
Abstract
Health disparities continue to negatively impact the well-being of Latines and are perpetrated due to internal and external treatment barriers. Cultural adaptations improve Latines engagement in research studies, however, are limited due to a lack of information about daily experiences and health-related challenges. Ecological momentary assessment (EMA) provides a potential solution to understanding Latines daily behaviors and challenges as it reduces recall bias, collects behavioral data in real-time, provides information about maladaptive patterns, and can inform the cultural adaptation of behavioral health treatments. EMA has numerous benefits, however, there have been little to no cultural considerations for Latines. The Latine population exhibits high rates of cell-phone usage, yet it remains unclear how EMA has been used with this population specifically. This systematic review identified 26 articles with samples partially or completely consisting of Latines participants (18 years or older) who completed electronically delivered EMA prompts. Health behaviors and disparities directly targeted by these articles were summarized in addition to common EMA designs, adaptations, and challenges observed among the Latine community. Recommendations for using EMA more effectively with Latines were provided to serve as a guide for researchers who aim to produce higher quality research with this population.
Keywords
Introduction
Health Disparities Among Latines
Latine's constitute approximately 18.7% (62.1 million) of the U.S. population with continuous growth each year (Jones et al., 2021). Health disparities continue to persistent among this community due to internal (e.g., stigma, values, beliefs, etc.) and external (e.g., cost, scheduling flexibility, language barriers, lack of health care coverage, etc.) barriers (Falgas et al., 2017). Experiencing a greater number of treatment barriers results in diminished access to behavioral health services; this is problematic given the underutilization of behavioral health services and high dropout rates noted in Spanish-speaking Latine’s (Benuto & Leany, 2017). In fact, health disparities and consequences of these disparities (e.g., chronic diseases, higher mortality rates, etc.) are more common among many hard-to-reach Latine adults—those who live in rural communities, are predominant Spanish speakers, have low socioeconomic status, or have low mental health literacy (Benuto et al., 2019). The continuous growth of this population demonstrates the need for novel treatment and intervention modalities that can be easily distributed to hard-to-reach individuals, are feasible for those with limited access to health care and can lessen the health disparities that current intervention modalities have been unable to diminish or eliminate.
Cultural adaptations of health interventions have made treatments more accessible for Spanish-speaking Latines. In fact, tailoring behavioral health treatments to align with Latine cultural values and practices result in better outcomes for mental (Benuto & Leany, 2017) and physical health behaviors (Barrera et al., 2013). The first stage of cultural treatment adaptations is information gathering, followed by preliminary design, preliminary testing, refinement, and final trials (Barrera et al., 2013). Unfortunately, many hard-to-reach Latines remain underrepresented in research studies. This barrier tied with difficulties accessing many individuals of the Latine community creates difficulties beginning the first stage of treatment adaptation. Information about daily experiences with adapted treatments can provide rich data for the following stages of research (e.g., preliminary design) and enhance treatment interventions for this population. Fortunately, ecological momentary assessment (EMA) is a useful tool in bridging the current research gap given the high rates of smartphone ownership among Latines (Schueller et al., 2019).
Ecological Momentary Assessment (EMA)
Ecological momentary assessment collects sequenced data in real-time about daily health behavioral changes and outcomes electronically (Soyster et al., 2019). EMA is a feasible approach for adult Latines given that approximately 98% of Latines in the U.S. own a smartphone, 95% use the internet, and 25% utilize their phones as their primary way of accessing the internet at home (Nielsen Company, 2020; Pew Research Center, 2021). EMA is also useful in understanding momentary fluctuations in experiences, however, researchers continue to heavily rely on retrospective measures. Self-report measures are plagued by recall bias whereby the responses provide inaccurate information about current phenomena due to limited memory, estimations, or inferences (Runyan et al., 2013). Certain health conditions worsen memory performance among adults (Varghese et al., 2022), creating more biases with self-report measures. EMA with adults overcomes this issue while providing higher ecological validity as research is completed in a natural setting, allowing for greater generalizability to everyday life (Runyan et al., 2013). Recall bias continues to be problematic, therefore, an EMA approach increases the ecological validity of research studies and aids in the information gathering stage.
Benefits of EMA
Delivering EMA electronically combats the back-filling problem, which occurs when surveys are completed later than originally scheduled because participants fail to complete them at the scheduled time (Trull & Ebner-Priemer, 2009). Electronic surveys are time-stamped, making it easier to identify when participants have failed to complete surveys at the scheduled time. Additionally, electronic diaries result in higher compliance rates (Trull & Ebner-Priemer, 2009), which are not impacted directly by specific participant demographic characteristics (i.e., age, sex, race, education level) or psychopathology (i.e., PTSD, mood, anxiety, and substance use; Soyster et al., 2019). With increasing access to the internet and smartphones, EMA has become a feasible and valuable tool to study different phenomena and daily experiences within various contexts.
The use of EMA with adults is gradually increasing as it provides more accurate and reliable information of daily experiences. This approach shows dynamic changes in mood, thoughts, symptoms, and behaviors (Runyan et al., 2013), which are necessary to understand when culturally adapting health interventions for adults. Within a clinical setting, understanding client patterns is necessary to provide more effective clinical care (Soyster et al., 2019), accurately evaluate clinical problems, recommend appropriate treatments, and assess treatment outcomes (Trull & Ebner-Priemer, 2009).
Cultural Considerations for EMA
Thus far, there have been few discussions in the literature on cultural considerations when using EMA with Latines, despite that it can help us understand health inequities that are rampant among this population. Research implementing EMA as a mechanism for developing and disseminating culturally adapted treatments is limited. Of the studies delivering health interventions to adults using EMA, a literature review demonstrated that demographic characteristics are not provided in some studies and Latines continue to be underrepresented in other studies (Gonzalez et al., 2021). Most of the current literature discussing EMA and culture state the importance of including diverse samples (Greene & Maggs, 2018; Jelsma et al., 2021), while a few recommend adapting health interventions for minoritized people (Cohen et al., 2020; Hernandez-Ramos et al., 2022). Unfortunately, no peer-reviewed works were identified that provided specific and concrete recommendations on adapting EMA for adult ethnic/racial minorities, or Latines in particular.
As previously noted, EMA has a myriad number of benefits. EMA can be particularly useful for Latines as it is a low-cost methodology. Additionally, it can provide rich, within-person, culturally relevant data; identify real-time intervention adaptations; determine mechanisms maintaining health disparities among hard-to-reach populations; and determine novel methods of addressing health disparities (e.g., phone-based interventions). Information about cultural ideologies, meanings, beliefs, and values can also be generalized to others with similar cultural backgrounds rather than generalizing findings from predominantly non-Latine White samples. To reduce health disparities among Latines, further understanding of their daily behaviors is needed. Conducting EMA research with Latines would enhance current knowledge about cultural aspects that influence daily health behaviors, disparities, inequities, treatment dropout, and low use of health services. Recommendations for adapting EMA for Latines are drastically needed to produce high quality EMA research with minorities, develop a deep understanding of daily challenges with current treatments, and test the effectiveness of treatment adaptations for these hard-to-reach individuals.
This all suggests that studying daily behavioral health patterns of Latines electronically via EMA may be a useful methodology for increasing access to health services and target current health disparities. As of now, few EMA research studies have focused primarily on Latines. Therefore, the goals for this systematic review were to (1) identify health behaviors and disparities previously addressed using EMA with Latines broadly, (2) identify common design considerations, adaptations, and challenges when using EMA with Latines, and (3) develop guidelines and recommendations for using EMA with adult Latines.
Methods
Peer-reviewed studies published in journals through July 2025 using EMA with Latines were identified via searches on the following databases: Embase, PsychINFO PsycARTICLES, PubMed, and Web of Science. The search timeframe did not exclude studies based on publication date as long as the study was published by July 2025 and met the inclusion criteria. The following EMA search terms were used: EMA, ecological momentary assessment*, ecological momentary, real time, intervention, EMI, experience sampl*, electronic diar*, intensive longitudinal, cell phone-based EMA, CEMA, ambulatory assessment*, and momentary time sampl*. EMA terminology was combined with the keywords “Latin* OR Hispanic*” AND “Adult*” (see Figure 1 for search string). Inclusion criteria were: (1) sample included Latines/Hispanics, (2) all or part of the sample was 18 years or older, and (3) participants completed electronic self-report EMA.
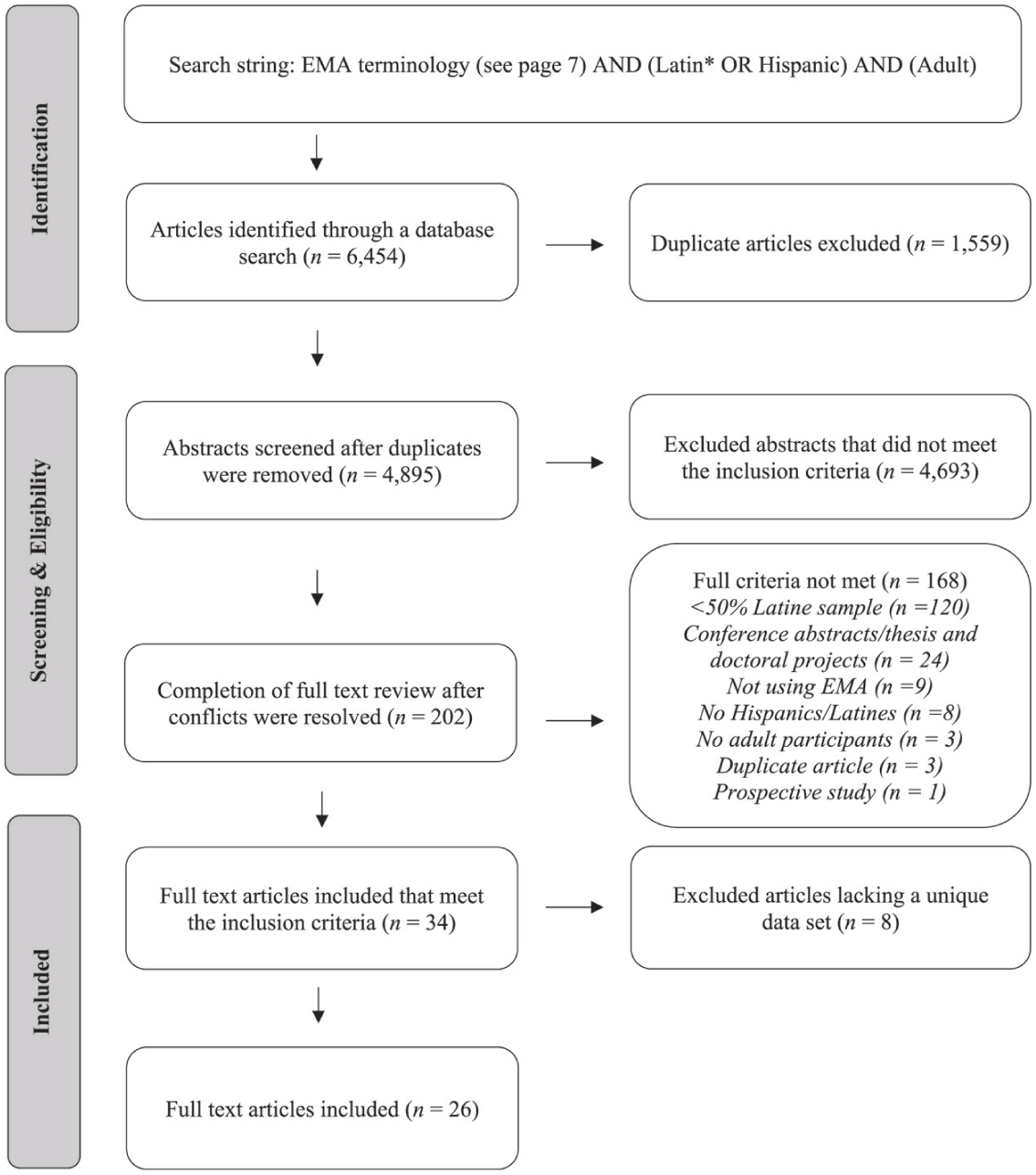
Flow chart showing the identification and selection of articles included in this review.
Studies were excluded if the study only included children or adolescents, the sample size was less than 50% Latine participates, they were duplicates, or they used the same sample as another study. Adult populations were the focus of this review as the approach between adults and adolescents/children may be different due to academic time constraints, which require EMA data collection to occur outside of school hours, or potential hesitancy related to sensitive topics, such as substance use behaviors. Articles that included less than 50% Latine participants were excluded due to low inclusion rates of Latines. Articles with a small number of Latine participants were excluded because of limited between-article comparisons and lower external validity. Duplicate studies were removed, and articles were screened using the inclusion criteria by two independent reviewers on Rayyan. The following data was extracted from the studies meeting the inclusion criteria: basic study information (author and year), focus of the study, sample characteristics (sample size, percentage of Latine participants, age, gender), EMA prompt design, adaptations or challenges, and compliance rates.
Literature Search
As seen in Figure 1, the initial search identified a total of 6,454 articles and 1,559 duplicate articles were removed. Two separate reviewers screened the abstracts of the remaining articles to ensure the content met the inclusion criteria. After the abstracts were reviewed, 4,693 articles were excluded as they did not meet the inclusion criteria, resulting in a full-text review of 202 articles with 161 included articles and 41 conflicts (intercoder reliability was 98.79%). After the full-text review, 168 articles were removed for not meeting the full inclusion criteria (see Figure 1 for additional details). Given that the review is focused on EMA with Latines, articles that includes less than 50% Latine/Hispanics were excluded due to low inclusion rates of Latines. The conflicts were resolved by a third reviewer, resulting in 35 included articles. Eight articles were then removed to avoid counting participants twice as the data did not come from a distinct dataset. A total of 26 articles were reviewed.
Data Extraction
All studies that met the inclusion criteria underwent data extraction and a risk of bias quality assessment. Relevant information was extracted from the studies, including participant characteristics, health behaviors addressed, EMA-specific information (i.e., prompt design, adaptations, and challenges), and compliance rates (see Table 1).
Health Behaviors Addressed, Participant Demographics, EMA Information (Prompt Design, Compliance Rates), Study Risk of Bias Score.
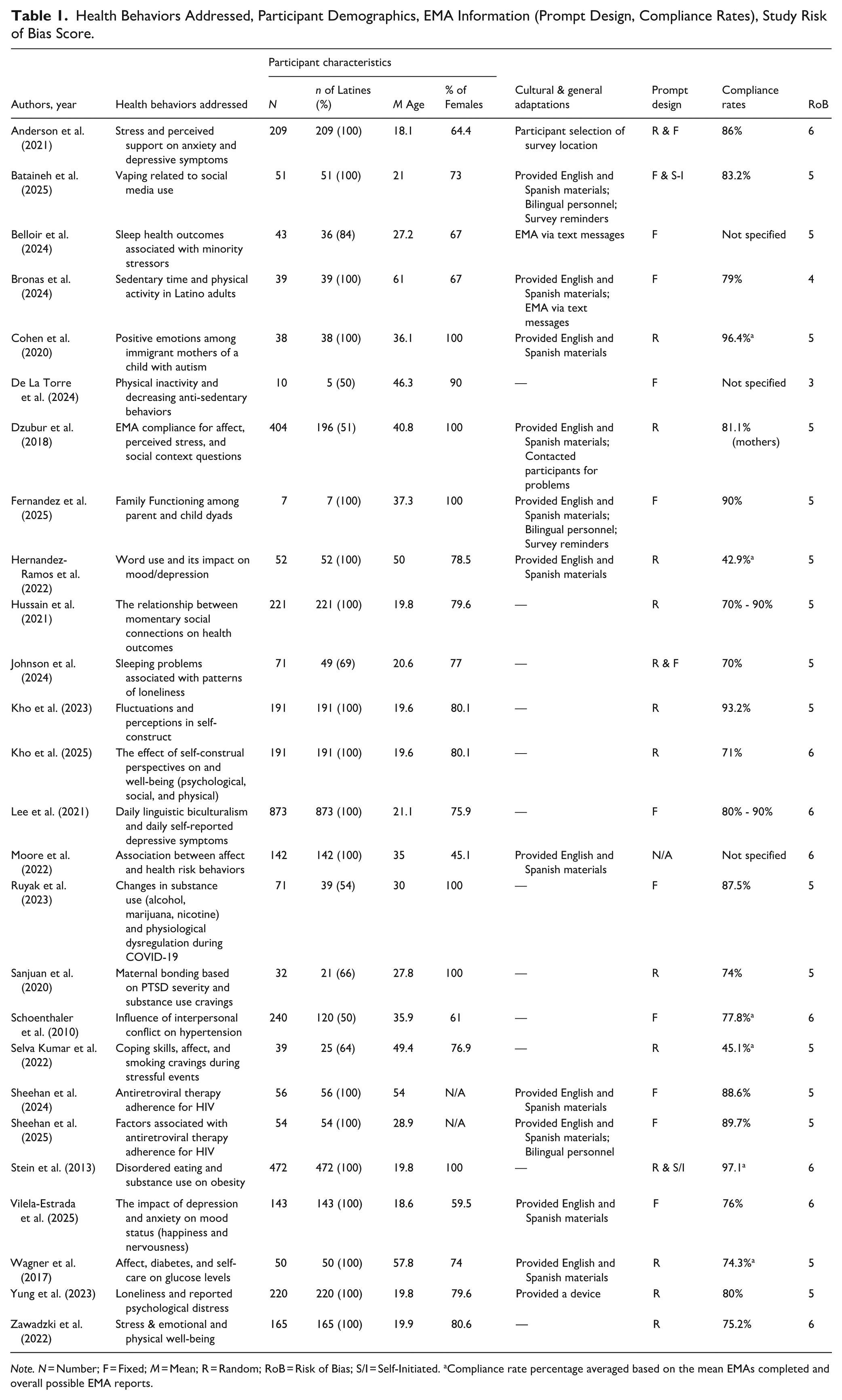
Note. N = Number; F = Fixed; M = Mean; R = Random; RoB = Risk of Bias; S/I = Self-Initiated. aCompliance rate percentage averaged based on the mean EMAs completed and overall possible EMA reports.
Quality Assessment and Risk of Bias (RoB)
To assess for possible biases, a quality assessment for non-intervention studies was used to determine if the articles were methodologically sound (Shepherd et al., 2006). The six criteria focused on the theoretical framework of the study, clearly stated aims and methodology, the interpretation of results, and a description of the sample (Gonçalves & Matos, 2016). All the studies were rated by two independent coders (intercoder reliability 95.16%). One point was awarded for each criterion met (range from 0 to 6) with higher scores indicating a lower risk of bias. All 26 articles obtained a score greater than or equal to 3 (M = 5.19; see Table 1).
Results
Sample Characteristics
As seen in Table 1, the sample sizes from the 26 studies ranged from 7 to 873 participants (M = 157.08) and majority of the studies (n = 18, 69.23%) had an entire Latine sample. From the overall combined number of participants (n = 4,084), 89.74% (n = 3,665) of the participants identified as Latine/Hispanic. All the studies were conducted within the U.S., except for one study (Vilela-Estrada et al., 2025) that was conducted in South America.
A few studies (n = 11) reported the number of Spanish-speaking participants within their sample. Six articles included a full Spanish-speaking sample (Bronas et al., 2024; Cohen et al., 2020; Fernandez et al., 2025; Hernandez-Ramos et al., 2022; Moore et al., 2022; Vilela-Estrada et al., 2025), followed by 96% (Lee et al., 2021), 86% (Sheehan et al., 2024), 82% (Wagner et al., 2017), and 63.7% (Kho et al., 2023; Kho et al., 2025). Of note, these numbers may not be fully representative of the true number of Spanish-speaking Latine participants in the studies given that language ability was not assessed. The studies asked about native language or language spoken at home while others only reported the number of participants who completed the assessments in Spanish. Therefore, it is probable that these numbers may be significantly higher within the articles because individuals may have had the ability to speak Spanish but were not directly asked.
Aim #1: Health Behaviors and Disparities Addressed Using EMA Among Latines
The health behaviors addressed fell within four categories: psychological well-being and emotional health (n = 11), social relationships and interpersonal dynamics (n = 6), physical health and chronic illness management (n = 5), and substance-use related behaviors (n = 4).
Psychological and Emotional Well-Being
Key findings from the articles found that psychological and emotional states impacted each other. Higher positive affect is related to higher physical activity, intake of fruits and vegetables, and time spent with family (Cohen et al., 2020; Moore et al., 2022) and the use of positive words (Hernandez-Ramos et al., 2022). In contrary, negative mood and events increase smoking, drinking, cultural stress, depressive symptoms (Anderson et al., 2021; Lee et al., 2021; Moore et al., 2022; Selva Kumar et al., 2022), with greater emotional variability observed in young Latino men than women (Vilela-Estrada et al., 2025). Subjective loneliness and stress are linked with higher psychological distress, sadness, anxiety, and poorer sleep quality (Belloir et al., 2024; Johnson et al., 2024; Yung et al., 2023; Zawadzki et al., 2022). Family support appears to buffer the impact of negative emotionality (Anderson et al., 2021).
Social Relationships and Interpersonal Dynamics
Social relationships and interpersonal dynamics contribute to current health disparities observed among Latines. Higher quality social connections improve health and sleep (Hussain et al., 2021) while harassment and unjust treatment can lead to higher rates of hypertension (Schoenthaler et al., 2010). Similarly, having better self-construal and self-image improves social interactions, decreases rumination, and enhances physical well-being (Kho et al., 2023; Kho et al., 2025). Additionally, studies that implemented EMA to assess family dynamics noted that Latine families often report high family functioning with better EMA compliance among mother-child dyads when the mother was present (Dzubur et al., 2018; Fernandez et al., 2025).
Physical Health and Chronic Illness Management
Furthermore, EMA was also implemented to understand physical health and chronic illness management among Latines. EMA was used to decrease sedentary time while increasing physical activity among Latine adults. Two separate interventions combined with EMA prompting were delivered and increases in daily physical activity were observed among those with higher motivation to change (Bronas et al., 2024; De La Torre et al., 2024). Another study assessing glucose levels associated with negative affect noted that higher negative affectivity increased glucose levels (Wagner et al., 2017).
Substance Use Related Behaviors
Lastly, substance use was further analyzed using EMA questionnaires. These EMA studies found various factors that increase the risk of engaging in substance use behaviors. Social media exposure exacerbates vaping (Bataineh et al., 2025) while COVID-19 related stressors were associated with the use of alcohol, cannabis, and nicotine (Ruyak et al., 2023). PTSD appeared to lower prenatal bonding and increase substance use cravings (Sanjuan et al., 2020). Lastly, disordered eating (e.g., purging, binge eating, fasting) among Latines escalates tobacco use (Stein et al., 2013).
Aim #2: Common EMA Designs, Adaptations, and Challenges
Common Designs
Table 1 demonstrates the common designs, adaptations and challenges noted with Latines. The three common EMA prompt designs (i.e., fixed, random, self-initiated) appear to be a feasible approach with Latines. Fixed prompts deliver questionnaires at a set time and day; random prompts are randomly delivered during a pre-selected time frame (e.g., any time between 8 am and 10 am); and self-initiated prompts are completed at any time and day (Shiffman et al., 2008). Among the studies in this review, prompting styles are as follows: random (n = 11), fixed (n = 10), random and fixed combined (n = 2), fixed and self-initiated combined (n = 1), and random and self-initiated combined (n = 1). Moore et al. (2022) did not specify the type of EMA design used. Twelve articles had compliance rates that were equal to or above 80%; only two articles had completion rates below 50%, demonstrating high feasibility with the EMA prompt designs used.
Adaptations and Challenges
The primary EMA adaptation directly implemented for Latines was language based. Eleven articles (42.31%) provided the study materials in English and/or Spanish (Bataineh et al., 2025; Bronas et al., 2024; Cohen et al., 2020; Dzubur et al., 2018; Fernandez et al., 2025; Hernandez-Ramos et al., 2022; Moore et al., 2022; Sheehan et al., 2024; Sheehan et al., 2025; Vilela-Estrada et al., 2025; Wagner et al., 2017). Three articles trained bilingual study personnel to conduct the EMA trainings, translate materials, capture “Spanglish” terminology, and provide technical support (Bataineh et al., 2025; Fernandez et al., 2025; Sheehan et al., 2025). General EMA adaptations included distributing the survey at home or university lab based on the participant’s preference (Anderson et al., 2021), sending reminders to complete the EMA surveys (Bataineh et al., 2025; Fernandez et al., 2025), sending EMA surveys via text messages (Belloir et al., 2024; Bronas et al., 2024), contacting participants to assess technical issues or noncompliance (Dzubur et al., 2018), and providing a device (i.e., a smartphone, tablet, iPod) if participants lacked a personal device (Yung et al., 2023).
Challenges with EMA for Latines were infrequently discussed across the articles. Some participants perceived the EMA surveys as burdensome. Fernandez et al. (2025) prompted participants daily for 7 days while Sheehan et al. (2024) prompted participants daily for 28 days. Interestingly, over half of the participants in the former study rated the daily EMA surveys as a “somewhat high or high” burden while only approximately 11% of the participants in the latter study reported feeling burdened by EMA. An additional challenge was recruitment; Bataineh et al., 2025 experienced difficulties recruiting a fully Mexican American sample and hypothesized that cultural hesitancy of participating in a study assessing substance use may have impacted recruitment. Technical issues with EMA were also reported, consisting of system failure to send notifications, unstable internet connection; issues installing the application, and battery-related issues (Bataineh et al., 2025; Fernandez et al., 2025; Vilela-Estrada et al., 2025).
Discussion
The current systematic review aimed to understand research conducted on Latines that use ecological momentary assessment (EMA). Many Latines are negatively impacted by health disparities, which persist due to internal and external barriers (Falgas et al., 2017). These barriers hinder access to health services, especially for hard-to-reach Latines, demonstrating a need to further study Latine’s daily experiences. Information about daily experiences related to health phenomenon would provide real-time information to inform the cultural adaptation of interventions. This review explored research conducted on the health behaviors and disparities that affect Latines in addition to designs, adaptations, and challenges in utilizing EMA with this population. Recommendations on the use of EMA with Latines are provided below to further guide researchers in designing and conducting higher quality research.
Health Behaviors and Disparities Addressed Using EMA Among Latines
Studies in this review researched a variety of health disparities among Latine adults. Most investigated psychological well-being, social relationships, physical health, and substance-use. Latines are adequately represented in these EMA studies, however, daily experiences associated with health disparities require further investigation. EMA represents a mechanism for obtaining rich data to better understand the health inequities that impact Latines and improve health-related interventions.
The majority of the articles focused on the first stage of culturally adapting treatments—information gathering. Although foundational information about health disparities was collected, EMA was not used in the stages that follow the preliminary stage (i.e., preliminary design, testing, refinement, and final trial), with the exception of two studies. These studies implemented a 6-week Spanish-based ecological momentary intervention (Bronas et al., 2024) and a year-long digital behavior change intervention (De La Torre et al., 2024) both focused on increasing physical activity among minoritized adults. EMA provided an understanding of the contextual conditions (i.e., being busy), psychological states, and type of messages (e.g., motivational) associated with higher physical activity. Building from these studies, the development of ecological momentary interventions to address health disparities appears beneficial as it can directly target the mechanisms maintaining the health disparities while simultaneously providing information about daily experiences to aid the development of future interventions.
Furthermore, EMA can aid the collection of daily experiences in each of the stages needed to adapt treatments by providing real-time data about behavioral changes, mood fluctuations, maladaptive behaviors, and perceived difficulties associated with a culturally adapted treatment. Assessing for challenges is critical given that novel or culturally modified interventions may be unsuccessful if common pitfalls are not understood or addressed. Much research on Latines remains warranted to lessen the current research gap, increase our understanding of health disparities, and adapt treatments based on the needs of Latines.
Common EMA Designs, Adaptations, and Challenges
Researchers lacked EMA design adaptations specifically targeting Latines, with the exception of Spanish materials. All prompting styles appear feasible for collecting information. While this is promising, researchers failed to conduct and report analyses that examined whether Latines manifested different patterns of responding than other ethnic groups or Latine subgroups—thereby it remains unknow whether there is heterogeneity in EMA responses among Latines. This is crucial given that EMA provides rich information about daily behaviors.
Cultural adaptations (with one exception) were also not discussed. The only EMA adaptation provided was language based and implemented to increase inclusivity for Spanish-speakers. Documents were provided in Spanish in a few studies; however, no additional adaptations were reported. This combined with the overall absence of how EMA functions with Latines relative to other populations makes the appropriateness, feasibility, and effectiveness of EMA with Latines limited. The generalizability of the current research findings may only be applicable to people with similar characteristics as those in the studies. The Latine community is highly diverse, however, many sub-populations are currently underrepresented in the literature as they may be considered hard-to-reach populations. Broadly, researchers documented general adaptations (e.g., providing devices, time adjustments, study hotlines), however, these adaptations were not modified for Latines specifically.
Only a few specific challenges were reported in delivering EMA to Latines. This suggests that either Latines does not have difficulties with EMA or a lack of knowledge about the needs of this population; however, because many researchers failed to provide any detailed discussion, we cannot assume either nor describe specific participant characteristics linked to challenges with EMA. It was hypothesized that cultural values may influence the research studies Latines participate in (Bataineh et al., 2025), however, this was not tested within the study. Broadly, further research is needed among this community to understand their needs and potential challenges that arise when conducting EMA research.
Guidelines and Recommendations for Using EMA With Latines
Using the findings from the literature as well as our knowledge of EMA and the Latine population the following guidelines were developed. These guidelines have been adapted to address the common internal and external treatment barriers Latines experience. An additional focus of the guidelines is applying the recommendations to culturally adapt health interventions to better serve the needs of the Latine community. The recommendations are as follow.
Cultural/Linguistic Adaptations
Translate and Provide Research Materials in Spanish
Only 11 articles (42.31%) provided access to Spanish study materials based on language preference, showing a lack of research studies making linguistic adaptations for participants. A lack of Spanish-speaking personnel often impedes research studies conducted with Spanish speakers (Benuto & Leany, 2017), which limits our knowledge of the hard-to-reach individuals in this community and generalizability of current health interventions. EMA is a potential solution to this issue as once materials are translated, EMA prompts can distribute the materials to gather daily initial information about health disparities and make between-group comparisons based on language spoken. In fact, Fernandez et al. (2025) provide this recommendation and noted that back translating documents, preparing training materials, and delivering one-on-one training sessions in Spanish reached a more diverse subset of Latines. English speaking researchers who use these methods would benefit collaborating with Spanish-speaking researchers and using Likert-scale responses to reduce the need for a translator once responses are collected from participants. Additionally, developing Spanish materials such as short instructional/informational videos, step-by-step guides, or photographs can reduce dropout and enhance EMA engagement.
EMA can also be used as a tool to deliver psychoeducation about health behaviors, especially to individuals with limited access to behavioral health resources or low knowledge about health-related topics. When possible, researchers are encouraged to include brief psychoeducational messages (e.g., coping strategies, behavioral explanations, health information or tips) within the EMA prompts to enhance knowledge of health disparities and aid engagement with future prompts. EMA prompts can simultaneously deliver and collect information to further adapt interventions for Spanish-speakers and reduce the treatment barriers perpetuating health disparities. This approach would also allow health interventions and information to be easily delivered to hard-to-reach individuals, such as those lacking health care coverage or financial stability.
Use EMA Platforms That Support Multilingual Delivery
While various EMA applications exist, using EMA platforms that have multilingual support built-in would enhance the research experience for Spanish-speaking Latines. Numerous EMA applications are available that support multiple languages, including Spanish (e.g., NeuroUX, RealLife EXP, REDCap, mEMA). These applications offer notification- and user-initiated sessions, reminders (via the app or text messaging), and insertion of visual media (e.g., pictures, videos, audio diaries). The use of visual media combined with instructional information or Spanish voice and audio prompts can simplify EMA research for participants with lower literacy. Of note, REDCap offers EMA prompts via text messages, which may increase adherence to surveys due to increased accessibility.
Pilot testing studies is crucial to determine potential challenges participants may encounter. One potential challenge to consider may be that while the survey is in Spanish, in-app features (e.g., settings, toolbars, menus, notifications) may remain in English, creating challenges for individuals with limited English proficiency. These challenges can be navigated by training the participants to utilize the application (via in-person, virtually, or through visual aids) and limiting the number of screens in the application that participants must open or scroll through to open the survey.
Train Bilingual Personnel and Provide Study Hotlines
While some studies in this review provided bilingual personnel to aid with the research project, access to study hotlines were lacking. It is recommended that bilingual personnel offer one-on-one onboarding trainings to participants via in-person, phone, or video to explain the EMA protocol, train on using the application, and explain the study hotline process. Providing study hotlines have been effective in addressing technological issues participants experience throughout the study (Dunton et al., 2012). Providing study hotlines in combination with bilingual personnel can allow participants to contact research personnel when needed. Training bilingual study personnel offer numerous benefits, including the translation of materials, providing information in lay language, helping with technological issues, conducting trainings, and capturing terminology used within Latine subgroups.
Through study hotlines with bilingual personnel, participants’ concerns can be addressed quickly and effectively. Benefits of this include participant retention, comfortability, continuity, and safety as there is a direct method of communication with research personnel. This can broadly improve participants rapport and trust in the researchers, increasing a participant’s comfort levels and likelihood of participating in future research studies. This may also enhance recruitment through word of mouth as individuals may recommend the studies to individuals close to them.
Utilize Culturally Appropriate Terminology
The Latine population consists of a variety of sub-ethnicities with heterogeneity between subgroups and preferred terminology. Cultural awareness is important in diversity research and including bilingual research personnel allows researchers to capture “Spanglish” terminology (Bataineh et al., 2025). In fact, cultural differences have been seen in response styles between ethnic subgroups (Burlew et al., 2019). This allows a deeper understanding of cultural context associated with health disparities. Conducting focus groups on appropriate terminology or preferred language among Latines is a culturally competent research approach. To promote inclusivity, this review selected the term Latine, rather than Latino or Latinx, because it encourages greater gender inclusion and has greater fluency in the Spanish language (Miranda et al., 2023).
Using biased or stereotypical language can damage the researcher’s relationship with the community and further reduce Latines involvement in research studies. For example, the term Latinx emerged as a gender inclusive term for people from Latin American, however, this term is not widely used among Latines and is often rejected (Salinas, 2020). These communities may prefer the use of specific language depending on the geographical origin of their family, demonstrating the importance of proper language. Piloting EMA studies will improve the comprehension, readability, and tone, while limiting culturally mismatched or inappropriate terminology.
Utilizing appropriate terminology can have numerous benefits among EMA research studies. First, using preferred terms by sub-ethnic Latine groups can result in more accurate data and higher engagement as participants will feel more of an association with the terms. Due to repeated assessments provided by each participant, EMA will provide more accurate data in real-time, reducing the need for higher sample sizes without comprising the quality of data collected. In this way, EMA allows for the comparison and understanding of Latine sub-groups. Additionally, this can prove useful in culturally adapting treatments based on Latine groups to improve health outcomes and reduce health disparities.
Methodological Adaptations for Latines
Technological Accessibility for Latines
EMA allows for research with Latines to be conducted with limited in-person contact, however, technological adaptations are often needed. Although approximately 98% of Latines own a smartphone (Nielsen Company, 2020), many Latines have lower educational attainment (Connelly et al., 2016; Falgas et al., 2017), potentially resulting in challenges using technology. Despite the need for online resources, there are virtually no behavioral health apps that provide resources in Spanish (Muñoz et al., 2021). Thus, while EMA can bridge this gap, participant capabilities and deficits with technology must be anticipated. In fact, an EMA mobile app for Latines with low literacy of unhealthy weight loss methods adapted the language to be suited for individuals with lower educational backgrounds and found improvements in knowledge (Connelly et al., 2016). This EMA application demonstrates how addressing external barriers can result in successful dissemination of interventions with Latines.
Due to Latines technological challenges, EMA adaptations to reduce these barriers should be anticipated. Such adaptations include offer online training sessions (Bronas et al., 2024), use familiar platforms (e.g., text messages, WhatsApp, Facebook Messenger) to distribute EMA surveys (Belloir et al., 2024), incorporate frequent check-ins to troubleshoot ongoing technological problems (Dzubur et al., 2018), provide interactive in-person trainings, offer physical and/or digital instruction manuals, simplify instructions based on education level, use visual aids (e.g., images, instructional videos), and allow access to the resources anytime. These strategies can allow researchers to reach many individuals in the Latine community who are experiencing numerous treatment barriers (e.g., financial instability, lack of transportation, scheduling difficulties due to lack of time, etc.) that hinder them from obtaining health services. For example, EMA can reach Latines who live in remote locations and obtain information about daily experiences without having participants leave their home to participate in the study.
Utilize Participants Personally Owned Devices
Another method to reduce participant burden involves using the participants personal device to download the EMA application. Loaning personal devices to participants can be beneficial, however, the type of device should be considered. For example, providing a tablet increases participant burden due to the size of the device when compared to a smartphone. Due to the complexity and duration of EMA questionnaires, utilizing personal devices can decrease burden, increase engagement and participation, and provide richer data sets that demonstrate daily behavioral patterns and changes. Latines have high rates of smartphone ownership (Nielsen Company, 2020), resulting in one less barrier to conducting EMA research with Latines. This strategy can also be especially useful for rural participants where it may be difficult to provide or deliver a device to be used for research purposes. In combination, participants can be allowed to select the prompting method (i.e., app-based vs text messaged based), to enhance compliance.
Reduce EMA Burden to Enhance Compliance
Latines in the reviewed articles reported EMA burden resulting in lower completion rates. EMA burden was presumed to be linked to the questionnaires becoming repetitive, longer study length, time-consuming, busy schedules, balancing obligations, caregiving responsibilities, study fatigue, and low-socioeconomic status (Dzubur et al., 2018; Fernandez et al., 2025; Sheehan et al., 2024). Response styles may also be important to assess given that cultural differences have been found in response styles (Burlew et al., 2019). When targeting understudied sections of the Latine population (e.g., rural communities, Spanish speakers, immigrants, etc.) minimizing EMA burden based on individual challenges observed within the participant can enhance compliance and research outcomes. Although this step appears uncomplicated, it requires understanding and maneuvering of the complexities hindering each individual participant from beginning or continuing research studies.
EMA can be particularly helpful because it is easily adaptable and customizable, thus, allowing for adaptations to meet the needs of each subgroup. EMA information collected, via pilot studies or community-based participatory research, can be adapted to fit specific characteristics, such as literacy levels or dialect, reducing participant experienced burden with EMA. It is recommended to conduct focus groups with Latines prior to EMA research to collect information about the community’s preferences, including preferred prompting, length of study, compensation rates, and length and/or diversity of surveys. Additional strategies to reduce EMA burden include having multiple sets of questionnaires prompted to reduce repetitiveness. Surveys with shorter completion times (<10 min) were frequently used and favored by participants (Bataineh et al., 2025; Selva Kumar et al., 2022; Sheehan et al., 2024), therefore, following this design can address burden experienced from EMA prompts among Latines. Additionally, Muñoz et al. (2021) recommended culturally adapting technological interventions and tools to meet the needs of Latine’s with specific characteristics due to large amounts of diversity in nationality, locality, dialect, literacy level, socioeconomic status, and stigma, which can be done with EMA. Additionally, participants should be provided with real-time feedback or psychoeducation about their behaviors based on their EMA responses to enact positive behavioral health changes and aid further compliance.
Allow Participants to Select Their Own Time Intervals to Receive EMA Prompts
Approximately 51% of Latine parents work nonstandard hours (i.e., hours beyond 8 a.m. and 6 p.m.) with higher rates among immigrant parents (Mendez et al., 2020). Dzubur et al. (2018) reported more missed EMA prompts before 5PM. Therefore, time-based adaptations for EMA should be allowed whereby individuals select their preferred time intervals to receive EMA prompts. This approach recognizes time constraints Latines often experience, providing validation for their experiences. If numerous daily prompts appear burdensome, researchers can provide fewer but more meaningful prompts during the preferred time slots to collect higher quality data.
Of importance, EMA response rates during the weekday should be compared to completion rates during the weekend to further establish more appropriate EMA prompting with Latines. This can increase compliance rates because there will be more flexibility in the prompting times based on the availability of the individual while providing a more comprehensive data set. This adaptation will also address external barriers, reduce EMA burden, and alleviate the pressure of having to respond to all of the prompts to receive compensation. Broadly, this will allow participants to select their own time slots, thus, increasing autonomy and willingness to participate in research studies, especially when tailored to their work schedules. By enhancing participation rates, data collected will be richer, more comprehensive, and of higher quality.
Community Engagement/Ethics
Bataineh et al. (2025) reported difficulties recruiting an entirely Mexican American sample due to cultural perceptions of substance use, resulting in expansions to the eligibility criteria. To reduce challenges in recruiting Latine populations and obtain diverse samples, developing community partnerships and building trusting relationships are essential. EMA studies are often conducted among college students due to convenience sampling; however, this excludes a large portion of the community. Latines report a lack of trust in researchers and health experts (Benuto et al., 2019; Hildebrand et al., 2018), potentially explaining their hesitancy to participate in research studies and recruitment challenges. Developing personal relationships helps researchers gain trust among the Latine community (Hildebrand et al., 2018), which creates a more welcoming, pleasant, and favorable research environment.
Develop Community Partnerships
Community members often report feeling unheard by organizations and researchers (Hildebrand et al., 2018), however, EMA can bridge this gap. Daily EMA questionnaires can be used as an outlet for community members to express daily ongoing health difficulties, concerns, or thoughts. Thus, providing researchers with daily information about contributors to health disparities while validating the individuals’ experiences. Additionally, these can be completed remotely, broadening engagement of hard-to-reach Latines.
Through recurring encounters at locations infrequently, such as community events, churches, Latine serving organizations, healthcare settings, investigators can become well integrated into the community and provide research opportunities for Latines that serve to reduce health disparities. While the primary focus should be implementing solutions to the issues raised, the dissemination of published health-related research and psychoeducation can aid in the development of community partnerships. For example, researchers can provide a psychoeducation health seminar once a monthly or every other month to develop and maintain trusting community relationships. Partnering with promotores de salud (community liaisons) can be a first step in connecting with harder to reach Latine community members. Taking such an approach can increase the community’s willingness to participate in future studies and develop trust in researchers as well.
Transparent Communication
Given the lack of trust in researchers, having transparent communication with individuals is needed. Researchers should explicitly address concerns Latines may have relating to immigration, insurance, misuse of information, privacy, or data sharing. Although this is completed during informed consent, Latines may hold higher confidence in the researchers if this information were covered in safe spaces where they frequently congregate, such as during church masses. If no insurance is required, making this clear is important as some individuals may qualify for the research study but may fear participating due to potential costs.
Overall, there are many approaches researchers can take to be culturally sensitive to Latines and implement EMA to improve health disparities. These approaches should be thoroughly considered to engage in better research practices and obtain diverse community samples in real-time. Researchers should also shift away from studying primarily English speaking, college student Latines given that they represent a small portion of the community. The guidelines suggested above are provided to ease the research process and help one integrate themselves into the community as a trusted, well-respected, and culturally sensitive community researcher.
Future Directions
Given the current research gaps in this field, several areas for future investigations have been identified. First, EMA studies should be conducted predominantly with Latine samples, preferably community-based or Spanish-speaking samples, to improve generalizability to the general population. Mitigating health equity tourism (HET), which occurs when academic researchers with limited experience conduct investigations potentially rooted in biases (Lett et al., 2022), in this process is crucial. HET can be mitigated by ensuring that researchers do not cause harm to Latines; increase one’s own awareness of privileges that may result in biases, such as gender-based privileges; engage in equal and/or equitable collaborations with researchers in the field; and resist the urge to engage in research due to taking quick action as this can result in an oversight of important health disparities and outcomes (Lett et al., 2022). Lastly, adapt EMA to better suit the needs of Latines and research challenges as this can produce higher quality and culturally competent research with Latines and reduce the impact of health disparities.
Limitations
The current review assessed studies only using adult populations, therefore, limiting the recommendations to this population. Multiple articles used the same parent data set, however, did not specify the portion of the data utilized. To reduce counting participants twice, the sample with the largest number of participants was selected, which means certain participants may have been excluded to reduce overreporting the true number of participants.
Conclusions
Although research has targeted health disparities among Latines and EMA has been a useful tool in understanding daily experiences, additional research is still needed. Various health disparities have been targeted in the current literature; however, few studies with predominantly Latine samples are scarce and there continues to be a lack of EMA adaptations for Latines, potentially explaining the small Latine sample sizes in many EMA studies. Further understanding potential challenges with EMA that Latines may experience can be useful in mitigating challenges in future studies. Lastly, recommendations are provided that can be used as a guide on conducting Latine EMA research studies and potentially improving engagement, adherence, and acceptability among this community. In all, there are many current research gaps that need to be addressed to develop a better understanding of Latines daily lives and the impact that health disparities have on their day-to-day experiences.
Footnotes
Consent to Participate
There are no human participants in this article and informed consent is not required.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Stephanie R. Reyes with support provided by Lorriane T. Benuto. The first draft of the manuscript was written by Stephanie R. Reyes and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data and materials can be provided upon request.