
Abstract
Background:
Corrosive esophageal injury causes serious clinical problems. We aimed to create a new experimental esophageal burn model using a single catheter without a surgical procedure.
Materials and methods:
We conducted the study with two groups of 12 male rats that fasted for 12 h before application. A modified Foley balloon catheter was inserted into the esophageal lumen. The control group was given 0.9% sodium chloride, while the experimental group was given 37.5% sodium hydroxide with the other part of the catheter. After 60s, esophagus was washed with distilled water. The killed rats were examined using histopathological methods after 28 days.
Results:
In comparison with the histopathological changes experienced by the study groups, the control groups were observed to have no pathological changes. Basal cell degeneration, dermal edema, and a slight increase in the keratin layer and collagen density of submucosa due to stenosis were all observed in the group subjected to esophageal corrosion.
Conclusion:
A new burn model can thus, we believe, be created without the involvement of invasive laparoscopic surgery and general anesthesia. The burn in our experiment was formed in both the distal and proximal esophagus, as in other models; it can also be formed optionally in the entire esophagus.
Introduction
Esophageal burns due to accidental caustic ingestion are a very important clinical problem in children (who represent up to 75% of all cases) in some countries. It is seen less frequently during adolescence than during postnatal and early puberty periods (Rothstein, 1986). Corrosive injuries of the esophagus play a very important role in morbidity and mortality rates of children aged between 1 and 3 years (Adam and Birck, 1982; Karnak et al., 1999; Keskin et al., 1991; Ocakci et al., 2006; Tanyel et al., 1988; Turan et al., 2000).
Caustic chemical substances such as strong acids and strong alkali bases, acid-like or slightly acidic solutions, and sodium carbonate cause some of the most serious corrosive esophageal burns in children (Adam and Birck, 1982). Many medications, antioxidants, and phytotherapeutic compounds have been used in the past to prevent stenosis and long-term complications (Karnak et al., 1999; Ocakci et al., 2006). But in clinical practice, the process of treating esophageal burns still has no specific therapy. Many experimental studies have thus been carried out on animals.
Corrosive esophageal burns are expressed as superficial or deep. The superficial type can be seen along with edema, erythema, slight ulcerations with hemorrhage, and bulla formation in the epidermis and subepidermal layer. Deep burns are seen as thick ulcerative burns with epithelial thickness and keratinization in the epidermis. In some cases, it may cause aortoenteric and tracheoesophageal fistula structures (Burrington and Raffenspenger, 1978; Kirsh et al., 1978).
The experimental esophagitis method of Gehanno et al. is one of the most commonly used methods to create caustic esophageal burns. Current studies indicate that different modifications of this model are still used in invasive studies (Gehanno and Guedon, 1981; Liu and Richardson, 1985). The aim of this study is to develop a new experimental esophagitis model with a minimal invasive procedure. Also, it seeks to offer ease of application and saves time, money, and instruments, as well as preventing loss of experimental animals.
Materials and methods
The protocol of this study was reviewed and approved by the Local Ethics Committee for Animal Experiments, School of Medicine, Rize University, Turkey (date: December 30 2011, meeting number: 37).
Animals
A total of 12 Sprague Dawley male rats of age ranging from 250 to 275 days and weighing between 300 and 350 g were used in the study; they were born and raised in Trabzon, Turkey and were provided with a standard 7–8 mm pelleted rat diet (Erzurum, Turkey) and water ad libitum before and after the procedure. During 4-week duration of all these experiments, air changes (15–18 per hour), temperature (20 ± 3°C), and normal relative humidity (55–60%) were maintained in the rooms in which the rats were housed. Lighting was provided by cool fluorescent lamps controlled with a 12-h light/dark cycle by an automatic timer system. Experiments were performed according to the National Institute of Health Guidelines for the Care and Use of Laboratory Animals.
New experimental model
The rats were divided into two groups, the control group and the study group, consisting of six animals each. Animals were fasted for 12 h before the study. Distance from the cardioesophageal entrance to the mouth was measured with a guidance catheter under light ether sedation before application. The Foley catheter’s balloon (2-way, 6FR, 5–15cc-Cod: CA100707, Hangzhou Fushan Medical Appliances Co., China; Figure 1(a)) was slowly inserted into the stomach.
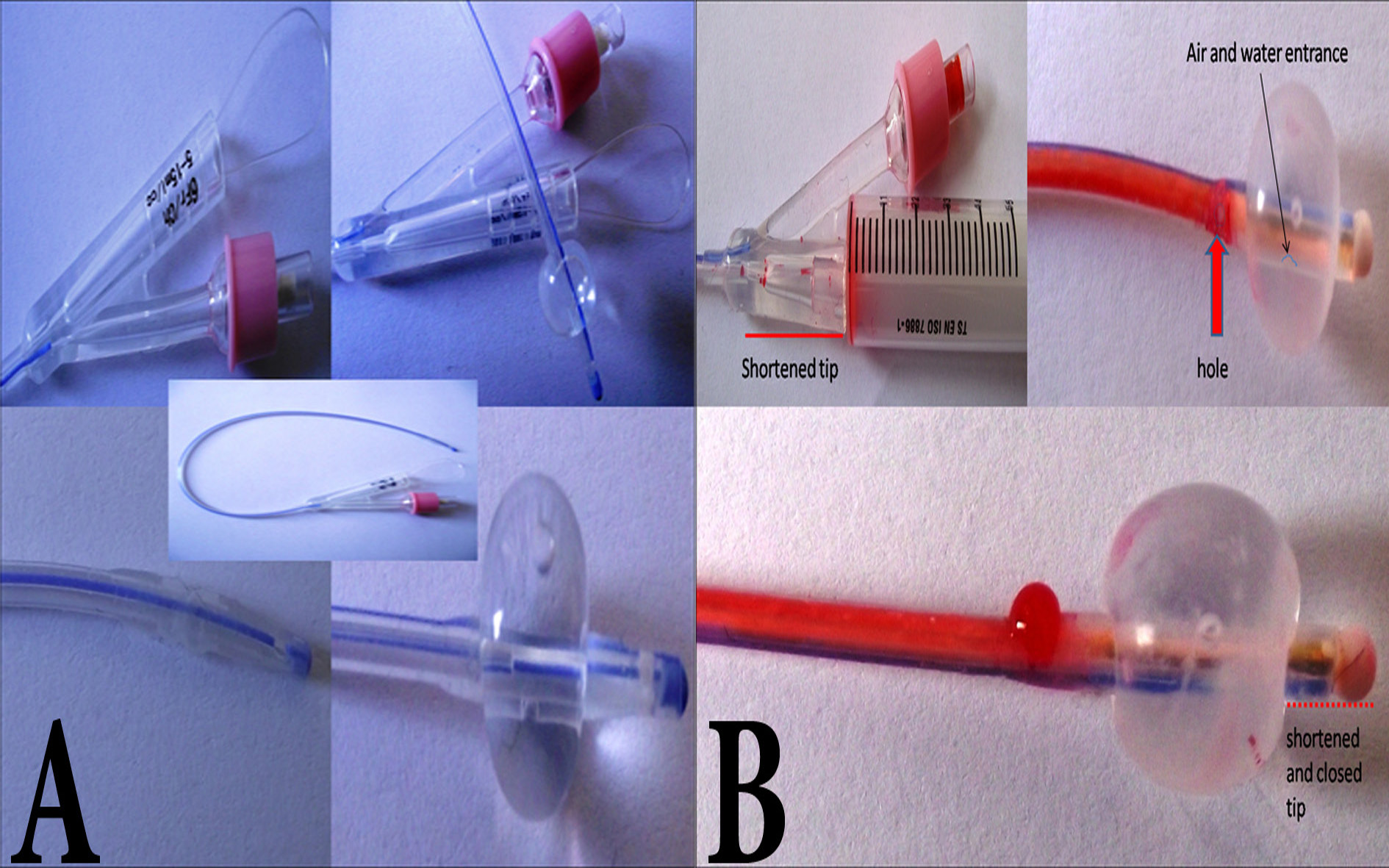
(a) Normal and (b) modified Foley catheter.
One end of the Foley catheter is inflated with air or warm saline solution, while it is in the stomach. The other end has a larger opening that allows sodium hydroxide (NaOH) to flow into the stomach. This part of the Foley catheter is normally open continuously to allow for the passage of urine. In our study, however, this way was closed with a strong adhesive (Figure 1(b)). The flow of NaOH was permitted by opening a hole just above the balloon. This hole in the catheter plays an important role in the exact withdrawal of the fluid from the esophagus. Liquid filling continues from the cardiac sections to the pharyngeal section. The pharyngeal part is thus not irritated and the rats can be fed with soft food for shorter period of time. The head of the channel where NaOH is introduced is shortened (Figure 1(b)), which prevents negative pressure from building in the syringe. The catheter is held in the stomach by a balloon filled with water. It is pulled upward slightly and the cardioesophageal entrance is thus completely closed by the balloon (Figure 2).
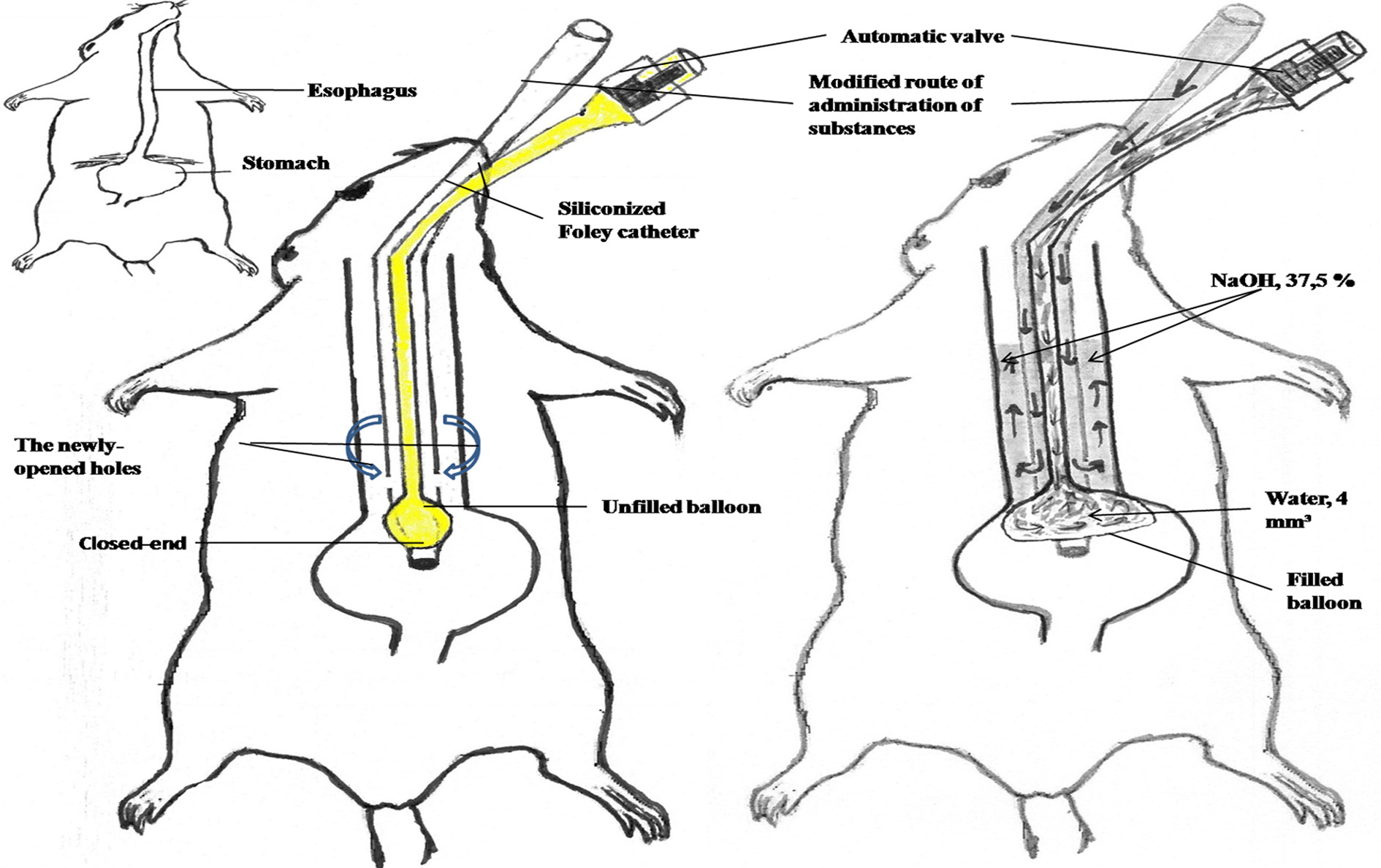
Catheterization of esophagus and stomach when 37.5% of NaOH was given and washed with distilled water in the rat. NaOH: sodium hydroxide.
The modified Foley catheter was inserted along the esophageal lumen. A part of the catheter was pulled back and the balloon was filled with water (4 mm3) in the stomach. The stomach’s entrance was closed by balloon block to prevent leakage of the liquid. Animals from the control group received 1 ml of 0.9% sodium chloride by oral gavage. The experimental group rats were treated with 0.3 ml of 37.5% NaOHby oral gavage. After 60 s, the esophageal lumen was washed with distilled water. After these applications, the balloon of the catheter was deflated by opening a valve and the catheter was withdrawn (Figure 2).
All animals were given liquid nutrition solutions in the first 24 h after the experiment, and pellet feed was available in their cages. On the second day, they were fed with soft food. Food consumption of the animals was observed daily and their body weights were recorded at 1-week intervals.
Blind histopathological evaluation of esophageal tissues was conducted by two histologists and one pathologist using a three-point scoring system with the grades weak (−), moderate (+), and intense (++) (Table 2).
Light microscopic histopathological examinations
At the end of 4 weeks, all animals were killed under deep ketamine (50 mg/kg) and xylazine (0.75 mg/kg) anesthesia, and esophageal pieces from the pharynx and cardia with the stomach were removed for the preparation of specimens. These tissues were fixed in 10% formalin solution for 24 h. After dehydration in a series of ethanol and xylene solutions, the tissue was embedded in liquid paraffin. The tissue was sectioned at a thickness of 4–5 μm using a rotary microtome and stained with haematoxylin–eosin. Light microscopy examination was used to confirm the definition of esophageal tissue structures.
Statistical analysis
Histopathological changes and body weights in the two groups were analyzed with χ 2 and Mann–Whitney U tests (SPSS 18 for Windows, IBM, Chicago, Illinois, USA). p Values of less than 0.05 were considered statistically significant.
Results
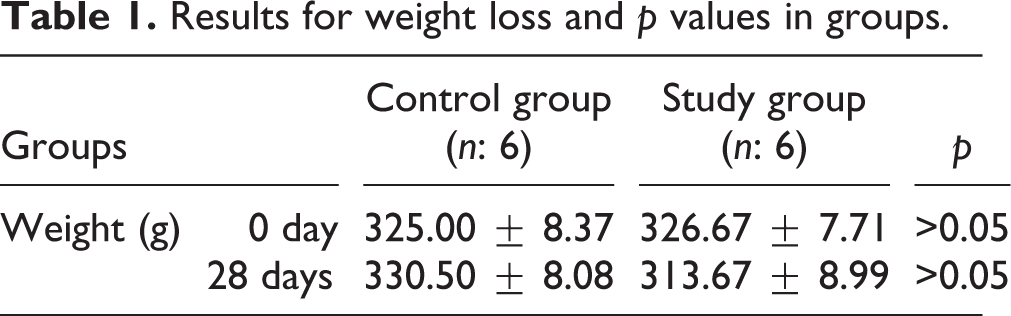
Our study produced a successful model that does not require surgery. No animal in the study group died during application of the new method. Weight loss was determined to be very low in the study group, and what loss there was observed over the first few weeks (5–7%). Weight loss was observed in the first few weeks due to esophageal burns and they are not statistically significant (p > 0.05; Table 1).
Results for weight loss and p values in groups.
The esophageal structure of the control group was observed in normal morphology through macroscopic and microscopic examination. Histopathological changes and narrowing at different levels of both the pharyngoesophageal and cardioesophageal pieces were observed in the esophagi of the study group. These changes in the lumen were less evident on the epithelial layer. We showed that superficial epithelial cells of the esophagus lumen differentiated from superficial injury. In some specimens, total necrosis and pigmentation were seen. There was no very dense stenosis in the lumen. Submucosa and muscle layers, however, had been replaced by slight scar tissue. We observed muscularis inflammation, submucosal collagen enhancement and oedema (OED) in the submucosa and degeneration in muscularis mucosal cells, when the study group was compared with the control group (Figure 3; Table 2).
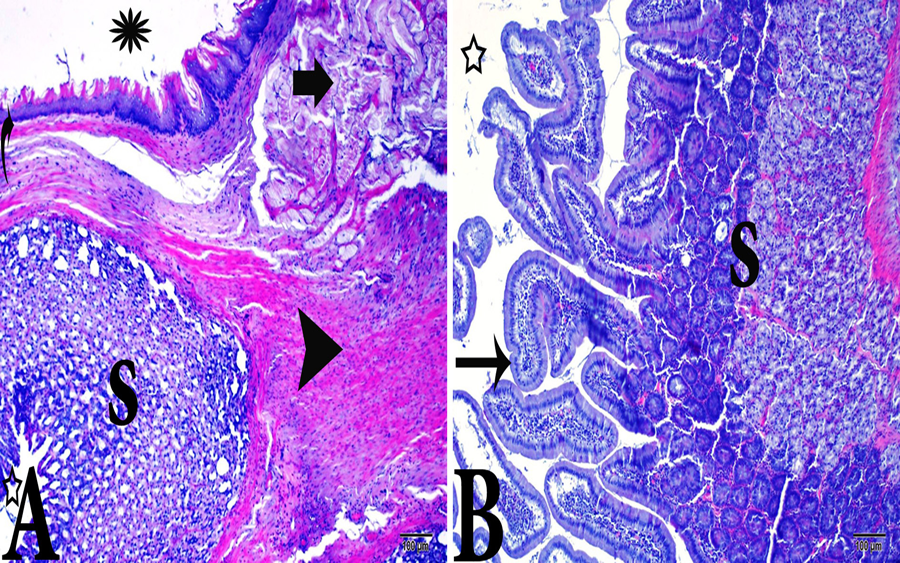
Cardioesophageal entrance section of the study group; (a) arrow: hypertrophic and degenerative muscle, s: stomach, headarrow: normal muscle in stomach, asteriks: esophagus lumen, and curved arrow: thinning of the epithelium due to the transition; there was no disorder in the stomach; (b) thin arrow: normal epithelium, s: stomach, star: lumen of stomach, hematoxylin–eosin stain, X10, 100 µm.
Results score for histopathologic evaluation and p values in groups.

EL: epithelial layer; MM: muscularis mucosae; OED: oedema; SC: submucosal collagen; TM: tunica mucosa.
Discussion
Corrosive esophagus burns have been reported in 18–75% of caustic ingestions occurring in children. Many experimental studies have used different materials to treat these burns (Senturk et al., 2011). Such experimental studies need to be practical and feasible. It is difficult to find adequate experimental models for researching corrosive esophageal injury or burn that are not costly and do not involve loss of experimental subjects. Our aim was to create a new experimental model using a single tool and not requiring a surgical procedure.
The corrosive esophageal burns were classified as grade 1, 2, or 3. Grade 1 injuries are superficial and limited to the mucosa. There is mucosal edema, mucosal erythema, and hyperemia, but no scar development. With grade 2 injuries, superficial noncircumferential burns are discrete, with deep ulcerations of the esophagus, and may cause strictures. This group is divided into two subunits, grade 2A (superficial ulcers, bleeding, and exudates) and 2B (deep focal or circumferential ulcers). Grade 3 injuries involve deep circumferential burns and are divided into two subunits. In grade 3A, strictures are developed in 70–100% of the cases and there is focal necrosis. The early mortality rate of grade 3B is 65% and necrosis is extensive. The risk of esophageal perforation is highest in this grade (Gupta et al., 2001). We can inflict all three types of injuries with this model. It can also inflict injuries in any part of the esophagus (Table 2).
The model of Gehanno and Guedon (1981) and other invasive approaches make the application more difficult because of anesthesia complications and the loss of 40–50% of experimental subjects (Gehanno and Guedon, 1981). In invasive models, postoperative care and feeding create complications that may affect the outcome of experiments because of, for instance, the use of antibiotics to prevent septicemia. In our model, there is no need for a surgical operation under general anesthesia. All applications can be performed with the help of a modified catheter under only light sedation. Our model also reduces the application time and required material, so it is time-saving and economical.
Gehanno’s model was modified when mortal complications occurred after the procedure (Liu and Richardson, 1985). Many approaches have been attempted to establish an experimental model without laparotomy (Senturk et al., 2010). Our model is one such approach that also has practical and specific applications.
In the corrosive esophagitis model of Gehanno et al., a surgical procedure is performed only at the lower end of the esophagus. In other models, this region is also considered the most important part for the purpose of application (Demirbilek et al., 1994; Koltuksuz et al., 2001) (Figure 4). This is because it was thought that this part of the esophagus sustained more harm from burns than did other parts. The most intense stenosis has been observed in the lower end of the esophagus because of its proximity to the stomach. Our model can also inflict burn wounds between the pharynx and the esophageal–stomach transition region. In other models, the chest must be opened surgically to create a wound near the pharynx. This approach is not desirable because of the difficulty of the operation. In our model, we can create burn wounds on each side of the esophagus without any surgical procedure.
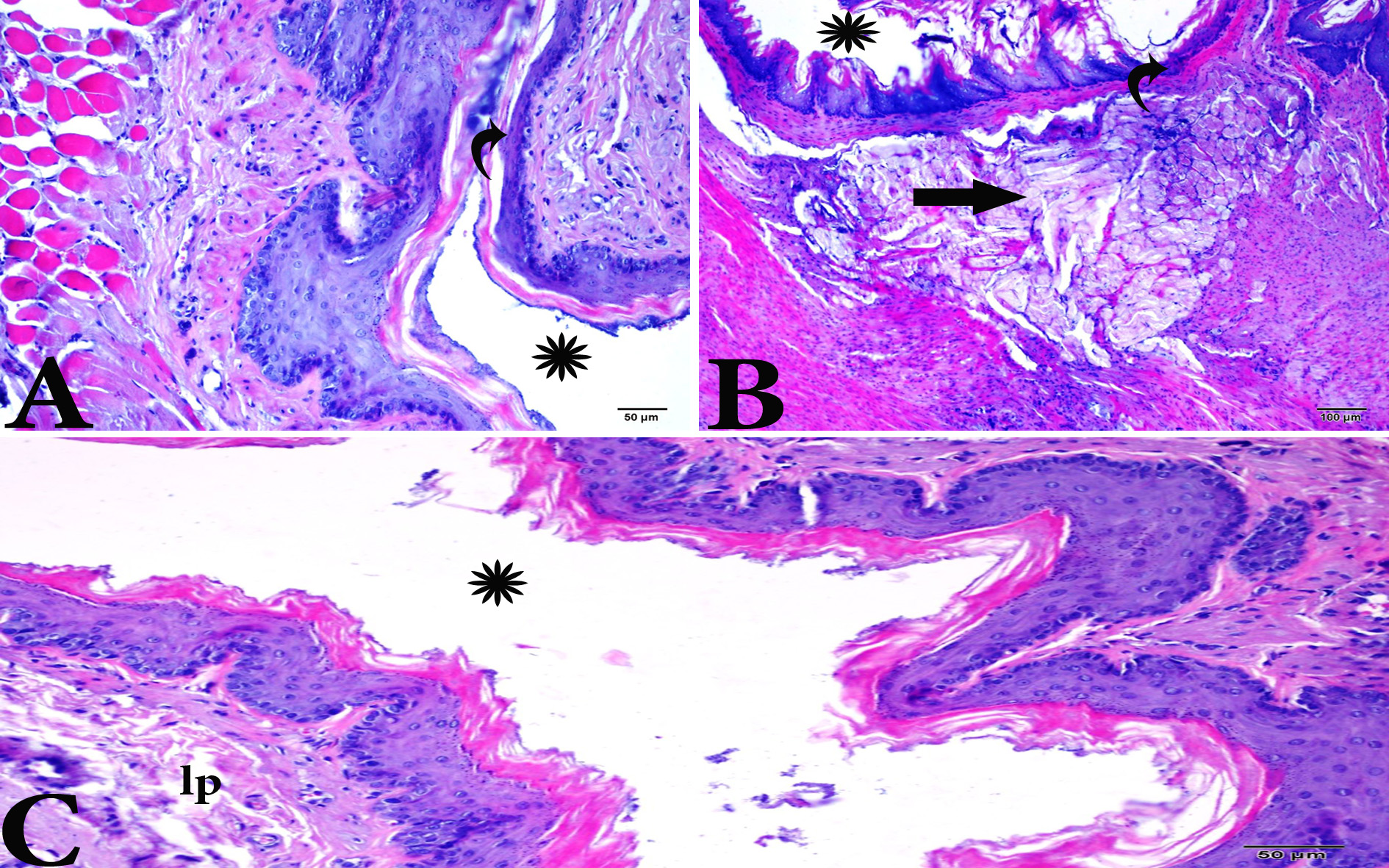
(a and b) Esophagus section of the study and (c) control group; (a) curved arrow: thinning of the epithelium, asteriks: esophagus lumen; (b) curved arrow: thinning of the epithelium, asteriks: esophagus lumen, arrow: hypertrophic and degenerative muscle cells; (c) asteriks: esophagus lumen, lp: lamina propria, hematoxylin–eosin stain, X10 and X20, 100 and 50 µm.
Senturk’s experimental model is different from other experimental burn studies using the rat model (Senturk et al., 2010). It has been presented as less invasive and very easily applicable. Although Senturk’s model shares aspects with ours, it also has drawbacks. One of them is simultaneous placement of the two catheters (Guide and Fogarty) into the esophagus. This tends to cause both pharyngeal damage and an undesired expansion in the esophageal volume at the end of the application, because total esophageal lumen volume is approximately 0.3–0.5 ml in male Wistar rats weighing 300–350 g. In Sprague Dawley male rats weighing between 375 and 400 g, the total length of the esophagus is approximately 9 cm, and the total volume of lumen is 0.4–0.7 ml (Koltuksuz et al., 2001; Liu and Richardson, 1985; Senturk et al., 2011).When NaOH is applied to the pharyngoesophageal section, liquid withdrawal requires insertion of the catheter upto the balloon. However, this can be difficult when 0.3 ml of liquid was introduced into the narrowing lumen of the esophagus, because the two catheters take up most of the esophageal volume of 3.5–4.5 mm. This may result in the fluid escaping into the lungs, which might cause pneumothorax. In our model, tracheal aspiration risk is lower than the other models.
Because of the hole’s location closer to the balloon, the flow of liquid is upward from the bottom. Therefore, the distal esophagus is exposed to the substance for much longer. This is the area of operation in the other models. Laparoscopic intervention is preferred at this region because of its easy application and burn wounds can cause more damage at this region.
The ideal application is to give slow and small doses in the form of instillation (Demirbilek et al. 1994). In different studies, NaOH solution (10–40%; Herek et al., 2010) was applied in the lumen between 60 s (Senturk et al., 2010) and 3 min intervals (Duman et al., 2011). In our study, NaOH solution was applied at a strength of 37.5% over a period of 60 s, and then the solution was aspirated. The burned area was irrigated with distilled water for 60 s.
Senturk’s experimental model uses a double catheter such as a Guide and Fogarty (Senturk et al., 2010). Some catheters were not siliconized, so they may cause irritation in pharyngoesophageal segments. In our model, the catheter is made of silicone and has two flexible tubes and thus does not have irritative properties. While a single catheter is easy for one person to introduce, two catheters are hard to fix and implement.
The gravity of corrosive esophagitis depends on the volume, concentration, and the type of the ingested material. The damage can lead to ulceration, bleeding, and perforation. As a rule, acids and alkalis are ingested, and there is no evidence-based standard therapy for these injuries. This user-friendly new method will give us the opportunity to find new treatment agents and modalities.
Our purpose was to develop a more secure and easier method of inducing esophageal injury in subject animals. This model can be used by anyone and is more practical and effective than other models. We think that our model is easier than the classical surgical method, because it does not require laparoscopic surgery under general anesthesia. All surgical models increase mortality and morbidity. They thus lead to a loss of time and economic resources because of the consumption of subject animals. In our study, the healing process can be shortened through prevention of extensive stenosis, and there is also a decrease in mortality and morbidity. Our model was applied more easily within a shorter period of time than other surgical models. Our model saves labor, money, and instruments.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.