
Abstract
Veterinary sciences are undergoing a paradigm shift in the way students are trained for practical skills since classical educational approaches, based on apprenticeships and wet labs, are no longer applicable due to the increasingly specialized nature of veterinary teaching hospitals, rising costs, and ethical issues. This paper presents and evaluates the effectiveness of a Virtual Reality Training System (VRTS) designed to allow students to train on equine upper airway endoscopy procedures without the risks and pressure associated with manipulating delicate instruments and approaching live animals, as well as avoiding stress for ill horses. Several pathological conditions have been implemented in the VRTS, whose design was carried out in collaboration with domain experts, aiming to improve the students’ diagnostic skills. The VRTS was evaluated against the established, traditional learning approach (based on a classroom lecture with image- and video-based instructional material) on a sample from the population of veterinary students by following a between-subjects design. Training effectiveness was assessed by evaluating the participants performing the endoscopy procedure on alive ill horses. Results suggests that students trained with the devised VRTS showed better control over the endoscopic tool and exhibited higher diagnostic accuracy during the in-vivo evaluation than those trained with the traditional learning approach.
Keywords
Introduction
Veterinary education is a one-of-a-kind university curriculum among biomedical sciences, and it is rapidly transforming all over the world, with an increasing need to train students using more ethical, sustainable, repeatable, and efficient teaching methods (Gordon et al., 2021). As a matter of fact, the traditional approach of acquiring basic clinical competences by following observational training or practicing on experimental animals, cadavers, or body parts now raises significant issues, especially at a scale. On the one hand, it must be considered that more simple and sustainable scenarios like the observation of medical or surgical procedures (potentially done via video recordings) do not allow the acquisition of the required technical skills and barely stimulate the students in the process of problem-solving and critical thinking, which are of paramount importance in these activities to develop diagnostic abilities (Andersen et al., 2023). On the other hand, practicing the required skills on experimental living animals, cadavers, or isolated body parts is associated with non-negligible costs, unaffordable for many institutions and educational facilities. Anyhow, even if these practical hurdles are overcome, the traditional approach alone is insufficient to guarantee effective learning. In fact, it has been proved that deliberate practice (i.e., intense, repetitive performance in controlled settings) is fundamental for fully developing practical and diagnostic skills, but such a learning setting is hardly achievable with experimental animals or cadavers due to the varying clinical conditions of the subjects, which hinder repeatability (at all, or under the same conditions) (Scalese & Issenberg, 2005). The urgency to find alternative methods for transferring and evaluating veterinary practical skills is further testified by the evidence that recent graduates lack confidence in their ability to correctly and safely perform clinical procedures (Hubbell et al., 2008). On top on that, animal-based practice is being increasingly recognized as ethically unsustainable (McCool et al., 2020, 2022) and the transition from cadaver-based training to animal-free veterinary education is strongly encouraged even by the European Parliament’s action plan (EU Parliament, 2021), which recommends the implementation of novel teaching and assessment methods under the circumstance that these will be tested and validated before introducing them in the curricula and employed on a daily basis (Kneebone & Baillie, 2008).
By looking at the broader field of medical education, it is possible to observe that similar issues have been tackled by exploiting simulation-based training tools, especially leveraging immersive Virtual Reality (VR) (De O. Sousa et al., 2022; Delgado & Mayer, 2025; Hannig et al., 2013; Tang et al., 2021). Since the early days of this technology, its application to training scenarios, particularly those in which trainees could benefit from “learning-by-doing” and “hands-on” approaches, has been identified as compelling. VR simulations easily enable medical trainees to practice disciplines or procedures characterized by high risks (for patients) and rare caseloads, possibly involving expensive and potentially delicate instrumentation (Buchner et al., 2022; Pedram et al., 2023).
Surgery and endoscopy are examples of scenarios in which the efficacy of VRTSs (VR training systems) has already been confirmed. These disciplines are characterized by a combination of technical skills (related to tools operation and dexterity) (Hannig et al., 2013; Wang & Wu, 2021) together with rapid analytic and problem-solving abilities (Andersen et al., 2023; Buchner et al., 2022; Delgado & Mayer, 2025; Spencer et al., 2019; Vining et al., 1996). Nonetheless, it is worth noting that a definitive scientific consensus has yet to be reached regarding the universal efficacy of VR-based tools in vocational and medical training. Indeed, there are studies that have demonstrated that, depending on the learning context, conventional and less interactive instructional formats (e.g., classroom lectures supplemented with video-based materials or observational learning) can yield comparable learning outcomes (Plotzky et al., 2023; Shao et al., 2024). These mixed findings underscore the critical importance of validating novel VR-based training systems against established educational practice. The educational value of immersive simulations cannot be taken for granted, as their ultimate effectiveness is highly contingent upon several interacting factors including the specific task at learning (Pratticò & Lamberti, 2021).
Despite these considerations, while for the medicine and nursery scenarios the body of literature on VR-based tools is quite extensive, in veterinary medicine it remains relatively underdeveloped compared to its human healthcare counterpart, particularly in scenarios involving large animals. While some studies have examined the educational benefits of simulation-based training for veterinary medical skills (Dhein, 2005; Fairs et al., 2023; Marcos et al., 2023), these approaches have yet to be validated in meaningful educational settings (Kneebone & Baillie, 2008). Notwithstanding, the complexities associated with veterinary medicine are not less significant than those characterizing human medicine. Moreover, veterinary graduates are typically required to demonstrate a minimum level of proficiency with the most common domestic species. This implies that they must acquire diagnostic skills across multiple species - each with distinct anatomical, physiological, and pathological characteristics - which students may not become adequately familiar with during their educational path (Scalese & Issenberg, 2005).
In particular, it is not uncommon for students to have little or no experience with large and potentially dangerous species like horses and to feel uncomfortable when approaching these animals, even at the end of their curriculum. Thus, among domestic species of veterinary interest, horses are the species for which the availability of alternative and effective training methods could have a remarkable impact.
A relevant example of another procedure frequently performed by equine veterinarians, especially in equine practice like in sport and racehorses, is respiratory endoscopy 1 .
Clinical training on this procedure, however, is limited by the paucity of clinical cases referred for this procedure (most of them are performed in the field), by the ethical and practical difficulties of collecting and exploiting diseased animals, and by the inadequate educational relevance of the so-called wet labs (in which practice is performed on cadaver heads) (Parente, 2018). The latter approach is specifically hampered by the lack of movements of the anatomical structures physiologically involved in breathing, as well as by the inability to reproduce clinically relevant changes.
Motivated by these challenges, this paper presents a VRTS designed to enable veterinary students to learn and practice equine respiratory endoscopy. As already introduced, the devised system aims to provide a risk-free, repeatable training environment specifically designed to enhance students’ diagnostic skills in equine endoscopy without compromising live animal welfare. In addition to focusing on the technical skills required to navigate the endoscope through the respiratory tract, the simulation incorporates a variety of diseases to further challenge students and foster the development of diagnostic accuracy. The effectiveness of the VRTS-based approach for this context was evaluated through a user study involving veterinary students, comparing it against the traditional classroom-based curriculum. The assessment measured both technical and diagnostic abilities, with students subsequently asked to perform the procedure in vivo on ill horses.
Background
This section presents a review of the literature relevant for the paper, focusing on the educational needs in veterinary education and the use of VR in endoscopy training.
Educational Needs in Veterinary Medicine
Nowadays veterinary graduates are usually mandated to demonstrate a minimum level of proficiency for at least the most common domestic species. This demand arises in a context in which the increasing number of students and the more and more specialized nature of the services offered by veterinary educational institutions cause the student to be exposed to a reduced number of first-opinion clinical cases, making practical training challenging (Kneebone & Baillie, 2008). Indeed, there is evidence that recent graduates lack confidence in their ability to correctly and safely perform clinical procedures (Hubbell et al., 2008). Practicing the required skills on experimental living animals, cadavers or isolated body parts, however, is associated with non-negligible costs and raises increasing ethical issues (Martinsen & Jukes, 2005). Moreover, it has been proved that deliberate practice (intense, repetitive performance in controlled settings) is fundamental for learning practical skills, but is hardly achievable with experimental animals or cadavers due to varying clinical conditions of the subjects, which hinder repeatability (Scalese & Issenberg, 2005).
Alternative methods are thus needed for transferring and evaluating veterinary practical skills, and VRTSs are promising candidates in this regard. Indeed, the use of immersive technologies in the medical field has already been associated with several advantages, such as high engagement (Xiong & Peng, 2024), improved performance (Loukas et al., 2010), and the possibility to leverage innovative interaction methods capable of accurately simulating real scenarios (Karambakhsh et al., 2019).
Nowadays, there is growing interest in the educational value of simulation-based training across various veterinary medical skills. Recent literature highlights the development and evaluation of diverse training tools, ranging from basic models for low-fidelity palpation and handling (Marcos et al., 2023) to more complex and high-fidelity ones such as surgical simulators, anesthesia trainers, and dental models (Dhein, 2005; Fairs et al., 2023; Muehlberg et al., 2023). While these simulation models, ranging from physical to desktop-based, have demonstrated positive impacts on students’ self-assessed confidence and basic skill acquisition, it has been acknowledged that rigorous validation in meaningful, ecologically valid educational settings is still required for widespread curricular adoption on a daily basis (Kneebone & Baillie, 2008).
Highlighting the importance of equine veterinary education, Xu et al. (2025) recently developed and validated two co-located Mixed Reality (MR) systems for equine diagnostic imaging training: one integrating MR with real radiographic equipment, and another relying entirely on virtual representations of both the horse and the imaging apparatus. Their comparative evaluation showed that the fully virtual system achieved usability and performance comparable to the hybrid setup, although physical equipment remained valuable for realism. These findings underscore the potential of immersive technologies to address safety, accessibility, and logistical constraints in veterinary diagnostic imaging and offer a relevant precedent for VR-based training tools in other equine procedures.
VR in Endoscopy Training
Endoscopy is broadly defined as a medical procedure in which an instrument (the endoscope) is introduced into the body through a natural portal (e.g., the mouth or the nose) to provide access to a view of its internal parts (Choi et al., 2015). Specifically, respiratory endoscopy is a procedure frequently performed in equine practice, especially in sport and racehorses. Due to the crucial implication of respiratory structures and their dysfunction in athletic performance, upper airway respiratory endoscopy is required to be performed without sedation (Parente, 2018). Thus, the ability to execute a rapid, delicate, and accurate examination is of paramount importance, not only for the animal’s welfare, but also for the veterinarian’s safety.
In recent years, several studies have explored alternative ways to simulate and train endoscopy procedures using different media. For example, 3D-printed airway models have been developed to reproduce the upper airways of small animals and proposed as an alternative to cadaver-based practice; these approaches have achieved good results per se, but have not yet been evaluated against existing curricular approaches (Munteanu & Hardy, 2025). Moreover, other physical practices have also been deployed and contrasted to more traditional ones, showing promising results. The use of a realistic physical reproduction of the internal apparatus of a cow, for example, was associated with an increase in students’ self-assessment of skills, knowledge, learning, and motivation compared to a simplified simulator (i.e., organs replica located inside a box), suggesting that increased realism may have a positive effect in learning scenarios (Muehlberg et al., 2023). Although these results are promising, physical approaches are hardly scalable and may not be suitable to create faithful reproductions of living specimens.
In the medical field, the use of VR for endoscopy training is not a recent development; it dates back to the late 1990s, when simulators were primarily designed for gastrointestinal and pulmonary endoscopy. For example, the first VR bronchoscopy system (Vining et al., 1996) consisted of a bronchoscope (an endoscope designed for examining the bronchial passages within the lungs) and a simulation station, which included a box - or a human mannequin - into which the endoscope was inserted, along with a computer interface that simulated the endoscopic view.
While first VR-bronchoscopy systems were developed for clinical purposes (Ramaswamy & Higgins, 1999; Vining et al., 1996), it became quickly obvious that this technology could be used also for educational purposes, as it allowed trainees to repeat procedural experiences at their own pace in a safe environment (Colt et al., 2001).
Besides the visual feedback, these simulators were providing auditory and tactile cues (by employing a mannequin and a mock-up endoscope) with the aim of reproducing real-life settings. Subsequent studies and systematic reviews have framed the capability of VR-endoscopy for training and assessing skills needed by bronchoscopists in terms of dexterity, ability to control the endoscope through the airways with minimal collisions against the walls, completeness of the examination through all the bronchial tree (i.e., accuracy), and operation speed (Bejani et al., 2023; Colt et al., 2001; Moorthy et al., 2003; Nilsson et al., 2017; Ost et al., 2001). Recently, the advantages of medical training in endoscopy procedures using immersive VRTSs have also been explored with positive results (Andersen et al., 2023).
Compared to the body of literature on simulation-based human endoscopy, the use of VRTSs for veterinary education is still under-investigated. To the best of the authors’ knowledge, only few studies have explored the use of VR-based simulation for veterinary endoscopy training, neglecting large animals and only focusing on small animals (McCool et al., 2020; Usón-Gargallo et al., 2014), and utilizing non-immersive VR technology. Since both the studies investigated aspects concerning dexterity and technical skills, special hardware was employed to interface with a mock-up endoscope and provide faithful haptic feedback, while the VR simulation was experienced on a desktop computer in an operating room (Yamauchi et al., 2024).
Despite the advantages in terms of fidelity, this kind of setup shows limitations in terms of scalability compared to an immersive VRTS relying, e.g., on consumer off-the-shelf hardware (Pedram et al., 2023). Another study that instead resorted to consumer VR hardware to provide VR-based training, yet still on small animals, is the one proposed by Yamauchi et al. (2024). The authors evaluated the proposed VRTS tool against more passive video-based learning and found that students that had used the simulator scored significantly higher than those who learned with an instructional video alone, and this result was achieved despite the relatively small sample size. However, their work primarily targeted the preparatory steps leading to endotracheal intubation rather than the manipulation of the tube within the specimen (which was not required by the specific airways procedure), making it in some way complementary to the VRTS and training scenario presented in this work. Moreover, regarding the current adoption in curricula, a recent literature review (McCool et al., 2022) highlights that only three institutions in the USA utilize VR-based software for endoscopy training in postgraduate programs, all of which concentrate on small animal internal medicine.
Considering the large number of veterinary students enrolled in university courses (as a reference, approximately 120 students/year at the University of Turin) together with the limited time at their disposal for deliberate training and generally limited economic resources, immersive VRTSs based on consumer hardware represent an interesting option that can enable pre-clinical training at scale. Moreover, the importance of leveraging immersive VR should not be underestimated, as its benefits extend beyond mere scalability. Such a system can simulate not only the clinical procedures and associated diseases but also the surrounding environment, thereby effectively recreating real-life clinical settings (Andersen et al., 2023; Xu et al., 2025). This capability has the potential to address some concerns related to simulation-based teaching in this field, such as the risk that an overly narrow focus on technical skills might overlook critical aspects of clinical practice, including communication, professionalism, and diagnostic reasoning (Gordon et al., 2021; Kneebone & Baillie, 2008).
Methods
This section presents the considered endoscopy procedure, the immersive VRTS devised for the procedure training, and the list of possible medical conditions that veterinary students should be able to identify during its execution. The overall aim of the developed system is to provide an effective tool for training in the procedure within a safe environment that does not expose live horses to potential risks and with a particular focus on developing the students’ diagnostic skills.
The VRTS design and implementation were carried out with the help of expert veterinary professors who were involved throughout the whole iterative process.
The system was developed using Unity (v2022 LTS), with the help of tools such as Blender (v3.3 LTS) for 3D modeling and Houdini (v19) for physics simulations. Thanks to the use of the OpenXR library in Unity, the VRTS can be run on different VR Head-Mounted Displays (HMDs). In this study, Meta Quest 2 and its bundled hand-held controllers were used for the experimental evaluation. A video showing the operation of the VRTS has been included as supplemental material and is available for download 2 .
Respiratory Endoscopy Procedure
The real-world procedure referenced in this study involves an invasive technique that uses an endoscope to examine the horse’s upper airways. The goal is to assess the general condition of the respiratory system and identify any abnormalities that would not be present in a healthy animal. Due to the complexity of the procedure and the involvement of a live horse, which may pose risks to both the veterinary staff and the animal, the procedure is typically performed by at least two operators. The first operator is responsible for inserting and maneuvering the endoscope cable while also restraining the horse to prevent sudden movements that could compromise the procedure or cause injury. The second operator supervises the process, manages the endoscope camera, and provides guidance to the first operator, such as directing the endoscope toward areas of diagnostic interest.
A crucial aspect of the procedure is the interaction with the horse, which responds to external stimuli. For example, the horse may remain calm if handled properly or become agitated in response to erratic or painful actions. To facilitate the insertion of the endoscope, the first operator must gently open the horse’s nostril and proceed with slow, precise, and controlled movements to avoid damaging the internal structures of the airways. Additionally, several secondary actions may be required during the procedure, such as occluding the horse’s nostrils to conduct a stress test, depending on the specific conditions being investigated.
VRTS Design and Implementation
The VR procedure was designed to closely replicate the real-world counterpart, with particular emphasis on the training component and the enhancement of diagnostic accuracy. Specifically, the behavior of the simulated endoscope was defined together with veterinary experts in an iterative way, with the aim of making the users perceive interaction with the virtual replica as a good proxy of the real one. The user begins the experience positioned beside the horse (Figure 1) and is prompted to insert the endoscope into the nasal passage of the animal. As in the actual procedure, the user must first interact with one of the horse’s nostrils using one hand in order to facilitate the insertion. Once the nostril is properly opened, the user can insert the 3D object representing the probing end of the endoscope with the other hand. The user then continues by manipulating the endoscope using one of the HMD’s controllers and pressing the corresponding buttons to explore the internal anatomy of the horse’s upper airways and identify any potential conditions. Additional actions may be performed to support the procedure when necessary. Virtual room where the experience takes place. At the beginning, the user (whose head is represented by a white sphere, in this non-embodied view) is located between the horse and the table
Specifically, the insertion of the probe is handled using the left controller. By pressing the grip button to simulate grasping the probe and moving the controller vertically in mid-air to replicate the gesture performed by a real operator, the endoscope advances or retracts within the virtual horse. Limited and calm movements are required to explore the internal anatomy, while sudden or exaggerated gestures result in collisions with the internal walls. These collisions are associated with potential damage and are registered as errors by the VRTS, as will be detailed later. Movement within the three-dimensional mesh of the horse’s airways is managed through the collision system provided by Unity. This implementation enables the probe to bend and curve in response to the shape of the mesh and the obstacles encountered during navigation.
The endoscope camera was implemented using a virtual camera attached to the probing end. The camera feed is re-projected onto a render texture that can be easily seen by the user (placed on a 3D model of a endoscopic monitor in the virtual environment), thus providing a continuous and realistic feedback that can be leveraged to accurately navigate the airways and detect conditions. The camera view (i.e., the probing end direction) is controlled mainly by the right VR controller. Specifically, to manage the endoscope probe rotations (3 DOF), it was decided to map the vertical rotation on the thumbstick up-down movement and the horizontal rotation on two controller buttons. According to the experts involved in the design process, this configuration was able to mimic the two gear knobs controlling such movements on the real endoscope better than, e.g., mapping the horizontal rotation on the left-right movements of the thumbstick (Figure 2). The remaining rotation (roll) was mapped on the thumbstick of the left controller. The probe light switch control was mapped on the thumbstick click of the right controller. First person view of the user in the VR experience holding the endoscope and controlling the movement of the camera using the buttons on the VR hand-held controllers: (a) user rotating the smaller gear knob on the virtual endoscope, which controls horizontal rotation (left-right), by using two buttons on the right-controller; (b) user rotating the bigger gear knob on the virtual endoscope, which controls vertical rotation (up-down), by using the top-down movements of the thumbstick on the right-controller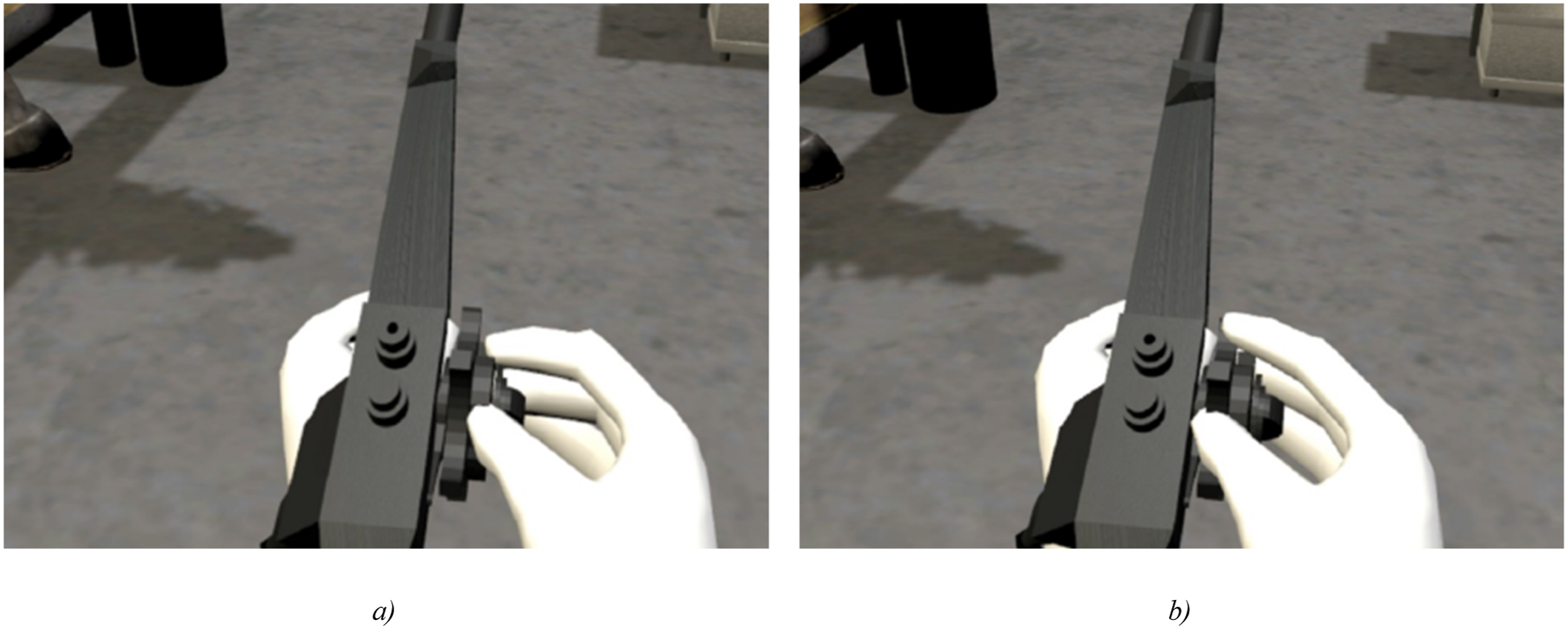
Finally, since a crucial part of the procedure is the ability to correctly detect and report the presence of any disease or condition, a virtual notebook was created, allowing the user to annotate the disease or condition currently framed by the camera and displayed on the monitor in the virtual environment (Figure 3). Specifically, a snapshot of the camera feed should be taken, and additional information added to the notebook to correctly label the detected condition. For assessment purposes, to check if a condition has been correctly framed by the camera, a custom mechanism was implemented: when the user triggers the snapshot capture, a ray is cast from the camera frustum, and if it reaches the simulated condition without colliding with other objects, the condition is considered as detected. If the name of the detected condition corresponds to the name marked on the notebook, the condition is also considered as correctly labeled. Notebook used to report the identified conditions; annotated information is leveraged by the system to provide an evaluation at the end of the experience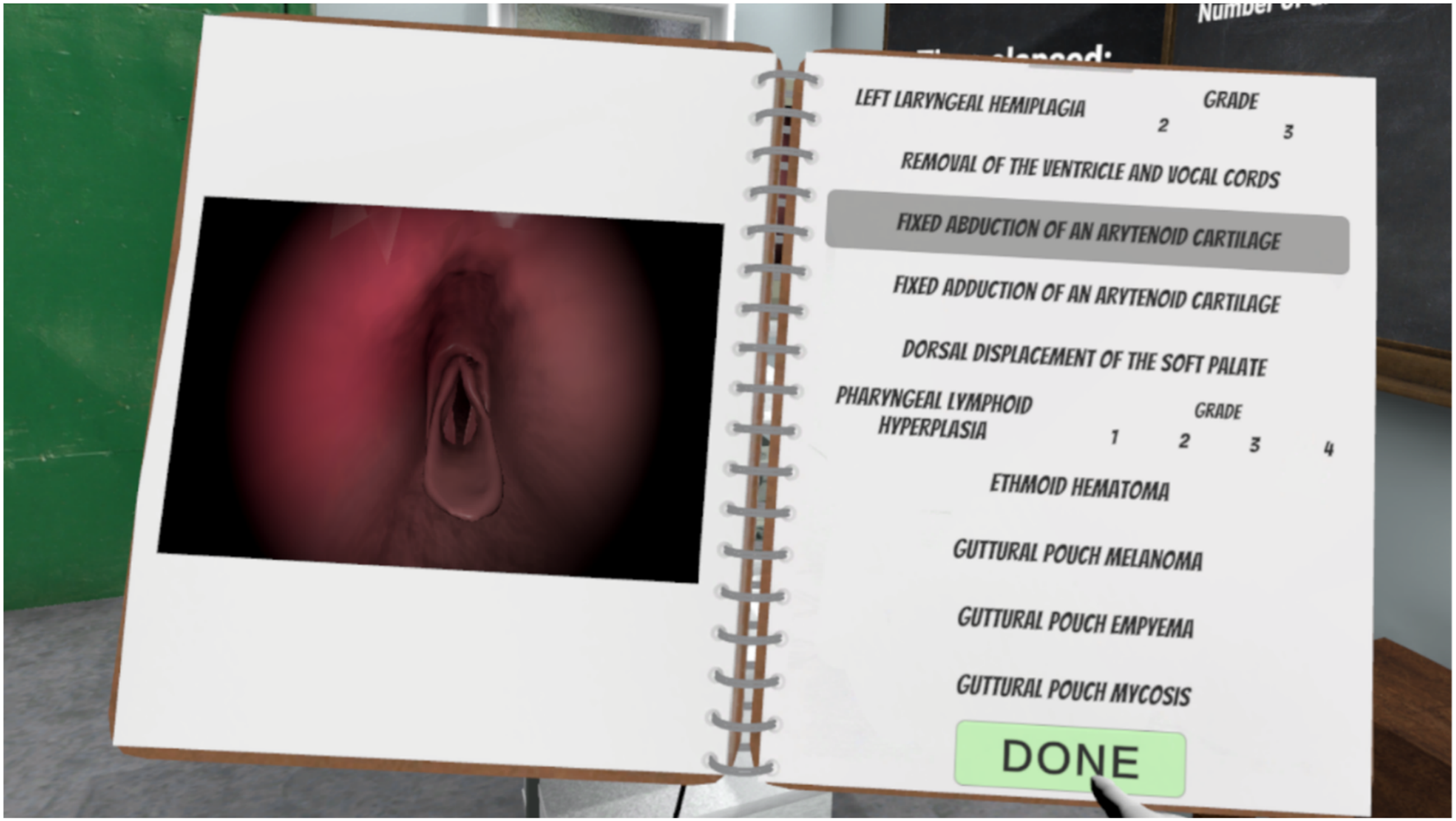
The current implementation supports the participation of two users, one wearing the VR headset and using the right controller (to operate the endoscope probe direction and light), the other observing the scene through a desktop monitor (non-immersive VR) and using the left controller (to move the endoscope further or backward in the airways). In the experimental evaluation, however, a single participant was requested to perform all the operations, thus preparing him or her to potentially interpret the role of both the veterinary operators.
Internal Horse Model
The internal model of the horse was developed from a Computerized Tomography (CT) scan of a healthy, medium-sized specimen under expert supervision and was subsequently imported into Blender. Within this software, the mesh was modified to eliminate holes and other extraneous components, and to reduce the number of vertices where high detail was not required. With continued expert support, the mesh was manually refined based on the observation of 12 horse specimens, resulting in a consolidated and representative 3D model of the horse’s airways.
Particular attention was devoted to the larynx, the organ responsible for regulating airflow through the respiratory tract during breathing. This structure was extensively remodeled to enable animation through a rig, allowing an accurate representation of the flexibility of the arytenoid cartilages. A similar approach was applied to the epiglottis to ensure proper animation when needed.
The final model was duplicated to create a low-polygon, segmented version (Figure 4(a)). These segments were used in Unity as colliders, which are responsible for detecting interactions between the probing end and the internal walls. This approach allowed the preservation of visual accuracy while reducing the computational demands associated with collision detection. An error in the CT scan regarding the anatomical entrance to the trachea and oesophagus was corrected directly in Unity by implementing an accurate mechanism for the opening and closing of the oesophageal sphincter. Finally, a procedural texture, closely resembling the appearance of flesh and thus simulating the horse’s upper airways walls was created and mapped onto the high-poly model (Figure 4(b)). 3D model of the inner horse’s head and upper airways: (a) segmented, low-poly version used for handling collisions, and (b) textured version that can be seen by the virtual camera of the endoscope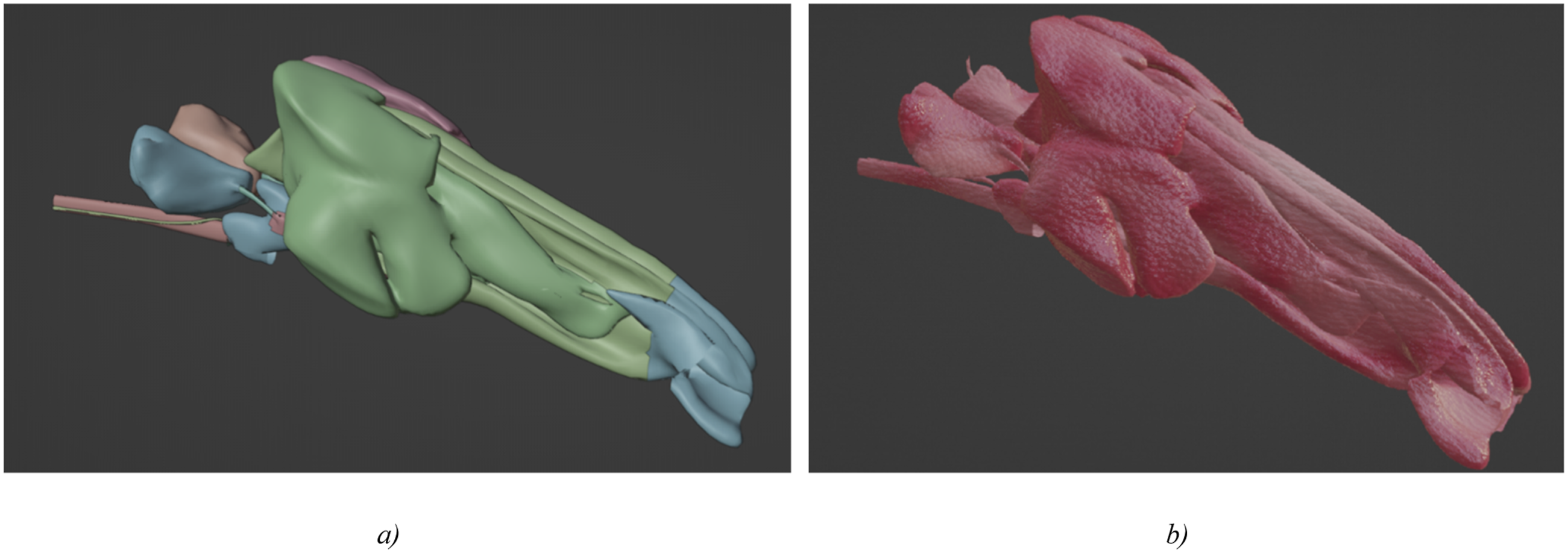
Diagnostic Challenges (Conditions)
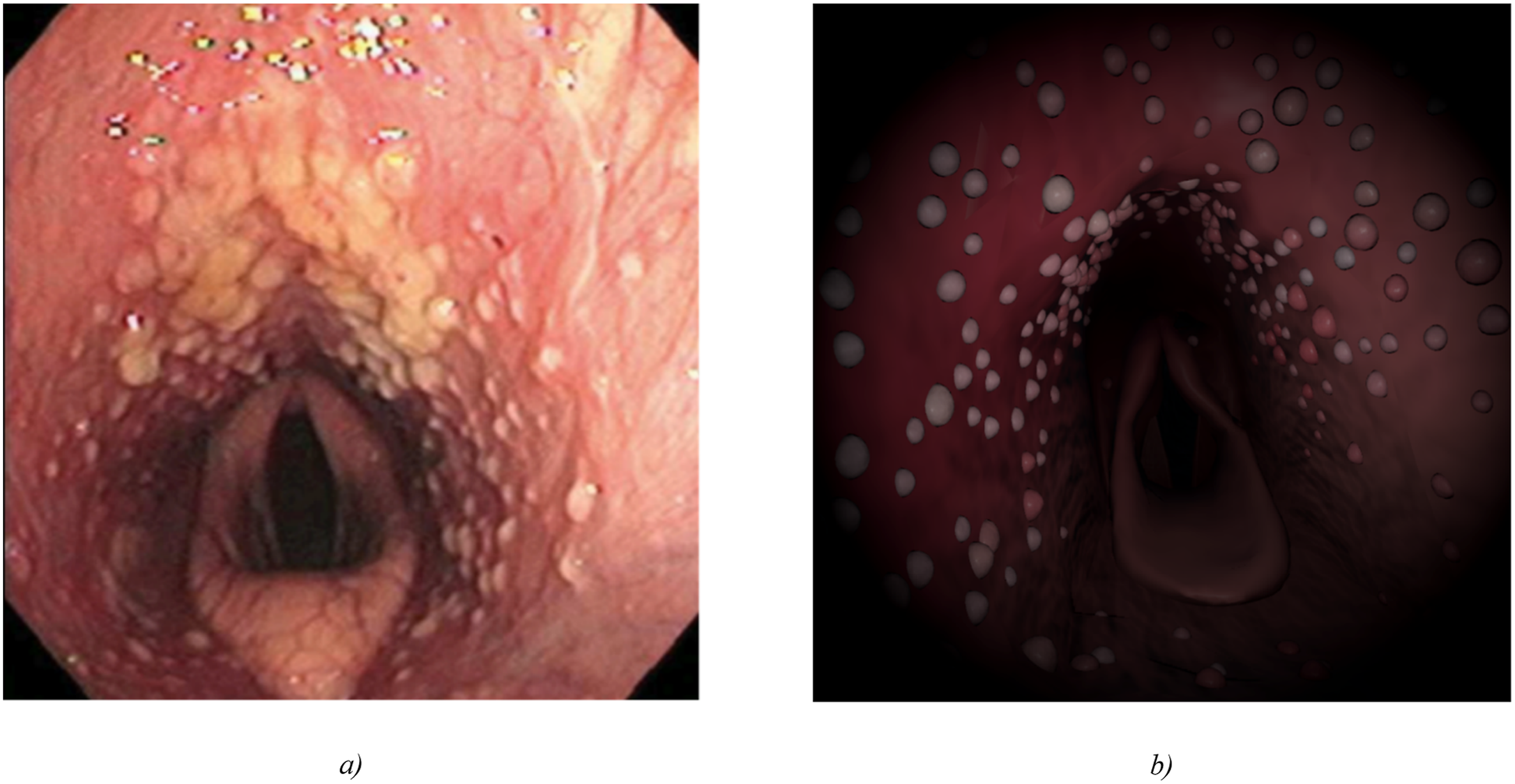
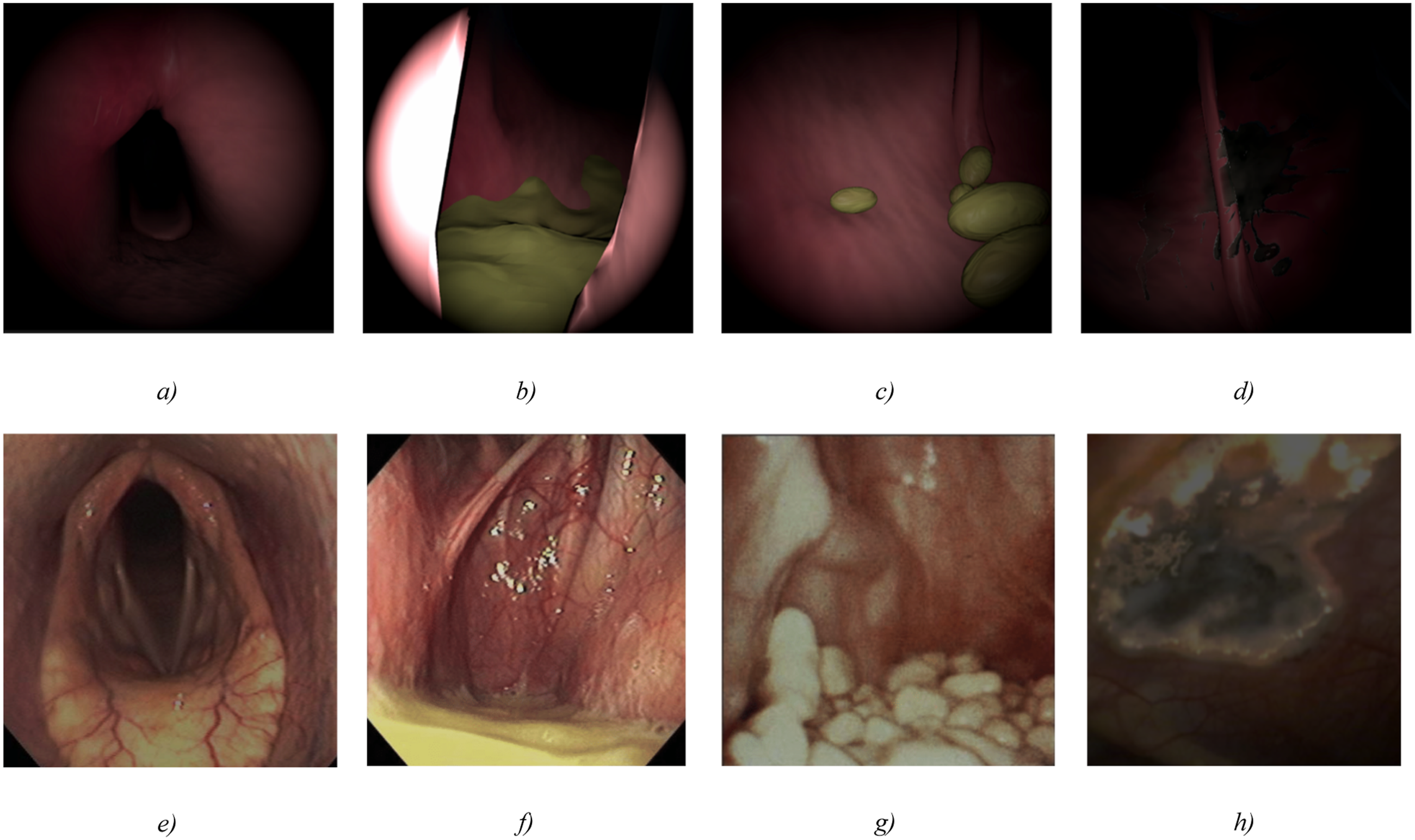
Since a key goal of the devised VRTS is the training of the students’ diagnostic skills, appropriate care was devoted to achieve an accurate simulation of possible conditions that could be encountered in a real endoscopy procedure. Thus, 10 of the most relevant conditions were modeled, both in terms of appearance and dynamics, and integrated in the simulation. Before starting the experience, from the main menu it is possible to selectively add, remove, or randomize the presence, in the VR session, of each condition. In the following, the nature of the considered conditions and their implementation is described. Video and photo references from real clinical cases available at the experts’ institution were used to define and implement the conditions. • Recurrent laryngeal neuropathy (RNL): a condition that affects one side of the larynx in horses, most commonly the left one, and is characterized by paresis or paralysis of the affected arytenoid cartilage causing a partial obstruction of the airway. An accurate replication of the larynx was required, with a focus on the symmetric and synchronous opening and closing of the cartilages, and the introduction of the asymmetric or asynchronous movement in the presence of the considered condition. • Removal of the laryngeal ventricle and vocal fold: a condition where the vocal cords are removed (ventriculocordectomy) to increase airflow and reduce noise as the horse breathes, alone or along with a prosthetic laryngoplasty. Starting from the accurate model of the horse’s upper airways, this condition was implemented by removing the parts of the mesh corresponding to the vocal cords. • Fixed abduction of an arytenoid cartilage: a condition that indicates a previous tie-back surgery, where the cartilage is pulled to the side and sutured to prevent it from interfering with the airflow, though not producing a completely normal airway. Surgical procedures could make horses somewhat more susceptible to pulmonary inflammation and infection. This condition was simulated by limiting the extreme position of the left arytenoid cartilage to 95% of the maximum value (that is reached in the normally animated mesh). • Fixed adduction of an arytenoid cartilage: a condition that indicates a previous reinnervation surgery if associated with the absence of respiratory noise. Sedation can cause false positives during exercise, or induce a severe RLN. Similarly to the previous one, this condition was simulated by limiting the extreme position of the left arytenoid cartilage to 95% of the minimum value (that is reached in the normally animated mesh). • Dorsal Displacement of Soft Palate (DDSP): a common respiratory condition in horses. The soft palate is a flexible tissue that separates the oral and nasal cavities, and is essential for breathing and swallowing. With DDSP, the caudal portion of the soft palate displaces above the epiglottis instead of laying below it, thus generating an obstruction to the expiratory airflow. DDSP can be fixed or intermittent. With intermittent DDSP, swallowing can replace the palate in its proper position. To simulate this condition, the part of the mesh corresponding to the nasopharynx was modified in order to animate the lifting of the soft palate. • Ethmoid hematoma: this condition is a rare and benign neoplasm that resembles a tumor in appearance and development, but is not neoplastic. It arises from the ethmoid turbinates and progressively grows into one or both nasal passages, paranasal sinuses, or nasopharynx, leading to respiratory obstruction and epistaxis. This condition was simulated by procedurally generating a mesh inside the nasal cavities, using the Unity physics system to follow the shape of the airways model. • Pharyngeal lymphoid hyperplasia: a condition that is characterized by the hyperplasia of pharyngeal lymphoid tissue within the submucosa of lateral and dorsal pharyngeal wall, and particularly around the dorsal pharyngeal recess. This condition is graded based on the size and extent of the lymphoid tissue enlargement. The lymphoid tissue forms small masses or nodules that can partially obstruct the airway, especially reduce nasopharyngeal tone and cause its dynamic collapse during breathing, leading to respiratory problems and decreased performance. Occasionally, follicles may enlarge and coalesce with surrounding follicles. This condition was simulated by randomly spawning a series of hemispheres in the submucosa, with different textures and sizes depending on the intensity of the condition (Figure 5). • Guttural pouch melanosis: a condition in which the guttural pouch mucosa is lined with a thin layer of tissue that can become discolored due to an excessive accumulation of pigmented cells known as melanocytes. This pigmentation is often brown to black in color, and can be seen on the surface of the tissue lining the pouch. Melanomas are often situated in the lateral compartment, on or near the external carotid artery (ECA) or maxillary artery (MA). They are usually very slow-growing, and hence rarely cause clinical signs. Malignant neoplasms of the guttural pouches are rare. This condition is simulated by either inflating the mesh of the pouch (Figure 6a, real counterpart in Figure 6(e)) or darkening the pouch using a procedural texture, thus simulating the different ways in which the condition can manifest itself. • Guttural pouch empyema: a condition caused by a bacterial infection that can result from a variety of sources, including respiratory infections, dental disease, or foreign bodies in the nasal cavity. The infection causes inflammation and accumulation of pus or chondroids in the guttural pouches. The former was implemented by spawning a mesh, created by displacing a plane using a texture, which was then modified according to the place of the spawning position inside the guttural pouch and the shape of the pouch itself (Figure 6(b), real counterpart in Figure 6(f)); the latter was implemented by spawning a series of oval-shaped 3D models inside the pouch (Figure 6(c), real counterpart in Figure 6(g)). The examination should allow the clinician to evaluate the extent of fluid and exudate accumulation, thus determining whether the disease is unilateral or bilateral. • Guttural pouch mycosis: a condition caused by the Aspergillus fumigatus, an opportunistic respiratory pathogen, that occasionally erodes the major blood vessels that lie just below the mucosa of the pouch, causing moderate or massive arterial epistaxis. Rarely, fungal plaques protrude from the guttural pouch entrance ostia and are visible from the pharynx. This condition was implemented by darkening the tissues using a procedural texture (Figure 6(d), real counterpart in Figure 6(h)), similarly to what done for the melanosis. Pharyngeal lymphoid hyperplasia: (a) condition as seen during a real endoscopy procedure, and (b) as seen by the camera of the virtual endoscope. Figure (a) Reprinted from “Atlas of Equine Endoscopy” by (Slovis, 2004), Elsevier. Copyright 2004 by Elsevier. License number: 6267541268180 Simulation of some of the other supported horse’s conditions in the VRTS: (a) pharyngeal collapse due to melanosis (b) guttural pouch empyema (i.e. pus) (c) chondroids, and (d) guttural pouch mycosis with darkening of the tissue. Sub-figures (e)-(h) are the respective real counterparts. Figure (e, f, g) Reprinted from “Atlas of Equine Endoscopy” by (Slovis, 2004), Elsevier. Copyright 2004 by Elsevier. License number: (e) 6267541268180; (f, g) 6267541013930. Figure (h) Reprinted from “Handbook of Equine Respiratory Endoscopy” by (Barakzai, 2007), Elsevier. Copyright 2007 by Elsevier. License number: 6267550083107
Assessment Module
During the VR experience, the user’s actions are constantly logged (performed/not performed, start/end time, etc.), in order to provide an assessment report at the end. For each possible action the system tracks whether it was executed correctly or not, and assigns a score that describes the level of performance. By carefully performing these actions and analyzing the report, the users can identify their strengths and weaknesses, and work to improve their skills. In this way, the VRTS can be used both as a tool for learning the procedure (with a trial & error approach, using the report as an assessment tool for improving in the next iterations of the experience) and to monitor progress over time. The aspects considered in the assessment which are common to all the sessions are reported below: • Sedation check: the animal must be examined in the absence of sedation, because sedation acts on laryngeal muscle control by simulating a pathological condition that does not really exist. • Left nostril check. • Right nostril check. • Left guttural pouch check. • Right guttural pouch check. • Nose plugged check: in the examination of the pharyngo-laryngeal cavity, it is necessary to plug the horse’s nostrils (for a limited time) in order to induce a negative pressure during inhalation, simulating what happens in high-speed exercise. • Swallowing check: advancing the endoscope into the uppermost portion of the trachea should induce swallowing; this operation is necessary to diagnose conditions such as DDSP. • Collisions during navigation: a number indicating the collisions between the probe and the internal walls while exploring the horse’s internal anatomy; a high number, especially in particularly sensitive areas such as the guttural pouches, could cause potential damage to the animal or to the operators (the horse could get annoyed and suddenly react, thus hurting the veterinary staff). • Time elapsed: a number describing the total time spent in the session.
In addition to these aspects, each condition included in the session is considered in the assessment and added to the report. In particular, if a condition is correctly detected and annotated in the notebook, it will be added with a positive value to the assessment report, whereas a detection of an incorrect condition (i.e. the user reported a condition that was not generated during the session or failed to give the correct label to a detected condition) will result in a negative score.
Experiment
In order to evaluate the effectiveness and usefulness of the devised VRTS, a between-subjects study was conducted, comparing the use of VR against a traditional, classroom-based teaching approach. In particular, an established M.Sc. course on Veterinary medical clinic and therapy taught at the Faculty of Veterinary Sciences at University of Turin was considered as a reference. This course includes a module dedicated to the use of the endoscope on live horses and is delivered through conventional lectures supplemented with printed and multimedia instructional materials covering the endoscopy procedure and the pathologies that may be encountered.
Participants were recruited from the third-year cohort of the degree program in Veterinary Medicine at University of Turin. Participation was voluntary, and students were informed that the study evaluated a new training tool. After providing consent, participants were divided into two groups using quasi-random assignment of participants (see Section Demographics): one group followed the standard approach used in the traditional course (Group SA), the other group experienced the endoscopy training using the VR-based approach (Group VRA).
Since the study aims to validate the VRTS against the traditional classroom-based curriculum, following an approach similar to that of Yamauchi et al. (2024), the control group (Group SA) was designed to adhere to this teaching practice. This approach provides a real-world benchmark, avoiding comparison with specially arranged programs (with participants training, e.g., on live animal) that, as discussed in introduction, are not feasible for routine implementation. In this way, it was aimed to perform the ecological evaluation of the VRTS tool integration against the current educational status quo experience established in the educational practice of University of Turin.
The experiment was organized in several phases. Firstly, all the participants (VR + SA) attended an introductory theoretical lecture on the procedure, with a focus on the normal conditions of the equine upper airway system; then, the participants in the SA group continued by following a classroom-based lecture which exploited the traditional material (videos and images of the procedure on representative clinical cases which demonstrated the conditions included also in the VRTS) akin to (Shao et al., 2024), whereas those in the VRA group used the VRTS to learn the endoscopy procedure and the diagnostic process for the considered conditions.
During the VR training session, each VRA participant operated on a virtual horse manifesting a set of four conditions, two of which were later expected to be encountered with the real horse (based on the pool of animals available for the experiment), while the other two conditions were chosen randomly among the remaining ones and were different for each participant.
After the training session, the participants in the VRA group received the automatic feedback provided by the system, whereas those in the SA group received no individual feedback on their training but, as normally done with students of the traditional course, they were involved in a 5 min long Q&A session after the lecture. The lecture focused on the same conditions that were used for the VRA group. The material of the two experiences was developed with the veterinary expert who taught the lecture, thus ensuring homogeneity of information provided.
Finally, all the participants experienced a practical evaluation session with live horses (which, for safety and animal welfare reasons, did not include the exploration of the left and right guttural pouches).
The evaluator was unaware of the group a given participant belonged to. During the evaluation, the participant performed the procedure in a team with another confederate (an expert that was not another student/participant and was consistent across all experiments) who strictly followed the student’s instructions to navigate the endoscope, without intervening to prevent or correct errors (thus potentially allowing for errors such as collisions to occur). It is worth noting that participants directly and manually controlled only the endoscope’s end-effector (which houses the camera) while verbally directing the confederate responsible for the insertion. Consequently, collisions and all related performance metrics reflected only the participants’ own control actions.
After each experimental phase, several questionnaires were administered to collect the participants’ feedback. The complete design of the experiment is illustrated in Figure 7. Design of the experiment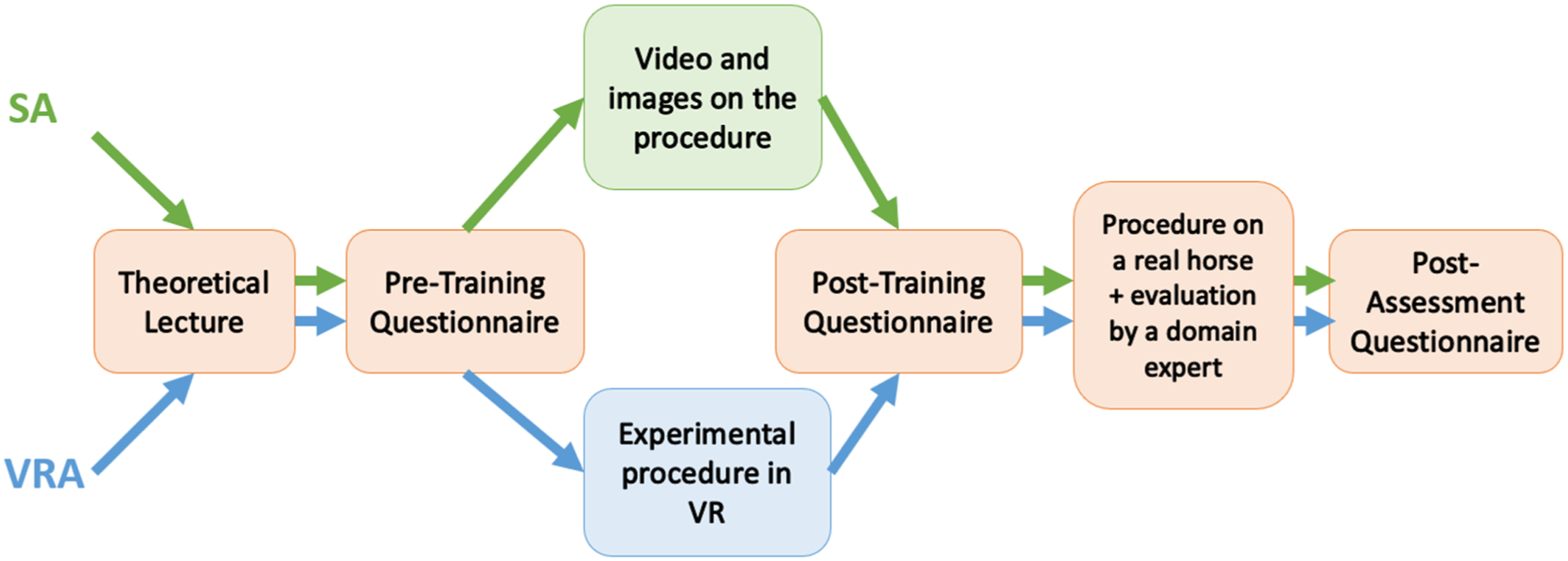
Evaluation Tools
The tools used for the evaluation encompassed standard questionnaires available in the literature, together with custom ones targeting specific aspects of the experience.
Specifically, the pre-training questionnaire consisted of general questions to collect information about the participants and their previous experiences with VR and in-vivo equine endoscopy (if any). The post-training questionnaire was composed of several constructs: • Usability was assessed using the System Usability Scale (SUS) questionnaire (Brooke, 1996), a widely adopted tool that provides a quick and reliable usability score. The questionnaire is frequently used to evaluate VR applications and the quality of user interactions (Rodrigues et al., 2022). Input usability was considered a key area of interest, as the real endoscope was simulated through VR controllers. Therefore, it was further evaluated using the input-related section of the VRUSE questionnaire (Kalawsky, 1999), whose items allow for a more detailed analysis of specific aspects of a VR system usability (Belger et al., 2024; Corelli et al., 2020). • Motivation at learning was assessed via the IMMS questionnaire (Keller, 2010), whose statements focus on Attention, Relevance, Confidence, and Satisfaction dimensions. More broadly, the questionnaire can be leveraged to evaluate the quality of learning experiences, and it is often used to assess activities involving VR technologies (Low et al., 2022). • Cognitive Load was measured using the questionnaire developed by (Leppink et al., 2013), which evaluates the mental strain associated with a training experience along the intrinsic, extraneous, and germane load dimensions.
In addition, the Cognitive Load Questionnaire (Leppink et al., 2013) was administered also after the practical evaluation in order to allow the measurements of pre/post effects.
The practical evaluation was performed by a domain expert (a confederate not involved in the VRTS design process) observing the participants of both the groups performing a real endoscopy procedure on living horses available at the Equine Veterinary Teaching Hospital of the University of Turin.
The confederate was supported by a structured check-list based evaluation sheet and asked to consider and annotate during the evaluation the number of collisions with internal walls, the number of successfully identified conditions, and the correctness of the endoscopy procedure measured in terms of steps performed correctly (sedation, left and right nostril check, nose plugging, and swallowing check), reported for each step with a binary flag on the sheet. For organizational reasons and to avoid overwhelming the same animal, four horses were used for the practical evaluation. The specimens were selected by the course instructor to be representative and to ensure comparable conditions (i.e. temperaments, handling ease, and clinical presentations) across participants. As said, the participants in the VRA group were assigned to a given horse by making sure to match at least two of the conditions encountered in VR.
Ethics Statement
The procedures involving animals in this study were conducted in accordance with relevant institutional and national guidelines for the ethical treatment of animals. The procedures performed in this study did not fall into a category requiring formal approval by a dedicated ethics committee. All operations were performed at the Equine Veterinary Teaching Hospital of the University of Turin and supervised by qualified veterinary staff, ensuring the highest standard of care and animal welfare. Written informed consent was obtained from the owner of each animal (horses) for all the operations performed in clinical settings.
Demographics
The sample (10 females, 3 males) was made of participants in the age range 22–25, with a mean of
Results and Discussion
Here below the results of the user study are reported and discussed.
Analysis Tools
Questionnaire scores and objective data obtained from the practical evaluation were first checked for normality with the Shapiro-Wilk normality test. Then the appropriate test (Student’s T-Test, Welch’s T-Test or Wilcoxon-Mann-Whitney U-Test) was used to determine statistically significant differences between the VRA and SA groups. For the Cognitive Load Questionnaire, a 2-Way ANOVA was used to investigate the differences between groups as well as the differences between the questionnaires administered after the training session and after the practical evaluation (pre/post analysis).
A sensitivity analysis was conducted using G*Power software (v3.1.9.7) based on the given sample size and between-subjects design. Considering parameters N = 13, α = 0.05, the smallest between-group effect this design could reliably detect at power (1–β) 80% is Cohen’s d = 1.47).
Duration
The time spent in the application ranged from
Usability
After the training session with the VRTS, the VRA group was administered with the post-training questionnaire, which included the SUS questionnaire and the section on Input usability of the VRUSE questionnaire. The average SUS score computed for the VRTS (obtained by combining scores assigned to its 10 statements, to be rated on a 1-to-5 Likert scale from “Strongly disagree” to “Strongly agree”) is
Usability of the VRTS According to VRUSE (Input) Results; All the Statements Were Rated on a 1-to-5 Likert Scale, From “Strongly Disagree” to “Strongly Agree”, Except the Last One, Rated From “Very Unsatisfactory” to “Very Satisfactory”
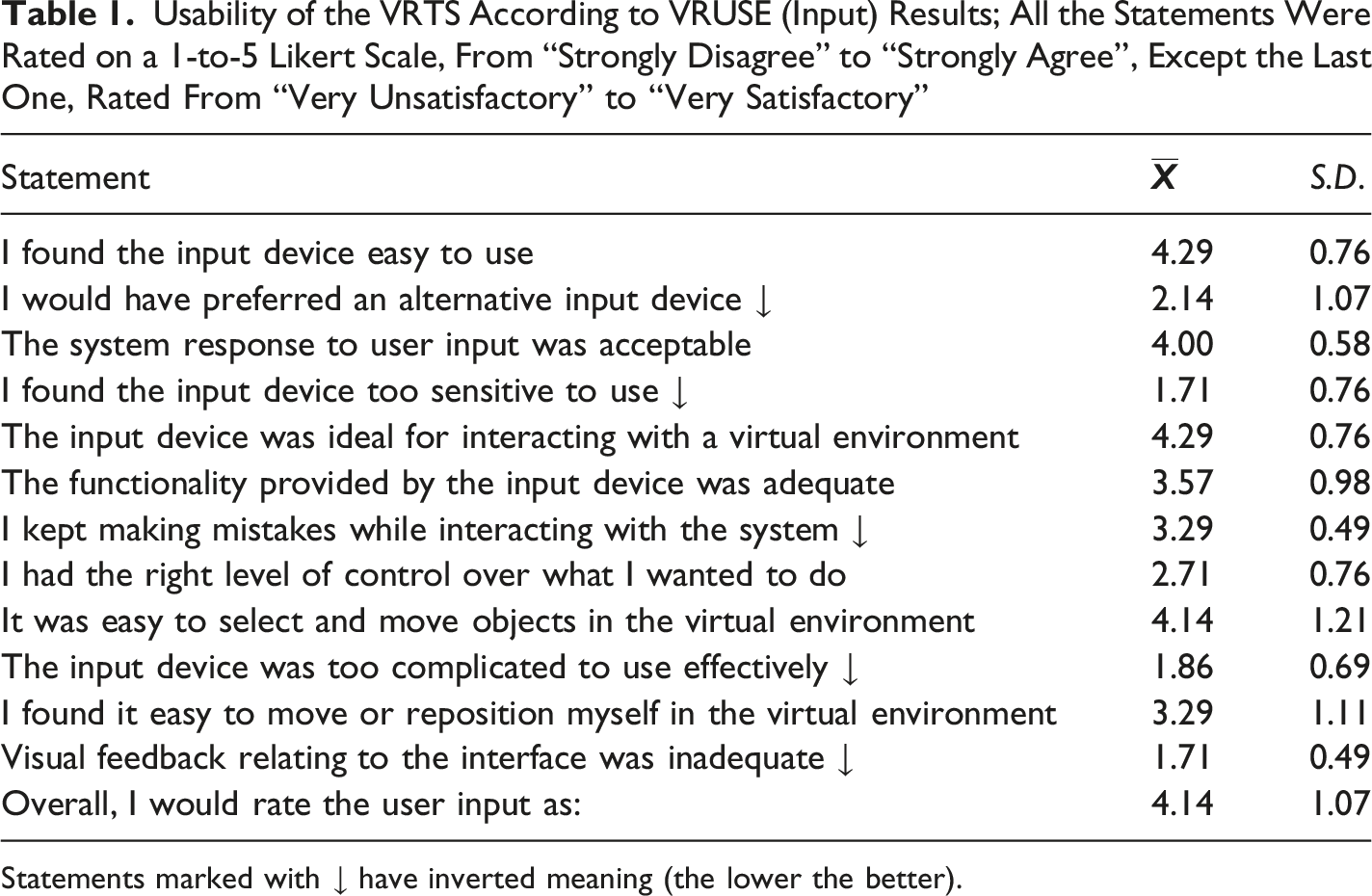
Statements marked with ↓ have inverted meaning (the lower the better).
Scores are generally satisfactory, with an overall Input Usability score of
The score for the question “I kept making mistakes while interacting with the system” (
Motivation at Learning
Motivation at Learning According to IMMS Results; its 36 Statements Were Rated on a 1-to-5 Scale
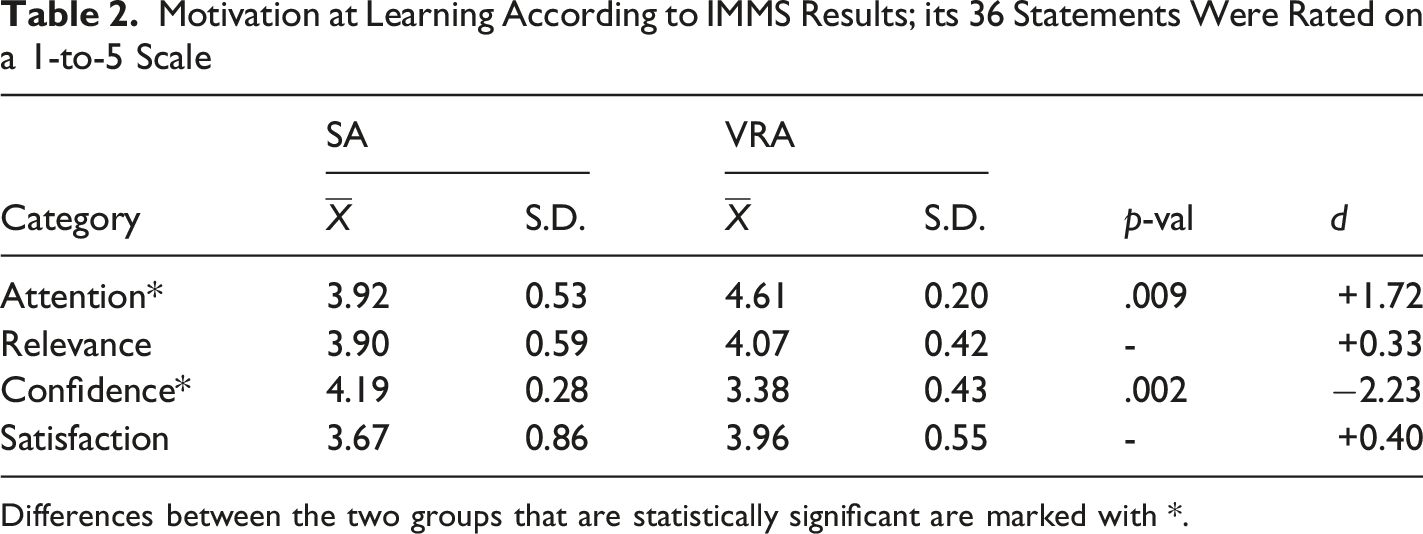
Differences between the two groups that are statistically significant are marked with *.
Statistically significant differences between groups were found for the Attention category, where the VRA group scored higher than the SA group, and for the Confidence category where, in contrast, the VRA group scored lower than the SA group. These results might initially seem contradictory, as the VRA participants reported being more attentive during the training session yet generally felt less confident.
However, this pattern is highly consistent with research on metacognitive calibration and desirable difficulties (Burson et al., 2006; Ehrlinger et al., 2008; Stanton et al., 2021). These frameworks suggest that active, hands-on engagement can increase a learner’s awareness of procedural complexity and effectively reduce overconfidence. In contrast, passive observation may foster an illusion of competence by cognitively simplifying the task demands. Therefore, the lower confidence reported by VR-trained participants may reflect a more realistic self-assessment rather than reduced preparedness. This, in turn, suggests better metacognitive calibration in the VRA group, particularly given that these participants demonstrated superior procedural skills during the in-vivo practical evaluation despite their lower initial confidence.
Furthermore, the lower confidence reported by the VRA group may also reflect differences in the educational activity. While the SA group received a brief Q&A session after their lecture, the VRA group did not have an equivalent opportunity for instructor-led clarification. This asymmetry may have contributed to differences in perceived clarity or reassurance, further complementing the metacognitive explanation that hands-on exposure independently increases awareness of procedural complexity.
Cognitive Load
Cognitive Load Based on Questionnaires Administered After the training Session (Post-Training) and After the Practical Evaluation (Post-Evaluation)
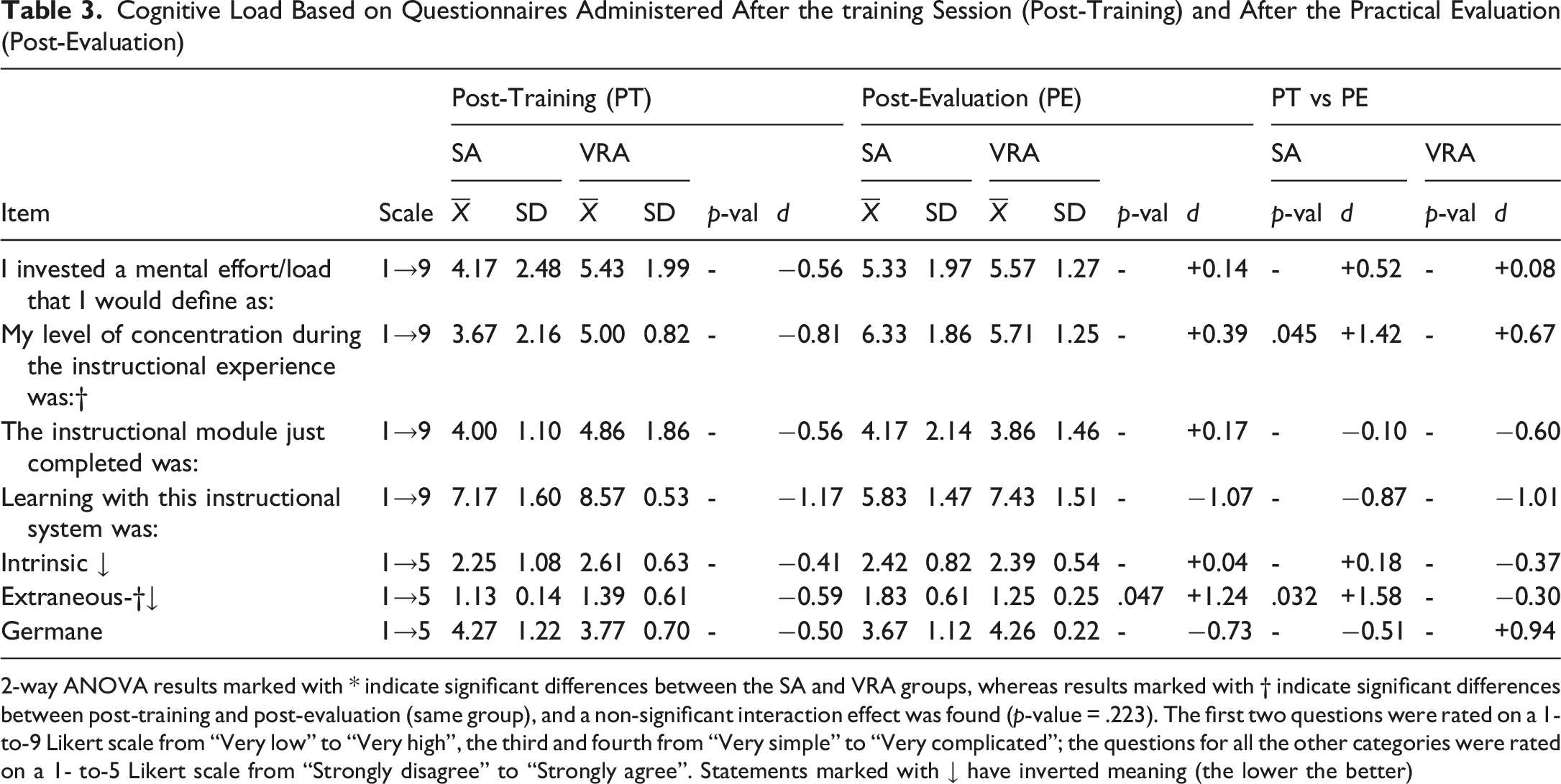
2-way ANOVA results marked with * indicate significant differences between the SA and VRA groups, whereas results marked with † indicate significant differences between post-training and post-evaluation (same group), and a non-significant interaction effect was found (p-value = .223). The first two questions were rated on a 1-to-9 Likert scale from “Very low” to “Very high”, the third and fourth from “Very simple” to “Very complicated”; the questions for all the other categories were rated on a 1- to-5 Likert scale from “Strongly disagree” to “Strongly agree”. Statements marked with ↓ have inverted meaning (the lower the better)
However, a significant difference in cognitive load emerged after the practical evaluation, with participants in the SA group reporting a higher degree of extraneous cognitive load in comparison to participants in the VRA group. It is worth recalling that this dimension of cognitive load encompasses factors related to the learning materials and environment, along with any external distractions that might impact concentration. The lower value associated with this dimension during the practical session with live horse for the participants in the VRA group can be attributed to the fact that they were already familiar with the operation of the endoscope, practiced during the VR training. The participants in the SA group, conversely, used the endoscope for the first time during the practical evaluation, a fact that likely contributed to increase their extraneous cognitive load. It can be speculated that another factor potentially contributing to the lower extraneous cognitive load observed in the VRA group is the increased familiarity with operating in close proximity to a large animal, an experience they had, at least virtually, during the simulation. In contrast, for the SA participants, their first direct interaction with a large animal may have had an emotional impact, potentially acting as a source of distraction and leading to reduced concentration during the procedure.
Further statistically significant differences were found comparing the results of the post-training and post-evaluation questionnaires for the same group. In fact, the participants in the SA group reported a higher level of attention - as indicated by question “My level of concentration during the instructional experience was” - and extraneous cognitive load after the practical evaluation than after the training session. These differences were not observed for the VRA group. This finding seems to indicate that the VRTS might be regarded as valuable tool for the considered training in this endoscopy context since, unlike the conventional lecture-based method, it can offer an experience akin to the real-life procedure.
Practical Evaluation
Practical Evaluation Results
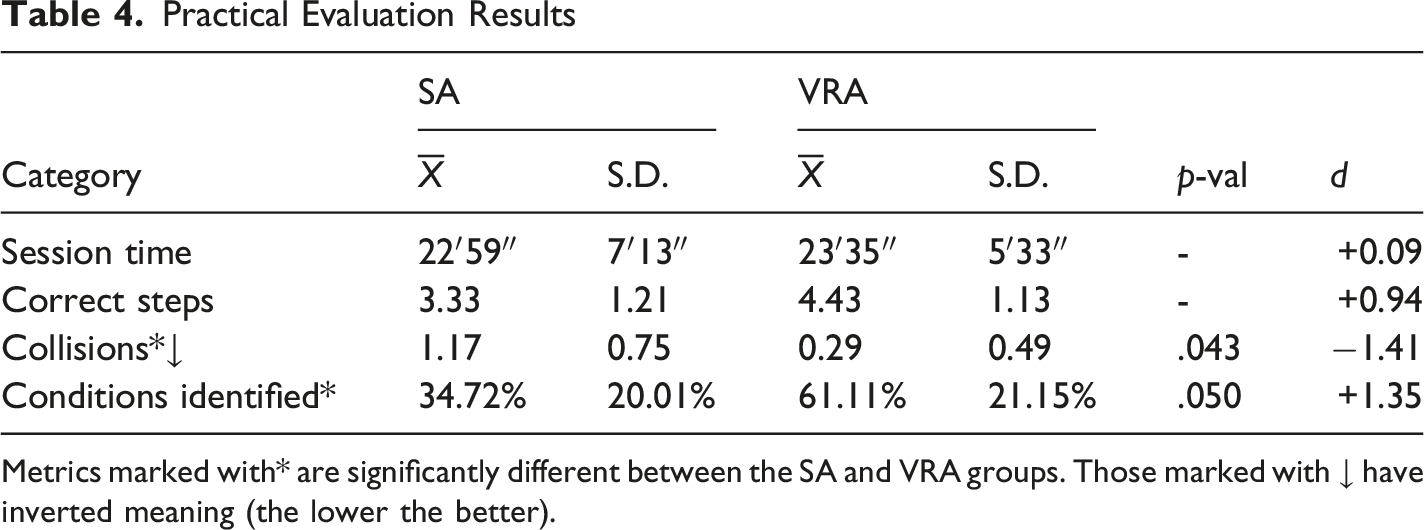
Metrics marked with* are significantly different between the SA and VRA groups. Those marked with ↓ have inverted meaning (the lower the better).
The domain expert reported the number of collisions with internal walls for each user. This metric is of particular importance, since avoiding collisions with internal walls denotes dexterity with the endoscope and, at the same time, prevents possible injuries and discomfort for the animal. For this metric it was found that the participants in the VRA group performed significantly better than those in the SA group (p = .043, d = −1.41), meaning that the VRTS successfully taught them how to handle the endoscope and navigate the horse’s anatomy. This outcome is coherent with the high scores for the usability of the VRTS in terms of input that emerged from the VRUSE questionnaire.
It is worth noting that a couple of qualitative learning transfers between the VR training phase and the in-vivo assessment were observed for the VRA. The first concerned the transfer of direct motor control. Although participants were required to verbally instruct a confederate for safety reasons, they also physically manipulated the same proximal portion of the endoscope that they had trained with in VR, and it was observed that the direct motor control developed (using hand-held controllers) bridged to the physical dexterity required to manually operate the real endoscope during the live evaluation.
The second transfer related to the in-vivo requirement to verbally direct the confederate to advance the insertion tube, as participants were able to demonstrate skill transfer within a distinctly different task format, which blended spatial navigation, communication, and supervision.
While this hybrid task format introduces a potential confounding factor, it is worth recalling that the confederate acted as a mere executor of the participants’ instructions. As a result, performance indicators such as the number of collisions reflected the participants’ own control actions indeed combined with the navigational decisions and ability to communicate them. Furthermore, to minimize any secondary variability in how instructions were received and executed, the same well-trained confederate was used across all exposures. The fact that VR-trained participants showed significant advantages in avoiding collisions despite this transfer gap suggests that the procedural understanding acquired during VR training transferred meaningfully to the real-world clinical task.
The participants in the VRA group also identified a greater proportion of the horse’s conditions than those in the SA group. While promising, this finding was only borderline significant, albeit with a large effect size (p = .050, d = +1.35). This result seems to suggest that the reproduction of the various conditions in the VRTS achieved an appropriate level of realism for effective diagnostic training. Moreover, encountering the conditions in the context of the interactive VR experience likely helped the users in remembering and recognizing them better than just relying on the images and videos used during the traditional lecture.
In summary, these results suggest that the training with the VRTS could represent a valid alternative to traditional methods for effectively teaching veterinary participants the diagnostic knowledge and skills needed to perform equine endoscopy.
Conclusions, Limitations and Future Work
This paper presents a VRTS developed as an alternative to conventional educational practice to support veterinary participants in acquiring the competences required for performing equine respiratory endoscopy. The investigation focused on a population of veterinary participants enrolled in a university course and involved a comparative analysis between this novel instructional approach and a traditional lecture-based method. The evaluation relied on both questionnaire-based assessments and objective metrics collected during an in-vivo study conducted by a domain expert and involving ill horses.
The experimental results indicated that the proposed approach was satisfactory in terms of usability. Participants trained with the VRTS tended to demonstrate more controlled procedural skills and higher diagnostic accuracy compared to those who received traditional training. Training time and cognitive effort were comparable across both groups, although the VR-trained participants showed advantages in attention and extraneous cognitive load at the evaluation time of the in-vivo procedure performance.
Despite these encouraging outcomes, the study has several limitations. A key limitation is posed by the relatively small sample size which constrains the statistical power of the findings to 75%. This was largely dictated by the nature of the study and, specifically, the limited availability of ill animals suitable for in-vivo evaluation (also considering the constraint of comparable conditions across specimens) and the need to guarantee minimal standards for the animal welfare (as prescribed by the informed consent collected from each specimen’s owner). Moreover, due to practical and organizational constraints, including those mentioned above, it was not possible to include a delayed follow-up evaluation in the study design to assess medium- or long-term retention of competencies. Although this choice is in line with other studies on virtual endoscopy (Cassidy et al., 2022), it leaves open the question of how well the acquired skills persist over time, which warrants further investigation, especially given that such data are not available for either the evaluated VRTS-based training protocol or the standard educational practice (SA).
Also, although the use of consumer-grade hardware makes the VRTS scalable and suitable for diverse educational contexts (and was positively received by participants, as reflected in usability scores) it may not fully replicate the haptic experience of clinical practice. It is plausible that, despite the positive learning transfer, the differences between the VR controllers and a real-world endoscope may still have resulted in some reduced learning gains in terms of dexterity, compared to what could be achieved using specialized hardware as demonstrated in previous studies (McCool et al., 2022; Xu et al., 2025). An additional limitation stems from the in-vivo assessment methodology, which introduced inherent variability that may have affected the sensitivity of the evaluation. Specifically, the inability to reuse a single ill horse required the use of four different specimens. Although appropriate care was taken to ensure a minimum subset of common clinical conditions and comparable specimen features across all selected specimens by allowing the course instructor to deliberately select the animals as to be representative and to ensure fairness across participants, there could be still some variability introduced by the intrinsic differences across not-clone animals. Moreover, even though appropriate care was taken to effectively minimize the impact of the subjective component of the single-evaluator on the scoring by explicitly avoiding heuristic or holistic assessment in favour of a more structured feedback via checklist of observable events, it is still worth mentioning that the inclusion of a second evaluator would have been a valuable methodological addition to further bolster the robustness of the assessment and relax the constraint of the structured feedback enabling to collect more nuanced evaluations. It can be speculated that any future fluctuations in the number of identified conditions are unlikely to be substantial enough to reverse the observed trends.
Another limitation is posed by the scope of this study. The proposed experiment design aimed to support an ecological evaluation of the VRTS-based activity against the current educational status quo. Although the VRA group engaged in more hands-on practice than the SA group, this increased exposure was not incidental but a direct consequence of the integration of the VRTS tool in the learning format for the sake of evaluating it in an ecologically relevant setting. The goal was to assess whether the VRTS could serve as an effective and practical solution to the severe logistical and ethical constraints inherent in teaching this endoscopy procedure, thereby providing actionable evidence to inform faculty members and decision-makers. The experiment design contrasts a more active, VR-based modality (VRA) against a more passive, lecture-based approach (SA), precluding the possibility of disentangling the specific contribution of VR from the broader benefits of hands-on practice (active vs passive learning. The observed performance differences should therefore be interpreted as evidence of the potential of the devised VRTS tool to overcome structural constraints in veterinary education (logistical, ethical, etc.) rather than as a definitive comparison of VR versus non-VR media in educational settings. Indeed, providing equivalent practical experience outside of simulation is challenging, and in this context, VR offers a practical way to deliver scalable and repeatable practice opportunities that would otherwise be difficult to provide.
To address these limitations, future studies, should also aim at disentangling the effect of passive/active training practice and the effect of VR vs non-VR media, by incorporating larger samples, delayed follow-up assessments, and utilize conditions that offer comparable levels of active engagement to more precisely isolate the added value of immersion and interacting factors.
Also, future experiments should potentially include students from multiple institutions. To mitigate the dexterity-related constraints introduced by VR controllers, a physical mockup of a sensorized endoscope will be integrated with the virtual endoscope logic to enhance the fidelity of the VR experience. This change in interaction modality will require additional validation to assess the contribution of the custom haptic interface. Another improvement, which has already been implemented in the course following this study, is the inclusion of a preparatory phase in which students interact with a real endoscope to practice gear-based control and use a horse nose mannequin to rehearse nostril insertion. It is also forecasted to widen the set of pathological conditions that can be encountered, as well as to integrate the non-technical facets of veterinary examinations, encompassing the simulation of clinical case presentations, history acquisition, and effective communication with animal owners, both prior to and following the endoscopy procedure. Finally, while the presence of the confederate was necessary for this evaluation study design to minimize potential confounding factors at assessment time, communication and team dynamics are relevant aspects which students are indeed expected to be trained on in the future. To this aim it is planned to extend the experimental evaluation to dyadic practice with pairs of students interpreting the role of two operators both working in VR, as this would recreate a setup that is common in real-world practice and known to increase performance (Nilsson et al., 2017).
To conclude, since the effectiveness and integration of VRTS tools in educational practice is dependent on several factor (Pratticò & Lamberti, 2021; Van Gog & Rummel, 2010), it is the authors’ hope that the validation of this VRTS for veterinary education on large animal endoscopy procedures supports non-obvious findings and provides actionable evidence for veterinary faculty members and policymakers who are eventually interested in the integration of this kind of tool into the teaching practices of veterinary higher education.
Footnotes
ORCID iDs
Ethical Considerations
The procedures involving animals in this study were conducted in accordance with relevant institutional and national guidelines for the ethical treatment of animals. The procedures performed in this study did not fall into a category requiring formal approval by a dedicated ethics committee. All operations were performed at the Equine Veterinary Teaching Hospital of the University of Turin and supervised by qualified veterinary staff, ensuring the highest standard of care and animal welfare.
Consent to Participate
Written informed consent was obtained from the owner of each animal (horses) for all the operations performed in clinical settings.
Author Contributions
Funding
The authors received no external financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data collected in the current study and software used are available from the corresponding author upon reasonable request.