
Abstract
Recent decades have witnessed a dramatic upsurge in the prevalence of autism spectrum disorder (ASD). As researchers have investigated the responsible sociohistorical conditions, they have neglected how clinicians determine the diagnosis in local encounters in the first place. Articulating a position “between Foucault and Goffman,” we ask how the interaction order of the clinic articulates with larger-scale historical forces affecting the definition and distribution of ASD. First, we show how the diagnostic process has a narrative structure. Second, case data from three decades show how narrative practices accommodate to different periods in the history of the disorder, including changing diagnostic nomenclatures. Third, we show how two different forms of abstraction—Type A, which is categorical, and Type B, which is concrete and particular—inhabit the diagnostic process. Our analysis contributes to the sociology of autism, the sociology of diagnosis, the sociology of abstraction, and social theory.
Keywords
Introduction: The Interaction Order of the Clinic
This article is meant as a counterpoint to Michel Foucault’s (1975) famous The Birth of the Clinic, the great historicist “archaeology” of the Western hospital and its “medical gaze.” In a 2004 paper, Ian Hacking calls for an analytic approach that unifies the Foucauldian study of macrohistorical processes with Goffmanian micro-level ones—an approach that, as his (Hacking 2004) paper’s title suggests, would stake out a position “between Foucault and Goffman.” Hacking notes that the Foucauldian approach tends to dominate in many areas of sociohistorical inquiry, whereas we know much less about how sociomedical phenomena are produced in face-to-face interaction. This observation certainly holds for autism, a topic of investigation in such diverse fields as history, anthropology, psychology, biology, philosophy, and sociology, to name a few. For the most part, when not pursuing reductionist accounts in neurobiology (Minshew and Williams 2007; Nadesan 2005) or genetics and genomics (Bumiller 2008; Rabeharisoa and Bourret 2009; Singh 2016), such studies emphasize the meso- and macro-level social, political, and cultural forces that have shaped and transformed autism, especially in the last thirty years, when its prevalence has risen dramatically. Within sociology, the focus has been on autism’s distribution within populations (King et al. 2006), social risk factors for receiving a diagnosis (Liu, King, and Bearman 2010), and how changes in the institutional environment, along with the relative power of lay and professional actors, have created a sociohistorical niche—or what Eyal et al. (2010; Eyal 2013) call an “autism matrix”—where autism can proliferate.
In combination with epidemiological studies (Durkin et al. 2010; Durkin et al. 2008), these investigations provide a rich store of knowledge about how meso- and-macro-level processes have resulted in the contemporary autism “epidemic” (Bishop et al. 2008). However, with the rare exception (Rossi 2012), there are virtually no studies of how the diagnosis is applied to patients “on the ground” (Duneier 2007)—due, no doubt, to the paucity of data. Thus, we are fortunate to have access to audio/video recordings of children being evaluated for autism in three decades: 1972, 1985, and 2011-2015. These data afford us the opportunity to establish a Goffmanian basis for what hitherto have been mostly Foucauldian-style accounts of autism diagnosis.
Interaction, Narrative Dynamics, and the Social Organization of Abstraction
Our paper has three goals. First, it develops and elaborates Goffman’s (1983) concept of the local interaction order (cf. Rawls 1987), explicating its operation in the clinical setting. Per Maynard (2014:213), Goffman (1983) sees three ways that investigators examine local social order: (1) it has an integrity in its own right that blocks or operates independently of externally based structures; (2) it has disparate relations to social structures due to “loose coupling,” whereby participants manage the variety of externalities brought to situated action according to circumstantial contingencies; and (3) it straightforwardly manifests social structural conditions “as indicators, expressions or symptoms of social structures such as relationships, informal groups, age grades, gender, ethnic minorities, social classes and the like, with no great concern to treat these effects as data in their own terms” (Goffman 1983:2). We deploy the second approach, while drawing on ethnomethodology (Garfinkel 1967) for its theorization of everyday practices and their accountability. Moreover, from the field of conversation analysis, we also explicate notions of context-freeness and context-sensitivity in interaction (Sacks, Schegloff, and Jefferson 1974), with a view to specifying what “loose coupling” entails in clinical interaction.
A second purpose of this article is to further elucidate the notion of “making up people” (Hacking 2006) by way of narrative. Although Hacking’s (1999) monograph The Social Construction of What? is a notable exception, he (Hacking 2002a:100, our emphasis) concedes, “I look more at what people might be than at what we are. I imagine a philosophical notion I call dynamic nominalism, and reflect too little on the ordinary dynamics of human interaction.” With respect to autism, researchers have examined the production of autistic personhood at the level of cultural discourse (Grinker 2007; Nadesan 2005), through the looping effects of genomic research (Navon and Eyal 2016), and through shifting claims to expertise among institutional and noninstitutional actors, mainly parent advocates (Eyal 2013). However, none of these studies documents how clinicians, professionals, and others produce autistic persons via “the ordinary dynamics of human interaction”—that is, how this production occurs at the Goffmanian interactional level of focused encounters. 1 Whereas for Foucault (1972) discourses are relatively static sets of interrelated material statements brought into being in different historical periods, narrative discourse is dynamic—assembled in real time through ongoing talk and embodied conduct, as well as text.
Our third purpose is to theorize about the overall process of diagnosis, which is one of abstraction. Foucault (1975:8-9, 91) proposes that patients have features such as their “age, way of life, and a whole series of events . . . that are only accidental and fortuitous,” and which require the physician “to abstract the patient” in order “to know the truth of the pathological fact” in a process of effacement, whereby the “real patient” is “beneath the observing eye” of the doctor who is “forearmed” with “a rational, well-founded body of medical knowledge.” More contemporaneously, Abbott (1988:40-41) writes, “Diagnosis not only seeks the right professional category for a client, but also removes the client’s extraneous qualities” (cf. Mirowsky and Ross 1989:12). Such abstraction is related to what Cassirer ([1923] 1953:6, original emphasis) discusses in terms of conceptual formulation, whereby through subtraction or “reduction,” “what is merely a part has taken the place of the original sensuous whole.” However, Abbott (1988:102-3) suggests that subtraction of information is just one kind of abstraction, albeit one that is characteristic of medicine. The other kind of abstraction is one whereby a professional engages in practices of formalization requiring concreteness in diagnosis—“that knowledge is abstract which elaborates its subject in many layers of increasingly formal discourse” (Abbott 1988:102). The notion of abstraction via concreteness involves preservation of individuality—as a “whole,” with its own constituent parts (Rickert 1986). In this kind of abstraction, it is as if the concrete individual—in the integrity of his or her very holism—is abstracted from any larger environment in which he or she could be embedded.
In studying autism diagnosis, we will probe these distinctions—abstraction by subtraction (to which we will refer as Type A) and abstraction by concreteness (Type B). Demonstrating that these two kinds of abstraction have orderly relationships, we aim to contribute to a sociology of diagnosis via an understanding of the social organization of abstraction. This adds another, more profound theoretical layer to the paper, as the problem of abstraction(s) is at the heart of sociological theorizing. Insofar as such theorizing aims to establish causality, investigators suppress “concrete individual variability” and “ignor[e] particularities” in favor of “general qualities common to members of a certain class” (Martin 2011:29). Seemingly, this is the only possible way to engage in social explanation. However, the loss of the particular, to use Martin’s (2011) terms, in “third-person” (causal) explanations also means that “first-person” (everyday life) explanations are eviscerated and, with them, those orderly ways whereby persons produce the meaning structures of their concerted activities. As we shall see, the study of abstractions in autism diagnosis presents something of a metaphor for assessing the state of social theory in sociology. As the term “metaphor” indicates, we are not suggesting that the problems of abstraction facing social theory are identical, in a literal sense, to those confronting diagnosticians. Rather, our intention is to point out an analogical relation between these domains of inquiry, thereby calling attention to potentially instructive parallels between medical diagnosis and theory so that the sociology of everyday life and its organization—that is, Goffman’s (1983) interaction order—both in medicine or elsewhere—can be put on firmer ground.
Social Constructionism Versus Interaction Order
A social constructionist or “social model” view of disability proposes that ASD “does not describe a coherent biological construct” (Timimi and McCabe 2016:38) and is not “any kind of stable conceptualization” such that “people with an autism diagnosis . . . have any significant condition in common with each other” (Hasall 2016:57). 2 Such a perspective is consistent with the sociology of illness, and medical sociology generally, which emerged from the influential work of Parsons (1951) and prompted research on professionalism and social control (Freidson 1972; Waitzkin 1991). As Timmermans and Haas (2008:662) suggest, “Sociologists are reluctant to attribute ontological value to conditions that appear ‘natural’ to clinicians and patients”—namely, disease as opposed to illness, and the tendency is to “turn data about specific diseases into medical sociology concepts.” When Hacking speaks of “making up” (Hacking 2006) autistic individuals, however, he is not referring to autism as a construct in the strong sense: he means that the term and what it describes were previously not in the realm of social experience for either those who now have the diagnosis or others who know them. The condition existed, but in other terms than those that Kanner (1943) and Asperger ([1944] 1991) made available in their early 1940s publications. The concept of “making up people” is meant to direct attention to the processes and practices, including those of professionals, by which an individual person becomes a member of a category. Clinics are where this happens and, in our (Maynard and Turowetz 2017a) view, a more felicitous phrase than “making up” autistic people—at least within the synchronic context of the clinic, rather than the more diachronic, historical one where different categories of persons emerge and disappear 3 —is “doing” autism diagnosis. Constructionist accounts such as labeling theory have been vague about the “how” of social accomplishment, particularly in terms participants’ local experience and knowledge (Gill and Maynard 1995).
In capturing the “how” of autism diagnosis and taking an interaction order approach, our strategy is to recognize Pollner’s (1974:37) observation that those who label view themselves as “confronting an order of events whose character . . . is presupposed as independent” of their own responses. In some senses, clinicians themselves are social constructivists with insights into the social accomplishment of diagnosis, and our task is to grasp what they already know, both tacitly and explicitly, about what they do. Our approach also is consistent with Latour’s (2004) proposal that studies of science and technology (in our case, the technology for testing) can entertain a “realist,” non-ironic approach to social accomplishment, instead regarding such accomplishment as a “matter of concern” in the sense that the constituted object (i.e., ASD), in the first place, matters for professionals and laypersons, who collectively contribute to its existence (cf. Mol 2002). Rather than staking out an independent stance on the existence of the constituted object, sociological analysis can work to capture that concerned contribution, as it is constituted through practices that belong to an interaction order of diagnostic clinics (Rawls 1987). These practices—the “ground rules” of mutual commitment to a working consensus (Goffman 1967)—are manifest in the interactional substrate of testing (Maynard and Marlaire 1992; Maynard and Turowetz 2017b); in clinicians’ mutual narration of their findings as they determine a diagnosis (or rule it out); and, subsequently, in the delivery of diagnostic news to family members and others.
Diagnostic Narrative
Our previous research (Maynard and Turowetz 2017a; Turowetz and Maynard 2018) has analyzed the narrative structure of diagnosis, showing how professionals participating in the interaction order of the clinic collaboratively make sense of test results and other information (e.g., teachers’ reports) by telling stories to and with one another about children’s behavior during examination or elsewhere (e.g., in school, at home). The resulting chain of stories coalesces in an overall narrative about the child that is, or is not, consistent with an autism diagnosis. Later, when clinicians tell the news to parents, narrative is a means of presenting evidence to families, persuading them of either the diagnosis’s correctness or inapplicability, and adducing recipients’ own stories and perspectives regarding the child. In this previous work, which concentrates on narrative structure using detailed transcripts, we have only alluded to the implications concerning the interaction order, historical conditions, the sociology of abstraction, and sociological theory that we explore in depth here.
The narrative structure for diagnosis, illustrated in Figure 1, includes (A) preface(s) that may introduce an overall narrative or its constituent stories; (B) story types that are either (1) “instantiations” portraying single episodes occurring at a particular time or place or (2) “tendencies” that focus on a child’s propensities by formulating multiples and measurements of a given behavior; 4 (C) typifications, which are relatively static assertions that evaluate or assess the behavior(s), aligning them either explicitly or tacitly with a diagnostic category; and (D) recipiency, consisting of ways that hearers of the story react during the telling and after its completion. In this structure, narratives are probative for diagnosis. Instantiation and tendency stories are produced in support of typifying statements, which are diagnostically relevant claims about a given child. (Instantiations also can support tendency stories.)
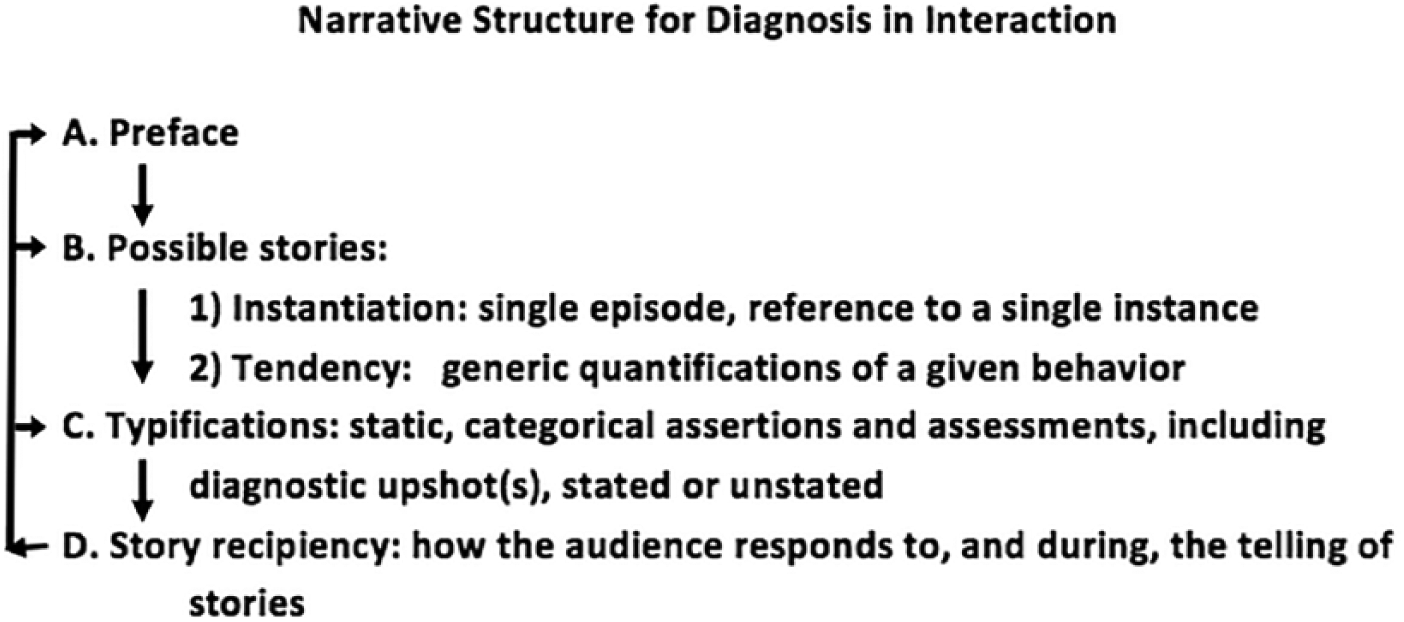
It may be that the narrative structure depicted in Figure 1 applies to other disorders or disabilities besides autism, since diagnosis—even for classical diseases such as cancer (Rabeharisoa and Bourret 2009), Huntington’s disease (Halpin 2011), cystic fibrosis (Hedgecoe 2003), and conditions for which neonatal testing can isolate genetic biomarkers (Timmermans and Buchbinder 2013)—is far from a Linnaean-type system of taxonomy (Hacking 2013), whose application to the natural world may be relatively straightforward. In psychiatry, at least, different but official classification systems can result in distinct groups of people being diagnosed for the same disorder; 5 our point, however, is that diagnosis takes interpretive work to achieve. Narrative structure comprises a set of “enabling conventions” (Goffman 1983:5) in the production of autistic persons and personhood. Rather than showing the “effects . . . as indicators, expressions or symptoms of social structures” (p. 2), such conventions or practices “do diagnosis” in a way that is sensitive to shifting historical contexts. These contexts are characterized by discourses defining autism through symptomatic terms encoded in testing protocols (Rossi 2012) and in successive editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD).
Narrative procedures by which clinicians apply the category of autism to children enable what Hacking (1999, 2002a) calls “dynamic nominalism” and “interactive” kinds of disability and disease, whereby diagnosis affects subsequent behavior that “loops” back into it—potentially altering its definition and application. However, just as diagnosis involves interpretive work and is interactive, it is also interactional: the success of doing diagnosis in clinics depends on how recipients—professionals, family members, patients, and others—respond to one another’s storied assessments while evincing forms of knowledge embedded in wider social environments than the clinic itself.
Data
In the analysis to follow, we use of data from three sources. The first consists of audio recordings made in 1972 at a clinic in the northeastern United States. The second and third, in different time periods, consist of audio and video recordings of children being evaluated for autism and other disabilities at a site we call Central Developmental Disabilities Clinic (CDDC): in 1985, as part of a separate but related study of news delivery in clinical settings (Maynard 1989, 2003), and from 2011-2015 (hereafter 2015). There are thirteen cases in the 1985 set (including two autism diagnoses) and forty-nine in the 2015 group (twenty eight ASD diagnoses). Audio and/or video recordings were made of all cases from intake to diagnosis delivery, and sometimes include follow-up visits with children and families and/or interviews with clinicians. Having data from three different decades, each corresponding to a different era in autism diagnosis, provides us with a unique opportunity to document the interplay of changing sociohistorical configurations and the situated interactional practices embodied in the clinic’s interaction order. Moreover, it allows us to do this not only for clinicians, but other stakeholders in the diagnostic process—parents and children (sometimes), teachers, caseworkers, and therapists. From each period, we use cases that are representative of wider patterns in the corpus. Because cases from the latter two periods (1985, 2015) have already been analyzed in depth (Maynard and Turowetz 2017a; Turowetz and Maynard 2018), in this article we include a transcript to illustrate the orderly detail of narrative structure only from the earlier era (1972) and summarize the more recent interactions.
Doing Autism Diagnosis In 1972
Our starting point involves detailed analysis of a case from data collected in 1972 at a clinic we call Eastern Developmental Disabilities Clinic (EDDC) (Lipton and Svarstad 1977; Svarstad and Lipton 1977). In this corpus, 37 of 55 children were diagnosed with mental retardation, a proportion vis-à-vis the one case of autism that reflects the era. Deinstitutionalization of the mentally retarded was underway, but only gradually; accordingly, “substitution” effects reducing that diagnosis in favor of autism were only slowly being felt (Eyal et al. 2010:98-110). Just one child (to be discussed here) was straightforwardly regarded as having autism, along with childhood psychosis. When, in 1972, “David Hamilton” (all names are pseudonyms) was diagnosed with autism at the age of 5 years, 7 months, the prevalence rate was around 1-2 in 10,000 (cf. Yeargin-Allsopp et al. 2003). In DSM-II (APA 1968), 6 there were no separate criteria for autism; rather, autistic behavior was described under section 295.8 for “Schizophrenia, childhood type.”
On an intake form, a social worker at EDDC, Vivian Greist, reported that David’s pediatrician referred him to be evaluated “for marked emotional immaturity and echolalia, aggressive behavior and hyperactivity.” At EDDC, Ms. Greist interviewed Mrs. Hamilton, after which a pediatric psychiatrist, Dr. Leonard Reiser, evaluated David, and a psychologist, Dr. Jim Smith, performed cognitive examinations. Subsequently, Dr. Reiser, accompanied by Ms. Greist, conducted an “informing” interview with Mr. and Mrs. Hamilton (Maynard 1989). This role for Dr. Reiser surely reflects an era when medical psychiatry, rather than other professions, held diagnostic responsibility.
Staffing Interview for David
Both of David’s parents attended the interview, which began with Dr. Reiser asking the parents their view of David (“Have you noticed any improvement since I saw him last?”). Mr. H answers Dr. R’s initial query with, “improvement isn’t really much,” and formulates a series of complaints regarding David’s inability to follow instructions: doing “what he wants to do in his own way,” being a “rough child to handle,” and “not listening.” He then proposes what “basically the problem is . . . that uh when you reach at the age of about four or four and a half you more or less stop maturing right there.” Dr. R follows Mr. H by confirming that David’s development had indeed “stopped”; he employs a tendency story format (Maynard and Turowetz 2017a:258), using a “when” clause and invoking the tendency term itself (our emphasis): “. . . and uh, when tested he then tends to look to us like a kid with retarded development.” The parents receive this with only minimal-type responses (“mm hmm,” and “mm”), and Dr. R backtracks from “retarded” to his initial version of David’s disability, which he typifies as being “stopped.” As this represents a retreat to what Mr. H has said about “stopped development,” he now agrees, saying, “Right.”
So far, we have two tendency stories, one suggesting “stopped development” and the other proposing “retarded development.” In the narrative sequencing, taking into account recipiency (see Figure 1), and thus how Mr. H affects the delivery of diagnosis, only the former is collaboratively validated. Dr. R proceeds to broach David’s “way of functioning,” thereby drawing a contrast between cognitive and social functioning, which may indicate the era when, as stated, autism was just beginning to be differentiated from mental retardation. However, it was also a period when the two conditions could be diagnosed in the same child, whereas previously they were considered mutually exclusive (Eyal et al. 2010:200). Dr. R continues at line 1 below (in the transcript, underlining of a word indicates prosodic stress; square brackets indicate overlapping utterances; numbers in parentheses are silences measured in tenths of a second):
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
We can see here how further tendency stories project a forthcoming diagnostic assertion: David “seems” oriented inwardly (line 1), with which, after a slight delay (line 2), the parents agree (lines 3, 4). And, Dr. R adds, his functioning “seems” to come from inside (line 5), depicting these tendencies as being in contrast with how others (“you or I,” line 6) perceive things “out there.” At line 7, Dr. R starts another tendency story, but then hesitates, cutting off the word “his” at line 7 and pausing at line 8, after which Mr. H produces a “candidate” completion (line 9)—a candidate because it requires affirmation from the original speaker. Dr. R follows by affirming (line 10, “Right . . .”). Interactionally, the parents and Dr. R mutually ascribe characteristics of inward orientation that these tendency stories suggest.
Tendency stories serve as evidence for typifications that, in turn, can align to diagnostic categories. The pattern we see here fits diagnosis as abstraction in the Type A, subtractive (Abbott 1988) sense of that term, where information is being removed (Mirowsky and Ross 1989) from the accounts regarding David’s behavior: what he “seems” to do has no concrete referents. In line with this pattern of aligning tendencies to categories, Dr. R goes on to suggest that David’s tendencies are a “reason” (line 11), along with others that are in the “emotional realm” (line 12), for typifying his difficulties as an “emotional” or “psychiatric problem” (line 13). Dr. R’s tendency stories, one of which is built on the father’s own such story about David’s development being “stopped,” follows the design of citing evidence as predecessor accounts to “asserting the condition” (Maynard 2004). Mr. H affirms the condition with an overlapping agreement token at line 14. Notice, however, that this token, arriving just after “emotional problem,” targets that formulation while partially competing with (by overlapping) “psychiatric problem.”
Subsequently, Dr. R moves stepwise to provide a more formal diagnosis, disclaiming the ability to be specific, and elliptically proposing, “this could be . . . a childhood psychosis” (lines 16-18). This official term from that era’s DSM (APA 1968) meets with silence (line 19), and Dr. R suggests “childhood autism” (line 20). Following another silence (line 21), he suggests compatibility between the two terms (line 22). After yet another silence (line 23), Mr. H receives the news (lines 24-25) by suggesting that the psychologist, Jim Smith, had said something similar, although not in the same diagnostic terminology, and instead regarding “thought process.” Insofar as this term would seem to revert to what was said at lines 5-6 about David’s perceptions, David’s father is offering a different characterization from that of Dr. R. While Mr. H can be said to claim agreement, he does not demonstrate it in the terms Dr. R has set. Despite the palpable resistance to those terms, Dr. R, in ensuing talk, remains insistent on two problems for David: “retarded development and very severe emotional problems” (1972, Informing Interview #17:20).
We have two points about this discourse: first, via tendency stories, narrative structure accommodates the era’s vocabulary for abstracting multiples of concrete behavior that are fitted to diagnosis. 7 Second, this structure accommodates to the period when this informing interview took place—one characterized by great unreliability in diagnosis. Eyal et al. (2010:195) point to parent-activist Bernard Rimland’s (1971) paper, which showed that, between 1964 and 1971, only 55 percent of 445 children seen by two different clinicians received the same autism diagnosis. As embodied here, such inconsistency was surely a resource for the father’s tactic of citing another clinician to contest the diagnosis. Later in this case, when the family discontinued their contact with EDDC, he stated in an interview with the researchers that a recent neurological exam had shown “nothing wrong” with David, but that he was “very sensitive.” And the father’s tactics, in turn, exhibit the kind of looping in disorders of “human kind” that Hacking (1999:104, 2007:299) formulates: in 1972, insofar as Mr. (and Mrs. H’s) 8 resistance to the clinical narrative could be emblematic, there was less likelihood of autistic experience in the society—not just statistically, but at the level of interaction.
Outcomes of the Case: Autism as Interactive and Interactional
The participants in this staffing go back and forth between seeing David as neurologically damaged with “retarded development” (per the clinicians), as opposed to having a “mental block or psychological problem” and deserving of regular schooling (in the father’s view). After the informing interview, the social worker wrote a note on the clinic’s “Continuation Record” for David: the parents were “very upset and refused to come back.” Indeed, she wrote another memo one month later, reporting that Mr. H had left a message to cancel an appointment, and he “seemed upset—wants no further service from clinic.” And six months later, a note on the Continuation Record stated flatly, “The family has refused further service because of the informing interview. Case is closed.” In part, the parents may have been dealing with the potential stigma then associated with autism, stemming from Leo Kanner’s early characterizations of parents as emotionally frigid (Eyal et al. 2010:52; Silverman 2011:38), and representing what Silberman (2015:6) calls “a dark age when psychiatrists falsely blamed ‘refrigerator mothers’ for causing their children’s autism by providing them with inadequate nurturing.” In Goffman’s (1963) terms, due to the difficulties he presented, David was a potentially “discreditable” person and, by consanguinity and what Goffman also called “courtesy” stigma (cf. Gray 1993), so were his parents. Their control of information (Goffman 1963:41-48) about David was crucial to stigma management.
We do not know whether David was able to participate in a regular classroom. From the tensions in the clinic and subsequent withdrawal from treatment for David, we can infer that the diagnostic process was degrading for the parents. This inference is confirmed in a post-informing interview conducted by the Lipton-Svarstad team soon after the informing interview: Mrs. H said that they had obtained a neurological opinion suggesting that David had an emotional problem, but nothing more. They did not regard David as retarded, psychotic, or autistic, and felt their experience at EDDC was “shocking” and a “rigmarole” that was utterly unhelpful. Then, in a follow-up telephone interview seven months later, Mrs. H repeated that there was “nothing neurologically wrong” with David, that he was doing “just great now,” and that their experience at EDDC was “so terrible that we just don’t want anything more to do with them.”
Social Interaction and Its Effect on Diagnostic Sequelae
In Hacking’s (1999:120) view, autism is neither a “natural kind” of disorder, where there is some underlying pathology the term references, nor is it a social construction, in the nominalist sense of existing only in the practices that bring it into being (Hacking 1999:33-47). Rather, as mentioned, autism is an “interactive kind,” having components with some referential basis or resistance (i.e., ascriptions of disorder are constrained, to some degree, by a pre-referential object)—what Hacking (1999:101-3) calls “indifference.” Further, it is constituted through the descriptive work the term does. The very children so designated may be affected by it—if not directly, then through the medium of their parents, clinicians, or others. “Interactive,” says Hacking (1999:104) may be an “ugly phrase,” but it “has the merit of recalling actors, agency, and action.” Hacking is pointing to, but not explicating, the workings of the interaction order. In the case of David Hamilton, doctor and parents are engaged in contestations over “person making” (Hacking 2006). All parties make use of praxiological resources endogenous to the organization of talk and social interaction in the clinic as an institution. Put baldly, despite the artful deployment of narrative practices, Dr. R failed in making David into an autistic child because his parents, in their ways of receipting the clinical stories, resisted and ultimately refused that categorization. They also refused the category of retardation. Their influence on the narrative for David was substantial.
Hence, clinical and narrative discourse regarding autism in relation to psychosis, both institutionally based but also transitory, was not, for this family, at this time, the operative one. As a single case, their experience sheds light on both the rarity of autism—recall that only one case of 55 from EDDC resulted in that diagnosis—and the opposition that accompanied its narration in the clinic. This is how Hacking’s notion of autism as an “interactive” diagnosis can be expanded to say that it has interactional properties. As a feature of the interaction order, clinicians, with typifying statements, can propose diagnoses through tendency and other stories. However, parents can accept or reject a proposal, resisting in ways such that clinicians mitigate what they are saying. And even then, parents can reject a diagnosis out of hand. As an interactional accomplishment, such dynamics can have long-term consequences for the child’s life, and for the diagnosis itself.
Interactional effects are indelibly related also related to interactive outcomes. Diagnosing David in 1972, Dr. Reiser was utilizing DSM-II, with its subordination of autism to childhood psychosis. When DSM-III emerged in 1980, its relaxed criteria for an autism diagnosis responded to the narrowness of the earlier definition and its imputation of internal pathology (cf. Eyal et al. 2010:18; Grinker 2007:136-37). It is consistent with the literature to suggest that the clinic-based diagnostic refusal of parents like the Hamiltons, in a way related to what was going on with parents nationwide, who organized themselves and formed collaborations with therapists (Eyal et al. 2010:25), or were themselves professionals with children who were diagnosed (Eyal et al. 2010:172), affected how clinician-researchers saw what they were dealing with. Parents, as well as professionals, contributed to the development of DSM-III. In other words, interaction shapes interactivity.
Doing Diagnosis In 1985
By 1985, at least three important happenings concerning autism had occurred. First, in the late 1970s, major British (Rutter 1978; Wing and Gould 1979) and American (Schopler et al. 1980) researchers had published articles describing autism as a spectrum—a “continuum of severity rather than discrete conditions” (Wing and Gould 1979:26). However, discrete conditions comprised the “classical” version of autism that Kanner (1943) had described, and this version was the cornerstone of autism diagnosis in DSM-III (APA 1980). Although the manual had dispensed with the autism-childhood psychosis connection, to diagnose what was called “Infantile Autism” (IA), the clinician needed to follow “‘objective’ lists of criteria” (Baker 2013:1091; Grinker 2007:117-18), including onset before thirty months of age, pervasive lack of responsiveness to other people, gross deficits in language development, peculiar speech patterns, and bizarre responses of various kinds, but with no delusions or other psychotic symptoms (APA 1980:89-90).
Despite (or because of) the official list of criteria used to diagnose IA, there was widespread dissatisfaction—“a chorus of complaints from clinicians who found the criteria difficult to apply in practice” (Eyal et al. 2010:234-35; Silberman 2015:389; cf. Silverman 2011:51). Clinicians—who increasingly were psychologists and other professionals rather than psychiatrists (Eyal et al. 2010:117-18), as in the Hamilton case—were already deploying what would come to be embodied in the revision, the DSM-III-R (APA 1987), using either “Atypical Pervasive Developmental Disorder” (APDD) or “Childhood Onset Pervasive Developmental Disorder,” which were also in the DSM-III but with much more flexible definitions than IA. 9 In other words, in 1985, even as autism in the DSM-III (APA 1980) was under revision to encompass variable conduct (Eyal et al. 2010:205-11), the criteria were already being relaxed in clinical contexts. Citing Croen et al. (2002), Eyal et al. (2010:235) observe, “DSM criteria follow practice rather than the reverse,” which once more suggests the “interactive” kind of diagnosis that autism is.
Second, the Autism Society, an advocacy group originating in the parent-activist Bernard Rimland’s National Society for Autistic Children (NSAC), had become a powerful lobbying organization, and influential for the 1975 Education for All Handicapped Children Act (EAHCA), 10 which guaranteed equal access to public education for children with disabilities (Switzer 2003:62-63). NSAC “lobbied to include autism as one of the developmental disabilities covered” by the act (Silverman 2011:49-50). Its effort reflected a wider concern for what the Goffman-influenced reformer Wolf Wolfensberger (1972) called “normalization.” This included strategies designed to deinstitutionalize children considered mentally retarded, and to dismantle the monopoly that psychiatry exerted over autism and related disabilities—to “subsume and subordinate” (Eyal et al. 2010:117) the profession to a more comprehensive system of care.
Third, a consequence of the EAHCA was to mandate services and therapy for children with disabilities, including those with autism in particular. These opportunities were not available when David Hamilton was diagnosed, but were in 1985. By then, the focus was (and remains today) on early interventions, which could give parents hope for bettering their child’s condition. Clinicians used the existence of services to persuade families of the relevance of an autism diagnosis (Gill and Maynard 1995; Grinker 2007:130).
These three factors played out in the diagnosis of Ronnie Martin in 1985.
Ronnie Martin
At the time of his evaluation at CDDC, Ronnie Martin was four years old. According to the intake report, Ronnie’s teachers were concerned “about some unusual behaviors and difficulty in playing with peers,” and, together with his parents, were seeking clarification of diagnosis and recommendations for his academic programming. A team of clinicians, including a psychologist, psychiatrist, pediatrician, special education specialist, occupational therapist, and speech and language pathologist, conducted individual evaluations of Ronnie over two days. The organization of this team in 1985 is dramatically different from the constricted professional pair who diagnosed David in 1972, when the psychiatrist was the primary actor and the psychologist more of a consultant. The 1985 team at CDDC had the psychologist (rather than psychiatrist) as team leader, while the number of other clinicians exhibits exactly what has been documented in terms of the expanding network of expertise surrounding autism (Eyal 2013; Eyal et al. 2010). During the pre-staffing meeting about Ronnie, team members—ignoring the category of IA in DSM-III—contributed to a narrative substantiating a diagnosis of APDD, but also referred to autism, using it almost interchangeably with APDD.
Pre-staffing for Ronnie
Bill Pender, the psychologist and case coordinator, started things by eliciting a report from the special education clinician. After a preface alluding to her overall assessment (“I did everything that I do with four-to-five-year-olds”), Debbie Jones told a tendency story: while Ronnie performed “everything at age level,” when he “takes those skills” and tries to “apply” them, he “falls down.” The when-then structure to this utterance marks it as a tendency story, which Debbie concluded with a typification: “He doesn’t have the generalization skills.” Debbie then segued to a second story, an instantiation: having been shown a movie about child abuse at school which conveyed the message that, if approached by an adult, one is “supposed to say no, run away, and tell two friends,” Ronnie went home, “viewed his dad telling him to pick up his toys as child abuse,” and told him, “I can say no, and I’m going to run away and tell two friends.” This instantiation story is one that is concrete and particular, and thus formalized abstractly (Type B) in Abbott’s (1988) sense. Rather than subtract information, it individualizes through a detailed accounting of what happened on a singular occasion. The story occasioned laughter from the other clinicians, and Debbie followed with a typification: “He’s very literal.” So, instantiations, like tendencies, can be evidential for typifications; but, unlike tendency stories, they provide constituent, ordered particularities.
Subsequently, others, including the speech and language clinician (Barb Miller) and the psychologist Bill, told tendency stories aligning to Debbie’s stance. 11 Barb depicted Ronnie’s literalness in stories about his “one way” of playing with toys, and Bill reported on how Ronnie does not do “creatively . . . new things with toys.” After hearing their accounts, Debbie produced a typifying upshot: “He’s a real good person for imitating and modeling.” As the clinicians continued their discussions, each systematically alternated between tendency and instantiation stories on behalf of typifications fitted to APDD and autism as a diagnosis. Along the way, a resident reported that his psychiatric supervisor (Molly Rinehart), who had a scheduling conflict and could not be present at the pre-staffing, had, during her interview with the parents, mentioned APDD. As the clinicians prepared to meet with Ronnie’s parents during the informing interview (“staffing”), they anticipated that the parents, as Debbie said, were “really afraid that he’s gonna be labeled.”
Staffing for Ronnie
The overall pattern during the interview with the parents was that each of the clinicians prefaced a delivery of findings, and then gave a report using the various narrative components to replay for the parents what they had told one another during the pre-staffing (Maynard and Turowetz 2017a:261-64). Although the parents accepted these findings, and sometimes told their own confirming stories, when it came to delivering the diagnosis, the clinicians were tentative and cautious. Bill, the psychologist-coordinator—reflecting a time when parents had become advocates—referred euphemistically to autism by suggesting how “some parents . . . find it helpful to hook up with organizations with other parents who have kids who have this kind of handicapping condition.” That “this kind of handicapping condition” tacitly referenced autism became apparent when he subsequently said, “So there’s something called the autistic society,” presumably referring to the Autism Society—that is, the successor organization to NSAC.
As the parents sat rigidly, and after Mrs. Martin whispered “Yeah,” Bill delivered the diagnosis as a tendency story. Referring to Molly, the psychiatrist who was now sitting across from him, he said (our emphasis): “When Dr. Rinehart uses a term called pervasive atypical developmental disorder, I think what we really mean by that is he shows many of the signs that other people called autism.” As in the case of David Hamilton, a feature of such tendency stories is that they allow for retreat: as the parents remained silent, Bill followed by saying, “But maybe not all of the signs and maybe to a somewhat milder degree.” After this small concession, Mrs. Martin gave a slight head nod.
Narrative Structure in the Era of DSM-III
Narrative structure imbued the diagnostic determinations in Ronnie Martin’s case, just as it had in David Hamilton’s. In both the pre-staffing and the staffing, as clinicians (with parental participation in the staffing) assembled a diagnostic narrative, the bulk of stories (about 80 percent) were about tendencies (Maynard and Turowetz 2017a). Clinicians used fewer instantiation stories (20 percent), suggesting that abstraction as subtraction (Type A) outweighs abstraction in the sense of concreteness (Type B) during diagnosis.
Ronnie’s parents were resistant, but not oppositional. After Bill proffered his formulation of Ronnie’s autistic tendencies, he reinvoked the experience of “other parents” who were “going through what you’re going through.” With this, Mr. M took a practical stance, neither showing acceptance nor agreement with the diagnosis, but only with Bill’s advice about working “it” into household maintenance—thereby sidestepping the diagnostic news, but not rejecting it as the Hamiltons had done. In subsequent talk, Bill addressed Mr. M’s concerns about income and costs by proposing that, with the diagnosis, state funding for treatment could be available.
Historical Context Sensitivity
In sharp contrast to our case from 1972, in 1985 we can see how autism, as an “interactive” kind of diagnosis, evinces at least three major developments in the interaction order of the clinic. One is the aforementioned size of the diagnostic team. Another is that, as the clinicians suggested APDD and autism as relevant diagnostic terms, they are moving past not only DSM-II, but already turning the terminology of DSM-III (APA 1980)—the manual then current—into a discourse, soon to be embodied in DSM-III-R (APA 1987), which avoids a strict checklist of items. Clinicians’ stories about Ronnie’s difficulty in applying his otherwise age-level skills, his tendency toward imitative playing, his literalness, and other matters are not matched to discrete definitions or IA as a catalogue of symptoms required for the diagnosis. Rather, these stories fit an emergent, interpretive “clinical picture” that “determines intervention, and provides a framework for medical education” (Jutel 2009:279).
A third difference, comparing 1985 and 1972, concerns features of the larger society, which the clinicians used as resources for doing diagnosis via narrative: Bill suggested that “organizations,” such as the Autism Society, which had emerged in relatively recent years, could be helpful to Mr. and Mrs. Martin. This move shifts the ground from “asserting” an autistic condition for Ronnie as such (cf. Maynard 2004; Peräkylä 1998)—even elliptically, as happened in David Hamilton’s case—to a recommendation that only implies Ronnie’s diagnosis. Then, after the tendency story about Ronnie having “many of the signs” of autism, and Mr. Martin’s receiving this news by stating his practical concerns, Bill addressed his apprehensions about income and costs by proposing that with the diagnosis, state funding for treatment may be available: “there are state regulations and local boards that are required, you know, to pick up the tab on certain kinds of services, and they may be willing to pay perhaps for all of the kinds of things that we’ve been bantering about in the last few minutes” (1985, Informing Interview J:74).
These resources were not available in 1972, nor was the possibility of pinning the diagnosis to now-accessible services. The only treatment recommendations for David Hamilton were for special schooling—“classes for children with emotional problems” (1972, Informing Interview #17:20)—aided by medication if necessary. The Hamiltons were particularly incensed that David could not participate in a regular classroom.
To return to autism as an “interactive kind” (Hacking 1999), Ronnie’s parents may have been resistive to the diagnosis but ultimately accepted it, partly on the basis of available state- and federally-funded programs, and remedial opportunities both at home and school. To complement autism as an “interactive kind” of malady, we again emphasize the importance of interaction. Clinical diagnoses are proposals deriving from narrated evidence that require acceptance for their realization in the life of a child, his family, his school, and other arenas. Even if Ronnie’s parents were hesitant, they continued participating in discussions about support and resources for a full half hour after the delivery of diagnosis. The combination of trans-situational interaction order—narrative structure—and sensitivity to mutable social and clinical contexts and opportunities means that the diagnosis spirals from the clinic to those contexts, which are ever-changing, and then back from the environment to the clinic, which process can further grow (or possibly shrink) 12 the autism matrix (Eyal et al. 2010) through further changes to testing, diagnosis, and the relations between children and caretakers. In other words, while “making up people” captures the historical development of different kinds of people, we think that “doing autism diagnosis” is a more felicitous description of the synchronic clinical work that applies the term to a given person and initiates a new looping process for that, and possibly other, individuals.
Doing Diagnosis In 2014
In 1985, autism’s estimated prevalence rate was on the order of 3-4 per 10,000 children. By the time Sara Brennan received the diagnosis nearly thirty years later, rates had increased dramatically—recent estimates suggest the condition affects 1 in 58 U.S. children (Baio et al. 2018). Several revisions of the DSM (in 1987, 1994, 2000) had produced broader diagnostic criteria encompassing a greater variety of cases. In a related development, called “substitution” (Eyal et al. 2010), clinicians were replacing other diagnoses, especially “mental retardation,” with autism.
Public perceptions of autism had also dramatically changed. For starters, there was much greater public awareness of its existence in 2014 than in 1985 or 1972 (Grinker 2007:14). Parents were more familiar with its characteristic features, either because of media coverage or through personal knowledge of friends, family members, acquaintances, or others with the condition (Liu, King, and Bearman 2010). To some degree, associations between autism, scientific genius (Nadesan 2005) and technical acumen (Silberman 2015) may have blunted the stigma surrounding it (Gray 2002:746-47), while parental activism successfully challenged the notion that “refrigerator mothers” or parents in general were to blame for autism, creating a sense of community and solidarity among people who, in prior eras, would have had far fewer social and material sources of support (Silverman 2011).
When Sara Brennan, then three years and four months old, arrived at CDDC in 2014, the operative diagnostic manual was DSM-5 (APA 2013), which had just been published. Whereas DSM-IV (APA 1994) and DSM-IV-TR (APA 2000) depicted autism as a family of disorders, DSM-5 collapsed discrete categories—autism, Asperger’s, and pervasive developmental disorder—into a single autism continuum, though not without controversy (Barker and Galardi 2015). Clinicians administered the second edition of the Autism Diagnostic Observation Schedule (ADOS II), a play-based assessment tool targeting various areas of a child’s social functioning, usually in conjunction with the Autism Diagnostic Interview–Revised (ADI-R), a structured interview with parents that elicits the child’s developmental history and current symptoms. At CDDC, pediatricians and psychologists assumed more responsibility for diagnosis, rarely consulting with the one, part-time psychiatrist (who otherwise practiced in a local school of medicine). This reflected considerable ferment in the field of pediatric medicine: in 1997 the American Board of Pediatrics had approved a subspecialty certification in developmental-behavioral pediatrics (Haggerty and Friedman 2003). The widening of expertise also showed the diminishing authority of psychiatry over autism (Eyal 2013).
Clinicians still used other instruments in combination with the ADOS, but the cumulative effect of the changes meant that, in 2014, there were different ways to be an autistic child than there had been previously. Children like Sara are identified earlier, may have milder symptoms that would have escaped early versions of the DSM, and may have parents and family members with knowledge about the condition.
Sara Brennan
Sara’s family doctor initiated the request for an evaluation for “developmental delay and concern for social interaction.” Previously, Sara was found to have language and gross motor delays, and had received remedial services through a “birth-to-three” intervention program. When the family was seen at CDDC, the team evaluating Sara consisted of a developmental pediatrician, who interviewed the parents, and a psychologist, who administered the ADOS. A speech and language clinician observed the ADOS to assess Sara’s language, but did not do a separate interview due to scheduling conflicts. Given the exponential increase in autism, CDDC, which, in 2014, had a year-long waiting list, was under pressure to streamline diagnostic evaluations. The center administration strategically cut back on the number of specialties involved, as reflected in the comparatively fewer professionals assessing Sara—although again, it is noteworthy that the two central figures were a developmental pediatrician and psychologist, with no psychiatric evaluation.
Pre-staffings for Sara
The developmental pediatrician (Leah Grant) and psychologist (Ruth McCain) met twice for pre-staffings, once after Leah’s evaluation but before Ruth’s, and then again after Ruth’s. As with Ronnie Hamilton’s case, we summarize these meetings, focusing on their narrative structure and diagnostic findings (cf. Maynard and Turowetz 2017a:264-68). This case may be emblematic of the time period, in that Sara’s ASD turned out to be a marginal one. In previous periods, it is probable that she would have passed under the radar of the clinical gaze.
At an initial pre-staffing with Ruth, Leah, having interviewed Sara’s parents and examined Sara, reported “a lot of red flags,” reproducing the parents’ own tendency stories in support of this claim. Afterward, Ruth left to administer the ADOS. Upon its completion, but before scoring the test, Ruth reviewed the notes she’d taken during the test, meeting with Aaron Burke (speech and language clinician) for a second pre-staffing. When asked for his observations, Aaron, primarily using tendency stories, developed a narrative consistent with ASD, although an issue emerged regarding whether Sara exhibited “joint attention” or not. Ruth observed, “I didn’t see any initiation of joint attention. So, like looking at me and an object and back? I didn’t see any of that.” Notice the negative form of quantification here (i.e., not seeing “any”). However, Ruth subsequently aired a qualification: “She did a pretty nice job with me, with some things.” After further review, Aaron produced an instantiation story: “Well there was the one time when she had the book open, and she said, ‘uh oh,’ then pointed to it, and looked right at you, and looked back to the book.” Ruth responded with an assessment, “Yeah, it wasn’t that great.” At this point, Aaron had to “run” to get ready for another case. Consequently, the matter of eye contact and joint attention remained unresolved.
Afterward, Ruth met with Leah for a third pre-staffing. Having not scored the ADOS, Ruth told Leah that the diagnosis was “definitely not super clear”: Sara had “some nice strengths” but was “pretty rigid in her play,” and evinced other behaviors that were “atypical”—for example, apparent lack of joint attention.
Staffing for Sara
Ruth left her meeting with Leah and, scoring the ADOS, determined that Sara did qualify for ASD. Subsequently, both clinicians met with the family. Following introductory remarks apologizing for time the family spent at CDDC, Leah turned the floor over to Ruth, who narrated the stories she had earlier delivered to her colleagues, and then relayed the diagnosis. The borderline status of the diagnosis was reflected in a pattern of praising statements, followed by diminishments. Ruth observed that Sara had a lot of strengths, a lot of pointing, a lot of gesturing, nice imagination, and no unusual sensory interests. Then Ruth produced a contrast term (“but”), and proposed how Sara had a lot of repetitive behavior, inattention to her interlocutor, and lack of interest in social communication. The parents displayed recipiency by periodically responding with “mm hmm” and “right.” Striking a cautionary note, but not deploying the circumlocutions that either the psychiatrist in 1972 exhibited with David’s parents or the psychologist in 1985 used when addressing the Martins, Ruth delivered the diagnosis as a “so-prefaced upshot” (Raymond 2004): “So, having said all of that, she did meet the cutoff for an autism spectrum disorder, in terms of what I saw in the assessment today.” Mrs. B, treating this tendency formulation as unclear, asked, “So what does that mean?” (cf. Maynard 2006), and Ruth replied, “It means that we can go ahead and give her a diagnosis of autism.”
At this point, Mrs. B looked down, put her hands over her face, and produced muffled sobbing sounds (Hepburn 2004:274). Mr. B, meanwhile, was nearly expressionless, although nodding his head in a possible display of alignment to—if not affiliation with—the diagnosis (cf. Stivers 2008). Ruth subsequently expressed empathy (Hepburn and Potter 2007:104; Heritage 2011; Ruusuvuori 2005)—“I know that’s really a difficult thing to hear.” Unlike our earlier examples, where parents were more resistive, Mrs. B displayed ambivalence: “It just . . . in a way it’s a relief but at the same time it’s not.” Leah, consistent with the pre-staffing discussions, qualified the diagnosis: because of Sara’s young age and strengths, they would call it “provisional” and recommend a reassessment before kindergarten. But, Leah continued, even if the diagnosis continued to fit over time, Sara had “all these really nice strengths” that would “serve her well.”
Compared to the 1985 Hamilton case, the proportion of tendency stories in Sara’s (79 percent) almost identically outweighed that of instantiation stories (21 percent); however, this staffing next shows an element that is very different from the earlier data. Shortly after the diagnostic news delivery, Mrs. B told a story based on her own experience: a man “probably in his forties” comes into the store where she works “every day” and carries on “a one-sided conversation where it’s just him talking for . . . like three minutes and then he walks out.” Mrs. B portrayed her coworkers and customers—they “are like, I don’t understand.” In quoting their portrayal, she also rolled her eyes, but then reported telling them, “I think he’s autistic . . . we’re just part of his routine,” and produced an upshot: “So I kinda understand it a little bit.” She then claimed a connection to her own daughter’s situation: “You know, his parents have done well with him too so . . . I can see that there’re gonna be challenges but . . . she’s happy.” Whereas a pattern in regular presentations of diagnostic news is for clinicians as deliverers to suggest a bright side or “good news” exit (Maynard 2003:177-82), here it is the mother as recipient who does so. The staffing then continued as Ruth briefly shared the results of Sara’s cognitive tests, proffering a typification that Sara was “a smart girl.” The interview ended with recommendations for a return visit with the speech therapist, advocacy at Sara’s school, and dealing with her sleep and behavior at home.
Narrative Structure in the Era of DSM-5
The narrative structure whereby clinicians built a case for Sara’s diagnosis, and then delivered it to her parents, is patterned like those we observed in 1972 and 1985. As in earlier eras, clinicians produce instantiation and tendency stories on behalf of typifications, building a probative rationale for diagnosis (Maynard 2004; Peräkylä 1998). Accordingly, while diagnostic terminology, criteria, tests, professional involvements, and other matters have changed markedly over time, the narrative organization of diagnosis follows the structure outlined in Figure 1; the imbalance between story types remains the same as well.
However, a further change, which the narrative framework accommodates, is the pattern of recipiency the parents exhibit. Whereas David Hamilton’s parents contradicted the psychiatrist, and reactions from Ronnie Martin’s family were strongly resistive in the immediate environment of diagnostic news delivery, the Brenan parents’ responses were more muted. Mr. B was quiet, but nodded in what seemed like an affirmative gesture. Quickly after her emotive display, Mrs. B claimed at least partial relief, showed knowledge about the possible autism of the man who visited her workplace, and related her daughter’s diagnosis and prognosis to this experience. Like others observed in the current data, this mother more actively participated in “making-up” the autistic personhood of her child than did parents in earlier periods.
In the overall data, we observe a range of reactions to the diagnosis that are neither wholly negative nor wholly positive. For example, in another 2014 case, after the mother of two-year-old twin boys is told that her children have autism and breaks down in tears, the co-present grandmother consoled her by comparing autism to attention-deficit/hyperactivity disorder, which (she proposed) doctors could treat more effectively “today” than in the 1980s. As the grandmother talked, the clinicians waited patiently, effectively allowing a layperson to assuage and assist the mother in making sense of the diagnosis. In other cases, parents expressed frustration at not obtaining the diagnosis. Thus, the parents of a seven-year-old girl expressed hope that she would receive an autism diagnosis so that they could finally obtain the right services for her.
Historical Context Sensitivity
“Making up people” (Hacking 2006), we have seen, is not about the social construction of autism; it refers, rather, to the role of institutions, professionals, and lay people—either those diagnosed or their family members. We are proposing to expand Hacking’s (1995a, 1999, 2006) “looping” and “interactive” framework to include how participants talk with and relate to one another at the level of everyday interaction, reflecting what they know—their statuses as “epistemic” actors (Heritage 2012) in the society—and how they exhibit this knowledge through the narrative practices for ascertaining, delivering, and receiving diagnoses. As Eyal et al. (2014:239) observe, looping involves “a multiplicity of processes”; in our view, talk and embodied social interaction surrounding diagnosis is a sociologically crucial site for looping. In Sara’s case, we see how a borderline diagnosis both reflects, and has potential to widen, behavioral conduct subsumed under ASD.
The Social Organization of Abstraction in Diagnosis
The sociology of diagnosis emphasizes how diagnosis “removes information” (Mirowsky and Ross 1989:12), “subtracts . . . content” (Abbott 1988:102), and places the patient “in parentheses” to distinguish symptomology from fortuitous features (Foucault 1975). Subtraction is one kind of abstraction (Type A in our designation)—a “form of measurement” (Mirowsky and Ross 1989:12) whereby symptoms fit one of two categories: amounts that meet a criterion and amounts that do not. Across eras, in our data, tendency stories may establish amounts of behaviors that qualify a child for an autism diagnosis.
However, abstraction can be of another kind (Type B): It can be formalized in the sense of elaborating the levels that characterize a phenomenon, like the “tacit knowledge” that Polanyi (1958) documents in the accomplishment any kind of standardized task, such as “the actual work of managers” (Abbott 1988:103). As Martin (2011:194), drawing on Cassirer, puts it, subtractive abstraction “sacrifices the nature of the units as concrete wholes,” whereas judgment preserves such concreteness in something like a gestalt figure, emphasizing qualitative experiences that are presented as meaningful phenomena with full texture and pattern. Whereas subtractive abstraction ensures generalization by rendering concrete instances in terms that they share, the abstraction involved in judgment (cf. Cassirer [1923] 1953:226) and gestalt perception (Köhler 1947) evince “transindividual principles of regularity” (Martin 2011:199) in their very detail.
Martin illustrates this point with the way an aesthetic experience of an object can evoke like responses from multiple persons. Beyond illustration, conversation analysis demonstrates the generalizing aspect of Type B abstraction through the analysis of the very phenomenon we have investigated empirically in this article. Telling one story can occasion recipient displays of understanding through “second stories” exhibiting a meaningful point drawn from the first (Sacks 1992:764-72). In their specificity, stories have order that tellers produce and that recipients ascribe, such that abstraction is both particular and general for the participants. Analysis captures transindividual regularity, then, by building on participants’ practices (Schegloff and Sacks 1973:290): Our analysis has sought to explicate the ways in which the [conversational] materials are produced by members in orderly ways that exhibit their orderliness, have their orderliness appreciated and used, and have that appreciation displayed and treated as the basis for subsequent action.
In diagnosing ASD, we have seen that professionals engage both Type A and Type B forms of abstraction, and each genre articulates a distinctive kind of knowledge about a child, 13 as clinicians deploy them evidentially for doing diagnosis, with tendency stories predominating. We now consider what these distinctive kinds of stories and abstractions mean for diagnosis, treatment recommendations, and other outcomes of the diagnostic process. Then we turn to the implications of the sociology of abstraction for social theory.
Story Usages
Tendency stories, along with the typifications they support, provide a Type A abstract version of children, subsuming concrete behaviors under the standardized version of both diagnosis and treatment. In Schnittker’s (2017:40) terms, although autism is now considered to be on a spectrum, diagnosis is “categorical” in that, at least in the use of the ADOS, it is “regarded as present when an individual has a sufficient number of symptoms to exceed a diagnostic threshold.” In being categorical, and thereby eviscerating individuality, diagnosis is subject to critique concerning the labeling it entails, the stigma it evokes and, particularly in the case of autism, the focus on deficits (Hasall 2016; Timimi and McCabe 2016; Verhoeff 2013). Yet clinicians are not essentialists—for example, they “work around” (Whooley 2010) diagnostic categories to provide what they consider appropriate treatments, and they recognize the ambiguity of psychiatric nosology. Accordingly, as Schnittker (2017:140-41) has shown, the picture is more complex than many constructionist critiques suggest. Nevertheless, tendency stories and typifications, in the articulation of Type A abstraction, miss something that Type B abstraction and instantiation stories can facilitate.
In Ronnie Hamilton’s case, for example, while his literalist tendencies fit the then-current DSM-III of “deficits in language development” or “peculiar speech patterns” criteria for autism, his interpretation of the child abuse instructions, per the story, has other facets than literalism: it shows his seriousness, his desire to follow instructions, his application of the lesson from school in a specific (although not commonsense) context, his orientation to the moral order, and perhaps other forms of concrete competence that are avenues for ascertaining his learning style. In Sara Brennan’s case, the instantiation stories about joint attention suggest that, under some circumstances, her ability for achieving common ground may have been available. What were the circumstances, and how could those be enhanced? Such possibilities for both Ronnie and Sara get eviscerated in discussions of tendencies and typifications that support an autism diagnosis, but otherwise diminish particularity and its clues about accessing a child’s understandings (cf. Solomon 2015). Consider what a mother of a child with limited verbal abilities has said (Chew 2013:309): If you start from the premise that every utterance is meaningful and that Charlie, though severely limited in his speech, is bursting with communicative intent, you start to see how much he is communicating, however little he speaks in recognizable words.
The Sociology of Abstraction and Social Theory
The distinctions we draw between instantiation and tendency stories mirror what Martin (e.g., 2011:104-7) terms “first-person” (based on “entities with phenomenological validity”) and “third-person” (hypothetico-deductive) explanations in social theory. Third-person explanations represent what we call Type A, subtractive forms of abstraction: in the diagnostic realm, these report a child’s tendencies which, as quantities, enable the determination of diagnosis—as though the latter were the dependent variable in a regression equation with independent variables comprising variation in social, linguistic, and behavioral flexibility. First-person analyses, by contrast, represent judgment—or the kind of abstraction (Type B) where a holistic picture combines concreteness, individuality, and particularity in meaningful, orderly configurations. In social theory, third-person explanations are taken to organize first-person accountings, thereby assuming the latter have no intrinsic order, that is, are not part of an “interaction order” (Goffman 1983), or that there is “no order in the plenum” (Garfinkel 1988:106). Accordingly, if there are parallels between diagnostic practices and social theory, it is, per Martin (2011), because the history of theory is one where “Durkheimian epistemology” (e.g., [1895] 1938:31-32) required the “repudiation” of lifeworld concepts in favor of scientific ones that subsume or subtract from everyday views and orientations. 14 Further, although with his verstehen approach, Weber saw everyday life as meaningful for its participants, ultimately he was interested the ideal-typical reconstruction of their motives. Thereby, both traditions encourage suppression of what we call instantiations—the “whats” of social conduct—in favor of tendencies, including quantified patterns, which more conveniently align to causal accountings, or the “whys,” of such conduct.
Martin (2011) is not alone in his trenchant analysis of social explanation. It is almost as if there is a subterranean concern in sociology with the Type A/Type B contrast in abstraction. It is exemplified in Abbott’s (1988) work, to which we have already referred, but also in aspects of transactional and relational sociology (Emirbayer 1997) stemming from Cassirer ([1923] 1953), Dewey (1922), and others. A wide range of scholars, including Somers and Gibson (1994), Bates and Peacock (1989), Wellman (1988), and others, critique what Blumer (1956) classically termed “variable analysis” for how it “detaches elements (substances with variable attributes) from their spatiotemporal contexts . . . and their relations with other elements within fields of mutual determination and flux” (Emirbayer 1997:288). A matter we cannot explore in this article is how these investigators ultimately are after a different structural target, such as social networks (Bates and Peacock 1989; Wellman 1988) or narrative identity (Somers and Gibson 1994) in contrast to our patterned concreteness-in-interactional-detail aim. But, in their orientation to context, elements, temporality, and mutual determination—though without using the term abstraction as such—they can nevertheless be understood, in their discussions of actual situations with their order-properties, to suggest the presence and importance of the Type B variety. In some quarters at least, the sociological discipline has lamented the predominance of variable-based, third person, causal inquiry to the neglect of on-the-ground, particularized patterns, even though these patterns are demonstrably general in the conduct of participants and thereby available for sociological analysis.
Oliver Sacks (1985), the famous neurologist-author, describes a man he calls “Dr. P,” whose neurological disorder prevented him from recognizing the identities of objects, although he could relate their parts in terms of subtractive abstractions—their categorical properties. Shown a rose and asked to identify it, Dr. P replies, “about six inches in length . . . a convoluted red form with a linear green attachment” (1985, 12). Dr. P’s description of the rose is geometrically and anatomically correct, identifying construable variables that could eventuate in identification of different plants, but lacks utterly the judgmentally achieved entity that comprises its ordinary meaning—its existence as a rose. Accordingly, Sacks refers to Dr. P’s “absurd abstractness.” Moving to the lesson that Dr. P has for his profession, Sacks (1985, 19) says, By a sort of comic and awful analogy, our current cognitive neurology and psychology resembles nothing so much as poor Dr P.! We need the concrete and real, as he did; and we fail to see this, as he failed to see it. Our cognitive sciences are themselves suffering from an agnosia essentially similar to Dr P.’s. Dr P. may therefore serve as a warning and parable—of what happens to a science which eschews the judgmental, the particular, the personal, and becomes entirely abstract and computational.
Likewise, it is this sort of “comic and awful analogy” between social theory and diagnostic practice to which we are calling attention. It may be that the sociology of diagnosing autism, and understanding how the process emphasizes subtractive, Type A abstraction over its judgmental Type B counterpart, provides a metaphor for what, from some perspectives, today ails social theory in our own discipline, insofar as variable analysis subsumes the particulate realities of everyday life. But it may also point the way to a solution—one that emphasizes the concrete aspects of social action and its organization, sacrificing neither formalization nor generalization per se. Thus, Type B abstraction, in and through instantiation stories, preserves the individuality of its subjects while also being probative for diagnosis and eschewing the “misplaced idealizations” 15 that can result from focusing on Type A theoretical entities, such as “the clinical gaze” (Foucault 1975) or “the discourse of medicine” (Mishler 1984). It is our position that this “first person,” Type B approach to abstraction, just as it offers to fill out the diagnostic and treatment picture for children in clinical settings, is vital to moving social theory forward.
In light of the foregoing remarks, our position is a matter of emphasis and balance, rather than wholesale rejection of Type A inquiries. Oliver Sacks (1985), in talking about eschewal of “judgement” in the neurosciences, can be understood as asking for better balance between computational inquiry and preservation of individuality. In the clinic, Type A abstraction and standardized assessment are important because they enable reliable identification of ASD (for such purposes as access to resources), but diagnosis also needs Type B abstraction, which preserves the uniqueness of the individual and his or her qualities as these affect, and are affected by, the environments that he or she inhabits.
Similarly, our understanding of clinical diagnosis is potentially informative for the way in which social theory is done. Discussing what we call Type A abstraction, which involves subtraction, and its role in theory, Stinchcombe (1984:53) observes, “A successful abstraction is a great achievement.” However, he also suggests that a “new achievement in scientific abstraction is needed,” whereby theory additionally addresses “expressive and particularistic” aspects of a phenomenon. This is Type B abstraction as concreteness. It may also be what Martin (2011) has in mind when promoting “first-person” treatments of the “why” questions in social theory. Indeed, Martin (2011:348-49) observes that even Marxian critique entailed the continual counterposing of “historical fact”—a judgmental abstraction in its own right—to the “broadsweeping abstractions” extant in political economy. In short, if our study has implications for understanding ASD and other kinds of diagnosis, it also has analogical resonances for developing social theory more generally. Interaction order analysis, implicating ethnomethodology and conversation analysis, can help to redress a current abstractive imbalance in theoretical inquiry in the way that Oliver Sacks was suggesting the need for reparation in clinical diagnosis and that we are proposing about ASD diagnosis.
Conclusion
We began this article by stating that its title was meant as a counterpoint to Foucault’s (1975) “birth of the clinic” investigations. By interaction order of the clinic, we mean the practices embedded in actual talk and embodied behavior through which clinicians examine children, interview parents and others, and relate their own and others’ (such as parents’ and teachers’) findings to one another on behalf of ruling in, or out, the diagnosis of an autism spectrum disorder. From the clinical perspective, ASD is a real disability and not a socially constructed “illness” (Timmermans and Haas 2008).
We have attempted to capture how the interaction order for doing diagnosis is “loosely coupled” (Goffman 1983:11) to facets of social structure, such as changing diagnostic terminology and criteria, altered networks of expertise, and services for handling disease, illness, and disability. Both Foucault (1975) and Hacking (2002a)—the latter by his own admission—have neglected actual talk, real social interaction with its pragmatic and temporal constitution (Emirbayer and Maynard 2011), and the ways that professionals and lay persons reflect and contribute to the manner in which a child or other person comes to be constituted, in various eras, as having a given diagnosis. As stated earlier, such constitution is no simple seeing-and-saying phenomenon (Balogh, Miller, and Ball 2015; Maynard and Turowetz 2017a); it requires the clinical work of testing children, scoring examinations, and presenting results in coparticipatory ways. The doing of diagnosis, in other words, is interactional, and ordered through those practices of talk and embodied behavior that clinicians, parents, and others, deploy in situated relationships with one another. This means that autism, as an interactive diagnosis, is also an interactional production, and that loose coupling between social structure and everyday clinic life requires attention to tangible order in talk and concerted behaviors.
By now, another counterpoint to Foucault’s (1972) work should be apparent, which is to his “archaeology of knowledge,” wherein “discursive formations” are regularized statements in a field of knowledge that consolidate the experiences of diverse communities and delimit social objects and personages. The fundamental question about discourse, for Foucault (1972, 46), is not about what a concept means in a definitional way, but how it has come, through historical processes, to “constitute” its object. Discourse, in this sense, has the crucial element of historicity, but it is relatively static in relation to actual conduct. Surely Hacking’s (1999, 2006) references to “making up people” have their provenance in this shortcoming of discourse analysis, but such references have their own kind of inertia. Narrative for doing diagnosis also results in a discourse, but one that involves practices that are real-time, here-and-now coproductions rather than conceptual, historical constitutions, and their “loopings” as such—although, as we have shown, such practices are sensitive to historical developments and contexts, reflecting and promoting cycles of diagnostic determinations.
Footnotes
Acknowledgements
This study was made possible by grants from the National Science Foundation (1257065) and the National Institutes of Health (17803). We are also grateful for support from the Waisman Center at the University of Wisconsin and its University Center for Excellence in Developmental Disabilities grant (NICHD P30 HD03352). This research was also supported by a grant to the Center for Demography of Health and Aging (P30 AG017266) at the University of Wisconsin.