
Abstract
Healthcare waste should be managed carefully because of infected, pathological, etc. content especially in developing countries. Applied management systems must be the most appropriate solution from a technical, environmental, economic and social point of view. The main objective of this study was to analyse the current status of healthcare waste management in Turkey, and to investigate the most appropriate treatment/disposal option by using different decision-making techniques. For this purpose, five different healthcare waste treatment/disposal alternatives including incineration, microwaving, on-site sterilization, off-site sterilization and landfill were evaluated according to two multi-criteria decision-making techniques: analytic network process (ANP) and ELECTRE. In this context, benefits, costs and risks for the alternatives were taken into consideration. Furthermore, the prioritization and ranking of the alternatives were determined and compared for both methods. According to the comparisons, the off-site sterilization technique was found to be the most appropriate solution in both cases.
Keywords
Introduction
Healthcare waste materials include a larger portion of infectious wastes, which are potentially dangerous since they may contain pathogenic agents. The production of these waste materials will continue to be an on-going phenomenon as long as there are human activities (Abdulla et al., 2008; Birpınar et al., 2009). Safe management of healthcare waste is necessary, to avoid environmental and public health problems, especially related to transmission of infectious diseases, such as HIV infection and hepatitis. In this respect, healthcare waste producers should develop waste management plans to minimize the risks and overall management cost (Graikos et al., 2010).
Recently, a number of studies have focused on healthcare waste management practices in Turkey. Birpınar et al. (2009) carried out a survey about the current status of the generation, collection, on-site handling, storage, processing, recycling, transportation and safe disposal of healthcare waste through interviews made with healthcare services managers. Alagöz and Kocasoy performed a survey study of healthcare waste in Istanbul Metropolitan Region and discussed the optimum healthcare waste management system for Istanbul (Alagöz and Kocasoy, 2007, 2008).
There have been many studies about healthcare waste generation and composition in different countries or cities (Cheng et al., 2010; Graikos et al., 2010) and healthcare waste management (El-Salam, 2010; Jang et al., 2006; Mato and Kassenga, 1997; Taghipour and Mosaferi, 2009). In addition, there are several studies that have used decision-making techniques for healthcare waste management. Brent et al. (2007) used the life cycle management and analytical hierarchy process (AHP) for choosing a healthcare waste management system, Karagiannidis et al. (2010) used the AHP and Dursun et al. (2011) used a fuzzy approach. For the selection of healthcare waste disposal firms, Hsu et al. (2008) and Ho (2011) used AHP and fuzzy AHP, respectively. Karamouz et al., (2007) used an AHP in order to rank the hospitals and determine the share of each hospital in the total hospital solid waste pollution load.
In the present study, healthcare waste treatment/disposal alternatives were evaluated by two different multi-criteria decision-making (MCDM) techniques. Unlike other studies in the literature, the analytic network process (ANP) and ELECTRE, which are techniques that have different approaches, were used for healthcare waste management systems. The paper is organized as follows. In the next section, the current status of healthcare waste management in Turkey is briefly introduced. The problem is defined and solved using a spreadsheet evaluation tool for ELECTRE III and Super Decisions software prepared by Creative Decisions Foundation for ANP in the following section. The results for both methods are presemted in the next section and concluding remarks and recommendations are given in the final section.
Present situation of healthcare waste management in Turkey
The Healthcare Waste Control Regulation, which is the regulation that is related to healthcare waste management in Turkey, was published in May 1993 and this regulation was changed in July 2005 in accordance with the EU Directives. It clarifies the principles of healthcare waste management which include the collection, transportation and temporary storage in healthcare facilities, and the treatment and final disposal of healthcare waste (Turkish Ministry of Environment and Forestry, 2005).
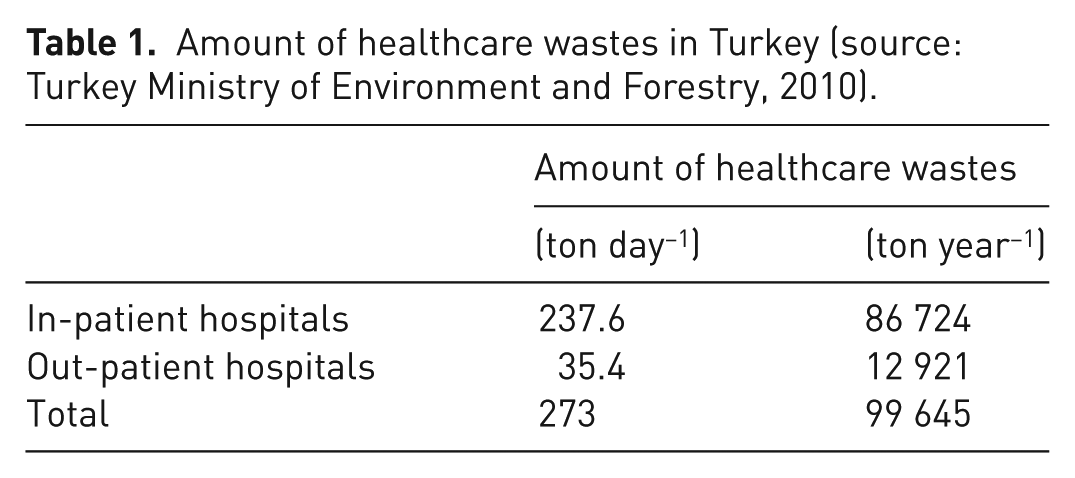
In 2010, a status report related to healthcare waste (its new name is Ministry of Environment and Urbanism) was published (Turkish Ministry of Environment and Forestry, 2010a). According to this report, the total number of hospitals in Turkey is 1328 and the number of beds in use is 175 141. As a result of calculations made according to provinces considering the bed occupancy ratio, inpatient and outpatient healthcare establishments generate a daily amount of 273 tons and an annual amount of 99 645 tons of healthcare waste. The daily total is shown in
Amount of healthcare wastes in Turkey (source: Turkey Ministry of Environment and Forestry, 2010).
To ensure the safe management of healthcare waste, a circular was published in 2006, which supported the use of healthcare waste sterilization systems. Furthermore, according to the Regulation on the Storage of Wastes (Turkish Ministry of Environment and Forestry, 2010b) landfilling of healthcare waste materials that have not been subjected to any pre-processing is prohibited. At present, there are 17 sterilization facilities and 33 648 tons of healthcare waste representing 34% of the total was sterilized. Furthermore, there is one incineration facility for healthcare waste in İstanbul. The current status of healthcare waste in Turkey is given in Figure 1.
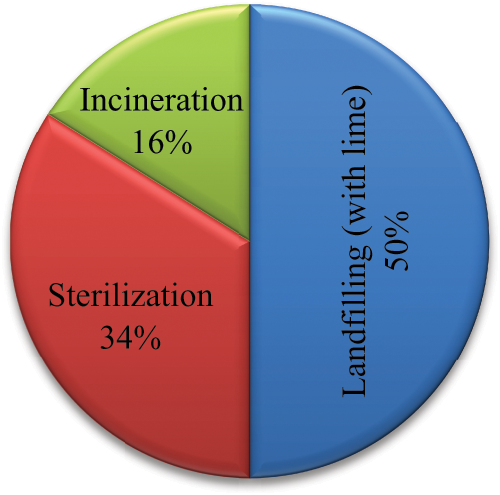
The current status of healthcare waste treatment/disposal in Turkey.
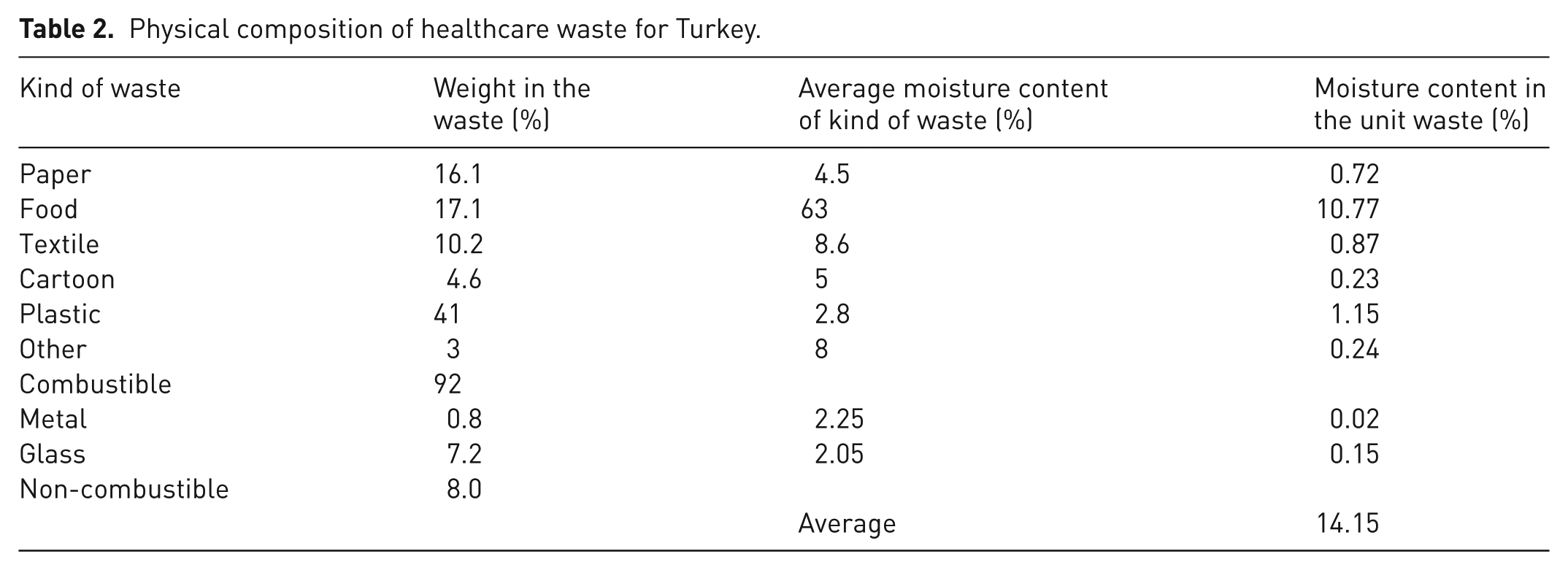
In 2008, a study was performed by Alagöz and Kocasoy for İstanbul Metropolitan Area. According to the results of this study, the percentage distribution of the composition of healthcare waste generated in the institutions of the Istanbul Metropolitan Area was determined to be 46% domestic, 17% infectious, 16% recyclable, 8% pathological, 5% sharps, 4% pharmaceuticals, 3% pressurized and 1% radioactive (radioactive wastes are handled by the Atomic Energy Commission according to the related regulations) (Alagöz and Kocasoy, 2008). Another study related to healthcare waste composition in Turkey was carried out by Altın et al. (2003). The results of the study are given in Table 2.
Physical composition of healthcare waste for Turkey.
Methodology
In the present study, two MCDM methods were employed: ANP and ELECTRE III. The alternatives and criteria – which were the same in both cases – were set out initially, followed by the MCDM methods. A flow diagram of the study is given in Figure 2.
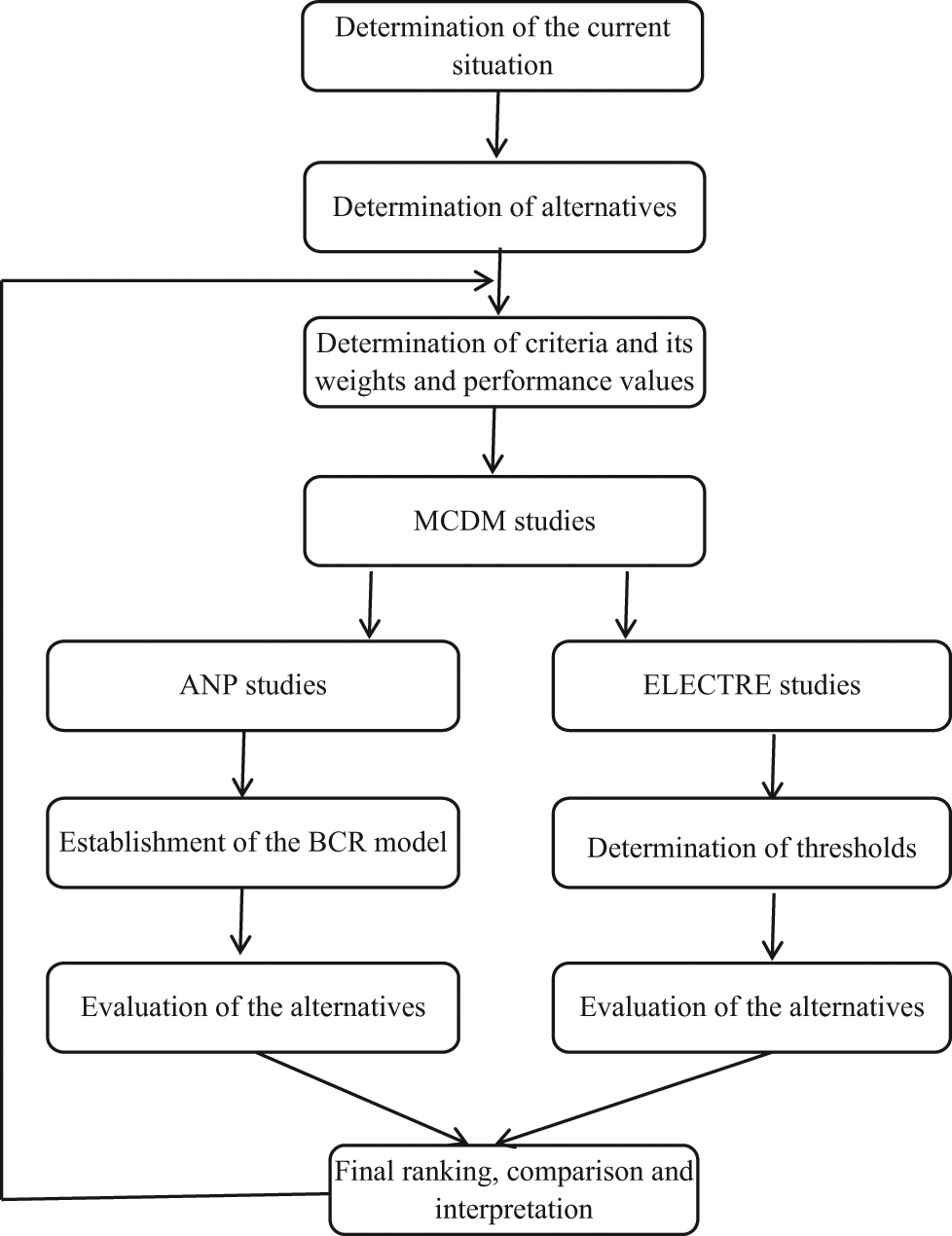
The flow diagram of the study.
Alternatives
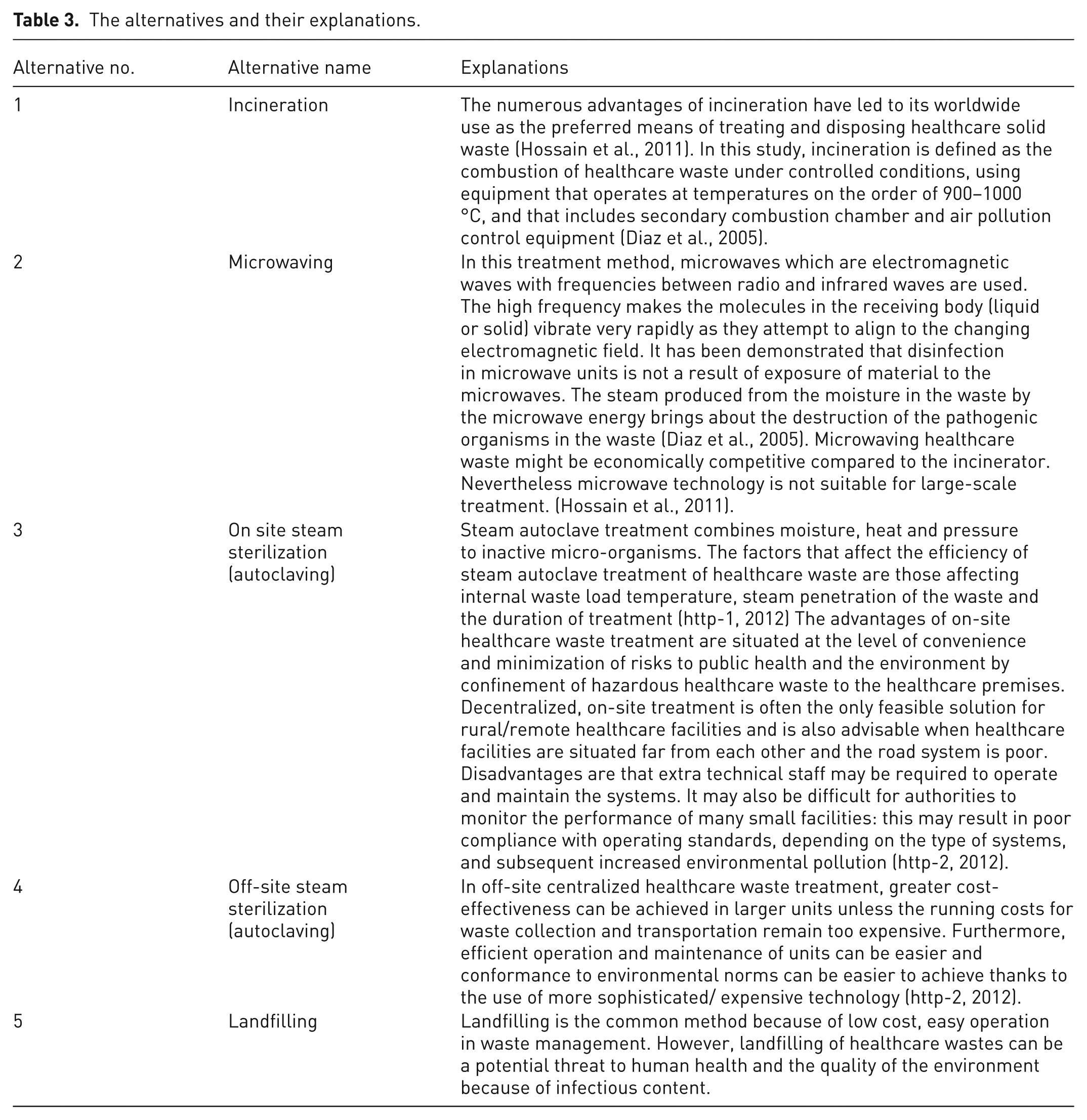
The alternatives were selected for evaluation within the frame work of the present study, after a survey of the relevant literature on contemporary technologies which is summarized in Table 3. In this context, the following five alternatives, namely incineration, microwaving, on-site steam sterilization, off-site steam sterilization and landfilling were determined. Explanations of these alternatives are also given in Table 3.
The alternatives and their explanations.
Criteria
The criteria used in this study are given in Table 4, in which the number and name of these criteria are specified for further MCDM applications. The same criteria were determined for ANP and ELECTRE III. In addition, for the ‘benefit opportunity cost risk’ analysis in ANP, the criteria were classified as benefit, cost and risk. For ELECTRE III studies, the units of the quantitative criteria and the scores for the qualitative criteria are given.
The criteria for ANP* and ELECTRE III applications.
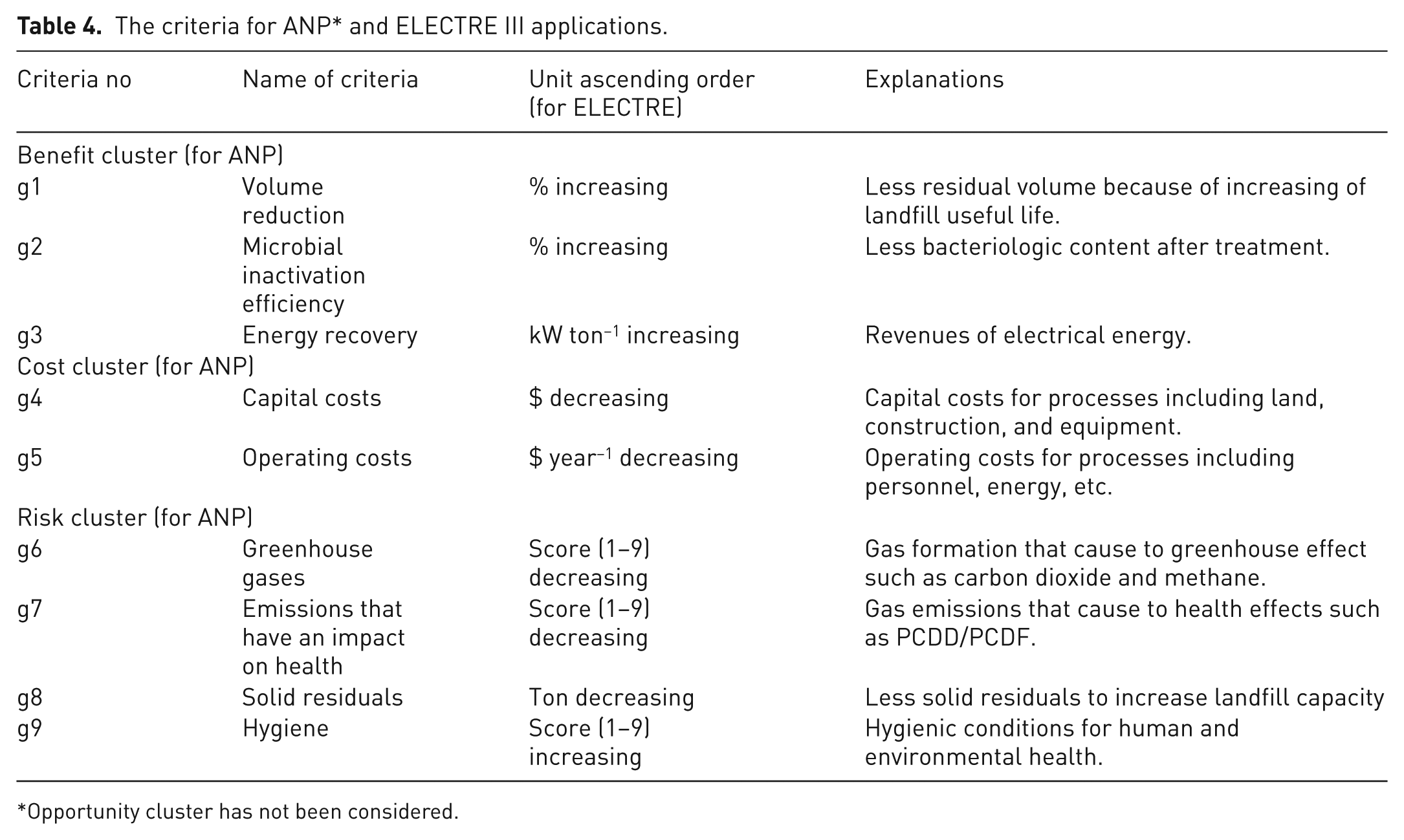
Opportunity cluster has not been considered.
Multi-criteria decision-making studies
Choosing the best alternative among a finite number of alternatives according to the given criteria is the focus of MCDM, which is a developing research area (Vincke, 1992). There are several methods used to solve MCDM problems, such as goal programming, AHP, ANP, PROMETHEE, TOPSIS, and ELECTRE (I, II, III, IV,TRI) (Figueira et al., 2005). Although these methods have been used in several disciplines, as well as in environmental engineering, ELECTRE and ANP were chosen for use in this study. ELECTRE III is one of the multi-objective ranking methods based on outranking relations. Indifference, weak preference, strong preference, and incomparability are used for the extended model of the decision maker’s local preferences in ELECTRE III (Zak, 2005). ANP, which is another MCDM method, is based on the utility function that aggregates different criteria (points of view) into one global criterion. The difference between ANP and ELECTRE is incomparability among the alternatives; specifically, ANP eliminates incomparability between alternatives, whereas ELECTRE III takes it into account. Hence, ELECTRE III and ANP were utilized in this study because of their different viewpoints.
ANP and ELECTRE III were used to choose the most suitable healthcare waste treatment/disposal system with particular regard to developing countries. In the present study, five alternatives and nine criteria were developed and evaluated by means of ANP and ELECTRE III. Super Decision software was used for ANP and MS Excel and VBA were used for ELECTRE III. Finally, the results obtained were compared and interpreted.
In MCDM studies, it is very important to define the decision maker. This may be one person or a group of people (e.g. a committee), who make the final choice among the alternatives. The decision maker(s) should have sufficient knowledge and experience to apply the decisions. In the determination of a healthcare waste treatment/disposal system, municipal authorities and academic staff were considered to be the decision makers in this study.
ELECTRE III studies
ELECTRE III, which was developed by Bernard Roy in 1968, was built based on the outranking relation for modelling the decision maker’s preferences. The method is based on pair-wise comparison. Comparison between alternatives proceeds on a pair-wise basis with respect to each decision criterion and establishes the degree of dominance or outranking of one option over another (Rogers and Bruen, 2000). The outranking relation in ELECTRE III is a fuzzy (imprecise and uncertain) binary relation (Roy, 1991).
Most complex decision problems include conflicting criteria that need to be accommodated. In most complex decision problems it is generally found that the numerical values of alternatives of some criteria are subject to imprecision, uncertainty and indetermination (Takeda, 2001). According to Takeda, Roy explained these three phenomena in the following manner.
Imprecision: because of the difficulty of determining a value, even in the absence of random fluctuation.
Uncertainty: because the value involved varies with time.
Indetermination: because evaluation results from a relatively arbitrary choice among several possible definitions.
ELECTRE III allows all three phenomena to be taken into account.
For more details on the calculation of the discordance matrix and distillation procedure the studies of Tam et al. (2003), Hokkanen and Salminen (1997) and Rogers and Bruen (2000) can be examined.
In the ELECTRE III studies of the present work, a performance matrix was first prepared. It is given in Table 5. The ascending orders were considered for the evaluation of the criteria with non-numerical values and the decision makers were asked to assign first place to the least important criterion. Then the other importance values were assigned based on how many times more important they appeared than the least important criterion. Thus, if a criterion was considered to be five times more important than the least important one, five was the value to be assigned to that criterion. The decision makers were asked to assign the weighting of criteria such that the sum of these values was 100.
Performance values of criteria.
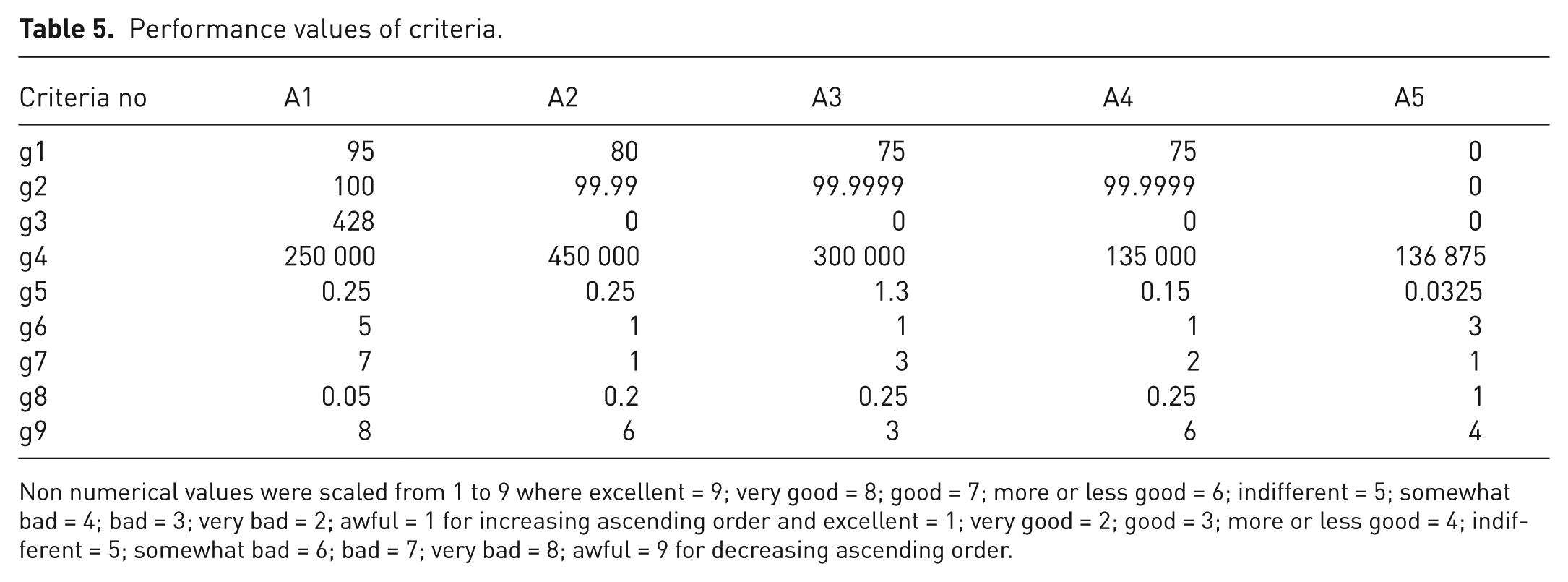
Non numerical values were scaled from 1 to 9 where excellent = 9; very good = 8; good = 7; more or less good = 6; indifferent = 5; somewhat bad = 4; bad = 3; very bad = 2; awful = 1 for increasing ascending order and excellent = 1; very good = 2; good = 3; more or less good = 4; indifferent = 5; somewhat bad = 6; bad = 7; very bad = 8; awful = 9 for decreasing ascending order.
The factors for score/values of the criteria are now explained and relevant references are included.
g1 (volume reduction). This criterion was based on the reduction in volume of healthcare wastes after the treatment/disposal. The values used were 95% for A1 (Şamat, 2006), 80% for A2 (Malkoç, 2004), 75% for A3 and A4 (Malkoç, 2004), and 0% was used for A5 because there is no treatment process.
g2 (microbial efficiency). The values used were 100% for A1 (Malkoç, 2004); 99.99% for A2 (DHV Consultant, 2010) and 99.9999% for A3 and A4 (Malkoç, 2004). Blenkharn (2006) reported that Staphylococcus aureus, Enterococcus spp., Salmonella spp. and other bacteria are found in healthcare waste landfill leachate. Therefore, it was deduced that there is no microbial removal in landfill.
g3 (energy recovery). In a healthcare waste incineration plant in Turkey, 5.22 ton h−1 steam and 428 kW h−1 electric power are produced for 1 ton of healthcare waste (Şamat, 2006). Large-scale microwave systems can have from one to six microwave generators (magnetrons). Generally, each magnetron has a power output of the order of 1.2 kW (Diaz et al., 2005). Similarly, steam is used for the sterilization process. Therefore, it was considered that there was no energy recovery for microwave and sterilization systems. It was also considered that there was no energy recovery in landfill due to low degradable organic carbon (DOC) content in healthcare waste (Karagiannidis et al., 2010).
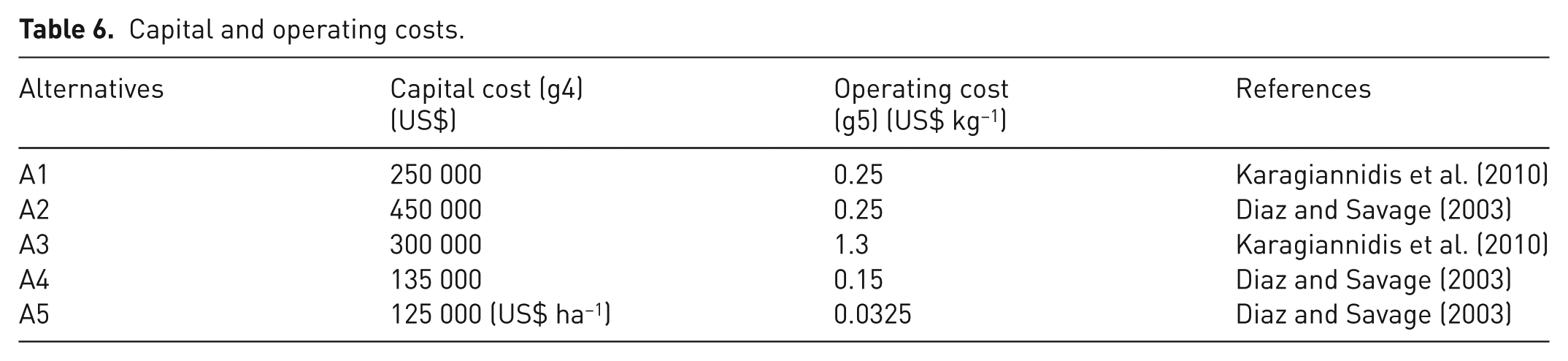
g4 (capital cost) and g5 (operating cost). The values used for these costs are given in Table 6 with references. The capacity for incineration, microwave and off-site sterilization was estimated at 250 kg h−1. The capacity for on-site sterilization was taken as 25 kg h−1 and the values were multiplied by 10 for correction of capacity difference. Healthcare waste density (100 kg m−3), landfill height (20 m), landfill useful life (10 years), amount of waste (250 kg h−1) were taken into account in the calculation of the capital cost of landfill and the calculated values are given in Table 6.
g6 (greenhouse gas emission) and g7 (emissions that have an impact on health). Incineration emits many harmful pollutants and those of particular concern include: carbon monoxide (as a result of incomplete combustion), hydrogen chloride, metals (e.g. mercury lead, arsenic, cadmium), dioxins and furans (Hossain, 2011). Hadar et al. (1997) reported that a number of volatile organic compounds are released at low levels during sterilization. For most volatile organic compounds, these concentrations do not constitute an acute health hazard. However, they may be higher than acceptable indoor air quality (IAQ) limits, and may cause discomfort, headaches or other symptoms when workers are exposed to autoclave emissions. Edlich et al. (2006) reported that air tests performed on the microwaving system confirm that no harmful air emissions are released during waste processing because the system includes a high efficiency particulate air (HEPA) filter. Furthermore, Karagiannidis et al. (2010) noted that greenhouse gas emissions from the final disposal healthcare waste were estimated in small amounts, as they were expected to be insignificant, due to low DOC content in healthcare waste. These criteria were graded accordingly.
g8 (solid residuals). The solid residuals of the process are related to the volume reduction. Therefore, the values of this criterion were given on the basis of the g1 criterion, which is based on 1 to n.
g9 (hygiene). For this criterion, human and environmental health was taken into consideration and numerical values of 1–9 were allocated. It was considered that as on-site sterilization should be accorded a lower score because it is carried out in plant and landfill sites and involves no microbial removal. Therefore, the values of this criterion were given as 8, 6, 3, 6 and 4, respectively.
Capital and operating costs.
With regard to the thresholds, all of the decision makers might assume different thresholds according to the criteria values. In this case, the average of these thresholds was used. The veto thresholds for all criteria were omitted. Using veto thresholds affects the final ranking. However, in this study, decision makers stated that there was no alternative that could be vetoed. Hence, the veto threshold was not used, and the discordance matrix was not considered. However, if needed, the spreadsheet tool developed for this study had the capability to incorporate the veto threshold. Parameters αq and αp were given values of zero, the values assigned to βq and βp for indifference and preference thresholds, respectively are given in Table 6. Similarly for ELECTRE III, the weights that were determined by the decision makers for each criterion are given in Table 7.
Threshold and weights of criteria for ELECTRE III.
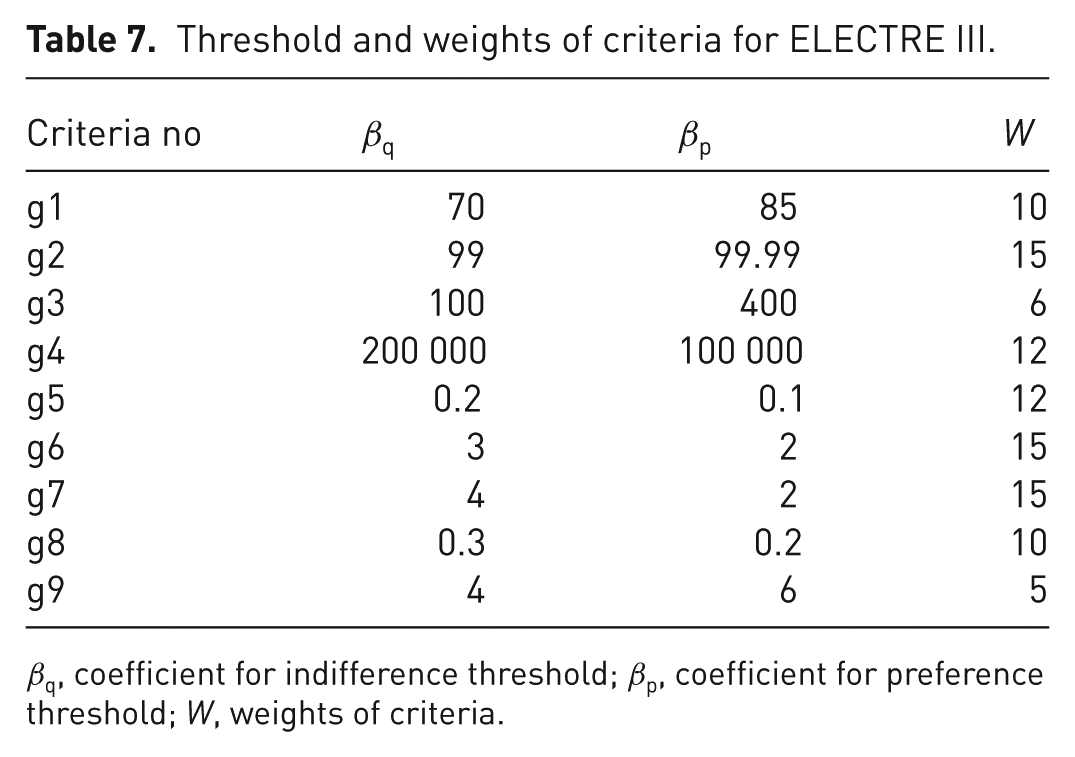
βq, coefficient for indifference threshold; βp, coefficient for preference threshold; W, weights of criteria.
Analytic network process studies
The ANP was developed by Thomas L. Saaty and provides a way to input judgments and measurements to derive ratio scale priorities for the distribution of influence among the factors and groups of factors in the decision. The ANP is a coupling of two parts. The first consists of a control hierarchy or network of criteria and sub-criteria that control the interactions in the system under study. The second is a network of influences among the elements and clusters. The network varies from criterion to criterion and a super matrix of limiting influence is computed for each control criterion. The super matrix is a two-dimensional matrix of elements by elements. The priority vectors from the paired comparisons are placed in the appropriate column of the super matrix. As the super matrix is built in this way, the sum of each column corresponds to the number of comparison sets. Finally, each of these super matrices is weighted by the priority of its control criterion and the results are synthesized through the addition of all the control criteria. In addition, a problem is often studied initially through a control hierarchy or system of benefits, a second for costs, a third for opportunities, and a fourth for risks. The synthesized results of the four control systems are combined by taking the quotient of the benefits multiplied by the opportunities to the costs multiplied by the risks to determine the best outcome (Ulutas, 2005).
The applications of ANP have been noticeably limited when compared with AHP, due to its complexity and time-consuming nature. So far, the ANP approach has proven itself to be successful when expert knowledge is used within environmental applications (Kone and Buke, 2007; Promentilla et al., 2006; Tran et al., 2004).
The decision makers are asked to make pairwise comparisons of the criteria of the network using a nine point scale suggested by Saaty. Whereas the basic ANP structure consists of only one network, the most complex one can analyse the benefit, opportunity, cost and risk that each alternative can cause together. The important issue is that benefit, opportunity, cost and risk may have different significance degrees according to the problem. This weighting procedure is called ‘benefit opportunity cost risk’ (BOCR) analysis. It should be noted that for costs and risks one must ask which is more costly and more risky (not which is less costly and which is less risky) because in paired comparisons it is only possible to estimate how much more the dominant member of a pair has a property as a multiple of how much the less dominant one has it and not the other way around (Saaty, 2001).
Super Decision software was used and BOCR analysis was conducted to apply ANP to the evaluation of a healthcare waste management system. In BOCR analysis, each alternative was evaluated in terms of its benefits, costs and risks; the opportunity cluster was not considered. The ‘benefits costs risks’ model was used to determine the values presented in Tables 5 and 6. For the criteria g1 to g5 and g8, the direct values of the criteria were entered into the program and for the other criteria, pairwise comparison was performed. In addition, a committee that included individuals from healthcare waste authorities and Anadolu University was set up to act as decision maker. It was pointed out that the consistency ratios were less than 10% due to the nature of the method; a self-evident fact.
In ANP, significance and impact weighting between each criterion may be determined by the decision maker. In this study, the significance of the weighting of the chosen criteria was been formulated in the program as additive (reciprocal)

In this context, first of all each cluster is rated separately. Then, these ratings are combined using the cluster weighting and the formulae including that to multiply the benefit ratios, reciprocals of cost and risk ratios. Finally these raw results are normalized and the values can be used as percentages for the evaluation of the alternatives (Saaty, 2001).
Results and discussion
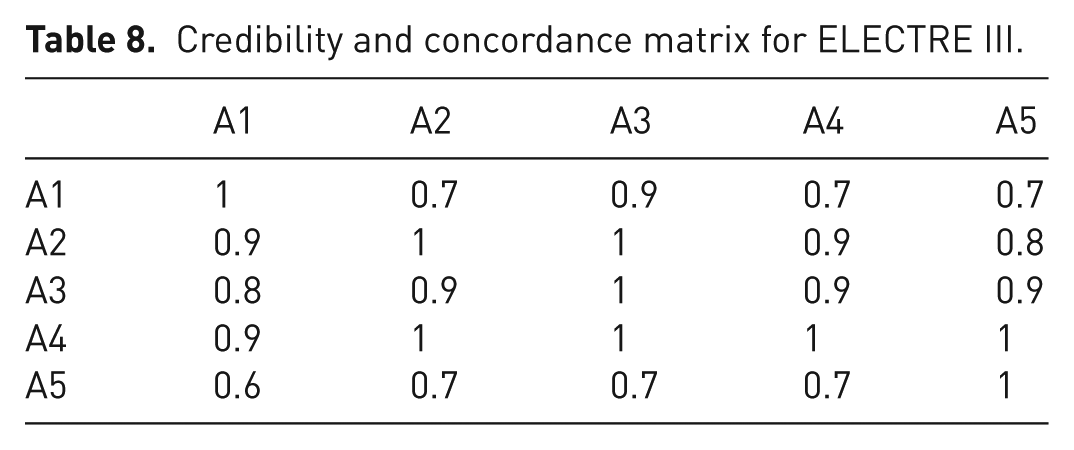
The alternatives for choosing the appropriate healthcare waste treatment/disposal system for developing countries were evaluated using the ANP and ELECTRE III techniques. For ELECTRE III, the concordance index and outranking degree means that the credibility matrix was obtained through the use of an Excel worksheet, which was developed by the researchers for similar MCDM problems. The distillation procedure that determines ranking orders in the present study is illustrated in Table 8. As the veto threshold was not used in this study, the discordance matrix was not calculated. The credibility matrix that gave the outranking degree was equal to the concordance matrix if the discordance matrix was not used. A value most approximate to 1 gave the most preferable alternative. For ANP, according to the criteria and the formula above, the appropriate order of the alternatives was evaluated and it is illustrated in Figure 3. The results of each cluster (benefit, cost and risk) and overall results as a percentile distribution can be seen in this figure.
Credibility and concordance matrix for ELECTRE III.
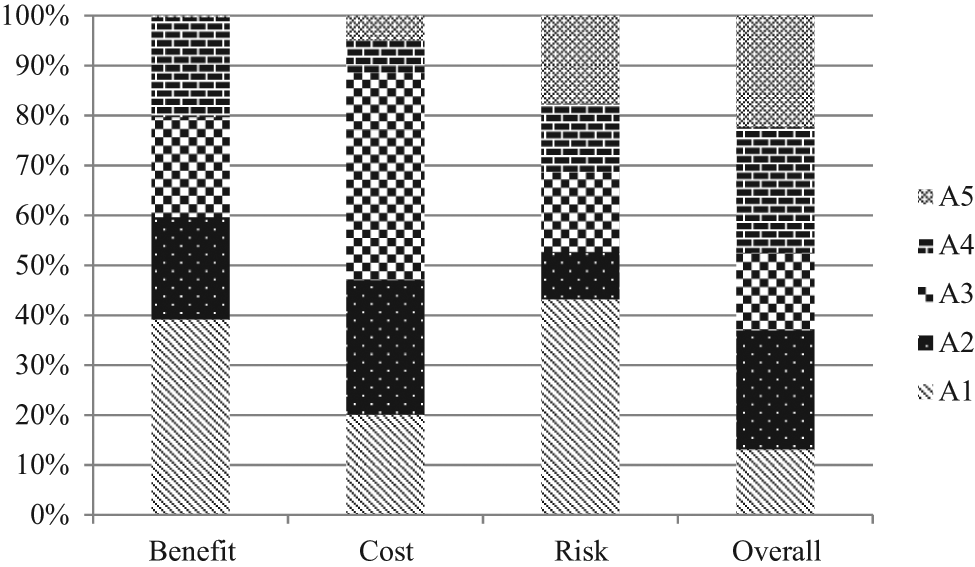
ANP results for healthcare waste treatment/disposal system (A1, incineration; A2, microwaving; A3,: on site steam sterilization; A4, off-site steam sterilization; A5, landfilling).
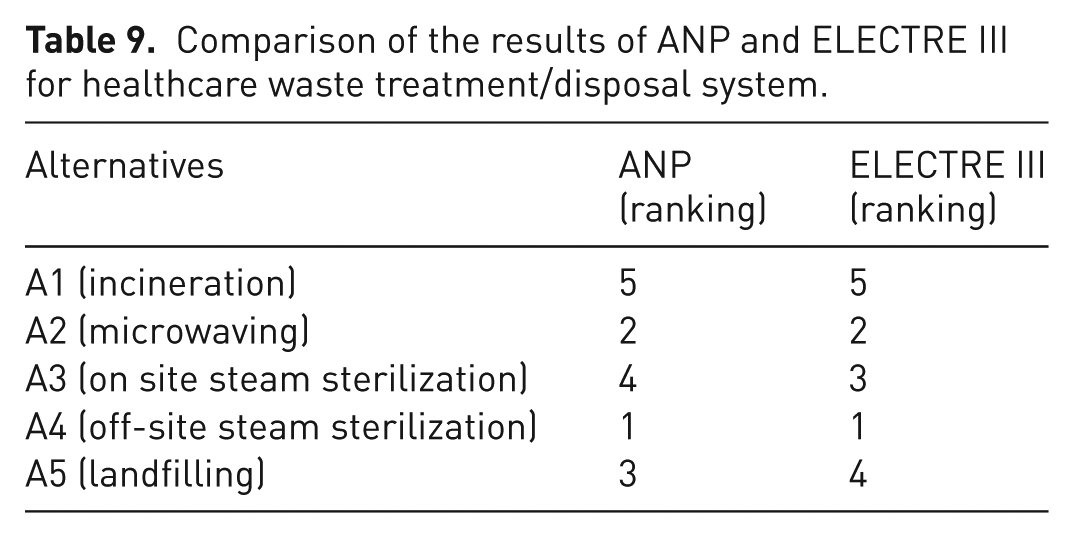
The results of both techniques are compared in Table 9. According to the overall results for both techniques, A4 (off-site sterilization) was the most appropriate alternative for healthcare waste treatment/disposal system on account of especially low costs and risks. A2 (microwaving) was in second place, because of low risks. Although A1 had the highest benefits in terms of energy recovery, it was ranked last overall because of the high risks due to hazardous constituents. A4 and A2 took first place in both techniques indicating the clear benefits of these alternatives. There were changes in the ranking of other alternatives. In the ANP technique, relations and directions between components represent a network. Therefore, it was considered that indirect interactions and feedbacks between components were not directly associated. On the other hand, although the ELECTRE III did not cover the above-mentioned network, there were preference and indifference thresholds for all criteria. Thus, it can be claimed that the most fundamental difference between these techniques is the cause of disparity in ranking. In this manner, the ranking of A3 and A5 changed.
Comparison of the results of ANP and ELECTRE III for healthcare waste treatment/disposal system.
Conclusion
Healthcare waste management has a different significance in an integrated solid waste management system especially in developing countries. In the planning of a healthcare waste management system in a given country, the decision makers of that country should consider various parameters including technical, economic, social and political factors. At this point, the MCDM procedure would be very helpful to decision makers in solving this complex problem. In the present paper, ANP and ELECTRE III, which are two well-known MCDM techniques, were used to decide between healthcare waste treatment/disposal alternatives. According to the evaluations, similar results were obtained using both techniques and off-site steam sterilization was found to be the most appropriate treatment option. The main factor influencing this result was low cost. The overall conclusion was that all of the healthcare waste generated in a city should be sterilized under the supervision of the local authorities. This is a process that has already been initiated in some cities in Turkey.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.