
Abstract
Immersive learning environments are increasingly being implemented in high-stress contexts; however, many designs emphasize technological affordances rather than theoretically grounded motivational support. Guided by self-determination theory (SDT), this study developed a need-supportive immersive learning design model, referred to as self-determination theory–based virtual reality learning (VR-SDT), that intentionally integrates autonomy, competence, and relatedness into interactive, scenario-driven experiences. A randomized controlled study involving 84 ICU patients with coronary heart disease compared an immersive SDT-based VR learning condition (VR-SDT) with a non-immersive app-based SDT-informed instructional condition (App-SDT). Results indicated that participants in the VR-SDT condition achieved significantly higher knowledge (F = 84.23, p < .001) and self-efficacy (t = 7.96, p < .001) than those in the App-SDT condition. Anxiety reduction was also significantly greater in the VR-SDT condition (t = −8.86, p < .001). These findings suggest that an immersive learning design informed by SDT principles may support improvements in disease-related knowledge, self-efficacy, and anxiety in high-stress learning contexts, while providing theoretically grounded guidance for the design of immersive learning systems.
Keywords
Introduction
Immersive learning environments are increasingly recognized for their role in helping learners navigate complex, emotionally charged, or highly stressful situations (Meese et al., 2021; Milasan et al., 2024; Rajabi et al., 2022; Ristor et al., 2023). By leveraging presence, interactivity, and embodied experiences, immersive technologies such as virtual reality (VR) offer unique pedagogical advantages for experiential learning (Meese et al., 2021). However, despite rapid technological advancements, most existing immersive learning designs remain technology-driven, rather than grounded in explicit theoretical frameworks. The underlying mechanisms by which such systems influence learners’ learning outcomes often lack systematic theoretical interpretation, with particular gaps in the motivational process dimension (Radianti et al., 2020). Research indicates that learning theories are frequently under-integrated in VR application development, resulting in designs that fail to effectively guide and support the achievement of intended learning outcomes (Radianti et al., 2020). Therefore, advancing educational computing research requires not only the development of immersive technologies, but also the establishment of theoretically grounded design frameworks to explain how and why such environments support learning.
Self-determination Theory (SDT) provides a well-established motivational framework for understanding how learning environments influence engagement, internalization, and self-regulatory behaviors. SDT posits that three fundamental psychological needs—autonomy, competence, and relatedness–are essential for fostering intrinsic motivation (Deci & Ryan, 1985). When these needs are met in a learning environment, individuals are more likely to experience deeper engagement, sustain their effort, and effectively regulate their emotional responses. In the educational and health settings, SDT-based interventions have been associated with enhanced knowledge acquisition, adherence, and self-efficacy. When learners perceive autonomy support, they are more likely to actively engage in learning tasks and internalize health-related information, thereby facilitating meaningful knowledge acquisition. Competence-supportive experiences, such as progressive feedback and successful task completion, may strengthen individuals’ beliefs in their ability to manage health-related challenges, contributing to improved self-efficacy. In addition, relatedness-supportive interactions and emotionally supportive environments may help reduce uncertainty and emotional distress, thereby alleviating anxiety in stressful learning situations. Such motivational and emotional regulation processes contribute to reinforcing long-term health care behaviors and promoting overall health (Saeedian et al., 2025; Sarboozi Hosein Abadi et al., 2020; Shackleford et al., 2019). However, most current SDT-based teaching methods rely on lectures, audiovisual media, and educational booklets (Saeedian et al., 2025; Shi et al., 2022). These formats offer limited opportunities for interactive choices, progressive mastery experiences, and relational engagement, potentially failing to effectively meet learners’ psychological needs while constraining their motivation and sense of active participation (Shi et al., 2022). Consequently, research on translating SDT principles into immersive and interactive system designs remains insufficient.
In high-stress health care settings, a theory-guided immersive learning design is crucial. Many individuals admitted to the Intensive Care Unit (ICU) for acute cardiac conditions remain fully conscious and are required to process complex treatment-related information and participate in health-related decision-making. When patients experience acute medical events requiring ICU admission, they often experience heightened anxiety and uncertainty while bearing a significant cognitive load (Alzahrani, 2021; Wang et al., 2025). High anxiety is not merely an emotional response; it also consumes working memory resources, disrupts attentional control, and interferes with knowledge integration and decision-making processes (Vince, 1998). Consequently, patients may struggle to effectively process critical health-related information under such conditions, despite needing to understand medical procedures, postoperative care, and self-management strategies during a highly stressful period. Research indicates that acknowledging and regulating emotional responses, rather than suppressing negative emotional experiences, can promote deeper reflection and adaptive behavioral adjustments (Chen et al., 2020; Vince, 1998; Zou et al., 2023). Providing clear, accurate, and contextually relevant information helps reduce uncertainty and promotes patient engagement in treatment-related decisions (Cuzco et al., 2022). However, in high-stress settings, an effective learning system cannot be limited to information delivery; it must also regulate emotions and deliberately address learners’ psychological needs. Therefore, developing immersive learning environments that integrate motivational principles and emotion-responsive design is essential for supporting learning and emotional adaptation in high-stress settings, including outcomes related to disease knowledge, self-efficacy, and anxiety reduction.
VR enables the construction of highly immersive and interactive learning environments, offering a unique opportunity to implement need-supportive design principles in interactive experiences. Through scenario-based simulations, learners can engage in first-person exploration, make meaningful choices, receive progressive feedback, and interact with empathetic virtual agents (Aardoom et al., 2022; Lin et al., 2025). These characteristics conceptually align with design features intended to support autonomy, competence, and relatedness. However, whether immersive VR environments actually satisfy these psychological needs and whether such support contributes to measurable cognitive and affective benefits remain to be empirically verified.
Therefore, this study developed a need-supportive immersive learning design model based on SDT, referred to as the “self-determination theory-based virtual reality learning model.” In addition, the cognitive affective model of immersive learning (CAMIL) was adopted as a conceptual interpretive lens for discussing potential cognitive and affective processes associated with immersive learning reported in prior literature, rather than as an integrated or empirically tested model in this study. Through narrative design, this model integrates autonomy, competence, and relatedness into an interactive, context-driven VR experience. To validate the system’s effectiveness, a randomized controlled trial was conducted in a high-stress medical learning environment. ICU patients were assigned to either the immersive VR-SDT learning (VR-SDT) mode or the app-based SDT-informed (App-SDT) learning mode. This study evaluated the effectiveness of an immersive intervention designed according to SDT principles by comparing groups’ learning outcomes related to disease knowledge, self-efficacy, and anxiety in a high-stress medical learning context. The research questions are as follows. (1) Can the VR-SDT mode improve ICU patients’ coronary heart disease (CHD) knowledge compared with the App-SDT mode? (2) Can the VR-SDT mode reduce anxiety in ICU patients compared with the App-SDT mode? (3) Can the VR-SDT mode enhance ICU patients’ self-efficacy compared with the App-SDT mode?
Literature Review
Immersive Learning Environments
Immersive learning environments refer to digital learning spaces that leverage immersive technologies, such as virtual reality, augmented reality, or mixed reality, to create highly presence-rich, interactive, and embodied environments (Seprum & Wongwatkit, 2025). Learners engage in scenario-based tasks from a first-person perspective, integrating their cognitive and affective processes through contextualized and embodied experiences. These environments enhance experiential learning and contextual understanding through sensory engagement and real-time feedback mechanisms, thereby gaining increasing attention in educational technology (Meese et al., 2021; Milasan et al., 2024; Rajabi et al., 2022; Ristor et al., 2023). Immersive systems can promote active exploration, contextual understanding, and deep engagement by placing learners in simulated scenarios that approximate the real world. Previous research has indicated that higher immersion levels in an immersive virtual solar system exploration course effectively boost learning motivation and participation, thereby enhancing learning outcomes (Huang et al., 2021). In another study using immersive VR as an earthquake safety education tool, immersive experiences were found to reduce anxiety and enhance safety decision-making capabilities more effectively than traditional face-to-face instruction (Rajabi et al., 2022). Furthermore, literature reviews indicate that immersive VR simulations mitigate the negative effects of stress in clinical and training settings while improving performance and emotional responses (Meese et al., 2021). Empirical and review studies have consistently demonstrated that immersive learning exerts significant positive effects on knowledge acquisition, learning engagement, and emotional regulation (Huang et al., 2021; Makransky & Petersen, 2021; Petersen et al., 2022; Radianti et al., 2020).
However, recent research has gradually shifted focus from the technology itself to the underlying psychological mechanisms. CAMIL has been proposed as a conceptual framework which suggests that immersive learning outcomes may be associated with a range of cognitive and affective processes (Makransky & Petersen, 2021). In the present study, CAMIL was used only as a conceptual lens for interpreting immersive learning processes discussed in prior literature, rather than as a directly tested explanatory model. Similarly, related studies have found that immersion and interactivity do not directly produce learning outcomes. Instead, they influence the learning process through psychological mechanisms such as attention allocation, cognitive load regulation, emotional arousal, and motivation (Parong & Mayer, 2021; Petersen et al., 2022). Therefore, the educational value of immersive technology does not stem from the technology itself but rather depends on whether its design features align with established learning and motivation theories.
Self-Determination Theory (SDT)
SDT provides a comprehensive framework for explaining how social and instructional environments influence individuals’ motivation, engagement, and self-regulatory behaviors (Deci & Ryan, 1985). SDT posits that when learning situations support three fundamental psychological needs–autonomy, competence, and relatedness–individuals are more likely to exhibit high-quality intrinsic motivation, sustained engagement, and deep learning (Ryan & Deci, 2000, 2017). When learning environments support these needs, learners are more likely to internalize extrinsic goals, develop adaptive emotion-regulation skills, and demonstrate perseverance during challenging tasks. Empirical research on health education supports the applicability of SDT-based interventions. For instance, Zhang et al. (2025) demonstrated that an SDT-based educational program significantly enhanced dialysis knowledge and self-management skills among hemodialysis patients. Similarly, Guo et al. (2023) showed that needs-supportive education for liver transplant recipients promotes the internalization of health-related behaviors and increases self-efficacy. These findings indicate that interventions based on SDT effectively enhance engagement, self-management, and motivational regulation in health-related learning contexts (Guo et al., 2023; Saeedian et al., 2025; Zhang et al., 2025).
Despite its solid theoretical and empirical foundations, SDT has primarily focused on instructional behaviors or interpersonal interactions in educational and health settings, with limited extension to system-level design features within digital learning environments (Al-Hoorie et al., 2025; Orsini et al., 2016). Prior SDT research has emphasized the importance of clearly specifying theory-aligned motivational support strategies to ensure conceptual consistency between intervention design and theoretical mechanisms (Ahmadi et al., 2023). Emerging research in recent years indicates that integrating SDT principles into digital interface designs, such as organic user interfaces, mixed reality, and human-robot interaction systems, can transcend mere novelty effects. This approach promotes the internalization of motivation, leading to sustained behavioral changes and deeper learning engagement (Alberts et al., 2024).
Immersive environments can support autonomy by offering learning path choices, pacing control, and situational decision-making opportunities (Patall et al., 2008; Reeve et al., 2004). Competence can be enhanced through task design, immediate feedback, and progressive scaffolding (Hattie & Timperley, 2007; Ryan & Deci, 2000), whereas relatedness can be strengthened through interactions with empathetic virtual characters and the creation of social presence (Klimmt et al., 2009; Oh et al., 2018). These design features are conceptually consistent with the prior immersive learning literature discussed in relation to CAMIL (Makransky & Petersen, 2021), which highlights the importance of cognitive and affective learning processes in immersive environments. Specifically, autonomy supportive experiences may facilitate learners’ active engagement and internalization of CHD-related knowledge, competence supportive interactions may strengthen self-efficacy through successful mastery experiences and feedback, and relatedness supportive environments may reduce anxiety by enhancing emotional support and familiarity with stressful clinical situations. Accordingly, SDT provides a theoretical basis for explaining how immersive learning environments may influence learning outcomes related to disease knowledge, self-efficacy, and anxiety in high-stress health care settings. To summarize, an immersive VR environment provides a feature-rich platform for implementing SDT principles through immersive, interactive, and embodied learning experiences.
The VR-SDT Learning System
In this study, we developed an immersive VR system based on SDT (VR-SDT) using CoSpaces Edu, designed specifically for high-stress learning environments. The structure of the system is shown in Figure 1. The learning system comprises an administrator interface, a learner interface, a CoSpaces VR database, a clinical case learning database, an SDT database, and a learning portfolio database. The CHD learning materials and clinical case scripts were integrated into the VR module through the administrator interface. Immersive scenarios and interactive tasks were designed according to the needs-supportive principles of autonomy, competence, and relatedness, enabling learners to experience and acquire knowledge regarding CHD, its treatment, and associated care within an ICU scenario. Learners accessed the virtual environment through a learner interface. They engaged in learning activities using interactive scenarios or objects embedded in the three core psychological needs of SDT. They were also required to respond to system-generated prompts. The learners’ operational processes and interactions were automatically recorded in the learning portfolio database. Structure of the VR-SDT learning system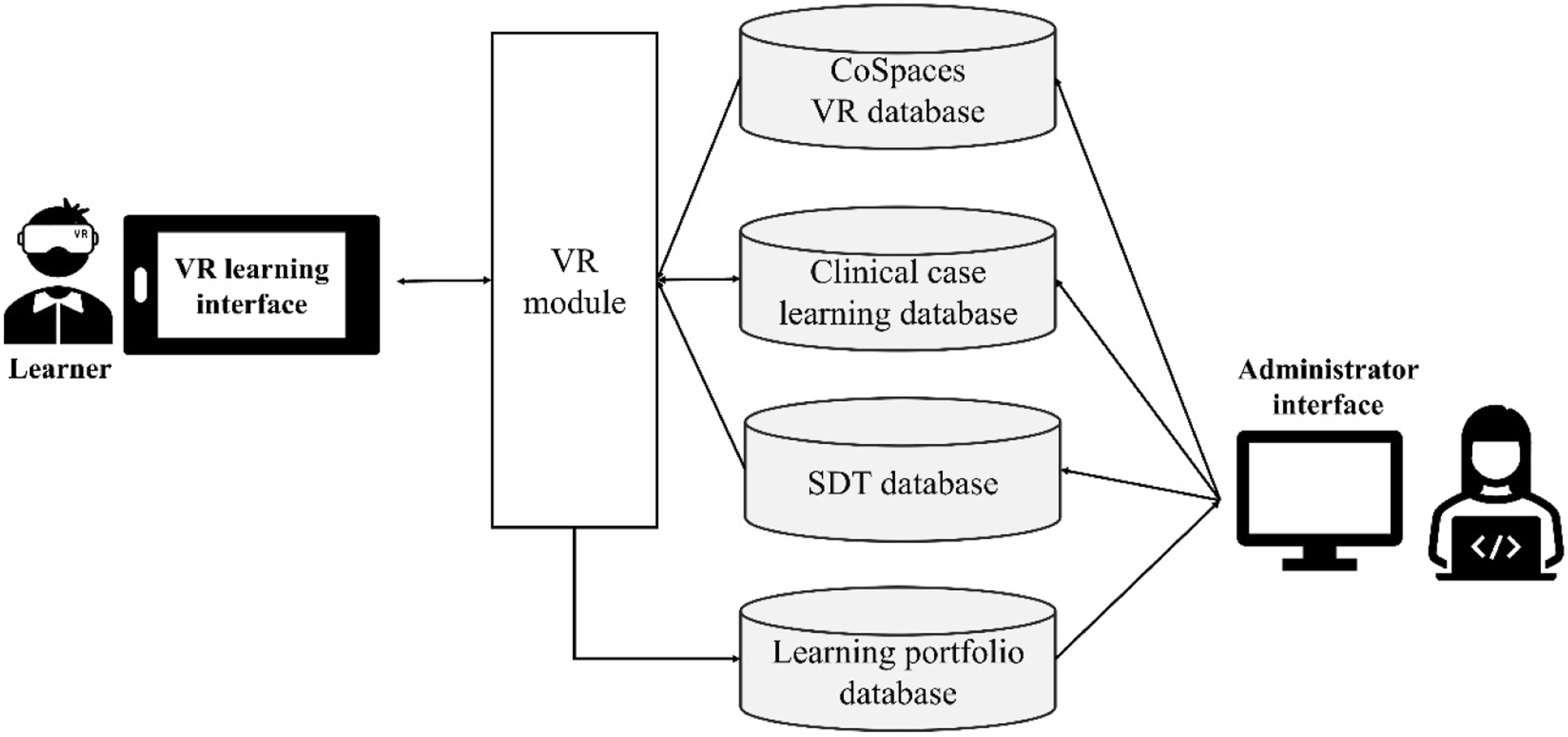
Psychological Needs of the VR-SDT Mode
The VR-SDT system was designed to address the three psychological needs of SDT by focusing on health education content related to the care of patients with CHD. Its primary objectives are to enhance patients’ understanding of the disease and its associated care, strengthen their confidence in health management, and promote sustained self-care, thereby reducing the risk of cardiovascular events and improving their quality of life. The health education content in this study was collaboratively developed by three experts with over 5 years of clinical and professional experience: a nursing instructor specializing in VR design, a cardiologist, and a senior ICU nurse.
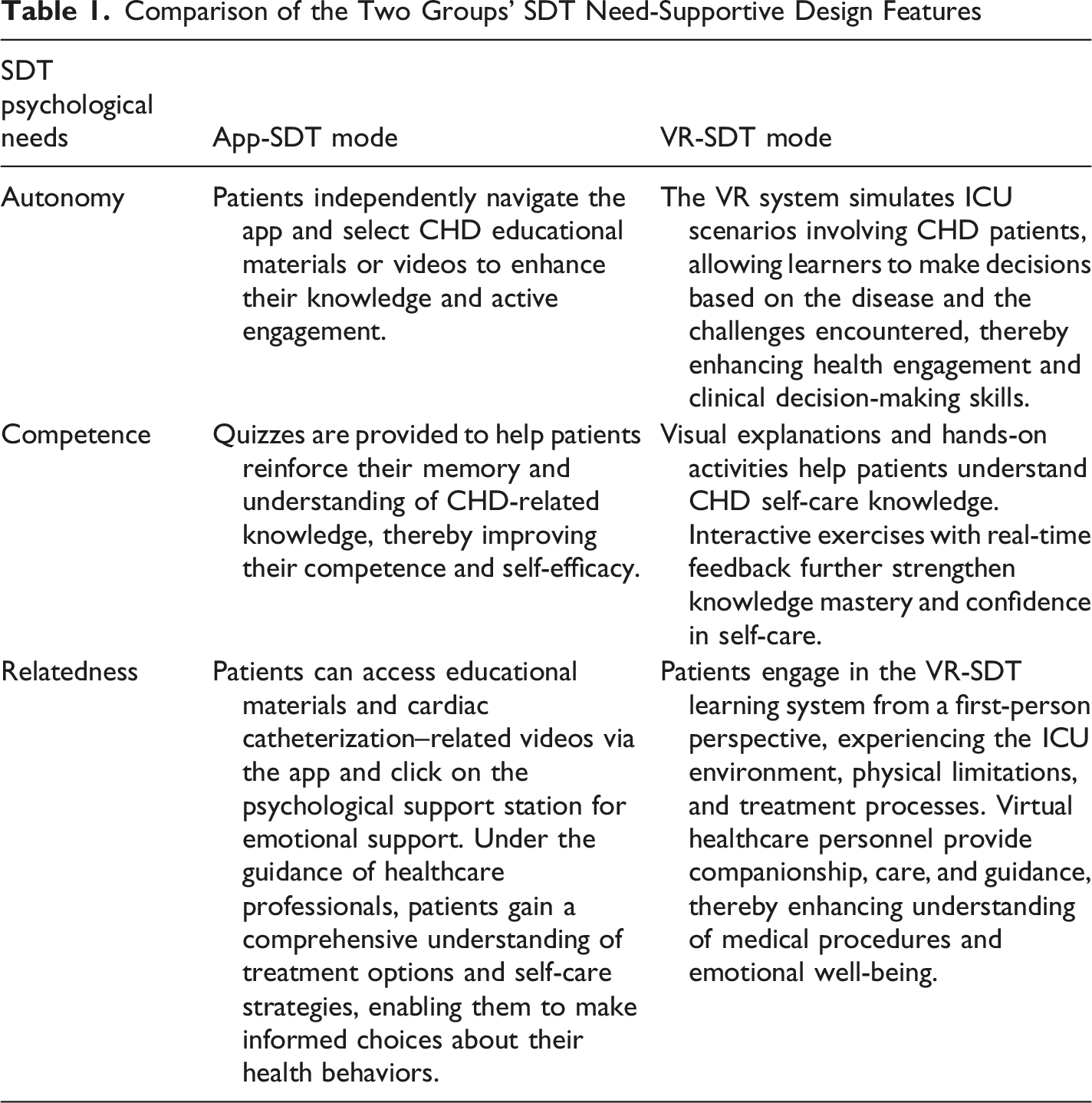
Comparison of the Two Groups’ SDT Need-Supportive Design Features
VR-SDT Learning Environment
The high-stress VR learning environment, designed around CHD care scenarios, and grounded in SDT, addresses three psychological needs (autonomy, competence, and relatedness) to enhance patient engagement and intrinsic motivation.
In terms of autonomy, the VR-SDT learning system simulated ICU clinical care scenarios, providing patients with opportunities to make choices and decisions that enhanced their participation in and motivation to engage in health behaviors (Figure 2). During the learning process, patients were able to make autonomous decisions in different situations, thereby strengthening their initiative in disease management. For example, through simulations of patient–provider shared decision-making, the VR system guided patients to explore various treatment options, including the advantages and disadvantages of medications and different cardiovascular stents (Figure 2(A)). This emphasizes that patients could make appropriate choices based on their preferences, evidence-based information, and medical advice, thereby increasing their engagement and agency in treatment (Figure 2(B)). Autonomy-supportive features of the VR-SDT learning environment. (A) Images presenting various treatment options in detail. (B) Supporting patient engagement in treatment decisions to enhance their agency. (C) An interactive feedback mechanism for users to receive immediate feedback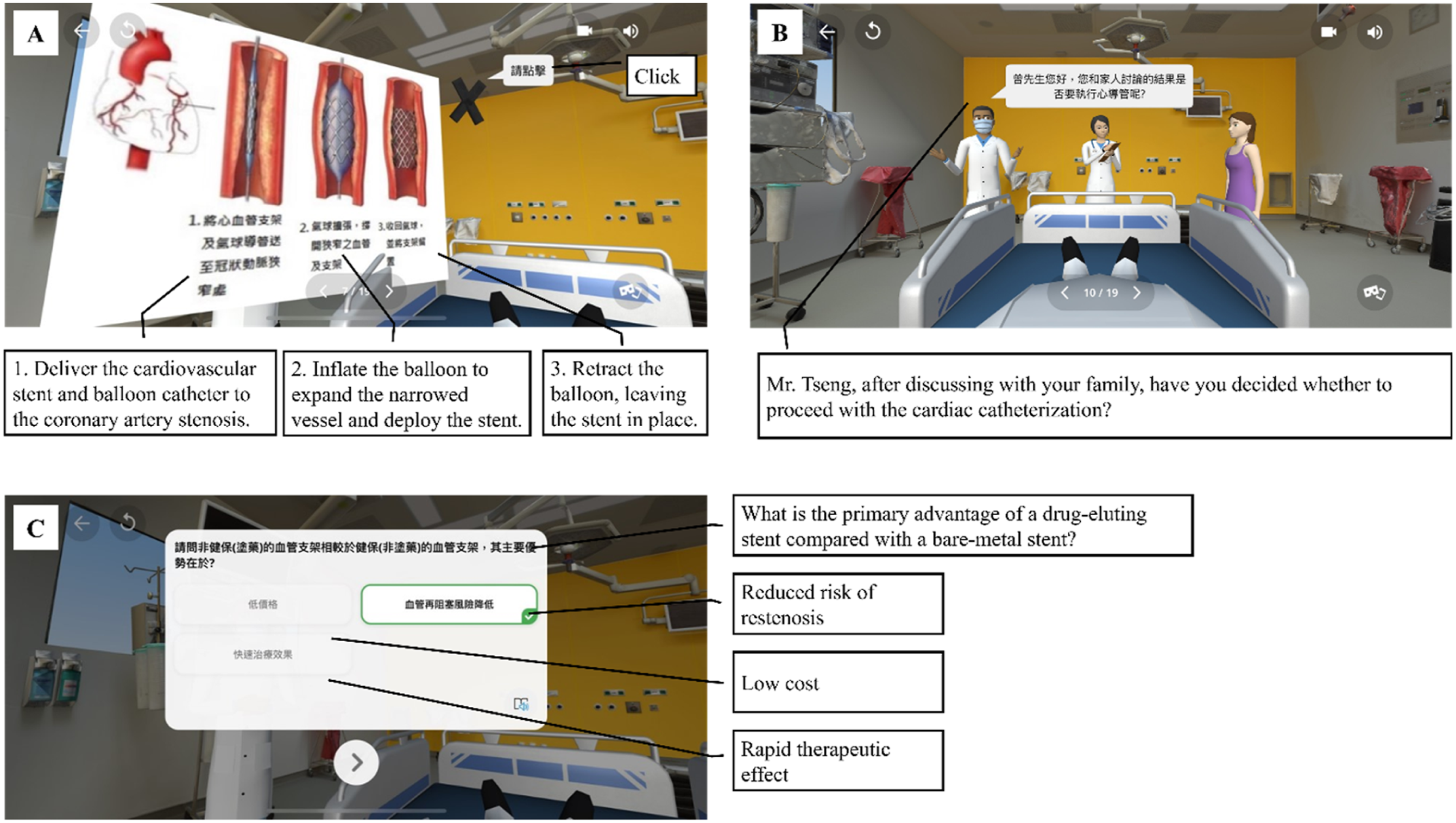
When explaining the cardiac catheterization procedure, the system provided detailed information on surgical risks, procedural steps, and preoperative instructions. It further simulates the process of signing an informed consent form, helping patients understand the relevant content and exercise their medical decision-making rights. The VR environment also incorporated postoperative care scenarios, presenting key aspects and precautions for self-care to promote patient self-management and autonomy after surgery. An interactive feedback mechanism was embedded throughout the learning process, allowing users to receive immediate feedback and guidance (Figure 2(C)). This supported the active correction of misconceptions and enhanced the learners’ agency and self-regulation skills.
Regarding competence, the VR-SDT learning system utilized visual explanations of medical knowledge and treatment procedures to help patients understand abstract health concepts, thereby strengthening their memory and application skills (Figure 3). In the simulated scenarios, patients encountered realistic situations following ICU admission, such as exposure to noise from medical equipment, feelings of isolation without family presence, physical restrictions (Figure 3(A)), and participation in the full process of cardiac catheterization. These experiences helped patients become familiar with the ICU environment and related medical procedures (Figure 3(B)), thereby reducing their anxiety and feelings of helplessness in unfamiliar settings, and enhancing their confidence and skills in health management and treatment compliance. Competence-supportive features of the VR-SDT learning environment. (A) First-person experience of physical limitations following ICU admission. (B) Simulation of the cardiac catheterization procedure. (C) Knowledge related to CHD self-management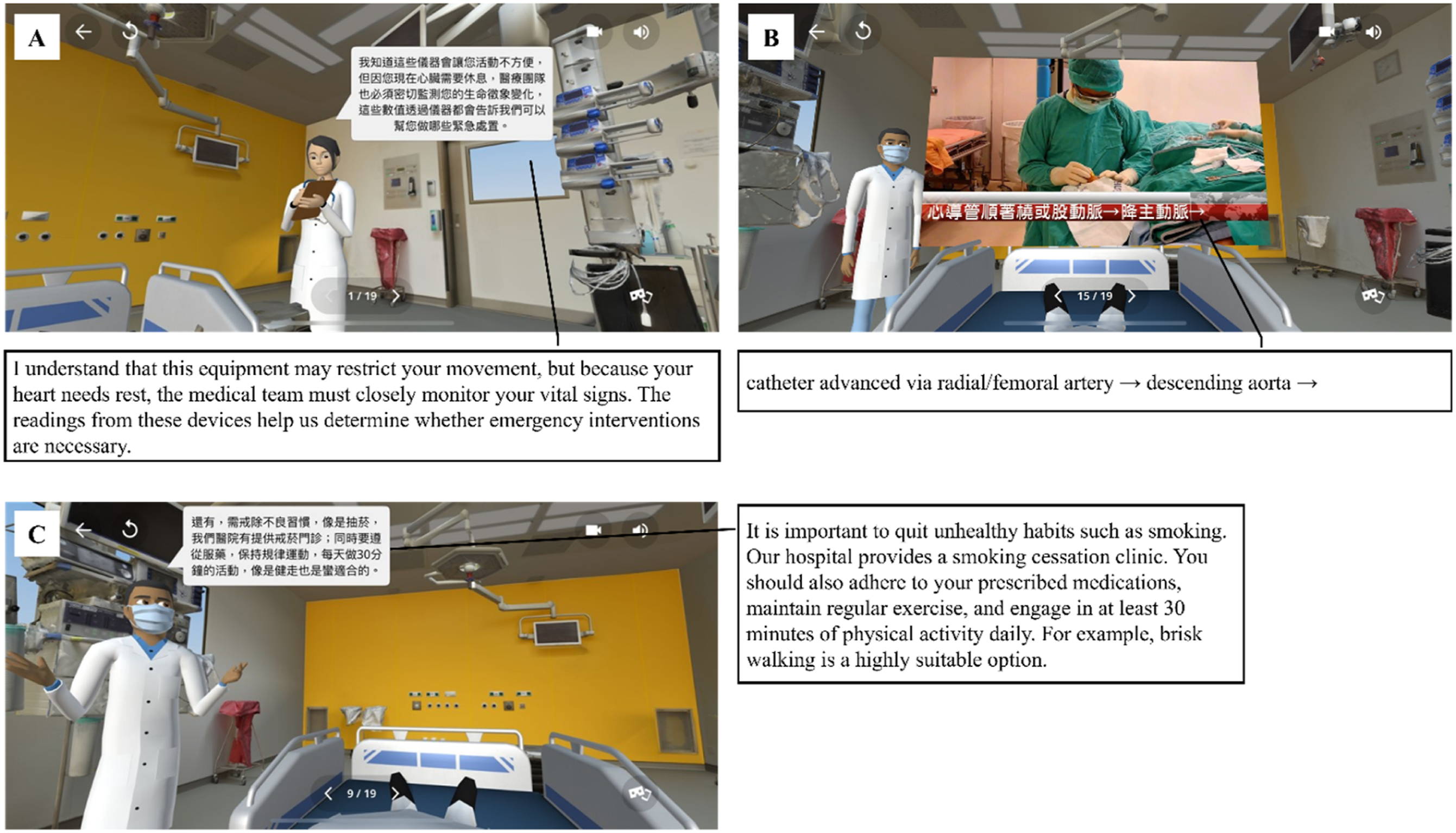
The system also integrates a real-time interactive assessment and feedback mechanism, enabling patients to evaluate their learning outcomes immediately, and correct their misconceptions to reinforce their understanding. Furthermore, the educational content included health promotion and preventive knowledge, such as dietary recommendations, exercise prescriptions, medication use, and lifestyle modifications (Figure 3(C)), to help patients recognize the impact of their daily behaviors on disease control and foster positive health beliefs and self-efficacy.
Regarding relatedness, patients engaged in the VR-SDT learning system from a first-person perspective, simulating the full ICU admission experience, including exposure to an unfamiliar environment, medical equipment, physical restrictions, and treatment procedures (Figure 4). Through the presence of virtual healthcare personnel providing companionship, care, and audio explanations, patients gained a deeper understanding of medical procedures while receiving emotional support and psychological reassurance (Figure 4(A)). Relatedness-supportive features of the VR-SDT learning environment. (A) Virtual healthcare personnel providing compassionate guidance and audio explanations. (B) ICU visitation regulations and precautions to encourage family participation in patient care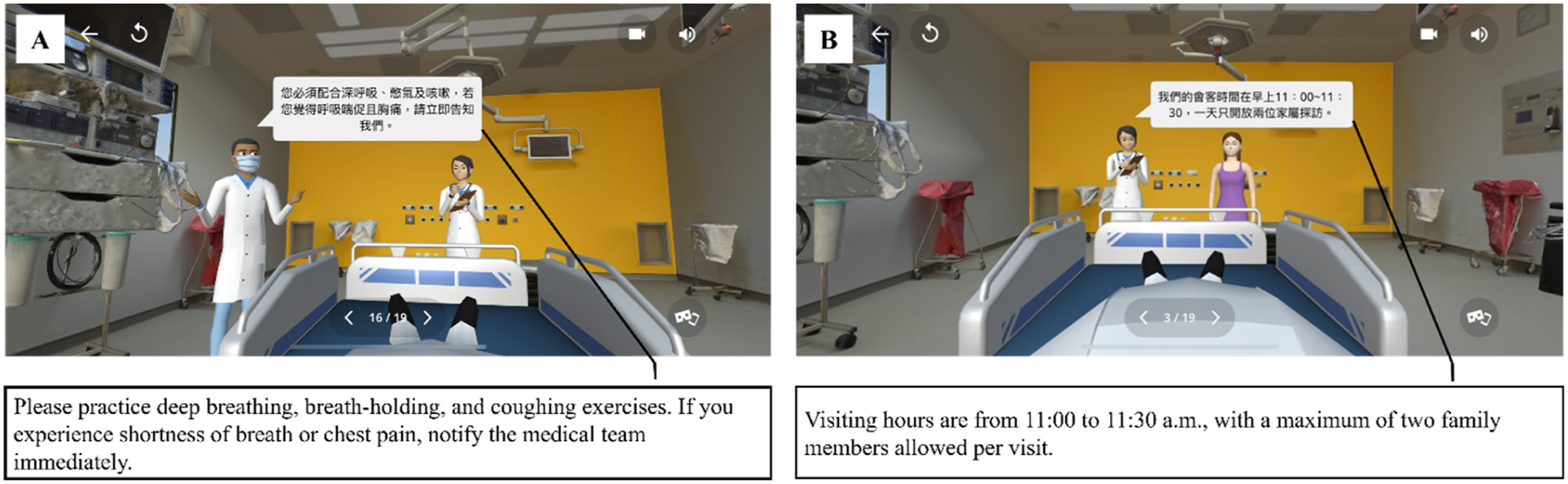
The system included scenarios in which healthcare personnel accompanied patients through surgical preparation, execution, and postoperative care, offering clear instructions and compassionate care. This created a sense of understanding and support, thereby reducing feelings of isolation and anxiety. Furthermore, by explicitly explaining the purpose of medical and care procedures, the VR system fostered patients’ trust in the medical team and their willingness to cooperate, promoting positive interactions between patients and providers. The educational content also introduced ICU visitation regulations and related precautions (Figure 4(B)), encouraging family members to understand and participate in the care process. This strengthened patients’ social support networks and enhanced their emotional connectedness and support.
Experimental Design
Participants
This study was conducted at a medical center in northern Taiwan and approved by the Institutional Review Board (IRB No. 24MMHIIS282e). Eligible participants were newly admitted ICU patients with CHD in the ICU who were over 18 years of age and fully conscious. Individuals with hearing or visual impairments were excluded from the study. All participants received a comprehensive explanation of the study before enrollment, including information that they would be randomly assigned to different learning modes and that their assigned mode would not affect the educational content or clinical care they received. Written informed consent was obtained from all participants prior to the experiment.
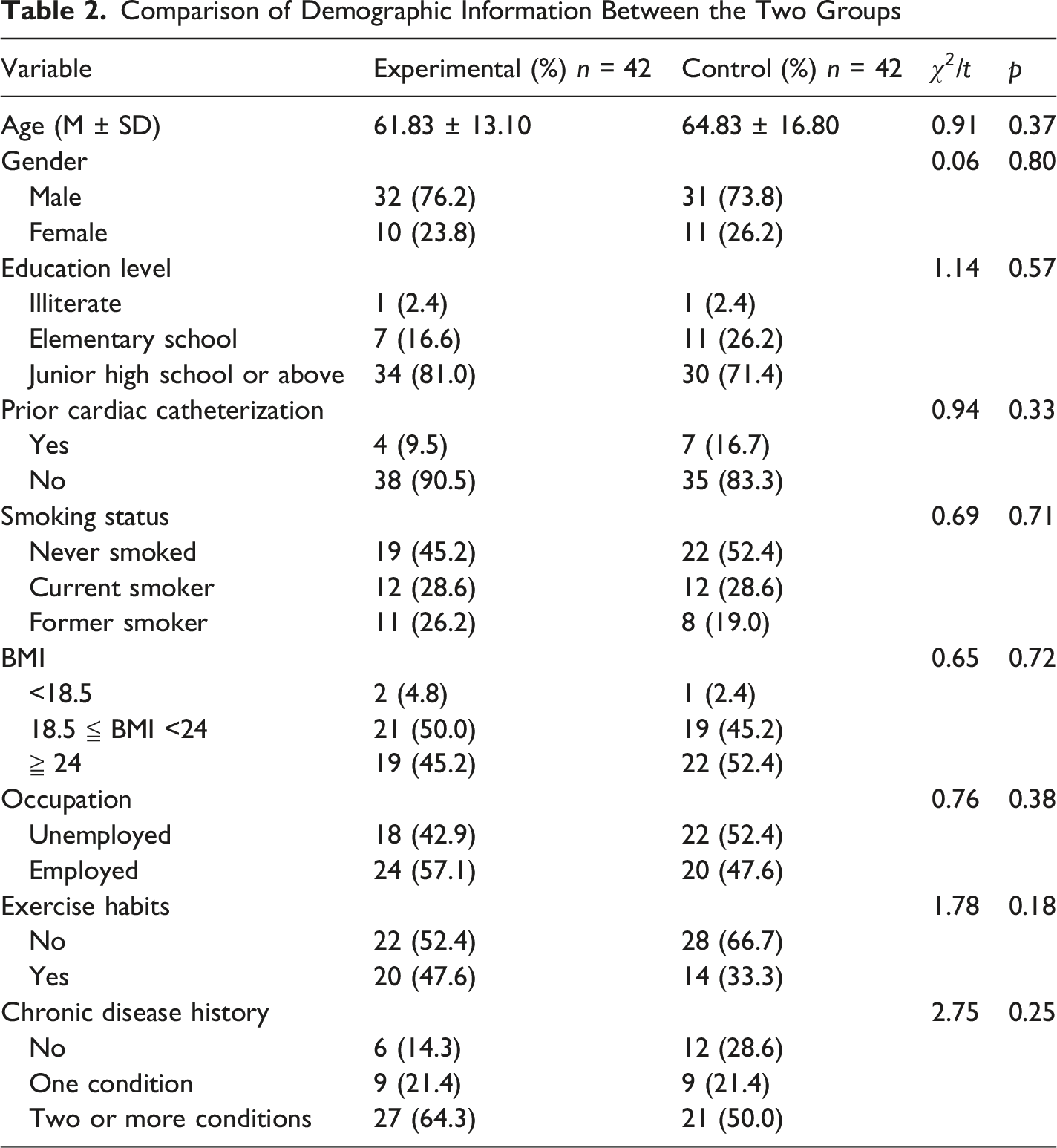
Comparison of Demographic Information Between the Two Groups
Experimental Process
This study was conducted over a 4-month recruitment period from September to December 2024. The experimental process is illustrated in Figure 5. The researchers screened ICU patients with CHD who met the inclusion criteria, obtained written informed consent, and enrolled them in the study. Experimental process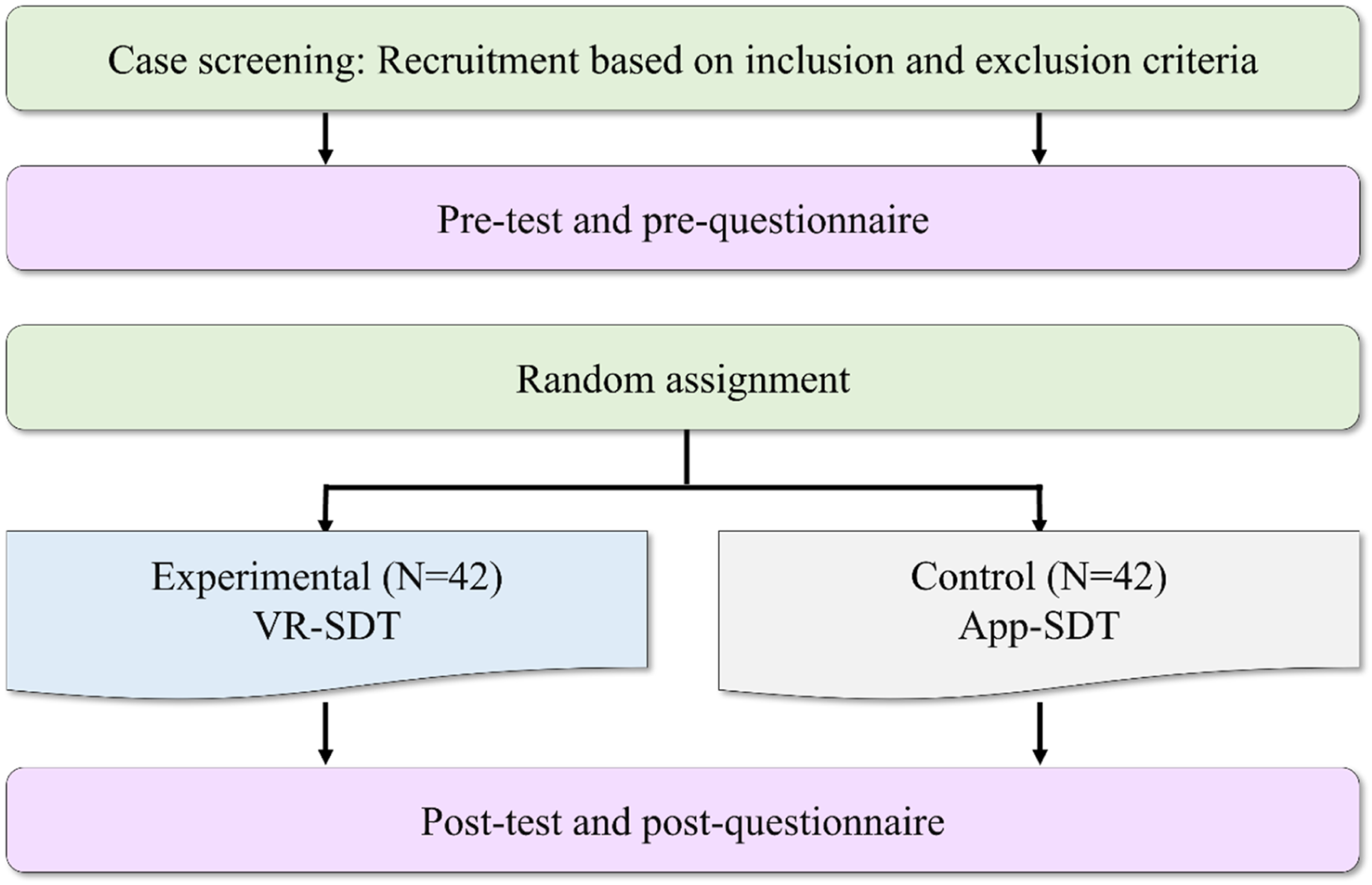
First, participants completed a pretest and pre-questionnaire and were then randomly assigned to either the experimental group or the control group. Subsequently, they participated in a health education intervention, which included an introduction to the ICU environment, CHD-related knowledge, shared decision-making regarding CHD treatment options, preoperative preparation for cardiac catheterization, an overview of the surgical procedure, postoperative care, and daily self-management of CHD. The experimental group adopted the VR-SDT mode to engage in approximately 20 minutes of immersive VR interaction. In contrast, the control group adopted the App-SDT mode to receive CHD education through the app, which presented the same educational content as the VR system using text, images, and multimedia files (Figure 6). Immediately after the intervention, all participants completed a posttest and post-questionnaire to assess their immediate cognitive and affective responses to the learning experience. Interface of the App-SDT health education application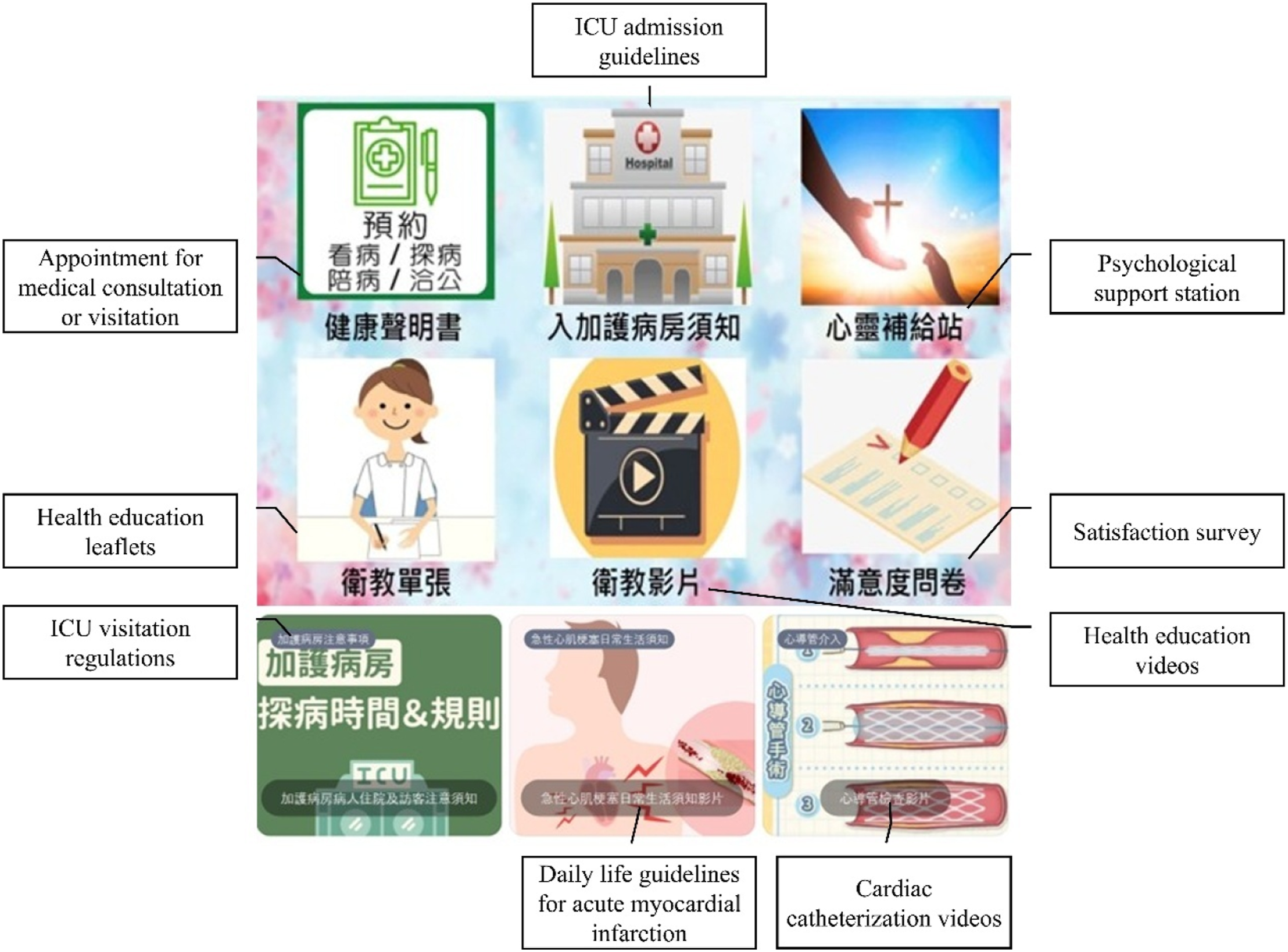
Measuring Instruments
The instruments used in this study included a pretest and posttest of CHD knowledge, the Hospital Anxiety and Depression Scale (HADS), and the Heart Health Self-Efficacy Scale.
To assess participants’ baseline CHD-related knowledge prior to the intervention, this study employed a CHD Knowledge Pretest developed by two experts with over 5 years of clinical experience in CHD care. The pretest was designed as a brief screening instrument to evaluate participants’ entry-level knowledge and baseline learning readiness, rather than to provide a comprehensive assessment of learning outcomes. It consisted of 10 dichotomous items covering CHD etiology, risk factors, symptoms, treatment, and nursing care. Each correct response was scored as 10 points, yielding a total possible score of 100. The test content was evaluated by three experts, including one physician and two head nurses, who assessed the appropriateness of the items for evaluating CHD knowledge, clarity of wording, and relevance to ensure content validity. The evaluation yielded a Content Validity Index (CVI) of .93, indicating good content validity. The internal consistency reliability of the pretest, assessed using the Kuder–Richardson Formula 20 (KR-20), was .42.
To evaluate participants’ learning outcomes regarding CHD knowledge following the intervention, this study employed a CHD Knowledge Posttest designed by the same two experts. Unlike the pretest, the posttest was intended as a more comprehensive outcome assessment to evaluate participants’ acquisition of the targeted educational content delivered during the intervention. Therefore, it included a broader range of detailed CHD-related concepts, and consisted of 20 dichotomous items addressing CHD pathophysiology, risk factors, symptoms, treatments, and nursing care. Each correct response was scored as 5 points, yielding a total possible score of 100. Higher scores indicate greater mastery of CHD knowledge. The posttest was reviewed by the same three experts for content validity. The evaluation yielded a CVI of .92, demonstrating good content validity. The internal consistency reliability of the posttest, assessed using KR-20, was .55. Because the pre- and posttest served different assessment purposes, they were not designed as parallel forms nor were they formally equated for difficulty. This should be considered when interpreting knowledge outcome comparisons.
This study assessed participants’ anxiety levels using the anxiety subscale of the HADS developed by Zigmond and Snaith (1983), with formal authorization obtained from the Mapi Research Trust. The subscale, designed to evaluate patients’ anxiety, comprises seven items, for example, “I get a sort of frightened feeling like ‘butterflies’ in the stomach” and “I feel tense or ‘wound up.’” It uses a 4-point Likert scale from 0 to 3, yielding a total score ranging from 0 to 21, with higher scores indicating greater anxiety. Cronbach’s alpha for the anxiety subscale was .829 (Michopoulos et al., 2007).
The heart health self-efficacy scale used in this study was derived from the Heart Health Self-Efficacy and Self-Management Scale (HH-SESM) developed by Mares et al. (2022). The original scale consisted of two subscales: self-efficacy and self-management. Considering the design and objectives of the present study, only the self-efficacy subscale was utilized as the instrument, with formal authorization obtained from the original authors. The heart health self-efficacy scale comprises 12 items covering six domains: physical activity, diet, medication adherence, psychosocial factors, body weight management, and smoking. It uses a 4-point Likert scale (1 = not confident at all, 4 = very confident), with total scores ranging from 12 to 48. Higher scores indicate greater self-efficacy in managing heart health. The Cronbach’s alpha of the scale was .83 (Mares et al., 2022).
Experimental Results
CHD Knowledge
ANCOVA Results for CHD Knowledge Between the Two Groups
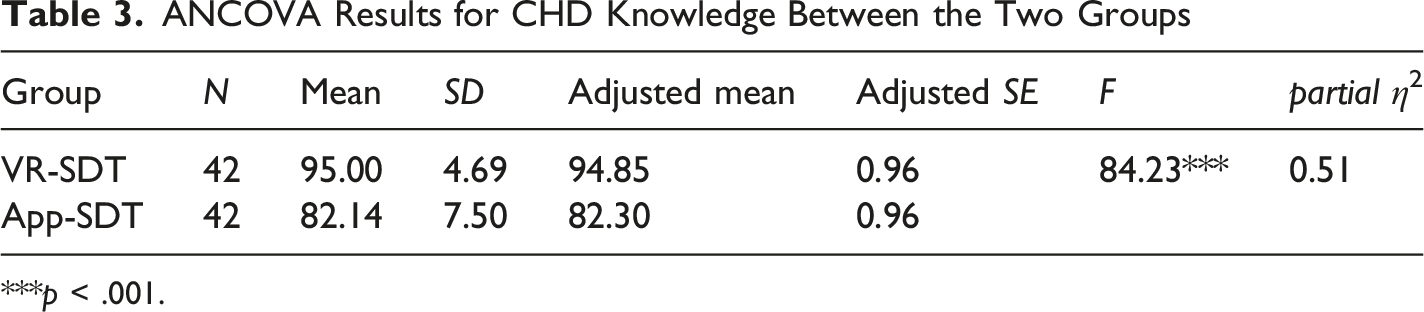
***p < .001.
Anxiety
Independent-Samples t-Test Results for Anxiety Between the Two Groups
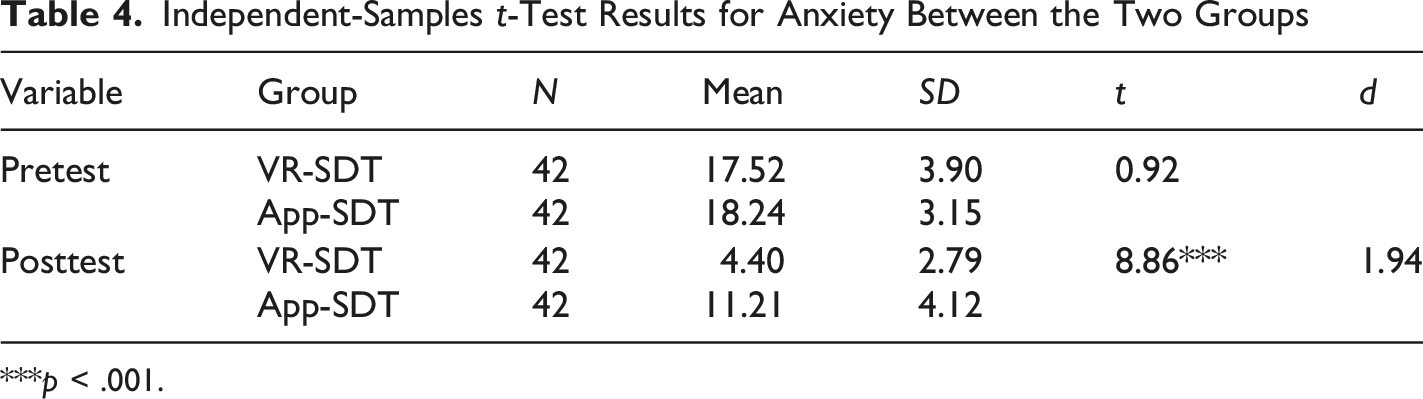
***p < .001.
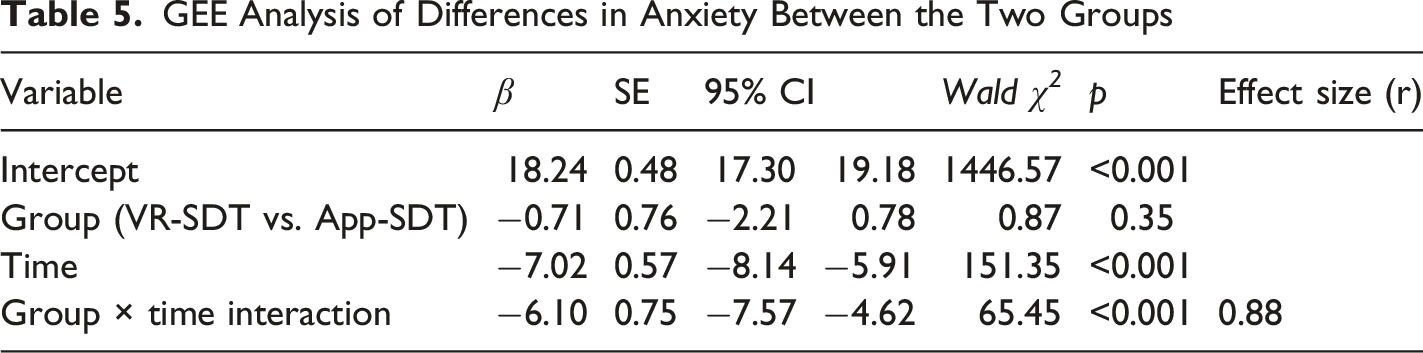
GEE Analysis of Differences in Anxiety Between the Two Groups
Heart Health Self-Efficacy
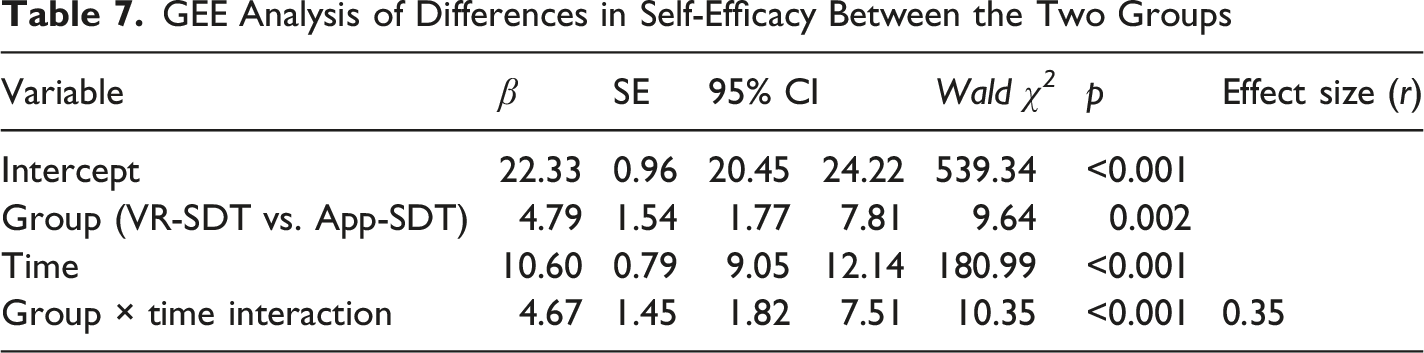
To examine the effect of the VR-SDT mode on patients’ self-efficacy, an independent-samples t test was conducted on the pre-questionnaire scores. The experimental group had a mean score of 27.12 (SD = 7.90), whereas the control group had a mean score of 22.33 (SD = 6.31). There was a statistically significant baseline difference in self-efficacy between the groups prior to the intervention, with the experimental group reporting higher initial self-efficacy than the control group. Therefore, generalized estimating equations (GEE) were used to account for baseline differences and to evaluate changes over time between groups.
Independent-Samples t-Test Results for Self-Efficacy Between the Two Groups
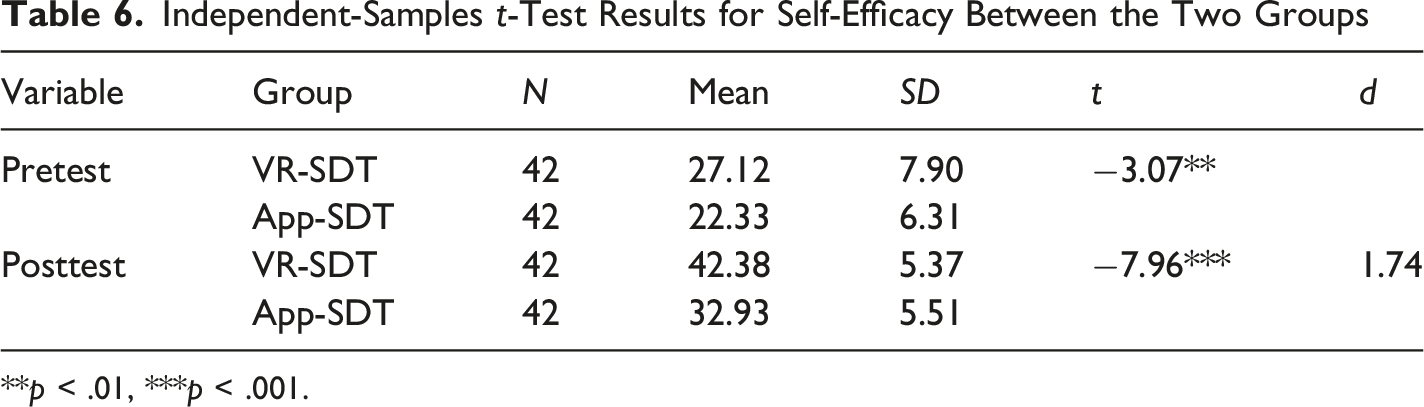
**p < .01, ***p < .001.
GEE Analysis of Differences in Self-Efficacy Between the Two Groups
Discussion
This study examined whether a needs-supportive immersive learning design based on self-determination theory could enhance learning outcomes related to disease knowledge, self-efficacy, and anxiety in high-stress healthcare learning environments. Compared to the App-SDT group, the VR-SDT group demonstrated significantly improved knowledge acquisition and self-efficacy, while exhibiting markedly reduced anxiety levels. However, the high posttest knowledge scores, particularly in the VR-SDT group, suggest the possibility of ceiling effects, which should be considered when interpreting the magnitude of the knowledge gains. Previous studies have demonstrated that SDT-based health education can effectively enhance patients’ disease-related knowledge, self-management skills, and self-efficacy while also reducing anxiety in high-stress situations (Guo et al., 2023; Huang et al., 2022; Saeedian et al., 2025; Sarboozi Hosein Abadi et al., 2020; Zhang et al., 2025).
RQ1: Effects on disease-related knowledge. The results showed that participants in the VR-SDT group achieved significantly higher disease-related knowledge scores than those in the App-SDT group. These findings suggest that the mode of material delivery significantly influences learning outcomes. From the perspective of self-determination theory, although applications can deliver disease-related care information through static text, images, and videos, their interactive capabilities are often limited to basic click-based operations and lack contextualized learning experiences and realistic simulations. Such limitations may reduce learners’ sense of agency and autonomy during the learning process. According to self-determination theory, diminished autonomy can undermine intrinsic motivation and willingness to actively engage with learning materials, thereby constraining deeper cognitive processing and long-term knowledge retention. In contrast, VR environments provide immersive, scenario-based simulations that enable learners to actively explore clinical settings and interact with relevant medical information. The enhanced sense of agency and freedom of choice afforded by VR supports self-directed learning, fosters motivation and engagement, and ultimately facilitates greater acquisition of disease-related knowledge (Conrad et al., 2024; Makransky & Petersen, 2021; Reeve et al., 2004).
RQ2: Effects on anxiety reduction. The results showed that, following the intervention, participants in the VR-SDT group experienced significantly greater reductions in anxiety than those in the App-SDT group. These findings suggest that the mode of intervention delivery may play an important role in alleviating patients’ anxiety. From the perspective of self-determination theory, although applications can provide psychological support through text, images, and informational resources, their interactions often lack social context and interpersonal simulation. As a result, users may find it difficult to experience a sense of being understood, emotionally supported, or socially connected during the learning process. According to self-determination theory, the fulfillment of relatedness needs is essential for fostering psychological well-being and adaptive outcomes. When these needs are insufficiently satisfied, the emotional benefits associated with social connection may be diminished.
In contrast, VR provides a first-person immersive experience that realistically recreates the ICU environment and allows patients to become familiar with potentially anxiety-provoking clinical situations before admission. Through interactions with virtual healthcare providers offering guidance, reassurance, and companionship, VR enhances social presence and fosters feelings of being cared for and supported. These experiences may strengthen emotional connections and trust, thereby helping to alleviate anxiety and promote psychological adjustment (Klimmt et al., 2009; Oh et al., 2018). The enhanced fulfillment of relatedness needs in the VR environment may therefore explain the greater reduction in anxiety observed among participants in the VR-SDT group.
RQ3: Effects on self-efficacy. The results showed that participants in the VR-SDT group achieved significantly higher self-efficacy than those in the App-SDT group. These findings suggest that the immersive and interactive characteristics of VR may be particularly effective in terms of strengthening patients’ confidence in managing their health and preparing for medical procedures. From the perspective of self-determination theory, competence refers to an individual’s perception of being capable of successfully performing a task. Although mobile applications can provide educational information, they often lack continuity, procedural demonstrations, and opportunities for active practice, making it difficult for learners to develop comprehensive mental models of medical procedures and apply acquired knowledge to real-world situations (Akinlofa et al., 2013). Consequently, learners may have fewer opportunities to experience mastery and competence during the learning process.
In contrast, VR provides realistic scenario-based simulations that allow learners to actively engage with procedural tasks in a safe and controlled environment. Through repeated practice and immediate feedback, learners can gradually build familiarity with medical procedures, accumulate successful experiences, and develop confidence in their ability to cope with clinical situations. Such experiences may reduce uncertainty, discomfort, and anxiety when encountering actual medical procedures.
Implications
The findings suggest that VR-SDT may be associated with concurrent improvements in disease-related knowledge, self-efficacy, and anxiety reduction, potentially creating a mutually reinforcing pattern. High anxiety levels consume working memory, impair information processing and problem-solving skills, and negatively affect knowledge comprehension and retention (Ashcraft & Kirk, 2001). By reducing anxiety, learners can allocate more cognitive resources to learning, thereby facilitating knowledge acquisition and long-term retention (Fredericks et al., 2021). Successful experiences with scenario-based simulations can further boost self-efficacy, increase confidence in facing challenges, and reduce anxiety. The accumulation of knowledge and strengthened self-efficacy consolidate the understanding of and intentions to implement health-promoting behaviors. Through this positive feedback mechanism, emotional stability and internalization of effective health management behaviors are reinforced.
This study provides evidence that immersive learning environments designed in accordance with SDT principles are associated with improved cognitive and affective learning outcomes under high-stress conditions. Although the observed effect sizes were relatively large compared with those commonly reported in educational and behavioral interventions, this may be partly attributable to the highly specific ICU context, the immediate personal relevance of the learning content, and the short-term post-intervention assessment, all of which may have amplified participants’ responses. The findings underscore that the educational value of immersive technology lies not only in its technical sophistication, but also in its skillful integration of motivational design principles. From a design perspective, the findings suggest that immersive learning environments should intentionally integrate need-supportive features rather than relying solely on technological immersion. Specifically, providing meaningful choices, immediate feedback, and supportive interactions may help promote learners’ knowledge acquisition, self-efficacy, and emotional adaptation in high-stress learning contexts.
Collectively, these findings suggest that immersive learning environments designed according to SDT principles may support the development of patients’ confidence in managing their health and treatment processes. These findings are also conceptually consistent with prior immersive learning literature discussed in relation to CAMIL, which suggests that immersive environments may involve multiple cognitive and affective learning processes (Makransky & Petersen, 2021). Nevertheless, it should be noted that CAMIL was used in the present study merely as a conceptual framework for interpretation, and the mediating mechanisms proposed by the model were not directly tested empirically.
Beyond statistical significance, the findings may also hold clinical relevance in high-stress ICU settings. Improvements in disease-related knowledge and self-efficacy, together with reductions in anxiety, may help patients better understand treatment procedures, engage more actively in health-related decision-making, and adapt more effectively to intensive care experiences. Nevertheless, because the outcomes were assessed immediately after the intervention, the long-term clinical significance and sustainability of these effects require further investigation.
Limitations
However, this study has some limitations. First, the study was conducted in a specific high-stress medical environment. Although substantial effect sizes were observed for improvements in knowledge, self-efficacy, and anxiety, the participants were ICU patients with CHD, representing a single population with a limited sample size. Consequently, the generalizability and external validity of these findings may be restricted. Future studies should consider expanding this study to other populations or settings for validation. Second, although significant improvements were observed, this study did not directly measure satisfaction of the three basic psychological needs, namely autonomy, competence, and relatedness. Accordingly, although the intervention was designed based on SDT principles, the motivational mechanisms underlying the observed outcomes remain inferential rather than empirically verified. Future research should incorporate validated SDT need satisfaction scales to examine whether these psychological needs mediate the observed effects. In addition, despite random assignment, a statistically significant baseline difference in self-efficacy was observed between the two groups, with the experimental group reporting higher initial self-efficacy. Although generalized estimating equations were applied to account for this pre-existing difference by modeling group-by-time interactions, this imbalance may still have influenced participants’ engagement with the intervention and the interpretation of self-efficacy outcomes. Participants with higher initial self-efficacy may have been more willing to actively engage with the immersive learning activities and may have responded more favorably to the VR-SDT intervention. Therefore, although the significant group-by-time interaction suggests greater improvement over time in the VR-SDT group, the self-efficacy findings should be interpreted with appropriate caution. Future research should consider stratified randomization or larger sample sizes to minimize baseline imbalances in key psychological variables. Third, both the intervention and outcome measurements were conducted over a short period, precluding assessment of the long-term effects on knowledge retention, sustained self-efficacy, and anxiety reduction. This immediate post-intervention design may also have contributed to the relatively large observed effect sizes, which may reflect short-term responses rather than sustained educational or behavioral changes. Similarly, the substantial reduction in anxiety observed in the VR-SDT group may partly reflect short-term emotional relief immediately following the immersive intervention, particularly through increased familiarity with the ICU environment, medical procedures, and supportive virtual interactions. Although these immediate affective responses are meaningful in high-stress medical contexts, the present study did not include longitudinal follow-up assessments. Therefore, it remains unclear whether the observed anxiety reduction can be sustained over time or translated into longer-term psychological adaptation. Future studies are encouraged to incorporate delayed posttests or longitudinal designs to examine the durability of these affective effects. Finally, this study employed app-based health education as the control condition. Variations in the interactivity and multimedia design within the app may have influenced the results. Future research should incorporate diverse control interventions with different design qualities to more comprehensively evaluate the relative advantages of VR-based health education compared to other digital modes.
Conclusion
This study examined whether a needs-supportive immersive learning design based on self-determination theory could enhance learning outcomes in a high-stress healthcare learning environment. Compared with the App-SDT condition, participants in the VR-SDT condition demonstrated significantly higher CHD knowledge and self-efficacy, together with greater reductions in anxiety. These findings suggest that immersive learning environments designed according to SDT principles may support both cognitive and affective learning outcomes in high-stress contexts. While additional research is needed to verify the underlying motivational mechanisms and long-term effects, the present study provides preliminary evidence supporting the value of theory-driven immersive learning design and offers guidance for future educational computing and healthcare learning applications.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported in part by the National Science and Technology Council of Taiwan under contract number NSTC 113-2410-H-038-025-MY2 and by the Taipei Medical University -National Taiwan University of Science and Technology Joint Research Program under contract number TMU-NTUST-112-06
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.