
Abstract
Background
Sleep problems are common in later life and linked to increased morbidity and mortality. African American and low-income older adults disproportionately experience sleep problems.
Objective
Our aim was to identify factors perceived to affect sleep and garner feedback on potential components of a behavioral sleep intervention.
Methods
We conducted 21 semi-structured interviews with adults in an underserved urban community aged 50 to 74 (77% African American) reporting persistently poor sleep. We used a rapid qualitative analysis approach to develop themes.
Results
Results revealed multilevel sleep barriers related to both life stage and setting: for example, stress, chronic pain, vigilance due to security concerns and caregiving, and noise. All participants wanted to improve sleep without medications. Intervention components of most interest were contact with a community health worker, a watch to track sleep, and educational resources. The barriers identified here should be addressed in interventions to improve sleep in this population.
• This study uses qualitative interviews to explore how age/life stage and residence in an underserved community intersect to shape the perceived causes and consequences of poor sleep among older adults. • Findings confirm that factors affecting sleep quality are situated at multiple levels, aligning with socioecological models of sleep health that help to explain sleep inequities.
• Given identified barriers to sleep at household and neighborhood levels, problem-solving and providing resources may be a helpful part of a behavioral intervention for older adults in an under-resourced setting. • Most study participants were interested in contact with community health workers as part of a sleep intervention. This role could include teaching cognitive-behavioral sleep skills in a culturally congruent way and connecting participants to resources that would reduce stress and/or improve their sleep environment.What This Paper Adds
Applications of Study Findings
Introduction
More than 40% of older adults live with insomnia (Beydoun et al., 2021), a burdensome disorder which leads to adverse health effects over the short-term (e.g., increased fall risk (Chen et al., 2017)) and the longer term (e.g., a higher risk of cardiovascular disease (Javaheri & Redline, 2017)), and dementia (de Almondes et al., 2016). Reasons for the increased burden of insomnia and other sleep disturbances or disorders in later life include a higher prevalence of chronic diseases that interfere with sleep (Vaz Fragoso & Gill, 2007) as well as mood disturbances triggered by events common at this life stage such as bereavement (Simpson et al., 2014) and residential changes (MacLeod et al., 2018). Age-related changes in sleep-wake physiology may predispose older adults to being more vulnerable to these and other risk factors for poor sleep (Vaz Fragoso & Gill, 2007).
Insomnia and other sleep disorders are more common and more severe in African American, Hispanic, and low-income older adults (Caraballo et al., 2022; Jackson et al., 2020; Sheehan et al., 2019). For example, 18% of African American vs. 7.3% of White older adults in a national study reported ≤6 hours of sleep per night (Petrov et al., 2020), a difference that may contribute to racial disparities in cardiometabolic disease (Jean-Louis et al., 2022). Minoritized and economically disadvantaged older adults are disproportionately exposed to risk factors for insomnia and other sleep disorders. Socioecological models of sleep health (Billings et al., 2020; Johnson et al., 2018) place these factors at multiple, interacting levels: individual (e.g., chronic health conditions), family/household (e.g., poor temperature control and family stress), neighborhood (noise and crime), and societal (e.g., policies affecting healthcare access). Disproportionate exposure to chronic stress is a well-documented individual-level determinant of poor sleep, which contributes to allostatic load (Murkey et al., 2022); for example, via increased inflammation, HPA-axis dysregulation, and reduced synaptic plasticity (Farmer et al., 2022; Mokhlesi et al., 2012; Reffi et al., 2022). Examples of determinants at other levels include poor air quality in predominantly African American neighborhoods that have experienced residential segregation, which is associated with poor sleep quality and sleep apnea. Potential mechanisms include inflammation and a higher prevalence of diseases such as dementia that are linked to both air pollution and poor sleep (Billings et al., 2020; Cao et al., 2021). Another study showed neighborhood disorder was associated with poorer sleep efficiency (Kim et al., 2023).
To improve sleep health in disparity-affected populations, sleep researchers have called for interventions that address these multi-tiered factors (Johnson et al., 2018; Williams et al., 2015). While the literature includes sleep-related interventions that have been culturally tailored for African Americans (Nam et al., 2024; Robbins et al., 2019; Zhou et al., 2022), we were unable to identify interventions for insomnia disorder that explicitly account for factors beyond the individual level, for example, the home or neighborhood environment. As a first step in developing such an intervention, qualitative inquiry can deepen our understanding of how older adults in underserved communities experience poor sleep quality and how they perceive its causes and consequences.
Examples of similar investigations can be found in the literature. Baron and colleagues conducted focus groups among African American adults in an urban setting ages 25–75 years to explore sleep attitudes, beliefs, and practices (Baron et al., 2019). Participants were not selected for existing sleep problems, however, and the broad age range means that findings may not reflect the full range of later-life sleep issues. In another study, semi-structured interviews were conducted with retirement community residents who reported trouble sleeping (Berkley et al., 2020). Participants attributed their insomnia symptoms to chronic illnesses as well as stress from transitions such as bereavement and retirement. Study participants described employing a range of self-management strategies, including following sleep hygiene guidelines, which they generally felt to be ineffective. Participants were exclusively White non-Hispanic and from a single retirement community; it is therefore important to explore these issues among diverse groups of older adults in other settings.
The present study builds on this work to lay a foundation for developing a behavioral sleep intervention for older adults living in disadvantaged communities. We conducted qualitative interviews with adults age 50+ living in an economically disadvantaged, predominantly African American community, all of whom reported persistently poor sleep quality. Our objectives were to (1) identify perceived factors affecting sleep and (2) elicit preferences for a behavioral sleep intervention for older adults living in an underserved community.
Methods
The University of Michigan’s Institutional Review Board reviewed the protocol and deemed this study exempt from further review (HUM00261430).
Sampling and Recruitment
All participants had previously participated in one of two behavioral clinical trials (A Trial of a Positive Psychology Intervention for Older Adults [RESET] During the COVID-19 Pandemic [R01NR020442] or STEPS: An Efficacy Trial of a Chronic Pain Self-Management Program for Older Adults [R01AG071511]). Inclusion criteria for the present study were reporting “very poor” or “poor” sleep quality in the last 7 days at both baseline and 2-month assessments on an item from the PROMIS-29 Health Profile (Buysse et al., 2010; Yu et al., 2012). Of the 60 individuals meeting these criteria, study staff selected 22 individuals representing a range of ages and a balance of men and women. Potential interviewees were sent a letter inviting them to participate in a telephone interview. A study team member subsequently phoned to explain the interview process and to set up a time to be interviewed. Of the 22 individuals, 21 agreed to be interviewed (one could not be reached). Interview participants were given a $25 incentive.
Data Collection
Interviews were conducted by two trained interviewers (JH and LN) between December 9, 2024, and February 12, 2025. A semi-structured interview guide was created, guided by the socioecological model of sleep health. Questions were also formulated to yield information that could inform the development of a behavioral intervention for sleep health that would be responsive to the needs of older adults in underserved communities. Interview questions were related to the participant’s sleep history, factors that hinder their sleep, strategies they have attempted to improve sleep, and feedback on potential components for a behavioral intervention to promote better sleep (Appendix A). We asked about potential components that could support learning cognitive-behavioral skills to improve sleep and address environmental barriers to sleep. Interviews were audio-recorded, de-identified, transcribed, and checked for accuracy. We obtained verbal consent for participation and for audio recording. Interviews lasted an average of 44:43 minutes (range: 22:01 to 71:47 minutes). Data collection continued until thematic saturation was reached.
Data Analysis
We utilized a rapid qualitative analysis approach (Lewinski et al., 2021), which entails organizing and interpreting qualitative data through a process of reviewing raw data, organizing into distinct domains, and summarizing across participants. One member of the study team began by reading a sample of interview transcripts to become familiar with the data and to note initial ideas. Next, we constructed a template table (Appendix B) with 8 distinct domains, definitions for each domain (including inclusion and exclusion criteria), data summary points/themes for each domain, and supporting quotations. One team member conducted a primary review of each transcript and the second team member completed a secondary review to ensure consistent and accurate data capture. Any differences in characterizing the data on the templates were discussed until consensus was attained, after which all previously completed templates were revised accordingly. Once all templates were complete, data from each domain was aggregated across interviews and reviewed for main findings.
Results
Participant Demographic and Health Characteristics (N = 21)
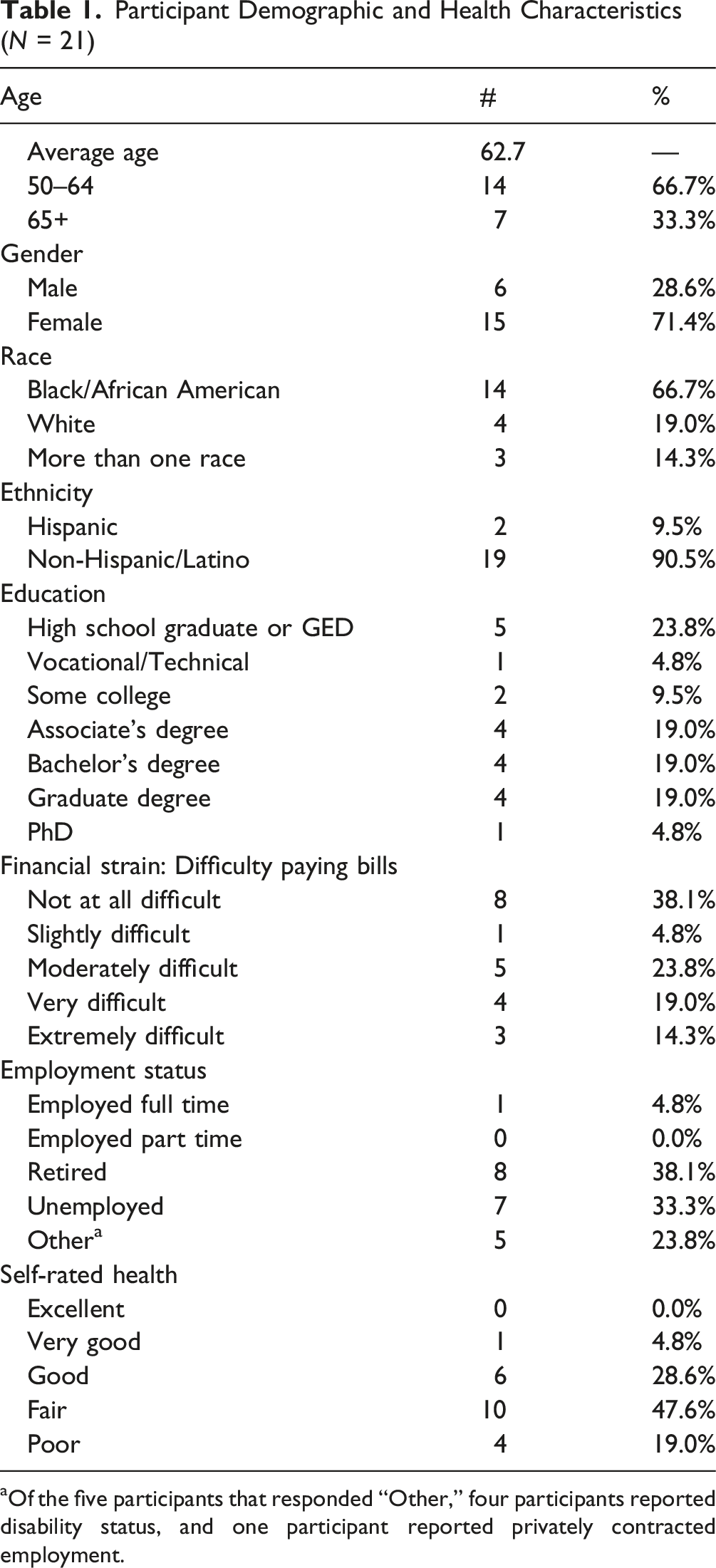
aOf the five participants that responded “Other,” four participants reported disability status, and one participant reported privately contracted employment.
Sleep Study Domains and Themes (N = 21 Interviews)
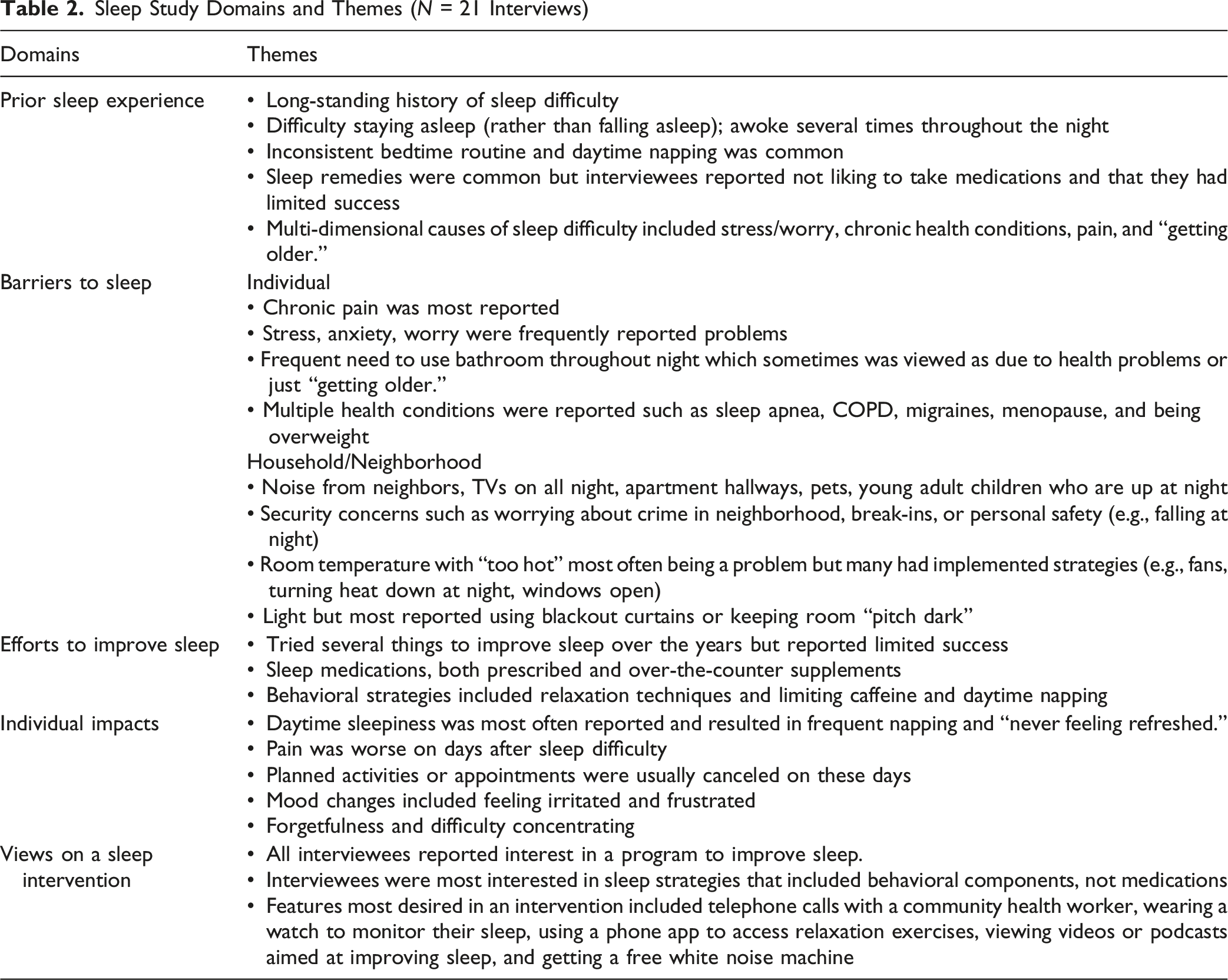
Domain 1: Prior Sleep Experience
Participants talked about having a long history of sleep difficulty that had gradually worsened over time. Most individuals reported having more difficulty staying asleep rather than falling asleep. They described being able to fall asleep quickly but waking throughout the night. I usually go to sleep … maybe 12:00 midnight [or] 1:00. And even then, I’ll sleep for an hour or two and I’ll wake up for maybe another hour, then I’ll fall back asleep. So it’s kind of like off and on, off and on. I very rarely sleep more than four hours at one time. (Female, 67)
Most interviewees did not have a regular bedtime nor a consistent bedtime routine. Some talked about having a habit of falling asleep in chairs, on couches, or while watching television. Some reported needing background “white noise” from the TV to help them sleep. Some participants also reported napping during the day, lasting from 20 minutes to several hours. My sleep routine is so out of whack. I used to be in bed at 11 o’clock. I done showered or washed up, in my pajamas and in the bed. My sleeping habits have been, for the past several years, and I will probably say four plus years, maybe more, my sleep is just all over the place … I generally pass out, put it that way. I don’t get prepared for bed, I don’t get to shower or any of that. I just generally pass out whether that is if I sit down somewhere, whether it’s a couch, a chair, chaise lounge, I’m out. (Female, 60)
When participants were asked if they had discussed their sleep problems with a doctor, responses varied. Many who had consulted a doctor reported limited or no success with prior treatments such as sleep medications or a Continuous Positive Airway Pressure (CPAP) machine. Others reported that more pressing health concerns were a higher priority.
Domain 2: Barriers to Sleep
Participants reported varied factors impeding their sleep, including individual-level and neighborhood/household factors.
Individual Factors
Chronic pain was a frequently cited cause for sleep disturbances. The pain was often described as longstanding and, in some cases, debilitating. However, for others the pain was not severe but nonetheless made it difficult for them to get comfortable at night. If I lay a certain way, the pain in my arm will keep me from going to sleep, so I have to position myself just right. And then once I fall asleep, if I move, or move into a certain position, or lay a certain way, that pain will wake me up. (Female, 67)
Stress, anxiety, and worry were also frequently discussed. Some participants reported having mental health conditions such as depression, anxiety, and post-traumatic stress disorder. Others said their stress was from worrying about financial concerns, health problems, caregiving, or family strife. They reported having a “racing mind” or “stewing about their problems.” Right now I don’t have an income, so that’s another reason why I’d probably be up too. I’ve applied for disability, and I just got some bad news that they denied my claim again, and that just sent me into a dark place and upped my anxiety … I got grandchildren. I can’t provide [for] them … My children, I got three children. I have a son that’s in prison, been in prison seven years. My two daughters rarely communicate. I got one, she don't even know that I’ve been going through an issue because she’s … mental illness runs in my family. (Female, 51)
Frequent need to use the bathroom during the night was reported by many. In some cases, this was due to a medical condition but, in other cases, participants attributed it to “getting older.” I’m 60 and there’s a lot of problems with sleep as we get older. I’m up, sometimes I go to the bathroom three or four times too, like problems with urination. A lot of people my age have that, too. (Male, 59)
Chronic health conditions other than pain were also reported as factors hindering sleep. These included sleep-related conditions (e.g., sleep apnea and restless leg syndrome) as well as chronic obstructive pulmonary disease (COPD), migraines, menopause symptoms (including nighttime hot flashes), and being overweight or obese. Well, I’m on that CPAP machine. I’ve got sleep apnea … I’ve got severe COPD. I have arthritis, pretty sore moving around in bed, trying to get comfortable. That’s it, the breathing and the arthritis, the pain. I’m on medications for it, but it doesn’t help a lot. (Male, 64)
Household/Neighborhood Factors
Participants frequently reported that noise from within their home and from their neighborhood or apartment buildings kept them awake. My son, he’s 18 so he is up all night. And he will cook and I smell the food. I know, I get so mad at him. (Female, 54) I live next to the elevator so in the middle of the night you can hear the elevator going up and down. You hear everything everybody is saying on the elevator. (Female, 57)
Security concerns related to crime in their neighborhood or recent break-ins were an added concern. Last week at four in the morning I had to call the police. (Female, 61) I live in back of the building back here where the parking lot is and then the hospital just built a new garage next door to us. You got people back here breaking in cars. They stealing the catalytic converter from under the car. They stealing the gas out the car. They stealing steering wheels out the car. You got a couple people that around here just hanging around. (Female, 57)
Other household factors included a fear of tripping and falling at night and sleeping in a room that was too hot. A few people mentioned that they were the sole caregiver for an aging parent or another family member who lived with them. These responsibilities often caused frequent sleep interruptions. I’m his sole caregiver. No one else helps with his care. So, I’m his caregiver, 24/7 … I monitor him because if I’m up at 3:00 in the morning or 2:00 in the morning and his blood sugar goes down, then I’ll give him a half peanut butter and jelly sandwich or something like that to keep it up. So, that happens a lot. I might have to do that two times during the middle of the night. (Female, 67)
Domain 3: Efforts to Improve Sleep
Participants talked about ways that they had tried to improve their sleep, including taking sleep medication or supplements and employing various behavioral strategies. However, they reported limited success and many were at a loss for what else to do. Some said they just “push through.” You name it, I’ve tried them all. (Female, 73)
Most participants reported having tried both over-the-counter and prescription sleep medicine. Participants reported that they didn’t like taking sleep medication because they disliked the way it made them feel and/or they didn’t want to develop dependence. Some described taking “cold medicine” or “pain pills” hoping that would help with sleep but had limited success. About a third of the sample said they had tried cannabis products to help with sleep but all except one said they didn’t like it, or, as one participant commented, “I wasn’t raised that way.” Others reported that the medications they had tried did not help. Melatonin is like a Tic Tac for my body. Five milligrams don’t work, 10 milligrams don’t work. And like I said, when I was just taking melatonin, it still would take me three or four hours to go to sleep. My body was like, “What is that, candy?” (Female, 51) … my doctor has prescribed a sleeping pill, but I don’t like the way it makes me feel the next day. (Female, 72)
Some discussed efforts to change their habits and behaviors to improve sleep. These included relaxing before bed by taking a warm shower or bath, practicing meditation, or using heating pads or blankets. Others talked about drinking “sleepy” tea. Some restricted their fluid intake at night and limited caffeine and alcohol intake, as they believed these interfered with their sleep. Some also tried to avoid or limit napping during the day. Most participants reported that watching TV in bed helped with sleep onset. However, some said they felt or had heard that it interfered with sleep and tried to keep the TV off at night.
Domain 4: Individual Impacts
Participants reported negative impacts of chronic sleep difficulty. They talked about constantly feeling tired. This daytime sleepiness often resulted in taking naps throughout the day, or in some cases, just falling asleep while reading, watching TV, or working on their computer. Participants said that daytime naps, which could last 2-3 hours, made it more difficult to sleep well at night. I never feel refreshed. I always feel groggy, tired, frustrated. Yeah, I feel sleep-deprived… I can’t even remember the last time that I actually had a good night’s sleep and woke up in the morning well-rested. (Male, 58) I’ve learned to adjust my life to [little sleep], but I stay a little exhausted. I really do. I try not to let it bother me as much, but I’m getting older and it’s slowing me down a little… (Female, 61)
Several individuals talked about canceling appointments or planned activities on the days following sleep difficulty. Sometimes I miss my appointments. I just don’t feel good. (Male, 64)
They reported feeling “knocked out” and not wanting to get out of bed or get dressed for the day. Many said that their chronic pain was worse on the days following sleep difficulty. One participant said she missed being able to participate in morning activities, like going to church or meeting friends at the senior center. Others noticed mood changes, including feeling irritated and frustrated. A few experienced forgetfulness, difficulty concentrating, or “brain fog” due to sleep difficulties. It definitely affects my mood. I literally just stay in the house and just try to stay in bed, barely to get up to eat … And I try not to make major decisions when I'm that tired. (Female, 57) Unfortunately, if it’s one of the days where my son brings the kids over, I have to keep checking myself because they’re just being three and four-year-olds. But I’m like, “I don’t want to…” And I’ll have to tell him, “No, don’t bring them today because I’m not in a good mood today.” (Female, 67)
Domain 5: Views on a Sleep Intervention
When asked about a potential educational/behavioral program aimed at improving sleep, all participants expressed interest. I want to have better sleep. I’ve tried other things that are not working, so I would try a program and see how that works. (Female, 72)
A common theme among interviewees was that they were looking for ways to improve their sleep without taking medications. I don’t want to medicate. I’m a person who don’t take meds for much of anything. (Female, 74)
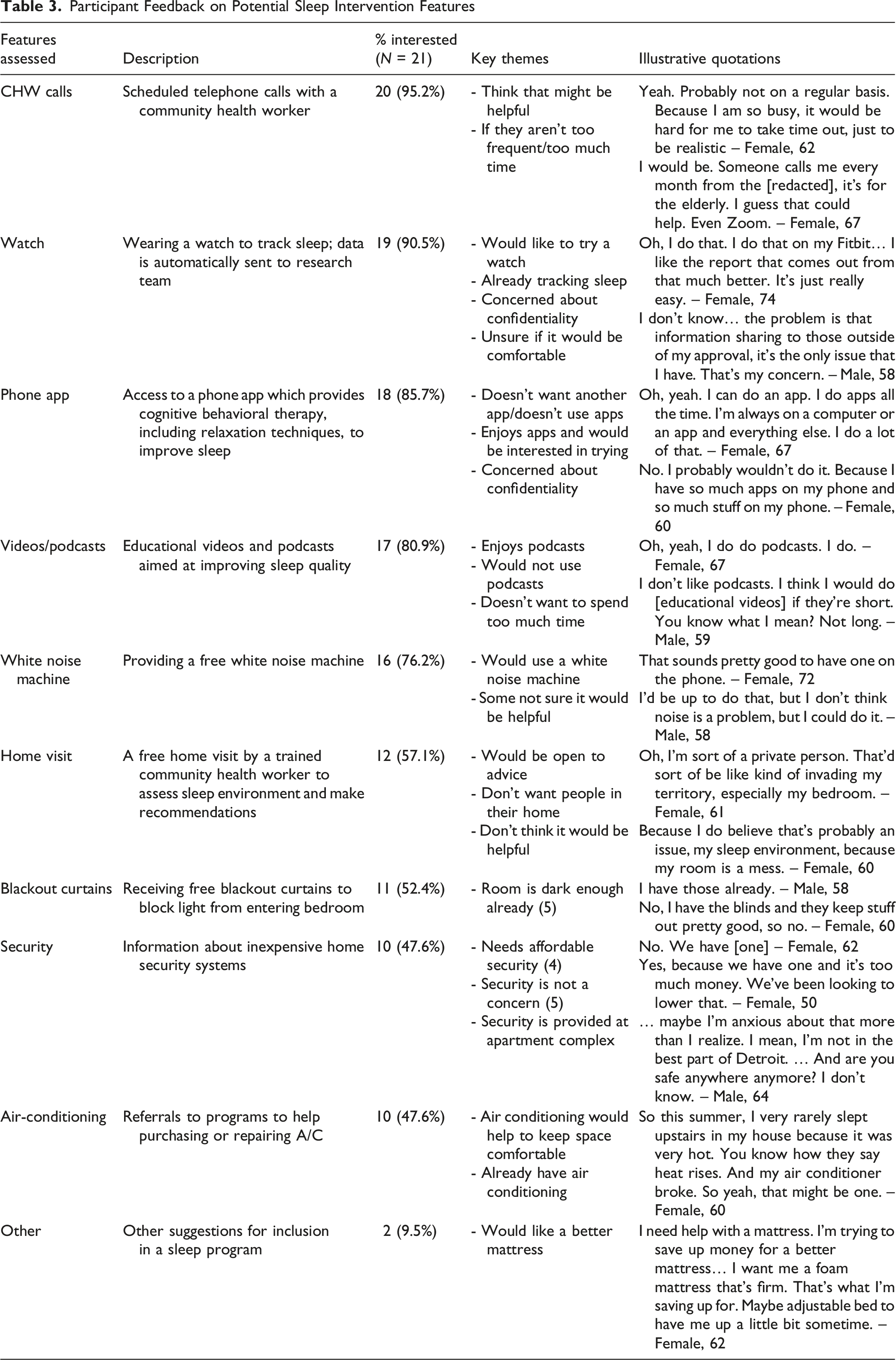
Participant Feedback on Potential Sleep Intervention Features
Discussion
This qualitative study consisted of 21 in-depth interviews with predominantly African American midlife and older adults with poor sleep quality. The study’s setting is Detroit, Michigan, an overburdened urban community whose residents contend with racialized residential segregation, economic disinvestment, air pollution, and chronic psychological stressors. Participants reported a longstanding history of sleep difficulty, which they said worsened with age and health problems. Participants attributed their sleep problems to a variety of factors. These include individual-level factors such as chronic pain, stress and anxiety, and medical conditions; family/household-level factors, including household noise and in-home caregiving responsibilities; and neighborhood/community factors, including concerns about crime, and noise from outside of the household. Every participant could cite examples of the detrimental impact of poor sleep on their functioning and well-being, including constant fatigue and never feeling refreshed, reductions in activity, mood disturbances, and forgetfulness. Adverse effects of insufficient sleep on social relationships were also described, demonstrating that the effects of poor sleep ripple outward to family and friends.
Themes developed from the data echo those in other qualitative studies of older adults regarding consequences of inadequate sleep on well-being and functioning (worsened mood and cognition; Berkley et al., 2020) and factors disrupting sleep, including the prominent role of medical problems, especially chronic pain (Berkley et al., 2020; Robbins et al., 2021). Our findings highlight how life stage and socio-environmental context shape the perceived causes and ramifications of chronic poor sleep. For example, external noise issues were a particular issue for those living in multi-unit senior residences – a common living arrangement in this community. While most participants were no longer employed, they described how their poor sleep caused them to miss non-work activities critical to health and well-being, including attending medical appointments, caregiving for grandchildren, and engaging in social activities. The life-stage-dependent nature of factors affecting sleep becomes clear when our findings are compared to those in a qualitative study about sleep hygiene behaviors conducted with a broader age range of adults in low-income housing reporting short sleep (Rottapel et al., 2020). Major themes in this younger sample included work stress, balancing work and home responsibilities, childcare, and pregnancy issues. Some of the themes associated with living in an economically marginalized community were similar in both studies, such as safety-related fears disrupting sleep.
Implications for Interventions
Participants felt like they had “tried it all” in pursuit of better sleep; however, there was no mention of first-line behavioral treatments even when probed about prior use of formal behavioral therapies for insomnia. Medications appear to be the only sleep treatment that participants ever received from the healthcare system. Participants also attempted strategies that seem intuitive but may actually be counterproductive (e.g., naps and baths close to bedtime). Together, this suggests that both the participants and their care providers had limited knowledge of effective insomnia treatments. This finding is unsurprising, given that cognitive behavioral therapy for insomnia (CBTi), in spite of being considered first-line treatment for insomnia disorder, is seldom recommended to patients by providers (Hughes, 2024). Underserved communities and racial and ethnic minority populations are even less likely to have access to this type of treatment (Jackson et al., 2020). Importantly, participants consistently expressed a strong preference for improving sleep through behavioral or other non-medication approaches, with much less interest in taking medications or supplements.
As awareness of sleep disparities has grown, there have been calls for sleep-related interventions that are tailored for minoritized and economically disadvantaged populations and that consider a life course framework in their design (Jackson et al., 2020). Our findings suggest several considerations for CBTi-based interventions to ensure their responsiveness to social-contextual factors, stage of life, and their intersection. Core components of CBTi include encouraging sleep hygiene behaviors, cognitive restructuring, stimulus control, sleep restriction, and relaxation/mindfulness. Tailoring these components may facilitate uptake and adoption of recommended behaviors. For example, standard CBTi does not provide support to help manage chronic pain, but our findings suggest that this could be a helpful enhancement for some. Stimulus control (training one’s body and mind to associate the bed with sleep) typically involves getting out of bed after a period of not sleeping. Fear of tripping and falling during the night, expressed by some of our participants, should be addressed, for example, by ensuring a safe path to an out-of-bed location. Recommended sleep hygiene behaviors, such as consistent wake/sleep times, limiting naps, and staying active during the day, were difficult for some in our sample, in part due to no longer working full time and having less defined schedules and daytime activities that are more optional. Encouragement and strategies for maintaining behavior change may be helpful for this demographic.
Our findings suggest that incorporating problem-solving and providing resources may be helpful intervention components for older adults in an under-resourced setting. Given the chronic life stressors faced by participants, a greater emphasis on learning and practicing relaxation techniques may also be indicated, combined with connections to resources to address stressors related to social determinants of health, including challenges with housing, food, and transportation. Noise issues experienced in senior housing communities or multigenerational households may not be completely remediable but could be mitigated through problem-solving. Financial constraints expressed by some participants suggest the need for assistance in identifying affordable means to improve the physical sleep environment and/or to address crime/security-related worries, for example, with inexpensive home security systems.
There is a small but growing body of sleep-related interventions tailored to the needs of specific groups. Wu and colleagues (2025) developed a culturally tailored “sleep extension” intervention for African Americans aged 21-75 that uses elements of CBTi over four virtual sessions. Jean-Louis and colleagues (2020) tested a web-based educational program for obstructive sleep apnea tailored to the needs of African American, Black, or Caribbean American adults. Zhou and colleagues (2022) tested culturally tailored and standard internet-delivered CBTi for Black women; both interventions were superior to sleep education, but the tailored version had a higher completion rate. Development of an intervention for sleep problems that is responsive to the needs of older adults in under-resourced communities could apply the present study findings to integrate and build upon these prior efforts.
Study Strengths and Limitations
There are several strengths of this study. Most participants were from populations that have been underrepresented in sleep research; namely, African American and low-income older adults. We identified our sample using responses to a single item (global assessment of sleep quality) instead of a formal screening tool or diagnosis for insomnia or other sleep disorders and ended up successfully engaging participants whose lives were markedly affected by the persistent inability to get adequate sleep and to feel well-rested. There are also limitations to consider. All individuals had previously participated in trials of behavioral interventions, suggesting above-average interest in behavioral approaches for sleep improvement. Similarly, approximately half had participated in a study for which chronic musculoskeletal pain was an inclusion criterion. This may have led to greater reporting of chronic pain interfering with sleep than would be found in the general population of adults in this age group reporting sleep difficulties. We did not have information on participants’ sleep-related diagnoses. Finally, this approach predominantly captures patient-centered experiences. These findings should be interpreted within the broader context of sleep and aging, including underlying physiological changes (e.g., alterations in synaptic plasticity), particularly in relation to chronic stress exposure. Notably, the first-line treatment for insomnia disorder involves therapeutic strategies that directly influence sleep-related physiological processes.
Conclusion
Older adults living in a primarily African American, low-income urban community describe multifactorial causes and consequences of poor sleep. Our findings underscore the importance of addressing both individual and environmental contributors to sleep quality in behavioral interventions that are designed to address well-documented disparities in sleep health. Ultimately, due to the long-term impacts of sleep on health and mortality, identifying effective ways to improve sleep in disparity populations may help to mitigate health disparities overall.
Supplemental Material
Supplemental Material - A Qualitative Exploration of Factors Affecting Sleep Experiences Among Older Adults in a Resource-Challenged Urban Community Journal of Applied Gerontology
Supplemental Material for A Qualitative Exploration of Factors Affecting Sleep Experiences Among Older Adults in a Resource-Challenged Urban Community Journal of Applied Gerontology by Mary R. Janevic, Martha Quinn, Philip Cheng, Daniel Whibley, Jennifer Hopson, Linda Nkemere, Rebecca Lindsay, Kimberlydawn Wisdom in Journal of Applied Gerontology.
Supplemental Material
Supplemental Material - A Qualitative Exploration of Factors Affecting Sleep Experiences Among Older Adults in a Resource-Challenged Urban Community Journal of Applied Gerontology
Supplemental Material for A Qualitative Exploration of Factors Affecting Sleep Experiences Among Older Adults in a Resource-Challenged Urban Community Journal of Applied Gerontology by Mary R. Janevic, Martha Quinn, Philip Cheng, Daniel Whibley, Jennifer Hopson, Linda Nkemere, Rebecca Lindsay, Kimberlydawn Wisdom in Journal of Applied Gerontology.
Footnotes
Acknowledgments
We would like to thank our participants, who were willing to share their sleep experiences with us.
Ethical Considerations
The University of Michigan’s Institutional Review Board deemed this study exempt from further review (HUM00261430).
Consent to Participate
Verbal informed consent was obtained from all participants for participation and for audio recording.
Consent for Publication
Verbal informed consent was obtained from all participants for publication.
Author Contributions
Conception and design: MJ, MQ, PC, RL, and DW; drafting: MJ and MQ; data acquisition: MQ, LN, and JH; data analysis: MQ and JH; data interpretation: MQ, MJ, PC, and DW; critical review of the work: all. All authors have also given final approval of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study engaged participants from the RESET (R01NR020442) and STEPS (R01AG071511) trials, both funded by the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the potential for participant identification due to details shared during the interviews, we are not planning on making interview transcripts publicly available. Please contact the corresponding author to inquire about obtaining redacted versions of the transcripts.
Clinical Trial Registration
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.