
Abstract
Youths (N = 57; mean age = 13.83 years) residing near Tororo, Uganda, were interviewed to obtain quantitative and qualitative data pertaining to negative life events, adjustment problems, coping, social support, self-worth, and hope. On average, they experienced nearly half of the 22 negative life events assessed. The experience of negative life events related positively to internalizing problems and negatively to social support and self-worth. Coping strategies (problem-focused, positive reframing, avoidance, and support-seeking) were positively associated with hope. Problem-focused coping was negatively related to externalizing problems. Furthermore, social support was positively associated with coping strategies, self-worth, and hope and was negatively related to adjustment problems. The qualitative data shed light on the difficult events the youths endured and what types of coping strategies they used. Ultimately, interviews suggested that youths experienced many negative events, but they remained optimistic.
In many third-world countries, particularly those challenged by HIV and limited medical services, youths face severe difficulties. They are exposed to social and material deprivation at levels not experienced by most youths in Western cultures. Given these situations, one might expect maladjustment, especially if coping skills are taxed and rendered ineffective.
Uganda recently has made progress in lowering the prevalence of HIV (Hallett et al., 2006). Moreover, the introduction of universal primary education dramatically increased primary school enrollment. Nonetheless, Ugandan youth face a number of challenges. The number of orphans in Uganda began to swell as result of war and civil unrest in the 1980s and continued to rise with the spread of HIV (Wakhweya et al., 2002). United Nations Children’s Emergency Fund (UNICEF, 2008) reported that almost half of Uganda’s 2.3 million orphans were orphaned because of AIDS. In addition, 85% of Ugandans lived on less than US$ 1 per day between 1995 and 2005 (UNICEF, 2008).
The goal of this study was to obtain a greater understanding of youths’ difficult life events, coping strategies, and hope for the future, as well as, to examine the interrelations of life events, hope, self-worth, social support, coping strategies, and maladjustment in a sample of youth in Uganda. Understanding the manner in which life events, protective factors associated with resilience (e.g., coping, social support, self-worth), and adjustment relate may provide clues regarding how resilience and adjustment can be fostered in challenging contexts.
Life Events/Stressors: Risk Factors for Adjustment Problems
Experience of negative life events may be a risk factor for developing internalizing and externalizing problems. Ugandan youths are likely to experience a number of negative life events/stressors, such as loss of a parent, and this may increase the likelihood of many other stressors (poverty, lack of food, and limited access to education) by reducing available resources. AIDS-related bereavement may be especially difficult. Wood, Chase, and Aggleton (2006) noted that children of parents suffering from HIV/AIDS may experience a host of issues before their parents pass away including anticipatory loss, low parenting quality, and social stigma.
Stressors associated with parental loss may introduce barriers between youths and their education. In Northern Uganda, Oleke, Blystad, Fylkesnes, and Tumwine (2007) found that of the households caring for school-aged orphans, only 55% of the male and 62% of the female orphans lived in households in which all of the children were in school. According to community members, many enrolled youths did not attend regularly, sometimes due to work responsibilities.
Researchers have found that life stressors (e.g., illness, poverty, school transitions, loss of a parent) have been related to youths’ internalizing and/or externalizing problems (see Grant et al., 2003; Worden & Silverman, 1996). In Grant et al.’s (2003) conceptual model, stressors relate to psychopathology through their influence on biological, psychological, and social processes. With regard to health problems, which Ugandan youths often experience, Timko, Stovel, Baumgartner, and Moos (1995) theorized that the association between stress and maladjustment is due to the disruption in functioning that occurs and the emotional arousal that typically accompanies stressors.
Numerous researchers have found that life stressors are related to externalizing and internalizing (e.g., Kim, Conger, Elder, & Lorenz, 2003; Work, Parker, & Cowen, 1990); however, some researchers have found positive relations between life stressors and internalizing but not externalizing (e.g., Hagen, Myers, & Mackintosh, 2005). Most of this research has been conducted with Western samples, but there has been some research conducted with Ugandan youths. For instance, in Northern Uganda, war-related events (e.g., seeing dead bodies, being threatened) were positively related to internalizing but not externalizing; however, non–war-related events (e.g., death of parents or siblings) were positively related to youths’ internalizing and externalizing (Amone-P’Olak, Garnefski, & Kraaij, 2007). Similarly, Atwine, Cantor-Graae, and Bajunirwe (2005) found that Ugandan 11- to 15-year-old orphans, compared with nonorphans, had higher internalizing and externalizing problems.
Protective Factors Associated With Resilience and Adjustment
Resilience has been defined as a “dynamic process wherein individuals display positive adaptation despite experiences of significant adversity or trauma” (Luthar & Cicchetti, 2000, p. 858). Hope, self-esteem, social support, and coping may be protective factors related to youths’ resiliency and adjustment.
Hope
Hope may help protect youth from maladjustment. Snyder (1995) defined hope as, “the process of thinking about one’s goals, along with the motivation to move toward those goals (agency), and the ways to achieve those goals (pathways)” (p. 355). Hope may also lead people to appraise situations in a positive manner and foster mastery-oriented responses (Snyder, 2002).
To our knowledge, African youths’ hope seldom has been examined as a protective factor in relation to adjustment. In high-risk U.S. 6- to 12-year-olds, hope was negatively related to internalizing and externalizing even after effects of social support and stress were controlled (Hagen et al., 2005). In another study, however, U.S. youths’ hope was related to lower levels of internalizing 1 year later but was unrelated to externalizing after controlling for baseline levels of maladjustment (Valle, Huebner, & Suldo, 2006). Valle et al. (2006) also found that hope buffered the relation between stressful events and internalizing but not between stressful events and externalizing.
Self-esteem
Self-esteem (or self-worth) has been negatively related to internalizing and externalizing. To our knowledge, self-esteem has not been examined in relation to life events or maladjustment in Uganda. However, South African youths’ global self-worth has been inversely related to suicidality and aspects of externalizing (Wild, Flisher, Bhana, & Lombard, 2004). In addition, Dubow, Edwards, and Ippolito (1997) found self-worth related negatively to U.S. inner-city youths’ antisocial behavior. In very low-income U.S. youths, self-esteem was related positively to resilience (Buckner, Mezzacappa, & Beardslee, 2003). Kliewer and Sandler (1992) suggested that youths with high self-esteem appraise stressors and choose coping strategies in a manner different from youths with low self-esteem.
Social support
Social support has been viewed as promoting adaptive behavior (e.g., DuBois et al., 2002). Sandler, Miller, Short, and Wolchik (1989) suggested that social support may boost self-esteem, perhaps because of approval from others or by offering emotional or tangible resources. In turn, self-esteem may prevent the development of maladjustment.
Social support has been inversely related to maladjustment in Western samples (DuBois et al., 2002; Jackson & Warren, 2000). Number of social support providers negatively related to depression and conduct problems for U.S. adolescents who had a parent with HIV/AIDS (Lee, Detels, Rotheram-Borus, & Duan, 2007). Furthermore, family social support has been found to buffer the relation between stressful events and antisocial behavior (Dubow et al., 1997).
Coping
Coping is defined as “conscious volitional efforts to regulate emotion, cognition, behavior, physiology, and the environment in response to stressful events or circumstances” (Compas, Connor-Smith, Saltzman, Thomsen, & Wadsworth, 2001, p. 89). Various types of coping have been identified and sometimes these types predict different outcomes (see Compas et al., 2001; see Compas, Malcarne, & Fondacaro, 1988). In a review, Compas and Reeslund (2009) reported that for adolescents experiencing controllable stressors, primary control coping (coping by influencing the condition or emotional reaction; e.g., problem solving) was related to better adjustment. When the stressor was out of the adolescents’ control, secondary control coping (attempting to create a fit between the person and situation; e.g., cognitive restructuring, distraction) was related to better adjustment. Adolescents using disengagement or avoidance (disengaging from the situation or emotional response) had poorer adjustment in response to controllable or uncontrollable stressors (Compas & Reeslund, 2009).
Compared with Western cultures, common stressors in Uganda are likely to be out of youths’ control (e.g., death of family member or friend, illness). Thus, secondary control coping may relate to better adjustment. Coping strategies of African youths seldom have been examined, making it difficult to ascertain whether avoidance would relate to adjustment problems. It is possible that in such an adverse context as Uganda, any coping style is desirable as opposed to dealing with the stressor with nonconstructive means (e.g., ruminating).
Religiosity and spirituality
According to the Uganda Bureau of Statistics’ 2002 census, Uganda has more than 20 million Christians (mostly Catholic and Anglican), about 3 million Muslims, and smaller numbers of people with other or no religious endorsements. As in other parts of the world, religion has been used to justify conflict in Uganda (e.g., Lord’s Resistance Army [Adam, De Cordier, Titeca, & Vlassenroot, 2007] and the recent antihomosexuality bill). Nonetheless, religion has had a positive influence on many fronts. Religious institutions in Uganda have affected literacy (Openjuru & Lyster, 2007), promoted monogamy and discouraged taking multiple wives—which have effects on HIV transmission (Otiso, 2006; but see Kinsman, Nakiyingi, Kamali, & Whitworth, 2001), and faith-based groups provide medical, financial, and other forms of aid.
Religiosity (e.g., beliefs and involvement with religious institutions) and spirituality (e.g., prayer and devotion) shape one’s identity (see Roeser, Issac, Abo-Zena, Brittian, & Peck, 2008), and anecdotal reports suggest they are very important to Ugandan’s identity. There is a strong emphasis on prayer in public life and in the government. It is possible that the general lack of material items leads to a strong spiritual focus. Gratification cannot be obtained from “things” and must be derived elsewhere. Furthermore, there is so much suffering and death that there is a need for hope beyond the grave. Given the role religion plays in Ugandan life, religiosity and spirituality may be particularly relevant in promoting Ugandan youths’ resiliency.
Religious coping (e.g., asking God for guidance, prayer/meditation, trusting God’s plan) may foster resilience. For example, based on interviews, Tankink (2007) described how a Ugandan pastor instructed his congregation to deal with painful memories of war by using self-control to stop negative thoughts and to focus on God. Spirituality and religiosity may be especially helpful in situations in which the stressor cannot be modified through problem solving. Park and Folkman (1997) suggested that meaning-making, which sometimes entails religion, may allow people to cope with major trauma and loss. Park (2005) also argued that religion often assists individuals in appraising the meaning of stressors (e.g., viewing the stressor as God’s plan), reappraising situational meaning (e.g., positive reinterpretation), and in some cases, changing global meaning (e.g., resolving that some things are beyond understanding).
Religiosity has been viewed as a protective factor associated with positive outcomes. For example, religiosity is related to social support, well-being, purpose and meaning in life, prosocial and moral behavior, feelings of belonging, and health benefits (e.g., see Johnson, 2008; see McCullough & Willoughby, 2009; Pargament & Maton, 2000; Smith, McCullough, & Poll, 2003). Furthermore, religious/spiritual practices (e.g., prayer) have been related to self-control and regulation, which are relevant to coping and a host of other positive outcomes (see McCullough & Willoughby, 2009). Youths’ religiosity has been related to higher self-esteem and more hope for the future and has been negatively related to depression and loneliness (for review, see King & Roeser, 2009). Similarly, in Smith et al.’s (2003) meta-analysis, religiousness was at least modestly associated with fewer depressive symptoms. The relation was the strongest in samples experiencing high psychosocial stress. In addition, Sallquist, Eisenberg, French, Purwono, and Suryanti (2010) found that Muslim Indonesian youths’ religiousness was negatively related to concurrent externalizing and internalizing, although it was not related to externalizing or internalizing 8 months later when controlling for earlier adjustment problems.
The Present Study
In the present study, Ugandan youth were interviewed to address three aims. First, we wanted to describe Ugandan youths’ negative life events. Determining how prevalent negative life events were for the sample, as well as what events were perceived as being the most difficult, might provide information to guide intervention efforts with limited resources needing a targeted aim of intercession. Second, we sought to examine relations between negative life events and adjustment. Relevant research with Ugandans generally has been focused on adjustment in relation to a specific event (e.g., parental death). We surveyed events ranging from extreme to comparatively mild to determine whether number of life events, both large and small, related to internalizing and externalizing. Third, we explored coping strategies and other protective factors (social support, self-worth, and hope) that may relate to resilience. Such constructs infrequently have been examined in African youth but may provide insight regarding promoting resilience in Uganda and similar cultures. Related to this goal, we asked open-ended questions about coping, optimism, and hope.
On the basis of the research just reviewed, the number of negative life events was expected to relate positively to internalizing and externalizing but negatively to social support, self-worth, and hope. Social support, self-worth, and hope were expected to be positively related with one another and to negatively relate to externalizing and internalizing. We tentatively predicted that problem-focused, positive reframing, and support-seeking coping would relate negatively to internalizing and externalizing; however, we were unsure whether avoidance would relate to greater adjustment problems as it has in Western cultures. Moreover, it seemed possible that secondary control coping (positive reframing), when compared with primary control coping (problem focused), might relate to fewer adjustment problems.
Method
Participants
A total of 57 (n = 35 girls; 61%) youths (9-20 years old, M = 13.83, SD = 2.83) participated. Four participants were missing age data but were at least 11, 11, 13, and 17 years old based on grade level. Fifty-four (95%) attended school; however, education often was interrupted because of a lack of school fees or because of illness. According to youths’ reports, 13 lived with both biological parents, 2 lived with two parents through remarriage, 22 lived with one parent, 13 lived with a relative, and 1 lived with a Pastor (six gave no response).
Participants lived in rural areas near Tororo, Uganda. Ugandan youth were of interest because of the stressors they face, such as illness, poverty, and loss of parents. We expected that coping would be extremely important for these children. Most youths lived in mud huts or in rented rooms of cement buildings. Many youths described daily life as busy with chores. A 13-year-old girl discussed her day, “I wake up, sweep the house, get water, do cooking, wash the plates, and bathe the small children.” No participants had running water or electricity in their homes. The region receives some degree of assistance; for example, 30% of the participants reported receiving support (a school uniform, mosquito net, and mattress) from an organization.
It would be difficult to recruit a sample with methods typically used in Western samples, particularly because of lack of reliable means of communication (e.g., phone, Internet) with potential participants when not face-to-face with them. Thus, Ugandan staff members of a local nonprofit organization explained the study to youths and their caregivers/parents (henceforth called caregivers) near places such as the local church, clinic, water well, and school. Nearly all of the people approached were interested in participating. They were told which days interviews were being conducted. To be culturally sensitive, participants came to the interview on the day that was best for them rather than at a scheduled time.
Procedure
Data were collected in July 2007 by trained American women. Although English often is spoken in the area (e.g., in the classroom), local Ugandan interpreters proficient in the dialect of the child and in English were used for seven of the interviews.
Written consent from caregivers and verbal assent from youths were obtained. To establish rapport, the interviewer asked the child to draw a picture of his or her home and to explain the drawing. All questionnaire items and open-ended questions were read aloud, as literacy levels varied substantially, and participants verbally responded. To facilitate responding to questionnaire items and to reduce demands on memory, visual aids depicting the Likert-type scales were utilized. The order in which the responses appeared on the visual aid (e.g., very bad to very good or very good to very bad) was counterbalanced across participants. Youths often gave more than one response to open-ended questions, but reported results represent the first response. Responses to open-ended questions were audiotaped for transcription and coding. Sessions took 1 to 2 hr and were conducted in private rooms of the hospital or orphan center.
At the end of the interview, participants were asked whether they had any questions or concerns. Any serious concerns were referred to local social workers. Participants received a bag of rice and a bag of beans, as well as a small toy, as compensation.
Measures
Several Ugandans and Americans who were very familiar with Ugandan culture reviewed questionnaire items to assess applicability to the population. After an American Peace Corps volunteer who resided in the village conducted pilot interviews, further decisions were made. Items (e.g., “I don’t have much energy”) occasionally were reworded so that they did not contain negatives, were omitted because they did not apply (e.g., “You went skateboard riding or roller skating”), or were omitted because they likely assessed normative rather than problem behavior in the culture (e.g., “Do you set fires”; details available from the first author).
Time limitations prevented interviewing both caregivers and youths, and it was assumed that youths could provide better information about life events and a number of other variables than could their caregivers. Youths responded to questionnaire items and open-ended questions regarding the following (in order of appearance in the interview): background information, life events, internalizing and externalizing, coping, self-worth, social support, and hope. Participants’ responses to open-ended questions were transcribed from audio recording. Categories were created based on common response themes and then two coders categorized participants’ responses (agreement ranged from 89% to 98%). Discrepancies were resolved through consensus.
Life events
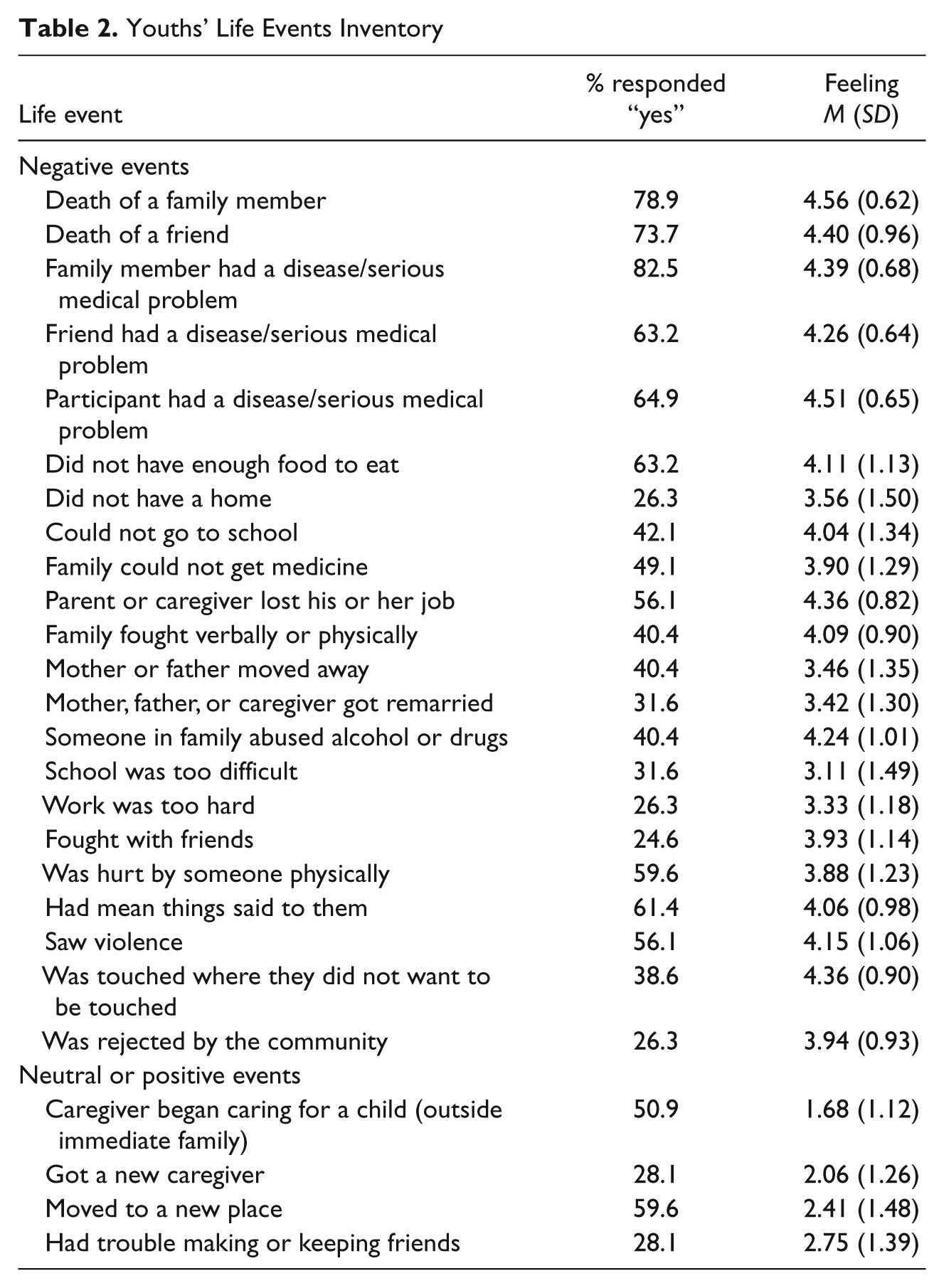
On the basis of conversations with community members and Americans very familiar with the culture, items were created to assess the occurrence of 26 events and compiled in our Youths’ Life Events Inventory. To ensure the event experience was interpreted as negative, if a participant responded, “yes” to an item, he or she was asked to indicate how it made him or her feel (1 = really good to 5 = really bad). Four items were omitted because participants experiencing these events, on average, rated them as eliciting neutral or positive feelings (i.e., “Did your parent or caregiver begin caring for a child from outside of your immediate family,” “Did you have trouble making or keeping friends,” “Did you get a new caregiver,” and “Did you move to a new place”). Some of these items may have been rated as positive because experiencing the events signaled an improvement in their lives. The reason that the item regarding difficulty with friends was rated as neutral was unclear. The remaining 22 items were summed. The alpha coefficient is not reported because the events were not all expected to correlate (e.g., Haine, Ayers, Sandler, Wolchik, & Weyer, 2003).
Internalizing and externalizing
Participants responded to items from the Youth Self Report (Achenbach, 1991). Several original items were not administered because they were not culturally appropriate. Twenty-seven items from the Aggression and Delinquency subscales were summed to form an externalizing composite (α = .83), and 20 items from the Anxiety/Depression and Withdrawal subscales were summed to form an internalizing composite (α = .75).
Coping
Participants rated items (1 = never to 4 = most of the time) from the Children’s Coping Strategies Checklist-Revision 1 (Program for Prevention Research, 1999). A few original items were modified or omitted to be culturally appropriate (e.g., “You went skateboard riding or roller skating”). Retained items assessed the frequency with which children utilized problem-focused coping (12 items; e.g., “You thought about what you could do before you did something”; α = .78), positive reframing coping (12 items; e.g., “You tried to notice or think about only the good things in your life”; α = .80), avoidance (12 items; e.g., “You tried to stay away from things that made you feel upset”; α = .72), and support-seeking strategies (9 items; e.g., “You told others how you would like to solve the problem”; α = .72) within the past month when they had problems. The distraction strategies subscale (four items; e.g., “You went for a walk”) was dropped because of a low alpha. Items were averaged within subscale. Subscale scores were positively related, range rs(50) = .41 to .70, ps < .01 (controlling for age); however, subscales were not combined because coping types may relate to adjustment in different ways.
Self-worth
Self-worth was assessed with the Perceived Competence Scale for Children’s Global Self-Worth subscale (Harter, 1982; six items). The interviewers described two different kinds of children (e.g., “Some children are often unhappy with themselves, but other children are pretty pleased with themselves”). Participants indicated the type of child to which they were more similar. Then participants indicated whether that kind of child was really like them or sort of like them. After recoding reversed items, the items were averaged (α = .72).
Social support
Participants rated (1 = never to 5 = always) items from the Survey of Children’s Social Support (Dubow & Ullman, 1989; e.g., “How often can you find someone to talk to when you are angry about something?”). Some of the original items were dropped to be culturally appropriate (e.g., “When you want to know all about a new movie or TV show, can you find someone to tell you about it?”). The remaining 19 items were averaged (α = .85).
Hope
Youths rated (1 = never to 5 = always) six items from The Children’s Hope Scale (Snyder et al., 1997). Hope was conceptualized as perception of ability to initiate and sustain action toward a desired goal and perceived capacity to achieve goals (e.g., “I can think of many ways to get the things in life that are most important to me”; α = .70).
Results
Means, standard deviations, and correlations are reported in Table 1. Age was negatively and positively related with externalizing and problem-focused coping, rs(51) = −.42 and .39, ps < .01, respectively. For this reason, and because age varied, zero-order and age-partialled correlations (which resulted in the loss of four participants without age data) are reported.
Means, Standard Deviations, and Correlations
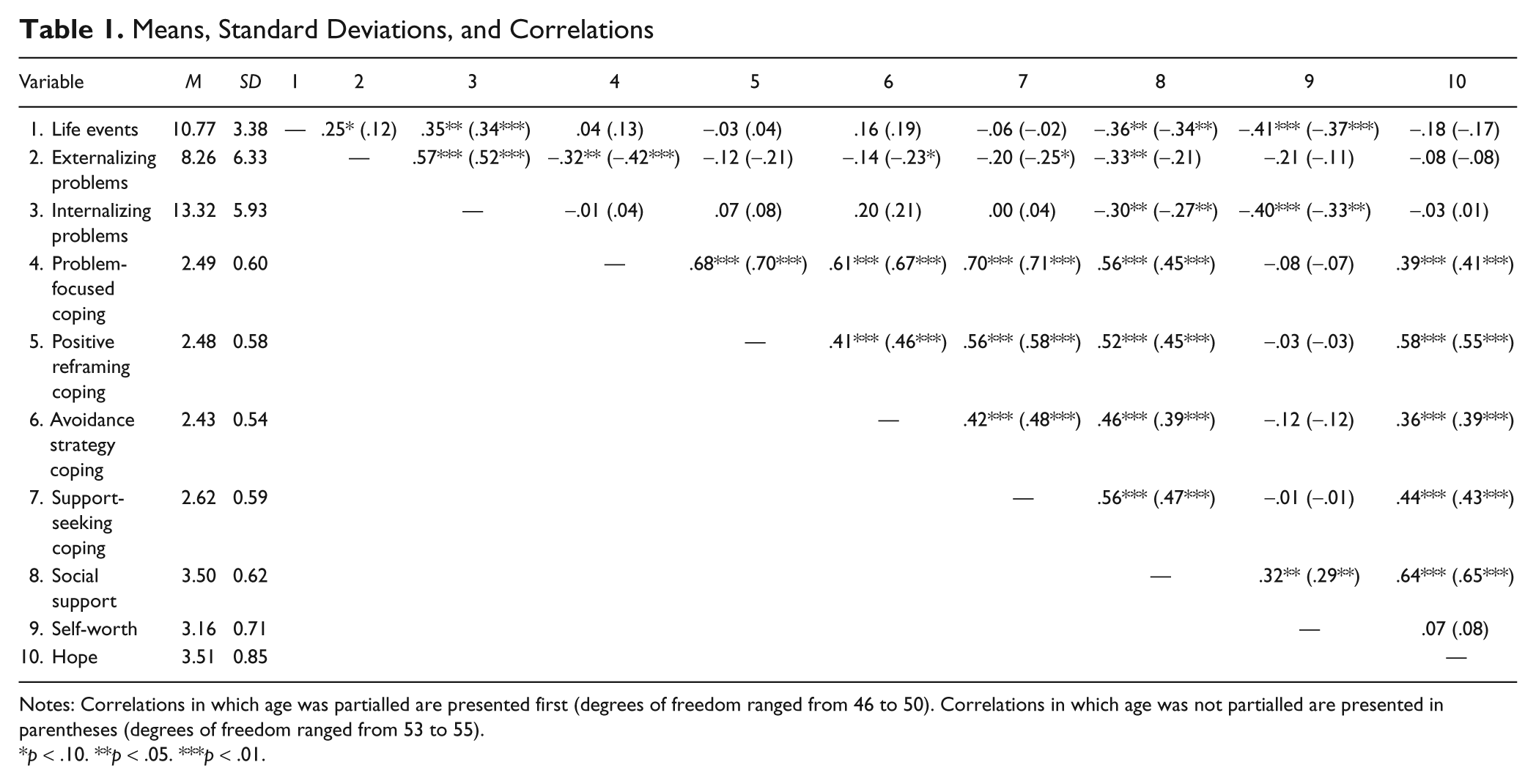
Notes: Correlations in which age was partialled are presented first (degrees of freedom ranged from 46 to 50). Correlations in which age was not partialled are presented in parentheses (degrees of freedom ranged from 53 to 55).
p < .10. **p < .05. ***p < .01.
Correlations Among Study Variables
Experience of negative life events related to higher internalizing and lower social support and self-worth. Problem-focused coping was negatively related to externalizing. Social support was negatively related to externalizing (although not when age was controlled) and internalizing problems but positively related to each type of coping, self-worth, and hope. Self-worth related negatively to internalizing. Each type of coping was positively related to hope. Consistent with previous research (Achenbach & Edelbrock, 1983), internalizing and externalizing were positively related. No sex differences in the correlations were detected with Fisher’s r-to-z tests.
Negative Life Events and the Most Difficult Events
On average, youths reported experiencing 10.77 of the 22 negative events assessed in the Youths’ Life Events Inventory. They are presented in Table 2 and elaborated on in the Discussion section.
Youths’ Life Events Inventory
In an open-ended question, youths were asked to describe the most difficult event in their life. Common themes emerged in their responses. The most frequently reported difficult life event was the death of, or separation from, a parent (n = 12 [21%]). For example, one boy said, “It was very difficult when my father died. I thought I was going even to leave the school. It was a long suffering because he left us when we were still young . . . no way we can get even food. Even our mummy did not have work or a way to get a job” (15 years old). A girl explained her most difficult time, “[It was] after my daddy died. Life really became very difficult for me. There was nothing I was getting at all. Now my aunt came and picked me up but still . . . I’m getting difficulty in my life. Now I’m staying with her but she lacks a good job and money to get me my personal materials. I really feel bad when some people have all materials, and me, I’m just there and I lack material things. When I’m at school . . . no stockings. Shoes I have, because they give them to us . . . So I find my life difficult” (13 years old). A boy explained his most difficult time, “When I didn’t see my dad because he was murdered. It was difficult because we were left without help” (19 years old).
The next most frequently discussed difficult event was being unable to go to school (n = 8 [14%]). Examples of education-related responses included: “It’s when I’m not at school and I feel bad” (15-year-old boy), “When I first started secondary school and I can’t pay school fees. My uncle paid for them, but now he doesn’t have a job” (20-year-old girl), and, “When I couldn’t go to school because I was carrying a baby or when I had to work. I was very sad” (11-year-old girl).
Other youths described their illnesses or injury (n = 7 [12%]). For example, a boy stated, “[It was] when I got wounded on my foot by some metal” (9 years old). A girl explained her illness, “It was when I had a headache. They refused me to go to school for one week” (14 years old). A boy discussed his difficult time, “When we lived in the village. We got sick and didn’t have enough food” (15 years old).
Some children described their basic needs not being met (n = 6 [11%]). Examples of this included: “Sometimes it feels difficult when we don’t have food or when we have food but we don’t have charcoal or firewood for cooking” (14-year-old boy), and, “It was a long time ago with my mom when we lived with my grandfather. Money was hard” (11-year-old boy).
A few youths said that the most difficult thing was school or work being too hard (n = 5 [9%]). A girl stated, “My studies. [There is] a lot of work which I have at home and reading is very difficult” (19 years old), and a boy said, “When washing dishes and clothes” (12 years old).
Others mentioned being abused (n = 4 [7%]). For example, a girl said, “When I was staying with my auntie in town. She used to punish me and beat me for nothing” (14 years old). Other youths replied with their most difficult times, “[It’s] when they cane me” (11-year-old girl), and, “Some people came close to me and started beating me” (10-year-old girl).
Another response was loss of a nonparental family member (n = 3 [5%]). A girl explained her most difficult time, “When my half-sister died when she was eight” (10 years old). Another girl said, “When my grandfather died. Life was difficult for me because he helped me with my studies” (14 years old). Seven (12%) youths said they did not know and five (9%) had an inaudible or missing response (e.g., due to recording device failure).
Responses Related to Coping
Youths were asked open-ended questions pertaining to coping: (a) “How do you try to make yourself feel better when you feel bad?” and (b) “Do you ever do things to make yourself feel better? (If ‘yes’), What do you do?” The results are presented in Table 3.
Youths’ Coping
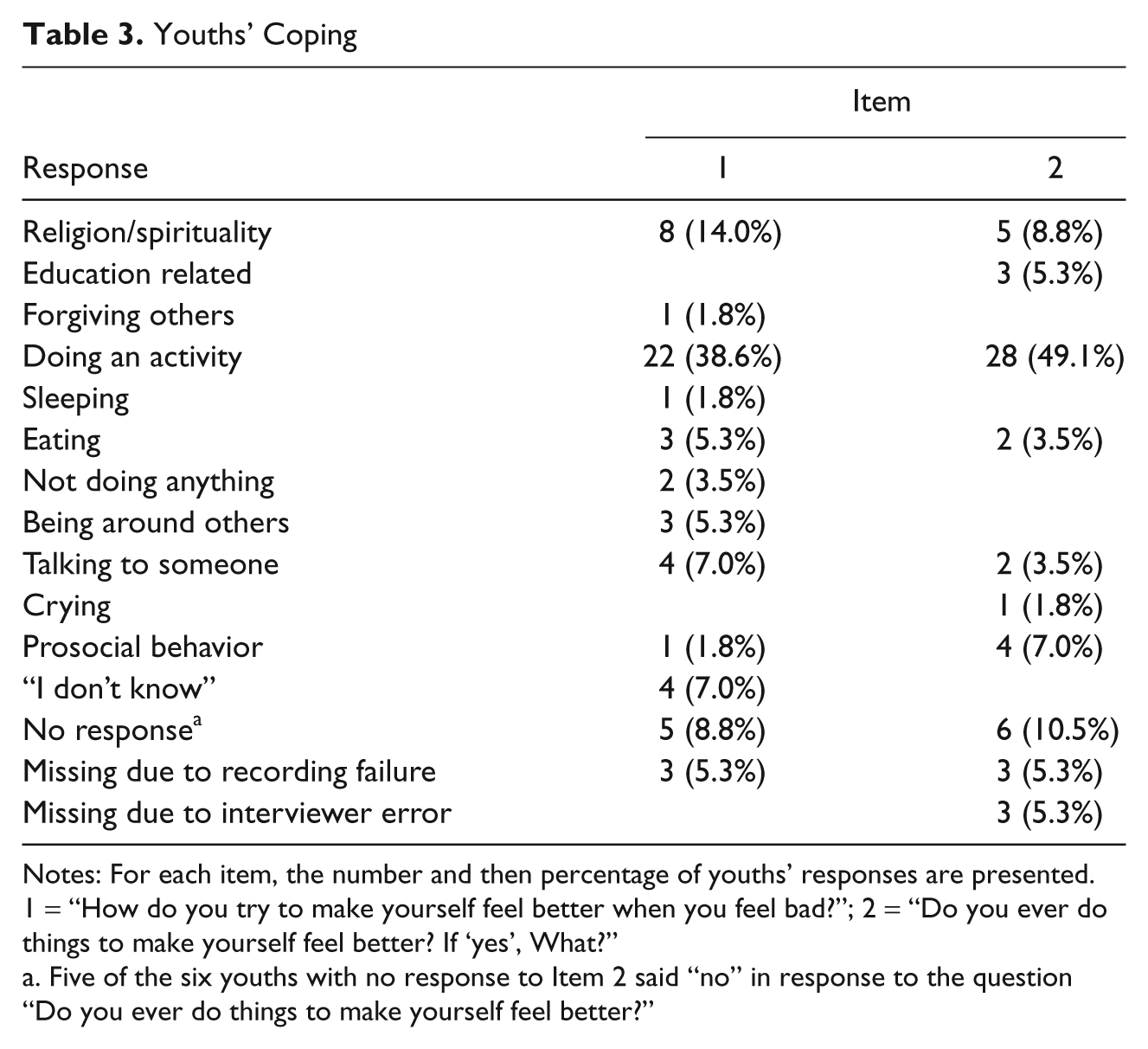
Notes: For each item, the number and then percentage of youths’ responses are presented. 1 = “How do you try to make yourself feel better when you feel bad?”; 2 = “Do you ever do things to make yourself feel better? If ‘yes’, What?”
Five of the six youths with no response to Item 2 said “no” in response to the question “Do you ever do things to make yourself feel better?”
For both questions, the most frequent responses were related to doing an activity (39% and 49%). Examples of activities included: “I can get a story book and begin reading” (14-year-old boy), “playing netball” (16-year-old girl), “I sing” (14-year-old girl), and “when someone abused me, I would go play football” (15-year-old boy). Another boy explained, “I feel bad because now I am not with my father. Anybody can abuse you and it makes you feel bad. Instead of being annoyed, I can go to my books and be happy” (9 years old).
For both coping questions, the second most frequent responses were related to religion/spirituality (14% and 9%). A girl answered, “I pray to God to help me” (15 years old). One boy said, “I pray with others and we share. We share God’s things and we go for fellowship with others . . . our brothers who are in the hospital or our brothers in imprisonment” (15 years old). He further explained, “When I get sad I just go and open my Bible and I read some verses where it tells us that if you’re sad you just go toward the Lord’s stilling arms.”
A variety of other types of responses were given by the rest of the children. For instance, youths described discussing their problems with others and being around others. Examples of these responses included: “If I can even begin to discuss it, I feel better” (9-year-old boy), and “I play with my friends, I talk” (19-year-old girl). Others mentioned that working or studying made them feel better, for example, “I study and if I get good marks, then I feel better” (15-year-old girl), and “If I have planted crops, I check on them” (11-year-old boy).
Hope
Participants were asked, “What gives you hope?” The most frequent three responses were education (33%), something religious (14%), and other people (12%; see Table 4). In terms of education-related responses, children often mentioned that having school fees gave them hope. Examples of this included: “When I’ve got school fees, it gives me hope” (13-year-old girl), “I have hope if I do well in my work at school, if I have the hope of passing my final exams, if I get school fees” (15-year-old girl), and, “My studies. I want to be a pilot” (16-year-old girl).
Youths’ Hope
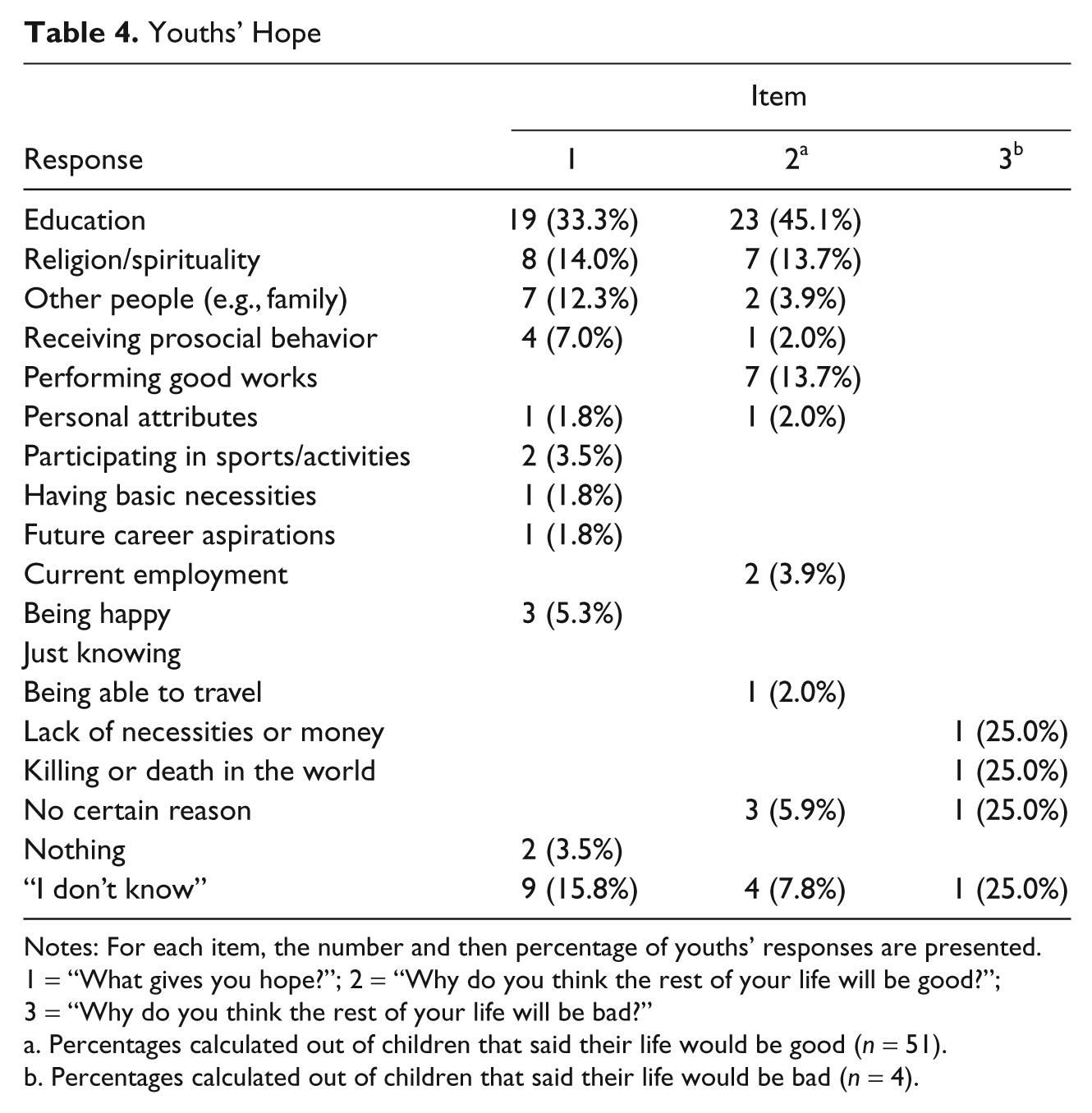
Notes: For each item, the number and then percentage of youths’ responses are presented. 1 = “What gives you hope?”; 2 = “Why do you think the rest of your life will be good?”; 3 = “Why do you think the rest of your life will be bad?”
Percentages calculated out of children that said their life would be good (n = 51).
Percentages calculated out of children that said their life would be bad (n = 4).
Responses related to religion/spirituality included the following: “When I’m reading my Bible, I get hope and I remember God exists” (9-year-old boy), “I have hope because I know God and God will make me have successes in the future” (14-year-old girl), and “Praying. If one doesn’t have faith, he doesn’t have any gain” (11-year-old girl). Another girl shared, “God. If I believe he will do everything. He is my strength” (19 years old).
When youths mentioned other people giving them hope, they mentioned friends, parents, and teachers. For instance, youths responded, “When I talk to my mum” (12-year-old girl), and, “When we [his friends] share . . . I’ll be happy and I get hope” (15-year-old boy).
Other answers regarding what gave them hope were given as well. A girl said, “If I go to work so hard! I hope to get money for a business in the future” (14 years old). A boy shared what gave him hope, “If somebody does for me good things” (11 years old).
Will the Rest of Your Life Be Bad or Good?
When participants were asked, “In general, do you think the rest of your life will be bad or good,” 51 (89%) replied, “good,” 4 (7%) replied, “bad,” and 2 (4%) did not respond. Depending on the response, he or she then was asked, “Why do you think the rest of your life will be good/bad?” Results are presented in Table 4.
The number of youths who reported the rest of their lives would be good was quite striking, particularly given the types of events they previously had encountered. For example, a 16-year-old girl described the loss of her family,
I was born in Tanzania. I lived there for 11 years with my dad. He brought me back to Uganda because this way was his birth country, but my mom was in Tanzania. I had brothers and sisters but they died. We were born, five of us, and four died. So I was left alone [She previously had discussed the death of her father]. I don’t know what actually killed them but eventually I thought it might be AIDS.
The same girl reported that the rest of her life would be good, “because I’m still studying. My education is good . . . also, my health and my family [she was living with her aunt]. The church tells me that.”
The top response for why life would be good was education/implications of education on employment (42%). For example, one boy said, “I’m studying and growing crops. I’ll be a farmer” (missing age data, but was in Primary School-4), and, “If I achieve my goals like my education. If I get something like a job, I can keep myself . . . then it will be good” (15-year-old boy). Another boy stated, “If I study, I can get a better future” (9 years old).
Religion/spirituality or previously performed good works were the second most given responses (both 14%). Religion-related responses included answers such as, “I know God will make my life good” (19-year-old girl), and “Because I have God in my heart” (14-year-old girl).
Previously performed good works entailed the notion that they had been good people who had done good things. For instance, a girl said, “I do good things to others. I go to church and I sing a praising song which can make people rejoice” (15 years old). Another girl stated, “Because I am a good child and give parents and other people respect” (11 years old).
A variety of other responses were given for why life would be good. For instance a girl said, “Because the work is hard, and there’s a lot of it” (9 years old), and a boy stated, “By giving respect and by being treated when I am sick” (11 years old).
Each participant who indicated life would be bad gave a different reason, including killing and lack of money (see Table 4). Examination of other data for these four cases indicated that each youth had experienced loss (e.g., death of father and four siblings, father was killed fighting with people over cows), abuse (e.g., repeated beatings), and/or lack of necessities (e.g., begging for food, having no money). Nonetheless, the histories of these children did not immensely differ from those reporting their lives would be good.
Discussion
The present study provides insight to Ugandan youths’ negative life events, adjustment, coping, social support, self-worth, and hope. Associations among negative life events, adjustment, and variables related to resilience often were as predicted, and qualitative data provided additional information regarding difficult life experiences, coping, and hope.
Negative Life Events
The first aim of the study was to describe youths’ negative life events. On average, youths experienced nearly half of the negative life events assessed. Qualitative data supported the idea that the events assessed encompassed those that youths described as being difficult.
There have been few studies conducted in Uganda to which these data may be compared. As an exception, Wakhweya et al. (2002) reported similar responses from Ugandan orphans and nonorphans. Their saddest experiences included death of parents, being mistreated/abused, being unable to attend school, and sickness (Wakhweya et al., 2002). Paardekooper, de Jong, and Hermanns (1999) interviewed children in northern Uganda. The percentages of youths reported to have experienced having an insufficient amount of food and not having access to medical care (58% and 36%, respectively) were somewhat similar to the present study (63% and 49%, respectively). In contrast, the percentage of children reported to have experienced sexual abuse (0%) greatly differed from the present study (39%). Parents reported children’s life events in Paardekooper et al.’s study, whereas youths self-reported life events in the present study. Parents may not have been aware of, or may have wanted to conceal, sexual abuse of their child.
In the present study, the majority of the youths indicated that a family member or friend had passed away. In interviews, children mentioning the death of a family member often stated that it was their father. They often discussed the changes occurring after their father’s death, for example, not having as much money or food. Some of them indicated they had to stop going to school after the death of a parent. In addition, about 40% of the youths said that they had been separated from one or both parents because the parent or the child moved. Youths indicated this was due to their parents separating, or the child leaving to attend school or to live with another relative when one parent passed away.
In addition, the majority of participants indicated that a family member, themselves, or a friend had experienced a serious medical problem. Furthermore, slightly less than half of the children said there was a time when their family could not get needed medicine. During the interviews, illnesses such as malaria, tuberculosis, and HIV/AIDS were mentioned.
On the basis of these findings, improving access to medical care and health education is important and could reduce the number of negative life events experienced. Efforts to address the health crisis have been made by the government and numerous organizations. Still, many health problems exist that can be decreased by improving access to clean water and mosquito nets.
About 26% of the participants said that they had been rejected by the community. This likely was due to being labeled an orphan or potentially due to their HIV status. In addition, the majority of youths indicated that someone physically hurt them. Physical punishment by parents and teachers is accepted in this area, but qualitative data indicated that it sometimes was quite distressing. About 39% of the participants said that someone had touched them where they did not want to be touched. We were surprised at the number of youths who reported abuse and the ease with which they spoke about rape and abuse. Raising awareness about the problem, although being careful not to stigmatize, is important. Teaching children that they do not need to endure abuse is necessary but may be a challenge. When this finding was discussed with members of the community who work with Ugandan youth, they thought abuse may be endured for acceptance and to secure shelter. In addition, sexual abuse sometimes occurs due to the false belief that intercourse with a child may prevent or cure HIV (Wakhweya et al., 2002).
The issue of child protection from abuse and exploitation has received attention from the government. One obstacle is birth registration, which serves as proof of age so that action may be taken against age-related exploitation. Efforts are being made to increase the number of birth registrations. Furthermore, Wakhweya et al. (2002) recommended that restoring the traditional way of interacting with one another in which child care is a village responsibility might minimize abuse. A feeling of community might prompt neighbors aware of abuse to intervene.
Education often was raised during the interviews. Nearly one third of the youths indicated that school sometimes was too difficult, but what seemed to be more distressing was when they could not attend (42% said there was a time when they could not attend). Not being able to go to school was the second most frequent response when asked about the most difficult time in their lives, and education was the number one reason children had hope and thought the rest of their lives would be good. Oleke et al.’s (2007) interviews of families caring for orphans in Uganda, as well as Betancourt et al.’s (2008) study of former child soldiers in Sierra Leone, produced similar findings. School may provide a sense of normalcy and self-worth, be a safe haven, encourage hope and goal setting (Betancourt et al., 2008), and provide employable skills for youths facing adversity.
Universal primary and secondary education have been implemented; however, youths must be able to afford a uniform. This keeps some children out of school. In discussions with teachers, it became apparent that hunger or illness hindered concentration for children who were present. Similar problems have been noted in other studies in Uganda (Oleke et al., 2007) and other developing countries (e.g., Kenya; Clark et al., 2008). Finding ways to eliminate absenteeism and maximize participation for students who are present at school is crucial.
One approach that may increase enrollment is the use of Child Development Accounts (CDAs). Curley, Ssewamala, and Han (2010) studied Ugandan, AIDS-orphaned 13-year-olds who received access to a CDA in which funds were matched at a rate of 2:1 (2 intervention funds:1 child’s family/child’s funds) or did not receive CDA access. Youths in the CDA group received mentorship with regard to financial and career planning. Children receiving the intervention saved money and also had better grades in school, positive change in educational plans, and confidence in their educational plans relative to control children at the follow-up.
Negative Life Events and Adjustment
The second aim of the study was to examine relations between negative life events and maladjustment. Although direction of causality cannot be determined, we expected experience of negative life events to be a risk factor for adjustment problems. As predicted, the number of negative life events experienced was positively related to internalizing (see Table 1) and near significantly positively related to externalizing when age was controlled. Negative life events and adjustment problems have been related in Western samples (e.g., Kim et al., 2003) and in northern Uganda (Amone-P’Olak et al., 2007). For example, death of a loved one and other events (e.g., sickness, being unable to pay school fees) have been identified as depression triggers for Ugandan youths (Verdeli et al., 2008).
Interrelations of Negative Life Events, Protective Factors, and Adjustment
The third aim of the present study was to explore youths’ coping and protective factors that may be related to resilience such as social support, self-worth, and hope. We also were interested in examining how negative life events related to these factors. As predicted, negative relations were found between the number of negative life events and social support or self-worth. The experience of negative life events might be expected to relate to social support in this manner, particularly because those events often entailed losing, or being separated from, a family member, hence reducing children’s social support systems. One reason that negative life events may have related to lower self-worth that has been discussed in the U.S. bereavement literature is that losing family may reduce the positive attention that children receive (e.g., Haine et al., 2003). In this sample, it is also possible that the stigmatization and rejection associated with many of the negative events, such as being an orphan and having an illness, reduced children’s self-worth. Negative life events did not relate to hope. It may be that children’s hope is influenced to a greater degree by dispositional factors (e.g., low neuroticism, control beliefs) or environmental factors other than negative events. Results suggested that social support may be one such factor.
Social support, self-worth, and hope were expected to be positively related with one another. Social support was positively related to children’s self-worth and hope, but self-worth did not relate to hope. Social support has been positively related to self-worth and hope in U.S. samples (e.g., Franco & Levitt, 1998; Warren, Jackson, & Sifers, 2009, respectively). Furthermore, social support has been found to contribute to overall well-being and relates to feelings of efficacy (see, for example, Cohen & Wills, 1985). It is likely that approval and positive feedback from others translates to approval of the self. Others providing support may offer ideas or tangible resources that aid in coping. Indeed, social support was positively related to coping in the present study. Others may assist youth in processing negative affect induced by life stressors by allowing “venting” or validating emotion or beliefs (see Kessler, Price, & Wortman, 1985).
In addition, each coping type was positively related to hope, which makes conceptual sense given that hope was operationalized as the perception of being able to initiate and sustain action toward a desired goal and achieve the goal. Youths who have efficacious beliefs and tendencies to take an action-oriented approach to goals might also be prone to take action with regard to coping with problems. In Western samples, avoidance has been found to relate to poorer outcomes (e.g., Compas & Reeslund, 2009), but perhaps due to the uncontrollable nature of many problems faced by the present sample, avoidance was positively related to hope.
We predicted that problem-focused, positive reframing, and support-seeking coping would be negatively related to internalizing and externalizing. Predictions were not made for avoidance. As expected, problem-focused coping was negatively related to externalizing. Avoidance and support-seeking coping were marginally, negatively related to externalizing, but only when age was not covaried. Coping was not related to internalizing. Furthermore, number of life events was unrelated to coping. Perhaps youths used strategies other than those assessed with the questionnaire, including some that are more or less adaptive, or relied more on their religion and spirituality. There was no evidence that secondary coping (positive reframing) was related to lower maladjustment.
Consistent with the Western resiliency literature (e.g., DuBois et al., 2002), social support was negatively related to externalizing (but only when age was covaried) and internalizing. Causality cannot be inferred, but teaching youths to rely on each other may foster adjustment.
Self-worth was negatively related to internalizing, but the relation with externalizing was not significant. Self-worth has been negatively related to internalizing and/or externalizing in the United States (e.g., Dubow et al., 1997). Children with internalizing symptoms may be prone to isolating themselves or retreating from others. It is possible that cutting off connections with others has a negative influence on children’s self-worth. However, perhaps high self-worth protects against internalizing. Steinhausen, Haslimeier, and Metzke (2007) found that self-esteem appeared to be both an antecedent and a consequence of depression from preadolescence to young adulthood.
Somewhat unexpectedly, hope was unrelated to externalizing and internalizing problems. In other samples, hope has been negatively related to internalizing and externalizing (Hagen et al., 2005) or internalizing but not externalizing (Valle et al., 2006). Negative relations previously have been attributed to hope promoting a mastery orientation or facilitating positive appraisals of situations. It is possible that hope may moderate the relation between negative events and adjustment problems, but the sample size precluded testing moderation in the present sample.
Descriptions of Coping, Optimism, and Hope
Open-ended questions were asked which likely tapped typical coping strategies. Youths often mentioned doing activities to cope, such as playing, singing, working, and reading. These may be classified as distraction strategies. The questionnaire measure of coping contained a Distraction subscale, but it was not used in analyses because of a low alpha. Likely contributing to the problem, many distraction items were omitted because they were not culturally appropriate.
Youths also mentioned religion and spirituality (e.g., going to church, praying). These strategies often highlighted getting comfort from God. Wood et al. (2006) reported religion-related responses from adolescents in Zimbabwe. The strategies mentioned for dealing with their parents’ deaths included asking for God’s help.
Many of the youths described unimaginable tragedies. Despite the events described, hope for the future was evident in youths’ responses. Nearly 90% of them said the rest of their lives would be good. The top reasons given for saying that it would be good were related to education, religion/spirituality, and previous performance of good works. Education and religion also were frequent responses when asked, “What gives you hope?” This hope may provide a basis for working with youth to improve their lives.
As a whole, results from youths’ open-ended reports of their most difficult events, coping, and what gives them hope were consistent with Cluver and Gardner’s (2007) interviews regarding AIDS-orphaned children in South Africa. Beliefs regarding factors influencing emotional/behavioral problems were assessed. Protective factors included supportive friends, school, and medical care. Risk factors included parental bereavement, physical/sexual abuse, family conflict, poverty, lack of medical care, and stigma/gossip (Cluver & Gardner, 2007).
Limitations and Future Directions
These data provided novel insight into relations among children’s life events, protective factors, and adjustment. In many cases, relations were consistent with expectations.
Limitations include the small sample (N = 57). This number limited what could be done statistically, and results from this sample may not generalize. The cross-sectional, correlational nature of these data limits interpretation. For example, adjustment problems may have influenced the occurrence of life events (e.g., externalizing may influence fighting in the family). A longitudinal study could provide information regarding processes of adjustment and reveal potential long-term effects related to negative life events (Worden & Silverman, 1996).
In addition, only children’s reports were collected. Collecting data from other informants would allow for assessment of multiple perspectives on the child. Reports of youths’ adjustment problems often vary across reporters (Achenbach, McConaughy, & Howell, 1987).
Furthermore, although the questionnaires were modified to be more culturally appropriate, these measures were not validated in Uganda. Future studies may benefit from the qualitative data in the present study. Developing and utilizing measures that assess Ugandans’ religiosity and spirituality, as well as forms of coping such as distraction may provide information regarding adjustment to life events.
There has not been much research conducted in Uganda with respect to psychosocial processes, although there is a growing body of research on the mental health and recovery of war-affected and displaced youths in northern Uganda (e.g., Betancourt, 2008; Bolton et al., 2007; Verdeli et al., 2008). Thus, there is much work to be done. In future work, investigators might use a larger, longitudinal data set to examine the effect of life events on adjustment. External resources, such as social support, as well as person-centered variables (e.g., attribution style, religiosity) may moderate or mediate the relation. Furthermore, positive life events have been related to better adjustment in Western samples (Rowlison & Felner, 1988). Determining the types of positive events Ugandan children experience (e.g., passing exams) and whether they predict adjustment may be interesting future directions.
Footnotes
Acknowledgements
We thank the following individuals whose passion for improving the welfare of children and wisdom regarding the children of Uganda inspired and informed this research: Tom Eggum, Rachel Eggum-Cinader, Elizabeth Flynn, Angie Simon, and Carla Crain. We express our gratitude to the employees of True Vine Team Ministries in Tororo, Uganda: Klephas Ojiambo, Nekesa Babra, Buluma Joshua Hajusus, Oketch Samuel, Ikibo Robert, and Obel Jessica. Without your dedication, recruitment of the sample and interpretation would not have been possible. Thank you for allowing us into your culture and space. We thank the volunteers who assisted with data collection: Stephanie Bender, Mary Bope, Kendra Byrd, Porshe Chambers, Kelsey Farrar, Kathee Gaskin, Sandra Goerdt, Brittnie Heuett, Cheryl Johnson, Christina Maurry, Ashley Merrell, Sandra Merrell, Kathleen Nelson, Kayleen Nelson, Kayla Osterwyk-Boogerd, Jennifer Radie, Sarah Roork, Elizabeth Schaffer, and Karen Schaffer. Thank you for your hard work and patience. We also express gratitude to the participants.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Nancy Eisenberg’s work on the manuscript was partially funded by a grant from NIMH.