
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has created widespread disruption in individuals’ personal and occupational lives all around the world. Vacationers and tourism, recreation, and leisure employees were among those who experienced substantial disruption. Cruise ships, especially, faced turmoil on a global scale for both their customers and workers. COVID-19 outbreaks were reported on cruise ships beginning in February 2020, presenting new and unique challenges for the industry. Conditions on cruise ships, including close and frequent contact between passengers and crew members, use of common areas, the confined nature of the vessels, and gathering of passengers from different countries, aided in transmitting the disease both onboard and in the community. As the pandemic evolved, federal and state governments and industries worldwide, including cruise ship companies, developed response plans. In this article, we provide a high-level overview of the US government and cruise ship industry’s response to the COVID-19 pandemic, as well as a brief commentary on lessons learned, and recommendations for the cruise ship sector going forward. The outlined suggestions may be used as a starting point to increase emergency preparedness and to inform outbreak response plans in the event of future infectious disease outbreaks.
Introduction
Over the past few months, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19), has quickly spread across the world, leading to major personal and professional disruption. The spread of SARS-CoV-2 to several continents and dozens of countries prompted the World Health Organization (WHO) to declare a global pandemic (WHO, 2020a). In addition, the onset of COVID-19 has resulted in the deaths of hundreds of thousands of people globally. Specifically, in the United States, as of September 2, 2020, the COVID-19 pandemic has resulted in over six million cases and approximately 184,000 deaths (CDC, 2020a).
Based on current scientific understanding, the virus is believed to be transmitted from person-to-person primarily via respiratory droplets and secretions, as well as through contact with contaminated surfaces (Abebe et al., 2020; WHO, 2020b). Recent evidence has suggested that airborne transmission may also play a role in spread; however, the extent of that role is currently unknown and requires further investigation (WHO, 2020b). In addition, presymptomatic and asymptomatic individuals can shed the virus, further complicating transmission control (Abebe et al., 2020). Limited testing and difficulty in monitoring mild, presymptomatic, and asymptomatic cases have created distinct challenges for case management, contact tracing, and adequate care for COVID-19 patients. The novelty of the virus, combined with the variation in pandemic response across countries, has illuminated gaps in infection control preparedness across governments and industries worldwide.
Cruise ships, in particular, have been heavily affected by the COVID-19 pandemic, resulting in an industry-wide halt in their US operations. Historically, cruise ships have managed and controlled occasional gastrointestinal (GI) and respiratory disease outbreaks, including common pathogens, such as norovirus, hepatitis E, influenza A and B, Escherichia coli, Salmonella enterica, Shigella, Legionella, and other viral, bacterial, and parasitic pathogens (Bert et al., 2014; Kak, 2015). The cruise ship environment, including passengers in close and confined quarters, cohabitation of common areas, consistent contact between passengers, and contact between passengers from different geographical regions, can facilitate infectious disease spread (Kak, 2015; Moriarty et al., 2020). These factors, along with the infectious nature of SARS-CoV-2, create susceptible conditions for rapid transmission and infection. Further, cruise ships typically have a large population of passengers over the age of 65, who are more vulnerable to infection, which may result in a higher proportion of severe cases among infected individuals onboard (Mallapaty, 2020; Moriarty et al., 2020).
To date, COVID-19 outbreaks have occurred across a range of different cruise ships. On February 1, 2020, the first COVID-19 case was detected on the Diamond Princess off the coast of Japan (Mallapaty, 2020). Reported cases of COVID-19 on the Grand Princess off the coast of California followed on March 6, 2020 (Moriarty et al., 2020). By mid-March, at least 25 more cruise ships reported confirmed COVID-19 cases (Moriarty et al., 2020). Recently, the Centers for Disease Control and Prevention (CDC) reported that 99 COVID-19 outbreaks occurred on 123 different cruise ships in the US jurisdiction between March 1, 2020, and July 10, 2020, totaling 958 confirmed and 2015 suspected COVID-19 cases (CDC, 2020b). Following disembarkation, secondary community-acquired COVID-19 cases associated with cruise ship passengers were also reported to the CDC (Moriarty et al., 2020).
In this article, we briefly explore the government and cruise ship industry’s approaches to controlling SARS-CoV-2 transmission, potential opportunities for improving the infection control response, lessons learned in the context of the COVID-19 pandemic, and future considerations. Our primary goal is to provide broad commentary on the key takeaways from COVID-19 outbreaks on cruise ships and to highlight several recommendations for reducing the risk of a future disease outbreak on cruise ships.
US government oversight of infectious diseases on cruise ships: The Vessel Sanitation Program
The CDC currently oversees, monitors, tracks, and provides training on infection control in the cruise ship industry through the Vessel Sanitation Program (VSP). The VSP was established in 1975 with the specific mission to “prevent and control the introduction, transmission, and spread of GI illnesses on cruise ships” through increased sanitation efforts (CDC, 2020c; Kak, 2015). This program was developed in response to typhoid fever, shigellosis, and acute gastroenteritis cases on cruise vessels in the early 1970s (Kak, 2015). Cruise ships that carry 13 or more passengers and include the US ports on their itinerary fall under the VSP’s jurisdiction (CDC, 2019). As part of the VSP, the CDC inspects cruise ships, monitors GI illnesses, investigates outbreaks, trains cruise ship employees on public health practices, and provides health information to stakeholders (CDC, 2019; Kak, 2015).
Cruise ships’ medical centers, potable water systems, galleys and dining rooms, swimming pools and whirlpools, housekeeping, pest and insect management, child activity centers, and heating, ventilation, and air conditioning systems are inspected twice per year during periodic unannounced operation sanitation inspections (CDC 2018a, 2020d; Kak, 2015). As part of the inspection process, vessels are scored on the following topics, and scores are posted on the VSP website: water sanitation, food handling and preparation, personal hygiene and sanitation practices by ship staff, pool and spa sanitation, potential for food and water contamination and disinfection, and general cleanliness (CDC, 2020d; Kak, 2015). Additionally, cruise ships are required to report cases of GI symptoms and illness and onboard deaths to the VSP (CDC, 2018b; Kak, 2015). The VSP monitors these notifications and conducts epidemiological and environmental investigations when at least 3% of a ship’s passengers or crew members report GI symptoms (CDC, 2018c; Kak, 2015). Furthermore, the VSP provides training to cruise ship staff on topics included in the VSP operations manual, including food safety, potable water protection, environmental sanitation procedures, and GI illness surveillance and outbreak investigations (CDC, 2018a, 2018d).
In light of the COVID-19 pandemic, there are opportunities for the VSP to expand its scope to incorporate risk mitigation techniques and monitoring for established and emerging (e.g. COVID-19) respiratory illnesses. The existing VSP framework is ideal for developing guidance for respiratory infectious diseases. Updated guidance and an expansion of the VSP would include inspection procedures, surveillance, outbreak investigations, training, and communications targeted to respiratory illnesses. In summary, the current VSP provides sound structure and a unique opportunity for cruise ships to prepare for, and respond to, future infectious respiratory disease outbreaks.
US government and industry response to the COVID-19 pandemic
Government responses to the COVID-19 pandemic have varied widely between nations. In the United States, the CDC’s first response occurred on February 21, 2020, when it recommended that individuals avoid cruise ship travel in Southeast Asia. On March 8, 2020, it expanded its recommendation to include all cruise ship travel for individuals over the age of 65 and those with underlying health conditions (Moriarty et al., 2020). The following week, on March 15, 2020, the CDC distributed a recommendation through the Health Alert Network that “all persons defer any travel on cruise ships, including river cruises, worldwide because of the increased risk of SARS-CoV-2 transmission onboard ships” (CDC, 2020e). The notice was updated on March 17, 2020, to include advice regarding in-cabin isolation for affected patients and the 14-day quarantine following the completion of a cruise voyage (CDC, 2020e). This recommendation is consistent with the CDC’s level 3 travel warning for cruise ships, originally released on March 17, 2020 (CDC, 2020f).
In addition, the Cruise Lines International Association (CLIA), the leading industry trade group, voluntarily suspended cruise ship operations from the US ports of call beginning on March 13, 2020 (Moriarty et al., 2020). The voluntary suspension of cruise operations from the US ports was continued on June 19, 2020, until September 15, 2020 (CLIA, 2020a). More recently, the CLIA extended the voluntary suspension on August 5, 2020, until at least October 31, 2020 (CLIA, 2020b).
On March 14, 2020, the CDC director issued a No Sail Order for cruise ships (CDC, 2020g). For this order and future orders discussed below, note that the CDC orders apply to: “All commercial, noncargo, passenger-carrying vessels operating in international, interstate, or intrastate waterways and subject to the jurisdiction of the United States with the capacity to carry 250 or more individuals (passengers and crew) with an itinerary anticipating an overnight stay onboard or a twenty-four (24) hour stay onboard for either passengers or crew” (CDC, 2020g: 1).
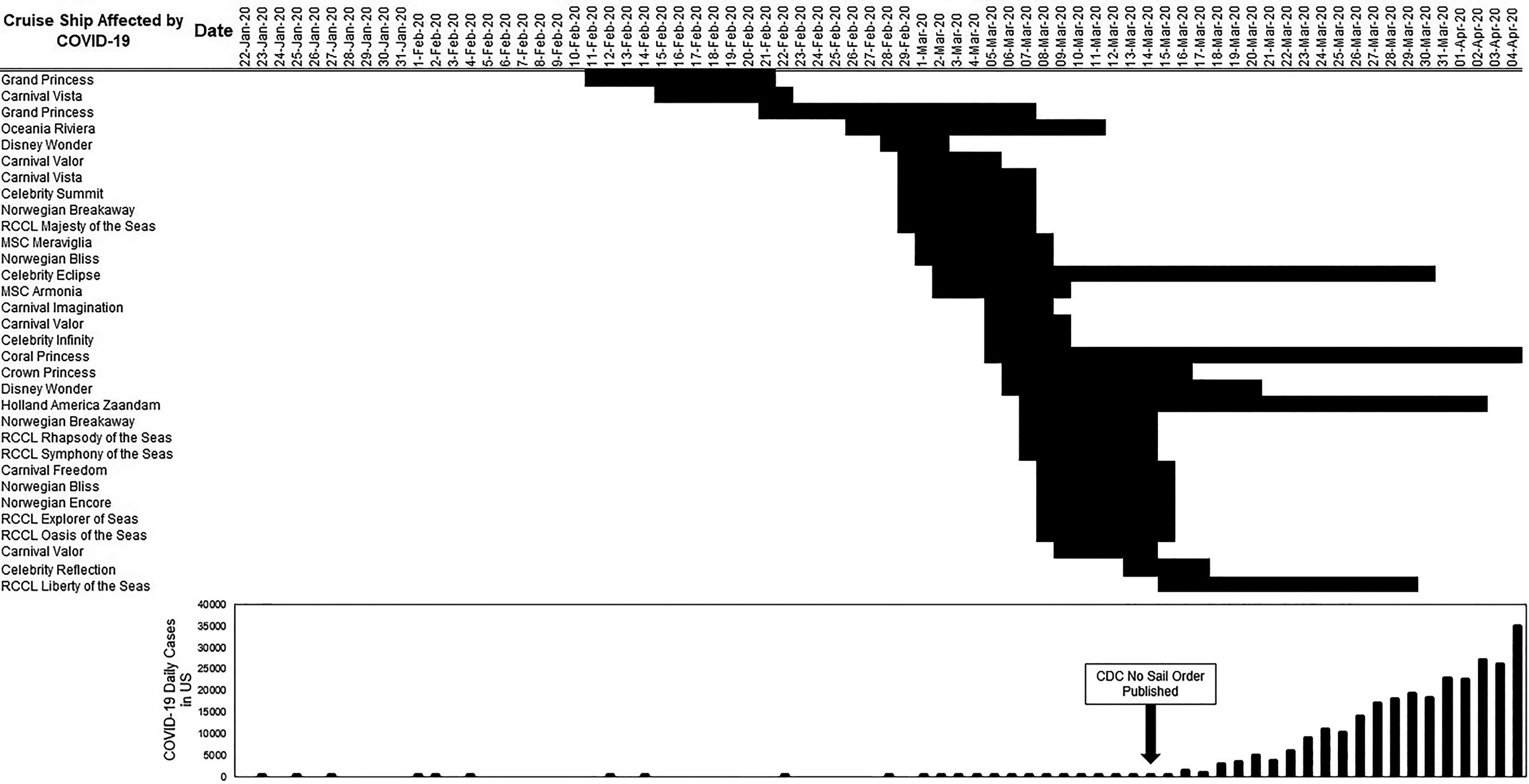
Timeline showing cruise ship travel dates affected by COVID-19, relative to the daily incidence of COVID-19 in the US. Black shaded dates represent voyage dates. Figure adapted from CDC data on cruise ships affected by COVID-19 (travelers testing positive for COVID-19 onboard and/or 14 days after disembarking) and daily case counts of COVID-19 in the United States (CDC, 2020a, 2020i). COVID-19: coronavirus disease 2019; CDC: Centers for Disease Control and Prevention.
Following the mid-April extension of the No Sail Order, the CDC also released interim guidance for mitigating COVID-19 among cruise ship crews during the period of the No Sail Order (CDC, 2020j). This interim guidance covers important topics, including preventative measures, COVID-19 surveillance, crew monitoring, disembarking asymptomatic crew for transfer or repatriation, isolation of symptomatic crew and confirmed cases, quarantine of close contacts of symptomatic or confirmed cases, medical management of suspected or confirmed COVID-19 cases, disembarking crew members to obtain medical care, discontinuation of isolation and quarantine, cleaning and disinfection, and a COVID-19 color-coding system for cruise ships. Several additional interim CDC guidance documents went into more detail on different aspects of risk mitigation, such as case management. Currently, the CDC interim guidance documents are the most comprehensive guidance documents released for COVID-19 guidance in the cruise ship industry within the United States. The timeline of the US government and CLIA’s response to the COVID-19 pandemic is outlined in Figure 2.
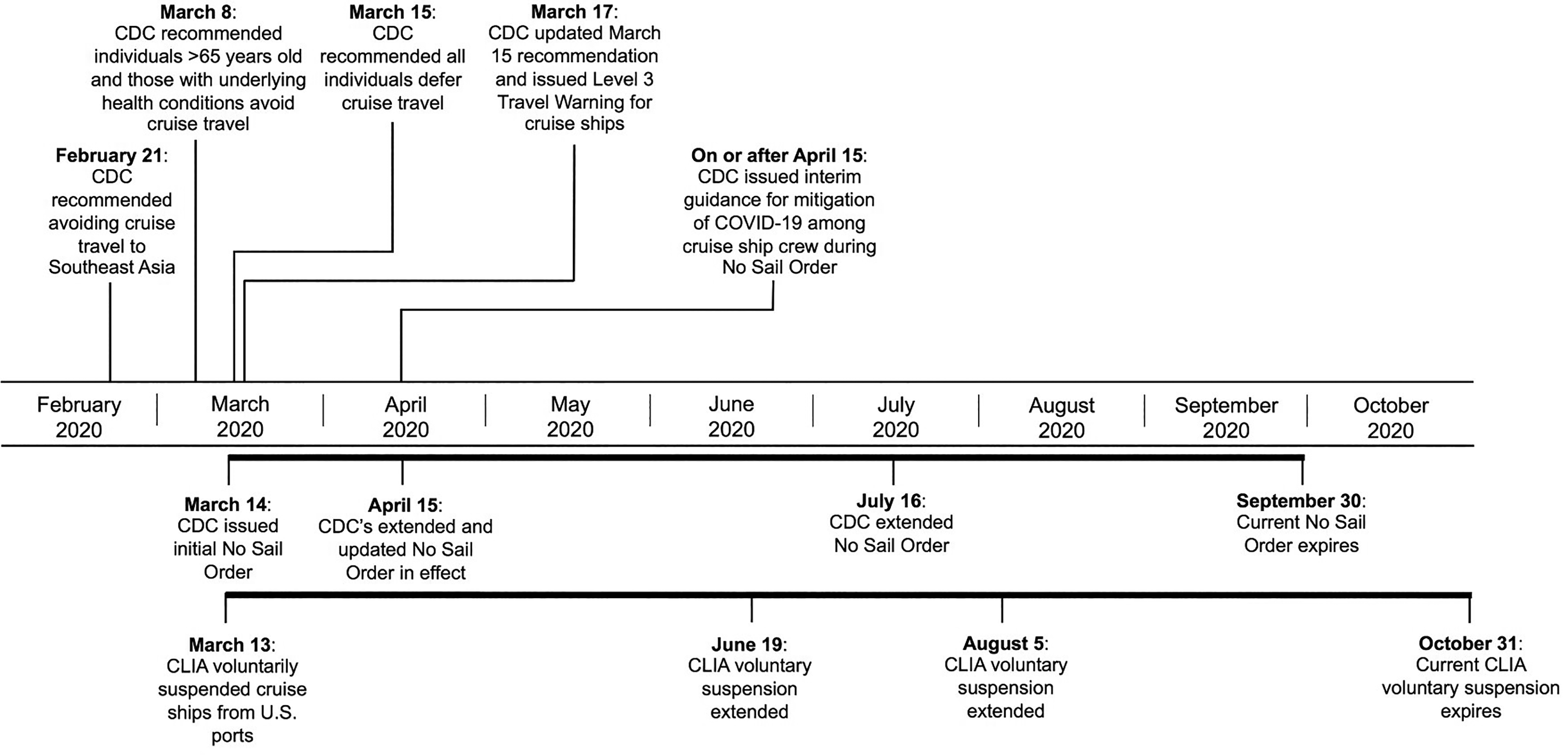
Timeline of the US government and CLIA’s response to the COVID-19 pandemic (current through September 2, 2020). Dates above the timeline represent recommendations initiated at single points in time. Bars below the timeline represent government (CDC No Sail Order) and industry (CLIA voluntary suspension) action over periods of time. COVID-19: coronavirus disease 2019; CDC: Centers for Disease Control and Prevention; CLIA: Cruise Lines International Association.
Lessons learned from the COVID-19 pandemic
Cruise ship responses to early outbreaks of COVID-19
The US government and industry orders have provided guidance for managing COVID-19 outbreaks in the cruise ship industry. However, some cruise ships experienced outbreaks prior to the execution of these orders. The Diamond Princess and Grand Princess, for example, had early COVID-19 outbreaks, and, as a result, response plans were developed under rapidly evolving circumstances. Both outbreaks serve as examples of early infection control response in the industry.
Upon the first confirmed COVID-19 case on the Diamond Princess, passenger and crew health was evaluated by questionnaire, and more than 3000 tests were performed on passengers (Dahl, 2020; Mallapaty, 2020). Older and symptomatic passengers, crew, and close contacts were tested first, and some passengers were tested multiple times (Dahl, 2020; Mallapaty, 2020). Four days after the first positive COVID-19 detection, passengers were quarantined in their cabins for 14 days (Mallapaty, 2020). COVID-19 cases initially increased during quarantine, which may be due in part to shared cabin spaces and crew members who continued to perform essential duties (Dahl, 2020). One study estimated that the basic reproductive number decreased from seven to one during the quarantine (Mallapaty, 2020). Another study approximated the initial basic reproductive number onboard the ship as 14.8, which declined and stabilized at 1.78 after the quarantine was initiated (Rocklöv et al., 2020). These results highlight the importance of rapid testing and quarantining of individuals on a cruise ship when an outbreak occurs. Instituting these measures in a timely manner creates separation between individuals and consequently disrupts disease transmission.
Recently, Plucinski et al. (2020) surveyed and analyzed specimens from American passengers on the Diamond Princess, and found the highest virus attack rate (AR) for passengers with at least one symptomatic SARS-CoV-2 positive cabinmate (81%), followed by those with at least one asymptomatic SARS-CoV-2 positive cabinmate (63%), and the lowest AR for individuals in single-person cabins or cabins without any SARS-CoV-2 positive cabinmates (18%). The authors noted that while the quarantine of passengers onboard likely prevented many new cases, it did not preclude intracabin transmission (Plucinski et al., 2020). Therefore, if COVID-19 is detected on embarked ships, warranted responses that may further reduce transmission onboard include widespread testing of asymptomatic individuals and implementing strategies to limit transmission between cabinmates.
Community transmission is a concern for cruise ships, as disembarked passengers use various modes of travel to return to their homes. As part of the response to the Diamond Princess COVID-19 outbreak and subsequent community spread, the US tried to mitigate community transmission by implementing travel restrictions for persons and cruise ships, infection prevention and control measures, disinfection plans onboard the ships, communication to health departments, and contract tracing (Moriarty et al., 2020). These measures helped reduce the likelihood of community transmission by targeting the source of the outbreak and discouraging the movement of passengers and crew members who may have been exposed, thus underscoring the importance of repatriated passengers following government recommendations for quarantine.
Following reports of confirmed COVID-19 cases among disembarked passengers from the Grand Princess, symptomatic passengers and crew members were tested for SARS-CoV-2 and self-quarantined in their cabins, and public dining was replaced by room service (Moriarty et al., 2020). Upon docking in Oakland, California, passengers were quarantined on land for 14 days and were offered SARS-CoV-2 tests (Moriarty et al., 2020). Again, implementing testing and quarantining and closing public gathering spaces on the ship reduced contact among passengers and crew members, and therefore, were instrumental at limiting the disease spread onboard. Further, the additional land-based quarantine and extensive testing following disembarkation helped limit interactions between passengers and community members, and thereby, curbed the spread of infection into communities.
Future considerations for the cruise ship industry
Throughout the course of the pandemic, the novelty and infectiousness of SARS-CoV-2 have presented challenges for maintaining the health and safety of passengers and crew members onboard cruise ships. To increase outbreak preparedness and infection control response, several recommendations for the cruise ship industry, as well as a high-level discussion, are included below.
Prevention through design
Both cruise ship layout and extended sea voyages help to create an environment that allows for infectious disease spread among passengers and crew, should an outbreak occur. As cruise lines continue to create larger ships with greater capacity, the risk of disease transmission onboard may increase. The risk of an outbreak on a cruise ship may be mitigated or reduced by “designing out” hazards or implementing engineering controls when hazards are unable to be “designed out.” The concept of anticipating workplace hazards and configuring the work environment (e.g. a cruise ship) to “design out” the hazards is known as prevention through design (PtD). This paradigm is advocated by the US National Institute for Occupational Safety and Health. PtD techniques can be applied during vessel design, construction, and retrofitting.
The PtD approach can be used to control cruise ship capacity. Passenger and crew member reduction would allow for social distancing guidelines to be implemented and would discourage large gatherings onboard vessels. To achieve this goal, architects and engineers may consider creating fewer and larger cabins, more dining areas with fewer seats, and redesigning other shared spaces to accommodate fewer people and increase personal space. Additionally, future cruise ships can be designed to automate select crew tasks and responsibilities to decrease the number of crew onboard without compromising safety. Cruise ship design plays an important role in limiting the number of individuals onboard and therefore can be leveraged to help reduce disease spread.
In addition, incorporating improved engineering controls (e.g. ventilation) throughout vessels can help mitigate disease transmission risk. According to the hierarchy of controls, if the hazard is unable to be eliminated or substituted, engineering becomes the preferred control method. Optimized ventilation, for example, may reduce transmission risk on a cruise ship by limiting recirculating air, allowing more dilution with outdoor air, and applying filtration (e.g. high efficiency particulate air filters). Engineering controls such as these can be implemented at any ship construction stage, including retrofitting existing ships.
Disease monitoring and surveillance
In addition to rethinking the design and layout of vessels, the cruise ship industry can increase disease monitoring and surveillance programs. Wastewater-based epidemiology (WBE) may serve as a surveillance tool for cruise ships in the future. Many documented preprint studies have correlated the RNA viral concentration at water treatment facilities as a predictor of detected COVID-19 cases within a community (Nemudryi et al., 2020; Wu et al., 2020). If scaled and validated properly, an onboard WBE program for SARS-CoV-2 may act as an early indicator for a potential outbreak or presence of SARS-CoV-2 onboard a cruise ship.
Additionally, as part of the VSP, cruise ships are required to report onboard GI symptoms and illnesses, which are then monitored, and may trigger an outbreak investigation. Establishing a protocol for reporting, monitoring, and investigating cases of respiratory symptoms and disease onboard vessels can help workers quickly implement infection control measures and limit transmission.
Multilayered risk management
Lastly, cruise lines should create a multilayered risk management approach for infectious diseases to ensure that there is no single point of failure. The VSP overseen by the CDC represents an applicable and longstanding framework that can be further optimized to address COVID-19 and other pathogen-caused respiratory illnesses. Crew members, for example, are currently trained on how to handle GI illness outbreaks via the VSP. An expanded training program could help crew members built upon their foundational knowledge and equip them with the tools needed to mitigate respiratory illness outbreaks onboard cruise ships. Further, key stakeholders in the cruise ship business, including trade groups, industry leaders, infection control experts, and government agencies, could work together to develop more extensive emergency plans that would ensure effective outbreak response onboard vessels and onshore assistance at ports.
Conclusion
The emergence of SARS-CoV-2 and the subsequent COVID-19 pandemic has posed new challenges for governments and industries worldwide, including cruise lines. Cruise ships operate under unique circumstances that may promote the spread of infectious disease through contributing factors, such as close and frequent contact between passengers and crew members, many shared spaces, and an international passenger population. In response to COVID-19, cruise ships and the CDC implemented swift protection measures to prevent COVID-19 spread, including No Sail Orders and comprehensive interim guidance. Moving forward, more robust preventative measures should be considered to mitigate risk and increase preparedness for future disease outbreaks. These measures include a multitude of planning, design, hygiene, and surveillance interventions that aim to increase safety for all passengers and crew onboard cruise ships. By learning and evolving from the current pandemic, the cruise ship industry has an opportunity to make a long-lasting and impactful change regarding infection control, potentially saving lives in the process.
Footnotes
Authors’ note
Alexander Sundermann is no longer affiliated with Cardno ChemRisk, Pittsburgh, PA, USA.
Author contributions
Two of the authors (RKB and CB) are currently employed by Cardno ChemRisk and one author (AS) was formerly employed by Cardno ChemRisk, a consulting firm that provides scientific advice to the government, corporations, law firms, and various scientific/professional organizations. Cardno ChemRisk scientists have been engaged by numerous companies to provide COVID-related toxicology, epidemiology, and industrial hygiene health and safety advice. CB has served as a contributor to the AIHA Back to Work Safely Task Force by drafting industry-specific guidance for businesses and consumers to safely reopen after emerging from COVID-19 shelter-in-place/quarantine. The time invested by these three authors to write this article was provided by their employer.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.