
Abstract
In an effort to better understand possible pathways that lead to a relatively high incidence of depressive symptoms among Mexican American youth, an interpersonal stress model of depression was tested using a community sample of 674 Mexican American mothers and their 5th grade children. Structural equation analyses revealed that maternal depression was positively related to mothers’ interpersonal stress in their relationships. Additionally, maternal poor parenting quality was associated with three child outcomes: lower social competence, higher interpersonal stress, and higher depressive symptoms. Child difficulties with peers, however, were not related to child depression. Overall, evidence suggests that familial factors, rather than peer factors, were related to child depression for these study participants.
Numerous studies have demonstrated that Latino youth report higher levels of depression in comparison to youth from other ethnic backgrounds (e.g., McLaughlin, Hilt, & Nolen-Hoeksema, 2007; Roberts, Roberts, & Chen, 1997; Twenge & Nolen-Hoeksema, 2002), and that these differences are not accounted for by socioeconomic circumstances (Polo & Lopez, 2009; Wight, Aneshensel, Botticello, & Sepulveda, 2005). Yet, little is known about why Latinos might have elevated levels of symptoms. Gaining a better understanding of potential risk mechanisms can be useful for both better understanding the etiology of depressive symptoms and providing better intervention and treatment efforts for depression among Latino youth.
One model that holds promise for understanding pathways to depression is the intergenerational interpersonal stress model. This model posits that youths’ depressive outcomes are largely due to stresses in the family environment that interfere with optimal parenting by the mother. More specifically, the association between maternal and child depression is hypothesized to be mediated by family and interpersonal stress effects. According to the model, maternal interpersonal stress and parenting quality, as influenced by maternal depression and grandmother depression, affect the youth’s interpersonal relations and stress, leading to youth depression (Hammen, Shih, & Brennan, 2004). Other comprehensive models of the transmission of depression from mother to child have, likewise, identified stressful family environments and maternal depressive symptoms as key mechanisms of risk for depression (Goodman & Gotlib, 1999). Such models hold promise for serving as a foundation to examine depressive outcomes, but have not yet been tested specifically among Latino youth.
In this study, we sought to test to what extent an interpersonal stress model of depression can be applied to a community sample of ethnic minority Mexican American youth and their mothers. Specifically, the goal was to examine the consequences of interpersonal and family stressors for the child’s social competence, stress, and depression among Mexican American youth. Examination of potential etiological models of depression for Mexican American youth remains important given the dearth of research testing processes related to the development of depression among Latinos.
There are numerous reasons to expect that associations between family influences and youth depression may apply to Mexican American youth and their families. First, there are relevant cultural factors that are consistent with the model. As an ethnic minority group with higher than average rates of poverty and stress, the stress aspects of the model seem especially appropriate for helping to explain child depression in this group. Moreover, research has shown that people of Mexican origin and other Latinos tend to be very family-oriented and identify with a familistic orientation. That is, familism, a core cultural value across Latino groups, carries an expectation that the family is the main source of support, loyalty, and solidarity (e.g., Cauce & Domenech-Rodriguez, 2002; Rodriguez, Mira, Paez, & Myers, 2007). Accordingly, familism values have been found to predict psychological well-being among Latino youth (Fuligni & Pederson, 2002). Additionally, other studies have shown that for Mexican American youth, both family and peer stressors are directly related to depressive symptoms (Deardorff, Gonzales, & Sandler, 2003). Likewise, family stress factors such as marital conflict, parent-child conflict, and low nurturing-involved parenting have been found to contribute to youth depression among a wide range of samples including Mexican American families (Conger et al., 2002; Gonzales, Deardorff, Formoso, Barr & Barrera, 2006; Parke et al., 2004; Smokowski & Bacallao, 2007).
A theoretical model that incorporated maternal and child factors was evaluated for this study. Specifically, we sought to test whether: (a) maternal depression directly relates to child depression; (b) maternal interpersonal support and parenting quality are associated with maternal depression and relate to child interpersonal factors; and (c) child interpersonal difficulties, parenting quality, and maternal interpersonal support are associated with child depression.
Method
Participants and Procedures
Participants in the study were part of the California Families Project (CFP), a longitudinal study following 674 Mexican origin families, as determined by their self-identification and ancestry. All families included a nonhandicapped, normally functioning child attending the 5th grade in a public or Catholic school in a single metropolitan area in Northern California. Data for these analyses were collected between 2006 and 2008. Children and their families were drawn at random from rosters of students from school districts in this metropolitan area. First, second, and third generation children of Mexican origin were eligible for the study. To be eligible, the focal child had to be living with his or her biological mother. Married/coupled mothers (N = 549, 82%) and single mothers (N = 125, 18%) families participated. In two-parent families, the father had to be the child’s biological father. In a small number of cases (N < 5), stepfathers who had become a father to the focal child when the child was 2 years old or younger were also allowed to join the study.
Participants were recruited by telephone or, in cases where they did not have a telephone, by a recruiter who went to their home. Trained research staff interviewed the mother and child separately in their homes. The mother provided demographic information about the family and household members. Interviews were conducted in Spanish or English based on the preference of the participant. The majority of the interviews with mothers were conducted in Spanish language, with 81% in Spanish and 19% in English.
The mothers’ ages ranged from 26 to 57 (M = 36.7, SD = 5.93) and they had a mean education level of grade 9 (SD = 4.01). Eighty-four percent of mothers were born in Mexico and 16% were born in the United States. The childrens’ ages were from 9 to 12 years old (M = 10.39, SD = .60), with 43.1% female, 53.3% male, and 3.6% missing or failing to report. Twenty-nine percent of the children were born in Mexico and 71% were born in the United States. The average total family income was US$32,300.
Measures
Maternal depression
Maternal depression was derived from two measures, both of which were based upon mother’s self-reported current depressive symptoms. The first consisted of 8 of the original 20 items from the Center for Epidemiological Studies Depression scale (CES-D; Radloff, 1977), a widely used and well-validated instrument for assessing depressive symptomatology in the general population. All items were scored on a 4-point scale (1 = never, 4 = always), and had an α of .85 for the present sample. For this study, the short form developed by Cole, Rabin, Smith, and Kaufman (2004) was used. This short form version was derived using Rasch modeling in a cross-validation sample of college undergraduates and designed to preserve the four factor solution found in the full form CES-D and revealed that the short form preserved the structural similarity of the full form. Furthermore, other studies have also investigated short form versions of the CES-D among diverse samples of immigrants from Mexico and have found that the short forms were valid and reliable, accounted for most of the variance in scores from the full CES-D, and showed good concurrent validity with anxiety, acculturation, farmworker stress, and social support (Grzywacz, Hovey, Seligman, Arcury, & Quandt, 2006).
The Mini-MASQ (Mini-MASQ; Casillas & Clark, 2001) was the second measure from which two subscales were included in the current study. All items were scored on a 4-point scale (1 = not at all, 4 = very much). The General Distress Depression subscale used in the current study consisted of 10 items and assessed negative affect and general distress symptoms common to depression (α = .90.) The Anhedonic Depression subscale consisted of six items and assessed symptoms more specific to depression such as loss of interest and low positive affect (α = .85).
Maternal interpersonal support
Interpersonal support was assessed with mother self-report questionnaire variables measuring three domains of interpersonal relationships: marital or intimate relationship, close friends, and family. To assess the quality of mothers’ intimate or marital relationship, a relationship quality one-item scale was used as an overall evaluative judgment of the relationship. The scale was developed by the Iowa Youth and Families Project (Yeh, Lorenz, Wickrama, Conger, & Elder, 2006), and is scored on a 4-point scale (1 = very dissatisfied, 4 = very satisfied).
Relationships with friends and family were measured with the Multi-dimensional Scale of Perceived Support (MSPS; Canty-Mitchell & Zimet, 2000). Two subscales were used from this questionnaire to assess perceived support from interpersonal relationships: friends and family (1 = not at all true, 4 = very true). In the present study, the 4-item Friend scale had an α of .91, and the 4-item Family scale had an α of .88.
Perceived parenting quality
The child’s report of positive perceived parenting quality was derived from two questionnaires. The Behavioral Affect Rating Scale (BARS; e.g., Lorenz et al., 1991) contained two subscales used to measure the mother’s warmth and hostility as perceived by the child, scored on a 4-point scale (1 = never, 4 = always). The 9-item Warmth subscale had an α of .82, and the 13-item Hostility subscale had an α of .76.
The second questionnaire included one subscale of the Parent-Adolescent Conflict scale (PACS-RSC; Ruiz, Gonzales, & Formoso, 1998): the Mother-Child Conflict subscale. The Mother-Child Conflict scale consisted of 8 items assessing perceived conflict over the past three months and the scale was scored on a 4-point scale (1 = never, 4 = always; α = .72).
Child social competence
Two variables measured the child’s social functioning. The Peer Competence scale, derived from the Coatsworth Competence Global Scale (Harter, 1982), was a 6-item set of questions measuring effective functioning with respect to age-appropriate tasks with friends and other kids the same age. All items were scored on a 4-point scale (1 = not at all true, 4 = very true), yielding an α coefficient of .78 was present in the present study. The second measure was the Friends subscale from the Multidimensional Scale of Perceived Support (MSPS; Canty-Mitchell & Zimet, 2000). This measure assessed social support from friends on a 4-point scale (1 = not at all true, 4 = very true). The 4-item subscale had an α of .87 in the present study.
Child interpersonal stress
The child’s report of stressful negative life events was derived from the Peer Hassles subscale of the Multicultural Events Scale for Adolescents (MESA; Gonzales, Gunnoe, Samaniego, & Jackson, 1995). This subscale reflects interpersonal conflicts with peers, and asks about the occurrence of events within the last 3 months. The subscale consists of 9 items and generates symptoms counts with higher scores indicating higher interpersonal distress (α = .60).
Child depression
Depressive symptoms in the child were obtained using the Computerized Diagnostic Interview Schedule for Children (C-DISC-IV; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000). The C-DISC-IV is a comprehensive, highly structured interview designed to assess Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV) psychiatric disorders and symptoms in children and adolescents aged 6 to 17 years. It has a child version, which asks about the child’s psychiatric symptoms. The interview was administered using a laptop computer. The items are organized by diagnosis. The students are asked if they had specific symptoms during the past year, and answer follow-up questions in case of positive endorsement. The DISC generates symptoms counts and diagnoses. The Mood Disorders module from the C-DISC-IV was used to measure the child’s endorsed depressive symptoms, using symptoms counts (α = .82).
Data Analysis
Structural equation modeling (SEM) was used to test predictions from the theoretical model using EQS version 6.1 (Bentler, 2002). In order to adjust for any deviations from multivariate normality in the data, robust maximum likelihood estimation was used. Three different indices were used to assess the overall fit of the model: the Yuan-Bentler-scaled chi-square (Y-Bχ2), the comparative fit index (CFI), and the root mean square error of approximation (RMSEA) (Yuan & Bentler, 2000; Hu & Bentler, 1999).
The structural model consisted of four latent variables and two manifest variables. Maternal depression was a latent factor with three indicators: the scaled sum of the CES-D, the scaled sum of the General Distress Depression subscale, and the scaled sum of the Anhedonic Depression subscale from the Mini-MASQ. These three factor indicators were coded so that higher values indicated more depressive symptoms. Maternal interpersonal support was a latent factor with three indicators: relationship quality with intimate partner, support from friends, and support from family. All three factor indicators were coded so that higher values indicated more interpersonal support. Perceived parenting quality was a latent factor with three indicators: child reports of warmth, hostility, and mother-child conflict. All three indicators were coded so that higher values indicated better perceived parenting quality. Hostility and conflict were reverse-coded such that higher values indicated lower levels of hostility and conflict. Child social competence was a latent variable with two indicators: child report of peer competence, and perceived social support from friends. The two indicators were coded so that higher levels indicated greater social competence. Child interpersonal stress was a manifest variable with a single indicator: child report of Peer Hassles. Higher values indicated greater stress with peers. Child depression was a manifest variable derived from the C-DISC Mood Disorders module. The child endorsed symptoms were summed for the present analysis into a symptom count measure. Higher values indicated more depressive symptoms.
Results
Measurement model
Confirmatory factor analyses were first used to determine whether our measurement model provided an acceptable fit with the data. The model tested consisted of the latent variables stated above, and all factors were allowed to correlate freely. This original model generated significant factor loadings on all indicators; however, this model had marginal fit, Y-B χ2(52, N = 674) = 203.67, p < .00, CFI = .88; and RMSEA = .08. On the basis of the Lagrange Multiplier Test, and on conceptual reasoning, the following error residuals were freed to correlate: (a) CES-D and general distress in the latent variable for maternal depression, (b) friend support and family support in the latent variable for maternal interpersonal stress, and (c) hostility and conflict in the latent variable for perceived parenting quality. As indicated by the chi-square difference test, the fit of this respecified model was significantly better than that of the original model, χ2(3, N = 674) = 42.95, p < .001, and the fit indices were now in the acceptable range; CFI = .91; and RMSEA = .07. The correlation coefficients, means and standard deviations for the measured variables in this model are depicted in Table 1.
Means, Standard Deviations, and Correlations for the Measured Variables
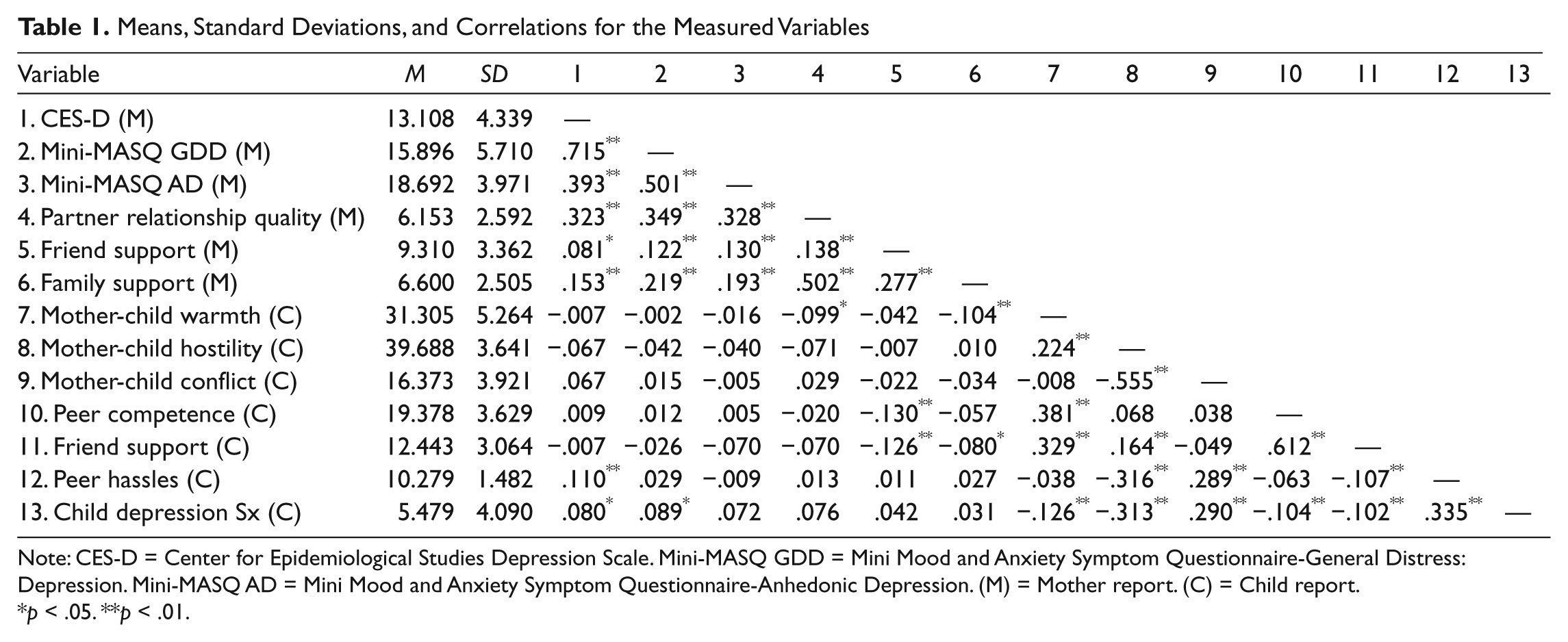
Note: CES-D = Center for Epidemiological Studies Depression Scale. Mini-MASQ GDD = Mini Mood and Anxiety Symptom Questionnaire-General Distress: Depression. Mini-MASQ AD = Mini Mood and Anxiety Symptom Questionnaire-Anhedonic Depression. (M) = Mother report. (C) = Child report.
p < .05. **p < .01.
Structural model
In the first step of the SEM analyses, the model was estimated exactly as hypothesized in the original interpersonal stress model (Hammen et al., 2004). Results from the SEM indicated that this model did not demonstrate an acceptable fit to the data; Y-Bχ2 (51, N = 674) = 106.93, p < .000, CFI = .88; and RMSEA = .07. A reduced, more parsimonious model that dropped the nonsignificant paths as suggested by the Wald test statistics was analyzed next. The fit indices of this model were improved, with a CFI value of .90 and RMSEA of .06, with no significant difference in chi-square compared to the original model ( χ2(7, N = 674) = 2.57, p = .92). All of the indicators loaded significantly on their respective constructs and thus, the nested model was accepted as the final model (Figure 1).
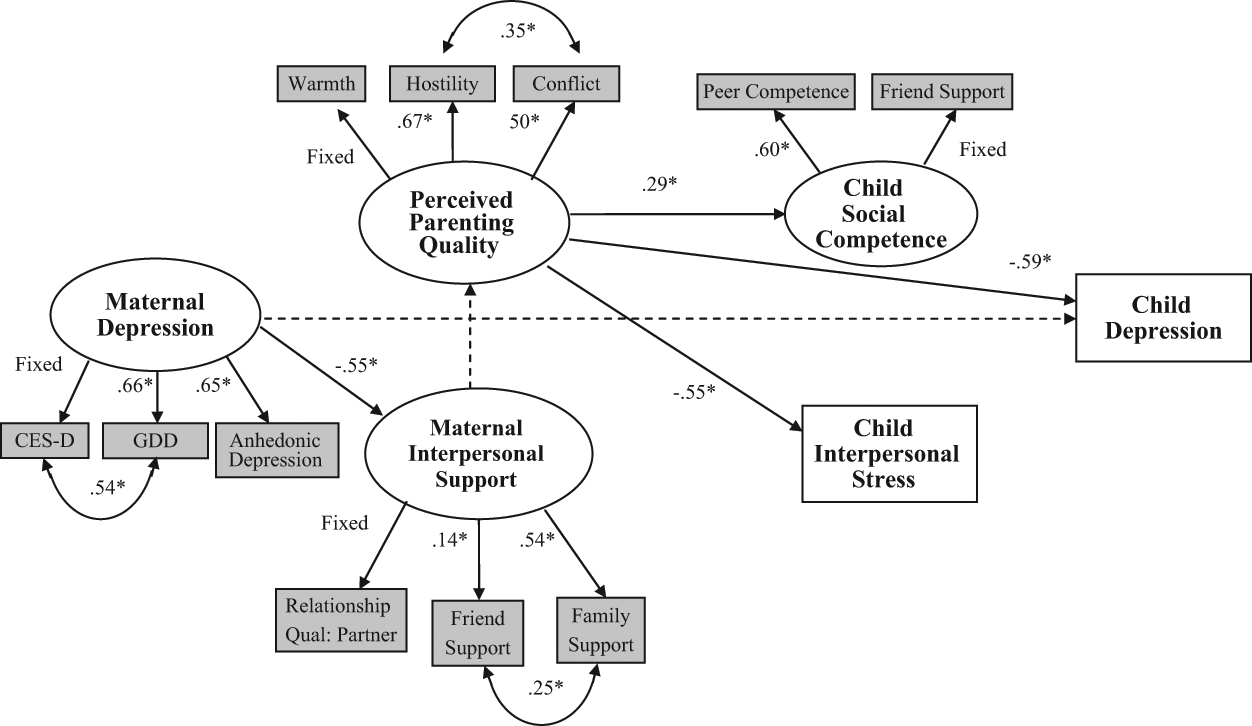
Final structural model for the test of the theoretical framework. Coefficients are standardized parameter estimates. Curved lines with double-headed arrows represent residuals allowed to correlate.
First, the final model indicated that maternal depression was significantly associated with maternal interpersonal support, but was not significantly associated with child depression. Maternal interpersonal support demonstrated a nonsignificant trend (p < .10) in association with poorer parenting quality. However, maternal interpersonal support was not associated with child interpersonal stress or child depression (pathways dropped from the model). Second, better parenting quality was associated with higher child social competence, fewer child depressive symptoms, and lower child interpersonal stress. Third, child social competence was not associated with child interpersonal stress or child depression, nor was child interpersonal stress associated with child depression (paths dropped).
We then tested for indirect effects among the significant paths in the model using four Sobel tests of mediation. The first test examined whether maternal depression was related to parenting quality indirectly through maternal interpersonal stress. This test did not indicate a significant meditational effect for the relationships among these variables, z = −1.27, p = .20. The second test examined whether parenting quality served as a mediator between maternal interpersonal stress and child social competence. Results indicated that this indirect effect was not significantly greater than zero, z = −1.18, p = .23. The third test evaluated whether parenting quality mediated the association between maternal interpersonal stress and child depression. This indirect effect was not supported, z = 1.26, p = .20. Lastly, the fourth Sobel test evaluated whether parenting quality mediated the association between maternal interpersonal stress and child interpersonal stress and was not found to be significant, z = 1.24, p = .21.
Discussion
The goal of this study was to test an interpersonal stress model of psychosocial risk factors predictive of depression among Mexican American children, a sample at relatively high risk for elevated depressive symptoms. Whereas the research reported so far has mostly focused on establishing ethnic differences in depression among this group, our goal was to move towards testing a model that examined potential pathways to depressive symptoms. Overall, our findings provided some support for particular aspects of this model with Mexican American families, while showing less robust evidence for particular links. Below, we review the findings of this study.
Overall, there were two major findings. First, within the interpersonal aspects of the model, maternal depression was related to interpersonal stress and conflict with partners, friends, and family members. Similarly, Parke et al. (2004), in their cross-sectional analysis of Mexican American families, also found that maternal depression was associated with conflict in the marital relationship. This finding extends the stress-depression linkage to a community sample of Mexican American women, and is consistent with other literatures suggesting that stress creates vulnerability to depression and that depressed individuals contribute to stress in their own life events, particularly within the interpersonal context (Hammen, 2005). While the causal directionality of the observations cannot be concluded without the use of longitudinal data, such findings hold promising directions for stress generation and stress vulnerability research and indicate support for its relevance among Mexican Americans.
The second important finding relates to the intergenerational aspects of the model, and suggests that poorer parenting quality, in the form of low warmth, high hostility, and high conflict, is related to deficits in the child’s competency and increased risk for depressive symptoms. Consistent with this suggestion, similar findings of maladjustment have been documented with other samples of Mexican Americans where harsh maternal parenting, in forms such as verbal punishment and displays of anger, directly related to the youth’s depressive symptoms (Manongdo & Ramirez Garcia, 2007). Indeed, intervention studies with Latino youth have showed that harsh parenting and parenting efficacy mediated changes in internalizing problems for young adolescents (Gonzales et al., 2008). This finding is consistent with general reviews and meta-analytic findings which have also indicated that an absence of parental warmth is strongly linked to childhood depression (McLeod, Weisz, & Wood, 2007; Sander & McCarty, 2005).
Differences from previous models also emerged in the mediators associated with the prediction of youth depression. Whereas Hammen et al.’s (2004) original findings indicated the transmission of maternal depression to youth depression was fully mediated by maternal interpersonal stress, parenting quality, and youth social competence, no such significant meditational findings emerged in the current study. Additionally, the association between parenting quality and child interpersonal stress was very strong (β = −.55) in our model. The large effect could be due in part to the salience of the maternal relationship in Mexican American families, which may have carryover effects on children’s social relationships. Mexican American youth with positive maternal relationships are either experiencing or perceiving lower levels of stress in relating with their peers. Perhaps they have learned positive ways of relating with others through their mother’s modeling, and are more resilient to interpersonal stress as a result. Another difference emerged in the relationship from maternal interpersonal stress to parenting quality, where our results showed a trend in the direction of a lack of maternal interpersonal support from husband, friends, and family being associated with a more negative parenting quality. However, this trend was not statistically significant. Our findings parallel those of Parke et al. (2004), in whose sample of Mexican American mothers, marital problems were not found to relate to hostile parenting.
Given the importance and centrality of family within Latino cultures (see Sabogal, Marín, Otero-Sabogal, Marín, & Perez-Stable, 1987), it is not surprising that the family context, and not peer context, played a more salient role in child depression. The vital role of family relations for these Mexican American youth appears to be primary in contributing to depressive symptoms, taking on greater influence than relationships with their peers. Additionally, the children in the present study were preadolescents (ages 9 to 12), whereas many models of youth depression have examined older adolescents. In comparison to preadolescents, adolescents report more interpersonal stress events that contribute to a stress-depression relationship (Rudolph & Hammen, 1999), and place a greater influence in the peer domain than the familial domain (Larson & Ham, 1993). Thus, from a developmental perspective, it is highly likely that the preadolescents in this sample are at an age in which social competence and social relationships are less salient than they are for older adolescents, and they may be less vulnerable to developing depressive symptoms in response to interpersonal stress.
There are several methodological limitations in the current study. First, it is important to acknowledge that our study was cross-sectional, and effects over time cannot be captured unless longitudinal data are examined. Second, although the DISC is a validated instrument that is widely accepted for assessing depressive symptoms, diagnoses were not modeled due to low prevalence rates among our sample, and this may have influenced the pathways in our model. Finally, culture-specific variables, such as acculturative stress, were not taken into account. Acculturation is a multidimensional process, and while we did not directly capture it within our model, data that we reported on maternal language and nativity indicates the fact that these mothers may be less acculturated to U.S. culture. Conceptualizing a model that includes acculturative variables for both mothers and children in order to examine how such stressors influence depressive symptoms might reveal interesting and important findings for future developmental psychopathology research. For example, the sample of mothers in this study was predominantly born in Mexico, and while the sampling was not deliberately meant to oversample immigrant women, this may influence the results of the study in that the mothers of these children face increased risk for psychopathology. Mexican immigrant women is a population that has been previously found to have high rates of depression in some studies (e.g., Vega et al., 1998), but not all, as other studies have found that Mexican immigrants reported significantly lower prevalence of depressive disorders compared to U.S. born counterparts (e.g., Alegría et al., 2008). Moreover, these mothers may also face issues of acculturation in their everyday lives, such as separation from family members, language barriers, and assimilation to a new culture. It is important to consider issues of acculturation in future studies that examine mothers of Mexican descent. Another limitation relates to finding that maternal depression was related to interpersonal stress and conflict with partners, friends, and family members. In our study, we did not distinguish single mothers from those with a spouse or partner. Such a distinction may shed light on this finding as single mothers, particularly single immigrant mothers, may be less likely to have social support, which in turn may also influence other aspects of the model such as parenting. Despite these limitations, this study makes an important contribution by testing a theoretical model of depression with a large sample of Mexican American children and their families. Samples such as this are necessary to evaluate and better understand potential contributors to the higher risk of depression among young Latino groups.
There are two major implications from the current study. First, because we found that stress and depression are linked in Mexican American mothers, interventions for depression among Mexican American women may focus on minimizing stress generation and addressing stressful life events. Evaluating the relationships that serve as a source of both stress and support would likely be one strategy for considering factors that may precede or follow depression. For example, greater levels of social support and positive marital quality have been related to a decline in depressive symptoms among Mexican American mothers during the perinatal period (Diaz, Le, Cooper, & Muñoz, 2007), indicating the association is evident during the mother’s childbearing period as well. One might expect to see that addressing interpersonal relationships as they relate to the generation of stress would address depressive symptomatology among Mexican American women, and prevention efforts for this population could incorporate approaches to improve stressful aspects of these relationships.
Second, given the higher rates of depression for children and adolescents of Latino descent, targeting the parenting relationship may be an especially promising approach for interventions aimed at reducing depressive symptoms among these groups. It appears that interventions that improve the quality of maternal parenting could potentially impact social competence, interpersonal stress, and depressive symptoms for Mexican American youth. While less is known about parenting interventions aimed at improving social competence and interpersonal relationships, there are data to suggest that focusing on the promotion of warmth and affection, and decreasing conflict and hostility within the mother-child relationship would be beneficial in the prevention of depression among Mexican American youth (Hill, Bush, & Roosa, 2003). In general, family-focused interventions that address parenting appear to be optimal for this age-group of Mexican American youth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Support for this work was provided by a grant from the National Institute on Drug Abuse and the National Institute on Alcohol Abuse and Alcoholism (DAO17902).