
Abstract
Despite a recent decrease in the U.S. prison population, the proportion of offenders who might classify as elderly has increased exponentially during the same period—the likes of which have created new challenges for administrators tasked with the supervision of, and provision of resources to, this demographic. We review the current literature regarding functionality assessments for elderly inmates to highlight the difficulty associated with using existing instruments that are not specifically designed for the prison setting. We further argue that current efforts to identify elderly inmates are lacking, resulting in the potential misclassification of an already vulnerable group. We propose that future functionality assessments within correctional facilities incorporate a number of age-related factors that focus less on chronological age and more on the mental, physical, and social aging processes of incarcerated individuals.
The number of older inmates sentenced and housed in state and federal correctional facilities within the United States has precipitously increased over the last three decades. As recent data from the Bureau of Justice Statistics demonstrate, the number of state and federal inmates aged 55 or older increased by 250% from 1999 to 2014—a period during which the nation’s overall prison population dropped (McKillop & McGaffey, 2018; see also Fellner & Vinck, 2012; Human Rights Watch [HRW], 2012; Porter et al., 2016). Likewise, of the approximately 1.5 million adults currently housed in the state and federal system, those aged 55 and older constitute approximately 12%, which represents a 300% spike in the older population since the turn of the century (Ahalt et al., 2013).
Research also indicates that the number of older inmates will continue to rise over the next decade, particularly within states housing a larger proportion of the prison population. According to a 2012 report from the American Civil Liberties Union, the number of older prisoners is expected to eclipse 400,000 by the year 2030, representing a 4,400% increase since 1981 (ACLU, 2012). Similar patterns have been documented in other countries such as Canada and the United Kingdom; a pattern referred to by some scholars as the “graying of prison populations” (Aday, 2003; Kakoullis et al., 2010; Stoliker & Varanese, 2017). Despite this trend, older inmates remain an understudied population in the criminological literature; indeed, from an academic standpoint, they remain largely a “forgotten people” (Vito & Wilson, 1985). This is problematic for several reasons, three of which are addressed in this article.
The first reason is that older inmates represent a sizable, vulnerable group of individuals who pose unique budgeting challenges for prison administrators regarding the provision of basic amenities and resources, relative to their younger counterparts. This is especially true with respect to health care, and research shows that older inmates are particularly susceptible to chronic physical illnesses (e.g., dementia, cancer, arthritis, hypertension) and mental health disorders (e.g., depression, anxiety, nervousness; Aday, 2003; Barry et al., 2017; Williams et al., 2006). For example, older inmates average three chronic conditions and as many as 20% have been diagnosed with some form of mental illness (Mitka, 2004). Likewise, recent data from the Bureau of Justice Statistics regarding the medical problems of state and federal prisoners show that older inmates (over 50) are approximately 3 times more likely than younger inmates to have chronic conditions or infectious diseases while in custody (Maruschak et al., 2015).
These conditions often emanate from, and are exacerbated by, prolonged lifestyle choices such as smoking, drug and alcohol abuse, poor nutrition, and risky behaviors such as unprotected sex and needle sharing (Aday, 2003; Anno et al., 2004; Shimkus, 2004). Many of the aforementioned conditions are also often comorbid/co-occurring which, in turn, increases the probability of health care use by older inmates including, among others, services provided by pharmacists, X-ray and lab technicians, infirmary bedding, and 24-hr nursing coverage—all of which have proven costly for prison administrators across the country (Bishop & Merten, 2011; Chiu, 2010).
Reports also show that older inmates tend to incur higher per-inmate health care spending. For instance, recent estimates indicate that the cost of health care nationally for older inmates per year is 2–3 times higher than younger inmates (Luallen & Kling, 2014). Individual-level patterns among older inmates are further buttressed by macrolevel trends. A 2015 audit by the Department of Justice’s Inspector General revealed that, at the federal level, facilities with the highest proportions of older inmates spent approximately 5 times more per inmate on medical care (and 14 times more per inmate on medication), relative to facilities with the lowest proportions of older inmates (Office of the Inspector General, 2015).
Parallel observations have been made at the state level. In a 2014 joint report from the Pew Charitable Trusts and MacArthur Foundation, researchers found that of the 42 states surveyed, 40 witnessed a significant increase in the number of older inmates housed in their facilities; these states also tended to incur higher per-inmate health care spending. For example, median per-inmate spending was 37% higher among the 10 states with the largest share of inmates aged 55 and older, such as California and Texas, relative to the 10 states with the smallest share of older inmates (see also Hill et al., 2006).
A second and related problem is the way in which administrators define older inmates, the likes of which may intensify their preexisting vulnerabilities. As several scholars have noted, the concept of age is qualitatively different (i.e., “accelerated aging”) in the prison setting compared to the general population (Aday, 2003; Bingswanger et al., 2009; HRW, 2012). Yet, as we discuss in subsequent paragraphs, considerable variation exists between the various instruments used during the intake process to identify aging prisoners. For instance, the National Institute of Corrections defines inmates over the age of 50 as elderly or aging; a number that is considerably lower than its definition (65 years or older) among nonincarcerated populations, which is based on “chronological or numeric age” (Aday, 2003; Falter, 2006; Williams et al., 2006; Williams et al., 2009). Importantly, the disjuncture between, and ambiguity regarding, the respective definitions and the instruments they inform affects who is classified as older/elderly and who qualifies for the services and provisions afforded to this demographic.
A failure to classify an offender as older during intake can have dire repercussions in terms of their physical safety and psychological well-being. Several studies, for instance, indicate that older inmates are more susceptible to physical victimization at the hands of younger inmates (Stoliker & Varanese, 2017; see also Pare & Logan, 2011). This, in turn, can foster feelings of anxiety and insecurity as well as subsequent (mal)adaptive practices (e.g., avoidance behaviors) to avoid perceptions of weakness from other inmates (Stoliker & Galli, 2019). The extent to which elderly inmates are specifically targeted by their younger counterparts also creates challenges for the correctional staff who supervise them with respect to order maintenance and general prison safety (Steiner, 2008).
Third and finally, definitional ambiguity regarding the classification of older inmates ultimately hinders the scientific process that has characterized criminological research in recent decades. Indeed, the marked shift toward embracing evidence-based practice as a means of informing criminal justice is predicated on the replication of studies across time, various samples, and social contexts; the aims of which are hampered and compromised by inconsistencies across functionality assessments (McNeeley & Warner, 2015). Functionality for aging populations broadly refers to a “decreased ability to carry out everyday activities” (Algilani et al., 2014, p. 69). To this end, it is therefore necessary, from both a practical and policy perspective, to “take stock” of the extant literature regarding the assessments of elderly inmates used by correctional facilities as a means of determining “what works” in reducing adverse outcomes among vulnerable criminal justice populations (Cullen et al., 2009; Logan & Link, 2019).
We address the aforementioned issues in the following sections. First, we review the concept of age and how its definition has been (mis)applied by administrators in the prison setting. Next, we examine the various functionality and aging assessments that have been used in the past within the prison. Following this, we analyze newer assessments that measure aging and functionality through the lens of four domains from the gerontological literature, providing suggestions for future conceptualization within the prison. We conclude by exploring how improved functionality and aging assessments benefit correctional staff and older inmates, as well as how these tools can operate in concert with existing state and federal correctional policies and programs.
Managing Older Inmates: Definitional Issues and Challenges
Chronological Age and Inmate Status
Although there remains debate regarding how older inmates are classified in the prison setting, the definition of age is uniform outside of prison. Around much of the world, the classification of aging is based on the recognition that significant cognitive, physiological, and psychological decline is likely to occur around the age of 65 (Binswanger et al., 2009). This is one reason why the threshold for elderly/older status, according to the U.S. Census Bureau, remains at 65 years and why citizens in many societies become eligible to receive social security or full pension benefits upon turning this age. The general consensus regarding the definition of older age status has facilitated the development of instruments that reflect the general functionality of older persons without conflict or debate.
Conversely, the lack of consensus on who is considered elderly/older in prison remains an issue among practitioners and academics alike. For example, according to the National Institute of Corrections, elderly or older prisoners include anyone over the age of 50 (Duckett et al., 2000; Falter, 2006), while the National Commission on Correctional Health Care uses 55 as its threshold (Anno et al., 2004). Survey data also suggest discrepancies regarding a formal definition of older prisoners: Of the 27 states who explicitly classify “older prisoners,” 15 states use age 50 as the cutoff, 5 use age 55, 4 use age 60, 2 use age 65, and 1 uses age 70 (Sterns et al., 2008).
These inconsistencies are the by-product of some states relying solely on chronological age—setting a numeric marker for elderly populations based on the average age of onset of health problems—versus the use of instruments in assessing a degree of disability or health problem(s). Classifying inmates as older or elderly based on their chronological age can result in misunderstanding or underestimating the problems experienced by aging populations (Thivierge-Rikard & Thompson, 2007). As a result, the disagreement regarding older status inside (often 50–55) and outside of prison (65 and older) has created challenges among practitioners and administrators with respect to the issues of health care, housing, and geriatric-release decisions.
The most apparent and empirically supported explanation for this disparity is based on the general acceptance by correctional scholars of the accelerated aging process that often occurs within the inmate population (Binswanger et al., 2009; Chiu, 2010; Williams, Goodwin, et al., 2012). As Aday (2003) suggests, the effects of accelerated aging suggest that inmates over 50 maintain health profiles equivalent to persons outside of prison who are 65 and older; a rapid decline that has been attributed to unhealthy lifestyles, inadequate health care, and stresses related to incarceration.
Inmates remain a heterogeneous population, especially with respect to age. To this end, variations in length of prison term, preparedness for prison placement, and prior health and offense histories can drastically impact how older inmates fare in prison (Maschi & Aday, 2014; Maschi et al., 2015). The extent to which inmates are classified as “older” also determines in large part whether prison administrators are able to accommodate their unique needs (Williams et al., 2006). While indicators of inmate aging and health can give correctional staff a more nuanced view of the gerontological age of inmates, there is no formula or universally accepted assessment of elderly status in prison. In sum, while most correctional systems acknowledge that accelerated aging within the institution reduces the chronological threshold that defines age brackets outside of prison older status, it remains the primary indicator (Sterns et al., 2008).
Beyond Chronological Age: Toward an Integrative, Comprehensive Assessment
The tendency of correctional administrators to define older inmates based on their chronological age has been heavily criticized by the members of the medical profession as an incomplete, inaccurate marker of ability and impairment that omits important quality of life indicators (Haugebrook et al., 2010; Kouyoumdjian et al., 2017; Loeb & Abudagga, 2006; Williams & Abraldes, 2007). To this end, they posit that criminal justice practitioners and policy makers fail to acknowledge that age is a complex and multidimensional issue, one that is contingent on a litany of sociodemographic variables (Calasanti, 2010; Tinetti et al., 1995). For instance, gerontological approaches highlight four dimensions of aging, only one of which is chronological age. Others include indicators of biological, psychological, and social processes associated with aging and functionality.
Beyond chronological age, scholars recognize the need for understanding the biological implications of aging including, most notably, physiological changes such as diminished breathing capacity, elevated blood pressure, and mobility among older inmates (Khan et al., 2017). They also stress the importance of understanding the psychological changes that accompany the aging process. These include changes in, among others, mental functioning related to problem-solving, cognitive recall, and information processing (Hooyman & Kiyak, 2011). Finally, social aging refers to the roles and responsibilities of individuals in society that evolve over time. Throughout the life course, expectations for work and responsibilities change for aging individuals and the family members who care for them, sometimes resulting in anxiety related to the perceived loss of independency, freedom, respect and financial ability, health, and attractiveness (Nelson, 2011). Studies show that many of these fears are linked to the experience of discrimination (e.g., ageism) in society (see Azulai, 2014, for a review), a fear that may exacerbate many of the “pains of imprisonment” (Sykes, 1958).
An explicit focus on chronological age not only neglects the multifaceted nature of the aging process, it also ignores several factors that can either intensify (i.e., accelerate) or ameliorate its effects, including poverty, exercise, nutrition, and heredity, metrics which are particularly important in the prison setting and warrant a contextualized approach for understanding the specific needs of older inmates (Mathers, 2015; Williams et al., 2006). For instance, research indicates that the experience of aging among incarcerated women differs dramatically from their male counterparts. As Aday and Farney (2014) observed, the prevalence of mental health problems and chronic health conditions among older female inmates is significantly higher when compared to men of the same age and creates specific challenges in caring for older male and female inmates (see also Williams et al., 2006). Taken in combination with considerations of safety and care, these domains underscore the necessity of understanding not only the specific ailments, problems, and concerns of older inmates but also the importance of being able to pinpoint such issues to effectively allocate resources within the criminal justice system.
Method
As mentioned, many of the current assessments used to identify older prisoners fail to recognize the specific challenges they face daily (Williams & Abraldes, 2007). To determine the degree to which functionality assessments were (in)appropriate for use in prison, we used Google Scholar to review the medical and correctional literature on existing assessments (Edemekong et al., 2019). We utilized a variety of search terms, including combinations of the terms commonly used to refer to the incarcerated (e.g., prisoners, inmates, incarcerated), assessment (e.g., assessment, evaluation, functionality), and aging to identify relevant research. We found that several hundred assessments exist to capture functionality across a variety of domains, including those associated with emotional, cognitive, and physical processes (Applegate et al., 1990; Skarupski et al., 2018). For the sake of parsimony, however, we focus on assessments that are widely used (Wales et al., 2016) to illustrate the primary limitations of relying on existing instruments that were not designed for inmates (Taxman et al., 2007), with a specific focus on the psychometrics incorporated into each. To this end, we also suggest the incorporation of various items as a means of improving existing instruments; metrics that gerontologists have long suggested should be included in the assessment of risk and decline among older inmates (Hooyman & Kiyak, 2011).
Defining Functional Capacity
Understanding how functionality is defined, conceptualized, and measured is critical to the development of appropriate age and functionality assessments within prison. We adopt Millán-Calenti and colleagues’ (2010) definition, who note that “functional capacity refers to the possibility and ability to carry out the daily activities in a normal or accepted way” (p. 306). For older inmates, maintaining a level of functional capacity can be an important indicator of overall health, the loss of which can lead to a rise in illness, disability, and mortality (Stuck et al., 1999).
Functional capacity in prisons has traditionally been measured by two of the most popular functionality tools, the activities of daily living (ADL) assessment (Katz et al., 1963) and the instrumental activities of daily living (IADL) assessment (Bernstein & Munoz, 2016; Lawton & Brody, 1969). Both were created to determine whether the daily routines of individuals can be accomplished independently (i.e., without the aid of someone else). The ADL is oriented toward activities of self-care and includes basic questions on bathing and food preparation, while the IADL includes a broader range of activities such as shopping, housekeeping, and financial activities. Although the ADL is ultimately an assessment of functional capacity and independence, its applicability to older inmates in prison is limited and oxymoronic because, as scholars have previously noted, correctional facilities are “total institutions” whereby all elements of life are closely monitored (Logan et al., 2017; Logan & Pare, 2016; see also Goffman, 1968). Likewise, many of the activities listed on the IADL—such as handling finances, doing laundry, or taking correct medications and amounts—are largely irrelevant to the inmate population.
Indeed, the ADL and IADL fail to capture the “…multifactorial health conditions that occur when the accumulated effects of impairments in multiple systems render [an older] person vulnerable to situational challenges” (Inouye et al., 2007, pp. 2–3). These include concerns germane to inmate life such as isolated showering and feeding as well as social interactions with guards and other inmates, all of which are in the absence of supplemental care typically provided outside of prison. One of the most significant concerns is the issue of conceptualizing functional capacity and disability through instruments originally designed for other settings (Katz et al., 1963; Lawton & Brody, 1969). Perhaps even more problematic is the fact that the level of impairment determined by the ADL uses dichotomous scoring and misses a substantial amount of variation with respect to various ailments or conditions. Such coding strategies are also particularly useful (and are often preferable over binary measures) regarding empirical assessments and the validity of these instruments (see Britt & Weisburd, 2010).
In an effort to reconcile these weaknesses, Williams and colleagues (2006) measured the functional capacity and impairment of older inmates in California using an adapted version of the ADL with measures specifically designed for prison functionality. Referred to as the prison activities of daily living (PADL) assessment, this instrument includes items that tap challenges unique to aging inmates such as dropping to the floor for alarms, hearing orders from staff, climbing onto the top bunk, and standing for count. Importantly, this assessment was designed specifically by prison experts. All five activities were chosen as the most commonly required activities for inmates on a daily basis. While the PADL addresses prison functionality, it is limited in the gerontological domains of aging (Williams et al., 2006), and methodological concerns remain with respect to many of the health problems associated with accelerated aging that confront older inmates (Aday & Farney, 2014; Rakes et al., 2018). These include, among others, biological and psychological impairments that are unrelated to physical tasks performed in prison. While the improvements of the PADL are noteworthy and mark a compelling evolution in the use of functionality and aging assessments in prisons, a more nuanced evaluation of the specific domains of aging and functionality must be considered when evaluating an inmate’s true age and health status.
Improving the Measuring of Functional Ability and Older Status in Prison
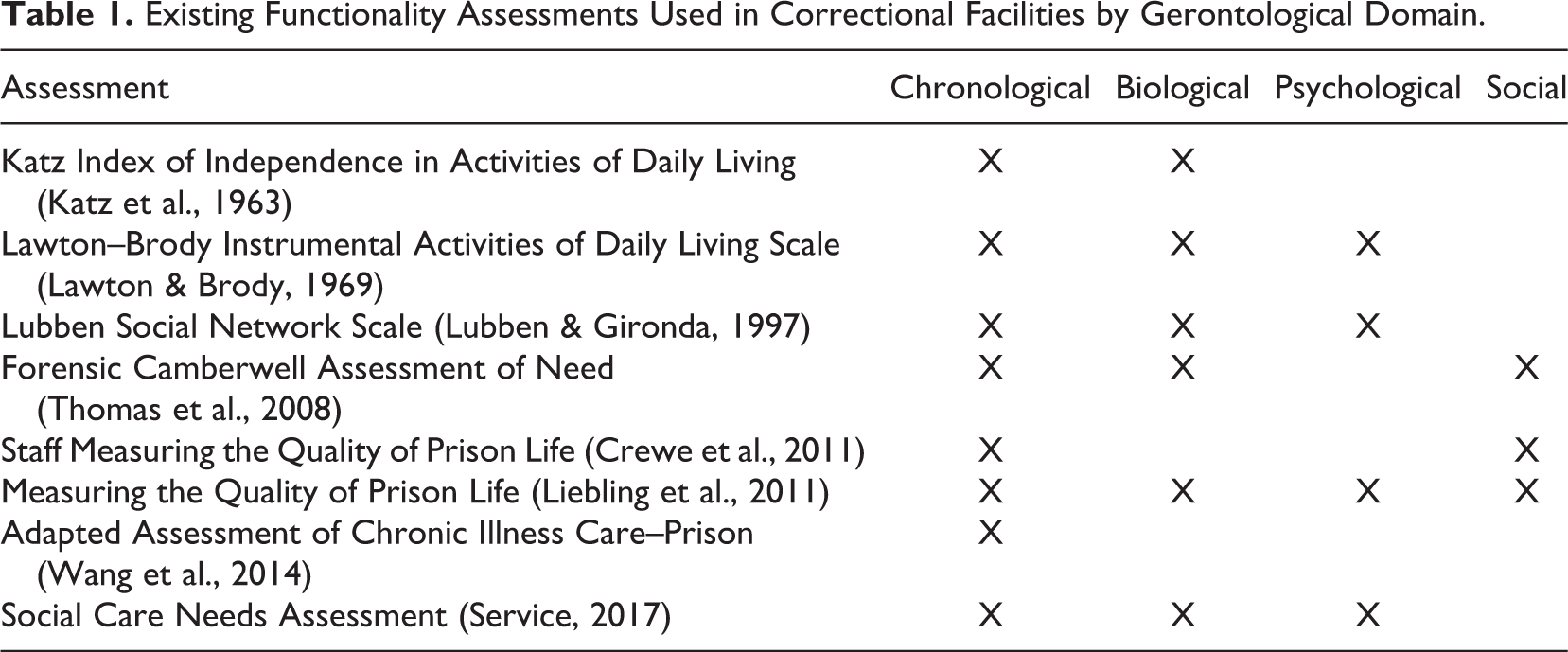
As Table 1 demonstrates, more recent functionality assessments attempting to “fill the gaps” left by the ADL, IADL, and PADL have begun to address more than physical functionality and aging, instead focusing on indicators of biological, psychological, and social aging, as well a host of geriatric syndromes that manifest in each domain. This is based on the general acceptance that chronological age fails to fully reflect the true aging process nor does it take into account that individuals experience aging idiosyncratically (i.e., accelerated aging in prison; Kotter-Grühn et al., 2016). Recognizing these more nuanced domains of aging is vital in assessing overall functionality and health and assisting in making more informed health care decisions for older inmates. For example, studies have shown that impairment in even one of these domains can leave individuals vulnerable to illness and injury (Bavafa & Mukherjee, 2019; Joynt & Bishop, 2018) and complicate already existing challenges for correctional staff within these facilities (Stibich, 2015). Using a more complex and nuanced assessment of aging offers the opportunity to not only assist correctional staff in understanding the individual health issues of older inmates but also to develop a more well-rounded measurement tool of functionality.
Existing Functionality Assessments Used in Correctional Facilities by Gerontological Domain.
Addressing biological markers of aging and functionality
The gerontological literature suggests that problems unique to older inmates, such as accelerated aging, are best understood by assessing disparities between biological and chronological indicators (see Khan et al., 2017). This is illustrated by the fact that inmates are much more likely to experience age-related health problems which begin to occur 10–11 years earlier, relative to the general population (Reimer, 2008; Spaulding et al., 2011). Chief among these issues are diminished breathing capacity and elevated blood pressure, not captured in any of the existing measures for incarcerative setting (Hooyman & Kiyak, 2011).
More recently, markers associated with biological aging have been analyzed in medical studies to determine the subjective age of patients. Some of these include an individual metrics of disease burden, grip strength, pulmonary and muscular functions, and waist circumference (Kotter-Grühn et al., 2016). Scales that tap biological mechanisms can provide correctional staff and health care providers with a more in-depth interpretation of the causes of impairment rather than a cursory observation of the effects. While it may not be feasible or appropriate to use every known biological measure of aging and functionality in an improved assessment, acknowledging the research and the plethora of measures to capture biological aging is a first step in the creation of such instruments. For instance, the functional independence measure includes indicators of aging, such as bladder and bowel management (Zidén et al., 2008). Similarly, the Fulmer Spices assessment of aging includes indicators of biological aging, including skin breakdown (Fulmer, 1991).
Addressing psychological markers of aging and functionality
Elderly offenders may also experience significant stress and psychological trauma upon entering prison, especially those considered “first-timers” (Williams & Abraldes, 2007). Manifestations of psychological stress include feelings of acute or general anxiety and depression and may stem from the fact that older prisoners may give up hope regarding their release and subsequently lose contact with the outside world (Aday, 2003; Crawley & Sparks, 2006). Anxiety and depression may also contribute to the accelerated aging process with respect to other components of psychological aging in prison, including elderly inmates’ problem-solving abilities, cognitive recall, and the ability to process information, all of which have been evaluated by a plethora of assessments such as the Caregiver Assessment of Function and Upset, Klein–Bell Activities of Daily Living, and Nottingham Extended Activities of Daily Living (Hooyman & Kiyak, 2011; Martin et al., 2013; see Table 1).
In addition to the measures of psychological aging, the measures of psychological function and mental health are of primary concern within the older population. In fact, using the Kessler Psychological Distress Scale, Baidawi and colleagues (2016) found that older inmates are disproportionately distressed with self-reported safety, prison victimization, perceived social support from staff and inmates, current employment, and level of exercise. In addition, older inmates who exhibited low PADL scores were significantly more likely to be depressed or experience suicide ideation (Barry et al., 2017). These findings further complicate the already complex task of measuring “functional capacity” since daily activities like being employed and/or exercising can generate psychological distress that may prohibit older inmates from feeling comfortable and safe in their surroundings, leading to psychological issues like depression and suicide ideation. Currently, the measuring, the quality of prison life (MQPL) assessment captures a psychological well-being, including items about prisoner perception of psychological safety (Liebling et al., 2011).
Addressing social markers of aging and functionality
Gerontologists classify social functionality to include the invariable shift in the roles and relationships individuals serve in relation to their family and social world as they age. These roles and responsibilities can change even more drastically within the prison, as this setting may provide more limited adaptations for functional decline due to cost or institutional safety concerns (Aday, 2003, 2006; Prison Reform Trust, 2008). Perhaps the most well-studied area of social functionality and aging is the correlation between age and fear of victimization in prison (Aday, 2003; Kerbs & Jolley, 2007; Krabill & Aday, 2005; Trotter & Baidawi, 2015; Williams et al., 2006). Regardless of whether or not older inmates are actually victimized more often (the research is conflicted), the fact remains that fear of victimization (psychological domain) often results in lack of social engagement and feelings of isolation (Dawes, 2009; Snyder et al., 2009).
This overlap between domains is illustrative of why it is crucial to measure all elements of functionality and impairment; as in this example, measures of psychological fear of victimization can influence measures of social engagement and feelings of isolation. Indicators of personal safety and fear of victimization are found in the MQPL assessment. Indicators of social functionality include scales tapping financial literacy, such as management of day-to-day finances (Lawton & Brody, 1969). Existing assessments also measure social connectedness to family and friends by asking questions about the frequency of contact with others, measured through instruments such as the Forensic Camberwell Assessment of Need (Thomas et al., 2008) and the Quality of Life Assessments (Staff Measuring the Quality of Prison Life and MQPL; Crewe et al., 2011; Liebling et al., 2011).
Addressing geriatric syndromes
Many of the nuanced difficulties that are common among older inmates are referred to as “geriatric syndromes,” impairments that increase the risk of experiencing negative outcomes during their incarceration (Heidari et al., 2017; Williams et al., 2014; Williams et al., 2009). The term is not mutually exclusive from the aforementioned functionality domains; rather, geriatric syndromes encompass a variety of afflictions that occur across, and overlap with, indicators of biological, psychological, and social functionality. Within the biological domain, for example, older inmates are particularly susceptible to vision and hearing impairment issues, which greatly increase their dependence on staff to avoid falls, social isolation, and depression (Landefeld et al., 2004; Williams & Abraldes, 2007). The risk of falling is also associated with an increased risk of serious injury, further loss of function, increased nursing home placement, and death. This is an understudied area in the existing prison assessments we examined. Other issues that may go undiagnosed among older inmates include urinary incontinence (the biological domain), delirium, and dementia (psychological domain; Inouye et al., 2007; Williams et al., 2006).
Research suggests that symptoms that characterize a number of geriatric syndromes such as frailty, delirium, dementia, and bladder incontinence are often undiagnosed in the general population (Inouye et al., 2007) and, given the structure and content of the aforementioned assessments, are likely to go unnoticed in prison. Not surprisingly, the extent to which symptoms remain undiagnosed (or are exacerbated because of their neglect) can have significant repercussions for inmates, including an increased risk of morbidity, mortality and treatment costs; both of which should serve as incentives for correctional staff with respect to the general order maintenance of facilities (Barry et al., 2017; Hollenbeak et al., 2015; Kerbs & Jolley, 2009; Stibich, 2015).
While many of these more recently developed assessments target specific gerontological domains of aging, they lack a comprehensive evaluation of all four. In addition, many of the aforementioned assessments provide basic information about the abilities and functionality of the aging but fail to address the unique and complex needs facing aging prisoners (Rosen & Reuben, 2011). Table 2 provides a list of functionality and aging assessments commonly used inside and outside prison that have attempted to measure these processes over time. To our knowledge, no existing assessments of aging designed for use in correctional facilities address prison-specific functionality, while also addressing all of the necessary domains identified by gerontologists.
Characteristics of Popular Functionality and Aging Assessments.
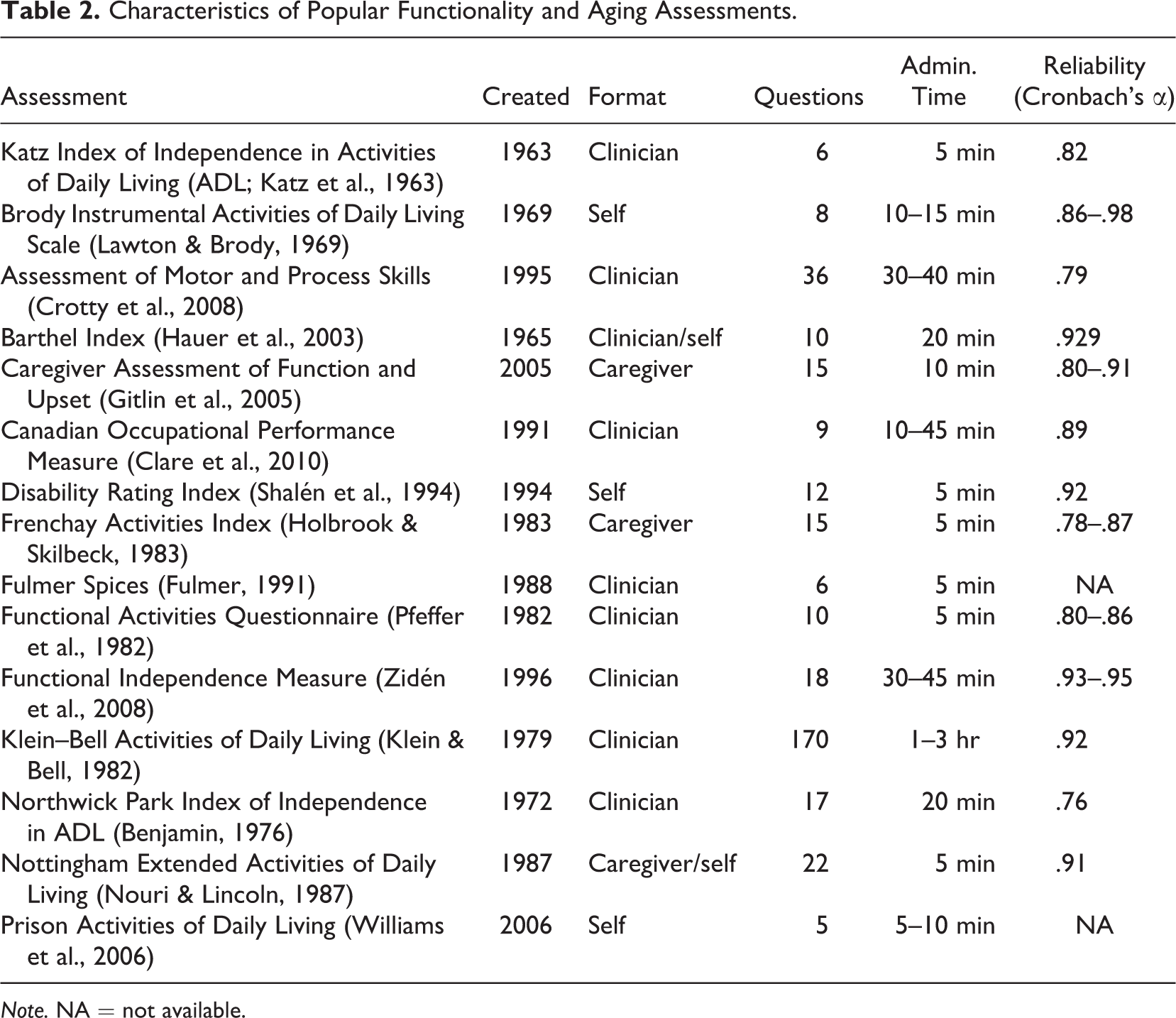
Note. NA = not available.
Discussion
Characteristics of an Improved Functionality and Aging Assessment
The creation of improved assessments that measure the unique challenges of aging inside prisons would be a significant step forward in meeting the needs of older inmates. In order to do so, however, a comprehensive evaluation of aging must include multiple factors. First, it must consider the complex problems—above and beyond the four gerontological domains—associated with aging that are often overlooked in traditional assessments, such as geriatric syndromes. For instance, a revised instrument might include questions about frailty, symptoms of incontinence, issues of balance or instability, and issues associated with diet and feeding deemed too minor by physiological or medical assessments (Hooyman & Kiyak, 2011). Capturing these concerns and potential problems before they are exacerbated offers correctional staff the opportunity to decrease cost and time associated with addressing more serious problems.
Second, a comprehensive assessment must account for the specific challenges that are the characteristic of the prison environment. As previously mentioned, many prison administrators have historically relied on functionality assessments—such as the ADL and IADL—that were not intended for use in the prison population (Katz et al., 1963; Lawton & Brody, 1969) and which fail to account for the contextual nuance of this setting. For instance, one of the items included in the ADL refers to the ability to prepare food—an activity not afforded to the majority of inmates. Similarly, the IADL includes questions about handling money and finances, which is irrelevant to prisoners who have little or no access to money. Instead of asking whether an inmate can handle money independently, a more appropriate indicator might ask about the management of funds through the inmate’s commissary account. Likewise, instead of asking about the ability to manage travel through public transportation, a more appropriate question might ask about the inmate’s ability to move between locations within the prison without assistance or in a timely manner (since inmates are often limited in the time they are allotted for getting from one location to another).
Third, the current approach to assessing activities of daily living included in the ADL is based on dichotomous measures of functionality, indicating that those assessed either do or do not have problems. As noted previously, this approach is inherently limited because it ignores important variation that may exist with respect to several measures/symptoms associated with aging. Functionality is better determined using a graduated or continuous scale—one that allows correctional staff to determine the extent to which prisoners are able to complete tasks rather than whether or not they are able to complete activities. In doing so, staff have the opportunity to address potential or minor problems before they become costly and much more involved.
Lastly, in an effort to save cost and improve efficiency, improved functionality assessments should be able to assist in alleviating multiple burdens placed on older inmates and correctional staff. It is well known that the primary purpose of a prison is to incapacitate, as opposed to treat and rehabilitate inmates in a cost-effective manner; yet research suggests that the two are not mutually exclusive. Legal and moral arguments for appropriate health care in prisons are based on Eighth Amendment protections from the U.S. Constitution (including cruel and unusual punishment), requiring that prisoners have timely access to an appropriate level of care for serious medical needs. In a 2012 meeting to propose a policy agenda to improve the care of older prisoners, 29 national experts in correctional health care, academic medicine, nursing, and civil rights convened and identified 9 priority areas to be addressed (Williams, Stern, et al., 2012). Of the nine areas, seven could be directly affected and improved by more appropriate functionality assessments. These included issues relating to the definition of the older prisoner, correctional staff training, definition of functional impairment in prison, geriatric housing units, issues for older adults upon release, medical early release, and prison-based palliative medicine programs. By understanding an older inmate’s “true age” and actual level of functionality, more informed decisions can not only assist in the correct placement of inmates into geriatric units but also aid in reentry. Furthermore, improved assessments can ease the burden of correctional staff by removing the clinical diagnosis requirements from those not trained in health care–related fields.
Functionality and Aging Assessments in Concert With Correctional Policy
As the U.S. prison population continues to age, the need for consistency in the treatment and supervision decisions of older inmates becomes increasingly important. Currently, differences in sampling, definitions, and measurement render comparisons between assessments problematic at best and unattainable at worst (Fazel et al., 2001; Trotter & Baidawi, 2015). To this end, a shift toward uniform assessments will yield benefits for both staff and inmates alike by aiding in the decision-making process and establishing “what works” in the managing of older inmates. Indeed, prison functionality assessments fulfill a major requirement of evidence-based practices: an actuarial assessment tool that can be objectively measured with the goal of delivering more targeted services. A significant advantage of uniform assessments is the ability of evaluators to attribute differences in results to the individuals being assessed rather than to the instrument of measurement. By holding the instrument constant, focus and attention can be given to the subject of study without concerns of validity. If uniform assessments are successfully employed in a variety of correctional settings, the true functionality and age of elderly inmates will be more accurate, allowing for more informed correctional staff and health care providers. This is especially true regarding the instrument’s use to establish best practices for the delivery of health care and housing considerations for older inmates—the likes of which should strike a balance between cost-effectiveness and necessary treatment.
One established solution to reducing costs while simultaneously providing care for elderly inmates is the early release of particular elderly inmates (see Chiu, 2016). Indeed, elderly inmates have greater access to services outside of state and federal correctional facilities that may contribute to an improved quality of life (Ahmed & Siegler, 1997). While the release of specific inmate populations may be untenable due to sentencing restrictions, older inmates are generally less likely to recidivate (Rakes et al., 2018; Steffensmeier et al., 1989), violate parole, or be reincarcerated (Williams & Abraldes, 2007). For the terminally or mentally ill, compassionate or medical release policies have been formally adopted in over 80% of states (Aday & Krabill, 2012; Anno et al., 2004; Chiu, 2010). Although each state varies in the criteria used to determine eligibility for release, most consider characteristics that are indistinguishable from risk assessments measuring recidivism such as remaining sentence length, projected life expectancy, prior criminal history, and evidence of future residency (Aday & Krabill, 2012).
It may be possible, then, for functionality assessments to operate in concert with early release risk assessments as a means to determine how and where eligible inmates are released. For example, inmates with chronic diseases may be referred to residential centers that are within close proximity of appropriate health care facilities. Elderly parolees with severe physical limitations may also be referred to residential centers with greater handicap access or transportation services. Correctional authorities may even develop new supportive services for inmates without family, friends, or nursing homes willing to accept them back into the community in an effort to protect against homelessness (Williams et al., 2010). Assistance in alleviating these stressors may reduce risk of recidivism and cost for correctional systems, while also increasing the individual’s chances for successful reintegration into society.
While some states like Texas have made concerted efforts to ensure that medical or geriatric release is streamlined (see Chiu, 2010, for a review), audits and reviews of this consolidated approach have previously cited lack of resources and legislative restrictions as barriers to this shared system. We posit that as the necessity for more efficient and collaborative relationships between and among various criminal justice agencies continues to develop, uniform functionality assessments will be an essential component of release decisions.
Another method by which improved functionality assessments can assist correctional staff in making informed decisions stems from the use of geriatric prisons or specialized, segregated housing units for the older offenders. Research shows that when health declines with age, most inmates report a desire and willingness to move into segregated units (Marquart et al., 2000)—a decision often influenced by the fear of victimization from younger inmates (Aday, 2003). Functionality assessments can operate in concert with specialized housing units designed with adaptive aids like ramps, nonslip surfaces, or grab bars to cater to the individual functionality needs of inmates within these spaces. Conversely, removing elderly inmates from the general population may remove the positive influence that they have on their younger counterparts (Mara, 2003) or even encourage social isolation or boredom. In either case, improving the accuracy of functionality assessments within prisons will give correctional staff valuable information on the individual needs of elderly inmates and can assist in determining eligibility for specialized housing in the future.
Conclusion
A more comprehensive method for understanding and addressing the needs of older inmates is necessary to deal with the aging population within correctional facilities. The ability to adequately define who should be included in this group is the first step in approaching a clearer understanding of this population. Such efforts are dependent on the development of accurate assessments targeting the many facets of the accelerated aging process. Further, these facets must be explored while taking into consideration the challenges and unique conditions presented by correctional facilities. Without a comprehensive assessment, addressing the needs of older inmates and the challenges they routinely face will become increasingly difficult. Improved functionality assessments also offer facilities a method to better understand and address the needs of the aging prior to such problems occurring, alleviating many of the financial and temporal strains associated with these issues. These problems are beyond the scope of the extant research and can be addressed using more thorough and appropriate assessments in the future.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.