6 times larger increases in frailty than the reductions associated with comparable increases (β = −0.028). This asymmetric pattern is consistent with stress process theory and related perspectives emphasizing the disproportionate impact of negative social experiences on physiological dysregulation and health decline (Kiecolt-Glaser & Newton, 2001; Pearlin et al., 2005). Moreover, it aligns with broader evidence from prior research indicating that losses and adverse interpersonal events exert stronger and more enduring effects than gains of similar size (Baumeister et al., 2001; Taylor, 1991).
The gender-stratified analyses further refine our understanding of the asymmetric association between marital satisfaction and frailty by revealing pronounced gender differences in how relational changes are reflected in functional health. Among women, both increases and decreases in marital satisfaction are significantly associated with frailty, but the absence of a significant asymmetry suggests that improvements and deteriorations exert effects of comparable magnitude. This pattern is consistent with prior research indicating that women tend to maintain more diverse social support networks and adaptive coping resources beyond the marital relationship, which may buffer the health consequences of marital strain while also allowing them to benefit from improvements in relationship quality (Thoits, 2011). In contrast, among men, declines in marital satisfaction are strongly associated with increases in frailty (β = 0.085), whereas improvements in marital satisfaction show no corresponding protective effect (β = −0.024) (Courtenay, 2000). This pronounced asymmetry aligns with a substantial body of literature suggesting that men rely more heavily on their spouse as their primary source of emotional support, health monitoring, and daily assistance, rendering them particularly vulnerable to relational deterioration in later life (J. Kim et al., 2025; Waite & Gallagher, 2001).
The distributional analyses further underscore the gendered and asymmetric nature of the association between marital satisfaction and frailty by revealing substantial heterogeneity across the frailty distribution. Among women, increases in marital satisfaction are consistently associated with lower frailty and decreases with higher frailty across most quantiles. However, the absence of significant asymmetry tests indicates that while the direction of change matters, the relative magnitude of gains and losses does not systematically diverge across levels of frailty. This pattern is consistent with prior research suggesting that women’s health is responsive to relationship quality while also buffered by broader coping resources and nonmarital social ties, which may stabilize the impact of marital changes across heterogeneous risk levels (Nam & Kim, 2026; Thoits, 2011; Umberson et al., 2010). In contrast, men exhibit a markedly nonlinear pattern of vulnerability. Declines in marital satisfaction are increasingly associated with higher frailty toward the upper tail of the frailty distribution—reaching approximately 2.5 times the magnitude of improvements at the 60th percentile (β = 0.052 vs. β = −0.021) and 2.2 times at the 70th percentile (β = 0.057 vs. β = −0.026)—whereas improvements in marital satisfaction show comparatively smaller and less consistently detected associations. This “steeper at the top” pattern accords with stress-process and physiological-reserve perspectives, which posit that psychosocial stressors exert stronger effects when physiological reserve is diminished and coping capacity is constrained (Clegg et al., 2013; Rockwood & Mitnitski, 2007). It also aligns with evidence that older men rely disproportionately on spouses for emotional regulation, health monitoring, and instrumental support, rendering relationship deterioration particularly consequential when functional needs are greatest (Song & Kim, 2024).
This study makes several important theoretical and methodological contributions to the literature on social relationships and health in later life. Theoretically, it advances existing work on marital quality by moving beyond static or average associations to conceptualize marital satisfaction as a dynamic, relational process with potentially asymmetric health consequences. By integrating insights from stress process theory, socioemotional selectivity, and cumulative disadvantage perspectives, the study offers a more nuanced framework for understanding how changes in close relationships shape functional aging, particularly under conditions of heightened vulnerability. Methodologically, the application of asymmetric fixed effects models allows for explicit testing of whether increases and decreases in marital satisfaction exert differential effects on frailty, a dimension rarely examined in this literature. In addition, the use of unconditional quantile regression within a fixed effects framework represents a novel contribution, enabling the analysis to capture heterogeneity across the frailty distribution and to identify patterns that would be obscured in mean-based models. Together, these theoretical and methodological innovations provide a more refined understanding of the social determinants of frailty and highlight the importance of considering relational dynamics, asymmetry, and distributional heterogeneity in studies of health and aging.
Despite these strengths, several limitations warrant consideration. First, although the use of longitudinal fixed effects models reduces bias from unobserved time-invariant individual characteristics, the study remains observational and cannot fully establish causal relationships. Unmeasured time-varying factors—such as acute health shocks, changes in caregiving arrangements, spousal health decline, or major marital events—may simultaneously influence marital satisfaction and frailty, potentially biasing the estimated associations. Moreover, potential bidirectionality cannot be ruled out, as worsening frailty may itself erode marital satisfaction over time. Third, potential mediators such as depression, health behaviors, and social isolation are not examined in this study, and future work would benefit from formally testing mediation and moderation where data allow. Fourth, the data do not capture spouses’ marital satisfaction due to limited spousal relationships measures and inconsistent couple identifiers across waves—a notable gap given that marital satisfaction is often shaped by spousal well-being (Carr et al., 2014). Future studies should incorporate dyadic measures to further clarify the mechanisms linking marital satisfaction and frailty. Additionally, the findings may have limited generalizability beyond family-centered contexts like South Korea, where gendered caregiving obligations concentrate support work disproportionately among women and elder care is delegated predominantly to the family rather than the state. The observed effects may thus be less pronounced in societies with stronger public care infrastructure or broader kin-based networks.
The findings of this study have several important policy implications for promoting healthy aging, particularly in family-centered care structures. First, the results underscore the importance of marital and relational contexts as modifiable social determinants of frailty, suggesting that policies aimed at improving older adults’ health should incorporate relationship-centered approaches (Berkman et al., 2000). Programs that promote healthy communication, conflict resolution, and emotional support within long-term partnerships—such as couple-based counseling or relationship enrichment interventions tailored for older adults—may help mitigate the adverse health consequences of declining marital satisfaction (Auclair et al., 2009). Moreover, the heightened vulnerability observed among men, particularly those with elevated frailty, highlights the need for gender-sensitive interventions that explicitly attend to wives’ well-being (Carr et al., 2014). Community-based programs incorporating practical life-skills training may reduce older men’s instrumental dependence on spousal support while alleviating the caregiving burden on wives. More fundamentally, however, these gendered patterns may reflect structural conditions in which elder care is delegated disproportionately to women within families (Jang & Kawachi, 2019). Addressing the upstream drivers of gendered frailty risk will ultimately require expanding public long-term care services and institutional mechanisms that redistribute care responsibilities beyond the spousal dyad, without which couple-level interventions are likely to remain insufficient.
Supplemental Material
Supplemental material—Marital Satisfaction and Frailty in Later Life: Asymmetric, Gendered, and Distributional Associations
Supplemental material for Marital Satisfaction and Frailty in Later Life: Asymmetric, Gendered, and Distributional Associations by NaKyung Nam, Hyunseo Rim, Taehoon Kim, and Jinho Kim in Journal of Applied Gerontology
Footnotes
Acknowledgments
All authors contributed equally to this research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The KLoSA data are available at ![]() with the permission of the Korea employment Information Service. Analytic methods and materials specific to the current study are available upon request from the corresponding author. The current study was not preregistered with an analysis plan in an independent, institutional registry.
with the permission of the Korea employment Information Service. Analytic methods and materials specific to the current study are available upon request from the corresponding author. The current study was not preregistered with an analysis plan in an independent, institutional registry.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.