
Abstract
The authors conduct afield experiment to investigate whether fears regarding the misleading effects of implied health claims, especially in educationally disadvantaged populations, are well founded. Results show that, regardless of educational attainment, consumers seem capable of evaluating the nutrition facts panel, even in the presence of a contradictory implied health claim.
A health claim “means any claim made on the label or in labeling of a food, including a dietary supplement that expressly or by implication … characterizes the relationship of any substance to a disease or health-related condition” (GPO 1998, p. 67). Permissible health claims are limited to the following: diet-disease relationships for which there is “significant scientific agreement”; foods that do not exceed disqualifying levels for total fat, saturated fat, cholesterol, and sodium; foods that contain a sufficiently high or low level of the substance that is the subject of the health claim; and foods with some minimal nutritional value (FDA 1993; GPO 1998, p. 67).
Proponents of restrictions on health claims have argued that permitting health claims by foods with any nutritional drawback invariably is misleading (Kessler 1989; Silverglade 1991). One concern is that though a particular health claim (e.g., prevents cancer) may be true with respect to one relevant attribute (e.g., high fiber), consumers may be misled to the extent that other relevant attributes (e.g., high saturated fat) contradict the health claim (Andrews, Netemeyer, and Burton 1998; FDA 1993). Another concern is that less well-educated consumers, who know and understand less about diet-disease relationships (Avis, McKinlay, and Smith 1990; Cotunga et al. 1992; Fullmer, Geiger, and Parent 1991; Ippolito and Mathios 1991) and use label information less effectively and less often (Bass 1991; Bender and Derby 1992; Moorman 1990; Wang, Fletcher, and Carley 1995), may be at particular risk (Alba and Hutchinson 1991; Alwitt and Doneley 1996; Preston 1994).
Opponents of these restrictions contend that health claims on food labels result in increased consumer awareness of diet-disease relationships (Calfee and Pappalardo 1991). They argue that, in effect, the FDA's regulatory efforts withhold useful information from consumers by substantially limiting health claims on food packages (Ippolito and Mathios 1993) and predict that the negative consequences of these rules will be felt disproportionately by educationally disadvantaged consumers. As evidence to support these arguments, they rely on studies in the ready-to-eat cereal market, which suggest that health claims likely played a major role in raising consumers’ awareness levels about the relationship between fiber and cancer (Ippolito and Mathios 1990a, 1990b, 1991). Moreover, the largest gains in knowledge and the most significant changes in behavior were found among consumers with low educational levels. Opponents of restrictions on health claims also argue that allowing health claims provides manufacturers with incentives to increase the levels of positive nutrients and/or decrease the levels of negative nutrients for new products. Research by Ippolito and Mathios (1989) and Moorman (1998) is consistent with this perspective.
The purpose of this study is to investigate whether fears regarding the potentially misleading effects of health claims raised by proponents of stringent restrictions are well founded. Specifically, this study examines (1) whether consumers are able to interpret nutritional information on a food product label when the label also features an implied health claim and (2) whether this ability to interpret nutritional information in the presence of an implied health claim differs for less versus more educated cohorts.
Research Issues
Interpretation of Nutrition Facts Panel in the Presence of an Implied Health Claim
Prior research has examined how various characteristics of nutrition information (e.g., format, content), as well as individual differences (e.g., personality characteristics, age, prior knowledge, motivation), affect acquisition, comprehension, and use of nutrition information (for comprehensive reviews, see Moorman 1996; Moorman and Matulich 1993; Russo and Leclerc 1991). In particular, in the course of designing the standard nutrition facts panel mandated by NLEA, the FDA evaluated the impact of several formats on product comparisons, verification of claims, estimates of servings needed to meet daily nutrient requirements, and balancing nutrients in a daily diet (Levy, Fein, and Schucker 1991, 1992, 1996). Although the formats differed significantly on each performance measure, the results of these studies generally indicate that most consumers are able to use nutrition information to complete these tasks successfully. What has yet to be evaluated, however, is how well consumers are able to interpret the NLEA nutrition facts panels and use the information in these disclosures in making judgments about product healthfulness. This study provides an opportunity to assess consumer interpretation of the nutrition facts panel mandated by the FDA.
More important, this study examines the effect of an implied health claim on consumer interpretation of the nutrition facts panel. That is, though consumers might be able to accurately interpret the nutrition facts panel presented alone, an implied health claim might bias the interpretation of these disclosures substantially and thereby influence product healthfulness judgments. To date, only two studies have examined the ability of consumers to interpret nutrition information in the presence of a health and/or nutrient-content claim (Ford et al. 1996; Keller et al. 1997). In Ford and colleagues’ study, consumers were able to interpret nutrition information presented in two different formats accurately, and health claims did not influence this ability. Participants in this study were undergraduate and graduate business students and, therefore, were likely to have been relatively homogeneous in education and nutrition knowledge.
The second study, by Keller and colleagues (1997), was conducted with a mail panel of adult consumers and thus likely provided a more representative sample of the adult population (e.g., the sample median age was 46 years, 73.5% of the sample were women, and all respondents were primary food shoppers for their households). The authors find that “consumers rely on the nutrition facts panel to a greater extent than they do on nutrition claims on the front of the panel” (Keller et al. 1997, p. 265).
In summary, the studies by Ford and colleagues (1996) and Keller and colleagues (1997) suggest that consumers are less likely to rely on a health or nutrient-content claim when the nutrition facts panel is available. However, because Keller and colleagues (1997) report no information about respondents’ education and Ford and colleagues (1996) use a highly educated sample, neither study provides insights into whether consumers’ ability to interpret the nutrition facts panel accurately in the context of a health claim varies with educational attainment.
Differences between Less and More Educated Consumers
Educational attainment has been found to be associated positively with health information acquisition and health-enhancing behaviors in contexts as varied as medical care, stress management, exercise, diet, alcohol consumption, and tobacco use (Moorman and Matulich 1993). With respect to diet, education is associated positively with diet and health knowledge, food label use and comprehension, competence in product comparison tasks, and dietary intake. Thus, less well-educated consumers know less about diet and disease relationships (Avis, McKinlay, and Smith 1990; Cotunga et al. 1992; Ippolito and Mathios 1991), exhibit lower comprehension of diet-disease messages (Fullmer, Geiger, and Parent 1991), and use nutrition labels less often and less well (Bass 1991; Bender and Derby 1992; Moorman 1990; Nayga, Lipinski, and Savur 1998; Wang, Fletcher, and Carley 1995).
In summary, prior research suggests that the ability to comprehend nutrition facts panels may vary significantly by education levels. Moreover, less educated consumers might have a greater likelihood of being misled by health claims (either explicit or implied) for foods with nutrition drawbacks. For these reasons, the FDA has identified the educationally disadvantaged as a segment of particular concern. However, no study has examined directly the possibility of differential processing of health claims and nutrition information by educationally disadvantaged versus educationally privileged consumers.
Hypotheses
The discussion in the preceding section highlights the polarity of views in the literature about whether consumer interpretation of nutrition information is influenced by an implied health claim and whether this effect is amplified for less educated consumers. The position espoused by opponents of restrictions on health claims is captured in the following hypotheses:
H1a: Consumer interpretation of nutrition information is not influenced by an implied health claim.
H2a: Neither less nor more educated consumers show any effect due to an implied health claim on their interpretation of nutrition information
In contrast, proponents of restrictions on health claims would posit the following hypotheses:
H1b: Consumer interpretation of nutrition information is influenced by an implied health claim.
H2b: Less educated consumers show a stronger effect due to an implied health claim on their interpretation of nutrition information.
The research described here investigates these competing hypotheses in a field study context.
Method
Sample
For the purposes of this study, educationally disadvantaged people are defined as those without a high school degree, and educationally privileged people are defined as those with a high school degree or more. Quotas were set for the educationally disadvantaged (50%) and educationally privileged (50%). Within each group, quotas were established for race (50% white, 50% non white), age (50% 18 to 34 years, 50% 35 to 64 years), and gender (50% male, 50% female). The rationale for setting quotas for these other demographic variables was to ensure that any results suggesting differences between the educationally disadvantaged and educationally privileged consumers held, regardless of race, age, or gender. 2
Although not of primary concern in this research, the study design also enabled us to examine whether factors such as age, race, and gender influence the interpretation of health claims and/or nutrition facts panels. A preponderance of evidence suggests an inverse relationship between age and use of nutrition information (Burton and Andrews 1996; Cole and Balasubramanian 1993; Mathios 1996; for exceptions, see Nayga 1997; Wang, Fletcher, and Carley 1995). Results pertaining to the relationship between race and nutrition information are equivocal (Nayga 1997; Wang, Fletcher, and Carley 1995), whereas research on gender suggests that women are more nutritionally conscious than are men (Bender and Derby 1992; Mathios 1996; Nayga 1997).
Thus, a 2 (without a high school education [<HS] or high school degree or more [>HS]) × 2 (white or nonwhite) × 2 (18–34 years or 35–64 years) × 2 (male or female) quota sample was recruited. Cell quotas were set at 25 for each of the resultant 16 cells. Four hundred ten participants were sampled from five U.S. cities: Edison, N.J.; Roanoke, Va.; Albany, Ga.; Kansas City, Mo.; and San Francisco, Calif. Forty-nine percent had not completed high school, 26% had attended college, 15% had completed an undergraduate program, and 7% had entered or completed a postgraduate program. Fifty-one percent of the sample were nonwhite, and of these, 92% were African-American. Fifty-one percent were men.
Product and Stimuli
Fronts and backs of packages for a fictitious brand of frozen dinner were created. The front of the package (i.e., front panel) was designed to simulate typical front panels found on a variety of actual frozen dinner brands, whereas the back of the package (i.e., back panel) was designed in accordance with the new FDA regulations (FDA 1993).
Two versions of the front panel, an implied health claim version and a no health claim version, were created. The implied health claim version made the explicit claim “does your heart good,” showed a picture of a heart, and showed a portion of a cardiogram to visually reinforce the claim (see Figure 1). The no health claim version made the claim “ultimate in cooking convenience,” showed a picture of a clock, and made the supporting claim “ready in minutes.”

Front Panel of Frozen Dinner Package: Health Claim Version
We should note that the health claim we used (“does your heart good”) is an implied claim, in that an explicit link between a nutrient and a disease or health-related condition is not provided. Because the label did not provide a reference statement to steer consumers to more information about the underlying diet-disease relationship, our implied health claim is not strictly in conformity with NLEA regulations (GPO 1998). We had two reasons for choosing an unqualified implied health claim. First, we were interested in examining the effects of less restrictive claims, which, though not in compliance with the NLEA, are being advocated by the opponents of the current regulations. Second, this health claim is the same as that used by Ford and colleagues (1996) and thus enables us to test the robustness of their findings and assess whether they extend to educationally disadvantaged consumers.
The back panel was modeled after the FDA-mandated nutrition facts panel. Four versions were created; these were identical in all respects except the amount of total fat, cholesterol, and sodium. Version 1 was high in total fat (30 grams [g]), cholesterol (150 milligrams [mg]), and sodium (1250 mg) (see Figure 2). Version 2 was low in total fat (6 g), cholesterol (20 mg), and sodium (240 mg). Version 3 was high in total fat (30 g) and cholesterol (150 mg) but low in sodium (240 mg). Version 4 was low in total fat (6 g) and cholesterol (20 mg) but high in sodium (1250 mg). In summary, two extreme versions (1 and 2) and two intermediate versions (3 and 4) were created. 3
FDA disqualifying levels for a meal product are 26 g of total fat, 120 mg of cholesterol, and 960 mg of sodium (FDA 1993).

Back Panel of Frozen Dinner Package: Version 1 (High Fat, Cholesterol, and Sodium)
Design
Respondents first were assigned to one of two groups on the basis of their education level (<HS versus ≥HS). Next, each group was assigned randomly to 1 of 14 conditions, thereby creating a total of 28 experimental cells. These 28 cells constituted the cells of three independent, completely crossed factorial designs.
The first design (hereafter referred to as Design 1) was a 2 (front panel: implied health claim versus no health claim) × 2 (education: <HS versus ≥HS) factorial in which respondents were exposed to the front panel only. The goal was to (1) establish and document the size of the implied health claim effect and (2) examine whether education moderates this implied health claim effect when the claim is presented alone. The second design (Design 2) was a 4 (back panel: Version 1, 2, 3, or 4) × 2 (education: <HS versus ≥HS) factorial in which respondents were exposed to the back panel only. In this case, the goal was to (1) establish and document the size of the nutrition facts panel effect and (2) examine whether education moderates this effect when the disclosure is presented alone.
The final design (Design 3) was 2 (front panel: implied health claim versus no health claim) × 4 (back panel: Version 1, 2, 3, or 4) × 2 (education: <HS versus ≥HS). In this design, respondents were exposed to one of the two versions of the front panel and one of the four versions of the back panel. The purpose was to assess whether education moderates the effects of an implied health claim and/or a nutrition facts panel when they are presented together.
Procedure
Participants were contacted at their homes by trained interviewers who were unaware of the purpose of the study. Participants were told that this “is a study to assess consumer perceptions of food packages.” In sequence, participants were exposed to the package front panel and/or the back panel, rated the product on several health-related dimensions, completed a short instrument designed to measure their nutrition knowledge, and provided demographic information.
Dependent Variables
Respondents rated the frozen dinner on several five-point rating scales. Key dependent measures were as follows: heart (1 = good for the heart, 5 = bad for the heart), fat (1 = low in fat, 5 = high in fat), cholesterol (1 = low in cholesterol, 5 = high in cholesterol), and sodium (1 = low in sodium, 5 = high in sodium) ratings.
Knowledge Measures
Consumer knowledge of dietary fats and cholesterol was assessed using nine questions taken from the Health and Diet Surveys conducted by the FDA and the National Heart, Lung and Blood Institute (NHLBI; for details, see Levy, Fein, and Stephenson 1993). This knowledge assessment was undertaken for two reasons. First, by using identical questions to those used in prior FDA/NHLBI studies, we were able ascertain the degree to which our sample was similar to the samples used in those studies. Second, it enabled us to confirm that knowledge levels varied as a function of educational attainment, as we would expect a priori (Ippolito and Mathios 1990a).
Results
Preliminary Analyses
In Table 1, we present responses to the nine knowledge measures from the present sample and the 1983, 1986, and 1988 FDA/NHLBI studies. Results show that our sample is comparable in knowledge of fat and cholesterol to the larger samples used in prior FDA/NHLBI Health and Diet Surveys.
In Table 1, we also display the percentage of correct responses for the nine knowledge measures broken down by level of educational attainment (<HS versus ≥HS). 4 T-tests comparing the two groups show that for five of the nine knowledge questions, a higher proportion of those with a high school education or more had correct responses relative to those without a high school degree. Thus, as expected, educational attainment was associated significantly with knowledge of dietary fats and cholesterol. 5
Percentages of Correct Responses to the Dietary Fat and Cholesterol Knowledge Questions

<HS = less than high school, ≥HS = high school or more.
Difference between <HS and ≥HS significant at p < .01.
Note: For each question, the correct answer is in italics.
Effects due to educational attainment on the processing of health claims and/or nutrition information are interesting only if the less and more educated groups also differ on relevant knowledge. Without knowledge differences, there is no reason to expect any education-based effects on processing of health information and no logical explanation for any effects that might be obtained.
We also compared the percentage of correct responses to the nine knowledge measures broken down by race (white versus nonwhite), gender (male versus female), and age (18–34 years versus 35–64 years). Results showed that whites performed significantly better than nonwhites on six of the nine measures (1, 2, 3, 4, 6, and 7), and older respondents performed better than younger respondents on four of the nine measures (1, 2, 7, and 9). There were no differences in performance between men and women on any of the measures.
Effects of an Implied Health Claim Alone (Design 1)
A 2 (implied health claim versus no health claim) × 2 (<HS versus ≥HS) between-subjects MANOVA was conducted with the heart, fat, cholesterol, and sodium ratings as the dependent variables. This was followed by separate ANOVAs for each of the four dependent measures. We present cell means in Table 2 and ANOVA results in Table 3.
Effects of Implied Health Claim Alone on Product Ratings: Cell Means and Standard Deviations

<HS = less than high school, ≥HS = high school or more.
Note: Standard deviations are in parentheses.
Effects of Implied Health Claim Alone on Product Ratings: ANOVA Results
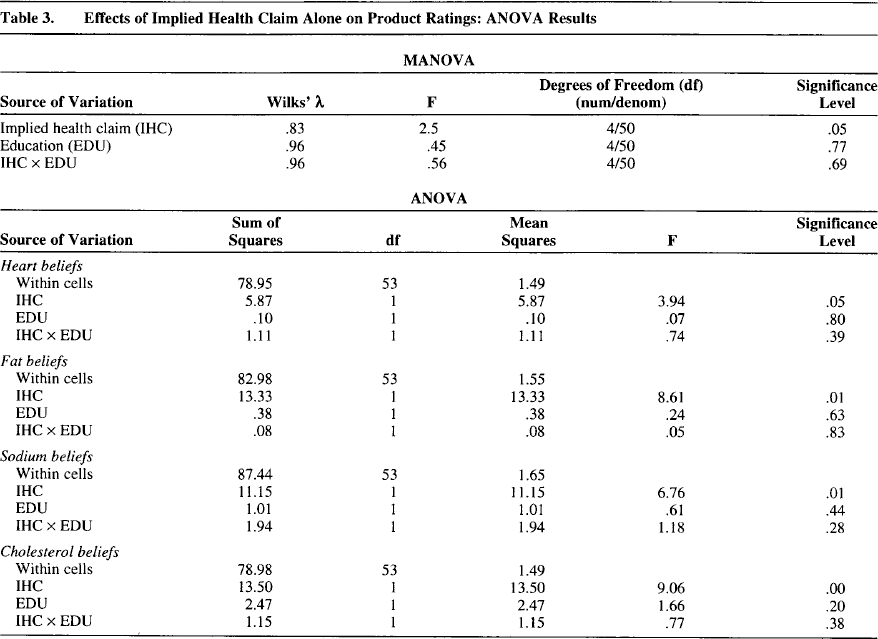
The MANOVA results showed that only the implied health claim effect approached significance (F(4,50) = 2.50, p < .06). The ANOVAs revealed a significant implied health claim effect for three of the four product ratings (heart rating: F(1,53) = 3.94, ω2 = .05, p < .052; fat rating: F(1, 53) = 8.60, ω2 = .12, p < .005; cholesterol rating: F(1,53) = 9.06, ω2 = .13, p < .004; sodium rating: F(1,53) = 6.76, ω2 = .09, p < .012). In each case, respondents rated the product more favorably when an implied health claim was present than when it was absent. In summary, the implied health claim influenced respondent perceptions of product healthfulness on several dimensions. Furthermore, this implied health claim effect was similar for the more educated as well as the less educated cohort. 6
We also ran 2 × 2 MANOVAs and ANOVAs and replaced the education factor with race (white versus nonwhite), gender (male versus female), and age (18–34 years versus 35–64 years). These analyses produced results similar to those obtained with education. That is, the implied health claim factor consistently influenced product ratings (significant in 14 of 16 ANOVAs). Neither gender nor age had any significant main effects, and there were virtually no significant two-way interactions. Somewhat surprising, race produced significant main effects on fat, sodium, and cholesterol ratings. In each case, whites rated the product as less nutritious than nonwhites did.
Effects of the Nutrition Facts Panel Alone (Design 2)
A 4 (four versions of the nutrition panel) × 2 (<HS versus ≥HS) between-subjects MANOVA was conducted with the heart, fat, cholesterol, and sodium ratings as the dependent variables. This was followed by separate ANOVAs for each of the four dependent measures. We present cell means in Table 4 and ANOVA results in Table 5.
Effects of Nutrition Facts Panel Alone on Product Ratings: Cell Means and Deviations

<HS = less than high school, ≥HS = high school or more.
Note: Standard deviations are in parentheses. Within each education level
(<HS and ≥HS), means that do not share a common superscript letter are significantly different at p < .05 using the Bonferroni test for post hoc comparisons. Note that these post hoc comparisons are underpowered because of the small cell sizes.
Effects of Nutrition Facts Panel Alone on Product Ratings: ANOVA Results
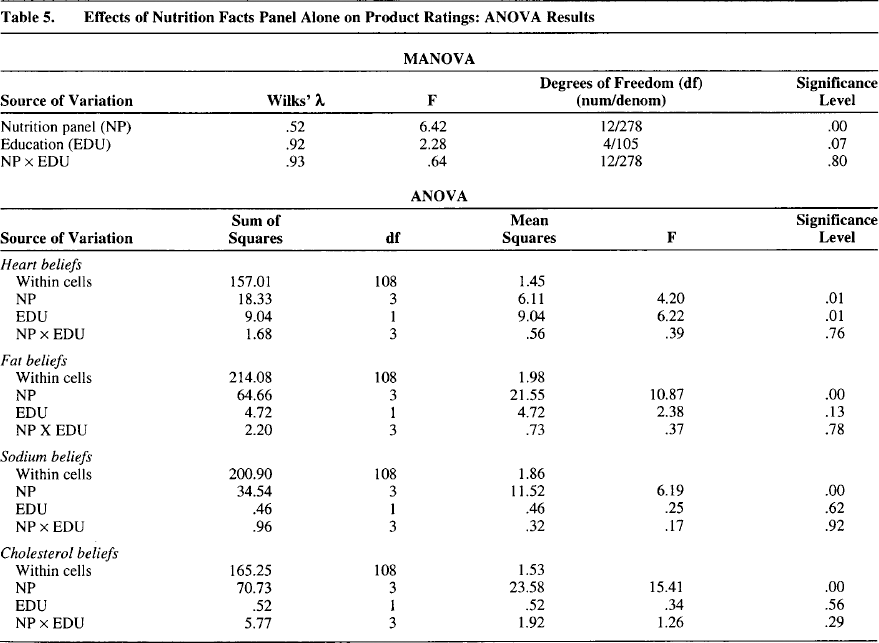
The MANOVA revealed only a significant effect due to the nutrition facts panel (F(12,278) = 6.42, p < .001). The ANOVAs revealed a significant nutrition facts panel effect for all four product ratings (heart rating: F(3,108) = 4.20, ω2 = .08, p < .007; fat rating: F(3, 108) = 10.87, ω2 = .20, p < .001; cholesterol rating: F(3,108) = 15.01, ω2 = .27, p < .001; sodium rating: F(3,108) = 6.19, ω2 = .12, p < .001). Respondents consistently rated the product as higher (lower) in fat, cholesterol, and/or sodium when the stated amount of these nutrients was actually high (low). Furthermore, respondents gave the best heart rating to the product described as low in fat, cholesterol, and sodium (m = 3.03), the worst heart rating to the product described as high in fat, cholesterol, and sodium (m = 3.96), and intermediate heart ratings to the two intermediate products (low fat, low cholesterol, high sodium: m = 3.04; high fat, high cholesterol, low sodium: m = 3.62).
In summary, the nutrition facts panel also influenced respondent perceptions of product healthfulness. Furthermore, these effects were similar for the more educated and the less educated cohort. 7
We also ran 4 × 2 MANOVAs and ANOVAs and replaced the education factor with race (white versus nonwhite), gender (male versus female), and age (18–34 years versus 35–64 years). These analyses produced results identical to those obtained with education. That is, the nutrition facts panel factor consistently influenced all product ratings (significant in 16 of 16 ANOVAs). Race, gender, and age did not have any significant main effects, and there were virtually no significant two-way interactions.
Effects of the Implied Health Claim and the Nutrition Facts Panel Presented Together (Design 3)
As evidenced in the analyses previously reported, both educated and less educated respondents were similarly influenced by the implied health claim and the nutrition facts panel when these informational items were presented alone. This section examines the effects of these factors when they are presented together and whether these effects are also independent of respondent education levels.
A 2 (implied health claim present versus absent) × 4 (four versions of the nutrition panel) × 2 (<HS versus ≥HS) between-subjects MANOVA was conducted with the heart, fat, cholesterol, and sodium ratings as the dependent variables. This was followed by separate ANOVAs. We present cell means in Table 6 and ANOVA results in Table 7.
Effects of an Implied Health Claim and Nutrition Facts Panel on Product Ratings: Cell Means and Standard Deviations

<HS = less than high school, ≥HS = high school or more.
Note: Standard deviations are in parentheses. Within each education level
(<HS and ≥HS), means that do not share a common superscript letter are significantly different at p < .05 using the Bonferroni test for post hoc comparisons. Note that these post hoc comparisons are underpowered because of the small cell sizes.
Effects of Implied Health Claim and Nutrition Facts Panel on Product Ratings: ANOVA Results
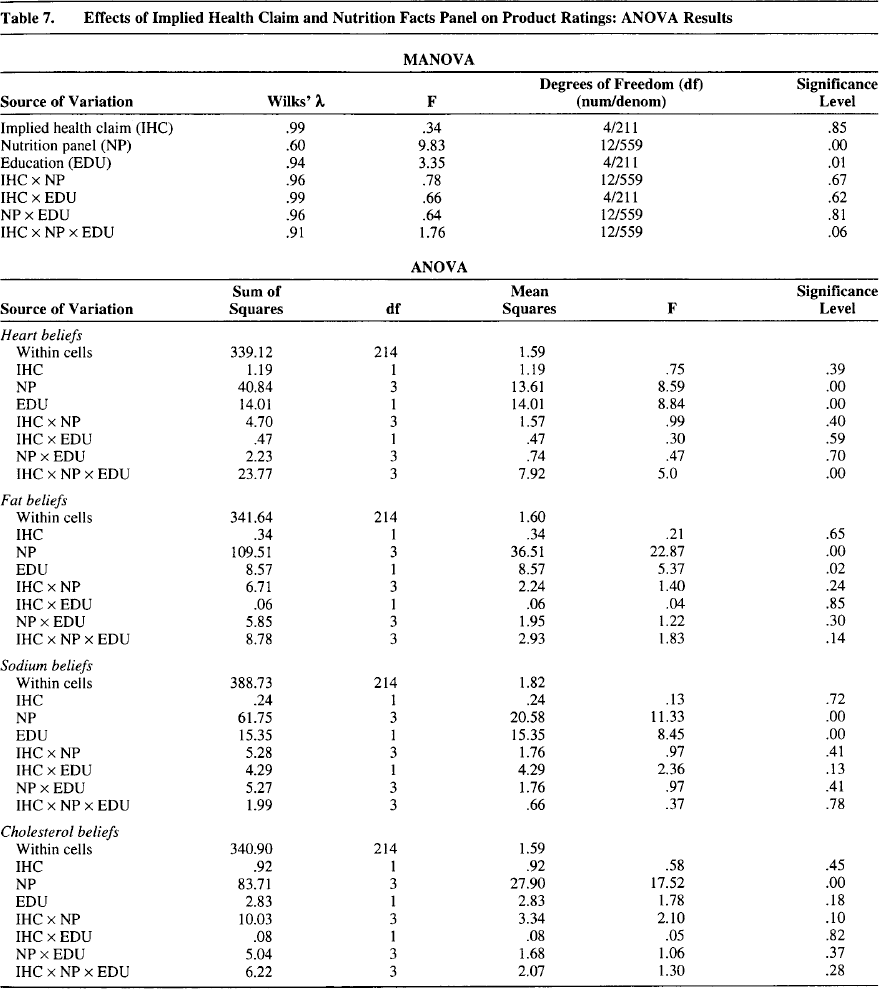
The MANOVA revealed significant effects due to the nutrition facts panel (F(12, 558) = 9.83, p < .001) and education (F(4,211) = 3.35, p < .02) but no effect due to the implied health claim and no two- or three-way interactions (p > .05 in all cases). The follow-up ANOVAs, which are described subsequently, produced results virtually parallel to these MANOVA results.
The follow-up ANOVAs revealed significant nutrition facts panel effects for all four product ratings (heart rating: F(3,214) = 8.60, ω2 = .08, p < .001; fat rating: F(3, 214) = 22.87, ω2 = .22, p < .001; cholesterol rating: F(3,214) = 17.52, ω2 = .18, p < .00; sodium rating: F(3,214) = 11.33, ω2 = .12, p < .001). Similar to the results obtained when the nutrition facts panel was presented alone, respondents consistently rated the product as higher (lower) in fat, cholesterol, and/or sodium when the stated amount of these nutrients was actually high (low). Also as previously, respondents gave the best heart rating to the product described as low in fat, cholesterol, and sodium (m = 2.6), the worst heart rating to the product described as high in fat, cholesterol, and sodium (m = 3.54), and intermediate heart ratings to the two intermediate products (low fat, low cholesterol, high sodium: m = 2.80; high fat, high cholesterol, low sodium: m = 3.48).
The education effect was significant for three of four ratings (heart rating: F(1,214) = 8.84, ω2 = .03, p < .003; fat rating: F(1,214) = 5.37, ω2 = .01, p < .021; cholesterol rating: F(1,214) = 1.78, p > .15; sodium rating: F(1,214) = 8.45, ω2 = .03, p < .004). Less educated respondents rated the product more favorably (heart rating: m = 2.86; fat rating: m = 2.76; cholesterol rating: m = 2.89; sodium rating: m = 3.14) than more educated respondents (heart rating: m = 3.34; fat rating: m = 3.12; cholesterol rating: m = 3.09; sodium rating: m = 3.66).
There were no effects due to the implied health claim factor for any of the four product ratings. Also, with one exception, there were no significant two- or three-way interactions. The exception was the three-way interaction for the heart rating (F(3,214) = 5.00, p < .002). Follow-up analyses suggest that this interaction was because more educated respondents gave significantly better heart ratings than did less educated respondents for products with intermediate levels of heart healthiness (i.e., Versions 3 and 4) when a convenience claim was made but not when an implied health claim was made. With this exception, it would appear that the ability of respondents to interpret the nutrition facts panel was unaffected by the implied health claim and did not vary by level of educational attainment. 8 In summary, our results provide support for H1a and H2a, which are consistent with the views of opponents of strict restrictions on health claims. The implications of these findings are explored in more detail in the next section.
We conducted 2 × 4 × 2 MANOVAs and ANOVAs and replaced the education factor with race (white versus nonwhite), gender (male versus female), and age (18–34 years versus 35–64 years). The results were similar to those obtained with education. That is, the nutrition facts panel factor consistently influenced all product ratings (significant in 16 of 16 ANOVAs). The implied health claim factor was not significant in any of the ANOVAs. Furthermore, race, gender, and age did not have any significant main effects, and there were virtually no significant two- or three-way interactions.
Discussion
Summary and Implications
The FDA's implementation of the NLEA has effected profound changes in the regulation of claims on food labels. Although the NLEA is designed, in part, to prevent deceptive or misleading claims on labels, Congress also noted that health claims can educate consumers and assist them in maintaining healthy dietary practices (ITC 1994). Because of the potentially beneficial effects of health claims on consumer knowledge and food choice behavior, it is important that the regulation of health claims not be overly stringent unless there is compelling evidence that consumers are being misled.
This research investigated whether, and the extent to which, one particular type of health claim (i.e., an implied health claim) may mislead consumers by biasing their ability to comprehend nutritional information on food labels accurately. The FDA's approach of not allowing implied health claims, such as that investigated here, would be justified if consumers were unable to interpret the nutrition facts panel accurately in the presence of such a claim. However, if implied health claims do not bias consumers’ ability to process the nutrition facts panel, the FDA's approach might warrant reconsideration. 9
Keller and colleagues (1997, p. 265) come to essentially the same conclusion when they state that “if such results are shown to extend to more realistic in-store purchase settings, this suggests that a less restrictive approach to front package nutrient claims may be preferable if the claim can be verified by the information in the nutrition facts panel, and is presented in a truthful and non-misleading manner.” Keller and colleagues (1997, p. 265) also note that their results “may not hold for all consumers or all claims that are allowed.”
Several of the findings of this study suggest that consumers are not misled by implied health claims. First, the nutrition facts panel significantly influenced all health-related product ratings. That is, respondents were able to comprehend fat, cholesterol, and sodium information correctly and could discern between high and low levels of these nutrients. Second, these nutrition facts panel effects were independent of the implied health claim used in the study. That is, the implied health claim did not bias the processing of the nutrition facts panel. Third, when both the implied health claim and the nutrition facts panel were available, only the nutrition facts panel influenced consumer perceptions of product healthfulness. Thus, the implied health claim seems to have been ignored in the presence of other, more diagnostic information. Fourth, this pattern of results was independent of respondent education levels. Both less and more educated cohorts demonstrated an ability to comprehend the nutrition facts panel, and this ability was largely unaffected by the implied health claim.
However, one of our results suggests that consumers are not completely immune to the influence of implied health claims. The implied health claim we used had a significant effect on three of four health-related ratings when it was presented alone (i.e., in the absence of the nutrition facts panel). Thus, to the extent that consumers ignore detailed nutrition information on food labels and rely solely on health claims (asserted or implied), they may make overly broad judgments about product healthfulness that might not be supported completely by the product's nutrition profile.
Overall, however, our results parallel those of Ford and colleagues (1996) and suggest that consumers are able to interpret the FDA-mandated nutrition facts panel, even in the presence of a contradictory implied health claim. We show that this pattern holds even for less educated consumers. This an important result because no study to date has investigated the differences between educationally disadvantaged and educationally privileged consumers in terms of their ability to process and comprehend health claims or nutrition information. The paucity of research on the educationally disadvantaged segment may be partly because this cohort is difficult to reach through traditional mall-intercept data collection techniques. We employed in-home personal interviews to ensure adequate representation of this group in our sample. 10
We should emphasize that our data do not suggest that consumers can interpret the nutrition facts panel with complete accuracy. For example, an examination of Table 4 reveals that, when presented with the nutrition facts panel alone, consumers consistently rated the sodium content of the product at or above the midpoint of the five-point rating scale, even when actual levels of sodium were low. In contrast, ratings for fat and cholesterol show greater sensitivity to variations in actual levels of those nutrients. Our finding that respondents may have a tendency to overestimate the sodium content in a product is consistent with preceding literature. However, the data in Table 4 show a significant main effect of the nutrition facts panel factor on sodium ratings but no significant interaction with education. Thus, the most logical interpretation is that respondents were able evaluate sodium information to a degree, and their ability to do so largely was unaffected by education levels.
Although not the focal point of our research, this study also showed that the ability to process nutrition information in the presence of an implied health claim is independent of other demographic variables such as race, age, and gender.
Our finding that there are no differences between the educationally disadvantaged and educationally privileged consumers in their ability to process nutrition information is somewhat surprising in light of previous research (discussed previously), which suggests a positive association between education and health knowledge, food label use, and dietary intake. In this study, less educated respondents displayed lower levels of nutrition knowledge (see Table 1) but did not differ from the more educated cohort in their ability to interpret the nutrition facts panel.
One possible explanation is that the FDA-mandated disclosures present nutrition information in a manner that is easily interpretable, even by consumers with relatively lower levels of educational attainment. Another possible explanation is that consumers are already familiar with a heart health claim that involves the relationships between heart disease and fat, sodium, and cholesterol.
It also could be argued that though the less and more educated cohorts differed in nutrition knowledge in our study, the differences were modest in absolute terms. Furthermore, we must note that our knowledge measure did not include a question on sodium, which was a target belief in our study. It is possible that a more precise measure of nutrition knowledge may have revealed subtle differences in information processing that are not evident in our comparisons involving less versus more educated cohorts. More research is needed to understand better the relationships among educational attainment, nutrition knowledge, and ability to comprehend health claims and nutrition facts panels.
Limitations and Further Research
Several aspects of the study limit the generalizability of our findings. For example, we focused on a single health claim (heart health claim) that involves nutrients that may be familiar to consumers. It is unclear whether our results would hold for unfamiliar health claims such as folate and neural tube defects (GPO 1998) or soluble fiber from psyllium husks and coronary heart disease (GPO 1998). Would consumers pay more attention to an unfamiliar claim because of its novelty, or would they tend to give less weight to it because they are unable to comprehend its implications? These are important issues to be addressed in further research.
In addition, we used an implied health claim that is not strictly in conformity with NLEA regulations. Although the use of such a claim was justified because of the objectives of our study, we acknowledge that our findings may not generalize to claims that provide more complete information on diet-disease relationships. More research is needed in this area.
Furthermore, respondents were exposed to the front and back panel information in sequence. Our rationale for using this approach was to enhance ecological validity. Consumers in a store environment are likely to look at the front panel of a package before turning it around to examine the detailed nutrition facts panels. We also should note that, after respondents had been exposed to the front and back panel in sequence, they provided product ratings with both panels in front of them. Thus, we do not believe that recency effects pose a problem in this study. However, additional research that examines the effects of presentation order is needed to establish the robustness of our findings.
Finally, our study used black-and-white copies of the front and back panels of a fictitious frozen dinner product. It is not known how consumers actually evaluate product healthfulness with real product packages. One possibility is that consumers may choose to rely solely on a health claim and bypass the nutrition facts panel completely. Sole reliance on a health claim might produce unwarranted inferences on related and unrelated attributes uncorrected by the nutrition facts panel. Further research is necessary to explore the ways in which health claims (asserted and implied) are used by consumers in everyday decision situations.