
Abstract
The aim of this study is to report ophthalmic findings of acute mercury poisoning in 48 adults referred to emergency department. Full ophthalmologic examination including the best corrected visual acuity, external eye examination, reaction to light, a slit-lamp examination, funduscopy, intraocular pressure measurements, and visual field (VF) and color vision (CV) tests were performed at the presentation and repeated after 6 months. The parametric values of VF test, the mean deviation (MD), and pattern standard deviation (PSD) were recorded in order to compare patients and the 30 healthy controls. The mean parameter of color confusion index in patients was found to be statistically different than controls (p < 0.01). The MD and PSD in patients were different from controls statistically significant (p < 0.01 and p < 0.01, respectively). There was no correlation between the ocular findings and the urine and blood mercury levels. Methyl mercury, held in the school laboratory for experimental purpose, may be a source of poisoning. In this case series, we showed that acute exposure to mercury had hazardous effect on the visual system, especially CV and VF. We propose that emphasizing the public education on the potential hazards of mercury is crucial for preventive community health.
Introduction
Mercury toxicity in the eye results from a direct, accidental or occupational exposure and the systemic uptake of retinotoxic mercury compounds and their action on the retina and optic nerve (Bernhoft, 2012). Mercury enters the body through gastrointestinal tract, skin, or inhalation, and the most harmful effects are caused by inhalation route (Bernhoft, 2012; Mahajan and Sharma, 2011). Inhaled mercury is transported through the blood to various tissues and accumulates in there. The most potent effect is experienced on the neurological system and the eye because of their close proximity (Roels et al., 1982). The mercury has a short half-life in the blood due to its rapid distribution to many tissues, but its half-time in the body is about 2 months (Bernhoft, 2012; Mela et al., 2010). The mercury is absorbed through optic membranes or from the circulation. It accumulates and leads to local or systemic action in the vitreous (Bridges et al., 2007; Tanan et al., 2006). The ionic mercury, carried in the blood to the retina pigment epithelium, is distributed into photoreceptors, plexiform layer, and ganglion cells (Beuter and Edwards, 2004; Bridges et al., 2007; Toimela and Tähti, 2001; Warfvinge and Bruun, 2000). Since the earliest affected cells are scotopic cells, decreased night vision may be seen as the first clinical sign. In addition, other clinical signs such as decreased color vision and the contrast sensitivity, central visual impairment, and visual field constriction may appear subsequently (Bridges et al., 2007; Mahajan and Sharma, 2011).
Although there are numerous studies published on the chronic effects of mercury exposure on the visual system, there is no enough studies on the acute exposure. In this study, we aimed to determine the ophthalmologic findings in 48 adults exposed to acute mercury vapor.
Material and method
The study was approved by local ethics committee and conducted in accordance with the ethical principles described by Declaration of Helsinki. Informed consent was obtained from participants.
We evaluated ophthalmological findings in 48 subjects exposed to hazardous mercury levels and in 30 age- and sex-matched healthy controls for visual field and color vision test. The subjects were inhabitants of a small town located away from the city center. When the children heated mercury on the stove, the vapor dispersed into the air; they had been exposed to mercury vapor in their homes. Affected individuals were presented to the emergency department (ED), and mercury poisoning was diagnosed following a detailed anamnesis and examination, which were confirmed with positive laboratory results.
The initial ophthalmological examination was performed at presentation and repeated after 6 months. The ophthalmologic examination included best-corrected visual acuity, external eye examination, light response evaluation, a slit-lamp examination, fundoscopy, intraocular pressure measurements, and visual field and color vision tests. Initially auto refractometer measurement was performed in each participant, and those who have refractive error were corrected based on the results of best corrected visual acuity measurement that was evaluated with Snellen chart. Patients with previous eye diseases leading to visual impairment were excluded from the study.
A total of eight subjects with previous ocular, neural, and systemic diseases that might affect the visual system were excluded.
The visual field assessments were made using Humphrey visual field analyzer (Carl Zeiss Meditec, Dublin, California, USA). Central 24-2 SITA fast strategy protocol was used. The visual field test was performed for all of the patients. The tests that met the criteria for reliability parameters were recorded for interpretation. The data from the right eye were used for statistical analysis. The visual field test results of 43 (89.5%) patients in the study group and 28 (93%) participants in the control group were appropriate for evaluation. The mean parametric values of mean deviation (MD) and pattern standard deviation (PSD) were compared for each group.
Three patients with family history or aware of color-blindness were excluded. Color discrimination was evaluated with Anthony 15-D test. Color vision test was performed separately for each eye while closing the other eye. The participants with spectacles had them on during the examination. The color confusion index value of Anthony 15-D test was used for statistical analysis.
Independent sample t test was used to compare mean values, Pearson correlation test was used to evaluate the correlation between parametric values, and Spearman test was used in ophthalmic findings and mercury levels in blood and urine. p Values under 0.05 were accepted as significant. SPSS 17.0 for Windows was used for calculations.
Results
The study group consisted of 48 adults, 25 males and 23 females. The mean age was 45 ± 2.9 years. The control group consisted of 30 (15 males, 15 females) healthy volunteers and the mean age were 44.82 ± 2.36 years. There were no statistically significant differences based on the age and gender distributions between the groups (p = 0.472).
The average mercury level in subjects was found as 12.7 ± 7.3 (10–50) in blood and 304 ± 745 (25–4800) μg/L in urine, at the time of the first ophthalmological examination. N-acetylcysteine and chelation treatments were started. It was 2.3 ± 1.2 in blood and 564 ± 776 μg/L in urine, 1 week afterward. The mercury levels in blood and urine of all subjects were below the toxic level in the last ophthalmologic examination.
The decreased visual acuity was detected in 12 (25%) patients. Of the 12 patients, 6 had prior ophthalmic pathology, leading to decreased visual acuity and were excluded from the study. Remaining 6 (12.5%) patients had no evidence of previous ophthalmic disease. The visual acuity was found to be less than the mean two lines with standard Snellen chart in these patients, and the visual acuity did not change at the end of 6 months of follow-up. There was no correlation between the visual acuity and the blood and urine mercury levels (r = −0.128, p = 0.486 and r = −0.265, p = 0.598, Pearson test).
The study group’s mean intraocular pressure (IOP) was 14.24 ± 2.35 mmHg in the right eye and 15.09 ± 2.31 mmHg in the left eye. The mean IOP were found to be 16.49±2.14 mmHg in the right eye and 15.73±2.42 mmHg in the left eye, in the control group. There were no statistically significant differences in the mean IOP measurements between the groups. (p = 0.454). There were no pathologically high IOP levels at any time. Fundus examination revealed normal optic nerve, macula, and retinal vasculature.
The mean values of MD were −3.25 ± 1.9 in the study group and −2.46 ± 1.73 in controls and were found to be statistically significant (p < 0.01). The mean values of PSD were 2.60 ± 1.39 in the study group and 1.72 ± 1.02 in controls, and the difference was statistically significant (p < 0.001). The parametric values of visual field test were summarized in Table 1.
Comparison of affected and control groups.
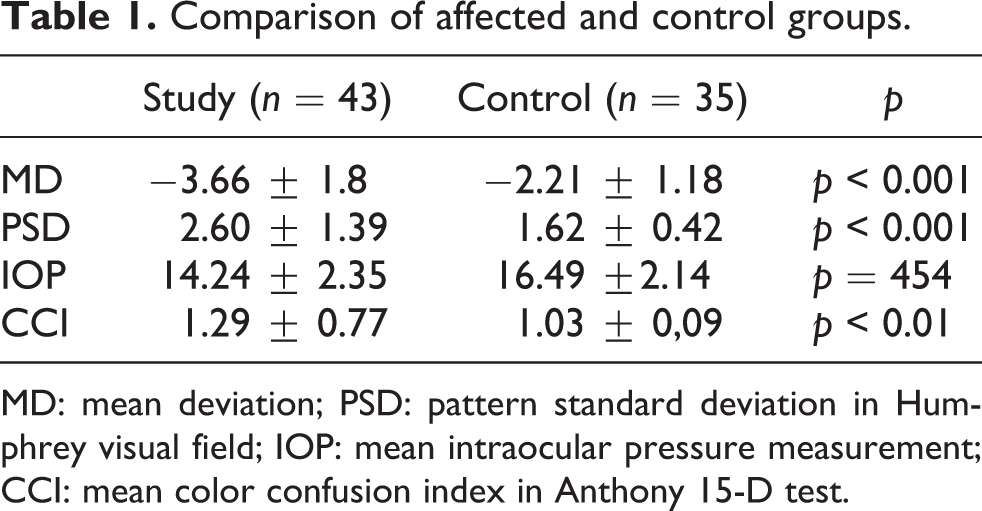
MD: mean deviation; PSD: pattern standard deviation in Humphrey visual field; IOP: mean intraocular pressure measurement; CCI: mean color confusion index in Anthony 15-D test.
Color vision was assessed with Anthony 15-D test. When the color confusion indexes of patients were compared to controls, there was statistically significant difference (p < 0.01, t test) (Table 1). , Using Anthony 15-D test, discromatopsia was found in 5 (10%) patients. There was no correlation between the color impairment and the blood and urine mercury levels (r = 0.351, p = 0.819, Spearman test). Those who had a positive family history or are aware of the own discromatopsia was determined as, respectively, 4 patients (8.3%) in the study group and 3 individuals (10%) in the control group, and they were excluded the study.
Discussion
Environmental exposure to mercury occurs though seafood consumption, waste incineration, energy production, and use of dental amalgam (Baughman, 2006; Gabal and Raslan, 1995). Children playing with mercury and its compounds could also be a source of exposure, as in the present study. Elemental mercury is in liquid form and can easily be obtained by children. They enjoy playing with mercury because of its attractive properties. Our study was an example that public, particularly children, are not aware about hazards of mercury on human health (Bose-O’Reilly et al., 2010) . A total of 48 adults exposed to acute mercury vapor were included in the present study. Eight of them had some complains such as abdominal pain, skin rash, arthralgia, limitation of movement, and nausea, but others did not have any symptoms. However, all people within the exposure area were evaluated at a health care facility and those who had mercury levels in blood and urine samples above the maximum acceptable value (tolerance limits) proposed by World Health Organization (WHO) were hospitalized (Bernhoft, 2012).
The most important point in mercury exposure is to diagnose poisoning earlier and to determine the source (Remø et al., 2011). In our study, mercury poisoning was detected early due to the clinician’s attention. Since an experiment regarding mercury was done in a school a week before, the source of contamination was discovered easily. The characteristics of the houses of the affected individuals and the winter season had important roles in poisoning. The houses were small and crowded. In addition, they were using burners for heating, and the doors and windows were kept closed for insulation. However, the early diagnosis of the poisoning, detection of the source, and transfer of the people from the contaminated area prevented widespread exposure by decreasing the contact time. The significance of the exposure time to toxic impact was demonstrated in various studies. The most important evidence of this was that most of the studies regarding the mercury poisoning were on chronic exposure. Besides the exposure duration, the concentration of mercury or the body level was important for the tissue damage. A study conducted in Iraq (Sabelaish and Hilmi, 1976) showed serious clinical symptoms associated with excessive exposure to mercury, in 1972. However, clinical symptoms unrelated to the duration of exposure were observed in men mentioned in that study. On the other hand, even some family members living together and exposed to the same amount of mercury did not show any ophthalmologic symptoms, but others were affected severely, leading to blindness. The variety of the clinical symptoms point to the personal sensitivity differences and various degrees of effect can be observed even at similar exposures. There were no correlation between the mercury levels and ophthalmologic examination findings in our study. Besides, similar studies regarding the chronic exposure did not demonstrate any association between body mercury level and the symptoms (Lansdown, 2011; Rustagi and Singh, 2010). It is also reported that the findings from one eye might not be the same with the other, so it is recommended to evaluate each eye separately.
One of the family members from the study group was affected more than the other family members. That family had also very high level of mercury in their body. Their mercury level in urine was also very high and it was found to be up to 4800 md/L in some patients. Two of them were hospitalized for 2 weeks and one was hospitalized for 1 month. Although the central vision and color vision tests of these patients were normal, a generalized constriction was detected in the visual field test.
Lack of ophthalmologic signs prior to the exposure and subjective nature of the signs are some of the disadvantages of this study. However, there was a statistically significant difference between the two groups. The number of patients with ophthalmological signs was small, and they were minimally affected. When the cases were reevaluated in 6 months, the mercury levels were below the toxic level, however visual signs persisted.
The visual field test shows the damage of retinal ganglion cells and visual pathways, from optic disk to occipital cortex. Even if the central vision is not affected, it can give information about the peripheral vision (Bridges et al., 2007; Herba et al., 2004). The visual field test is an indispensable diagnostic tool for glaucoma and optic nerve disease. It can also be used in the diagnosis of drug intoxications (Bridges et al., 2007; Herba et al., 2004; da Costa et al., 2008).. However, the test is subjective and the test results may be affected due to patient compliance. Moreover, test outcomes are based on the probability as related to the presence of damage. Each parameter of visual field test showed statistically significant differences in the individuals exposed to mercury vapor compared with healthy control. The visual field test shows abnormality in the retina and optic nerve damage, causing the nervous system defects. Korogi et al (1997) reported that the range of visual field might correlate with the degree and extent of atrophy in striate cortex on magnetic resonance images.
Ishihara test is an important test to demonstrate the hereditary color blindness. The Ishihara pseudoisochromatic plates are probably the most frequently used test for screening red–green defects especially the congenital types (Dain, 2004). However, the test is not capable enough to discover blue-color defects. Therefore, we used Anthony 15-D test in this study. In all, Eight patients were determined for color vision impairment test. However, three of these patients either had a positive family history or were aware of their situations. Other six patients did not have any medical history regarding color vision, and this impairment was mostly on the blue–green band. Although central vision was normal, visual field defect was detected in three patients with color blindness concurrently, but there were no statistical correlation between two situations. Irreversible color vision loss has been reported in previous studies in chronic mercury exposure (Feitosa-Santana et al, 2008 and Feitosa-Santana et al, 2007). Jedrejko and Skoczyńska (2011) reported that there was borderline corresponding to the early stage of developing dyschromatopsia type III in the men employed in a chloralkali plant. Even though the right eye was more affected, the level of urinary mercury and the duration of exposure were not found to be correlated with the color confusion indexes in the mentioned study. In conclusion, mercury is a toxic metal that can accumulate and cause irreversible damage in all tissues. Based on the ophthalmological findings, it was noted that central vision, color vision, and visual field were minimally affected. Even though it was an important disadvantage to use subjective methods for obtaining the clinical findings, the significant differences found compared to the control group support the theory regarding harmful effects of the mercury on the eye. Since the mercury is easily accessible and has an attractive nature, it is a potential public hazard for more vulnerable children and for people living around them. It is important to inform the children regarding the harmful effect of mercury and to keep the mercury secure in the school laboratories.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.