
Abstract
This observational study used descriptive analysis to improve understanding of the relationship between fathers’ presence or absence, the occurrence of mothers’ feeding practices, and child eating behaviors at evening meals. Participants were 141 Mexican-origin families with children aged 8 to 10 years. We coded behavioral observations of video-recorded meals. Three parental feeding practices were established a priori: (1) pressure to eat, (2) restriction of amount of food, and (3) positive involvement in child’s meals. Additionally, we identified child eating behaviors and food eaten. Fewer mothers engaged in certain types of positive involvement in child’s meals when fathers were present at the meals, compared to when fathers were absent. Regarding child eating behaviors, when fathers were present, more children engaged in positive talk about food, compared to when fathers were absent. Additionally, when fathers were present, more children ate grains and fewer ate fruit, compared to when fathers were absent. Family mealtime with Mexican American children may provide an opportunity for fathers, alongside mothers, to communicate about and participate in children’s food consumption. Research on obesity in families should include a focus on fathers’ feeding practices, such as positive involvement in a child’s meals, that may complement mothers’ feeding practices.
Introduction
Within the next decade, rates of overweight and obesity in the U.S. are projected to reach approximately 33% for children and 50% for adolescents (Wang et al., 2020). Latinos are the largest growing segment of the U.S. youth. The prevalence of overweight and obesity among Latine youths has remained high for the past couple of decades (Ogden et al., 2020; Skinner et al., 2018). As a subgroup of the Latine population, Mexican American children experience persistently higher rates of obesity when compared to non-Latine groups (Fryar et al., 2021). For example, in 2015 to 2018, 28% of Mexican American children ages 6 to 11 years were classified as having obesity, as defined by a body mass index (BMI) greater than or equal to the 95th percentile, compared to 23% of non-Latine Black, 16% non-Latine White, and 9% of non-Latine Asian children of similar ages (Fryar et al., 2021; Ogden et al., 2020). In the short term, children with obesity are at higher risk for health problems such as hypertension, type 2 diabetes, sleep disordered breathing, asthma, fatty liver disease, orthopedic problems, and abnormalities in menstruation (CDC, 2024; Jebeile et al., 2022).
The development of obesity in children is due to multiple socioecological factors, including genetic, environmental, and family-level behavioral risk factors (CDC, 2024; Hochgraf & Ruggiero, 2021). For example, structural and environmental factors, such as the cost of healthful food, junk food advertising, the abundance of fast food and lack of places to exercise, influence obesity-related health disparities, especially among disadvantaged populations (Jebeile et al., 2022). Among family-level behavioral risk factors, extensive research with mother-child dyads has focused on parental feeding practices (PFP; Eichler et al., 2019; Russell et al., 2018). PFP reflect the context in which families are embedded (Davison & Birch, 2001; Mena et al., 2015), and involve choices about the type of food children are offered, and when, how frequently, and how much children are fed, as well as verbal interactions about the child’s eating behavior (Birch & Ventura, 2009; Loth et al., 2013a, 2013b). Research findings focused on PFP suggest that prevention and treatment programs should incorporate guidance on PFP that foster food preference patterns and selection in children that are more consistent with healthy diets, and promote children’s ability to self-regulate (Birch & Ventura, 2009; Farrow et al., 2015; Larsen et al., 2015; Pfeifflé et al., 2019; Russell & Russell, 2019; Zhou et al., 2020).
The current observational study focused on three PFP: (1) pressure to eat, which consists of pressuring the child to eat everything on his/her plate and pressuring the child to eat more even if not hungry; (2) restriction of amount of food, which consists of limiting the amount of the child’s food and not allowing the child to control snacking; and (3) positive involvement in child’s meals, which consists of monitoring and limiting the child’s unhealthy food, and encouraging the child to eat new and healthy food. PFP that are high in control (i.e., pressure to eat and restriction of food) may impede children’s ability to self-regulate their food intake by shifting their focus to external cues and away from their own hunger and satiety (Birch & Ventura, 2009; P. W. Jansen et al., 2014; Ruzicka et al., 2021). Pressure to eat is associated with lower child weight status and restriction of food is associated with higher child weight status, possibly resulting in the opposite of what parents intend. In the long term, controlling PFP may increase children’s risk for an unhealthy weight status for their age and development (Harris et al., 2014). For example, in a 2-year longitudinal study in Mexican American families, results indicated that mothers’ and fathers’ restriction of food predicted higher subsequent child weight status at Year 1, and for fathers, this effect was also found at Year 2 (Tschann et al., 2015). In addition, mothers’ and fathers’ pressure to eat predicted lower weight status among boys but not girls at Year 1. In general, PFP high in parental control are associated with an unhealthy weight status in Mexican American children (Penilla et al., 2017; Tschann et al., 2015), yet they are modifiable behavioral factors for childhood-related obesity, particularly when compared to other parental risk factors such as genetic or environmental factors that are more challenging to modify (Holland et al., 2014).
In general, research on parental involvement in child rearing suggests that authoritative parenting that includes monitoring, firm control and warmth is associated with important positive developmental outcomes in children (Cruz et al., 2011; Pleck, 2010). Authoritative parents monitor children’s eating behavior and impart clear standards for their children, are assertive but not intrusive or restrictive, and want their children to be assertive, responsible, self-regulated as well as cooperative (Baumrind, 1991; Darling, 1999). In contrast to PFP high in parental control, such as pressure to eat and restriction of amount of food described above, positive involvement in child’s meals is thought to reflect an authoritative style of parenting (Darling & Steinberg, 1993; Rollins et al., 2015; Sanvictores & Mendez, 2024) and involves demandingness and responsiveness to children’s needs (Hughes et al., 2013; Shloim et al., 2015). For example, in one cohort study of Mexican American children aged 8 to 10 years old, both mothers and fathers engaged in positive involvement in their child’s meals (Tschann et al., 2015). In a subsequent observational study of this cohort, depending on the individual child’s needs, parents’ positive involvement in their child’s meal included talking about the food, such as asking their child if they are done eating or if they are full and offering or asking their child if they want food or more food (Penilla et al., 2022). Such parental behaviors are thought to be protective against overweight and obesity, but more research is needed, especially research that engages Mexican American fathers (Hennessy et al., 2010; Musher-Eizenman & Holub, 2007; Walton et al., 2019).
Fathers’ Feeding Practices and Child Eating Behaviors
There is limited information on fathers’ feeding behavior in child rearing. Nevertheless, socialization and family values building has been noted among fathers. In a qualitative study of fathers’ perceptions regarding feeding their children, Harris et al. (2020), reported that fathers’ self-reported connection and communication acted as a conduit between father feeding and child eating. Connection refers to the value fathers assign to mealtimes, while communication refers to how this value is transmitted and can consist of reciprocal verbal or non-verbal cues (Harris et al., 2020). Fathers’ connections with their children at mealtimes were informed by the belief that mealtimes enabled socialization, intergenerational transmission of values of family meals and their previous and present interactions with their children.
Recent qualitative research on the role of Mexican American fathers in the home food environment indicates that fathers collaborate with mothers and engage in PFP to shape their children’s eating (Boykin et al., 2020; Henry et al., 2020; Parada et al., 2016; Turner et al., 2014; Wong et al., 2017). In one study, Zhang et al. (2018) conducted focus groups with 26 Mexican American fathers on food-related practices for their children and reported that fathers were involved in the home food environment by working with mothers on meal planning, grocery shopping and preparing food. During the group discussion, fathers discussed using PFP such as pressure to eat, restriction of food and positive involvement in child’s meals. When discussing positive involvement in their children’s meals, over half of fathers reported that they encouraged their children to eat in a healthy way, such as by talking about the benefits of good nutrition and health properties of food (Zhang et al., 2018). Additionally, about one-third of fathers reported that they monitored the type and quantity of both healthful and less healthful foods consumed by their children. In another observational study examining PFP in 71 Mexican American families, results indicated that fathers engaged in positive involvement in the child’s meal, more often than applying pressure to eat and that fathers rarely engaged in restriction of food (Penilla et al., 2022).
Participating in family meals in childhood is protective against overweight and obesity in young adulthood and mothers have historically played a primary role in preparing food and serving children (Berge et al., 2015; Fiese, 2021). Although fathers may also influence children’s eating behavior through their own behaviors, pediatric obesity interventions have rarely engaged fathers (Davison et al., 2018; Morgan et al., 2017), focus primarily on mother-child dyads and do not consider the strategies used by fathers (Campbell et al., 2022; Davison et al., 2016). Examining fathers’ presence at evening meals and the co-occurrence of child eating behaviors may help inform family-level obesity treatment and prevention research about the ways fathers contribute to children’s meals.
The Current Observational Study
Fathers of Mexican origin report that they engage in family meals and that they promote their families’ as well as their own health and well-being, (Greder et al., 2021) yet there is a lack of qualitative observational research regarding fathers’ presence at family meals and potential connection to mothers’ and children’s mealtime behaviors. One way to approach this question is to qualitatively observe mothers’ and children’s behavior when fathers are present, versus when they are absent (Smit & Onwuegbuzie, 2018). With the goal of informing future family-level research aimed at preventing obesity among Mexican American children, the current study used a video-recorded observational approach to examine mothers’ PFP and children’s eating behaviors at evening meals at home. Observation as a research method allows researchers to shed new light on these behaviors, by using observed family interactions in a natural setting (i.e., meals at home) to produce insights that might otherwise not emerge in individual interviews or surveys (Pesch & Lumeng, 2017). Unlike surveys, interviews, and focus groups, where respondents report on their behaviors, video-recordings of family interactions in this study provide another window (through looking and listening) into understanding cultural norms and behaviors that family members might not be explicitly aware of or not asked about (Bergmeier, Skouteris, & Hetherington, 2015; Bergmeier, Skouteris, Haycraft, et al., 2015; Carter & Little, 2007). This observational study focused on family mealtime in the context of eating and obesity among Mexican American children, while considering PFP as a potential modifiable risk factor during children’s mealtimes. To enhance our understanding of fathers’ role in Mexican American children’s meals, we compared mothers’ PFP, child eating behaviors, and food eaten by the child at meals in which fathers were present or absent.
Methods
Study Sample
The current study used behavioral observations of children’s video-recorded evening meals at home. Family participants were from a larger cohort study of 322 Mexican American families living in the San Francisco Bay Area (Tschann et al., 2013; Tschann et al., 2015). Of the 322 families in the larger study, 46% (n = 147) of families agreed to have their child’s meal at home recorded. Of these, one child refused to be video-recorded and five mothers were not available during the meal; as a result, we analyzed 141 videos (84% two-parent families; 16% single-parent families) for this study. Participants in the larger study were recruited from an integrated healthcare delivery organization. Parents were mailed letters introducing the research and telephoned, screened for eligibility, and enrolled in the study. Families were eligible if the mother was of Mexican descent (born in the US or Mexico), the child was 8 to 10 years of age and had no illnesses that might influence their weight. If more than one child was aged 8 to 10 years, only one child per family participated in this research to avoid dependency in observations. Fathers who were the co-parenting figure in the children’s lives were invited to participate, including those living in separate houses (e.g., separated or divorced). During the first in-person meeting with the families, research assistants (RA) obtained written informed parental consent for themselves and their child in the language of participants’ choice (Spanish or English) and obtained verbal assent from child participants. Families agreeing to participate in this observational study signed an additional consent form to be video-recorded. At-home video-recordings lasted approximately 45 min. After the video-recording was completed, each participating study member was reimbursed $20 for their time. This study was approved by the university and the healthcare delivery organization’s institutional review boards.
Family Meal Video-Recording Procedures
In preparation for the home visit, an RA explained the video-recording protocol to parents over the phone. Based on previous research on family meals, one recording was required per family with participant child (Rhee et al., 2015; Stark et al., 2000), but two evening meal dates were scheduled within the same week in case of problems with the first date. Parents were informed that a RA would call 24 hr before the first selected date. It was emphasized that no special preparation was needed, that the food served should be typical, and that whoever would normally be present at the evening meal that day could be present.
A trained RA video-recorded the evening meal using a Sony HDR-CX12 digital video camera recorder, which was set up on a tripod facing the table and across from the participant child. Cameras were placed approximately six feet away from the table and captured family members attending the evening meal. Family members attending the evening meal, but not wishing to have their faces recorded, were allowed to sit with their backs to the camera. The RA began recording meals when family members began to gather around the table and left the room once the meal began. Recording ended when families decided they were finished with the meal. Overall, video and audio quality were good. To help ensure the validity of each recording at the conclusion of the meal, parents were asked to complete a brief questionnaire about the meal, including: “Was the food for tonight’s meal typical of the food you usually serve?” and “Was your child’s behavior typical of the way he or she usually behaves?” All parents (100%) reported that the food served and the child’s behavior during the evening meal were typical.
Coding Behavioral Observations During Family Meals
Consistent with guidelines for developing behavioral coding and analyzing a structured observational study with descriptive analysis, we used a multi-stage analytic deductive process that included verification techniques to strengthen the reliability of the behavioral observation coding scheme and validity of the findings (Carter & Little, 2007; Miles et al., 2014; Pesch & Lumeng, 2017). Only parents’ and participant child’s behaviors were coded (i.e., not siblings) and coding began when all family members were at the table. The codes for parental feeding practices were established a priori, and three authors viewed the videos using those established concepts from the literature. In the initial stages of the coding process, the three authors viewed videos to identify PFP (e.g., restriction of food), child eating behaviors (e.g., child asks for more food), and type of food child ate (e.g., grains). The three authors decided how best to capture the information (e.g., categorically or as a count). The three authors took notes to describe specific participant behavior in a detailed manner, defining specific parameters of feeding practices, child eating behavior, as well as the type of food. This level of specificity improved the likelihood that the codes would be applied in a reliable manner (Pesch & Lumeng, 2017). During the next stage, the behavioral observation coding scheme was tested and refined by two RAs using the same four randomly selected videos. The two RAs separately applied the coding scheme consecutively to all participant family members in each video of four videos, beginning with the participant child, next the mother, and finally the father, if present. Participant behaviors were counted if they occurred at least once. The RAs then met with the three authors to compare notes and discuss disagreement or points of confusion, which resulted in a refined coding scheme. The two RAs then applied this process to new videos until >90% agreement was reached, which required coding an additional 16 (11%) randomly selected videos for a total of 20 videos. This iterative coding technique led to a finalized behavioral observation coding scheme with 11 PFP codes (i.e., two codes for parental pressure to eat, one code for parental restriction of food, and eight codes for parental positive involvement in the child’s meal), six codes for child eating behaviors, and 13 types of food served.
Participant demographic characteristics were obtained as part of the larger study. Children’s demographic variables included age in years and sex. Parents’ and children’s height and weight were measured in duplicate by trained RAs while the participant was wearing light indoor clothing and no shoes (Lohman et al., 1988). Body mass index (BMI) was calculated [BMI = weight(kg)/height(m)2] for each participant. Child BMI was converted to age- and gender-specific BMI percentiles using CDC growth charts (Kuczmarski et al., 2000). Children were then classified as having a healthy weight, overweight, or obesity (Kuczmarski et al., 2000; Tschann et al., 2013). Parents’ demographic characteristics included age, weight status (BMI), years of education, Spanish and English-language acculturation, and occupational status. Acculturation was assessed using the Spanish and English language use subscales of the Bidimensional Acculturation Scale for Hispanics (BAS; Marín & Gamba, 1996). Items were scored from never (=1) to always (=5) and had good reliabilities (α = .88, mothers; 0.94, fathers). Higher scores on the two language acculturation subscales reflected greater use of those languages. Occupational status ranged from unskilled worker (=1) to major professional (=9; Hollingshead, 1975). A higher number indicates a higher status occupation.
Analysis
Using the finalized coding scheme, two RAs each coded half of the videos. To test for interrater agreement, 20% of coded videos were randomly selected and double-coded. Codes with less than an 80% agreement (indicating low rater agreement) between raters were dropped from subsequent analyses (Pesch & Lumeng, 2017). Because there was low rater agreement for codes assessing the frequency of all PFP, and child eating behaviors, all frequency codes were converted to binary (presence or absence of behavior). Three codes for PFP and two codes for child eating behaviors were also dropped due to low rater agreement. This strategy resulted in good interrater agreement for eight codes for PFP (agreement ranging from 80% to 97%; Table 1), four codes for child eating behaviors (interrater agreement = 80%–90%) and 13 codes for type of food the child was served (interrater agreement = 80%–100%; Table 2).
Observed Percentages of Eight Maternal Feeding Practices by Fathers’ Presence or Absence in an Evening Meal of 141 Mexican American Children Aged 8 to 10 Years.
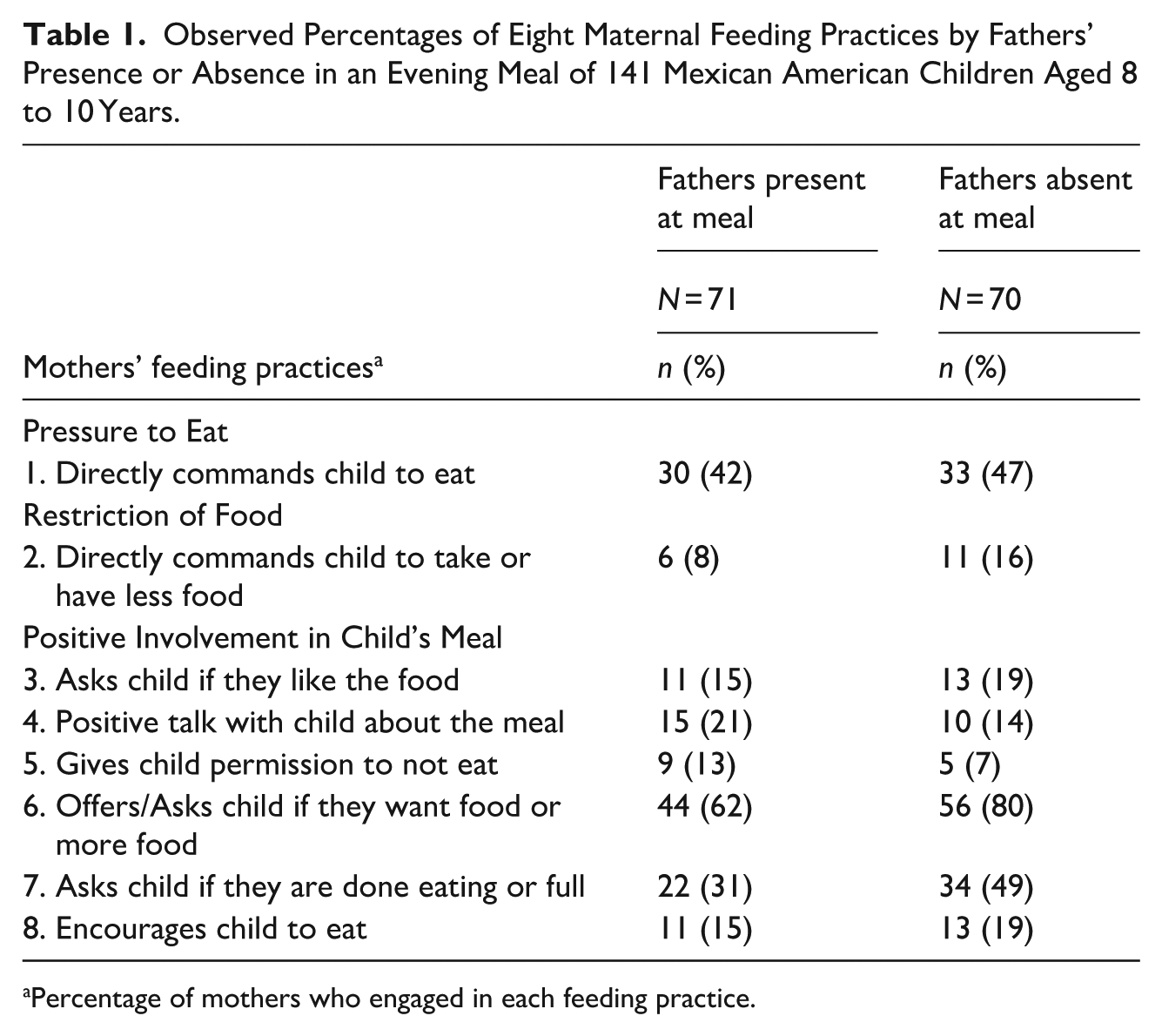
Percentage of mothers who engaged in each feeding practice.
Observed Percentages of Four Child Eating Behaviors and 13 Types of Food the Child Was Served, When Fathers Were Present or Absent in an Evening Meal of 141 Mexican American Children Aged 8 to 10 Years.
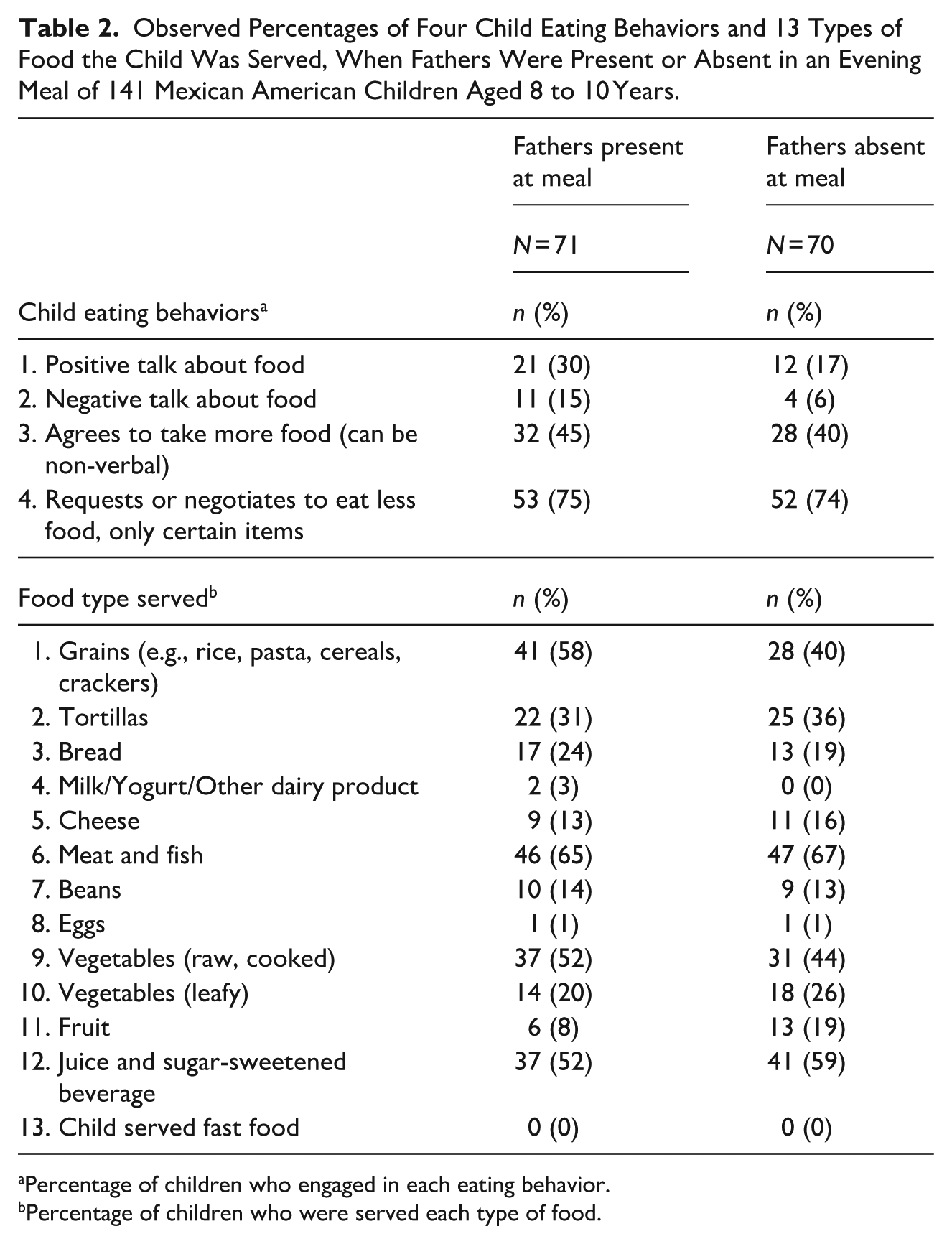
Percentage of children who engaged in each eating behavior.
Percentage of children who were served each type of food.
Descriptive statistics for demographic characteristics, and coded counts of PFP, child eating behaviors, and type of food child ate were computed. We compared percentages of PFP, child eating behaviors, and type of food child ate when fathers were present at the meal versus fathers absent at the meal.
Results
Family characteristics are summarized in Table 3. Mothers (100%) and most fathers (82%) were of Mexican descent. The majority of fathers were the biological parent (93%). Most parents were classified as having overweight (BMI > 25 and < 30; 35% of mothers, 42% of fathers) or obesity (BMI > 30; 43% of mothers, 44% of fathers). On average, mothers completed 11 years of education (M = 11.01, SD = 3.58; range 2–19) and fathers completed 12 years (M = 11.82, SD = 3.05; range 5–18). Most parents were employed (77% of mothers, 90% of fathers). On average, parents’ occupational status was skilled worker (mothers: median = 3, range 1–8; fathers: median = 4, range 1–9). Parents had higher acculturation scores in Spanish (mothers: M = 4.15, SD = 1.15; fathers: M = 3.94, SD = 1.20; on average, indicating moderate-to-high Spanish language use for both) than in English (mothers: M = 2.78, SD = 1.28; fathers: M = 2.95, SD = 1.12; indicating low-to-moderate English language use). Fifty-one percent of participating children were male, they were ages 8 to 10 (M = 9.14 years, SD = 0.86), and 95% had been born in the U.S. Based on age- and gender-specific BMI percentiles from the CDC website (Kuczmarski et al., 2000), almost half of children were classified as having overweight (14%; 85th to <95th percentile), or obesity (34%; >95th percentile).
Means, Standard Deviations or Percentages for Demographic Characteristics of 141 Mexican American Mothers, Fathers and Children.
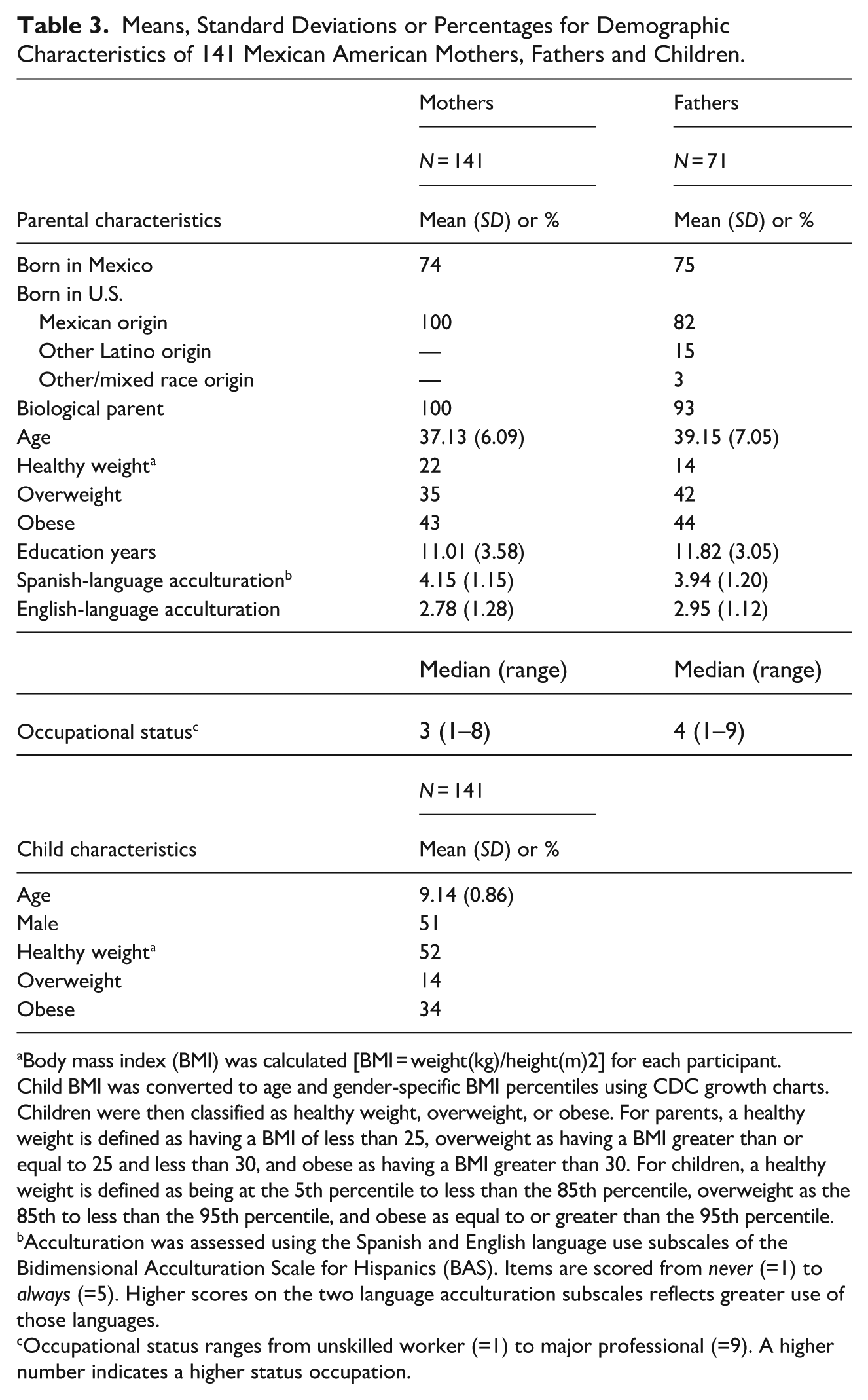
Body mass index (BMI) was calculated [BMI = weight(kg)/height(m)2] for each participant. Child BMI was converted to age and gender-specific BMI percentiles using CDC growth charts. Children were then classified as healthy weight, overweight, or obese. For parents, a healthy weight is defined as having a BMI of less than 25, overweight as having a BMI greater than or equal to 25 and less than 30, and obese as having a BMI greater than 30. For children, a healthy weight is defined as being at the 5th percentile to less than the 85th percentile, overweight as the 85th to less than the 95th percentile, and obese as equal to or greater than the 95th percentile.
Acculturation was assessed using the Spanish and English language use subscales of the Bidimensional Acculturation Scale for Hispanics (BAS). Items are scored from never (=1) to always (=5). Higher scores on the two language acculturation subscales reflects greater use of those languages.
Occupational status ranges from unskilled worker (=1) to major professional (=9). A higher number indicates a higher status occupation.
Fathers were present for half of the meals. If present, most fathers ate with the child (96%). Mothers mostly always served (96%) and plated (94%) the participant child their meal, and ate with the child (85%). Siblings (66%), and other family members or friends (17%) were also present during the child’s evening meal, and mostly always ate with the child (96%). The TV (16%) and music (8%) were seldom on and the majority of family conversations during meals were in Spanish (73%).
Children ate a variety of foods during their meal and no child ate fast food. The majority of children ate a type of meat, such as pork, chicken, beef or fish (66%), and drank juice or sugar-sweetened beverage (55%). Many children ate a type of grain, such as rice or pasta (49%), and raw or cooked vegetables (48%). Other types of food included tortillas, bread, cheese, leafy vegetables, and fruit (33%–13%). Only 1% of children ate eggs or a dairy product at dinner.
Mothers’ and Children’s Behavior at Meals With Fathers Present or Absent
We explored fathers’ presence in the context of mothers’ and children’s evening mealtime behaviors by stratifying the videos by whether or not the father was present (Table 1). For this analysis we report on differences of 10% or more in meals with fathers present or absent. The 10% threshold was arbitrarily selected to highlight differences in the occurrence of mothers’ and children’s behaviors. When examining mothers’ positive involvement in their child’s meal, a lower percentage of mothers offered more food (62% vs. 80%) when fathers were present, compared to when fathers were absent. Additionally, a lower percentage of mothers asked their child if they were done eating (31% vs. 49%) when fathers were present, compared to when fathers were absent.
Regarding child eating behaviors, a higher percentage of children used positive talk about food when fathers were present at the meal, compared to children with fathers absent at the meal (30% vs. 17%; Table 2). There were no differences between children whose fathers were present or absent at the meal, for negative talk about the food, agreeing to take more food, or requesting or negotiating to eat less food. Regarding the type of food children ate, a higher percentage of children ate grains, such as rice or pasta, when fathers were present compared to when fathers were absent (58% vs. 40%). A lower percentage of children ate fruit when fathers were present, compared to when fathers were absent (8% vs. 19%).
Discussion
To understand fathers’ family interactions during Mexican American children’s meals, this structured observational study with descriptive analysis examined video-recorded evening family meals. Specifically, we qualitatively observed mothers’ feeding practices, children’s eating behavior and type of food eaten, when fathers were present, versus when they were absent. Overall, fathers’ presence or absence at mealtimes co-occurred with certain types of mothers’ feeding practices and children’s eating behavior. To our knowledge, this is the first observational study to report that when Latine fathers were present at mealtime, fewer mothers engaged in certain types of PFP that reflected positive involvement in their child’s meal.
Fathers’ presence at children’s evening meals appears to allow mothers to share the responsibility with fathers for communicating with their children about the meal, including whether they have enough food or are done eating. Mothers remain engaged when fathers are present but may be choosing to pull back to encourage father-child communication. Moreover, because on average fathers were employed as skilled workers, it is likely that many fathers had early morning work schedules that left little opportunity to engage with their children (Martinez et al., 2014). Consequently, fathers may view being present at evening meals as time to “catch up” with other family members and as a time to bond with them outside of work hours (Harris et al., 2020). For some children, evening meals may also be the first time in a day that children may see and engage with their father opening up the opportunity for communication in families.
Relatedly, when we examined children’s eating behaviors, more children with fathers and mothers present, compared to children with only mothers present, engaged in positive talk about the food. Having fathers present may offer more opportunities for children to have discussions and learn about the food served. This finding is important as there is a dearth of research examining Latine fathers’ behavior around mealtimes in relation to their children’s eating behavior. The link between fathers’ behavior during meals and the development of children’s eating behavior deserves further exploration (Litchford et al., 2020).
Regarding type of food eaten, when fathers were present, more children ate grains, such as rice or pasta, and fewer children ate fruit. It may be that fathers managed meals with their child’s mother and chose the type of food served (Khandpur et al., 2016; Lora et al., 2017). For example, Khandpur et al. (2016) examined coparenting around food parenting practices among primarily Black and White fathers and found that because cooking was primarily the mother’s responsibility, fathers contributed by making the decisions around what to cook or what to eat. Intervention research with Mexican American fathers is still needed to understand how feeding practices between fathers and mothers during mealtimes, especially congruent parental practices, contributes to the development of children’s long-term eating behavior, and subsequently their weight status (Rahill et al., 2020).
Whether or not fathers were present during the meal, no families served fast food, and mothers almost always served their children homemade meals. Findings from a qualitative study with Latine mothers about attitudes and beliefs about feeding practices reported that serving home cooked foods was an important part of their role as caretakers (Martinez et al., 2014). Increasing access to grocery stores for Mexican American families in underserved communities would help support this protective cultural value and feeding behavior against obesity. Regarding fathers, results from a qualitative study conducted by E. Jansen et al. (2020), focused on fathers’ perceptions of mealtime strategies, indicated that fathers are open to helping with meals and that they view family meals as a complex set of arrangements between parents that are flexible and include a balance of structuring meals and assigning tasks to family members (E. Jansen et al., 2020). To enhance our understanding of paternal contributions to the family mealtime environment, further research should examine how Mexican American fathers across different family compositions describe, negotiate, and share the responsibility for family meals and child feeding.
Consistent with research indicating elevated consumption of sugar-sweetened beverages (SSB)s among Latine children in the US (Beck et al., 2020), more than half the children (55%) in this study also drank juice or other SSB, including soda, with dinner. SSBs are associated with negative health outcomes, including obesity and type 2 diabetes (CDC, 2024). Dietary management and educational campaigns directed at Latine mothers and fathers that support drinking tap water, diluting fruit juice with water, and reducing the stock of SSBs in the home may provide an important and culturally appropriate avenue to curb SSB consumption among children (Alman et al., 2021).
Regarding policy considerations, excise taxes on SSBs can drive down consumption and should continue to be promoted as a key policy to reduce the harms associated with sugary drinks such as obesity (Colchero et al., 2017). SSB taxes are thought to be related to decreases in weight because increased SSB prices and increased awareness of their harmful effects lead to decreased purchasing and decreased consumption of SSBs (Liu et al., 2025; Young et al., 2024). In one study, Young et al. (2024) examined city-level taxes on SSBs and changes in BMI percentiles among youth aged 2 to 19 years after tax implementation, and reported youth living in cities with SSB taxes had significantly lower BMI percentiles compared with youth living in cities with no taxes. In a separate study examining adults of this cohort, Liu et al. (2025), reported decreases in BMI among young adult White women living in cities with SSB taxes compared to those living in cities with no taxes. Public health leaders and policymakers should consider implementing taxes on SSBs to help prevent obesity (Kaplan et al., 2024).
Thirty-four percent of the Mexican American children in this study were classified as having obesity, which is higher than the national rate of 28% in this population. The development of obesity in children is due to multiple socioecological factors, including family-level behavioral risk factors (CDC, 2024; Hochgraf & Ruggiero, 2021). Anti et al. (2016) conducted a study of health care providers’ experiences with fathers and reported that fathers may take a passive role and defer to mothers in the management of their child’s weight. The providers also reported a perceived tendency of fathers to resist accepting their child’s weight as a problem and to resist change and even undermine family efforts to make healthier choices (Anti et al., 2016). Mexican American fathers, like mothers, may hold the cultural belief that “chubby is better” and that skinny children are perceived as malnourished and may have trouble accepting that their children have overweight or obesity (Martinez et al., 2017). Furthermore, in a focus group study of mostly mothers of Mexican origin, mothers reported that fathers’ resistance to change was often related to fathers’ own preferences for traditional foods or prepared foods that mothers perceived to be high-calorie or less healthy (Lora et al., 2017). In another qualitative study with Mexican and Puerto Rican mothers which focused on making meal changes to improve nutrition at home, mothers reported that resistance from children and fathers often led to more time preparing different meals for different family members (Hammons et al., 2021). Expanding training for pediatric care providers on how to talk to fathers about involvement in children’s meals, as well as about how to get fathers more involved in family-level obesity interventions could support mothers’ efforts to provide nutritious food, and may help reduce obesity risk among youth (Wong et al., 2017).
Parents’ and children’s mealtime practices reflect the context in which families are embedded and are modifiable risk factors. In addition to family-level factors, the development of obesity in Latine children is due to multiple structural and environmental factors such as easy access to sugary drinks and a lack of grocery stores or clean safe places to play and exercise (Cleveland et al., 2023). An Australian program, Healthy Dads Healthy Kids, guided by a socioecological framework, was the first program internationally to specifically target overweight fathers in a weight loss program together with their children for obesity prevention (Morgan, Lubans, Plotnikoff, et al., 2011). The program included seven weekly sessions and assisted overweight fathers to lose weight, improve lifestyle behaviors, and optimize their parenting practices. The primary outcome was father’s weight. Secondary outcomes included child BMI z-score and lifestyle behaviors, such as increased physical activity and improved dietary behaviors. The program demonstrated significant effects on fathers’ weight loss, and fathers’ and children’s lifestyle behaviors across efficacy (Morgan, Lubans, Callister, et al., 2011), effectiveness (Morgan et al., 2014), and dissemination trails (Morgan et al., 2019). The Australian program only included families of European descent and in a society with significant societal support (e.g. universal healthcare), and, as such the applicability to families of other races and ethnicities in the U.S. needs examination. Research that is tailored to fathers and their children holds promise for the prevention of obesity.
While this study makes important contributions to our understanding of the co-occurrence of fathers’ presence at meals and Mexican American mothers’ feeding practices and child’s eating behaviors, there are limitations to note. First, member checking, a process in which researchers’ interpretations of the data are presented to the participants, did not occur (Birt et al., 2016). To improve the validity and reliability of synthesized observational data, future studies should consider providing opportunities for participants to review selected film footage and related quotes to ascertain whether their reflections align with the interpretations of the researchers (Smit & Onwuegbuzie, 2018). Second, families could have been performing for the RA who was recording the meal and could have changed their mealtime behaviors due to the presence of a camera (Haidet et al., 2009). Nonetheless, this risk is outweighed by the potential for a new understanding of parents’ feeding practices and children’s eating behaviors (Rhee et al., 2015). Third, assessment of food amounts was challenging given that video-recorders were six feet away from the table and we were unable to discern serving sizes, identify which foods were on the plates, or quantify the amount of food consumed. Future observation research interested in examining if fathers’ feeding practices vary based on children’s serving sizes or what and how much was consumed may consider a semi-naturalistic environment that incorporates additional methods for measuring precise portions (Pesch & Lumeng, 2017). Fourth, only the meals of heterosexual and mostly (84%) two-parent families were analyzed. Future research about fathers should examine children’s meals when there is no mother present, with single fathers, and same-sex parents. Implications include ensuring greater generalizability about the influence of fathers, and enhancing interventions and clinical guidance for families. Additionally, because the sample size was relatively small, this study should be considered exploratory. Nonetheless, because previous qualitative studies usually had smaller samples (e.g., Harris et al., 2020; Turner et al., 2014; Zhang et al., 2018) this study contributes to the existing limited literature. Finally, as a qualitative study, statistical analyses were not conducted. Therefore, the percentage differences reported for mothers’ feeding practices, children’s eating behavior and type of food eaten, when fathers were present, versus when they were absent should be interpreted as descriptive and preliminary, requiring confirmation in future research using statistical analyses.
This study has several strengths. Video-recorded behavioral observation is a qualitative method based on ethnography that has not been commonly used in obesity prevention research with fathers, particularly during family meals. Conducting this study in the home allowed us to capture interactions between mothers, fathers and their children in a naturalistic environment, allowing for meaningful visual and auditory observations. Another benefit of our observational research is that it avoided the power dynamics between facilitators and participants that can emerge in interviews and focus groups, and encouraged a natural flow of communication and interactions among the members in the family (Tolley et al., 2016). For example, allowing parents and children to talk among themselves about the child’s meal may enable freer dynamics or conversations to emerge, and give space for parents and children to agree and disagree with each other, thus potentially deepening their discussion. Because study participants were recruited from an integrated healthcare delivery organization, they were all insured at the time of the study and therefore represented a wide spectrum of socioeconomic circumstances. This study provides insights about an understudied population, fathers, most of Mexican origin, on practices that may promote or inhibit children’s healthy eating behavior. This is particularly important, because most studies that have explored similar factors in Mexican American families have been based on mothers’ reports and have rarely engaged fathers. Recognizing that fathers play a role in parenting, and in the health and well-being of families, this study addresses the important goal of including fathers in research. Information from fathers of Mexican American children could be useful when developing strategies aimed at preventing obesity in children.
Conclusions
In this observational study on fathers’ presence or absence during children’s evening meals, we found that when fathers of Mexican American children were present during their children’s meals, fewer mothers engaged in certain feeding practices that reflected positive involvement in children’s meals, and more children engaged in positive talk about the food. These results highlight a pathway between fathers’ presence at mealtimes, mothers’ feeding practices, and children’s eating behaviors. If fathers are present during their children’s mealtimes, in addition to mothers, their presence may have a positive impact on children’s current and long-term health and well-being. Preventive behavioral health intervention strategies would benefit from including a focus on the importance of fathers’ presence at children’s meals.
Findings from this study are important, because fathers participate less often than mothers in research studies. Consequently, there is a lack of understanding of child feeding in the context of family meals with fathers present. Identifying innovative intervention strategies for fathers in two-parent families, that complement mothers’ strategies, could help to improve health outcomes for their children. Including fathers across varying family compositions, such as single-father homes, in pediatric obesity research could potentially enhance the effectiveness of family-level obesity prevention and treatment programs.
Footnotes
Acknowledgements
The authors wish to thank the families who participated in the study, and Celina Solis and Raquel Arellano for their assistance with coding the observations. The authors thank Jennifer Cho, Irene Takahashi, and the Kaiser Foundation Research Institute, who provided access to members of Kaiser.
Ethical Considerations
This study was approved by the University of California and Kaiser Permanente Northern California Research Foundation institutional review boards.
Consent to Participate
Written informed parental consent was obtained.
Author Contributions
Carlos Penilla: Conceptualization (lead); Writing-Original draft (lead). Suzanna M. Martinez: Methodology; Writing-Original draft. Julianna Deardorff: Analysis; Writing-Review and editing. Jeanne M. Tschann: Funding Acquisition; Writing-Review and editing. Louise C. Greenspan: Resources; Writing-Review and editing. Elena Flores: Writing-Review and editing. Lauri A. Pasch: Writing-Review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was primarily supported by the National Cancer Institute Diversity Supplement grant 3R01CA247705-02S1 awarded to Penilla. This research was also supported by the National Heart, Lung and Blood Institute (R01 HL084404, Tschann; K01 HL129087, Martinez). Additional support was provided by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under cooperative agreement U8DMC45901.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data from this study are not available in a public archive. De-identified data from this study will be made available (as allowable according to institutional IRB standards) by emailing the corresponding author.*