
Abstract
As Korea became a super-aged society in 2025, disparities in physical activity between urban and rural older adults have become increasingly important. Using data from the 2024 Community Health Survey, this study examined sociodemographic, health, lifestyle, and psychosocial factors influencing moderate-intensity physical activity among adults aged 65 years or older. Logistic regression showed that urban older adults with higher education and non-manual jobs, and rural older adults with increasing age and having a spouse, were less active. Walking practice and self-rated health were the strongest predictors in both regions. Cognitive impairment and depressive symptoms were positively associated with activity, possibly reflecting community-based rehabilitation participation. Findings suggest that physical activity in later life is a multidimensional behavior shaped by physical, emotional, social, and digital factors, supporting AI-integrated community care to promote equitable health management across regions.
Provides the first evidence comparing moderate-intensity physical activity determinants among Korean urban and rural older adults using national data. Demonstrates that physical activity is influenced by interconnected physical, emotional, and digital factors, not by individual will alone. Suggests AI-integrated community care as a structural solution to promote sustainable and equitable physical activity in aging populations.
Policymakers can use these findings to design AI-based monitoring and tailored exercise programs at community health centers. Urban areas may prioritize digital inclusion and social connection, while rural areas can strengthen mobile health services. The study supports integrating AI-driven feedback systems into community care to sustain older adults’ physical activity and reduce regional disparities.What This Paper Adds
Applications of Study Findings
Introduction
Korea became a super-aged society in 2025, and the decline in physical activity among older adults, together with chronic diseases and mental health problems, has emerged as a complex social challenge (Lee & Lee, 2024). More than 40% of adults aged 65 years or older do not meet the recommended level of walking practice (at least 30 minutes a day, five days a week) (Seo et al., 2022), indicating that a large proportion of older adults still fail to meet the moderate-intensity physical activity standard defined in the 2024 Community Health Survey as activities causing slight breathlessness or mild exertion for at least 10 minutes (Korea Disease Control and Prevention Agency, 2024). Such insufficient physical activity leads to chronic diseases such as hypertension and diabetes, cognitive decline, and increased depressive symptoms, thereby raising community-level healthcare expenditures and reducing the quality of life among older adults (Son & Jo, 2025).
Earlier Korean studies have consistently demonstrated that insufficient physical activity among older adults is closely associated with adverse physical and mental health outcomes, reinforcing the public health importance of promoting active aging (Jung et al., 2023; Roh et al., 2015). In addition, recent international evidence suggests that physical activity in later life is not only related to physical health but also to psychological well-being and access to supportive services, highlighting that physical activity is a multidimensional phenomenon shaped by broader contextual factors (Coşkun et al., 2023; Ercan et al., 2025; Çomaklı Duvar et al., 2025).
The gap in physical activity between urban and rural areas arises not only from differences in the physical environment but also from disparities in access to health information, care resources, and digital literacy (Kang et al., 2023). Urban older adults have relatively better access to exercise facilities and healthcare resources, yet decreased digital literacy and social isolation act as major barriers to healthy behavior (Shon & Kim, 2024). In contrast, rural older adults demonstrate stronger community bonds and higher participation in social activities, but lack of exercise spaces and limited access to healthcare professionals remain major obstacles (Kang & Kim, 2024). Similar urban–rural disparities in health behaviors and health outcomes among older adults have been documented in recent Korean studies, suggesting that regional differences reflect broader structural and social inequalities (Jung, 2023; Shin et al., 2024). These findings indicate that urban–rural differences are not merely lifestyle variations but reflect structural inequalities that influence health behaviors among older adults.
Given these structural disparities, traditional manpower-centered approaches alone are insufficient to address the complex needs of aging populations. Consequently, there is an urgent need to transition from manpower-centered care to an Artificial Intelligence (AI)-integrated community care system that enables continuous monitoring and personalized support. Recent initiatives in Korea have expanded AI- and Internet of Things (IoT)-based healthcare services for older adults, demonstrating the potential effectiveness of technology-driven care interventions (Kim et al., 2024; Lee et al., 2024; Park et al., 2024).
Recent large-scale studies have further highlighted the potential of data-driven and technology-supported health monitoring systems to improve population-level physical activity and health outcomes (Lee et al., 2022; Park et al., 2023). Internationally, digital healthcare systems for older adults are already expanding. Japan is implementing digital health and structural innovations to address population aging, with AI-assisted care and smart-home technologies forming key pillars of eldercare (Osawa et al., 2022). In Germany, the government has institutionalized digital health management through the Digital Health Applications (DiGA) system, which refers to physician-prescribed digital medical applications, including mobile apps and web-based therapeutic tools, that are reimbursed through the statutory health insurance system, and incorporated it into insurance coverage, thereby establishing digital care systems for older adults and patients with chronic conditions (Dittrich et al., 2023). Similarly, the United States utilizes AI and wearable technologies through the Medicare Remote Monitoring Program to support health management for older adults and reduce hospital readmission rates (Curtis & Willig, 2023). These examples illustrate that digital technologies can enhance both the sustainability and equity of care.
In contrast, Korea remains at the pilot stage; although substantial health data have been accumulated, translating such data into AI-based personalized care services remains limited (Kim et al., 2024). Previous studies have primarily examined the physical activity levels of community-dwelling older adults from sociodemographic, health, and social perspectives, while few have integrated digital literacy and technology-based care systems into their analyses (Kang et al., 2023; Kang & Kim, 2024; Shon & Kim, 2024). Moreover, Korean studies have reported complex and sometimes paradoxical associations between psychological stress, mental health, and health-related behaviors in later life, indicating the need for more nuanced, context-sensitive analyses (Min et al., 2023).
Furthermore, prior research has rarely focused on moderate-intensity physical activity, an activity level particularly amenable to community-based intervention, despite evidence that such activity is strongly associated with both physical and mental health outcomes in later life (Ercan et al., 2025; Park et al., 2022; Çomaklı Duvar et al., 2025). Compared with vigorous exercise, moderate-intensity physical activity is generally more accessible and sustainable for older adults because it can be incorporated into daily routines such as walking, light farming, or household activities. In addition, moderate-intensity activities are more feasible targets for community-based programs and public health interventions, particularly among older adults with chronic conditions or limited mobility.
Therefore, this study aims to examine the determinants of moderate-intensity physical activity among older adults in urban and rural areas using nationally representative data from the 2024 Community Health Survey (CHS). By identifying regional differences and associated factors, this study seeks to provide empirical evidence to support the development of AI-based community care systems and contribute to reducing health disparities in aging populations. In particular, as Korea began implementing an integrated community care system nationwide in March 2026 (Ministry of Health and Welfare, 2026), understanding region-specific determinants of physical activity has become increasingly important for designing effective and sustainable care strategies within this policy framework, highlighting the urgency of evidence-based and technology-supported approaches to community care.
Method
Study Design and Data Source
This study employed a cross-sectional design using secondary data from the 2024 Community Health Survey (CHS) conducted by the Korea Disease Control and Prevention Agency (KDCA). The CHS is a nationally representative dataset collected annually through stratified multistage sampling to assess regional health status and behaviors among community-dwelling adults in Korea (Korea Disease Control and Prevention Agency, 2024). Data are collected through standardized face-to-face interviews conducted by trained surveyors, ensuring consistency and reliability across regions. Because the study used publicly available secondary data without identifiable personal information, ethical approval and informed consent were waived in accordance with institutional review board (IRB) guidelines.
Study Population
A total of 83,794 individuals aged 65 years and older were included in the analysis. Participants were classified into urban and rural groups based on the administrative classification of their residence. Urban areas comprised dong (city districts), while rural areas included eup and myeon (towns and villages).
Variables
The dependent variable was the practice of moderate-intensity physical activity, defined according to the CHS criteria as performing activities causing slight breathlessness or mild exertion for at least 10 minutes per session. In the CHS, respondents were asked: “During the past week, on how many days did you engage in moderate-intensity physical activity that caused slight breathlessness or mild exertion for at least 10 minutes?” Responses ranged from 0 to 7 days. Moderate-intensity physical activity was categorized as 3 days or less and 4 days or more.
Independent variables included sociodemographic factors (sex, age, education level, household income, marital status, and occupation type), health-related factors (hypertension, diabetes, cognitive impairment, depression, and chewing difficulty), lifestyle factors (current smoking, walking practice, breakfast consumption, sleep duration, and weight control experience), and subjective factors (self-rated health, stress, and happiness). These variables were selected based on prior empirical and theoretical studies indicating that physical activity among older adults is influenced by a combination of sociodemographic, health, behavioral, and psychosocial factors (Jung et al., 2023; Min et al., 2023; Roh et al., 2015).
Cognitive impairment and depression were assessed based on self-reported physician diagnosis, while stress and subjective health were measured using self-reported single-item indicators provided in the CHS. Lifestyle variables such as walking practice and smoking status were assessed based on participants’ self-reported behaviors over the past week or current status.
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA). Binary logistic regression models were employed to examine factors associated with moderate-intensity physical activity, a dichotomous outcome variable. All analyses were conducted using complex sample survey weights, strata, and primary sampling units provided by the Korea Disease Control and Prevention Agency to account for the complex sampling design and ensure national representativeness. Descriptive statistics were used to compare the general characteristics of urban and rural older adults, and differences were tested using the chi-square test. Binary logistic regression analyses were conducted separately for urban and rural groups, and the results were expressed as odds ratios (Exp(B)) and 95% confidence intervals (CIs). Statistical significance was set at p < .05.
Prior to model estimation, key assumptions of binary logistic regression were examined. Multicollinearity among independent variables was assessed using variance inflation factors, and no problematic multicollinearity was identified. Influential observations were evaluated using diagnostic statistics, and no influential outliers were detected. Linearity in the logit for continuous predictors was assessed, and no meaningful departures from linearity were observed. All continuous variables were assessed for linearity in the logit, and categorical variables were entered as dummy variables; multicollinearity was evaluated using variance inflation factors, and no violations of model assumptions were detected.
Results
Sociodemographic Characteristics
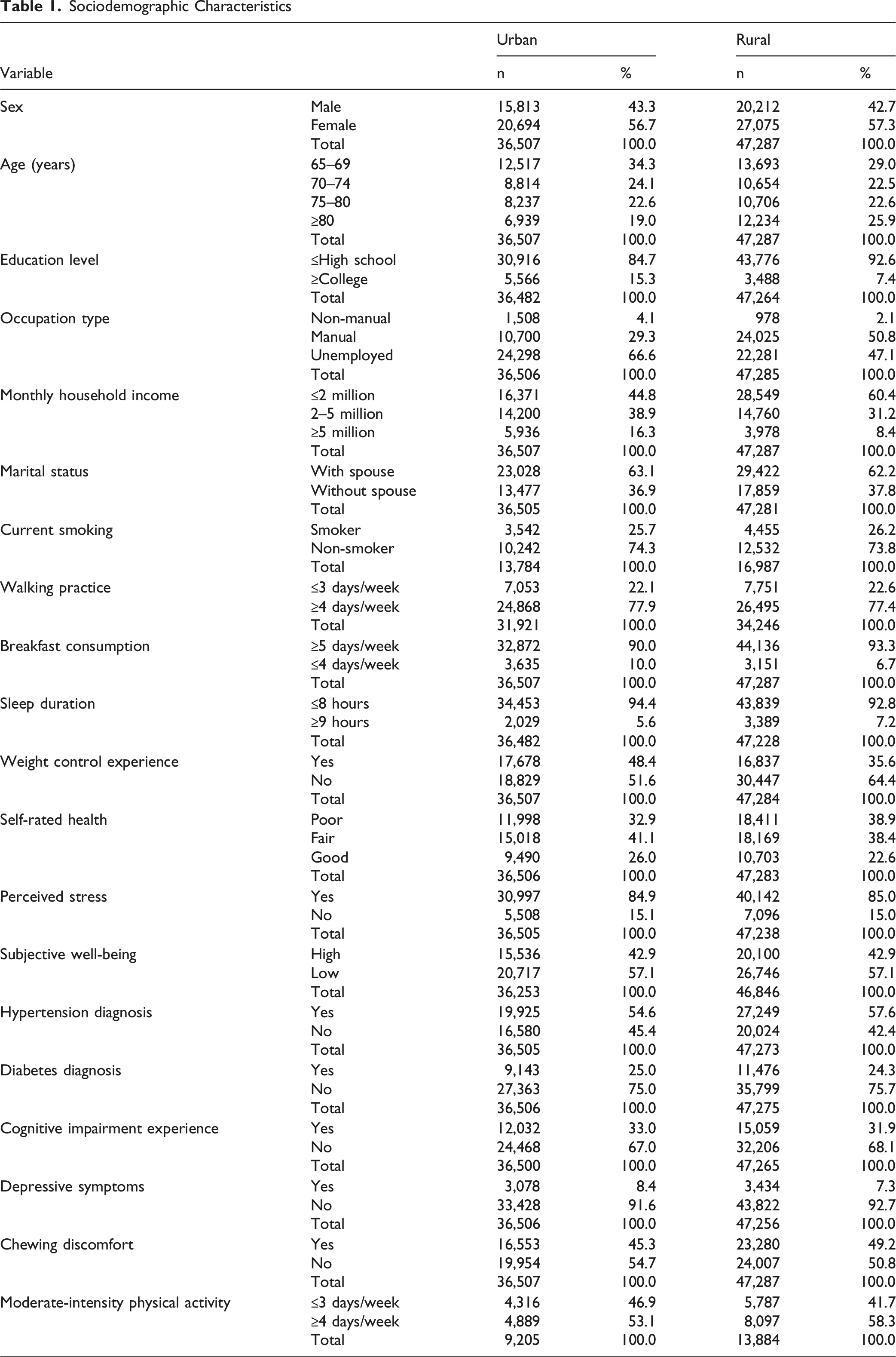
Impact of Regional Sociodemographic Factors on Moderate-Intensity Physical Activity
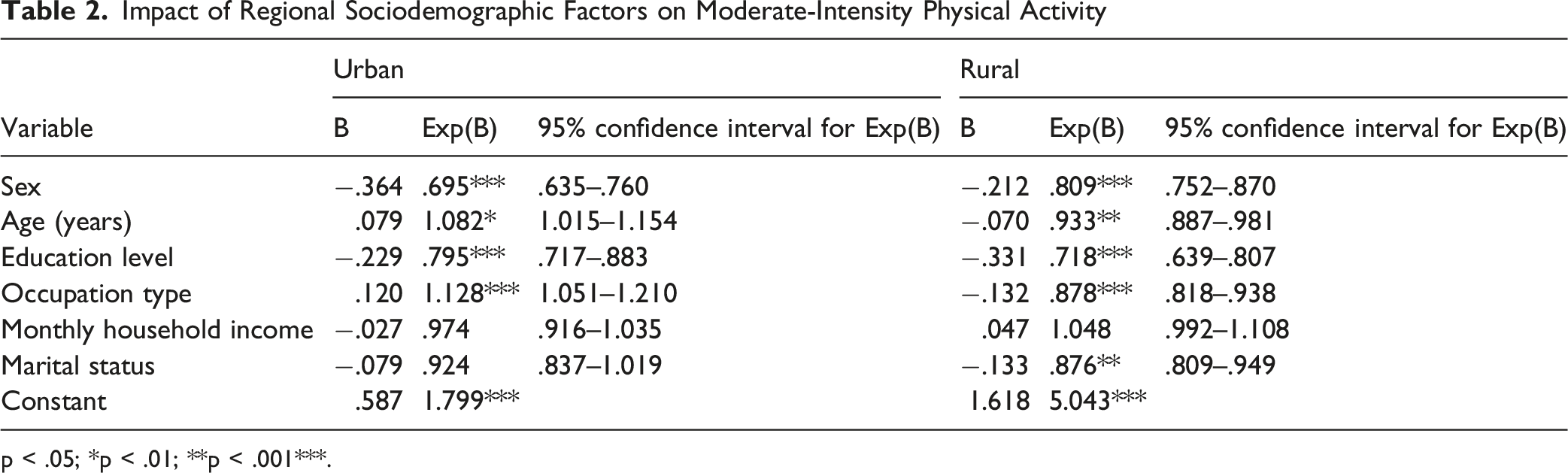
p < .05; *p < .01; **p < .001***.
In rural areas, age, education, occupation, and marital status were significant predictors. Older age (defined as per one-level increase across age groups: 65–69, 70–74, 75–80, and ≥80 years) was associated with lower likelihood of moderate-intensity physical activity (Exp(B) = 0.933, 95% CI: 0.887–0.981, p < .01) and higher education (Exp(B) = 0.718, 95% CI: 0.639–0.807, p < .001) was associated with lower activity levels. Occupation type was significantly associated with moderate-intensity physical activity (Exp(B) = 0.878, 95% CI: 0.818–0.938, p < .001), and older adults with a spouse were less active than those without one (Exp(B) = 0.876, 95% CI: 0.809–0.949, p < .01) (Table 2). This pattern indicates that demographic and social factors may influence physical activity differently in rural contexts compared with urban settings.
Effect of Regional Health Status on Moderate-Intensity Physical Activity
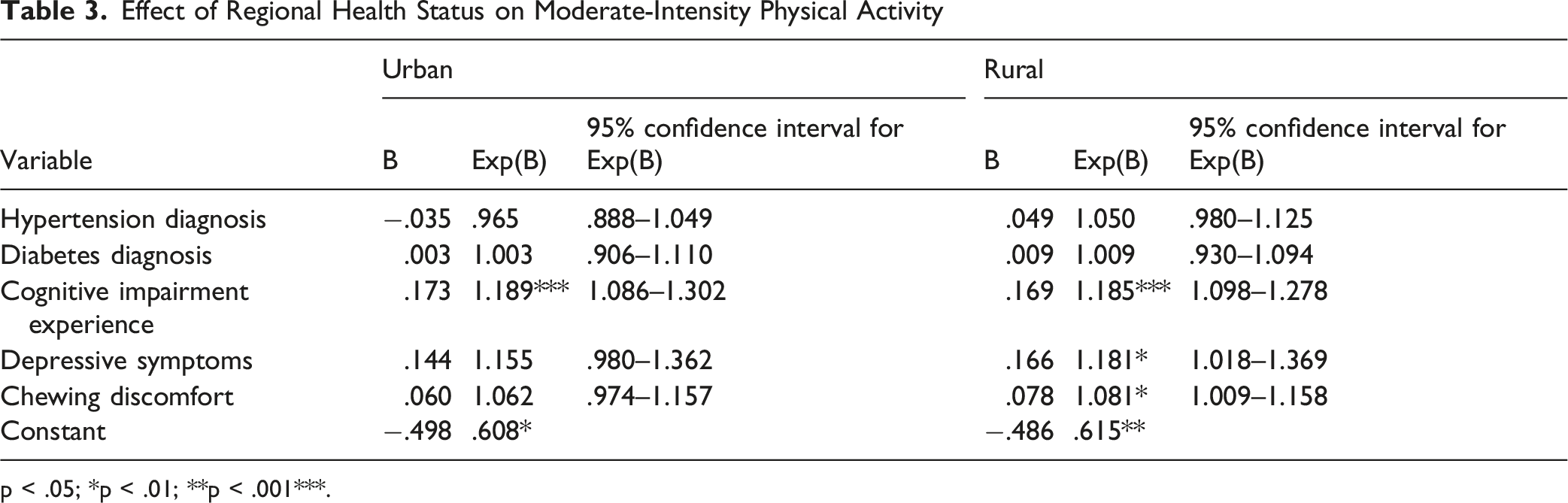
p < .05; *p < .01; **p < .001***.
Among lifestyle factors, in urban areas, current smoking, walking practice, and sleep duration were significant predictors. Current smokers were more active than non-smokers (Exp(B) = 1.229, 95% CI: 1.093–1.545, p < .01), and those walking four or more days per week were about 3.2 times more likely to engage in moderate-intensity activity than those walking 3 days or fewer per week (Exp(B) = 3.188, 95% CI: 2.658–3.824, p < .001). Longer sleep (≥9 hours) increased the likelihood of activity compared with sleeping ≤8 hours (Exp(B) = 1.889, 95% CI: 1.288–2.771, p < .01). Conversely, regular breakfast eaters (≥5 days/week) were less likely to engage in such activity compared with those consuming breakfast ≤4 days/week (Exp(B) = 0.726, 95% CI: 0.571–0.922, p < .01).
Effect of Regional Lifestyle Factors on Moderate-Intensity Physical Activity
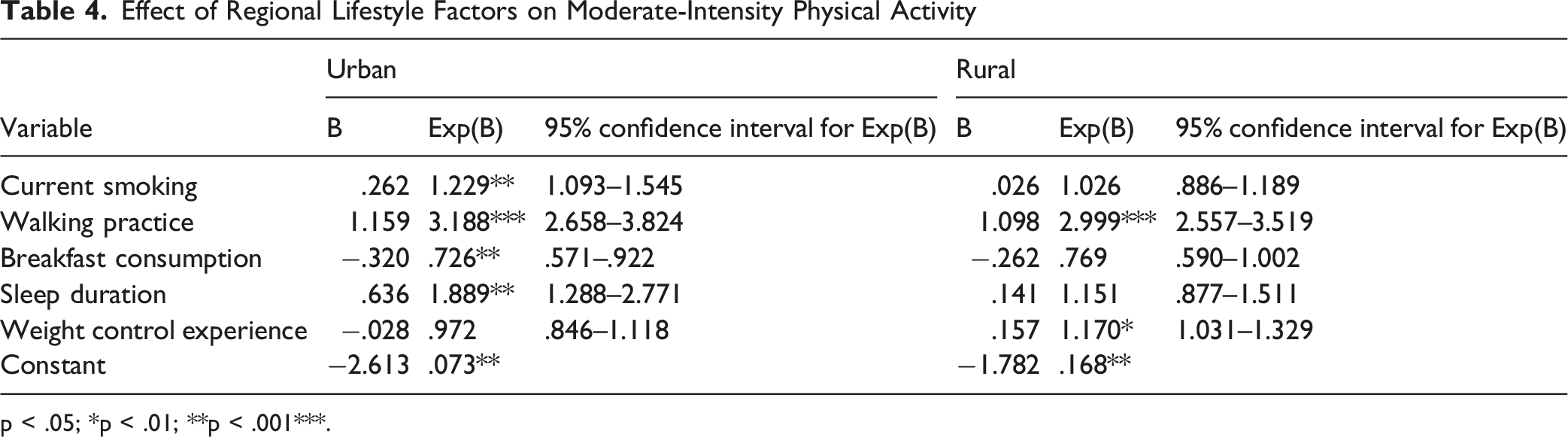
p < .05; *p < .01; **p < .001***.
Effect of Regional Subjective Perceptions on Moderate-Intensity Physical Activity
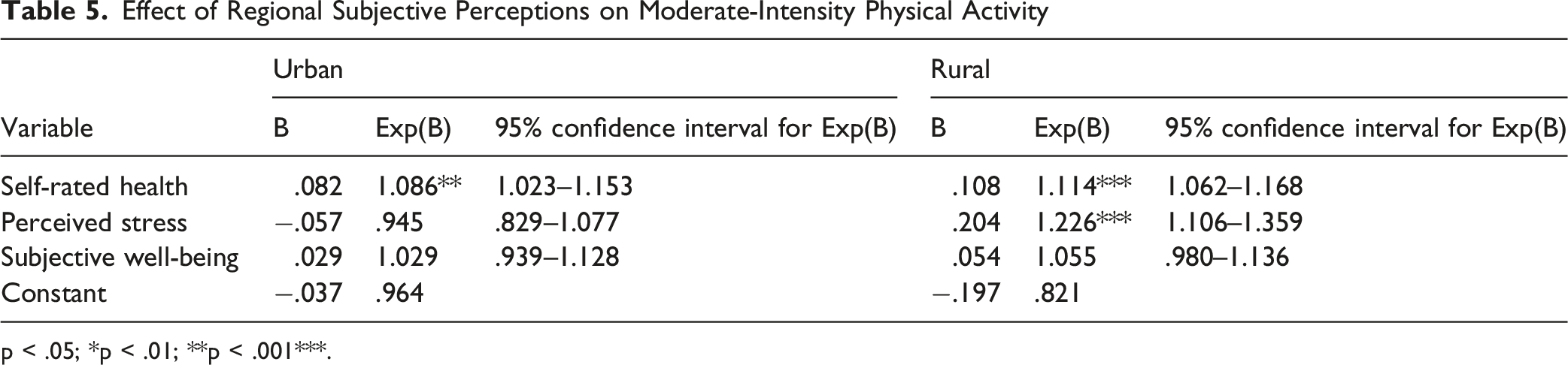
p < .05; *p < .01; **p < .001***.
Discussion
The present study identified significant urban–rural differences in moderate-intensity physical activity among older adults, highlighting the role of individual health status, lifestyle behaviors, and community context. These findings suggest that physical activity in later life is not solely an individual choice but is shaped by broader structural and environmental conditions. This interpretation is consistent with Korean studies emphasizing that health behaviors among older adults are embedded in social and regional contexts rather than determined solely by personal motivation (Jung, 2023; Shin et al., 2024).
Consistent with previous international studies, physical activity among older adults is closely associated with both physical and psychological health outcomes, as well as access to supportive services (Coşkun et al., 2023; Çomaklı Duvar et al., 2025). In particular, moderate-intensity physical activity has been shown to play a protective role in mental well-being and overall life satisfaction, underscoring its importance as a target for community-level intervention (Ercan et al., 2025). Similar associations between physical activity, mental health, and subjective well-being have also been reported in Korean older populations (Jung et al., 2023; Roh et al., 2015). However, prior studies have largely examined these associations without explicitly considering regional disparities or the implications for technology-enabled care systems.
The urban–rural differences observed in this study align with earlier findings that contextual factors such as resource availability, social networks, and healthcare accessibility influence health behaviors among older adults (Jung, 2023; Kang & Kim, 2024; Shin et al., 2024). Extending previous research, this study demonstrates that the determinants of moderate-intensity physical activity differ between urban and rural settings, suggesting that a uniform intervention approach may be insufficient to address regional inequalities (Coşkun et al., 2023; Ercan et al., 2025). Korean studies have similarly reported that socioeconomic conditions, occupational characteristics, and community resources contribute to divergent physical activity patterns across regions (Park et al., 2022; Shin et al., 2024). These results emphasize the need for differentiated strategies that reflect local contexts and community capacities.
From a policy perspective, the findings provide empirical support for integrating digital technologies into community-based eldercare. AI-based community care systems have the potential to translate such evidence into practice by enabling continuous monitoring of physical activity, delivering personalized feedback, and supporting timely interventions tailored to regional needs. Recent large-scale and data-driven studies have demonstrated that technology-supported health monitoring can improve physical activity engagement and population health outcomes, reinforcing the relevance of AI-enabled approaches in aging societies (Lee et al., 2022; Park et al., 2023). In urban areas, AI-driven tools may help mitigate social isolation and low digital engagement, whereas in rural settings, they may compensate for limited access to healthcare professionals by facilitating remote support and coordination.
Overall, this study contributes to the existing literature by bridging evidence on moderate-intensity physical activity with emerging discussions on AI-enabled community care. These findings may help guide region-specific community care strategies for older adults. This integrated perspective is particularly important given recent Korean evidence highlighting complex interactions between stress, mental health, and health-related behaviors in later life (Min et al., 2023).
Conclusion
This study analyzed factors influencing moderate-intensity physical activity among adults aged 65 years and older residing in urban and rural areas using data from the 2024 Community Health Survey (CHS). The results revealed that, among urban older adults, the practice rate of moderate-intensity physical activity was lower in women, highly educated individuals, non-manual workers, and those with longer sleep durations. In rural areas, the rate was lower among the oldest-old, married individuals, and those with higher education levels. Conversely, older adults who had experience in weight control or who engaged in regular walking were more likely to practice moderate-intensity physical activity.
In both urban and rural groups, walking practice and self-rated health consistently emerged as significant predictors of moderate-intensity physical activity. Maintaining daily physical activity plays a central role in sustaining healthy behaviors among older adults, and a positive perception of one’s health facilitates behavioral change. Furthermore, the higher rate of physical activity observed among older adults experiencing cognitive impairment, depression, or chewing discomfort indicates that participation in community-based rehabilitation and treatment programs may be linked to increased physical activity.
Overall, these results suggest that physical activity among older adults is not merely an exercise behavior but a multidimensional phenomenon shaped by physical function, emotional factors, social relationships, and digital competence (Kang et al., 2023). Therefore, future efforts should focus on developing an AI-integrated community care system that enables real-time analysis of older adults’ health information and activity data and provides personalized exercise and care feedback, while considering regional differences in resource availability and access to services (Kim et al., 2024).
In conclusion, this study provides empirical evidence supporting the establishment of an AI-based care system to reduce disparities in physical activity between urban and rural older adults and to promote health equity across regions. The findings may inform regional governments and community health centers in designing targeted interventions to reduce urban–rural health disparities among older adults. The results may serve as practical guidance for KDCA and local authorities in expanding evidence-based physical activity promotion and AI-driven community care services. National survey data such as the CHS may help support region-specific health policies for older adults.
Limitations
Several limitations of this study should be acknowledged. First, this study employed a cross-sectional design using secondary data from the Community Health Survey, which precludes causal inference between the identified factors and moderate-intensity physical activity. Although associations were observed, the temporal direction of these relationships cannot be determined. Therefore, longitudinal studies are warranted to clarify causal pathways and changes in physical activity patterns over time. Such approaches may provide a more comprehensive understanding of how physical activity behaviors evolve across different regional and social contexts.
Second, key variables, including physical activity, health behaviors, and psychosocial factors, were self-reported and may be subject to recall bias or social desirability bias. In particular, moderate-intensity physical activity was assessed based on respondents’ subjective perceptions, which may differ from objectively measured activity levels. Older adults may have difficulty accurately recalling the frequency or intensity of their physical activity, potentially resulting in over- or underestimation of actual activity levels. Future research incorporating wearable devices or objective activity monitoring could enhance measurement accuracy and reliability. Combining self-reported data with objective measures may further strengthen the validity of findings related to physical activity behaviors among older adults.
In addition, although this study comprehensively examined sociodemographic, health-related, lifestyle, and subjective health factors, some potentially relevant contextual variables such as neighborhood walkability, access to recreational facilities, and detailed indicators of digital literacy were not available in the dataset. These unmeasured factors may partially explain the observed regional differences in physical activity participation. For example, environmental conditions such as pedestrian infrastructure or access to green spaces may influence opportunities for regular physical activity regardless of individual-level characteristics. Future studies incorporating geographic or environmental indicators may provide a more comprehensive understanding of structural factors associated with physical activity among older adults.
Finally, while this study highlights implications for AI-based community care systems, the analysis did not directly evaluate the effectiveness of specific digital or AI-driven interventions. Future studies should integrate intervention-based or experimental designs to assess how AI-enabled monitoring and personalized feedback may improve physical activity engagement among older adults, particularly in underserved rural settings. In addition, factors such as technology acceptance, digital competency, and accessibility to digital devices may influence the effectiveness of AI-based interventions and should therefore be considered in future research. Experimental or longitudinal studies evaluating AI-integrated community care programs would provide stronger evidence regarding their practical applicability and scalability.
Footnotes
Acknowledgments
The author gratefully acknowledges the Korea Disease Control and Prevention Agency (KDCA) for providing access to the 2024 Community Health Survey data. The author also appreciates the efforts of the local public health centers and survey personnel involved in data collection.
Ethical Considerations
This study was exempt from institutional review board (IRB) review because it involved the analysis of publicly available, de-identified secondary data from the Community Health Surveys (2024). This study was conducted using publicly available secondary data provided by the Korea Disease Control and Prevention Agency (KDCA). The data are fully anonymized and collected under the national law (Regional Public Health Act, Article 4). Therefore, this study was exempted from institutional review board (IRB) approval according to Article 2, Paragraph 2 of the Enforcement Rule of the Bioethics and Safety Act of the Republic of Korea.
Author Contributions
Eun Gyo Son conceived and designed the study, performed the data analysis, interpreted the results, and drafted and revised the manuscript. The author approved the final version of the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.