
Abstract
This study evaluated a model linking internalization and dieting behaviors in a sample (n = 499) of Latina/o and White college students. Analyses revealed that the scales were invariant across ethnic and gender groups and generally supported the invariance of the proposed model across these groups. Analyses also revealed no ethnic mean differences between the constructs, but females did score higher than males on most constructs.
The National Eating Disorders Association (NEDA; 2010) estimates that there are currently approximately 10 million women and 1 million men suffering from eating disorders. Furthermore, a nationwide college poll revealed that nearly one fifth (20%) of female and male college students of various ethnicities have admitted to having an eating disorder, whereas more than four of five (80%) of the polled students were dieting (NEDA, 2006). With an increasing number of individuals experiencing body image dissatisfaction and eating disorder symptoms, researchers have focused on developing theoretical frameworks to understand the processes that link body image dissatisfaction to disordered eating. However, only a limited number of studies have examined these theoretical models across various populations (e.g., gender, ethnicity, age) to test for moderation effects and model generalizability.
Although researchers acknowledge that potential differences may be present with racial and ethnic minorities in relation to objectification theory, only recently has ethnicity been considered in objectification theory research. A review of literature revealed that a limited number of studies (Buchanan, Fischer, Tokar, & Yoder, 2008; Hebl, King, & Lin, 2004; Mitchell & Mazzeo, 2009) have examined the applicability of objectification theory or its constructs to ethnic minorities. As explained by Moradi (2010), “Reliance on andocentric and Eurocentric cultural field, journal, or other local conventions led to the exclusion of women and people of color from much of the pioneering work in psychology” (p. 142).
Overall little research and theoretical models exist related to the body image and dieting experiences of minority individuals (Chen & Russo, 2010; Moradi, 2010; Moradi & Huang, 2008; Tylka & Hill, 2004). Similarly, only until recently has research on body image and eating disorders included men’s experiences (Hallsworth, Wade, & Tiggemann, 2005). Although objectification theory was initially developed to explain sexual objectification and its effects on women, a limited number of studies have attested its applicability to boys and men (Hallsworth et al., 2005; Slater & Tiggemann, 2010; Tiggemann & Kuring, 2004), subgroups of men (e.g., bodybuilders and weightlifters; Hallsworth et al., 2005), and men’s increased concern with their physical appearance (Pope, Olivardia, Borowiecki, & Cohane, 2001).
Although objectification theory was developed to capture women’s experiences related to sexual objectification, there is increased evidence of men experiencing objectification (Tiggemann & Kuring, 2004). The question remains whether these experiences differ across ethnic groups. The present study aims to partially address these gaps in the literature.
In an effort to address gaps in the literature related to body image and dieting behaviors in minority individuals and men, it is necessary to use frameworks and models sensitive to the experiences of these groups. Likewise, it is vital to examine the role of moderators, such as ethnicity and gender, as the relationships between constructs may vary based on group membership. More specifically, this study is focused on dieting behaviors and body image concerns in Latina/o and White male and female college students.
This study may highlight the impact of cultural differences from a different perspective and address gaps in the literature by examining the relationships between some of the objectification theory constructs, including dieting behaviors. This study was built off research and constructs associated with objectification theory and tested whether a theoretical model was structurally invariant (i.e., the relationship between constructs was equal across groups) across gender and ethnicity and if mean differences emerged.
Introduction to Objectification Theory
Objectification theory, developed by Fredrickson and Roberts (1997), is described as a leading force in the field and is one of the more researched frameworks in understanding body image and eating disorders (Moradi, 2010; Moradi & Huang, 2008). Objectification theory tenets are represented in the research literature through various models. Although the majority of the models have similar variables and sequential links, there are several variations. These revised models expand on the original theory by adding variables such as internalization (Mitchell & Mazzeo, 2009; Moradi, 2010). Other variations of the original objectification theory model tested new variables in minority populations, including drive for muscularity in men (Hallsworth et al., 2005) and skin tone dissatisfaction in African American women (Buchanan et al., 2008). Unfortunately, much of the research using the original and modified models remained focused mostly on White females.
Current Study’s Model
The current study evaluated the relationship between internalization and dieting behaviors, with the following mediators: body surveillance, body shame, and body image dysphoria (see Figure 1). Although most variables (i.e., body surveillance, body shame, and dieting behaviors) are associated with constructs found in objectification theory (Fredrickson & Roberts, 1997), in this study internalization was added to determine whether it preceded body surveillance as suggested by previous literature (Moradi, 2010; Moradi & Huang, 2008). Overall, the proposed links were supported by prior research, including that by Mitchell and Mazzeo (2009), who indicated that internalization, body surveillance, and body shame were all directly or indirectly related to disordered eating. To determine the model’s generalizability, this study also explored whether the model was invariant across gender and ethnicity (White vs. Latina/o). Although this exact model had not been tested to date, the literature below provided support for its validity.
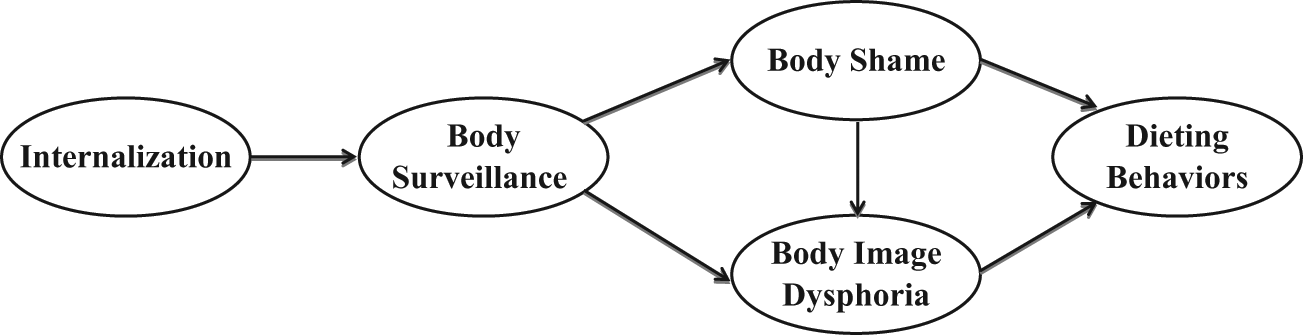
Proposed theoretical model of objectification theory.
Internalization
Internalization of societal pressures may be a key contributor to body dissatisfaction and eating disturbance (Heinberg, Thompson, & Stormer, 1995). Internalization may be defined as “awareness of societal pressure to be thin and attractive as well as internalization of these standards” (Mitchell & Mazzeo, 2009, p. 387). Internalization of the sociocultural standards of beauty has recently been included with the objectification theory constructs (Moradi, Dirks, & Matteson, 2005; Mitchell & Mazzeo, 2009). Although historically internalization has been omitted from objectification theory research, Moradi and Huang (2008) and Moradi (2010) recommended that it be incorporated in gender and ethnicity body image research.
According to Moradi et al. (2005), internalization was significantly related to body surveillance and body shame. In addition, body shame partially mediated the relationship between internalization and eating disorders symptomatology. Mitchell and Mazzeo (2009) indicated that internalization was correlated with disordered eating. Together, this research proposes that internalization was a precursor to dieting behaviors.
Body surveillance
Body surveillance has been examined as a manifestation of self-objectification and is defined as “the act of consistently measuring oneself against some internalized or cultural standard” (Moradi et al., 2005, p. 421). Although the term body surveillance is used in this study, previous research has also referred to it as self-surveillance and body monitoring. Fredrickson and Roberts (1997) asserted that habitual body surveillance could be a source of recurring and problematic shame in women, particularly in societies where women’s bodies are sexually objectified. As a result, body surveillance was a predictor of body shame (Moradi & Huang, 2008). Most studies have supported the link between self-objectification and body shame, including studies comparing men and women (Tiggemann & Kuring, 2004) and women of color (Buchanan et al., 2008; Mitchell & Mazzeo, 2009).
Body shame
McKinley and Hyde (1996) defined body shame as the negative feeling that arises when cultural body standards are not met. Body shame results when an individual believes that his or her appearance is unacceptable to others (Breitkopf, Littleton, & Berenson, 2007). Body shame may have psychologically damaging consequences and has been found to be associated with eating disordered behaviors (Denious, Russo, & Rubin, 2004) and a precursor to negative affect (Hallsworth et al., 2005) surrounding body image. In recent studies, body shame predicted disordered eating in samples of adolescent boys and girls (Slater & Tiggemann, 2010) and college men and women (Chen & Russo, 2010).
Body image dysphoria
Body image dysphoria was defined as “the person’s negative body image emotions” (Cash, 2002, p. 363). Rather than measuring depression as a broad construct, body image dysphoria measures negative emotions arising specifically in the context of situations influencing body image. The association of body image dysphoria and other negative affect constructs is evidenced by the high correlation found between body image dysphoria and both measures of depression and social anxiety (Cash, 2002). Many of the specific situational prompts described in the Situational Inventory of Body Image Dysphoria (Cash, 2002) could be considered triggers for sexual objectification and self-objectification, which are consistent with Fredrickson and Roberts’s (1997) criteria.
Research suggested that depression might be a consequence of objectification and self-objectification, particularly in women (Fredrickson & Robert, 1997; Moradi & Huang, 2008). Other studies have investigated specifically the role of depressed mood within the objectification theory framework (Chen & Russo, 2010; Hallsworth et al., 2005; Tiggemann & Kuring, 2004).
Of those, some reported gender differences in the pathways connecting body surveillance and depressed mood (Tiggemann & Kuring, 2004), specifically highlighting that depressed mood is a better predictor of eating disorders for women than for men. Tiggemann and Kuring’s (2004) study found that body shame and appearance anxiety predict both eating disorders and depression for women; however, it was not predicted for men. Other studies supported that body shame was a predictor of depression, bulimia, and drive for muscularity in men (Hallsworth et al., 2005).
Dieting behaviors
Fredrickson and Roberts (1997) proposed that body surveillance contributed to women’s eating disorders. Most of the aforementioned research identified disordered eating or eating disorders as the primary outcomes across different populations, including women (Mitchell & Mazzeo, 2009; Moradi et al., 2005; Noll & Fredrickson, 1998; Wood & Petrie, 2010), women of different ages (Augustus-Horvath & Tylka, 2009), men (Tiggemann & Kuring, 2004), and sexual minority men (Wiseman & Moradi, 2010). For this study, the Eating Attitudes Test (EAT-26; Garner, Olmsted, Bohr, & Garfinkel, 1982) was used to measure dieting and disordered eating patterns in male and female college students.
Research Purpose
Our primary objective was to incorporate the recommendations made by previous researchers (Moradi, 2010; Moradi & Huang, 2008) in an effort to better understand the relationships between the objectification theory constructs as they pertained to Latina/o and White female and male college students. The following were the goals for this study: (a) determine whether the psychometric properties were adequate and equal (i.e., factorial validity, measurement invariance, and equal reliability) across gender and ethnic groups (Goal A), (b) compare the latent factor mean scores across gender and ethnicity (Goal B), and (c) test the proposed model connected to objectification theory (Goal C; see Figure 1) and investigate whether the structural coefficients are equal across gender and ethnicity. The answers to the above-mentioned goals may help fill the existing gaps in the objectification theory literature related to gender and ethnicity.
As illustrated above, empirical support for our model exists (see Figure 1); however, the degree to which this model generalized to Latina/o and White male and female college students warranted further examination. Again, this study aimed to address existing gaps in the literature by testing whether the structural coefficients (i.e., relationship between constructs/latent factors) were equal across gender and two ethnic groups and, therefore, whether this model generalized across these groups. To complement these results, the present study also tested the equality of the factor loading (item metric), thresholds (item scalar), and internal consistency reliability coefficients across these groups, which is a statistical assumption to compare structural coefficients and mean scores. Continued exploration of theoretical models, along with information related to measurement and mean differences, may enhance the understanding of body image and eating disorders in various ethnic groups and both genders. Data gathered from these studies may then be useful in the prevention and treatment of eating disorders in Latina/os, as well as White women and men (Chen & Russo, 2010; Moradi, 2010; Moradi & Huang, 2008).
Hypotheses
Confirmatory factor analysis (CFA) and structural equation modeling (SEM) hypotheses using the full sample
Based on the measurement model’s (i.e., CFA model) complexity, we hypothesized that minor modifications would be required to produce a good fitting measurement model and strong factorial validity. However, these changes were expected to be rather minor based on the previous validation research using these scales, even though to our knowledge these scales have never been evaluated simultaneously. In terms of the structural model, we hypothesized that the theoretical model (see Figure 1) would fit the data well and produce large structural coefficients based on previous research. In particular, we theorized that internalization would be the driving factor in the model and significantly would predict body surveillance, which in turn would predict body shame and body image dysphoria. Body shame and body image dysphoria were then expected to predict dieting behaviors, which implies these two variables mediate the relationship between body surveillance and dieting behaviors.
Measurement invariance hypotheses across ethnic and gender groups
Because of the lack of research testing for measurement invariance across these groups, we hypothesized null finding (i.e., invariant measurement models) across ethnic and gender groups. It could be argued that Latina/os or males may respond differently (i.e., have different metric and scalar parameters) to these items because of cultural or internalization factors; however, we had no empirical evidence to suggest differently.
Mean difference hypotheses across ethnic and gender groups
Specific cultural factors that contribute to the individual experiences of Latina/os include skin color, body type, gender role expectations, double cultural standards, and other specific interactions, such as racism, discrimination, and sexual-objectification (Boie, 2012). Based on this research, we expected that these cultural factors may increase the internalization of societal standards, body shame, body image dysphoria, and disordered eating, thus resulting in mean differences across White and Latina/o subjects.
Gender difference studies found that compared to boys/men, girls/women displayed higher degrees (i.e., higher means) of body surveillance, body shame, appearance anxiety, and disordered eating (Slater & Tiggemann, 2010; Tiggemann & Kuring, 2004). Particularly, when focused on adolescents, girls reported higher scores on self-objectification, self- surveillance, body shame, anxiety, and disordered eating (Slater & Tiggemann, 2010). Similarly, the results from Hebl et al. (2004) indicated that women overall reported higher body image dissatisfaction and body shame than men. Consistent with extant literature, we hypothesized that women’s mean scores on internalization, body shame, body surveillance, body image dysphoria, and dieting behaviors would be higher than those of men.
Structural invariance hypotheses across ethnic and gender groups
Hebl et al. (2004) concluded that when exposed to the same situations, Hispanic (in our study Latina/o) individuals would be as vulnerable to self-objectification and would experience similar negative consequences as Caucasian women. Despite hypothesized mean differences across the groups, we expected that Latina/os would also be susceptible to self-objectification and the relationships between variables would not differ (i.e., be invariant) across these ethnic groups.
Similar to ethnicity, despite having mean differences across gender groups we did not anticipate these differences to influence the relationship between variables. In other words, even though we recognized that there were specific cultural and gender-related factors that may contribute to individual experiences, we expected to find that the processes related to dieting behaviors would be similar or invariant across groups. If the model failed to be invariant across groups that would imply that the relationships between variables differed across groups, which is of importance for both clinicians and researchers.
Method
Participants
Data were collected from 510 undergraduate students at a large Hispanic-serving institution in the Southwest United States. From those, 11 participants were removed because they consistently circled the same response option or were missing all survey data. Participants included 200 males and 299 females with a mean age of 21.67 years (SD = 5.47). Most participants identified as Hispanic/Latina/o (n = 85, 17.03%), Mexican American (n = 114, 22.85%), or White (n = 153, 30.66%). The remainder of the participants self-identified as Asian American (n = 29, 5.81%), African American (n = 26, 5.21%), American Indian (n = 1, 0.20%), Mixed (n = 62, 12.42%), and “Other” ethnicity (n = 29, 5.81%). Note that only White and Latina/o participants were used for the ethnicity analyses, whereas the entire sample was used for gender analyses. The Hispanic/Latina/o and Mexican American participants were combined (hereafter referred to as Latina/o) to allow an appropriate sample size for statistical analyses.
The participants reported that, when growing up, the typical family household income was as follows: $18,810 or less (n = 43, 8.62%), $18,810 to $30,000 (n = 76, 15.23%), $30,000 to $60,000 (n = 134, 26.85%), $60,000 to $100,000 (n = 142, 28.46%), and more than $100,000 (n = 80, 16.03%). The remainder of the data (n = 24, 4.81%) were missing. A slightly larger percentage of participants were Freshmen (n = 159, 31.86%), with a relatively equal distribution across Sophomores (n = 106, 21.24%), Juniors (n = 117, 23.45%), and Seniors (n = 106, 21.24%). A small percentage were graduate students (n = 4, 0.80%) or omitted this information (n = 7, 1.40%).
Of the 483 participants who reported both height and weight, their body mass index (BMI) ranged from 14.67 to 51.49 (M = 24.55, SD = 5.23). The BMI means and standard deviations for each ethnic group were as follows: Asian (M = 22.60, SD = 3.83), Black (M = 24.81, SD = 7.46), Latina/o (M = 25.67, SD = 4.82), Mexican American (M = 25.75, SD = 5.92), White (M = 24.54, SD = 4.36), Mixed (M = 24.77, SD = 5.46), and Other (M = 22.77, SD = 3.35). Females (M = 24.20, SD = 5.60) and males (M = 24.95, SD = 4.44) had comparable scores.
To explore group BMI differences, a 2 × 6 (gender by ethnicity) factorial analysis of variance (ANOVA) was conducted. The overall ANOVA was statistically significant, F(11, 470) = 2.95, p = .001, η2 = .07, although only the ethnicity variable revealed any group difference, F(5, 470) = 4.65, p < .001, η2 = .05. Using Bonferroni post hoc tests, analyses indicated that Latina/os (L) scored significantly higher than Asian (A) (M A = 22.64 vs. M L = 25.74, p = .044) and White (W) (M W = 23.52 vs. M L = 25.74, p = .044) students on BMI. No statistically significant gender, F(1, 470) = 2.06, p = .152, η2 ≈ .00, or ethnicity by gender interaction, F(5, 470) = 0.99, p = .426, η2 = .01, emerged.
Procedure
To represent the university population, instructors across various disciplines were emailed about 2 months before data collection to request the participation of their students. Of those instructors who granted access to their class, eight undergraduate classes were sampled. Class disciplines surveyed included Anthropology (n = 119), Bilingual Bicultural Studies (n = 78), Criminal Justice (n = 81), Education (n = 98), and History (n = 134). Participants were administered a questionnaire that required approximately 20 to 25 minutes of class-time to complete. The procedures included providing participants with a brief description of the study and a copy of the informed consent. Participation in this study was voluntary. The overall response rate of useable data was 88%. The university’s institutional review board approved the research protocol.
Measures
Internalization
The Sociocultural Attitudes Towards Appearance Questionnaire (SATAQ-3; Heinberg et al., 1995) was used to assess awareness and internalization of Western socially sanctioned standards regarding appearance, particularly the thin ideal. The SATAQ-3 is a 30-item scale, with the following four subscales: Internalization-General, Internalization-Athlete, Pressures, and Information. The responses ranged from 1 (definitely disagree) to 5 (definitely Agree). Heinberg et al. (1995) reported high internal consistently reliability coefficients (i.e., coefficient alphas) for Internalization-General (α = .92), Information (α = .94), Pressures (α = .94), and Internalization-Athlete (α = .89). This study only used Internalization-General, composed of nine items (e.g., “I would like my body to look like the models who appear in magazines”), because it is the only one that fits well within the objectification theory (Moradi, 2010). In determining the validity of the SATAQ-3, a significant main effect for Internalization in the samples containing individuals with eating disturbed and eating disordered compared to the control subjects (Thompson, van den Berg, Roehrig, Guarda, & Heinberg, 2004). Our analyses indicated acceptable internal consistency reliability estimates across the various groups explored (see Table 1) and provided strong evidence of construct validity based on the CFA results below.
Internal Consistency (Coefficient Alphas) Reliability Estimates for the Total Sample and Each Subsample.
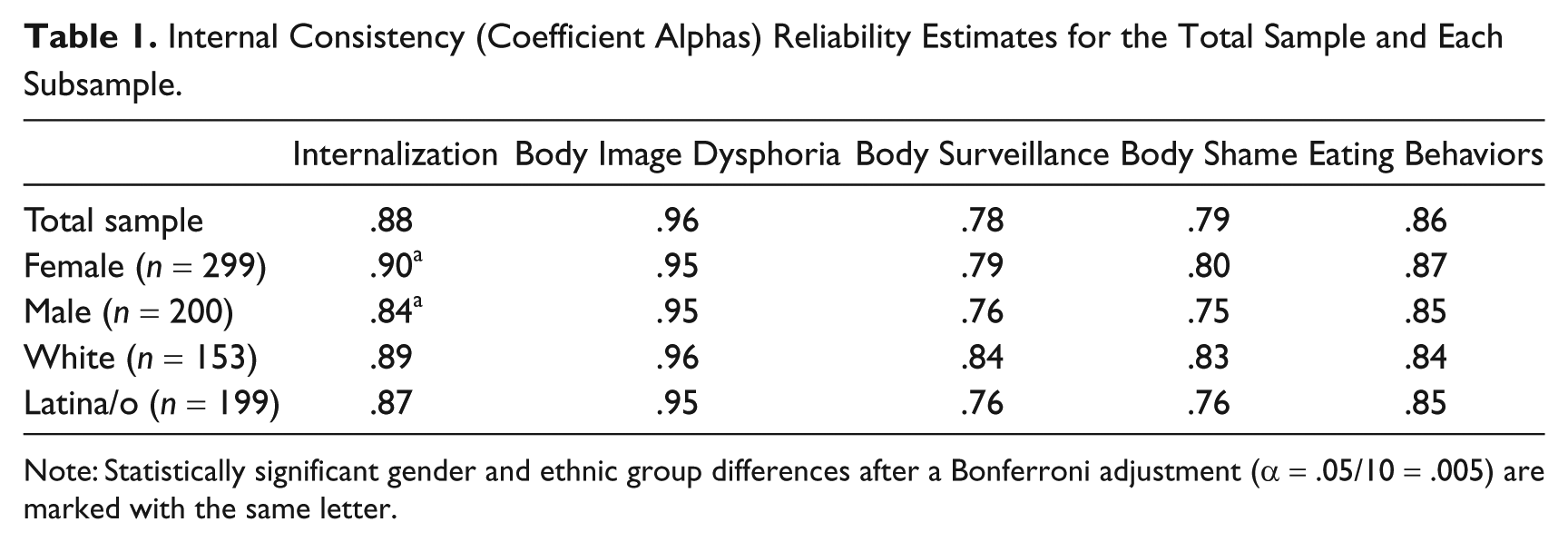
Note: Statistically significant gender and ethnic group differences after a Bonferroni adjustment (α = .05/10 = .005) are marked with the same letter.
Body image dysphoria
This construct was measured utilizing the Situational Inventory of Body-Image Dysphoria–Short (SIBID-S, Cash, 2002). This measure assessed the frequency of negative body-image emotions across specific situational contexts. Items capture how often participants experience body-image dysphoria or distress. Using a response scale ranging from 0 (never) to 4 (always), the 20-item measure identified situations in social and nonsocial contexts related to activities such as exercising, grooming, eating, intimacy, physical self-focus, and appearance alterations. Higher scores were associated with increased body image dysphoria. Two items (Items 10 and 11) with large cross-loadings (λ > .30) were removed to increase factor purity, as these items loaded on the Internalization (Item 10), Body surveillance (Item 10), Body shame (Items 10 and 11), and Dieting behaviors (Item 11) factors. Cash (2002) evaluated and concluded that the SIBID-S had a consistent pattern of moderately high correlations with other measures of body image, such as satisfaction-dissatisfaction and self-ideal discrepancies (Cash, 2002) and dysfunctional investment in physical appearance (Cash, 2002). Additionally, it was significantly and positively correlated with depression measures (r = .53), as well as social anxiety (r =. 61). Cash (2002) reported high internal consistency for women (α = .94 to .96) and men (α = .93 to .94). High internal consistency reliability estimates were obtained across groups compared in this study (see Table 1). After modifying the scale, strong construct validity evidence was suggested based on the CFA results below.
Body surveillance
This construct was assessed by using the Body Surveillance subscale of the Objectified Body Consciousness Scale (OBCS; McKinley & Hyde, 1996). This subscale consisted of eight items, some of the items included “During the day, I think about how I look many times.” The subscale responses were rated on a 7-point response scale ranging from 1 (strongly disagree) to 7 (strongly agree). In the validation study of this scale, convergent validity with self-consciousness in women, particularly with public self-consciousness, and discriminant validity with internal aspects of self and social anxiety was revealed (McKinley & Hyde, 1996). McKinley and Hyde (1996) reported high internal consistency reliability of α = .89 for undergraduate women and α = .79 for undergraduate men. Our internal consistency reliability coefficients were also adequate (see Table 1) and provided strong construct validity evidence based on the CFA results below.
Body shame
Similarly, the OBCS was also used to assess this construct. The Body Shame subscale consisted of eight items, such as “When I can’t control my weight, I feel like something must be wrong with me.” These items were rated the same as the body surveillance subscale items. McKinley and Hyde (1996) reported high internal consistency reliability for undergraduate women (α = .75) and undergraduate men (α = .73). Acceptable internal consistency reliability estimates were obtained across groups compared in this study (see Table 1). However, one item (Item 13) from body shame was removed because of its large cross-loading (λ > .30) on the Body image dysphoria factor, which suggested this item had rather poor discriminate validity. Body shame scale was assessed for its validity as a measure of internalization of cultural standards of appearance in both young and middle-aged women (McKinley & Hyde, 1996) and was strongly correlated with body esteem rather than personal endorsement of cultural standards. Note that the control belief scale from the OBCS has not been included in previous objectification theory models, nor was it included in this study. Not only was adequate internal consistency reliability estimates obtained in this study (see Table 1), but strong construct validity evidence was also obtained based on the CFA results below.
Dieting behaviors
The EAT-26 (Garner et al., 1982) assessed the degree of eating and dieting behavior and attitudes associated with eating disorders. The EAT-26 has often been used in nonclinical samples and “more broadly as a measure of abnormal, disturbed or exaggerated eating patterns” (Kashubeck-West, Mintz, & Saunders, 2001, p. 664). The EAT-26 contains three factors: dieting behaviors, bulimia and food preoccupation, and oral control. Because these factors were all highly correlated (rs > .75), only the dieting behaviors factor was used to gauge the degree of overall dieting behaviors. The EAT has been validated with anorexia nervosa patients, as well as in nonclinical samples. Specifically, it was useful in identifying eating disturbances in female college students (Garner et al., 1982). The subscales that were not included in this study were bulimia and oral control, as they were unsuitable constructs for non-clinical samples.
To avoid an artificially high interfactor correlation with body shame and to increase the factor’s unidimensionality (see Schmitt & Sass, 2011, for a detailed explanation), seven items with large cross-loadings were removed. For example, Tylka and Sabik (2010) who used the entire scale with item parcels obtained an inflated correlation (r = .82) between body shame and dieting behavior. This concern was eliminated by removing items (Items 1, 10, 11, 12, 14, 16, 22, and 26) that possessed significant cross-loadings on Body Image Dysphoria, Internalization, Body Surveillance, and Body Shame factors. The factor matrix that includes these items, along with the item content, can be obtained from the corresponding author. The remaining items (Items 6, 7, 17, 23, and 24) produced a unidimensional factor and acceptable internal consistency reliability estimates across groups (see Table 1). Although construct validity was a concern for the original scale, our CFA results provided evidence of acceptable factorial validity for our samples.
Data Analysis
Statistical analyses were conducted within Mplus 6.11 (Muthén & Muthén, 1998–2010) using a weighted least squares mean and variance (WLSMV) adjusted estimator and a polychoric correlation matrix using the delta parameterization for ordered categorical data. This estimator was selected given that it is more theoretically and statistically appropriate for estimating ordered categorical data (see Lubke & Muthén, 2004; Millsap & Yun-Tein, 2004), especially when item responses do not conform to a normal distribution and threshold differences exist across groups. Although not evident when evaluating the skew statistics (only four items had skews greater than −1 or 1), most item responses did not conform to a symmetrically distribution and thresholds were not always equal across groups. Therefore, WLSMV was clearly a better estimator choice for modeling these data than estimators that assume continuous multivariate normal data. To estimate the model, the latent factor variances were fixed at one to identify the model and set the metric. Other procedures exist to set the scale (Little, Slegers, & Card, 2006), although this procedure allows the assessment of all items for invariance (i.e., equality of unstandardized factor loadings and thresholds) while assuming the factor variances are equal across comparison groups. The small percent (2.05%) of missing data were treated using the default procedure in Mplus. This missing data estimator uses the univariate full information maximum likelihood estimates during the first stage to estimate the intercepts, thresholds, and slopes followed by the model estimating the correlations and covariances in the second stage after fixing those parameters in the first stage of model estimation. More specific details are available from Asparouhov and Muthén (2010).
Statistical models tested
Analyses were first conducted to determine whether the measurement and structural model fit the data well for the entire sample (n = 499). By means of the two-step approach, a CFA was estimated first to ensure factorial validity (or construct validity) followed by a test of the structural model using SEM. To fulfill Goal A, this study tested for measurement invariance (MI) across gender and ethnicity (White vs. Latina/o) for each factor in Figure 1 and ascertained whether internal consistency reliability coefficients (i.e., alpha coefficients) were equal across these groups. Goal A was critical to establish whether latent factor scores were created in an equivalent fashion across groups, which is required for group comparisons of means and structural coefficients. Goals B and C evaluated the equality (or invariance) of the latent factor mean scores and structural coefficients across these groups. The latter is critical to assess the model’s generalizability (or degree of invariance) across the groups compared.
Given that these analyses are less common in the literature, interested readers are encouraged to read the recent work of Dimitrov (2010), Millsap (2011), and Sass (2011). As indicated by these authors, there is no universally accepted approach to test for invariance, nor do all authors examine the same number of invariance models or test the models in an identical order. Below, we provide a brief overview of the analyses we conducted and the sequential order we elected to follow. To explore MI, the first sets of CFA analyses tested the factorial validity for each individual sample (males, females, Whites, and Latina/os) to evaluate the standardized factor loading magnitudes and model fit statistics. The configural invariance (CI or form invariance) model (i.e., tests the same factor structures across groups, meaning that the same parameters are freed and fixed) was then tested to establish a baseline model for the more restrictive MI models. Following the recommendations of Muthén and Muthén (1998–2010, pp. 433–435), the factor loadings and thresholds were set as invariant (i.e., equal) in tandem for the MI analyses. If the model is determined to lack invariance (i.e., functioning differently across groups) based on the model fit statistics, the modification indices and change in chi-square (Δχ2) statistics are evaluated to ascertain the cause of non-invariance.
After testing for MI, the latent factor means were compared by fixing the reference group (either males or Whites depending on the comparison) latent factor mean at zero and estimating the other group (either females or Latina/os). After comparing the latent factor mean scores, the covariance matrix between groups was evaluated to determine whether the factors were equally related or correlated across groups. To allow for the comparison of nested models, the next set of analyses compared a noninvariant SEM with MI (labeled SEM with MI) to an invariant SEM with MI (labeled SEM invariance) to test whether the theoretical model was invariant (i.e., possessed equal structural coefficients) across gender and ethnicity.
Overall model fit
The statistics employed to evaluate model fit for each group or sample were the robust χ2, comparative fit index (CFI), Tucker–Lewis index (TLI), and root mean square error of approximation (RMSEA). A detailed description of these model fit statistics is provided by Hu and Bentler (1999) and Marsh, Hau, and Wen (2004). Based on their research, TLI and CFI statistics greater than .90 and .95 were defined as an “acceptable” and “good” model fit, respectively, whereas RMSEA values less than .08 and .06 were considered as “acceptable” and “good” model fit, respectively.
Invariance model fit criteria
Concerns associated with evaluating model fit for invariance models are well documented (see Chen, Sousa, & West, 2005). Although the Δχ2 allows a statistical comparison between nested models, this approach may present several statistical concerns (Chen, 2007; Marsh & Hocevar, 1985). Like the χ2, the Δχ2 statistic can be large and statistically significant with complex models and/or large sample sizes. Therefore, researchers often evaluate the change in approximate fit statistics (i.e., ΔCFI, ΔTLI, and ΔRMSEA) to adjust for sample size and model complexity. Following Chen’s (2007) recommendations, acceptable invariance model fit was based on the following criteria: |ΔCFI| ≤ 0.01, |ΔTLI| ≤ 0.01, and |ΔRMSEA| ≤ 0.015 for tests of factor loading and intercept (similar to threshold) invariance. However, given that the WLSMV estimator adjustment inhibits a direct comparison between models based on the ΔCFI, ΔTLI, and ΔRMSEA (personal communication with Dr. Linda Muthén, July 7, 2010), thus models should be interpreted independently and greater emphasis should be placed on the Δχ2 from the DIFFTEST procedure. This was later confirmed in a simulation study by Sass, Schmitt, and Marsh (2012) that indicated these change in model fit statistics are only appropriate for correctly specified models. Therefore, we did not provide these results in the tables, as they should be interpreted with caution. The relative Δχ2 (Δχ2/Δdf) was also used to assess model fit, with values less than two deemed as a good model fit (Tabachnick & Fidell, 2007). These diverse model fit statistics provide an objective, transparent evaluation of invariance models.
Results
Complete Sample CFA and SEM Analyses
The measurement (i.e., CFA) and structural (i.e., SEM) model should fit the data well for the entire sample before exploring more restrictive and selective models. Using the entire sample (N = 499), the five-factor CFA model produced an adequate to good model fit, χ2(1,070) = 2461.90, p < .001, CFI = .945, TLI = .942, RMSEA = .051, and the standardized factor loadings (see Table 2) were practically (λ ≥ .30) and statistically (α = .05/48 = .001) significant after the Bonferroni adjustment. It is worth mentioning that the standardized factor loadings from the SEM analysis were nearly identical to the CFA (Δ|λ| < .05) results presented here, but again these results should in interpreted with caution. To accompany the CFA and SEM model, the correlation matrix was provided (see Appendix A) to demonstrate the bivariate relationships between factors and for other researchers to test competing structural models. Collectively, these results verified the factorial validity of the constructs investigated and justified the evaluation of our theoretical model (see Figure 1).
The Standardized Factor Loadings Associated With the Structural Coefficients in Figure 2.
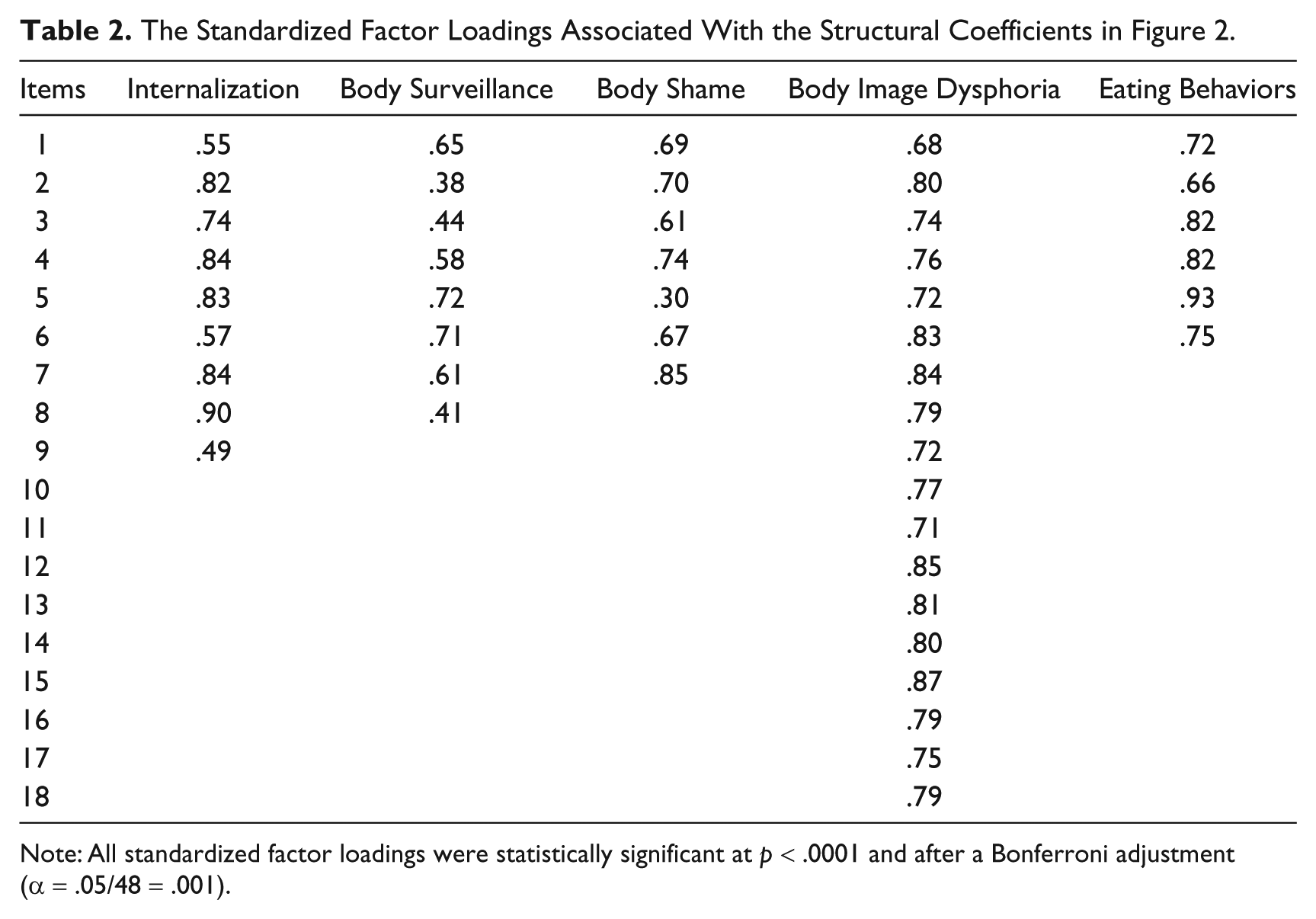
Note: All standardized factor loadings were statistically significant at p < .0001 and after a Bonferroni adjustment (α = .05/48 = .001).
The theoretical model generated a good model fit, χ2(1,074) = 2478.20, p < .001, CFI = .945, TLI = .942, RMSEA = .051, with practically and statistically significant structural coefficients (see Figure 2). The only exception was the relationship between Negative Affect and Dieting Behaviors, which was not statistically significant after controlling for Body Shame. However, the SEM model did fit significantly worse than the CFA model, Δχ2(4) = 22.06, p = .0002, thus suggesting that the SEM model fit statistically worse than the CFA model. Based on the modification indices, the path between Internalization and Body Shame was estimated to produce a nonsignificant Δχ2, Δχ2(3) = 3.50, p = .3213. This implies that the relationship between these two variables was partially mediated (rather than fully mediated) by Body Surveillance. Achieving a better overall model fit, χ2(1,073) = 2423.58, p < .001, CFI = .947, TLI = .944, RMSEA = .050, the results for this modified model are illustrated in Figure 2.
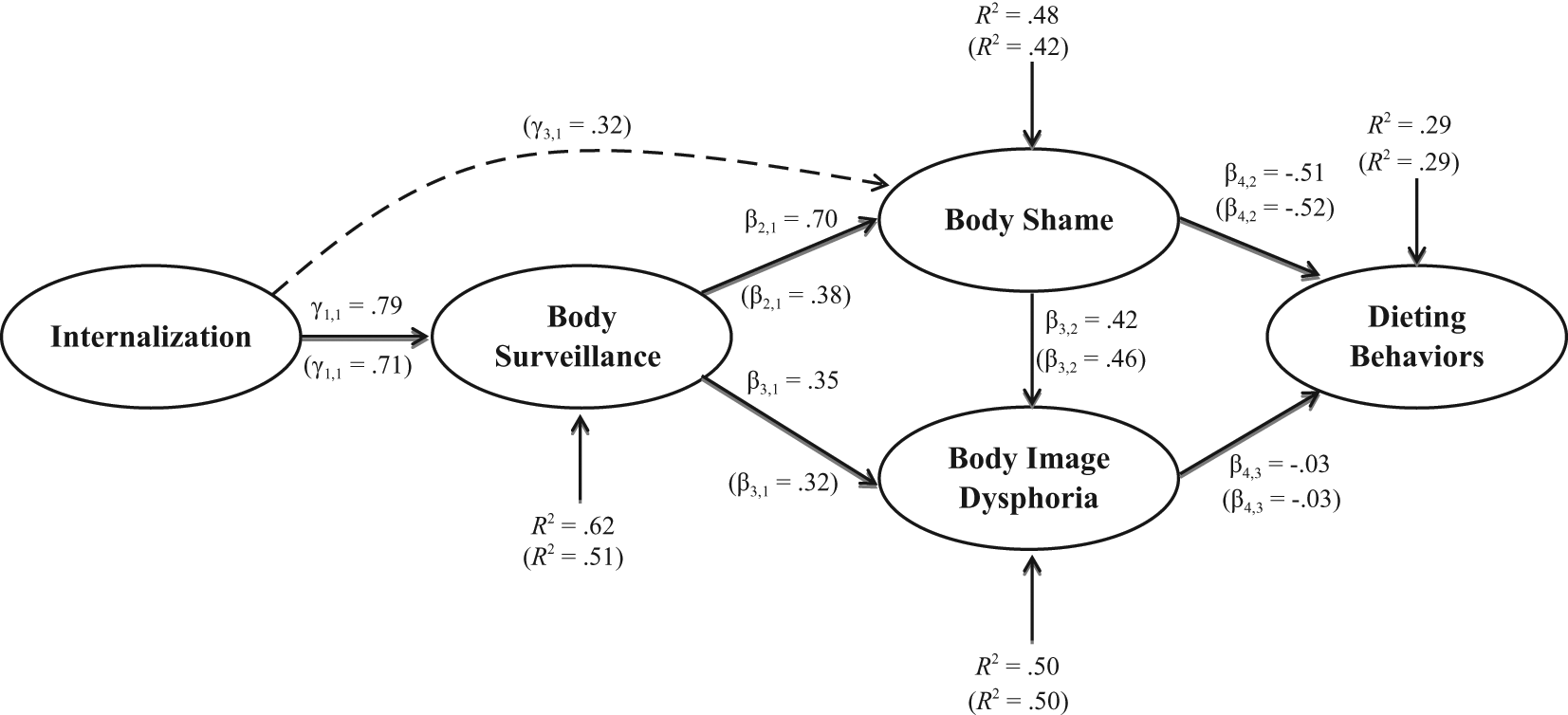
The structural coefficients and R2 statistics for the theorized and modified models of objectification theory.
In general, the structural coefficients (γ and β) and R2 statistics were promising for both models investigated. Internalization, the driving factor in the model, significantly predicted Body Surveillance and Body Shame. The modified model results infer the connection between Internalization and Body Shame was partially mediated by Body Surveillance, as γ3,1, was statistically and practically significant. This slightly contradicts the proposed model that theorized this relationship would be fully mediated and indicated that these variables were still related after controlling for Body Surveillance. The remainder of the model predicted that the association between Body Surveillance and Dieting Behaviors would be mediated by Body Shame and Body Image Dysphoria, with Body Shame partially mediating the link between Body Surveillance and Dieting Behaviors. Contrary to our theory, the association between Body Image Dysphoria and Dieting Behaviors was statistically nonsignificant, thus indicating that only Body Shame acted as a mediator between Body Surveillance and Dieting Behaviors. Importantly, the other relationships in the model were strong predictors (large structural coefficients and R2 statistics) of their respective criterion variables. Regardless of the model tested, the R2 statistics for all the latent factors were large in magnitude when using the standards tentatively proposed by Cohen (1988, pp. 413–414): small (R2 = .02), medium (R2 = .13), and large (R2 = .26).
Results related to Body Image Dysphoria and Dieting Behaviors were somewhat misleading, as it suggests these variables are unrelated. To the contrary, the bivariate relationship (r = −.38) between these variables was significant, thus suggesting instead that Body Shame was simply the dominate mediator variable over Body Image Dysphoria. As noted by James, Mulaik, and Brett (2006), this is one of the benefits of testing multiple mediators simultaneously.
To replicate previous research and investigate whether Body Image Dysphoria was a mediator (perhaps just not after accounting for Body Shame), the model in Figure 3 was tested. Analyses revealed a good model fit, χ2(776) = 1884.44, p < .001, CFI = .954, TLI = .951, RMSEA = .054, and evidence for the notion that Body Image Dysphoria acts as a mediator in isolation. Despite this confirmation, the results in Figure 2 provided a superior model due to the large R2 statistics, evidence that the Body Shame plays a stronger role in predicting Dieting Behaviors, and a more complete representation of the path to dieting behaviors prevailed. Therefore, the modified model in Figure 2 was tested for structural invariance across groups.

Evidence that Body Image Dysphoria significantly relates to Dieting Behaviors when not controlling Body Shame, thus mediating the relationship between Body Surveillance and Dieting Behaviors.
Tests of Measurement Invariance Across Gender and Ethnicity
Analyses revealed that the five-factor CFA model fit the data well for each gender separately, along with the CI model (see Table 3). Similar conclusions were obtained for the ethnicity analyses when evaluating Whites, Latina/os, and the CI model (see Table 4). These analyses provided confirmation that it was statistically appropriate to assess the MI model for the group comparisons. The MI analyses provided evidence of invariance (or equivalence) across both groups based on the model fit criteria above (see Tables 3 and 4). Although the Δχ2 was statistically significant at α = .0001 for the gender and ethnicity comparisons, the relative Δχ2 was less than two (1.62 for gender and 1.32 for ethnicity) and the MI model fit the data extremely well. Although interpreted very tentatively, ΔCFI, ΔTLI, and ΔRMSEA were also well within the recommended standards proposed by Chen (2007). For these reasons, each factor was concluded to possess MI across both gender and ethnic groups. These results imply that when conditioned on their factor score, subjects did not respond to items differently based on their gender or ethnicity; thus, it is appropriate to make group comparisons.
Separate Sample and Invariance Model Results Across Gender.
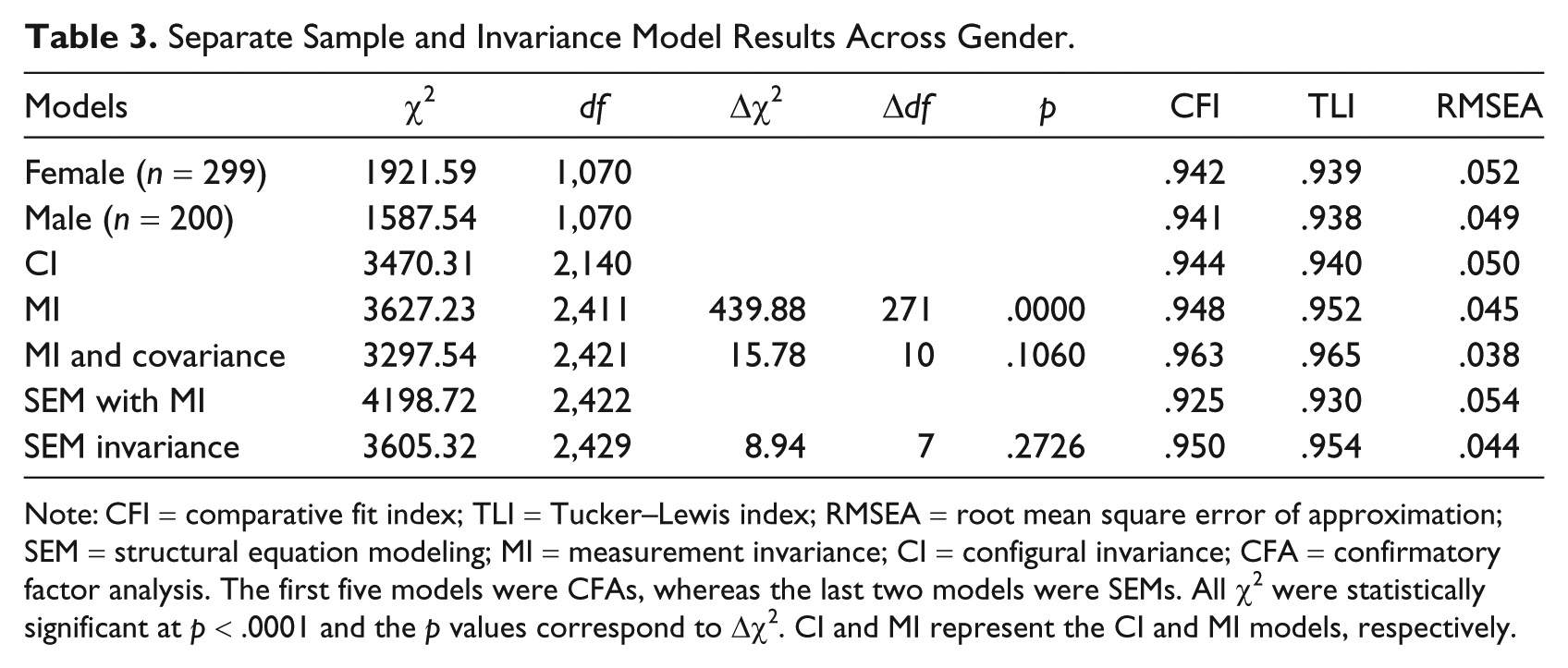
Note: CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; SEM = structural equation modeling; MI = measurement invariance; CI = configural invariance; CFA = confirmatory factor analysis. The first five models were CFAs, whereas the last two models were SEMs. All χ2 were statistically significant at p < .0001 and the p values correspond to Δχ2. CI and MI represent the CI and MI models, respectively.
Separate Sample and Invariance Model Results Across Ethnicity.
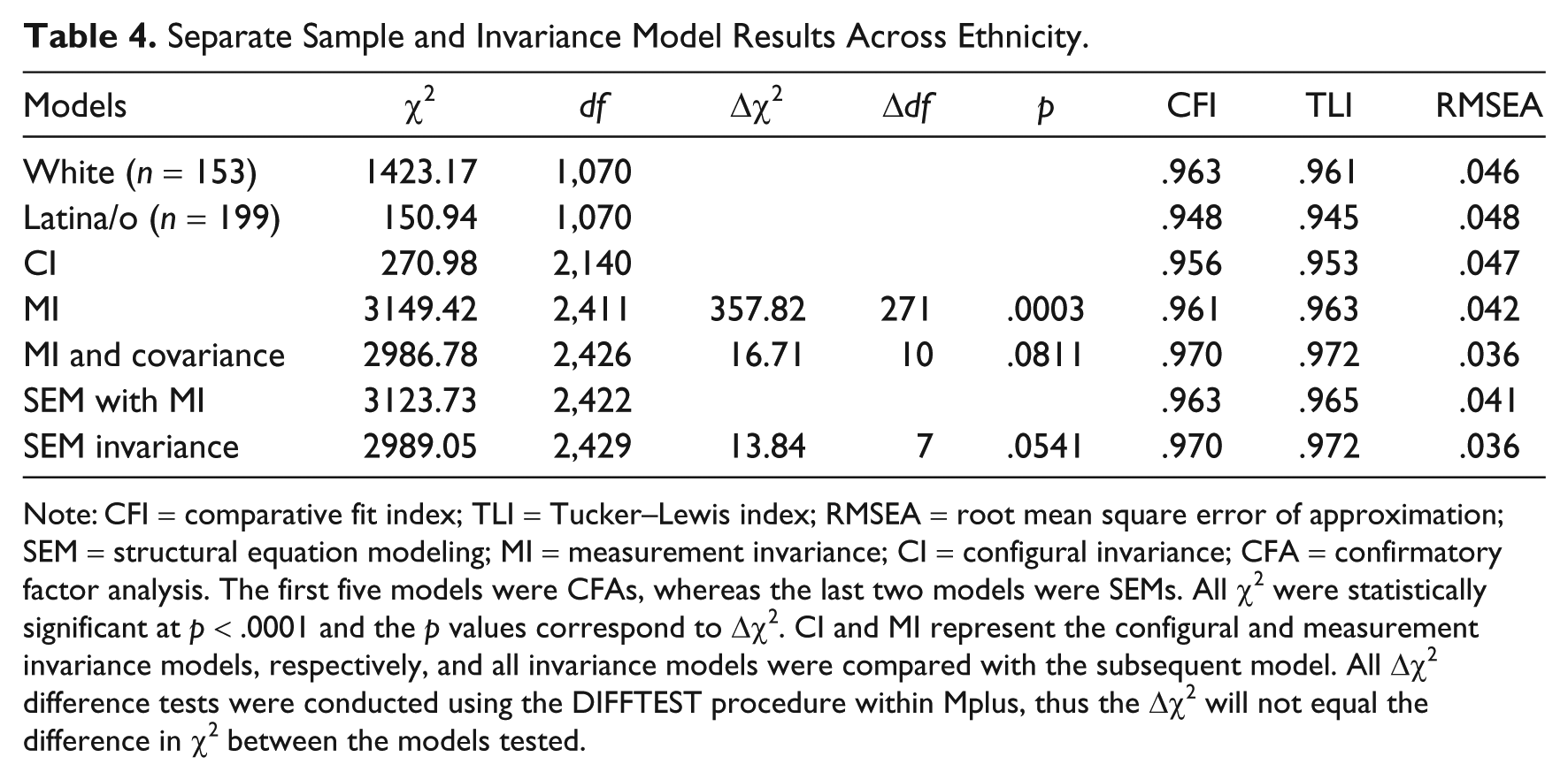
Note: CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; SEM = structural equation modeling; MI = measurement invariance; CI = configural invariance; CFA = confirmatory factor analysis. The first five models were CFAs, whereas the last two models were SEMs. All χ2 were statistically significant at p < .0001 and the p values correspond to Δχ2. CI and MI represent the configural and measurement invariance models, respectively, and all invariance models were compared with the subsequent model. All Δχ2 difference tests were conducted using the DIFFTEST procedure within Mplus, thus the Δχ2 will not equal the difference in χ2 between the models tested.
Covariance Matrix Invariance Across Gender and Ethnicity
To complement the structural invariance results below, the covariance matrix of latent factors was also constrained to be equal across groups. These analyses revealed that no differences emerged between the covariances based on gender (see Table 3), Δχ2(10) = 15.78, p = .1060, or ethnicity (see Table 4), Δχ2(10) = 16.71, p = .811. Given these results, it seems unlikely that variation in structural coefficients will emerge between groups. Note that ΔCFI, ΔTLI, and ΔRMSEA all improved, which is theoretically impossible given that a more restrictive model cannot fit better than a less restrictive model. Therefore, these ΔCFI, ΔTLI, and ΔRMSEA results should not be interpreted and demonstrate the concerns discussed above.
Internal Consistency Reliability Estimates Across Gender and Ethnicity
To supplement the factorial validity and MI results, internal consistency (i.e., coefficient alpha) reliability estimates revealed acceptable and relatively consistent coefficients across the gender and ethnic groups (see Table 1). Using the statistical approach by Hakstian and Whalen (1976), alpha coefficients were compared across gender (male vs. females) and ethnic (White vs. Latina/o) groups. After a Bonferroni adjustment (α = .05/10 = .005), the only statistically significant difference was between males and females on the Internalization scale, M statistics = 11.93, p = .0006. Although no other statistically significant differences emerged after the adjustment for Type I error, other notable variations were between White and Latina/o individuals on Body Surveillance, M statistics = 6.23, p = .0125, and Body Shape, M statistics = 4.41, p = .0357. No other differences between coefficients were significant at α = .05. Regardless of the statistical significance, practically speaking these differences in coefficients was relatively small.
Latent Factor Mean Differences Across Gender and Ethnicity
Given the attainment of MI, it was statistically appropriate to compare latent factor mean scores between gender and ethnic groups within the CFA model. Using males as the reference group (see Table 5), analyses revealed that females scored significantly (α = .05/8 = .006) higher than males on all but the Eating Behaviors factor. Focusing on Cohen’s (1988) effect size (small [|d| = 0.20], medium [|d| = 0.50], and large [|d| = 0.80]), most effect sizes were medium in magnitude. Since mean differences (M Diff) always favored the reference group, the mean difference of 0.37 on the Internalization factor indicated that females scored 0.37 units higher than males, with the effect size signifying females scoring 0.36 estimated standard deviations higher than males. Similar interpretations can be made for the other factor mean differences. No ethnic group mean differences emerged from a statistical or practical significance standpoint.
Latent Factor Mean Difference Score Comparisons Across Gender and Ethnic Groups.
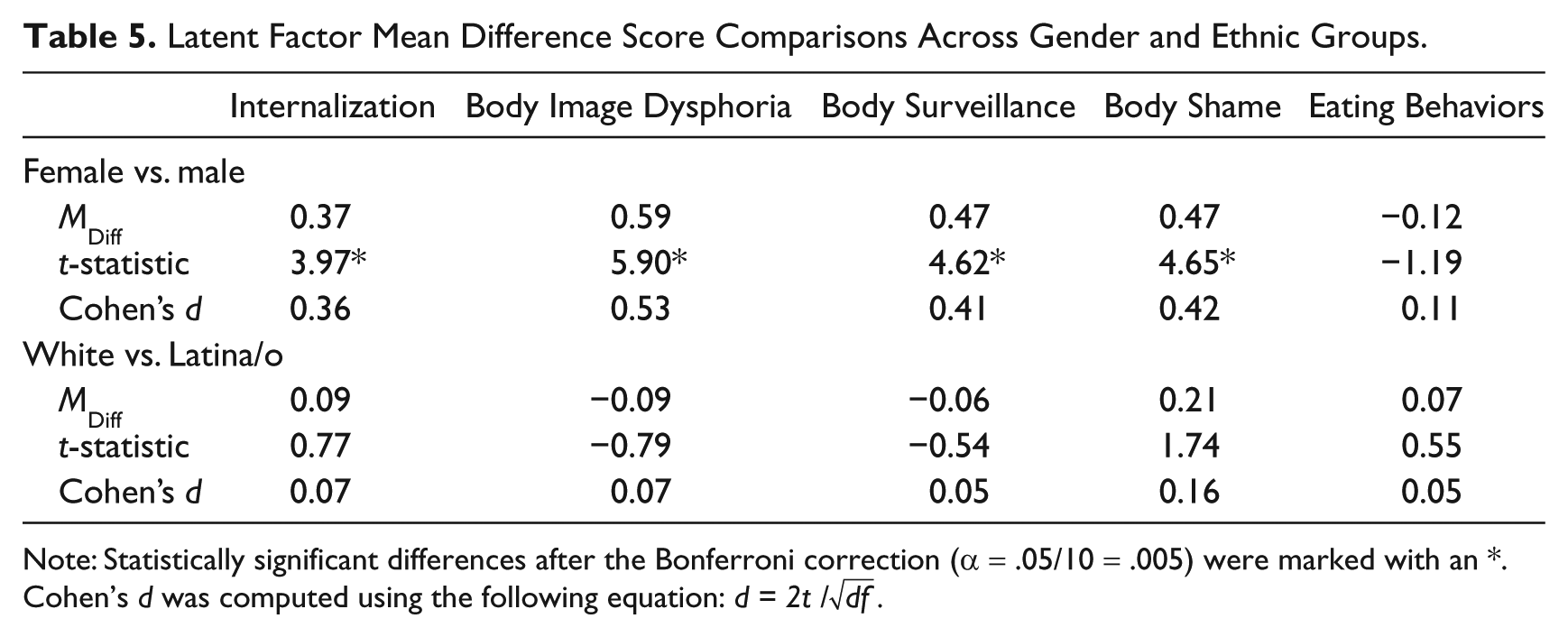
Note: Statistically significant differences after the Bonferroni correction (α = .05/10 = .005) were marked with an *. Cohen’s d was computed using the following equation: d = 2t / √df.
To replicate the latent factor score differences using observed scale scores (i.e., mean scale scores) and to include interaction terms (not tested within the CFA framework), a multivariate analysis of variance (MANOVA) using the five observed mean scores was conducted. The interaction terms were neither practically or statistically significant at α = .05, thus indicating that latent factor mean comparisons above are unaffected by the gender by ethnicity interactions. The other observed scale score main effects results (i.e., p values and effect sizes) were nearly identical to the latent factor score analyses for gender and ethnicity. Note, like the latent factor mean scores, White (M = 3.04, s = 1.31) individuals scored lower than Latina/os (M = 3.33, s = 1.23) individuals on the Body Shame scale, F(1, 327) = 5.39, p = .021, partial η2 = .016. However, this difference was not statistically significant after correcting for Type I error. The tabulated results for these observed score comparisons are obtainable from the corresponding author.
Structural Invariance Across Gender and Ethnicity
To evaluate structural invariance (i.e., whether the models have equal structural coefficients across the groups), a baseline model (labeled SEM with MI) was estimated with MI, but with noninvariant (or unequal) structural coefficients across the groups. The structural invariance model (labeled SEM invariance) was then estimated after constraining the structural coefficients to be equal (i.e., invariant) across groups, thus producing a Δdf equal to seven (one df per structural parameter constraint). Gender (see Table 3) and ethnicity (see Table 4) results both revealed no structural coefficient differences across groups, as the Δχ2 was nonsignificant. Similar to the covariance invariance models, ΔCFI, ΔTLI, and ΔRMSEA all improved and therefore should not be interpreted.
A small, but nonsignificant (p = .054), difference did emerge between ethnic groups. Follow-up statistical analyses (Δχ2) were not conducted to avoid Type I errors. However, small (|Δγ| or |Δβ| ≥ .15) standardized coefficient differences (White minus Latina/os, thus positive numbers signifies a larger coefficient for White individuals) existed between the following links: Internalization (Δβ = .22) and Body Surveillance (Δβ = −.16) to Body Shame, and Body Surveillance (Δβ = −.17) and Body Shame (Δβ = .15) to Body Image Dysphoria. Consequently, with larger sample sizes these differences might emerge as statistically significant. For gender, no standardized coefficient differences exceeded .15. Regardless, statistical analyses suggested that neither gender nor ethnicity moderated any structural coefficients and the proposed model functions equally well across these groups.
Discussion
This study investigated an extension of objectification theory across gender and ethnicity, while also testing for measurement invariance and equality of latent factor mean scores. Given the call for more generalizable models (Grabe, Hyde, & Lindberg, 2007; Moradi, 2010; Moradi & Huang, 2008), this study sought to fill the extant literature gap by exploring the applicability of our model across Latina/o and White female and male college students. Our results are especially important for Latina/o individuals, as these constructs have not been thoroughly examined in this population to date. Our findings were congruent with prior research, which stated that internalization, body surveillance, and body shame all contributed, either directly or indirectly, to dieting behavioral patterns. The one exception was that body image dysphoria did not predict negative dieting behaviors after controlling for body shame.
Modified Objectification Theory Model
Similar to previous research (Moradi et al., 2005), our results revealed that internalization predicted body surveillance and body shame. More specifically, the relationship between internalization and body shame was partially mediated by body surveillance. This means that individuals who internalize society’s standards of appearance (i.e., more internalization and body surveillance) are more likely to experience body shame when habitually comparing themselves against societal standards. Thus, body shame appeared to partially stem from the perception of not meeting these standards (Mitchell & Mazzeo, 2009; Moradi et al., 2005).
Our conclusions sustained the notion that body surveillance predicts both body shame and body image dysphoria. However, after controlling for body shame, body image dysphoria did not appear to predict dieting behaviors. These results were consistent with other research examining depression (in this study replaced by body image dysphoria) and anxiety that found that these specific risk factors might not be connected to eating disorders (Jacobi, Hayward, deZwaan, Kraemer, & Agras, 2004; Tiggemann & Kuring, 2004). Although depression and depressed mood (in our study referred to as body image dysphoria) have been identified as an essential part of objectification theory (Tiggemann & Kuring, 2004), our findings indicated that body shame was a stronger predictor of dieting behaviors. This was supported by other studies (Hallsworth et al., 2005; Slater & Tiggemann, 2010; Tiggemann & Kuring, 2004; Tylka & Sabik, 2010).
In general, the structural coefficients and effect sizes are relatively large, which implies that this model may be applicable for clinicians (e.g., counselors, psychologists) who work with clients experiencing dieting behavior problems. Specifically, those working with clients with dieting behavior problems should attempt to reduce the impact of environmental pressures to be thin (i.e., internalization and body surveillance) and seek to lessen their degree of body shame. Although diminishing body image dysphoria may be constructive, there is little evidence that it will reduce dieting behavior problems. Consequently, mental health professionals would benefit from focusing on body shame to address dieting behavior problems. On a positive note, these results indicate that interventions may be applicable regardless of gender and the two ethnic groups explored, with additional research needed to generalize these findings across noncollege student populations.
Measurement Invariance and Reliability
Although given less attention in other studies, an important contribution of this study is that of MI across gender and the two ethnic groups explored. Thus, at the item level no factor loading or threshold differences emerged between groups, meaning that the groups interpreted the items/factors in a similar fashion. To our knowledge, these analyses have not been carried out to date and, therefore, present a significant benefit to the measurement literature. Likewise, our analyses revealed that the internal consistency reliability coefficients were relatively similar across these groups. These results, along with the conclusion that these scales equally predict the designated criterion variables, provided strong support for the scales’ psychometric properties.
One potential limitation is that 10 items (seven from the Eating Behaviors factor) were removed from their designated factors because of model misfit and dimensionality concerns. Based on personal experience, this occurrence is commonplace when scales are originally evaluated in isolation without the opportunity to correlation (i.e., load) with other commonly related factors. Although our purpose was not to purify previous measures, this modification should benefit future researchers using these scales.
Gender and Ethnicity
Previous research has contended that objectification may have a different impact on ethnic minority women because they may deviate from the mainstream standards of feminine beauty (e.g., thin, blonde, youthful, light-skinned, heterosexual, and middle class). As described previously (Augustus-Horvath & Tylka, 2009), some dimensional differences may include the intersection of age, ethnicity, skin color, sexual orientation, and socioeconomic status. Alas, the sample size was not large enough to explore all subgroups of the population. Therefore, this study focused solely on gender and the two ethnic group comparisons and not the Latina/o female comparison with the other three subgroups.
Congruent with previous gender research (Slater & Tiggemann, 2010; Tiggemann & Kuring, 2004), this study found mean differences on various objectification theory variables. Specifically, women were more likely to internalize societal pressures, monitor their appearance, experience body shame, and possess negative feelings related to their body. It should be noted that Slater and Tiggemann’s (2010) findings were based on a sample of adolescent girls and boys, which highlights that these differences may be present in both adolescents and college-aged individuals. However, the absence of gender differences on eating behaviors countered the results in some of the previous studies (Slater & Tiggemann, 2010; Tiggemann & Kuring, 2004). Despite these mean differences, no structural differences emerged between gender groups, thus implying the system for treating eating problems may be similar across genders.
Regarding ethnic group mean differences, White and Latina/o participants reported similar levels of internalization, body surveillance, body shame, body image dysphoria, and dieting behaviors. The only trend was that Latina/o individuals indicated greater body shame than White individuals, which may be attributable to their higher BMI scores. Similar to gender, our structural invariance model results indicated that the relationship between constructs (i.e., structural model) was similar for White and Latina/o individuals. Shaw, Ramirez, Trost, Randall, and Stice (2004) indicated that a potential reason for the lack of differences among ethnic groups is because of widespread sociocultural pressures to be thin. Until more recently, relatively little empirical support existed for this deduction. Based on the work of Buchanan et al. (2008) and Mitchell and Mazzeo (2009), who compared African American and White individuals, along with our study evaluating White and Latina/o individuals, there appears to be evidence for this assertion. However, as indicated above, ethnic differences may have materialized with larger sample sizes.
Nevertheless, the explanation by Shaw et al. (2004) should be interpreted with some caution. These ethnic similarities may be due to several additional factors characteristic to this study’s sample. These may include the homogeneity of the samples (all college students), geographic location (high percentage [58.7%] of Latina/o and Hispanic individuals in our city; U.S. Census Bureau, 2000), generation level (mostly acculturated students), and developmental stage (typically younger adults seeking an undergraduate degree). For example, it may suggest that college students, regardless of ethnicity, encounter stronger pressures to acculturate and assimilate to the “mainstream culture,” and therefore, the model may not be equivalent across ethnic groups with noncollege samples.
Relationships (i.e., structural and interfactor correlation coefficients) were not moderated by gender or ethnicity, thus indicating that our model generalized across these two groups. A caveat is that with larger sample sizes some ethnic differences may materialize and that differences may emerge when comparing samples that are not in college. The equivalence observed in the relationships between these constructs and the overall mean results both supported that White and Latina/o college students may experience a similar process with regard to internalization of societal standards, body dysphoria, body shame, negative affect, and dieting behaviors. While no ethnicity mean differences materialized, several gender mean differences existed. In fact, men and women differed on every scale except dieting behaviors.
Limitations
Due to geographical location, participants who identified themselves as Mexican American and Latina/o individuals were combined into one group. This clustering prohibited the evaluation of culturally relevant differences that may have surfaced. Other ethnic (e.g., various Asian descents, etc.) and age (e.g., older adults) groups that have been neglected in past objectification theory literature were also not represented in our analyses. Another drawback is the scales and model did not include ethnicity- or gender-specific content; thus, these culturally sensitive factors (e.g., acculturation, acculturative stress, level of ethnic identity, skin color, and masculine/feminine characteristics) could mediate or moderate effects found in the proposed model. Because of sample size constraints, separate models could also not be tested for only Latina women and the other subgroups. Although the MANOVA results indicated no interaction effects, it is unknown whether the structural coefficients differ across these smaller subgroups.
When evaluating the correlations between scales by separate gender and ethnic subgroups (see Appendix B), some differences emerged between the subgroups. For example, the correlation between body image dysphoria and body shame was higher for White females than the other three subgroups. Also of interest was that internalization was highly correlated with dieting behaviors for females, but not for males. Therefore, structural invariance analyses need to be conducted with larger sample sizes and more homogenous subgroups (e.g., only Latinas). Again, these analyses could not be conducted within an SEM framework because of sample size constraints, but these simple correlation analyses suggest that differences may exists.
Implications for Prevention and Treatment
This study provides several implications for the prevention and treatment of body image concerns and disordered eating patterns. Research suggested that effective prevention involves breaking the link between internalization of beauty standards, body shame, and disordered eating (Stice, Marti, Spoor, Presnell, & Shaw, 2008). Effective prevention programs may include media literacy and techniques to promote positive body image in an effort to increase acceptance of different body types. Consistent with our model, prevention programs aimed at decreasing internalization of unattainable societal standards, along with addressing body surveillance, may lessen body shame and in turn reduce disordered eating patterns. Based on the results regarding gender differences, women and girls may benefit from a stronger emphasis on the link between internalization of societal standards and dieting behaviors.
It is also important to understand the relationship between cognitions and behaviors when treating negative dieting behaviors. This model may provide practitioners working with White and Latina/o clients with a framework to address etiological factors, including objectification and body shame contributing to eating disorders and body dissatisfaction. For example, some therapeutic strategies for treatment of dieting behaviors or disordered eating may include cognitive behavioral interventions aimed at challenging thoughts contributing to internalization, body surveillance, and body shame (identified as a major contributor to dieting behaviors). Even though minority populations are less likely to be diagnosed with an eating disorder (Gordon, Perez, & Joiner, 2002) and are often believed to have fewer body image concerns and eating disorders, studies have emphasized that they are just as likely to experience them. Because of this, it is imperative for mental health providers to use appropriate culturally sensitive frameworks.
Conclusions
This study’s findings have several potential implications for research, prevention, and treatment of eating disorders. Results indicate that our model based on several objectification theory constructs generalizes across gender and the two ethnic groups, but perhaps most important, it is applicable to the Latina/o college student population. As with previous research, our model suggests that the development of eating behavior problems stems from negative self-perceptions and body shame resulting from not meeting societal standards. Although a consistent bivariate correlation may exist between body image dysphoria and dieting behaviors, our analyses suggest that prevention and treatment should commence from self-perception in relation to others and body shame. Our results also provide a good foundation for the development of future more complex models that tap other consequences of negative internal perceptions of body image.
Footnotes
Appendix A
Estimated Interfactor Correlations From the CFA
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| 1. Eating Behaviors | — | ||||
| 2. Body Image Dysphoria | −.38 | — | |||
| 3. Internalization | −.30 | .51 | — | ||
| 4. Body Surveillance | −.30 | .61 | .71 | — | |
| 5. Body Shame | −.56 | .66 | .60 | .63 | — |
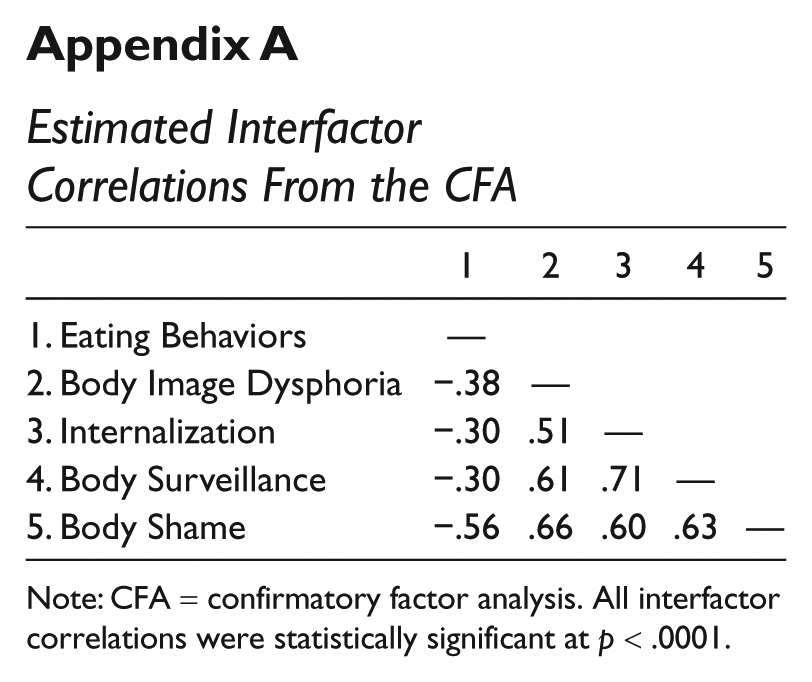
Note: CFA = confirmatory factor analysis. All interfactor correlations were statistically significant at p < .0001.
Appendix B
Interfactor Correlations Using the Mean Scale Scores for Each Gender and Ethnic Group Separately
| Scale | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Latinos (n = 76) | |||||
| 1. Internalization | — | ||||
| 2. Body Shame | .462 | — | |||
| 3. Body Image Dysphoria | .389 | . |
— | ||
| 4. Body Surveillance | . |
. |
. |
— | |
| 5. Dieting Behaviors | −.078 |
|
−. |
−.319 | — |
| White males (n = 59) | |||||
| 1. Internalization | — | ||||
| 2. Body Shame | .543 | — | |||
| 3. Body Image Dysphoria | .235 | . |
— | ||
| 4. Body Surveillance | . |
. |
. |
— | |
| 5. Dieting Behaviors | −.061 |
|
|
−.193 | — |
| Latinas (n = 107) | |||||
| 1. Internalization | — | ||||
| 2. Body Shame | .532 | — | |||
| 3. Body Image Dysphoria | .377 | . |
— | ||
| 4. Body Surveillance | . |
. |
. |
— | |
| 5. Dieting Behaviors | −.387 |
|
|
−.227 | — |
| White females (n = 89) | |||||
| 1. Internalization | — | ||||
| 2. Body Shame | .486 | — | |||
| 3. Body Image Dysphoria | .419 | . |
— | ||
| 4. Body Surveillance | . |
. |
. |
— | |
| 5. Dieting Behaviors | −.291 |
|
|
−.225 | — |
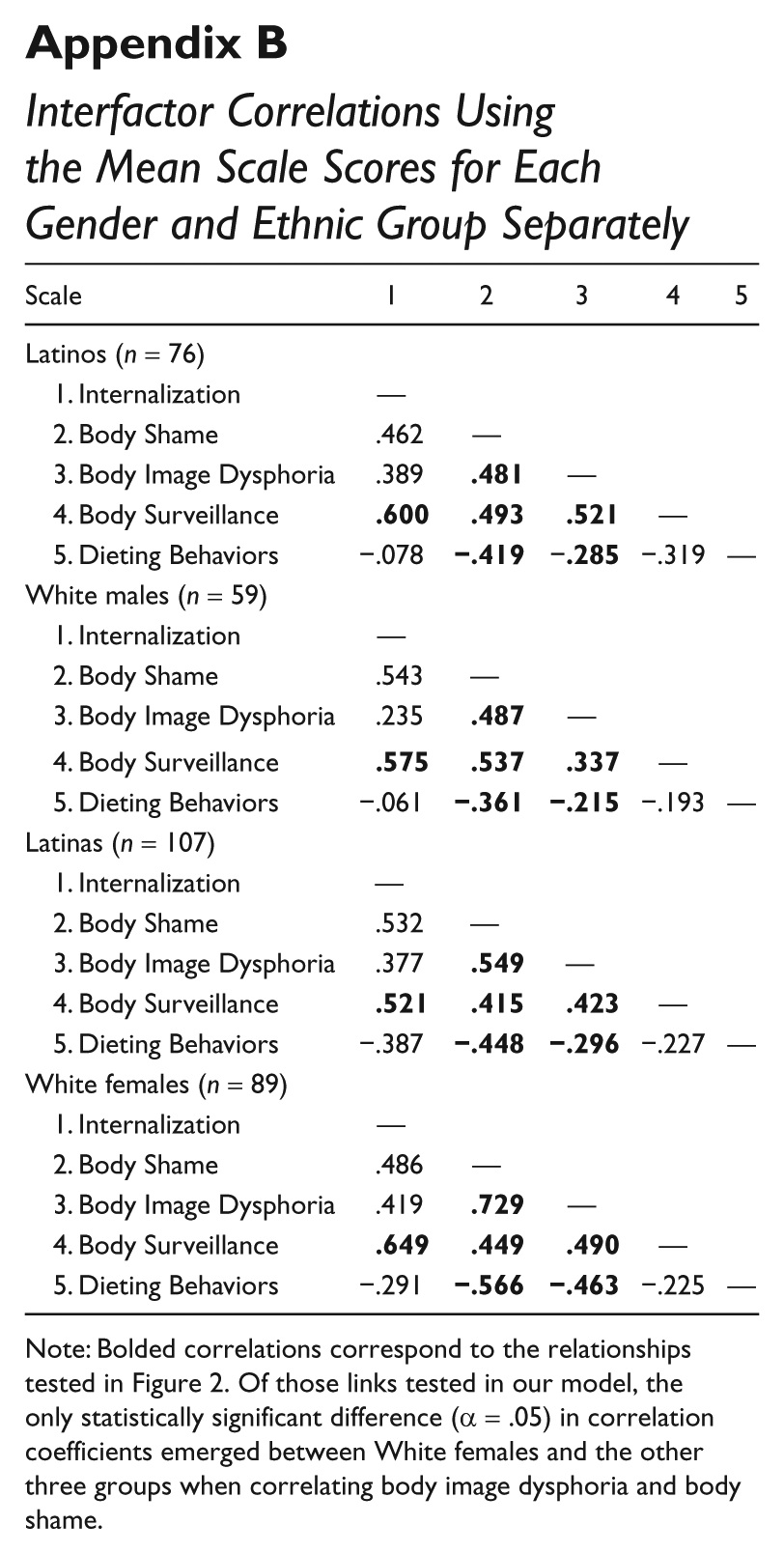
Note: Bolded correlations correspond to the relationships tested in Figure 2. Of those links tested in our model, the only statistically significant difference (α = .05) in correlation coefficients emerged between White females and the other three groups when correlating body image dysphoria and body shame.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.