
Abstract
This article discusses mental health principles for prevention and recovery of ministerial burnout, particularly those working with trauma or personally experiencing trauma. The article will define key trauma concepts. Risk factors and trauma informed care principles will be analyzed from a cross-national analysis of burnout among youth workers. Causes of burnout, recovery and prevention will be discussed. This research will be of interest not only to ministry practitioners, but also denominational leaders and ministry educators.
Keywords
Ministries that are committed to helping troubled youth thrive will vastly increase their chance of success by one fundamental policy change: to slow down their programming and put teens’ needs first. This change does not mean that ministers can haphazardly ignore their own health and needs in favor of the teens. Teens on the margins, whether they are experiencing homelessness, addiction, disability, or mental health issues, need healthy adults. Just as ignoring the teen in favor of a program focus can be detrimental, so can ignoring the person of the minister. A fundamental aspect of healthy trauma informed ministry is the minister themselves.
This article will discuss integrative mental health and trauma informed care principles’ application to prevention and recovery of ministerial burnout. The article will particularly address those working with teens experiencing trauma or ministers personally experiencing trauma and burnout. However, the insights here are unanimously believed to apply to the broadest level ministerial health and effective ministry practice. Trauma informed care is good ministry, for both the teen and the minister. After outlining the issues and prevalence of youth worker burnout, data regarding trauma informed care will be explored as it relates to keeping the minister healthy in difficult ministry settings.
Trauma-based ministry is holistic. When making a cake, eating ingredients separately would be awful, if not unsafe. Programmatic focus without considering the student's trauma or the minster engaging the student is a recipe for disaster. The student, the environment/program, and the minister are a “mix” of elements necessary for success. Ministerial burnout is real, prevalent, and dramatically increased when working with at-risk populations. This article will focus specifically on the person of the minster, but it would be wise to consider this factor in the broader scope of the entire ministry context and the individual students. Trauma-informed ministry must consider all three elements.
After defining key terms such as burnout and trauma-related stress and adverse childhood experiences, the article will turn to data from a cross-national analysis of burnout among youth workers. Insights for training youth workers to stay healthy while engaging teens with trauma will be outlined in the analysis.
Key Theoretical Terms
This section will address and define three areas, burnout, trauma-related stress, and adverse childhood experiences. Burnout and trauma-related stress are separate but related phenomena in the lives of youth workers.
Burnout
Professional burnout is a general phenomenon and well documented among all service professions including ministers and youth workers. A distinct malady, The World Health Organization, defines burnout as a “syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions: feelings of energy depletion or exhaustion; increased mental distance from one's job, or feelings of negativism or cynicism related to one's job” (World Health Organization, 2018). Burnout is not listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-V); however, psychiatrists from multiple countries argue burnout “can be considered a particular mental adjustment disorder and is described by the DSM” (Chirico, 2015, p. 443; Schaufeli et al., 2009, pp. 204–220). Dutch guidelines for the DSM-1V-TR lists burnout as an adjustment disorder (Signorelli et al., 2013). While no prescription is available for Burnout (Senior, 2013), the concept is described by researchers around the world.
Burnout is often defined in terms of outcomes. Cordes and Dougherty (1993) describe the results of burnout as “increased turnover, absenteeism, and reduced productivity” (p. 621). Other describe burnout as “exhaustion, cynicism, and perceived (lack of) job control” (Hatinen et al., 2007, p. 220) as well as “exhaustion and depersonalization” (Schmidt, 2007, p. 26).
The Maslach Burnout Inventory (MBI) has created a common language and tool for consensus on burnout. Maslach posits burnout as a multidimensional issue: “Burnout is a prolonged response to chronic emotional and interpersonal stressors on the job, and is defined by the three dimensions of exhaustion, cynicism, and inefficacy” (Maslach et al., 2001, p. 397). Engaging teens with Trauma, disability, or mental health concerns can be more than difficult. All of Maslach's three dimensions are likely heightened. The seemingly intractable nature of the issues can easily elevate exhaustion as the caregiver serves. Cynicism creates an emotional diffidence or distance and is strongly positively correlated with stress and anxiety (Viljoen & Claassen, 2017, pp. 499–503) which will be discussed extensively below as trauma related stress. Inefficacy is a poignant risk when battling the seemingly intractable and pervasive effects of trauma. It can be exceedingly difficult to see tangible results or changes in the life of a teen with trauma.
Burnout “can be brought about by workplace conflict, overload of responsibilities, perception of inequality and inadequate rewards, and consistent exposure to traumatic materials” (Chamberlain & Miller, 2008, pp. 237–250). Kaegler and Severe note that burnout is caused in youth workers by:
Misalignment (in values or philosophy) Work relationships (un-empowered, conflict typically with primary supervisor) Lack of Self-awareness (insecure calling, blind to weaknesses, lack of narrative of journey in ministry) Workload control (overwork, exhaustion, lack of boundaries) Personal issues (family, time management, loneliness) (Kageler et al., 2021, pp. 10–38).
While burnout is not unique to caring for teens of trauma, it can be exacerbated or caused by the environment and those whom youth workers serve. The following sections define specific issues related to trauma and working with those experiencing trauma.
Trauma-Related Stress and Secondary Traumatic Stress (STS)
Trauma-related stress is specifically related to work with trauma and can involve secondary traumatic stress (STS), vicarious trauma, and compassion fatigue (Newell & MacNeil, 2010, July pp. 57–68). “Secondary traumatic stress describes the emotional stress and behaviors resulting from an indirect experience of another individual's direct traumatic experience” (Senior, 2013). STS has been defined as “the natural consequent behaviors and emotions resulting from knowing about a traumatizing event experienced by a significant other—the stress resulting from helping or wanting to help a traumatized or suffering person” (Figley, 1995). The DSM-V defines PTSD as a set of symptoms caused by a direct or indirect exposure to a traumatic event. Thus, STS is often considered a subset of PTSD (Jang et al., 2023, pp. 176–181).
The detrimental effects of STS are said to be the same as those caused by primary exposure to the traumatic experience. “Symptom clusters described in STS overlap with those in the criteria for PTSD: intrusive symptoms, avoidance, negative cognitions and mood, and hyperarousal and reactivity” (Newell & MacNeil, 2010, July pp. 57–68). Negative effects can infiltrate every area of life from physical health, mental health, work, and relationships.
Vicarious Trauma
The DSM-5 describes vicarious trauma as part of the trauma and stressor-related disorders. It is “the emotional residue of exposure to traumatic stories and experiences of others through work; witnessing fear, pain, and terror that others have experienced” (American Counseling Association, 2021). It is sometimes referred to as secondary traumatization, insidious trauma, or secondary stress disorder. The data is clear, those who serve people with trauma can also develop trauma and experience its adverse effects.
Compassion Fatigue
While not diagnosable, compassion fatigue is considered a subset or synonymous with STS and is a condition characterized by a gradual reduction of compassion over time. “Compassion fatigue recently emerged in the literature as a more general term describing the overall experience of emotional and physical fatigue that social service professionals experience due to the chronic use of empathy when treating patients who are suffering in some way” (Newell & McNeil, 2010, pp. 57–68). Compassion fatigue can occur quickly compared to burnout or vicarious trauma, which develop over repeated exposure and manifests as emotional suppression, distance from those served, and other maladaptive coping skills. Compassion fatigue is readily treatable through therapy and can be experienced without vicarious trauma.
Despite the prevalence and risk of these issues, most youth pastors are likely unaware of the prevalence, risk, or the self-care necessary to avoid them. Being aware of the risk factors for both ministerial burnout and trauma related stress is necessary for healthy teens and their caregivers. Information on these topics should be included in youth ministry and youth worker education and curriculum.
ACEs and Burnout
In the 1990′s, Vincent Felitti and Robert Anda began studying the relationship between childhood trauma and adult health. In 1998, they published the landmark Adverse Childhood Experiences Study which compared trauma in childhood to later in life adult health outcomes (Felitti et al., 1998, pp. 245–258). The study interviewed 13,494 adults and compared their medical records. The higher the number of adverse childhood experiences (ACEs), the higher the occurrence of almost every negative health outcome, risk behavior, health status, and disease. Examples include obesity, heart disease, depression, sexual activity, cancer, and many more. ACEs were categorized in seven areas of childhood exposure to “psychological, physical, or sexual abuse; violence against mother; or living with household members who were substance abusers, mentally ill or suicidal, or ever imprisoned” (Felitti et al., 1998, pp. 245–258). A meta-study of 1,794 papers found that ACEs occur more often among the helping and medical professions than in the general population. Among this group, ACEs are “associated with several personal and professional outcomes, including poor physical and mental health, and workplace stress” (Mercer et al., 2023). Among mental health, medical, social work, and other helping professions, about 50% have at least one ACEs score.
Burnout and ACEs correlate strongly with each other, often at the p < .001 level. Those with four or more ACEs “have more than two and half times the risk of burnout” on various burnout scales (Yellowlees et al., 2021, pp. 159–163). Any youth worker with an ACEs score has a higher risk of burnout. An ACEs score, burnout, and working with teens with trauma compound these negative effects.
One benefit of exposure to trauma is that doctors, pastors, and social workers can empathize with difficult situations and thus increase work effectiveness. However, ACEs can compound burnout, compassion fatigue, and vicarious trauma.
Data and Methodology
A 2021 study by the author explored how youth workers in the US and UK experience and recover from burnout. A 19-item questionnaire was conducted generating 123 valid responses. Those who took the survey experienced youth ministry burnout. The survey explored both the causes and factors of burnout as well as recovery from burnout. For this article, the qualitative data from the study was analyzed for issues related to mental health, stress, ACEs, and the trauma of the students they served.
Sampling, Population, and Delimitations
A web-based survey from five youth ministry resource providers was conducted. The survey enabled elimination of potential duplicate responses. SurveyMonkey.com was the survey platform. The completion rate was 100% and the mean time taken to complete the survey was eight minutes. There were 123 valid responses, 90 from the USA, and 33 from the UK. As a convenience sample, the results are necessarily only true of those who filled out the survey. However, a sample of this size which includes quantitative and qualitative data is of interest to and relevant to the field of youth ministry and youth ministry education.
A comparison of relevant demographic characteristics will set the stage for further analysis later (Table 1).
Demographic Characteristics.
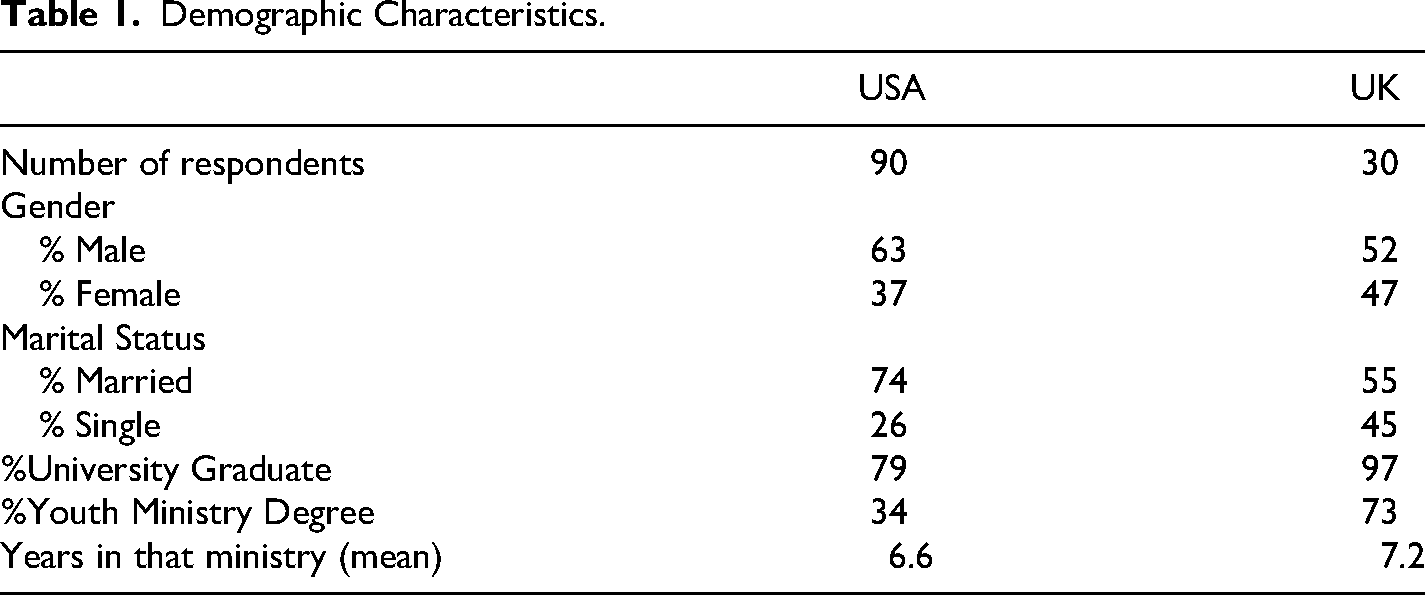
From this population, the majority of those who have experienced burnout are male in both the USA and UK. In the UK, woman have burned out nearly equal the percentage of men. Considerably, more US youth workers are married compared to the UK. Youth ministry educators, particularly in the USA, will be interested to see that a greater percentage of the respondents in the UK (73% compared to 34%) had an actual degree in youth ministry from a college, university, or seminary.
How long do youth workers, even those who experience burnout, stay in their ministries? When counting only the full-time paid category, the mean number of years stayed in the USA was 5.5 years (n = 44). For the UK, it was 5.2 years (n = 22). The US figure (5.5 years) is consistent with research indicating that youth workers, even ones who are having hard times, stay around five years.
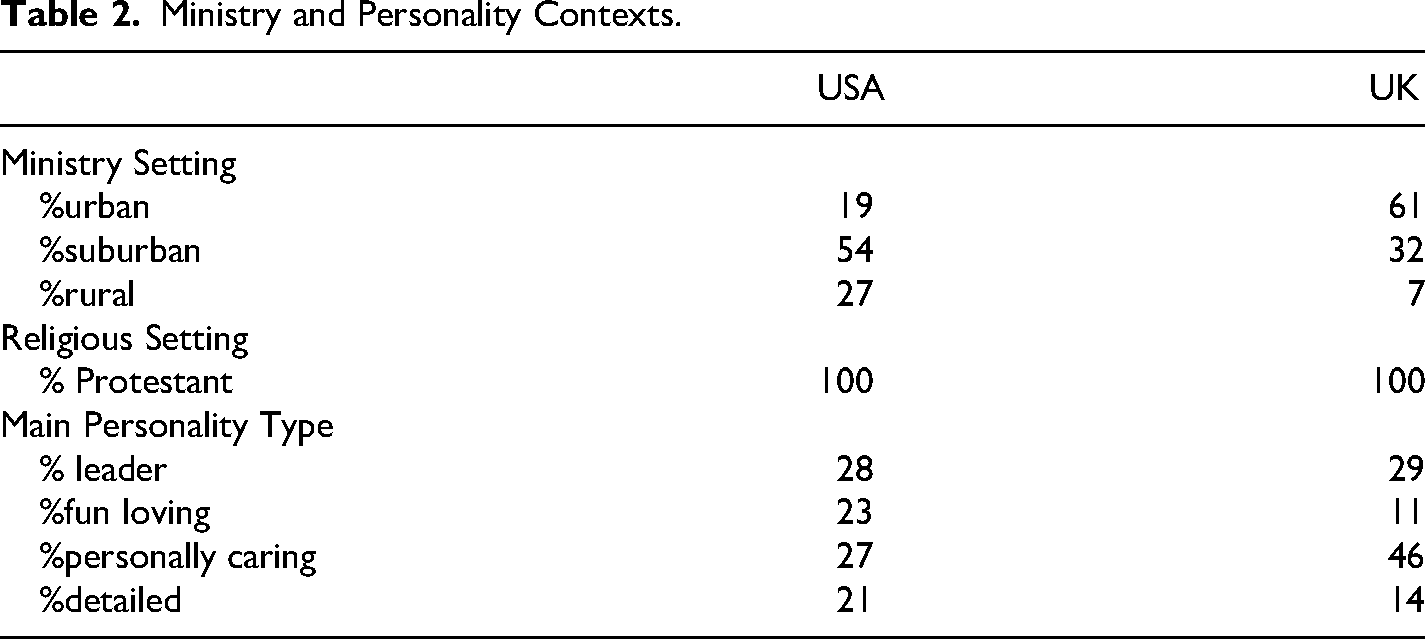
As to where these youth ministries took place, Table 2 demonstrates the majority of contexts in the USA were in a suburban context, but the vast majority of UK youth ministries were in an urban context. The sample is 100% Protestant as well. The main personality home bases of these youth workers are similar when it comes to those whose dominant style is positive leadership. There are significant differences in the others. In this sample, the UK youth workers are less fun loving than the Americans, but wow, they (UK) are a lot more caring.
Ministry and Personality Contexts.
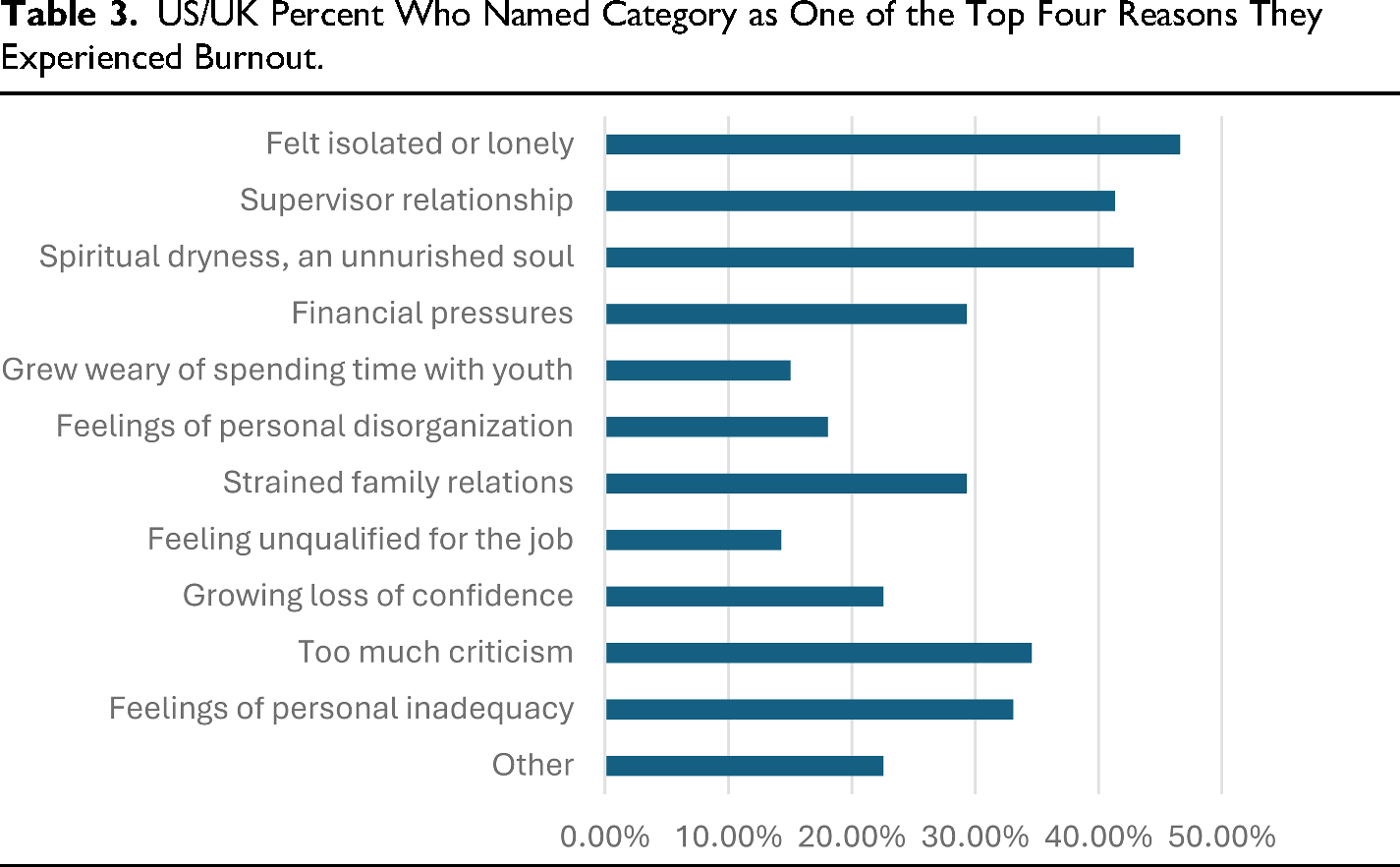
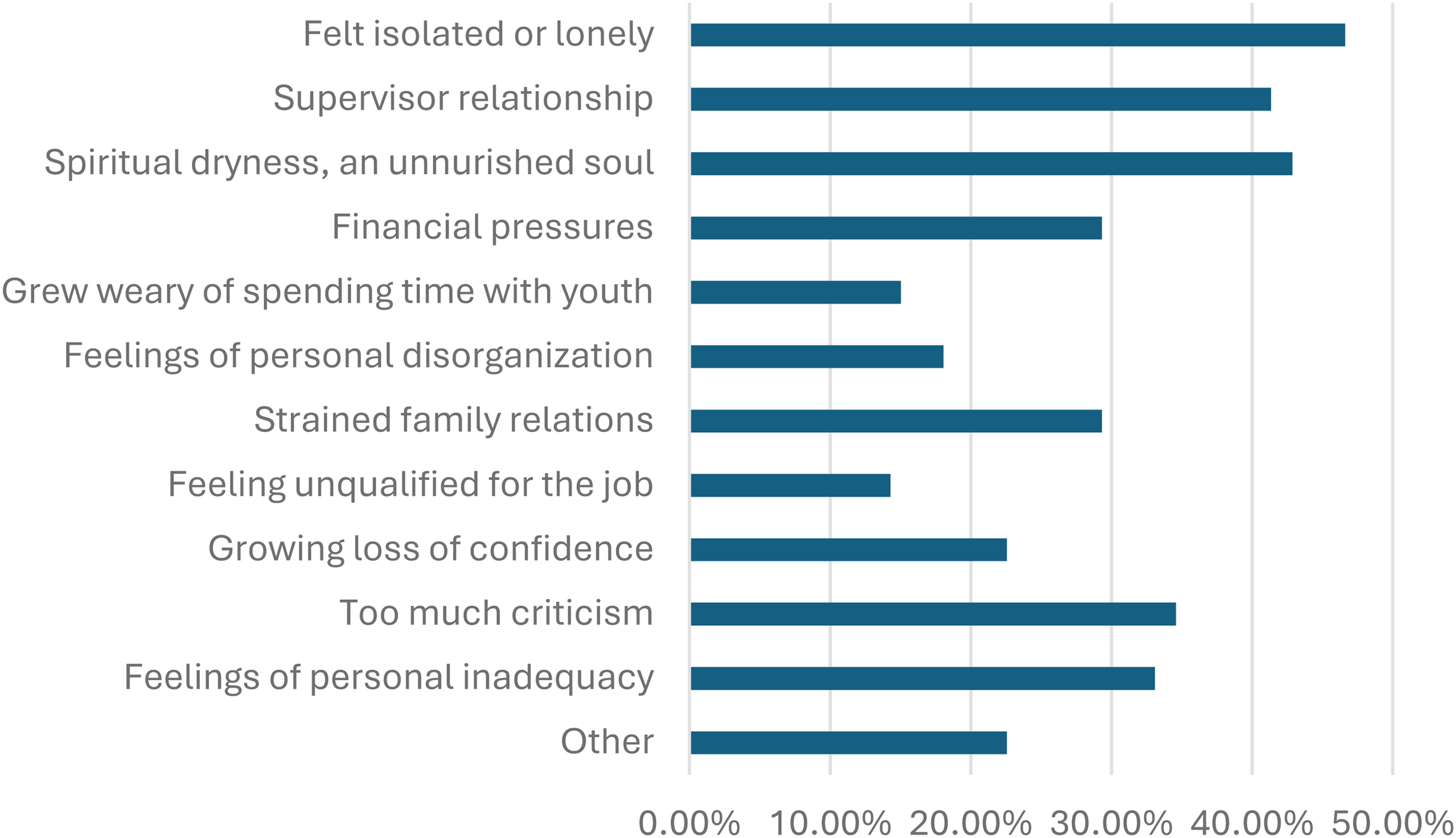
When it comes to what contributes to burnout among youth workers, Table 3 shows the most important causes of burnout within respondents.
US/UK Percent Who Named Category as One of the Top Four Reasons They Experienced Burnout.
Youth Worker Burnout Analysis
Regarding burnout, feeling isolated or lonely, spiritual dryness, pastor hard to get along with, and too much criticism are the top four items named by these US and UK youth workers. The data can help the issues become clearer for trauma, stress, and recovery.
A potential hypothesis would be that urban youth workers are more likely to burnout or experience STS due to challenges of ministry location, vicarious trauma, and compassion fatigue. This data set rejects that hypothesis. US primarily suburban youth pastors burnout more than majority urban UK youth pastors although differences in marriage rates, pay, and level of training may be factors affecting this outcome.
Problems
Noted earlier, ACEs increase burnout rates but do not preclude it. Working with teens with trauma increases STS rates and possibly burnout. Addressing loneliness, mental health concerns such as depression, supervisor relationship, and creating balance through boundaries and margins are paramount in the qualitative data regarding recovery (Kageler et al., 2021, p. 22). Three main areas of concern are identified in this research: Savior complex, busted boundaries, and burnout accelerants.
The Savior Complex: The Impact of ACEs on Workload
Workload and boundary issues were of significant difficulty for the study population. The 2021 burnout study data notes that a savior complex is an acute problem for youth workers. A savior complex can cause a pastor to take on too much responsibility or burden of care. This risk is even more poignant to those who serve among at-risk populations of teens. But the savior complex is not just about overworking to rescue an at-risk teen but can also be an over-identification with teens. Over-identification can remove the distinction between pastoral care and empathy and thus move the caregiver into an inappropriate posture to address their own personal concerns. The youth worker can take personal responsibility for a teen's trauma and needs often driven by a need to solve their own trauma vicariously through the relationship with the teen. This perspective entices youth workers to prioritize teens’ needs without personal care of their own needs leading to exhaustion both physical and emotional. A savior complex that produces unreasonable work expectations and lack of work boundaries is exacerbated by STS and ACEs in the caregiver. Additionally, inefficacy is heightened when all teens cannot be rescued. A savior complex can increase inefficacy and exhaustion, two of the three key burnout factors defined by Maslach earlier.
Busted Boundaries: Pac-Man Syndrome
“Lack of boundaries threatens the health of the ministry and minister” (Kageler et al., 2021, p. 28). Research on youth pastors participating in ministry networks describes a “Pac-man syndrome” where youth pastors often cannot stop working in order to reflect, are fulfilling an unrealistic quota of activities, and are driven to maintain a program that threatens to “consume” them (Severe, 2006, p. 75). One's own trauma or the overwhelming needs of at-risk youth both exacerbate the need for regular reflection and reducing the required quota of ministry activities. Using delegation, creating margin in the schedule and saying “no” are critical for the healthy life of the minister. “Boundaries, margins and delegation are vital to prevent burnout and are significant factors in recovery” (Kageler et al., 2021, p. 29).
Burnout Accelerant: Collision of Past and Present
As noted above, the higher the ACEs score of the minister, the greater the incidence and impact of burnout. Higher ACEs scores corelate with heightened baseline stress scores. In addition, many youth workers are in intensive and demanding roles working with teens having experienced trauma or under-resourced environments. Those in the helping professions who have ACEs are at greater risk for STS and Burnout. There are physical, emotional, and professional consequences well documented across the literature. Thus, it is vital to be aware of the issues revolving around STS, burnout, trauma, and ACEs. Having an ACE score or other trauma does not preclude effective long-term ministry. However, ministries and ministers are rarely aware of these issues, unable to define or recognize them, and do not have ongoing professional development for mitigation of their effects. For a majority of the population, the most basic self-care or therapeutic interventions are only engaged following burnout. The final section of the article now turns to addressing these issues.
Prevention and Recovery of Burnout and STS: Implications for the Practice of Ministry Training
Although lovely, moving to a cabin in the woods is not the solution to working with teens with trauma, ministry burnout, ACEs, or STS. The factors that create healthy trauma informed ministry are not only healthy for participating teens but are necessary for those serving those teens. Youth workers will need to address the vicarious trauma they experience from those they serve while often dealing with past personal experiences, work-related stress, and possibly burnout. The vast majority of those who recover from burnout self-describe a multifaceted approach with at least three elements. Half name four or more areas that contributed to recovery. Especially striking was the connection between Sabbath and reaffirmation of calling. Another major collection of responses connects counseling, self-care, boundaries, and spiritual discipline (Kageler et al., 2021, p. 25). The final section of the article will propose four clusters of solutions and areas of further study to address trauma and burnout among those who serve teens of trauma in churches or parachurch ministries.
Soul Care and Self-care Organizational Factors: Trauma Informed Workplaces Relationships For Further Study: Secure attachment and Mindfulness
Soul Care and Self-Care
It is time to get serious about the care of ministers. Among the 123 in the youth worker 2021 burnout survey, the majority reported self-care, soul care and relationships, and therapy as the main path back to ministry. Among burned-out but recovered youth pastors, 20% participated counseling and another 20% had formal mentoring. While not a majority, these two combined factors were the two most common recovery elements among participants. “Counseling focused on a variety of topics including forgiveness, self-care, accountability, calling, dealing with loss, and boundaries. Some form of encouragement from leadership, pastor, or mentor was often connected to receiving counseling and thus staying in ministry” (Kageler et al., 2021, p. 25).
There is much to learn from the medical and social work field's research on Burnout, STS, and trauma informed care. However, it is also vital to see the connectedness of the whole person in relationship to their spirit, relationship with God, calling in ministry, and spiritual disciples. Sabbath and mentors can give space and modeling to engaging in oft neglected spiritual practices and disciplines. “Ignoring disciplines such as mediation, prayer, study, worship and fellowship were connected to both the reason for burnout and the road to recovery. The practice of spiritual disciplines in the recovery process was noted to renew passion, personal health and increase faith” (Kageler et al., 2021, p. 30). Two poignant quotes from recovered youth pastors note, Through counseling I came to see the truths I needed to see and begin to believe in my calling as a leader again but from a place of a loved child of God, not having to prove myself. [I recovered through] times of quiet and reflection [and] more readily available and proper supervision. I cried out to God for a love for his church again rather than the hatred that had been building up…. After two years recognized completely changing attitude and renewed love and passion for his church so returned to church ministry.
It is clear soul care and self-care are vital elements in longevity in ministry, prevention of burnout, and proper effectiveness in working with youth experiencing trauma.
Organizational Factors: Trauma Informed Workplaces
The data demonstrates that organizational factors are dominant in keeping a youth worker or pastor healthy and serving in ministry. Reasonable workload expectations and healthy boundaries are not individual issues but are part of healthy organizational structure, engaged supervision, and professional training. Restoration from burnout often requires supervisor support, restructuring of the job responsibilities, new organizational rhythms like Sabbath and days off, and a sabbatical.
Workload and supervisor relationship are paramount in the youth worker burnout data. There does not appear to be any direct data relating burnout or STS to supervisor relationship and working with those who have experienced trauma. However, the direct supervisor is often a source of stress and one of the most significant causes of those who report leaving youth work in the church. Further study could be done on ministers with ACEs and supervisor conflict.
The goal is not to simply use trauma-informed care in our ministry programs but to become a trauma-informed organization. A trauma-informed church or ministry has at least three components.
Regular review and change of organizational policies to support both a trauma-informed ministry and a trauma-informed workplace. Workplace culture should develop to value and include wellness, rest, boundaries, Sabbath, sabbatical, and vulnerability. Church and para-church ministries can train and review trauma-informed care, how to recognize trauma in staff, and self-care best practices in helping professions.
As a bonus fourth element, youth ministry training, formal and informal, must progress to include Trauma informed care, ACEs, and self-care in the curriculum.
Relationships: Mentor, Peer, and Professional
Cloud and Townsend suggest that healthy boundaries cannot be developed apart from supportive relationships with God and others (Cloud & Townsend, 2002, p. 115). Their research aligns with the 2021 burnout study. Soul care, counseling, mentors, and supportive leadership were all regularly mentioned in connection with the creation of boundaries and delegation. Thus, the skill of creating boundaries, while necessary, is not solely the individuals responsibility. Proper boundaries, creating Sabbath and rest, and other key factors are all community and relational in fundamental nature. The conclusion is then that lack of supportive relationships creates conditions for lack of boundaries, rest, and margin. Additionally, relationships facilitate recovery from trauma and burnout in significant ways.
The 2021 burnout data notes five overall kinds of relationships:
Friendship Mentor Therapist Supervisor Community of practice/network
All of these were related to recovery from burnout and are recommended in the literature for dealing with STS. Being mentored, peer friendships, and professional relationships are all identified as key factors in three areas: overall health, reduction of burnout, and combating ACEs.
Hydon summarizes research on PTSD among helping professions noting that “interpersonal networks such as workgroups can promote recovery within an important organizational system2 and that these naturally occurring support structures, whether at work or among one's family and friends, are the most common ways by which traumatized persons recover” (Hydon et al., 2015, p. 321). It is important to note that most pastors in this study did not participate in a network. However, among those recovering from burnout, over 15% note a ministry network as central in their recovery. One participant noted, “friendships built among the youth leaders enabled us to talk and encourage each other through these times. We prayed for and carried each other in bad times.” Developing perseverance and recovery are most often tied to ministry partnerships and friendships. These resulted in perseverance, reaffirmed calling, encouragement, challenge, accountability, support, and prayer. While other factors above were often described as “playing a part” in recovering from burnout, these networks of support were most often described as “the reason I stayed in the ministry because of the community and support.” A network and community clearly added to the perseverance factor. These relationships gave “the confidence that God isn't done yet. That the vision God gave would see its fulfillment.”
For Further Study: Secure Attachment and Mindfulness
Secure attachment stems from an adult who can receive care and offer care. The literature focusing on youth workers and their own attachment is still lacking. The 2021 survey notes a lack of attachment language or awareness in the ministers and the ministry literature. Studying youth worker adult attachment would be a vital next step in the literature in caring for youth workers.
Avoidant dismissive patterns of attachment are far higher among helping professions than the general population (Mikulincer & Shaver, 2016, pp. 258–260). The goal for many helping professions, ministry not excluded, is to find a solution, start a program, solve the problem, or build an organization. Mindfulness requires an awareness and asking, “how am I affecting and interacting with everything around me.” When a dysregulated child or teenager creates a safety concern, defies a direct command, or triggers the minister's own past trauma, that minister is deeply affected whether they admit it or not. Trauma-informed care is based on connecting with other people, especially the child expressing trauma. Trauma-informed care literature seems clear that without mindfulness, relational connection will be impossible. The “connecting principle provides the foundation for attachment and self-regulation” (Purvis & Karyn, 2013, p. 368). Trauma-informed care posits connection as the fundamental factor in dealing with trauma. Integrating trauma-informed care and learning its impacts on ministerial health and discipleship would be a profitable next step in research.
Conclusion
This article has sought to integrate key trauma and trauma-informed care terms into youth ministry work. After exploring the results of ministerial trauma and burnout, a series of suggested pathways forward are recommended. Further research on youth worker trauma is needed as well as more formal and informal training for organizations. Trauma-informed care is not only vital for those who are served but for the life of the minister who serves.
Footnotes
Ethical Considerations
This study received ethical approval from the NYACK College IRB on November 13, 2019.
Consent to Participate
The central IRB determined that this research involved minimal risk and approved a waiver for informed consent. The waiver was completed online by all participants as part of the survey.