
Abstract
We adapted and piloted an intervention designed to increase condom use among young Hispanic heterosexual couples. Sixty-nine couples were recruited and randomly assigned to either an intervention group (n = 35) or a waiting-list control group (n = 34). Data on condom use and social support for safe sex were collected at baseline, post-intervention, and 3-month follow-up. Although the intervention group had a retention rate of 53%, 86% of all participants completed the 3-month follow-up assessment. Linear mixed-effects models revealed a significant increase in condom use during vaginal and anal sex among the intervention group compared to the control group. The intervention also resulted in increased social support for safe sex practices. These findings suggest that this adapted intervention holds potential for improving sexual health behaviors in this understudied population.
Puerto Rico is a territory of the United States of America (U.S.) severely and disproportionately impacted by the HIV/AIDS epidemic. By January 31, 2025, 52,426 cases of HIV/AIDS have been reported, with 31,773 (61%) resulting in death due to AIDS-related causes (Puerto Rico Health Department, 2025). In 2020 the island ranked 18th in the rate of diagnoses of HIV infection among U.S. states and dependent areas (Centers for Disease Control and Prevention, 2024). San Juan, the capital city of Puerto Rico, was one of the 48 municipalities accounting for 50% of HIV cases in the U.S., making it a national priority area for HIV prevention (Azar, 2019). Heterosexual transmission is the primary mode of HIV infection for women (78%) and the third for men (18%), while other cases (16%) have been reported among adolescents and young adults 15 to 24 years of age (Puerto Rico Health Department, 2025). Chlamydia is the most common sexually transmitted infection (STI), with young adults 20 to 24 years of age accounting for most cases (39%; Departamento de Salud de Puerto Rico, 2023).
Young adulthood is a period of semi-autonomy (Tanner & Arnett, 2009) characterized by identity exploration, career development, and the establishment of romantic relationships (Schwartz et al., 2013). It is also one in which young adults are more prone to engage in risky behaviors (Arnett, 2000). There is no consensus between researchers and national or international agencies about the age range that should be included in this developmental period. While some define young adults as those between 18 and 25 or 18 and 26 years of age (Bonnie et al., 2015; Walker-Harding et al., 2017), others consider a broader age period from 18 to 29 (Fry et al., 2020).
In 2022, young adults aged 25 to 34 years accounted for the highest rate of HIV infection (30.8%) in the U.S. (Centers for Disease Control and Prevention, 2024). Among ethnic groups, Black/African Americans ranked first in new HIV diagnoses, with Hispanic/Latinx individuals ranking second. Different health-related behaviors increase the frequency of their exposure to HIV/STIs, including unprotected casual sex (Lyons et al., 2013). Studies of young adults suggest that motivations for casual sexual encounters include factors such as sexual gratification, the influence of substance use, limited time for committed relationships, geographic transience, and a sense of being too young to pursue long-term partnerships (Lyons et al., 2014). In addition, the use of alcohol and other drugs is frequent among this group (National Institute on Alcohol Abuse and Alcoholism, 2025), as is having sex under the influence of alcohol (Bersamin et al., 2012). Different studies conducted with national samples reveal low rates of HIV testing among young adults who ever had sexual intercourse (Febo-Vazquez et al., 2018; Kaiser Family Foundation, 2017; Van Handel et al., 2016). One of these studies found that those between 15 and 24 years of age had lower rates of HIV testing (36.1% for women and 26.3% for men) when compared with adults 25 to 34 (Febo-Vazquez et al., 2018).
While HIV transmission requires interaction between individuals and often occurs within the context of a relationship, most preventive interventions have focused on individual behavior change rather than addressing the specific risk factors present within those relationships, such as communication patterns, power dynamics, or negotiation of safer sex practices (Pequegnat & Bray, 2012). Although successful in promoting behavior change among couples, interventions of this type have been non-existent in Puerto Rico. A meta-analysis published in 2013 found only 29 interventions that successfully promoted condom use among the main partners of heterosexual couples (LaCroix et al., 2013).
Condom use among ostensibly monogamous heterosexual couples and young Hispanic heterosexual adults is infrequent. Studies reveal that committed relationships are associated with less condom use (Godinho et al., 2024), whereas condom use is more common among casual partners (Milic et al., 2020). This is significant if we consider that Hispanic young heterosexual adults report high levels of unprotected sex and low levels of condom use (Reece et al., 2010).
Couples are an important population to focus on HIV/STI preventive interventions (Jiwatram-Negrón & El-Bassel, 2014; Pequegnat & Bray, 2012). Evidence shows that interventions with couples are more efficacious than those delivered to individuals in increasing protective behaviors (Fu et al., 2023). One meta-analysis published in 2015 showed that coupled-based interventions are more efficacious in increasing protective sex, HIV testing, and Nevirapine adherence among those who are HIV positive (Crepaz et al., 2015). Nevirapine is an antiretroviral (ART) medication used in pregnant women because of its efficacy and low toxicity (Ford et al., 2013). These interventions are not only efficacious for individuals and partners but also in preventing newborn children from getting the infection. Other meta-analyses showed that couple-based interventions are efficacious in increasing condom use (Burton et al., 2010) and decreasing partner concurrency (LaCroix et al., 2013). Partner concurrency refers to “situations in which an individual has overlapping sexual relationships with more than one person” (Pebody, 2009, para. 3). Couple-based interventions are also efficacious in preventing mother-to-child transmission by increasing HIV testing in both partners, uptake of ART by the mother, and increasing a free HIV survival among infants (Hampanda et al., 2022).
Purpose of the Present Study
We implemented a study to adapt and test the preliminary efficacy of a preventive intervention with Hispanic young heterosexual couples (HYHC) in Puerto Rico, called in Spanish Mujeres y Hombres Unidos por una Sexualidad Saludable (MHUSS@), which translates as “Women and Men United for a Healthy Sexuality.” The primary outcome of MHUSS@ was to increase condom use during oral, vaginal, and anal sex. As secondary outcomes, the intervention aimed to increase: (1) HIV knowledge; (2) sexual communication; (3) the endorsement of non-traditional gender roles; (4) sexual decision-making; (5) attitudes toward condom use; (6) relationship satisfaction; (7) social support; and (8) HIV risk perception. To our knowledge, this was the first intervention of this type to be implemented in Puerto Rico and the U.S. The original version of the intervention was implemented by the PI with adult couples in a small 2001 to 2005 pilot study (Pérez-Jiménez et al., 2014). We hypothesized that the intervention group couples would show an increase in main and secondary outcomes in contrast to the waiting list couples.
Our definition of prevention met three of the five dimensions proposed by Romano and Hage (2000). These include: (1) “Stops (prevents) a problem behavior from ever occurring”; (2) “Delays the onset of a problem behavior”; and (3) “Strengthens knowledge, attitudes, and behaviors that promote emotional and physical well-being” (pp. 740–741). The preventive intervention focused on decreasing the possibility of getting HIV/STIs by delaying the practice of high-risk behaviors such as unprotected sex. It was also designed to increase: (1) HIV knowledge, (2) positive attitudes toward condom use, and (3) the use of condoms.
Method
Participants
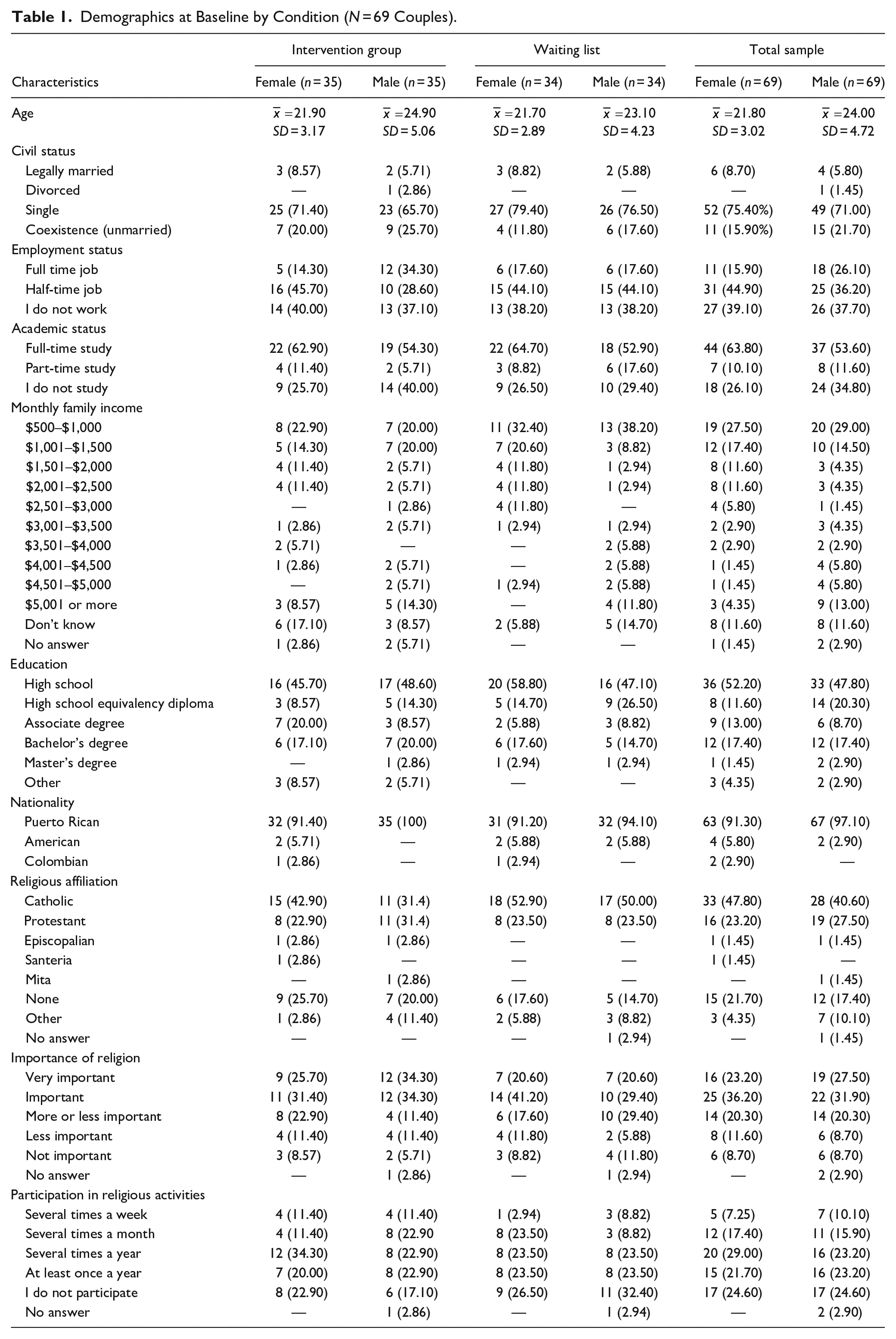
Table 1 shows the demographics of study participants measured at baseline. Demographics did not differ significantly between couples randomly assigned to either the intervention group or the waiting list. The mean ages were 21.9 and 21.7 for the women in the intervention group and waiting list, respectively; for men, 24.9 and 23.1, respectively. Most couples were unmarried, full-time students, and earned a monthly income of $1,500 or less.
Demographics at Baseline by Condition (N = 69 Couples).
We defined couples as those men and women who self-identified as heterosexual and engaged in an intimate relationship with another person, whether they were married or not. Couples were eligible if the woman was 18 to 30 years of age, and the man was 18 years of age or older. In addition, both partners expressed they: (1) had been together for the last 6 months; (2) had the intention to remain together for another 6 months; and (3) had unprotected intercourse in the last 3 months. The decision not to limit the age of the male partner was based on our observation that many young women engage in intimate relationships with older male partners which make them more vulnerable to get HIV/STIs. We did not want to exclude those couples. Eligible women were asked to invite their male partner who was also screened separately. Both partners had to meet these inclusion criteria, including having unprotected intercourse in the last 3 months. The practice of unprotected intercourse was limited to the main partner with whom they planned to attend the intervention.
Couples were excluded if: (1) the female partner was pregnant or planning a pregnancy within the next 12 months; (2) either partner was unwilling or unable to commit to participating in the study to completion; (3) either partner had participated in an HIV sexual risk reduction intervention in the last 12 months; and (4) either partner did not know how to read or write.
Sample Size and Power
Statistical power for the proposed study was calculated using Optimal Design v.1.77 (Raudenbush et al., 2011). This software calculates power and optimal sample sizes to test treatment effects. With n = 2 (one couple), we needed a minimum of 66 couples to have 0.80 power to detect a moderate effect size. At the time of these analyses, the only known intervention with heterosexual couples that had a significant effect on the experimental condition reported an effect size of 0.74 (El-Bassel et al., 2003). We collected more data to account for 10% attrition (a minimum of 33 couples per group, in addition to a 10% attrition rate).
Design
We implemented a 3-year randomized controlled pilot trial with two arms. Couples were randomly assigned to either an experimental condition that consisted of an HIV/STI risk reduction intervention or a waiting list. Couples were randomly allocated in groups of 20 with a single randomization procedure using the Random Allocation Software v.1.0. The expectation was to have groups of no more than 10 couples. The randomization procedure was conducted by the project coordinator, a Ph.D. psychologist. Only the couples that completed the baseline questionnaire were randomized.
Measures
Below we describe the instruments used to assess the feasibility and effect of the intervention. All instruments were administered in Spanish. Scales that were originally in English were translated by professional translators following a process of translation, back-translation, and then culturally adapted by a group of experts (Gjersing et al., 2010). The final questionnaire was piloted in March to April 2010 with a group of 30 students from the University of Puerto Rico. Small modifications were made to some items following students’ recommendations.
Feasibility and Adherence Measures
Each participant evaluated all sessions in a written survey comprised of closed- and open-ended questions. The questions assessed how much the participants learned, how they felt during the sessions, and what they thought of the content of the sessions and the work carried out by the facilitators.
To ensure facilitators’ adherence to the intervention, we designed and implemented a fidelity adherence protocol. The protocol measured adherence in four criteria: (1) structure of the activities; (2) content of the activities; (3) order of the activities; and (4) time allotted for each activity. Each criterion received a maximum of 25 points. To obtain the percentage of session fidelity, the fidelity scores for each activity were added and divided by the number of activities in each session. A score of 100 to 90 was interpreted as excellent; 89 to 80 as good; 79 to 70 as satisfactory; and 69 or less as poor adherence.
Primary Outcome Measures
Condom use was measured using the Sexual Risk Behavior Questionnaire, which covers the 90 days prior to the interview and is focused on sexual behavior with primary and secondary partners. It asks for the frequency of (1) vaginal, anal, and oral sex; (2) male condom use; (3) practice of mutual masturbation; and (4) sex under the influence of alcohol or drugs.
Secondary Outcome Measures
Knowledge of HIV/AIDS was measured using the Basic HIV/AIDS Information Scale, which was also used in a previous study by our research team (Pérez-Jiménez et al., 2014). This scale consists of 15 items and has a reliability coefficient of 0.62. It measures knowledge of HIV prevention and transmission and includes concepts such as safe sex, HIV, and high-risk behaviors. Couples’ sexual communication skills were assessed using an adapted version of the Dyadic Sexual Communication Scale (Catania, 1998). We used a 7-item scale that measures the level of reported comfort with safe sex communication. Traditional gender roles were measured with the Gender Roles Scale, which was developed by our research team for another study. This scale consists of 15 items with 9 questions about male gender roles and 6 questions about female gender roles. It has a reliability coefficient of 0.77 (Pérez-Jiménez & Orengo-Aguayo, 2012). To measure sexual decision-making, we used the Sexual Decision-Making Scale (SDMS) and the Sexual Relationship Power Scale (SRPS; Pulerwitz et al., 2000). The SDMS consists of 6 items and has a reliability coefficient of 0.72. The SRPS measures decision-making power, negotiation ability in intimate relationships, and the role of relationship power in sexual decision-making and risk of HIV. The SRPS contains two subscales with 23 items that assess certain conceptual dimensions of relationship control such as decision-making, condom negotiation skills, and freedom of action within the relationship. This scale has good internal reliability with low-income, minority women, and has a coefficient alpha of .84 (Pulerwitz et al., 2000).
Attitudes toward male condom use were measured using the Attitudes toward Male Condom Use Scale. This scale contains 16 items that measure opinions of condom use in terms of sexual excitation, comfort, embarrassment, and distractions. This scale has a reliability coefficient of 0.71. Relationship satisfaction was assessed with the Revised Dyadic Adjustment Scale (Spanier & Thompson, 1982). This scale consists of 31 items that ask each partner about intimacy, relational factors, how they spend their time together, and how they discuss family finances with each other.
Sexual satisfaction in couples was measured using the Golombok-Rust Inventory of Sexual Satisfaction (GRISS; Rust & Golombok, 1985). The GRISS has a male and a female version, each with 28 questions to which respondents indicate the frequency of occurrence on a 5-point scale. On both the male and female forms, responses to 4 of the 28 questions can be summed and then transformed to a 9-point scale to yield a global measure of sexual satisfaction. The subscales for the male version of the GRISS are (1) impotence; (2) premature ejaculation; (3) male non-sensuality; (4) male avoidance; (5) male dissatisfaction; (6) infrequency; and (7) non-communication. The female GRISS has subscales for (1) infrequency; (2) non-communication; (3) female dissatisfaction; (4) female avoidance; (5) female non-sensuality; (6) vaginismus; and (7) anorgasmia.
Social support for risk reduction was measured with the Social Support for Male Condom Use Scale. This scale consists of 11 items that measure opinions on social support in terms of tasks, advice, and emotional and material support. This scale has a reliability coefficient of 0.91. Finally, HIV risk perception was measured with a single question that asked participants how much risk they believed to have of getting HIV. The response scale for this question ranged from none to higher risk.
Intervention Description
The experimental intervention was an adapted version of a previous intervention designed and implemented by our research team in a pilot study with adult couples (Pérez-Jiménez et al., 2014). The intervention consisted of five 3-hr sessions, and its primary aims were to increase male condom use and the practice of mutual masturbation and reduce the frequency of unprotected sex.
The intervention was theoretically based on the Information-Motivation-Behavioral Skills (IMB) model of HIV preventive behavior (Fisher et al., 2009). The IMB model has been widely implemented with different populations and addresses different health issues including patients with coronary heart disease (Li & Zhu, 2022), prevention of Human Papillomavirus infection in women (Si et al., 2021), and adolescents with diabetes (Lee et al., 2019). The model includes HIV risk-reduction information, motivation, and behavioral skills as important determinants of HIV-preventive behavior. Its authors state that access to more accurate information about HIV transmission and prevention, and motivation to engage in HIV preventive behavior, influence the acquisition and development of the necessary behavioral skills for HIV preventive behavior.
To adapt the intervention we used the ADAPT-ITT model developed by Wingood and DiClemente (2008). It consists of eight sequential phases that guide the adaptation process. The intervention was delivered in Spanish and consisted of five 3-hour sessions. Weekly sessions were implemented by two psychologists, one male, and one female, experienced in group dynamics. In sessions 1 and 5, couples were placed in the same room. In sessions 2, 3, and 4, the male and female partners were separated to allow for free discussion of sensitive topics such as condom use, the practice of anal sex, and sexual negotiation.
The objectives of session 1 were to: (1) encourage couples to get to know each other; (2) clarify the roles and expectations of the couples and facilitators; (3) encourage couples to complete the intervention; and (4) identify the positive traits of each partner. The objective of session 2 was to improve couples’ communication skills via the speaker-listener technique. Couples were encouraged to identify the barriers that affected their communication.
The objective of session 3 was to increase HIV risk perception. We discussed the transmission and prevention of STIs and the physical indicators and repercussions of STIs. HIV/STI testing was promoted as a preventive measure. In addition, we addressed couples’ motivations behind high sexual risk decisions. Non-penetrative practices were promoted as safer sex alternatives.
The objective of session 4 was to promote condom use. Group dynamics were implemented to promote positive attitudes toward condom use and a sense of self-efficacy in condom use negotiation. These dynamics also promoted condom use negotiation skills to manage situations where a partner refuses to use condoms. Lastly, in session 5, we promoted the development of sexual negotiation skills. Couples were asked to identify their partner’s reasons for refusing to use condoms in the negotiation process. In this final session, we also addressed the importance of support between partners in the promotion and maintenance of safer sex practices.
Procedure
To recruit couples, we conducted different activities that included: (1) placing an ad in two of the main newspapers on the island; (2) sending a message through the email network of the UPR system; (3) distributing brochures at the UPR; (4) presenting the project to students of the UPR in Carolina; (5) promoting the project at a community-based organization that provides family planning services to couples; (6) through the snowball technique; (7) placing an announcement in online classifieds; (8) handing out flyers on the university avenue, which is a place where university students hang out; and (9) through a Facebook page of the project.
Couples were screened by phone with an instrument designed to determine eligibility. Post-screening, eligible couples were invited to an orientation session that was conducted in person about the objectives and characteristics of the study and the expectations for their participation. Unmarried and legally married couples were allowed to participate.
Couples completed the baseline questionnaire, post-test, and 3-month follow-up. In most cases, the couple came together to complete the questionnaire. Each partner was placed separately for the privacy and accuracy of the information and to prevent other partners’ influence. They were informed of this process at the orientation session, and they had to agree not to ask their partner how they answered some questions. Each room had a research assistant available to answer the participants’ questions. In the orientation session, the members of each couple were asked to respect and commit to the process, as well as not to inquire their partner about their answers to the survey.
The study was conducted at the Institute for Psychological Research of the University of Puerto Rico, Río Piedras Campus. Participants received monetary compensation for completing the baseline questionnaire ($30), post-test ($40), and 3 months follow-up ($50). To standardize protocol implementation, we designed a quality assurance procedure that included a detailed intervention manual, careful selection of qualified and experienced personnel, and ongoing monitoring of the fidelity of implementation and adherence to the intervention protocol. Data was collected using the Audio Computer Assisted Self-Interview (ACASI), which significantly decreases social desirability bias in contrast to face-to-face interviews (Pluhar et al., 2007). Preliminary analyses were performed to ensure the similarity of the two groups at pre-test.
Analysis
Unless otherwise noted, the effect of the intervention on primary and secondary outcomes was evaluated using multi-level modeling (Heck et al., 2014). A linear mixed-model regression was applied, and SPSS v.24 software was used. To account for design effects, the three-time points were nested within individuals, which, in turn, were nested within couples. In addition, the “variance components” covariance type was used since only the intercepts were allowed to vary randomly (Heck et al., 2014).
The following equation describes the multilevel model for individual i in couple j:

This equation implies that variation in intercepts is described by a couple-level intercept (γ00), or grand mean, and a random parameter capturing variation in individual couple means (μ0j) from the grand mean while accounting for the individual level error (εij). In addition, there are no random components in the slopes (μ1), which is why the slope coefficients are fixed to one value for the sample. In summary, this equation reflects that the components representing the individual level slopes (γ10, γ20, and γ30) are multiplied by Groupij, Timeij, and Groupij × Timeij, respectively, which suggests it is a cross-level interaction, but with variance fixed to zero at the couple level.
Results
Recruitment and Retention
Recruitment of couples took place from October 2010 to September 2011. The intervention took place from May 2011 to October 2011. The follow-up was extended through December 2011. The most effective strategies for recruitment were the advertisements published in the newspapers and sending a message through the email network of the UPR system. As shown in the CONSORT diagram (Figure 1), we screened 146 couples for eligibility, of which 24 did not meet the inclusion criteria. Of the screened couples, 122 (84%) met the eligibility criteria and were invited to the orientation session. Of the eligible couples, 69 (57%) completed the baseline questionnaire and were randomized: 35 to the intervention group and 34 to the waiting list. We had originally planned to recruit 66 couples, which was the sample size recommended by our statistical consultant as necessary to have 0.80 power and detect a moderate effect size. Twenty intervention group couples (57%) and 32 waiting list couples (94%) completed the post-test. At 3 months follow-up, we were able to retain 19 intervention group couples (54%) and 31 waiting list couples (91%).
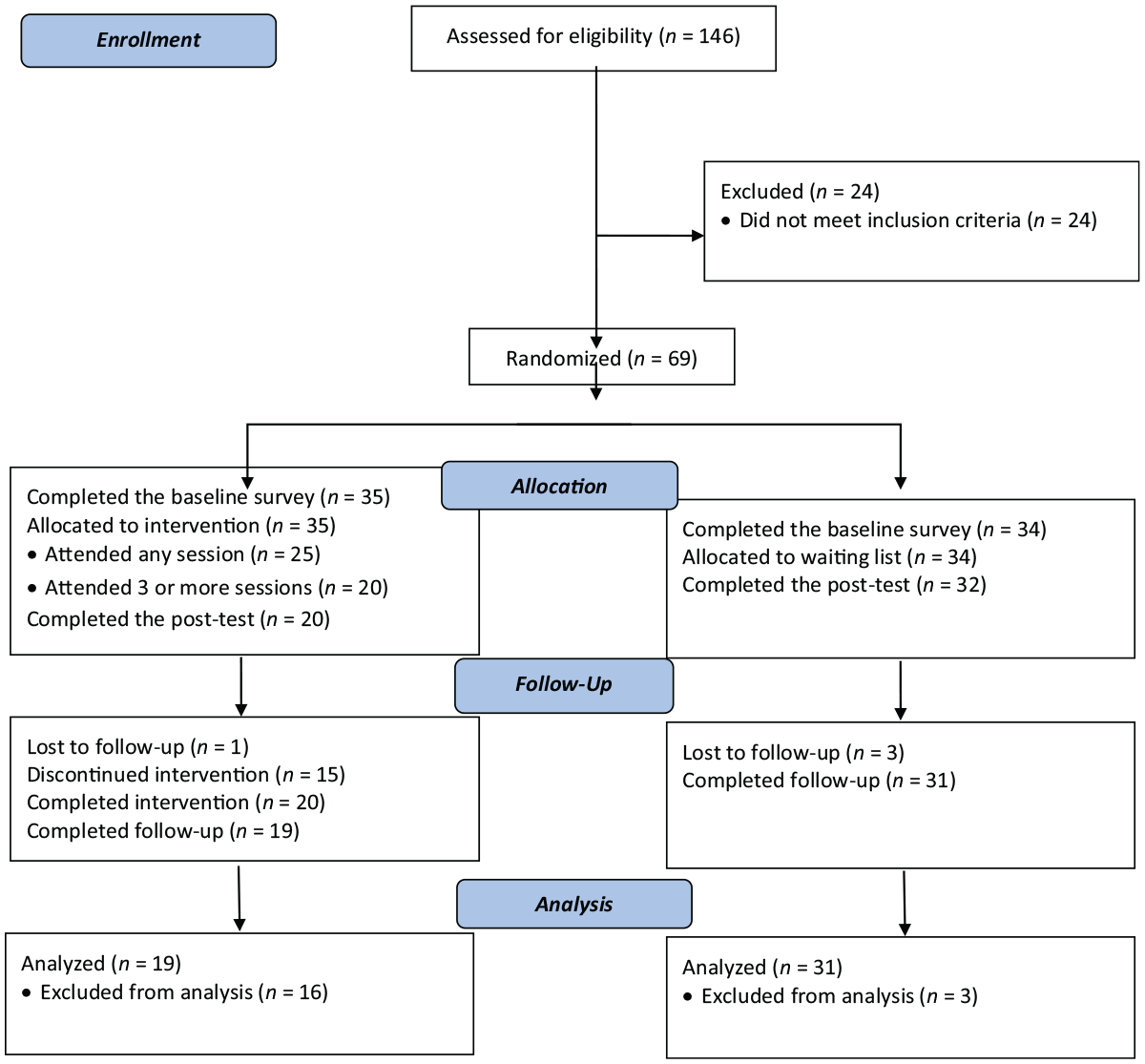
CONSORT flowchart of participant couples.
Of the 35 intervention group couples, 25 (71%) attended at least one session, whereas 20 (57%) attended three or more sessions. This attendance rate resembles that of other studies conducted with couples (Witte et al., 2004). Among the reasons couples provided for not attending were: (a) conflicting work schedules; (b) no longer in a relationship; (c) lack of time to attend all sessions; and (d) need for childcare. The retention rate for the assessment of the total sample was 52 couples (75%) at post-test and 50 couples (72%) at 3 months follow-up.
Acceptability
We evaluated the acceptability of every session and conducted a general evaluation of the intervention. We did not find significant variability by session. Most participants (95%) reported feeling comfortable or very comfortable during the sessions and that the sessions were good or very good. All participants (100%) rated the work of the facilitators as good or very good, and 88% reported that they learned much or very much during the sessions.
Facilitators’ Adherence to the Intervention
Session 1 had a facilitators’ adherence of 97%; session 2: 91%; session 3: 93%; session 4: 89%; and session 5: 91%. This produced an overall adherence of 92%, which we interpret as excellent. This slight decline in adherence is because the sessions became progressively complex in terms of activities and materials. We also evaluated the adherence to the orientation session, which consisted of a description of the study objectives and the couples’ expected participation. In addition, we further developed a manual that was used by the graduate psychology students who served as orientation facilitators. We simultaneously conducted 40 sessions with individual couples and 17 sessions with two couples. Of the 57 orientation sessions, we randomly chose a representative sample of 10 sessions that were evaluated for fidelity. We obtained 88% general adherence in the sessions.
Intervention Effect
Table 2 reports the means and standard deviations for the study’s primary and secondary outcomes at pre-intervention, post-test, and 3 months follow-up time points. As shown, the intervention group had a significant increase in the frequency of condom use during vaginal sex from the pre-intervention to the 3 months follow-up when compared with the waiting list (p < .05, β = .18). Similarly, the intervention group had a significant increase in the frequency of condom use during anal sex across the three-time points when compared to the waiting list (p < .05, β = .32). As shown in Table 2, while we did not find a statistical difference among groups, the frequency of condom use during oral sex increased after the 3 months follow-up for the intervention group, while it decreased for the waiting list.
Intervention Effect Compared to the Waiting List on Primary and Secondary Outcomes (N = 50 Couples).
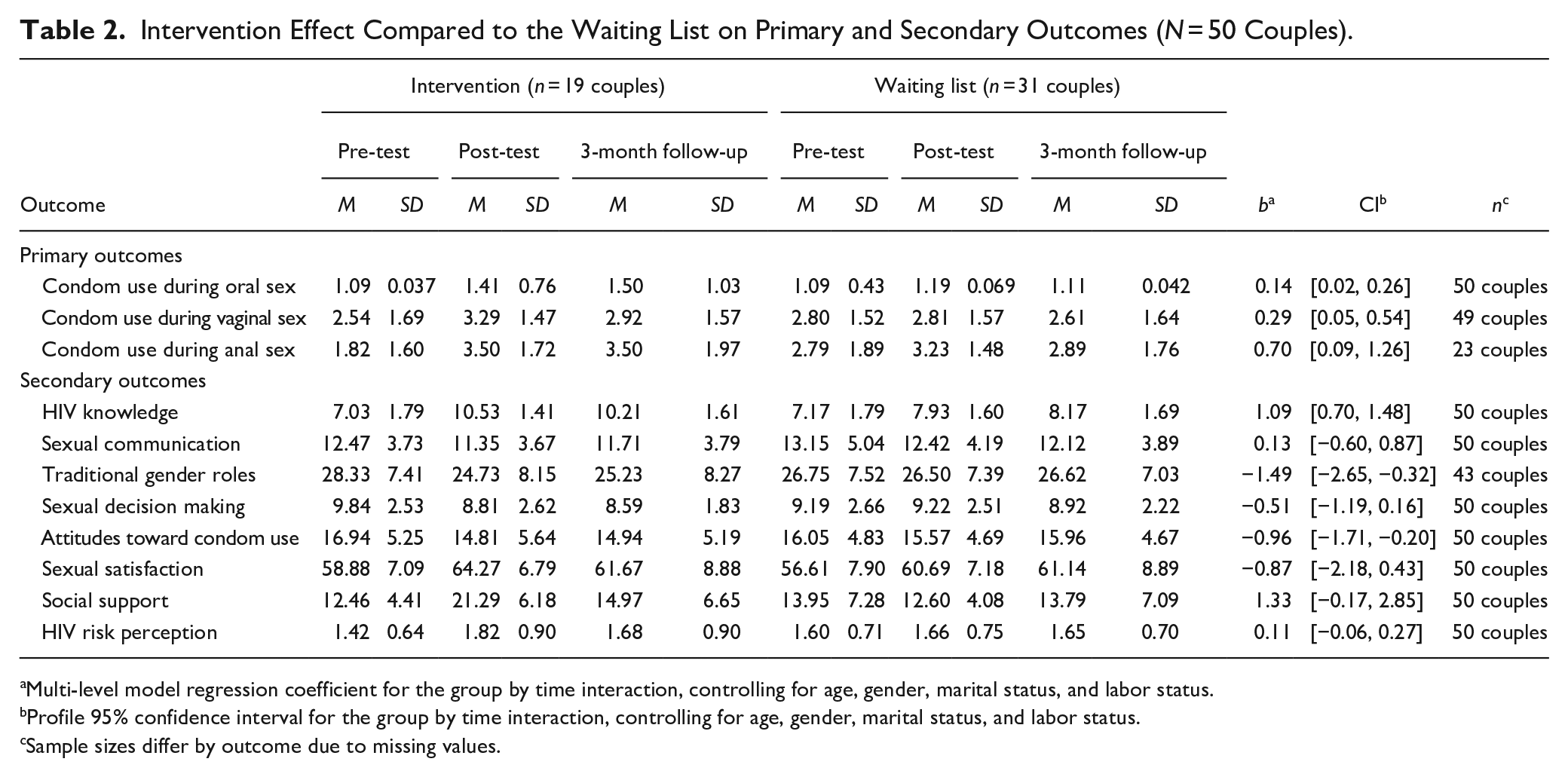
Multi-level model regression coefficient for the group by time interaction, controlling for age, gender, marital status, and labor status.
Profile 95% confidence interval for the group by time interaction, controlling for age, gender, marital status, and labor status.
Sample sizes differ by outcome due to missing values.
Regarding the secondary outcomes, the intervention group had a significant increase in social support from the pre-test to the 3 months follow-up when compared to the waiting list (p = .047, ηp2 = .03). Although generally small and not significant, all other effects showed inclination toward better outcomes for the intervention group. For example, participants in the intervention group had a non-significant increase in HIV risk perception (p > .05, β = .04) and a non-significant decrease in attitude problems toward condom use (p > .05, β = −.13), problems in sexual decision-making (p > .05, ηp2 = .02), and problems with traditional gender roles (p > .05, β = −.12) across the three time points. Contrary to expectations, there were no trends in the size of change between conditions in HIV knowledge (p > .05, β = .02), sexual communication (p > .05, ηp2 = .00), and relationship satisfaction (p > .05, ηp2 = .00) from the pre-intervention to the 3 months follow-up.
Discussion
To our knowledge, this is the first preventive study conducted with HYHC on the Island. The study yielded significant results on the feasibility and preliminary efficacy of an intervention aimed at preventing HIV/STIs among this group.
Intervention Feasibility
Study findings showed it is feasible to recruit and retain HYHC in prevention trials. For recruitment, it is important not to focus on only one activity, but to diversify the strategies to reach more people. We were surprised by the success of sending the promotion through the email network of the UPR system. We started receiving calls as soon as we sent the message. We are sure that this was due to a great need for counseling and education services that young couples have to improve their communication and resolve their conflicts, particularly on issues related to their sexuality. Our promotional material emphasizes the strengthening of communication skills to improve their sexual health.
Regarding the retention rate, it resembled that of similar studies (El-Bassel et al., 2003; Koniak-Griffin et al., 2011). We need to pay close attention to the barriers that may render it difficult to retain couples in group interventions. Research conducted with couples has found that other barriers to recruitment and retention include recruiting the couple through women versus both partners, talking about sensitive issues in front of other couples, which makes participants feel uncomfortable, lack of time, and child-care needs (Pappas-DeLuca et al., 2006). Sexuality remains taboo among Hispanics (Barral et al., 2020; Jerman & Constantine, 2010), which might have influenced couples to refrain from openly discussing their sexuality in the presence of others. Although the intervention did not require couples to openly discuss their sexuality, we believe that many participants may have felt intimidated by this possibility. In our work with HIV-discordant couples, we also found that working and fear of disclosing the serostatus were some of the main barriers to participating in preventive interventions in HIV-discordant couples (Hernández-Hernández & Pérez-Jiménez, 2010). In this study, we had couples where one or both partners revealed they had an STI (e.g., Human Papillomavirus). We believe there are couples who do not have difficulties in revealing intimate information to others, but also that there are couples who are not willing to do so.
This is particularly important if we consider the couples’ high level of acceptability and satisfaction with the intervention. Moreover, this data was obtained through a questionnaire that guaranteed anonymity, which encouraged them to openly express their feelings and opinions. Based on previous studies, we learned that evaluations of interventions cannot be limited to oral evaluations since participants will otherwise hesitate to openly express their dissatisfaction with any aspects of the intervention. Based on the high level of satisfaction, we believe that the retention rate should have been higher and that this issue warrants further research. The facilitators’ high level of adherence led us to rule out any problem with the implementation of the intervention.
Intervention Effect
In terms of the effect of the intervention on the primary outcomes, it showed promise in increasing the frequency of condom use for vaginal and anal sex, but not for oral sex, when comparing the intervention group with the waiting list. This finding is not surprising considering that young people use condoms more often to prevent a pregnancy than an STI (Blanc Molina & Rojas Tejada, 2018). Studies also show that oral sex is a common practice among young people, but condom use is very low, especially in those having vaginal intercourse (Stone et al., 2006), and belonging to racial and ethnic minorities (Holway & Hernandez, 2018). Reasons for not using condoms during oral sex include believing that oral sex is less risky than vaginal sex, being engaged in a committed relationship, the belief that it reduces pleasure, and lack of motivation (Holway & Hernandez, 2018). We recognize that promoting condom use within couples is challenging, especially if they are married. We believe that presumed monogamy, communication, and the desire to have children or prevent pregnancy can influence preventive behaviors.
Regarding the secondary outcomes, the intervention only demonstrated the effect of increasing social support to practice safer sex. We believe that this may be explained by the principle of “sufficient dosage” proposed as one of the principles of effective prevention programs (Nation et al., 2003). According to this principle, participants need “to be exposed to enough content of the intervention for it to have an effect” (p. 452). It caught our attention that the last session of the intervention was mostly dedicated to the importance of social support, contrary to the other secondary topics. Based on this principle, it is necessary that to have a greater impact, more time is devoted to those topics that are more important for the intervention, especially if they are focused on skills development. Meta-analysis has documented that one of the characteristics of effective interventions consists of promoting the development of interpersonal skills (Covey et al., 2016).
We did not expect that the intervention would show no effect on the secondary outcome variables of HIV knowledge and HIV risk perception. These are important predictor variables for behavior change according to different theoretical models (e.g., the Health Belief Model, the Theory of Planned Behavior), and the IMB framework used in this study (Fisher et al., 2009). Regarding HIV knowledge, studies reveal the existence of a mismatch between HIV knowledge and the adoption of safer sex practices. This means that, although people report knowing how HIV is transmitted and prevented, they continue to practice unprotected sex. Different factors have been identified as possible moderators of this relationship including, peer pressure (Do et al., 2014), the perception of condom use by peers (Yu et al., 2022), stoicism toward death, and the culture of silence (Mwale, 2008), and self-efficacy (Oppong Asante et al., 2016). We also believe that during the implementation of the study, there was a saturation of information regarding the transmission and prevention of HIV, which could have influenced these results. Concerning the HIV risk perception, the intervention had a positive effect, but the differences observed between groups were non-significant. A recent population-based longitudinal study showed that increasing HIV risk perception influences condom use, but also those who had a decrease in risk perception were more likely to use condoms when compared with those reporting no change in risk perception (Schaefer et al., 2020). Qualitative studies have documented that HIV awareness and risk perception are high among youth, but other factors such as hegemonic masculinity and perceptions of personal invulnerability difficult the adoption of safer sex practices (Ganle, 2016). This is reflected in the belief that “although I may be at risk, nothing will happen to me.” Research shows that increasing the HIV risk perception, although important, is not sufficient to reduce risky behaviors (Chimwaza et al., 2022).
Regarding the variable of attitudes, we were not surprised by the results because research reveals that, in general, young people have positive attitudes toward condoms (Appiah et al., 2017), and many use them for pregnancy prevention (Davids et al., 2021; Szucs et al., 2020). With the other secondary outcome variables (e.g., gender roles, sexual decision-making, sexual communication, and relationship satisfaction), we were also not surprised to find no significant differences. For example, studies previously conducted by our research team found that many younger, educated women already challenge traditional gender roles and demand more egalitarian relationships (Pérez-Jiménez & Orengo-Aguayo, 2012). In addition, changing couples’ dynamics that influence the adoption of safer sex practices is a more complex process that requires taking into consideration what Karney et al. (2010) call a process of “successful coordination.” This means that negotiating safer sex is a dyadic process that requires the coordination of two individuals who “act together to achieve a specific goal” (p. S190). Based on our experience, we are now convinced that pretending to change those unhealthy dynamics should be a primary outcome of any intervention.
Limitations
This study had several limitations. First, a university strike affected the recruitment process during the implementation of the study. Second, most calls were received from women interested in participating, but sometimes their male partners did not express the same interest. Third, many couples were reluctant to participate in a group intervention where they would have to share with other couples. Fourth, it proved a challenge to set a schedule suitable for all couples. Fifth, many couples expressed a preference to be assigned to the intervention group instead of the waiting list, proving a bigger challenge to retain couples assigned to the waiting list. Finally, a key limitation of this study is the over-representation of college students in the sample. This raises concerns about the generalizability of the findings to the wider Puerto Rican population, particularly those with less education or a lower propensity to participate in research. The heavy reliance on email recruitment targeted at students likely exacerbated this issue. Future research must actively employ diverse recruitment methods, beyond student-focused channels, to ensure a more representative sample and improve the validity of findings for the broader Puerto Rican community. Future research should also explore the relationship between marital status, reasons for condom use, and sexual health outcomes in more detail.
Conclusion
Despite the limitations, the present study showed promising effects of an intervention that aims to increase safer sexual practices in HYHC. Although we could not prove the effect of the intervention on most secondary outcomes, we believe that an efficacy study with a larger sample could yield better results. Future research should consider the social and cultural barriers that render it difficult for couples to participate in group interventions with other couples. We believe that using an individual couples’ counseling format in this intervention would have observed a higher retention rate and a greater impact on couples’ sexual health and overall well-being. The individual couples’ counseling format has been implemented in other studies and has proven to be a successful delivery format (El-Bassel et al., 2003).
Footnotes
Acknowledgements
We would like to acknowledge the following persons for their support: Lymari Díaz Meléndez (Program Co-Coordinator), Dr. Francisco Millán (Clinical psychologist, Co-facilitators of the intervention), Jesús M. Ortega-Guzmán (Data Manager), Nabila Irizarry-Martínez, David López-Garay, Stephanie M. Adorno-Galay, and Francisco Rodríguez (Research Assistants). Special thanks to Antonia M. Villarruel (Consultant) and Luis M. Reyes Rivera (Grammar Editor).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Award R34MH085511 from the National Institute of Mental Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health of the National Institutes of Health.
IRB Approval
This study was revised and approved by the Institutional Review Board (IRB #00000944) of the University of Puerto Rico, Río Piedras Campus (Protocol #0809-147).