
Abstract
While government-assisted housing programs primarily aim to reduce financial burden for low-income older adults, depression and anxiety rates remain elevated among residents, suggesting that housing environments shape mental health through pathways beyond economic relief. This study examined how housing environments influence mental health among older adults through a socioecological framework. We conducted semi-structured interviews with 16 older adults (ages 60–86) residing in government-assisted housing in rural Alabama between July and September 2024. Using hybrid thematic and framework analysis, we organized emergent themes across individual, interpersonal, community, and organizational levels following Bronfenbrenner’s framework. Eleven themes emerged revealing complex paradoxes: housing as simultaneously sanctuary and constraint, anxiety as active controller of daily life, social isolation providing protection while creating loneliness, and transportation barriers operating as gatekeepers across life domains. Mental health service gaps persisted despite explicit resident requests. Ten themes spanned multiple ecological levels, validating multi-level intervention approaches.
Keywords
• This study reveals housing’s paradoxical nature for older adults: simultaneously providing essential sanctuary while constraining daily life through restrictive policies and limited resources. Resident gratitude reflects relief from worse alternatives rather than positive quality of life gains, and may partly reflect constrained voice among those dependent on housing authorities for shelter. Standard satisfaction measures miss both dimensions of this relationship. • Ten of eleven themes span multiple ecological levels, validating that housing-mental health relationships require multi-level rather than single-level interventions. • Transportation uniquely operates across all four socioecological levels as gatekeeper to healthcare, social connection, spiritual participation, and independence, representing the highest-leverage intervention point.
• Housing authorities should establish transportation services as a core service with medical, grocery, and church routes addressing cascading impacts across life domains that residents identified as their most urgent need. • Mental health providers should develop on-site counseling partnerships integrating professional services while respecting spiritual coping practices. Residents want both professional counseling and faith-based support, not one in place of the other. • Policymakers should mandate organizational equity training and establish resident advisory boards with meaningful decision-making authority to address racism legacy effects shaping resident trust and advocacy.What This Paper Adds
Applications of Study Findings
Introduction
Government-assisted housing programs serve approximately five million low-income households in the United States, including a substantial proportion of older adults living on fixed incomes. These programs primarily aim to reduce financial burden by providing stable, affordable housing; however, whether this economic relief translates into improved psychological well-being remains an open and complex question (Dweik & Woodhall-Melnik, 2023; Jaramillo & Rohe, 2024). Depression and anxiety remain prevalent among residents of government-assisted housing despite reduced housing cost burden, suggesting that housing environments shape mental health through multiple pathways beyond economic relief (Dweik & Woodhall-Melnik, 2023; Jaramillo & Rohe, 2024). Understanding these pathways requires moving beyond individual-level explanations to examine how housing conditions, neighborhood contexts, and organizational policies interact to influence resident well-being.
Evidence on the relationship between subsidized housing and mental health is growing, though findings are mixed and causal pathways remain unresolved. Some systematic reviews document elevated rates of depression and anxiety among low-income households in publicly subsidized housing compared to general populations, while others report null or inconsistent associations depending on population characteristics, housing type, and contextual factors (Dweik & Woodhall-Melnik, 2023). Importantly, the direction of causality remains unclear: it is uncertain whether housing environments contribute to mental health challenges, or whether pre-existing mental health vulnerabilities increase the likelihood of individuals entering subsidized housing programs (Dweik & Woodhall-Melnik, 2023). Specific housing quality factors including pest infestation, inadequate maintenance, and environmental hazards associate with depressive symptoms among public housing residents (Shah et al., 2018). Older adults in urban subsidized housing experience particularly high rates of loneliness and depression, with social isolation emerging as a significant concern (Gonyea et al., 2016). The timing of housing crises matters substantially, with housing instability creating cascading impacts on mental health that extend beyond the immediate crisis period (Marcal, 2018). Despite this growing but mixed evidence base, significant gaps remain in understanding the mechanisms that link housing environments to psychological well-being, particularly for older adults in rural contexts.
Current research on housing and mental health faces important limitations. Quantitative studies dominate the literature, documenting prevalence and associations but offering limited insight into how residents experience and navigate housing-mental health relationships (DeVoss et al., 2022). Few studies have examined the lived experiences of older adults in government-assisted housing or explored how residents themselves understand connections between their housing situations and mental health. Additionally, most research focuses on urban contexts, leaving rural subsidized housing populations understudied despite documented disparities in mental health service access in rural areas. Rural older adults face compounded disadvantages including geographic isolation, limited public transportation infrastructure, scarce mental health services, and reduced access to social and community resources that urban-focused research does not adequately capture. Scoping reviews identify persistent gaps in understanding how federal housing subsidy programs integrate or fail to integrate mental health services, pointing to need for research examining service availability and accessibility from resident perspectives (DeVoss et al., 2022).
Socioecological frameworks offer a valuable lens for understanding housing-mental health relationships by attending to multiple levels of influence. These frameworks recognize that individual health outcomes emerge from interactions among individual characteristics, interpersonal relationships, community resources, and organizational policies (Bronfenbrenner, 1994). Housing environments operate across all these levels simultaneously, creating complexity that single-level analyses cannot capture. Permanent supportive housing research demonstrates that program implementation quality and management practices significantly influence effectiveness, suggesting organizational factors matter substantially (Aubry et al., 2020). However, few studies have explicitly applied socioecological frameworks to examine mental health among older adults in government-assisted housing.
This study addresses these gaps by examining how housing environments shape mental health and well-being among older adults residing in government-assisted housing in a rural southeastern community. Using qualitative methods grounded in a socioecological framework, we explored resident experiences across individual, interpersonal, community, and organizational levels. Rather than establishing causality, we sought to understand the mechanisms and pathways through which housing environments shape mental health, how challenges interact across ecological levels, and how residents navigate these challenges. The findings provide insight into mechanisms linking housing to mental health and identify intervention points for improving well-being in this population.
Methods
Study Design and Philosophical Approach
This descriptive qualitative study employed a social ecological framework to examine how housing environments shape mental health and well-being among older adults. We used a hybrid analytical approach combining exploratory thematic analysis (Braun & Clarke, 2006) and framework analysis (Ritchie & Spencer, 1994), allowing emergent themes to develop inductively while enabling systematic organization for intervention development. Our epistemological stance was pragmatic realism, recognizing that participant experiences reflect both subjective meaning-making and material realities of housing and service systems. The study adhered to Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Tong et al., 2007).
Setting and Context
The study took place in a government-assisted housing community in Walker County, Alabama, a predominantly rural area in the southeastern United States. The housing complex serves low-income older adults under federal housing assistance programs. Walker County is characterized by high rates of poverty, limited economic opportunity, and restricted access to health and social services that are typical of rural communities in the southeastern United States. The county lacks a robust public transportation infrastructure, and access to healthcare, mental health services, social support programs, and community resources is constrained by geographic isolation and limited service capacity. These conditions reflect broader patterns of rural resource scarcity that shape daily life for residents. The research team had no prior relationship with the housing authority or residents before the study.
Participants and Sampling
We recruited 16 older adults residing in the housing complex. Eligibility criteria included age 60 years or older, current residence in the community, ability to provide informed consent, and willingness to discuss housing experiences and mental health. We used purposive sampling to ensure diversity in gender, race, and length of residence through posted flyers and housing authority staff referrals. Staff informed residents about the study but did not influence participation decisions. No interested residents were excluded. The final sample included 11 women and 5 men, ages 60 to 86 years (mean 67.9, SD 8.2). Eleven participants identified as Black or African American and five as White. Length of residence ranged from 1 to 18 years (mean 7.3). Three participants were caregivers for ill spouses or family members. Mental health status was self-reported and not verified through clinical records. Participants used both formal diagnostic terminology, such as PTSD, and colloquial language, such as “nerves” and “anxiety,” to describe their mental health experiences. These reports were treated as experiential self-disclosures rather than clinical classifications, and the study did not distinguish between formally diagnosed and informally described mental health conditions. Data saturation was achieved after 16 interviews, as no new themes emerged in the final three interviews.
Data Collection Procedures
The first and second authors conducted all interviews between July and September 2025. The first author is an assistant professor of nursing, and the second author is a doctoral candidate in counseling, both trained in qualitative interviewing. Interviews took place in a private room at the housing facility, lasting 40 to 50 minutes each. We used a semi-structured interview guide with open-ended questions organized by socioecological levels: individual experiences, interpersonal relationships, community resources, and organizational policies. The guide was pilot tested with two residents not included in the final sample. Sample questions included the following: How has living here influenced your mental health and well-being? Can you describe your relationships with neighbors? What community resources do you access? How do housing policies affect your daily life? Interviewers used probes to explore responses in depth and encouraged participants to share stories and examples. Field notes captured nonverbal observations and contextual details immediately after each interview. All interviews were audio-recorded with permission and transcribed verbatim by a professional service. Transcripts were checked for accuracy against audio recordings. We did not return transcripts to participants for comment, as this was not included in original consent procedures. Participants received $50 gift cards.
Researcher Characteristics and Reflexivity
The research team consisted of three Black nursing scholars: the first author is an assistant professor with extensive qualitative research experience examining aging, housing, and health disparities; the second author is a doctoral candidate trained in qualitative methods; and the senior author is an experienced nursing researcher with published qualitative studies in gerontology. This shared racial identity facilitated rapport with the majority Black participant group while requiring attention to power differentials inherent in the researcher-participant relationship. All team members maintained reflexive journals documenting assumptions, reactions, and interpretive decisions. We explicitly discussed how our positions as university-affiliated researchers might influence participant responses and interpretation through regular debriefing sessions.
Data Analysis
We employed a two-phase analytical approach. Phase one followed Braun and Clarke’s six-step thematic analysis process (Braun & Clarke, 2006). Two team members independently conducted line-by-line coding of all transcripts without predetermined codes, meeting weekly to compare codes and discuss patterns. Initial coding generated 127 codes. Through iterative analysis, we collapsed and organized codes into candidate themes through constant comparison, reviewing them against original data to ensure internal coherence and clear distinctions. Themes were refined using participant language where possible. Phase two applied Ritchie and Spencer’s framework analysis method (Ritchie & Spencer, 1994), mapping inductively derived themes onto Bronfenbrenner’s socioecological framework across individual, interpersonal, community, and organizational levels. We created four analytical matrices populated with participant data, enabling identification of patterns, variations, and cross-level interactions. Analysis occurred concurrently with data collection. We used MAXQDA software to manage data and facilitate analysis. All analytical decisions were documented in detailed audit trails. The full research team met biweekly throughout analysis to discuss coding decisions, theme development, and interpretation. Disagreements were resolved through discussion and return to original transcripts until consensus was achieved.
Trustworthiness and Rigor
We employed multiple strategies to ensure trustworthiness following Lincoln and Guba’s criteria (Lincoln & Guba, 1985). Credibility was established through prolonged engagement, peer debriefing, negative case analysis, and triangulation of researchers with different perspectives and career stages. We provided thick description with detailed participant quotes and contextual information to enable readers to assess transferability. Dependability was addressed through detailed audit trails documenting all coding decisions, theme development, and interpretive choices. Confirmability was enhanced through reflexive journals and regular team discussions about how our backgrounds and assumptions influenced interpretation. We did not conduct member checking with participants, as this was not included in original consent procedures. However, we employed multiple other trustworthiness strategies and transparent reporting of analytical processes.
Ethical Considerations
All study procedures received approval from the appropriate ethics review board. Participants provided written informed consent after receiving detailed information about the study’s purpose, procedures, potential risks and benefits, and their right to withdraw at any time without consequence. We emphasized that participation or withdrawal would not affect their housing status. Participants were provided with referral information for counseling services, and the research team followed established protocols for responding to participant distress; no participants required crisis intervention. To protect confidentiality, pseudonyms are used for all participants. Audio recordings and transcripts were stored on password-protected, encrypted devices accessible only to the research team. In accordance with ethics board requirements, audio recordings will be destroyed three years after study completion.
Findings
Participant Demographic Characteristics (N = 16)
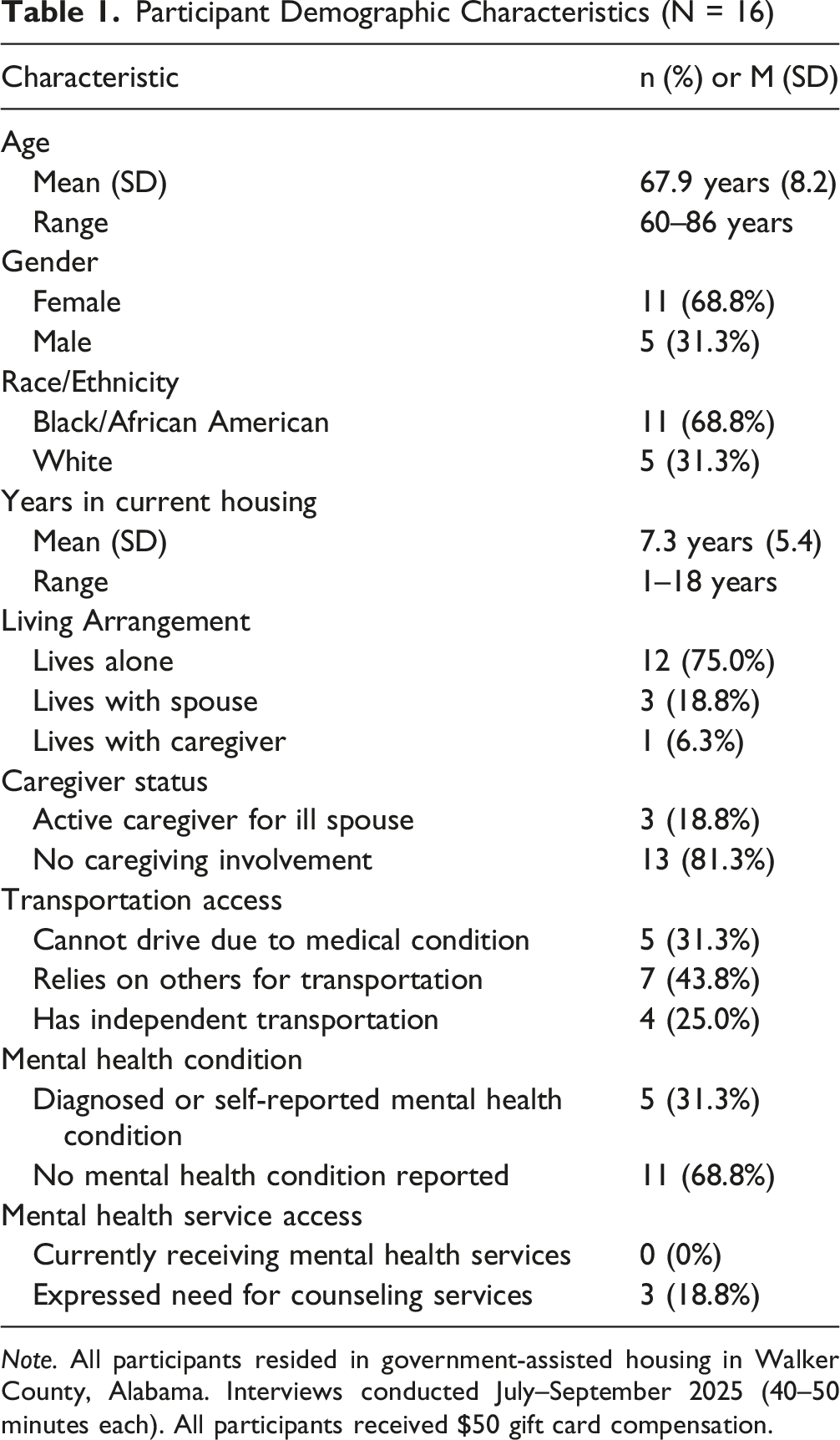
Note. All participants resided in government-assisted housing in Walker County, Alabama. Interviews conducted July–September 2025 (40–50 minutes each). All participants received $50 gift card compensation.
Individual Level: Personal Experiences and Mental Health
Three primary themes operated at the individual level: anxiety as a controlling force, social isolation as a protective strategy, and housing as sanctuary despite constraints.
Anxiety as Controlling Force
Nine participants described significant anxiety or mental health challenges that actively limited their daily functioning. For these residents, anxiety was not merely a background concern but an active force shaping decisions about when to leave the apartment and whether to interact with neighbors. One participant with diagnosed PTSD explained how anxiety dominated daily life. She stated, “My anxiety controls me a lot. My anxiety and my nerves are about shot. So I don’t come out of my apartment much.” She later added, “If I just had something for my nerve and anxiety, I would be more apt to go out and socialize.” Her PTSD remained untreated, reflecting not personal choice but the absence of any accessible mental health services in the rural community. With no local counseling available and no mental health partnerships through the housing organization, residents with formally diagnosed conditions were left to rely on informal or spiritual coping strategies, a gap described more fully under the Unmet Mental Health Service Needs theme. The impact of untreated anxiety extended beyond personal discomfort. Participants described how mental health challenges created barriers to community engagement, healthcare access, and relationship building. One woman caring for her ill husband described variable mood states. She said, “Sometimes I’m down, depends day to day. My mental health works in some ways and not in other ways.” Despite these struggles, participants identified no accessible mental health services in their community.
Social Isolation as Protection and Prison
Fourteen participants engaged in strategic social withdrawal, framing isolation as protective wisdom rather than loneliness. The phrase “stay to yourself” emerged repeatedly as guidance for navigating public housing successfully. One woman explained her approach clearly. She said, “I try to stay to myself. I don’t try to bother the neighbors. That way I don’t get involved in nothing. I go in and out. If I see somebody falling, I’ll get help, but other than that I try to tend to my business.” This strategic isolation served multiple purposes. Participants protected themselves from drama, maintained privacy, and avoided entanglement in neighbors’ problems.
It is important to distinguish between social isolation as a deliberate behavioral choice and loneliness as a subjective affective experience: participants described engaging in both simultaneously. While social isolation is conventionally understood in the literature as an objective, non-volitional condition reflecting an involuntary deficit in social contact and relationships, our participants engaged in a form of deliberate social withdrawal that complicates this characterization. Strategic withdrawal was intentional and agentic, reflecting accumulated wisdom about navigating shared housing environments safely. Yet, this same strategy produced feelings of loneliness and social disconnection that participants did not always desire or welcome. Many participants acknowledged loneliness and limited support networks. One resident noted, “I don’t really have nobody” when asked about sources of support. This statement captures the emotional cost embedded within strategic isolation: participants chose withdrawal to protect their housing stability and personal well-being, yet simultaneously experienced genuine longing for meaningful connection. These two dimensions coexisted in tension, with residents valuing the safety of self-imposed boundaries while expressing quiet grief over the social disconnection those boundaries created. The choice to isolate was real, and so was the loneliness it produced. Another resident described the paradox more directly, explaining that staying isolated keeps the apartment situation stable but creates social disconnection. Interestingly, two participants described themselves as naturally introverted, using this identity to justify limited social engagement. One man stated, “I’m an introverted people person. I can check their body language to see if they want to be bothered. I respect their privacy.” This framing positioned isolation as personality preference rather than circumstantial necessity.
Housing as Sanctuary Despite Constraints
Fifteen participants expressed profound gratitude for their housing while simultaneously acknowledging significant limitations. This paradox appeared throughout interviews. Residents compared their current situation to worse alternatives such as homelessness, abusive family situations, or unaffordable independent housing. One woman who previously lived with emotionally abusive family members described her reaction to getting her own apartment. She said, “When I got my apartment, it was like hallelujah.” However, she immediately qualified this gratitude by adding that the apartment is “no bigger than a mid-sized storage unit.” Religious language saturated descriptions of housing gratitude. Multiple participants stated they “thank the Lord every day” for having a place to live. One woman explained, “There’s a lot of people who don’t have anywhere to stay. I can wake up and see people out there on the bench sleeping. And I just thank the Lord that I do have somewhere to stay.” This comparative gratitude positioned even constrained housing as preferable to visible alternatives in the community.
However, it is important to consider whether gratitude expressions were entirely voluntary or whether they also reflected constrained voice. Residents who depend on housing authorities for their shelter may perceive limited safety in voicing complaints, potentially producing self-protective expressions of satisfaction that do not fully capture the complexity of their experience. Several participants tempered gratitude with immediate qualifications, as illustrated above, suggesting awareness of real limitations they nonetheless felt unable to fully articulate. Taken together, the findings suggest that housing may have supported mental well-being primarily by preventing worse outcomes, such as homelessness or abusive living situations, rather than by actively promoting positive psychological health. This distinction matters for how housing program effectiveness is measured and understood.
The constraints participants accepted included apartments too small for belongings, restrictive policies preventing personal touches like plants, delayed maintenance, and limited privacy. One man noted that apartments have rules and restrictions unlike homeownership, where “you don’t have the rules.” Despite these limitations, residents demonstrated pragmatic acceptance rather than resignation, recognizing that housing security required tolerance of imperfect conditions.
Interpersonal Level: Neighbor Relationships and Boundaries
Two primary themes operated at the interpersonal level: proximate but bounded relationships and noise as a bodily threat.
Proximate but Bounded Relationships
Physical proximity in housing complexes created unique relationship dynamics. Participants lived steps from neighbors’ doors, enabling mutual aid while simultaneously requiring careful boundary maintenance. One woman described helping a neighbor immediately. She stated, “It happened two or three days ago. My neighbor, she took me to get my medicine and paid for it.” This practical support demonstrated how proximity enables assistance during crises. However, most participants maintained strategic emotional boundaries despite physical closeness. They distinguished between “speaking” and “socializing” with neighbors. As one woman explained, “We get along good. We listen, we speak, we socialize. They go their way, I go mine.” This calibrated engagement allowed friendly coexistence without the complications of deeper intimacy. Several participants noted they got along better with neighbors than with family, suggesting that proximate relationships filled important social needs while respecting independence. One woman said, “I get along with my neighbors better than I did my family.” Yet, the same residents described staying inside most of the time to avoid excessive interaction.
Noise as Bodily Threat
Eleven participants described noise as a significant problem, but for some it transcended mere annoyance to become a bodily threat. Thin walls and concrete construction meant residents heard everything: footsteps at 3:30 in the morning, items dropping, neighbors singing, and music vibrating windows. For participants with PTSD or anxiety disorders, these sounds triggered physiological reactions. One woman with PTSD explained, “I live in the very middle of all these apartments and I hear everything. My upstairs neighbor can drop something, and it makes me jump like I’m shot. She gets up at 3:30 every morning and I can hear her footsteps as she steps on the floor.” The involuntary startle response to ordinary sounds created continuous stress. Participants had no control over their auditory environment and no escape from triggering stimuli. One woman described her neighbor who sings loudly on the porch. She said, “You see how close our apartments are. She stands out on her porch. My window’s right here. When she turns her radio up so it’s real loud for her to hear, then she starts singing. My bedroom window is right here. It gets irritating.” Multiple residents had complained, but the behavior continued, demonstrating limits of interpersonal solutions to structurally amplified problems.
Community Level: Infrastructure and Service Gaps
Two primary themes operated at the community level: transportation as gatekeeper and unmet mental health service needs.
Transportation as Gatekeeper to Life
Ten participants identified lack of transportation as a critical barrier affecting all life domains. Participants could not drive due to seizures, disability, or age. No public transportation existed in the rural community. The absence of mobility created cascading problems across healthcare, social connection, church participation, and independence. One man explained the daily frustration. He said, “When you need to go somewhere, you don’t really have no transportation. You have to pay somebody to take you places. Sometimes I get aggravated when I can’t get to the store or you have a doctor appointment and you’ll be late.” Transportation barriers particularly affected caregivers, who needed to attend both their own appointments and those of care recipients. One woman caring for her ill husband explained how immobility compounded caregiving stress. She stated, “Due to transportation issues, quite a few doctors I didn’t have to attend. Our transportation, getting out and doing stuff like we used to, we don’t visit people anymore.” Several participants proposed solutions. They suggested a community bus service that could take residents to grocery stores, medical appointments, and churches on a regular schedule. One woman explained the need clearly. She said, “People coming to help seniors get around, picking up seniors, taking them to the store once a week. People that don’t have washers and dryers, they can take them to do their laundry.”
Unmet Mental Health Service Needs
Nine participants explicitly identified a need for professional mental health services. This need emerged unprompted during interviews, indicating its salience for residents. One woman stated the community need directly. She said, “Need more counseling. A lot of people down here, they’ve gone through a lot and don’t share it with no one. People need someone to tell stories to. People don’t come out. They’d be so up in the house.” This participant recognized that isolated suffering characterized the community. Residents kept problems inside without outlets for processing trauma or managing mental health conditions. No local counseling services existed, and the organizational structure provided no mental health partnerships or referral systems. One woman described wishing for someone she could talk to comfortably without receiving negative feedback, noting that past attempts to seek advice through church connections had been unhelpful. The gap between mental health needs and available services left residents relying primarily on spiritual coping mechanisms. Thirteen participants described prayer and faith as their main coping resources. While spiritual practices provided comfort, participants distinguished these from professional mental health services and explicitly requested access to counseling.
Organizational Level: Housing Authority Practices and Policies
Two primary themes operated at the organizational level: policy enforcement gaps and organizational racism legacy.
Policy Enforcement Gaps
Eight participants described problems with unauthorized residents and visitors creating safety concerns, noise issues, and community disruption. Residents carefully distinguished between authorized residents, who were generally acceptable neighbors, and unauthorized people living in units or visiting excessively. One woman explained, “It’s not the residents, it’s the people that come down here. They bring all the noise, all the drama.” She later clarified, “You got people living with people that don’t be supposed to be on the lease. That’s where our stuff be coming in at.” Several participants referenced past law enforcement sweeps that removed unauthorized residents, expressing desire for similar actions. One woman stated she used to walk early in the morning but stopped “when them girls come down bringing guns.” She added, “They need to do one of those again,” referring to previous enforcement actions. The blurred boundaries around who belonged in the community created insecurity and enabled problems that residents felt powerless to address individually.
Organizational Racism Legacy
Two participants explicitly discussed experiences with racist housing management, though this likely represented underreporting of a broader experience. One woman provided detailed testimony about previous management practices. She stated, “The past management wasn’t any good. I can say this, she just seemed racist. She didn’t have any communication skills with people. She sent the workers out. You didn’t really get to socialize with her. You didn’t get to go in the office. You didn’t get to talk over the phone with her. She’d always pass the conversation off to another employee. Only thing she would like to do is enforce eviction.” This participant described a management approach characterized by inaccessibility, differential treatment, and use of eviction threats as the primary tool. The discrimination operated at the organizational level through patterns of communication barriers, policy enforcement disparities, and creation of a climate of fear. She acknowledged improvement under current management, stating “now I’m thinking it’s gonna be much better. It’s turned around a little bit more.” However, the historical experience shaped ongoing wariness about organizational trustworthiness.
Cross-Level Interactions
The themes operated not in isolation but through complex interactions across socioecological levels. For example, individual inability to drive combined with community infrastructure gaps and organizational service absence to create forced interpersonal dependence on neighbors for rides. Similarly, organizational building design with thin walls amplified interpersonal noise conflicts that triggered individual trauma responses. These cross-level interactions demonstrated that single-level interventions would inadequately address the complexity of housing and mental health relationships. Multi-level approaches addressing individual needs, interpersonal dynamics, community resources, and organizational practices simultaneously offer the greatest potential for improving resident well-being.
Discussion
This study examined how government-assisted housing environments shape mental health and well-being among older adults through a socioecological framework. Three primary contributions emerge from this work. First, housing functions simultaneously as sanctuary and constraint, a paradox that standard satisfaction measures fail to capture. Second, transportation barriers uniquely operate across all four socioecological levels, functioning as a cascading gatekeeper to healthcare, social connection, and independence. Third, ten of eleven themes spanned multiple ecological levels, validating the necessity of multi-level rather than single-level intervention approaches for this population.
The sanctuary-constraint paradox carries direct implications for how housing program effectiveness is measured. Prior systematic studies have documented associations between subsidized housing and depression or anxiety (Kyei et al., 2025a, 2025b) but our findings reveal that resident gratitude is fundamentally comparative rather than absolute (Dweik & Woodhall-Melnik, 2023; Kyei et al., 2026). Residents expressed thankfulness for housing precisely because they compared it to devastating alternatives such as homelessness, family abuse, or unaffordable independent living. Standard housing satisfaction surveys likely overestimate well-being by capturing relief from worse alternatives rather than genuine quality of life improvement. Additionally, gratitude expressions may partly reflect constrained voice: residents who depend on housing authorities for shelter may self-censor complaints to protect their housing security, a dynamic that qualitative inquiry is uniquely positioned to uncover. The religious language saturating gratitude expressions points to cultural and spiritual dimensions of housing security warranting greater attention in future research.
Our finding that anxiety functions as an active controller of daily life extends previous work in subsidized housing. Older adults in urban subsidized housing experience high rates of loneliness and depression (Gonyea et al., 2016), but our participants described anxiety not as a passive symptom but as a force actively directing decisions about leaving apartments and interacting with neighbors. This distinction matters for intervention design. The urgency of mental health service needs emerged clearly, with participants explicitly requesting professional counseling that did not exist locally. Significant gaps in mental health service integration within federal housing programs persist despite documented need (DeVoss et al., 2022).
The theme of social isolation as simultaneously protection and prison reveal strategic agency often overlooked in aging research. High rates of social isolation have been documented but typically framed as unintended consequence rather than deliberate strategy (Taylor et al., 2022). This study adds an important distinction to a literature that predominantly frames social isolation as an objective, non-volitional deficit (Fakoya et al., 2020): deliberate behavioral withdrawal and loneliness as a coexisting subjective experience operated simultaneously in most participants. This aligns with emerging work recognizing that older adults may develop strategic approaches to managing social engagement rather than passively experiencing isolation (Machielse & Duyndam, 2020). Interventions promoting social connection must therefore address felt loneliness without dismantling the protective boundary strategies residents rely upon to maintain housing stability
Noise emerged as bodily threat rather than mere annoyance, particularly for residents with PTSD or anxiety disorders. While housing quality factors such as pest infestation have been linked to depressive symptoms (Shah et al., 2018), noise has received limited attention as an environmental stressor. Our findings demonstrate how organizational building design, interpersonal behaviors, and individual trauma histories interact to amplify harm, illustrating the explanatory value of socioecological analysis.
Transportation barriers emerged as the only theme spanning all four socioecological levels. While transportation challenges among rural older adults are well established in the literature ([Authors, Year]; [Authors, Year]), this study extends that work by revealing the socioecological mechanism through which immobility operates: individual disability combines with community infrastructure absence, interpersonal dependence on neighbors, and organizational service gaps to produce cascading limitation across healthcare access, social connection, church participation, and independence. This multi-level mechanism explanation, grounded in resident experience, represents a novel contribution to understanding transportation as a social determinant of health in rural aging contexts. Participants actively proposed community bus solutions, demonstrating awareness of and appetite for organizational intervention (Jaramillo & Rohe, 2024).
Faith-based coping proved highly effective for many participants, providing comfort, acceptance, and community connection. However, participants carefully distinguished spiritual practices from professional mental health services and explicitly requested access to both, challenging either-or framings that position faith and professional services as alternatives. This aligns with literature documenting faith as an important coping resource in Black communities while affirming that spiritual strength does not excuse service gaps (Kohn-Wood et al., 2016).
The small caregiver subgroup experienced compounded disadvantage across all socioecological levels, with individual stress, community service absence, and organizational gaps combining to create extreme isolation and burnout risk (Bronfenbrenner, 1994; Marcal, 2018). The organizational racism legacy theme, though explicitly raised by only two participants, likely reflects underreporting given sensitivity concerns. Historical discrimination created lasting wariness toward organizational systems even when current management improved, pointing to the importance of trust repair alongside practice change (Aubry et al., 2020).
The ecological nature of our findings validates the socioecological framework application. Ten of eleven themes spanned multiple levels, demonstrating that housing and mental health relationships operate through complex interactions rather than simple direct effects. Single-level interventions will inadequately address the complexity revealed.
Recommendations
Drawing on the socioecological framework, we offer targeted recommendations organized by ecological level. At the individual and community levels, housing authorities should establish dedicated transportation services with medical, grocery, and church routes, directly addressing the cascading impacts residents identified as most urgent. At the interpersonal and community levels, mental health providers should develop on-site counseling partnerships that complement rather than replace existing spiritual coping practices; residents explicitly want both. At the organizational and policy levels, housing authorities should implement equity training and establish resident advisory boards with meaningful decision-making authority to address the legacy of institutional racism and rebuild organizational trust. These multi-level recommendations reflect the ecological complexity of the findings and the concrete priorities residents themselves articulated.
Several limitations warrant acknowledgment. The single geographic location limits transferability to other rural or urban contexts. The cross-sectional design cannot assess change over time or establish causality. Social desirability bias likely led some participants to moderate their complaints given housing security concerns, and the possibility of constrained voice should be considered when interpreting expressions of gratitude. The sample included no Hispanic, Asian, or Indigenous participants, limiting understanding across all racial and ethnic groups. Future research should examine these themes in diverse contexts and assess intervention implementation and outcomes.
Conclusion
This study reveals that government-assisted housing simultaneously provides essential sanctuary and imposes significant constraints on older adults’ mental health and daily life. Rather than simply resolving financial burden, housing environments shape psychological well-being through complex, interacting mechanisms operating across individual, interpersonal, community, and organizational levels. Residents demonstrated remarkable resilience, strategic problem-solving, and clear articulation of their needs, actively proposing feasible solutions and requesting accessible support. The finding that 10 of eleven themes spanned multiple socioecological levels makes clear that single-level interventions are insufficient. Transportation access, on-site mental health services, and organizational equity practices represent the highest-leverage, resident-identified intervention points. Housing authorities, mental health providers, and policymakers now have concrete, evidence-based directions for improving well-being among this underserved and understudied population.
Footnotes
Acknowledgments
We thank the residents of the government-assisted housing community in Walker County, Alabama, who generously shared their experiences and insights for this research. We also acknowledge the housing authority staff who facilitated recruitment and provided space for interviews.
Ethical Considerations
This study was approved by the University of Alabama Institutional Review Board (IRB Protocol #25-05-8673). All study procedures were performed in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. All participants provided written informed consent prior to participation.
Consent to Participate
Written informed consent to participate in this study was obtained from all participants. Participants were informed that participation was voluntary and that withdrawal would not affect their housing status or services. All participants received detailed information about study purposes, procedures, risks, and benefits before providing consent.
Consent for Publication
Not applicable. This study does not contain any individual person’s data in any form (including individual details, images, or videos). All participant data is presented in aggregate or anonymized form using pseudonyms.
Author Contributions
Funding
This research was funded through the Saxon Endowed Rural Nursing Grant from the Capstone College of Nursing, The University of Alabama. The funding source had no role in study design, data collection, analysis, interpretation, or the decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of the qualitative data collected and to protect participant confidentiality, the interview transcripts generated and analyzed during this study are not publicly available. The coding framework and thematic analysis outputs are available from the corresponding author upon reasonable request and with appropriate ethics approval.