
Abstract
Background
Cognitive impairment is a major concern in adults aged ≥80, yet evidence on combined social, clinical, nutritional, and psychological influences remains limited in low- and middle-income settings.
Objective
To identify factors associated with cognitive status in community-dwelling oldest-old adults in Türkiye.
Methods
This retrospective cross-sectional study included 295 adults aged ≥80 participating in the YASAM program. Cognitive status, frailty, depression, nutrition, functional ability, and laboratory parameters were assessed using validated tools. Multivariable logistic regression was used to identify factors independently associated with cognitive impairment.
Results
Cognitive impairment was present in 34.2% of participants (mean age 84.5 years; 62.7% female). Older age, female sex, lower education, and being unmarried were associated with impairment. Diabetes, chronic kidney disease, and cerebrovascular disease were more common. Higher frailty and depressive symptoms were associated with cognitive impairment, whereas educational attainment, being married, higher nutritional scores, and hemoglobin levels were associated with better cognitive status.
• Provides a multidimensional analysis of cognitive impairment in the oldest-old population. • Identifies frailty and depressive symptoms as key associated factors beyond chronic disease burden. • Highlights the role of educational, social, nutritional, and hematological factors.
• Integrating frailty and depression screening may improve identification of high-risk individuals. • Addressing nutritional status and anemia may help target potentially modifiable factors. • Community-based social and educational support may support cognitive resilience.What This Paper Adds
Applications of Study Findings
Introduction
The oldest-old population (≥80 years) is expanding rapidly worldwide and is projected to more than triple by 2050, particularly in low- and middle-income countries (“Ageing and health,” 2024). Türkiye is also experiencing this demographic shift, with 10.6% of its population aged 65 years and older; Konya is a central Anatolian city with over 2.2 million inhabitants (“Turkish Statistical Institute, Elderly Statistics,” 2024). This demographic shift presents healthcare challenges related to the identification and management of cognitive impairment.
Cognitive impairment, ranging from mild impairment to dementia, is a major geriatric syndrome associated with reduced independence, poorer quality of life, greater healthcare needs, and mortality (S. Li et al., 2024; Millán-Calenti et al., 2012). In late life, cognitive status is associated with multiple factors, including sociodemographic characteristics (M. Zhang et al., 2015), chronic diseases (Wei et al., 2020; Xing et al., 2024), nutritional status (Bhagwasia et al., 2023; Zhu et al., 2025), mental health, frailty (C. Li et al., 2023), and biological factors such as inflammation and anemia (Wang et al., 2023).
Current dementia prevention frameworks emphasize the multifactorial and potentially modifiable nature of cognitive impairment and support integrated, multidomain approaches to cognitive health (Livingston et al., 2024). However, much of this evidence comes from heterogeneous older adult populations, with fewer studies focusing specifically on the oldest-old. Evidence specific to community-dwelling oldest-old adults in low- and middle-income settings remains limited, especially within comprehensive geriatric assessment frameworks.
Geriatric syndromes such as frailty, malnutrition, depression, and falls are common in the oldest-old and often coexist with cognitive and functional vulnerability. Frailty, characterized by diminished physiological reserve, has been consistently associated with poorer cognitive outcomes in older adults (C. Li et al., 2023; Sharma et al., 2020).
Depression frequently coexists with cognitive impairment and is associated with poorer cognitive outcomes in the oldest-old (van der Slot et al., 2024). Depression and frailty frequently overlap and may reflect a broader vulnerability phenotype associated with cognitive impairment in the oldest-old (Zhao et al., 2024).
Cognitive reserve refers to the brain’s active capacity to cope with or compensate for pathology or damage, thereby helping maintain cognitive performance despite underlying neurobiological changes (Stern, 2002). The cognitive reserve hypothesis suggests that higher educational attainment, lifelong cognitive engagement, and socially stimulating environments may enhance resilience to neurodegenerative processes. In this context, socio-educational factors such as years of schooling and marital status may be associated with better cognitive status through mechanisms related to cognitive reserve and social engagement (Mao et al., 2019; Stern, 2002; D. Zhang et al., 2024).
Nutritional status is another important determinant; malnutrition is common in this age group and is associated with cognitive deterioration (Dominguez & Barbagallo, 2018; Feng et al., 2022). In addition, anemia and inflammatory markers such as the neutrophil-to-lymphocyte ratio have been explored as biological correlates of cognitive status (Wang et al., 2023).
Despite extensive research in high-income countries, evidence on the determinants of cognitive health in the oldest-old residing in low- and middle-income countries remains scarce. In Türkiye, most investigations have focused on younger segments of the older population or on institutionalized individuals, with limited data from community-dwelling adults aged ≥80 years. Moreover, while healthy aging programmes have been shown to reduce mortality and fall risk, improve physical and cognitive status and optimize healthcare utilization (Cesari et al., 2022), their evaluation in the oldest-old Turkish population is lacking. To address this gap, the Turkish Ministry of Health launched YASAM in 2023, providing nationwide, comprehensive geriatric assessments for home-dwelling oldest-old adults. Prior YASAM-based studies mainly focused on healthcare utilization, geriatric vulnerability, emergency department use, and short-term outcomes (Katipoglu et al., 2025; Katipoglu & Kocyigit, 2025)
Materials and Methods
Study Design and Settings
This retrospective cross-sectional study was conducted between February and November 2024 at the Healthy Aging Center (YASAM) of University of Health Sciences, Beyhekim Training and Research Hospital, Konya, Türkiye. YASAM is a population-based program targeting community-dwelling adults aged 80 years and older. During the study period, 378 individuals were identified through the YASAM registry and were evaluated as part of routine follow-up.
Medical records of participants who underwent a comprehensive geriatric assessment at admission were reviewed retrospectively. To minimize confounding, exclusion criteria were applied. Accordingly, individuals with a prior diagnosis of dementia (n = 27) were not included in the study. Participants with active infection (n = 3), malignant disease (n = 17), and rheumatological disease (n = 6) were excluded, as these conditions may increase systemic inflammation and potentially affect neutrophil-to-lymphocyte ratio (NLR) and monocyte-to-lymphocyte ratio (MLR). In addition, individuals who had received vitamin B12 replacement therapy within the previous 6 months (n = 21) were excluded, as this may alter serum vitamin B12 levels and obscure its association with cognitive status. Participants with incomplete clinical data (n = 9) were also excluded from the analysis.
After applying these criteria, a total of 295 participants were included in the final analysis. All assessments used in this study were obtained during the initial comprehensive geriatric evaluation performed as part of routine YASAM care.
Implementation of the YASAM
Participant data were sourced from the YASAM Project of the Turkish Ministry of Health, a nationwide public health initiative that includes records of community-dwelling adults aged ≥80 years followed within a structured healthy aging framework. YASAM is designed as a population-based initiative aiming to systematically reach all community-dwelling adults aged ≥80 years within defined geographic regions. The program is implemented nationwide, with designated Healthy Aging Centers established across secondary and tertiary healthcare institutions, ensuring standardized and coordinated delivery of comprehensive geriatric assessment services throughout the country.
The participants are identified through official population registries integrated into the primary healthcare system. Recruitment is conducted through proactive outreach rather than self-referral; specifically, individuals are contacted via telephone by the program coordination team to schedule comprehensive geriatric assessment visits. No recruitment through advertisements, flyers, or voluntary application is performed.
Eligibility criteria for participation in the YASAM program include. (1) age ≥80 years (2) residence in the community (i.e., non-institutionalized) (3) registration within the primary healthcare system.
There are no additional disease-specific inclusion restrictions. The Healthy Aging Team subsequently organizes structured home visits for all individuals who accept participation.
During the initial home visit, comprehensive geriatric assessment is performed according to Healthy Aging Center guidelines by a multidisciplinary team including a specialist physician, specialist nurse, and trained gerontologist. Medical, nursing, nutritional, functional, cognitive, and psychological domains are assessed using standardized forms and validated instruments, as described in the Comprehensive Assessment section. Routine laboratory tests and follow-up procedures are conducted according to the Ministry of Health protocol, with all data recorded electronically.
Comprehensive Assessment
Functional performance was assessed using the Katz Activities of Daily Living (ADL) Index and the Lawton Instrumental Activities of Daily Living (IADL) scales. While the ADL assesses basic self-care activities, the IADL evaluates more complex daily tasks; ADL scores range from 0 to 6, and IADL scores range from 0 to 8, with lower scores indicating greater functional dependence (Arik et al., 2015; Isik et al., 2020).
Vulnerability was assessed using the Clinical Frailty Scale (CFS), which rates individuals on a scale from 1 (very healthy) to 9 (suffering from a terminal illness); higher CFS scores indicate greater frailty. A validity and reliability study of the test in Turkish is available (Aşık et al., 2022; Rockwood et al., 2005).
Nutritional status was evaluated using the Mini Nutritional Assessment–Short Form (MNA-SF), where lower scores correspond to a higher risk of malnutrition; a score of ≤11 was used to define a risk of malnutrition (Sarikaya et al., 2015).
Cognitive status was assessed using the Mini-Mental State Examination (MMSE), which is scored from 0 to 30, with higher scores indicating better cognitive performance. A score of ≤24 was considered indicative of cognitive impairment (Küçükdeveci et al., 2005). Participants who had not completed primary school (≤5 years of formal education) were evaluated using the MMSE version adapted for individuals with low or no formal education (BABACAN-YILDIZ et al., 2016).
Depressive symptoms were assessed using the 15-item GDS, with higher scores denoting greater depressive symptomatology; a cut-off score of ≥5 was used to indicate clinically significant depressive symptoms (Durmaz et al., 2018).
All the instruments used in the study have undergone validity and reliability studies in Turkish, and are widely used in elderly populations.
Additionally, sociodemographic characteristics, comorbidities, and medication use were obtained from medical records. Comorbidities were defined based on documented diagnoses and physician-confirmed assessments as part of the comprehensive geriatric evaluation.
Laboratory Assessments
Laboratory data were retrieved from the hospital information system and included NLR, MLR, urea, estimated glomerular filtration rate (GFR), thyroid-stimulating hormone (TSH), vitamin B12, hemoglobin, and hemoglobin A1c (HbA1c). Blood samples were collected by trained nurses on the day of the comprehensive geriatric assessment after overnight fasting and analyzed the same day using standardized laboratory protocols.
Ethics Statement
The study adhered to the Declaration of Helsinki and received ethical approval from the KTO Karatay University Faculty of Medicine Ethics Committee for Non-Drug and Medical Device Research (approval date: November 28, 2024; decision no: 2024/041). Institutional authorization was also obtained from Konya Beyhekim Training and Research Hospital.
Statistical Analyses
All data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 22.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median (with minimum and maximum values) depending on the data distribution, while categorical variables were presented as frequencies and percentages. The Kolmogorov–Smirnov test was used to assess the normality of the data. Group comparisons were conducted using the independent samples t-test or the Mann-Whitney U test for continuous variables and the Chi-square or Fisher’s exact test for categorical variables. Correlations between non-normally distributed continuous variables were evaluated using Spearman’s correlation analysis.
The dependent variable, cognitive status, was analyzed in relation to chronic kidney disease (CKD), diabetes mellitus (DM), cerebrovascular disease (CVD), age, gender, frailty status, education level, marital status, depression score, Mini Nutritional Assessment (MNA) score, NLR, vitamin B12 and hemoglobin level. Variables that showed a significant association with the MMSE score in univariable analyses were considered for inclusion in the multivariable logistic regression model to identify factors independently associated with cognitive impairment. In addition, variable selection was guided by clinical relevance and existing evidence from the literature to ensure a conceptually sound and interpretable model. Before conducting regression analysis, potential multicollinearity among the independent variables was assessed using variance inflation factor (VIF) values and collinearity diagnostics, confirming that all VIF values were below 2. Although ADL and IADL were associated with cognitive impairment in univariable analyses, they were excluded from the multivariable model because of their overlap with CFS, which already reflects functional dependence. Thus, CFS was retained as the broader indicator of vulnerability to avoid overadjustment. The adequacy of the sample size was assessed based on the number of outcome events. The multivariable model included 13 predictors for 101 cognitive impairment events. Although this was slightly below the traditional 10-events-per-variable rule, variables were selected based on clinical relevance and univariable findings, and the results were interpreted cautiously. A p-value <0.05 was considered statistically significant.
Results
Univariable analyses were performed to assess the associations between individual variables and cognitive status prior to multivariable modeling.
Findings Related to the Descriptive Characteristics of Individuals
Effect of General Characteristics on Cognitive Status
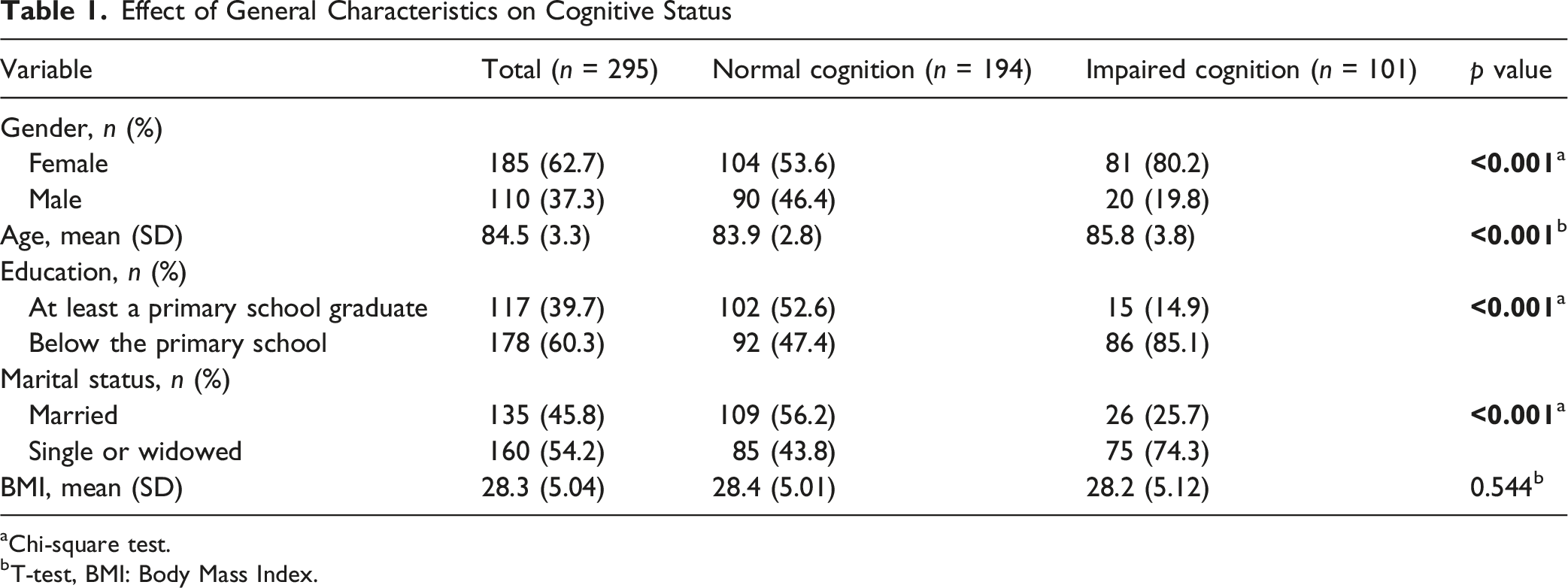
aChi-square test.
bT-test, BMI: Body Mass Index.
Findings Related to the Medical and Chronic Disease Characteristics of Individuals
Polypharmacy and Comorbidities on Cognitive Status
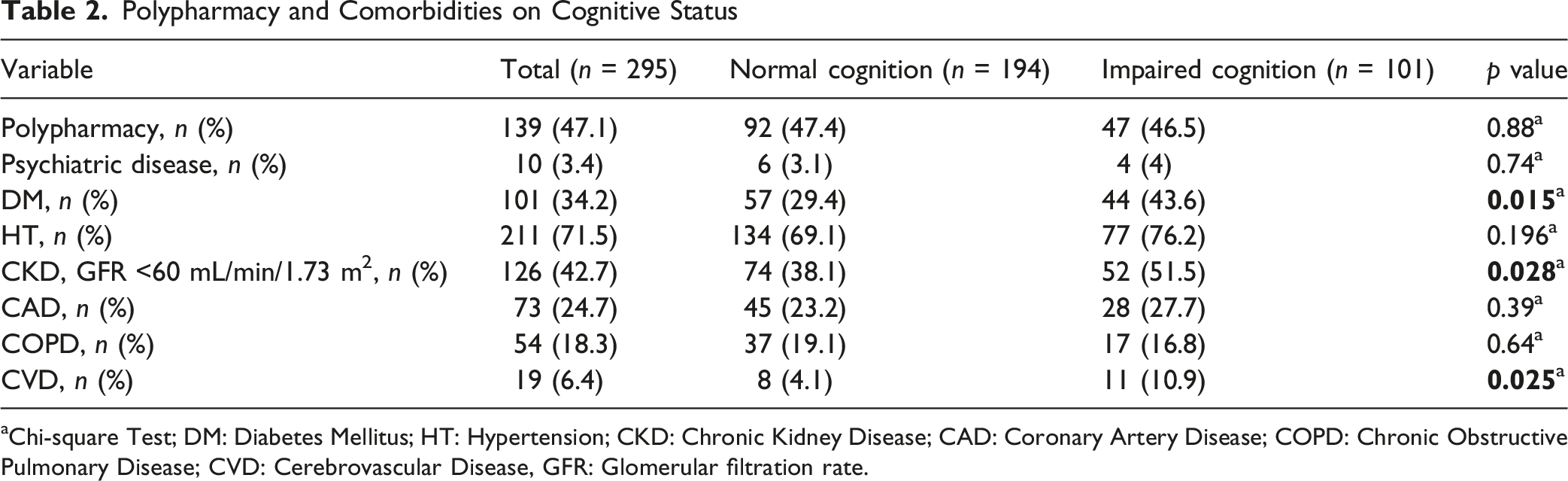
aChi-square Test; DM: Diabetes Mellitus; HT: Hypertension; CKD: Chronic Kidney Disease; CAD: Coronary Artery Disease; COPD: Chronic Obstructive Pulmonary Disease; CVD: Cerebrovascular Disease, GFR: Glomerular filtration rate.
Findings Related to Comprehensive Geriatric Assessments
The relationship between geriatric assessments and cognitive status
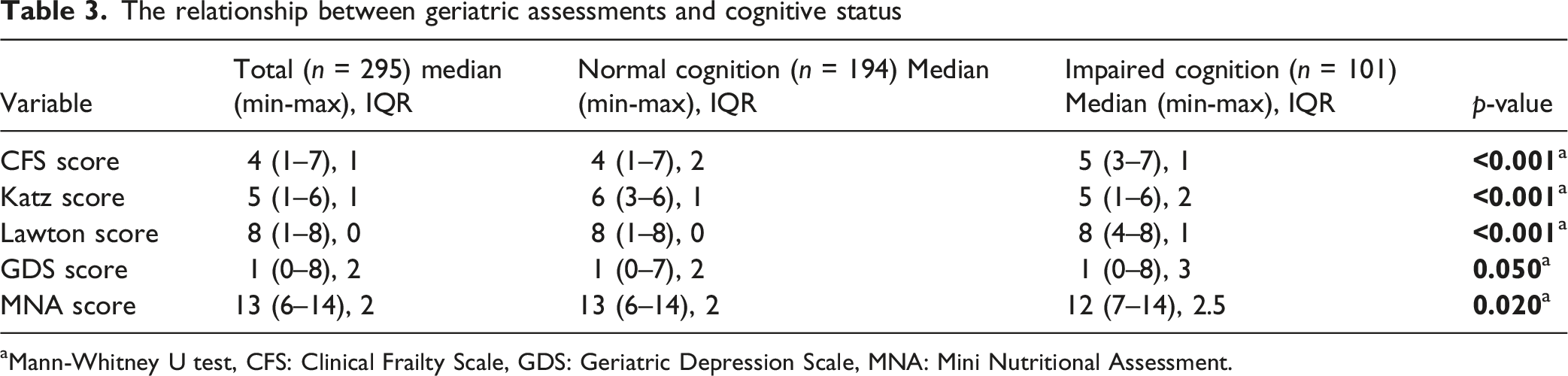
aMann-Whitney U test, CFS: Clinical Frailty Scale, GDS: Geriatric Depression Scale, MNA: Mini Nutritional Assessment.
Blood Parameters on Cognitive Status
Blood Parameters according to Cognitive Status
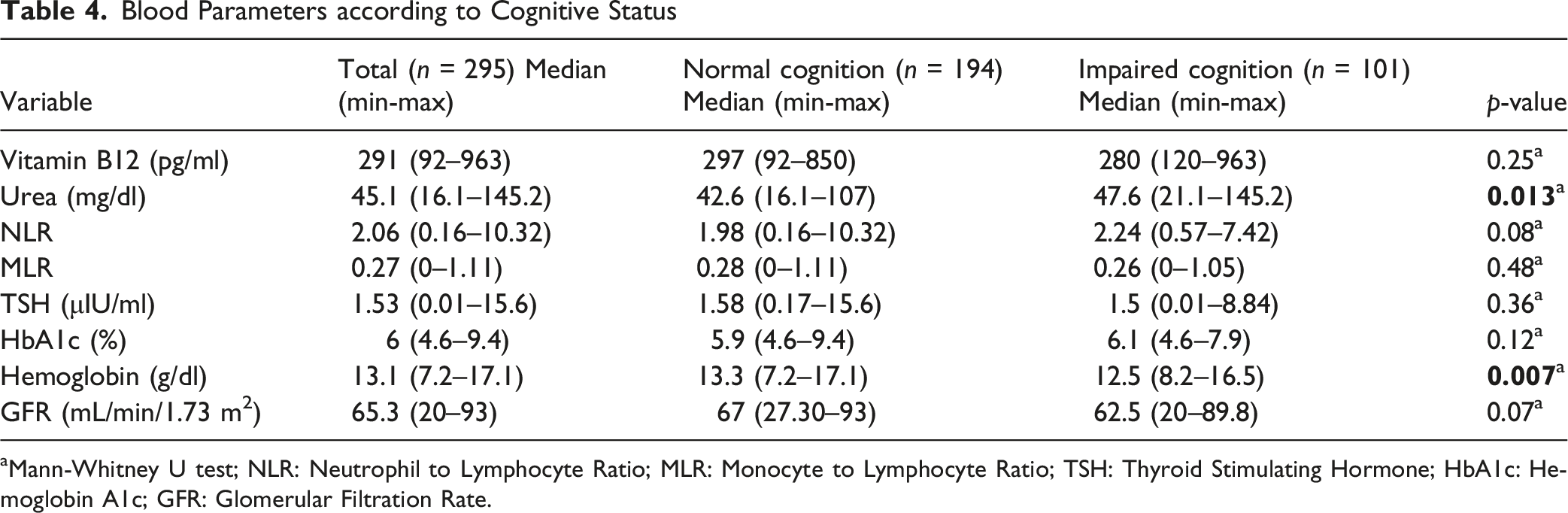
aMann-Whitney U test; NLR: Neutrophil to Lymphocyte Ratio; MLR: Monocyte to Lymphocyte Ratio; TSH: Thyroid Stimulating Hormone; HbA1c: Hemoglobin A1c; GFR: Glomerular Filtration Rate.
Correlation Analysis Between Blood Parameters and Cognitive Status
Correlation Analysis Between Blood Parameters and MMSE score

rho: Spearman’s rank correlation coefficient; NLR: Neutrophil to lymphocyte ratio; MLR: Monocyte to lymphocyte ratio; TSH: Thyroid stimulating hormone; HbA1c: Hemoglobin A1c; GFR: Glomerular filtration rate
Findings From Multivariable Logistic Regression Analysis
Multivariable Regression Analysis of Factors Associated with Cognitive Impairment
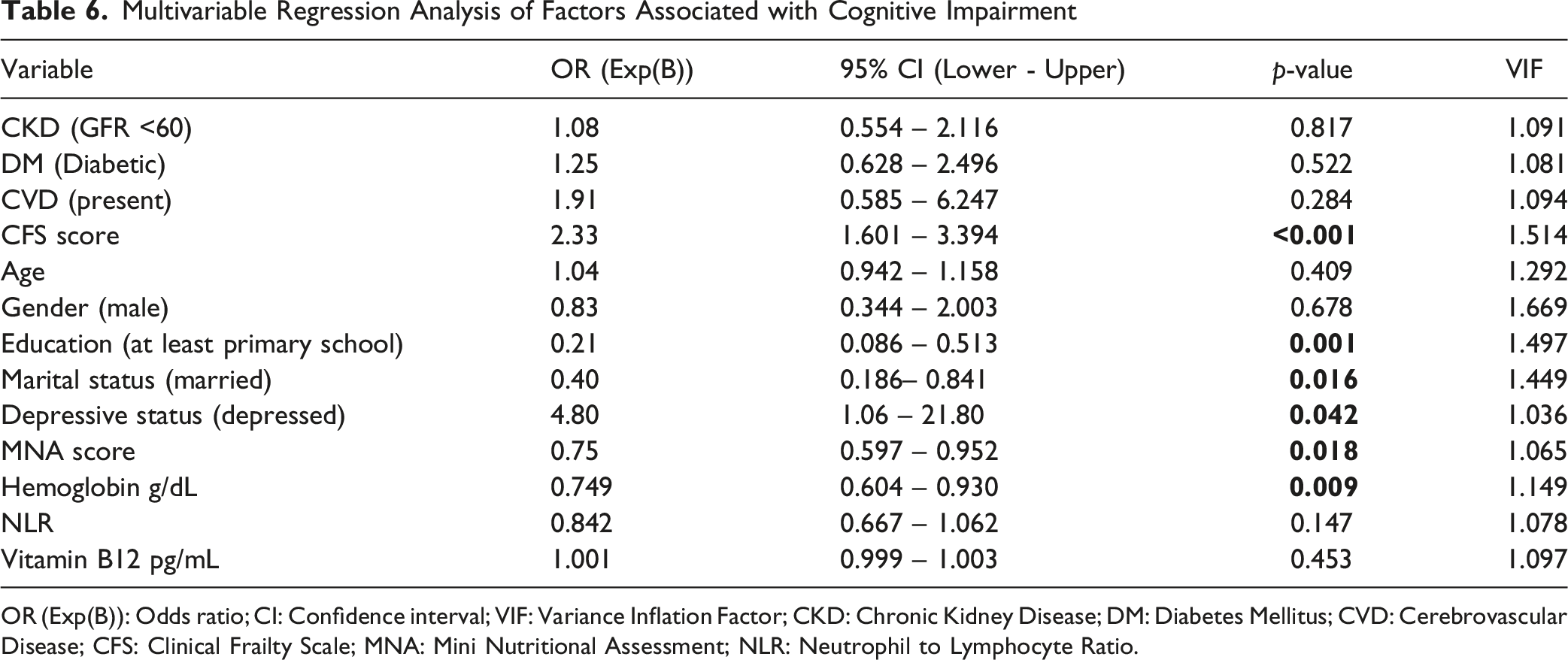
OR (Exp(B)): Odds ratio; CI: Confidence interval; VIF: Variance Inflation Factor; CKD: Chronic Kidney Disease; DM: Diabetes Mellitus; CVD: Cerebrovascular Disease; CFS: Clinical Frailty Scale; MNA: Mini Nutritional Assessment; NLR: Neutrophil to Lymphocyte Ratio.
Discussion
This study, the first community-based investigation in Türkiye focusing exclusively on adults aged ≥80 years, demonstrates that cognitive status in the oldest-old is associated with a complex interplay of social, functional, psychological, nutritional, and biological factors. We found that higher frailty and depression scores were strongly associated with cognitive impairment, whereas at least primary school education, being married, better nutritional status, and higher hemoglobin levels were inversely associated with cognitive impairment.
The prevalence of cognitive impairment increased with age in our sample, consistent with previous studies that have shown cognitive impairment accelerates after age 80 due to cumulative neurobiological changes, such as synaptic loss, reductions in brain volume, and vascular pathology (Ophey et al., 2023). Women had a significantly higher prevalence of cognitive impairment, which may partly be explained by their longer life expectancy (GBD 2019 Dementia Forecasting Collaborators, 2022), greater representation in the oldest-old age group, and the potential impact of postmenopausal hormonal changes on neuroprotection (O’Neal, 2024). Additionally, lower educational attainment among women is a factor strongly associated with reduced cognitive reserve (Giacomucci et al., 2022). May contribute to this disparity. In line with this, our findings showed that higher educational attainment was associated with better cognitive status, supporting the cognitive reserve hypothesis and highlighting the role of lifelong learning and mental stimulation in mitigating neurodegenerative processes (Clouston et al., 2020).
Marital status also emerged as an important socio-educational determinant. Being married was associated with better cognitive status, in agreement with the literature, which shows that social support and sustained interpersonal engagement are associated with better cognitive status (Cardona & Andrés, 2023). These results suggest that individuals living alone or lacking adequate social support may constitute a high-risk group that warrants closer monitoring and targeted preventive interventions.
Frailty showed one of the strongest associations with cognitive impairment in our cohort. Frailty is increasingly recognized as a multidimensional construct encompassing physical, social, and cognitive domains (Guo et al., 2022). Physical frailty in particular is consistently linked to increased dementia risk through shared pathways such as chronic inflammation, sarcopenia, and reduced physiological reserve (Kojima et al., 2016; Ma & Chan, 2020). Our findings reinforce the need for integrated geriatric care models that simultaneously address frailty and cognitive health to slow functional decline in the oldest-old.
Depressive symptoms were more prevalent among participants with cognitive impairment, consistent with evidence linking depression to cognitive impairment as a potential risk factor, prodromal symptom, or consequence (Jang et al., 2025; Wong et al., 2024). The nearly fivefold higher odds observed in our study supports the relevance of depression screening in primary care for the oldest-old; however, the wide confidence interval indicates limited precision and warrants cautious interpretation. Moreover, frailty, depressive symptoms, and functional limitations are conceptually interrelated and may reflect a broader vulnerability phenotype rather than entirely independent predictors of cognitive impairment.
Lower MNA scores were independently associated with cognitive impairment, consistent with evidence linking poorer nutritional status to worse cognitive outcomes (Feng et al., 2022). Higher hemoglobin levels were inversely associated with cognitive impairment, consistent with studies linking anemia-related reductions in cerebral oxygen delivery to poorer cognitive outcomes (Xiong et al., 2025). Although higher urea levels and lower vitamin B12 concentrations were associated with poorer cognitive performance in univariable analyses, these associations did not remain significant after multivariable adjustment. This attenuation may reflect the multifactorial and interrelated nature of clinical, nutritional, and biological factors in the oldest-old rather than independent effects of individual biomarkers. Therefore, these modest biomarker findings should be considered exploratory.
Our findings extend previous YASAM studies, which mainly focused on healthcare utilization, geriatric vulnerability, and short-term outcomes, by examining cognitive impairment and its multidimensional correlates in community-dwelling adults aged 80 years and older (Katipoglu et al., 2025; Katipoglu & Kocyigit, 2025)
This study has several strengths. First, it focuses exclusively on community-dwelling adults aged 80 years and older, a population often underrepresented in research, providing valuable, context-specific data from a low-to middle-income country setting. Second, the use of a comprehensive geriatric assessment allowed for the simultaneous evaluation of multiple domains, including physical function, frailty, nutrition, depression, comorbidities, and laboratory parameters, enabling a multidimensional analysis of factors associated with cognitive impairment. Third, standardized and validated assessment tools were applied by a trained multidisciplinary team, enhancing the reliability and comparability of the results.
However, several limitations should be acknowledged. Although YASAM is designed as a longitudinal initiative, the present analysis used a cross-sectional design based on baseline assessments because follow-up data were not yet sufficiently mature for robust longitudinal modeling. Therefore, causal inferences and temporal relationships between cognitive impairment and the associated factors could not be established.
Cognitive impairment was defined using a uniform MMSE cut-off value of ≤24. Although a low-education–adapted MMSE was used for participants with ≤5 years of formal education and education level was adjusted for in the multivariable model, some degree of misclassification may remain, particularly among participants with lower educational attainment.
Selection bias should also be considered. Although YASAM is population-based and targets community-dwelling adults aged 80 years and older, participation required acceptance of structured home visits, and institutionalized individuals were not included. Individuals with severe disability, advanced cognitive impairment, or limited social support may also have been less likely to participate, potentially leading to underrepresentation of more vulnerable older adults. In addition, participants with incomplete data were excluded using a complete-case approach; if missingness was not random, this may have further contributed to selection bias. These factors may have produced a relatively healthier or more functionally capable analytic sample, potentially underestimating cognitive impairment prevalence and influencing associations involving social and functional variables.
Although the multivariable model adjusted for several clinically relevant confounders, unmeasured factors such as lifetime occupational complexity, genetic background, or detailed dietary intake may have influenced the observed associations
Conclusion
This community-based study in Türkiye, focusing on adults aged 80 years and older, shows that cognitive status in the oldest-old is associated with interconnected social, functional, psychological, nutritional, and biological factors. Frailty, depression, poorer nutritional status, and lower hemoglobin levels were associated with cognitive impairment, whereas higher educational attainment and being married were associated with better cognitive status. These findings support the value of integrated geriatric care strategies that address medical, nutritional, and psychosocial domains together. Incorporating routine screening for these associated factors into primary care and healthy aging programs such as YASAM may facilitate early identification of vulnerable individuals and guide targeted geriatric assessment in this rapidly expanding population.
Footnotes
Ethical Considerations
Before the study began, ethical approval was obtained from the KTO Karatay University Faculty of Medicine Non-Drug and Non-Medical Device Research Ethics Committee on November 28, 2024, with decision number 2024/041.
Author Contributions
M. Y. (Conceptualization; Methodology; Data Curation; Formal Analysis; Writing—Original Draft Preparation; Supervision); I. S. (Formal Analysis; Validation; Writing—Review and Editing; Supervision); B. K. (Conceptualization; Methodology; Data Curation). All authors supported the editing of this paper and have approved the final manuscript for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.