
Abstract
Silicon is one of the most monitored elements in extractables and leachables studies of pharmaceutical packaging systems and related components. There is a need to review and evaluate toxicological thresholds of silicon because of its direct contact with drug products (DP) especially a liquid form of DP with the widely used pharmaceutical packaging systems made of silicon materials like glass and silicone. It is required by regulatory authorities to test silicon content in DP; however, there are no official guidelines on the toxicology of silicon that are currently available, yet the knowledge of toxicological thresholds of silicon is critical to justify the analytical limit of quantification (LOQ). Therefore, we reviewed the toxicity of silicon to derive a toxicological threshold by literature review of toxicity studies of both inorganic and organic silicon compounds. Oral toxicity is low for inorganic silicon like silicon dioxide or organic silicon polymers such as silicone tube/silicone oil (polydimethylsiloxane, or namely, PDMS as the major ingredient). In comparison, inhalational toxicity of silicon dioxide leads to pulmonary silicosis or even lung cancer. When orally administered, the toxicity of silicon dioxide, glass, polymers, or PDMS oligomers varies depending on their morphology, molecular weight (MW), and degrees of polymerization. PDMS with high MW has minimal toxic symptoms with non-detectable degradation/elimination by both intraperitoneal and subcutaneous administration routes, while exposure to either PDMS or small molecule dimethyl silicone compounds by the intravenous administration route may lead to death. We here determined a general parenteral permitted daily exposure (PDE) of 93 μg/day for inorganic silicon element and 100 μg/day for organic silicon element by reviewing toxicological data of both forms of silicon. In conclusion, this work provides evidence for pharmaceutical companies and regulatory agencies on the PDEs of silicon elements in pharmaceutical packaging and process components through a variety of administration routes.
Introduction
Element silicon (Si) is commonly regarded as a virtually safe element by the vast majority when exposed orally in our daily life. For pharmaceuticals, silicon in drugs can be administrated via routes other than oral intake (PDA, 1988; Zhao et al., 2014). As the mandatory requirement to conduct extractables and leachables studies, occasionally high levels of silicon compounds either as inorganic silicon or organosilicon compounds can be found in drug products. However, there is no official safety threshold for silicon in ICH Q3D Guideline for Elemental Impurities and also no standard is available for a permitted daily exposure level for silicon exposure via parenteral drug products and orally inhaled nasal drug products (ONIDP). (Colas et al., 2004; Jones et al., 2005; Mundry, 1999). No official guidelines are currently available; yet, it is required to justify the analytical limit of quantification (LOQ) of silicon with comparisons to the toxicological threshold of silicon by the Center for Drug Evaluation (CDE) of National Medical Products Administration (NMPA).
There have been plenty of animal toxicity experiments for silicon-containing inorganic and organic extracts through oral administration routes. However, the toxicity of silicon for the parenteral route of administration has not been reviewed. It is necessary to set a parenteral permitted daily exposure (PDE) value for silicon to supplement ICH Q3D (ICH Q3D, 2019) and EMA metal catalyst and reagent guide (EMA, 2008).
Since there are many types of organic and inorganic silicon compounds and polymers, a toxicological threshold of silicon to cover risks for most silicon compounds seems to be challenging but emerging. Meanwhile, the toxicity of silicon has been impacted by a large numbers of variables, most of which are the distributional consistency of three-dimensional arrangement of silicon molecules (crystalline vs non-crystalline), crystal structure system, molecular weight, etc.. Currently, there are very limited toxicological studies to show conclusive trends of effects from each one of these factors since the materials (for instance, glass or silicone polymers) themselves, in a lot of cases, are mixtures. Another challenge to this work is to understand the toxicological effects from some of these factors by reviewing toxicological animal studies conducted in different laboratories and exposed to mixtures of inorganic silicon or organosilicone.
This review used toxicological risk assessment as a tool to discuss the above issues from four aspects as follows: hazard definition, dose-toxicity relationship, exposure assessment, and risk characterization. It provided evidence and references for pharmaceutical industry and regulatory agencies on the PDEs of silicon elements through a variety of administration routes by literature review of toxicity studies of both inorganic and organic silicon compounds closely related to materials of pharmaceutical packaging and process components.
Methods
Data collection
In order to estimate the PDE for element silicon of oral, parenteral and inhalation, a thorough literature search was performed on Google, Google scholar, and Web of Science using the keywords or their combinations as follows: pharmaceutical, toxicity, toxicological risk assessment, intravenous, inhalation, oral, in vivo, in vitro; crystal, amorphous, colloidal, inorganic silicon, silica, silicon dioxide, glass, ampoules, particles, shedding, delamination; silicone elastomer, silicone fluid, silicone oil, tubing, polydimethylsiloxane, oligomers, siloxanes.
Variables analysis
There are many physical and chemical factors may affect toxicity of a silicon compound, and the most critical ones discussed in this work are listed below: 1) Route of administrations (oral, parenteral, inhalation), 2) Inorganic compounds versus organic compounds, 3) For inorganic compounds, a. Distributional consistency of three-dimensional arrangement of silicon molecules (crystalline, non-crystalline). b. Crystal structure system (quartz, cristobalite, tridymite, etc.). c. Particle size, 4) For organic compound, a. Molecular weight (large organic polymers such as polydimethylsiloxane vs small molecules such as the most commonly detected D3, D4, D5, hexamethyl disiloxane, etc.). b. Molecular structure (linear, cyclic, etc.).
Model development and data computation
PDE model per ICH Q3C is listed here (ICH Q3C, 2017), and all PDE were calculated according to equation below unless otherwise noted.

The Weight Adjustment assumes an arbitrary adult human body weight for either sex of 50 is in ICH Q3C.
Refer to ICH Q3C for the uncertainty factors for F1, F2, F3, F4, and F5. F1: A factor to account for extrapolation between species. F2: A factor of 10 to account for variability between individuals. F3: A variable factor to account for toxicity studies of short-term exposure. F4: A factor that may be applied in cases of severe toxicity. F5: A variable factor that may be applied if the no-effect level was not established. Other than F1 to F5, an additional factor F6 for bioavailability would be also used here. It is optionally used for route extrapolation when necessary. The value selection principles can be found in ICH Q3D.
The corresponding PDE for silicon element can be calculated according to equation below:
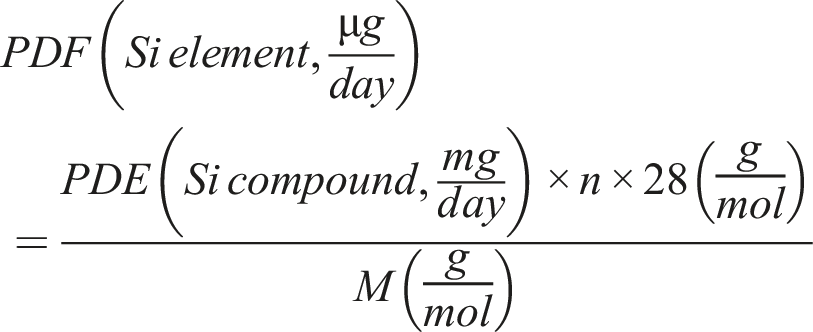
Results
Inorganic silicon compounds in pharmaceutical packaging and process components (exposure assessment study)
Glass
The main components of glass.
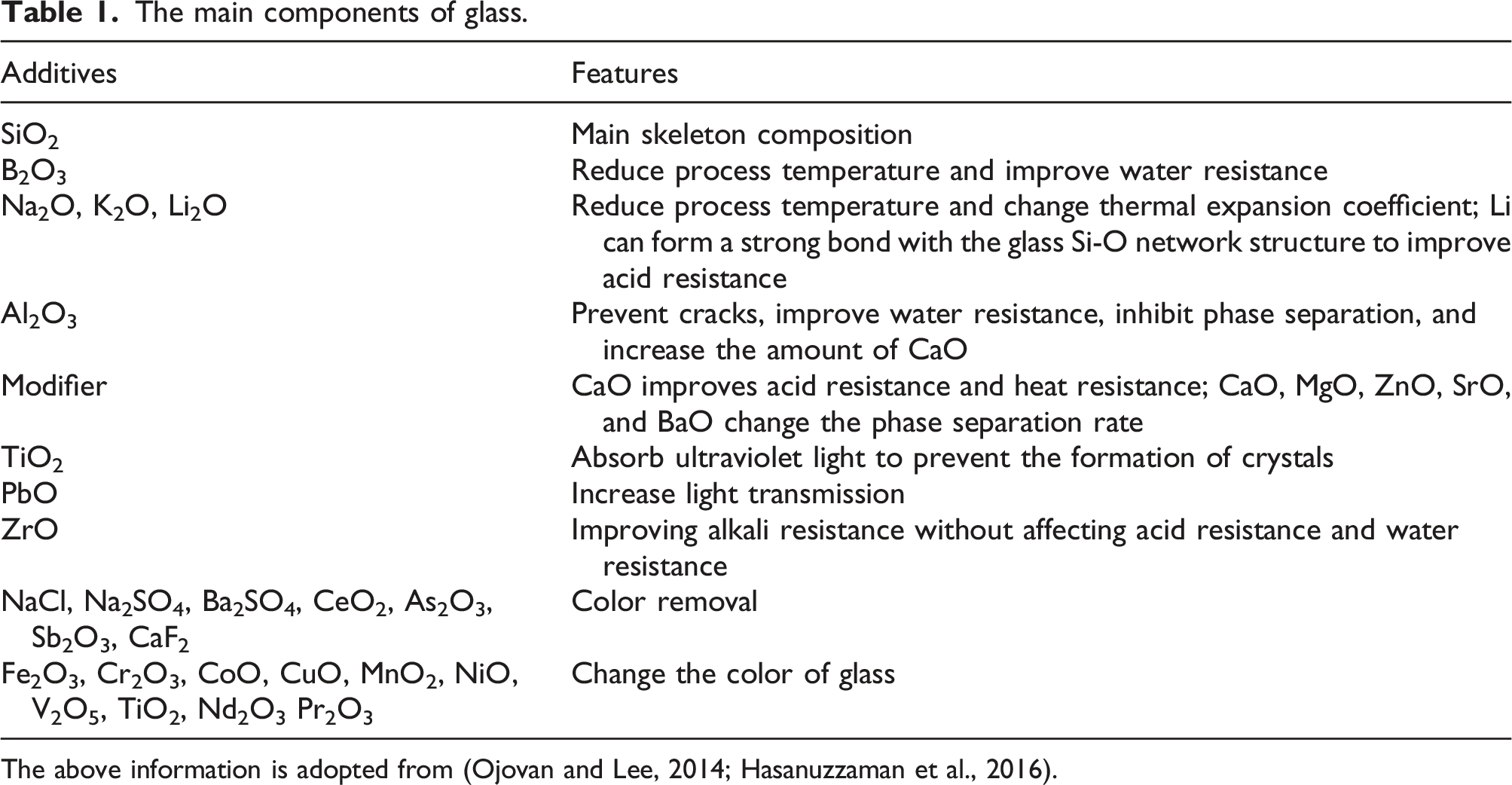
The above information is adopted from (Ojovan and Lee, 2014; Hasanuzzaman et al., 2016).
Ceramics
Compared with glass, ceramics have fewer applications in pharmaceutical packaging and process components. Common uses include ceramic pumps of the filling system. Ceramics are mainly made of pottery clay, and nearly half of the mass of pottery clay are SiO2 (Murray, 2006). Because of the short contact time between the ceramics in the process components and the liquid medicine, the risk of leaching is much smaller than that of glass packaging containers that is required to contact drug products for 2–3 years. Therefore, the silicon element for human exposure assessment refers mainly to glass.
Crystalline and amorphous silica
There are two types of silicon dioxide, crystalline, and non-crystalline. Crystalline silicon dioxide commonly observed is quartz, cristobalite, and tridymite. The Si-O-Si bond angle and Si-O bond length of crystalline silica are fixed values compared with various values in amorphous silica (Figure 1). In comparison, amorphous silica is a type of non-crystalline silica. Properties of amorphous silica are related to the duration since its formation. A freshly prepared amorphous silica is more toxic to rats via intraperitoneal injection than one that has been stored for a while, which was termed as silica sol. The lethal dose (LD) of freshly prepared silica is 35 mg/kg compared with 178 mg/kg for silica sol. After a silica sol was stored to solidify into a silica gel, a practical LD to rats was not found (Warheit et al., 1995). Different silica crystals and structures. (a) Quartz, (b) Cristobalite, (c) tridymite, and (d) Bond length and bond angle of the silica crystal.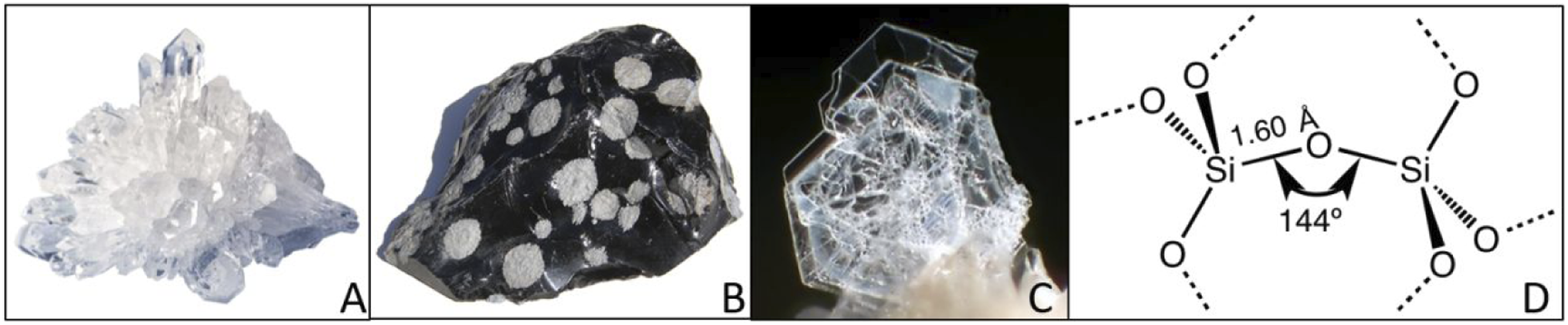
Common inorganic silicon exposed to patients
Glass detachment
Under alkaline conditions, the silica on the surface of glass dissolves and its structural network is disturbed and releases silicic acid into solutions. The alkali metal oxide in the glass on the top surface is released into the solution to expose the silica to the surface-solution interface. The silica layer gradually forms a silica gel. Then, the silicon gel layer cracks and releases glass fragments (EMA, 2008). This phenomenon is known as glass delamination. In summary, at least three types of silicon can be consecutively formed as follows: silicic acid, silica gel, and flakes based glass particles (Figure 2). Speculative mechanism for the formation of flakes or particulates after delamination and polymerization after dissolution.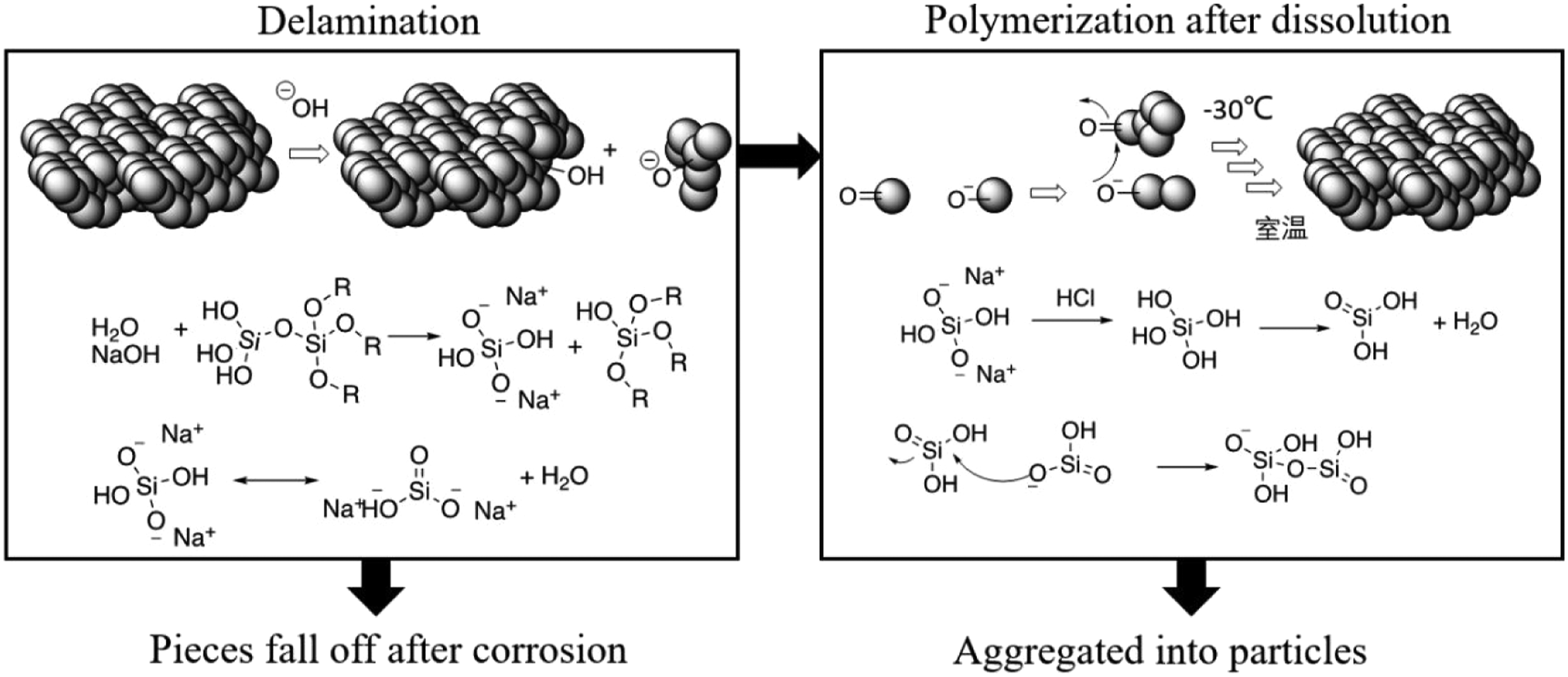
Glass corrosion dissolves the particulate matter formed by cold storage polymerization
Othosilicate (silicic acid, H4SiO4) is formed by the hydrolysis of silica. According to a report from Amgen (Ratnaswamy et al., 2014), glass erosion occurred to a batch of injectable drug during frozen storage, and insoluble particles were found after thawing. The particulate matter was formed by precipitation of saturated silicic acid solution under low temperature and subsequent aggregation. One possible aggregation mechanism of the particulate matter is, as shown in Figure 2, that orthosilicate is dehydrated to form silicic acid, mainly sodium silicate by NaOH solution, in which the silicic acid can be polymerized into a colloidal silica. Precipitation occurs when the particle is large enough through the aggregations of smaller size particles. Data from Fourier infrared spectroscopy (FTIR), scanning electron microscopy (Waegeneers et al., 2018), and energy dispersive X-ray spectroscopy (EDS) showed that the particulate matter was a mixture of SiO2 and Tween in an amorphous state.
Glass particles introduced from opening ampoules
A large numbers of glass particles can be produced by opening ampoules. They can be introduced into the human body by parenteral administrations of the drug product and the risk to cause adverse effects exists. Joo et al. (2016) found that an average of 108 glass particles (5–300 μm) were found in 180 opened ampoules. Shape of the particles varied from sharp needles to irregular flakes (Brewer and Dunning, 1947). In another comparative study of six common methods to break ampoules, it was found that 57.1%–77.7% of a total of 112 samples for each method contained glass particles with sizes mostly less than 60 μm, while particles larger than 120 μm, much larger than the diameters of most blood vessels, occurred in an average of 8% of all particles found in 10 mL ampoule samples, and 6% in 2 mL ampoule samples (Chiannilkulchai and Kejkornkaew, 2021). In addition, Hut reported that glass particles of 0.94–90.70 μm were detected in 94% of all samples from three types of medical ampoules during breakage in nursing practices, and syringe filter had no effect for one type of ampoule yet could only remove up to 85% of all particles in the other two types of ampoules (Erkoc Hut and Yazici, 2021).
Toxicity of inorganic silicon
Absorption, distribution, metabolism, and excretion
Glass particles of various size distribute in various tissues and organs via parenteral injection and may cause severe conditions as particle size decreases. As shown in Figure 3, capillary, venule, and arteriole have an inner diameter of around 8 μm, 20 μm, and 30 μm, respectively. Larger particles (10–12 μm) remain in the lungs, medium size (3–6 μm) in the spleen and liver lymph nodes, and smaller ones (around 1 μm) enter the liver. Brewer’s experiment pointed out that the larger particles pose weaker irritation effects, and that the smaller particles can cause severe conditions. Silica particles of 10–12 μm cause inflammatory infiltration in the lungs, while particles of 3–6 μm in the spleen and liver lymph nodes led to chronic and persistent alterations of the tissue, and particles of about 1 μm were mainly distributed in the liver and cause persistent hyperplasia of liver connective tissue and cirrhosis (Brewer and Dunning, 1947). Comparison of the sizes for silica particle, glass slag and the diameters of blood vessels.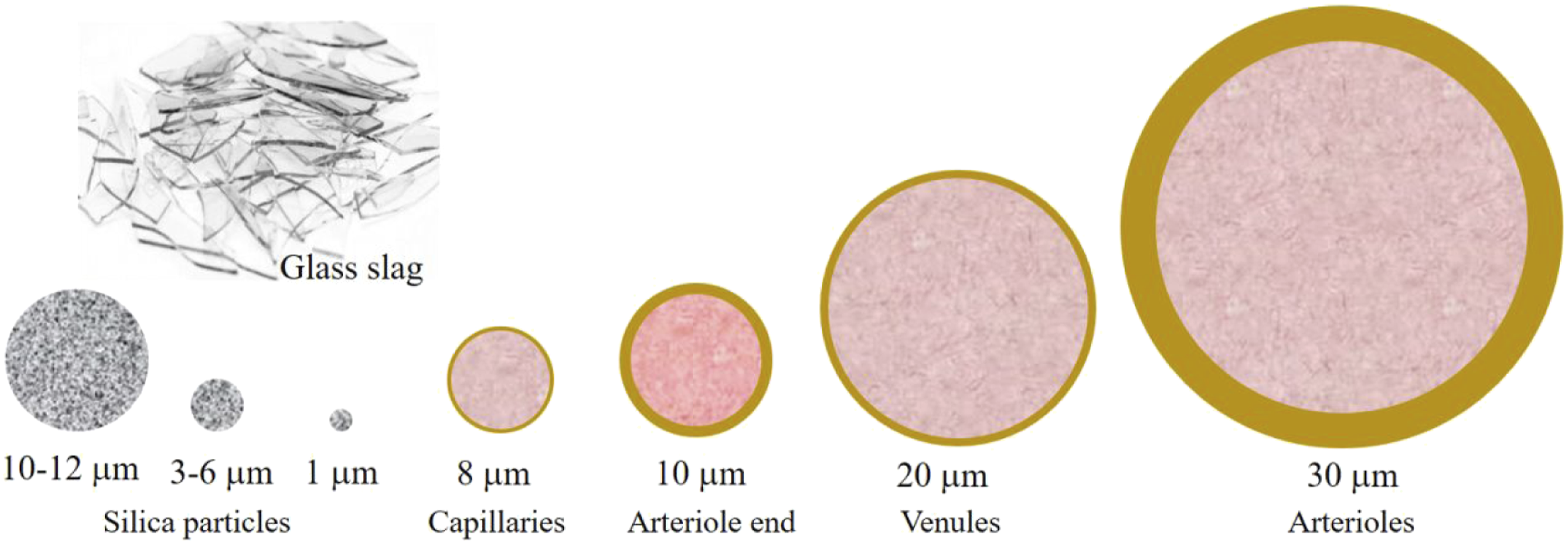
It should be noted that glass slowly degrades in tissue. Brewer found that most glass particles stay in the lungs of rabbit following intravenous injection of glass particles produced from ampoules, while 95% of the mass disappeared 1 year later. Presumably, silicic acid was produced after sodium and calcium ions are dissolved out, causing tissue necrosis and silicosis (Brewer and Dunning, 1947).
Oral route of administration
Summary of oral experimental structure of silica.

Our review focused on the toxic effect of glass particles or leachable compounds from pharmaceutical contact systems, most likely the inorganic silicon leachables/particles that exist as an amorphous form or particles of micrometer scale (Ratnaswamy et al., 2014), although the possibility of nanoparticle formations cannot be excluded. Therefore, using toxicological data of silica nanoparticle exposure may represent the worst-case scenario, while most likely the risk of Si element toxicity is conservative enough and may be overestimated.
Inhalational route of administration
The International Agency for Research on Cancer (IARC) lists crystalline silica as a Class I carcinogen, that is, a human carcinogen. Crystalline silica, usually with a size 100-fold smaller than sand particles is easily inhaled into the respiratory system (Szymendera, 2017). According to the reports from Occupational Safety and Health Administration (OSHA), inhalation of crystalline silica causes silicosis and may exacerbate other respiratory diseases (tuberculosis, lung cancer), autoimmune diseases (scleroderma, rheumatoid arthritis, lupus), and kidney diseases (Szymendera, 2017), and kidney diseases. OSHA determined a permissible exposure level (PEL) of crystalline silica at 50 μg/m3, which was derived from the PEL for quartz published in 2010, 100 μg/m3, considering that cristobalite and tridymite are more toxic than quartz.
Inhalation limits of silica.
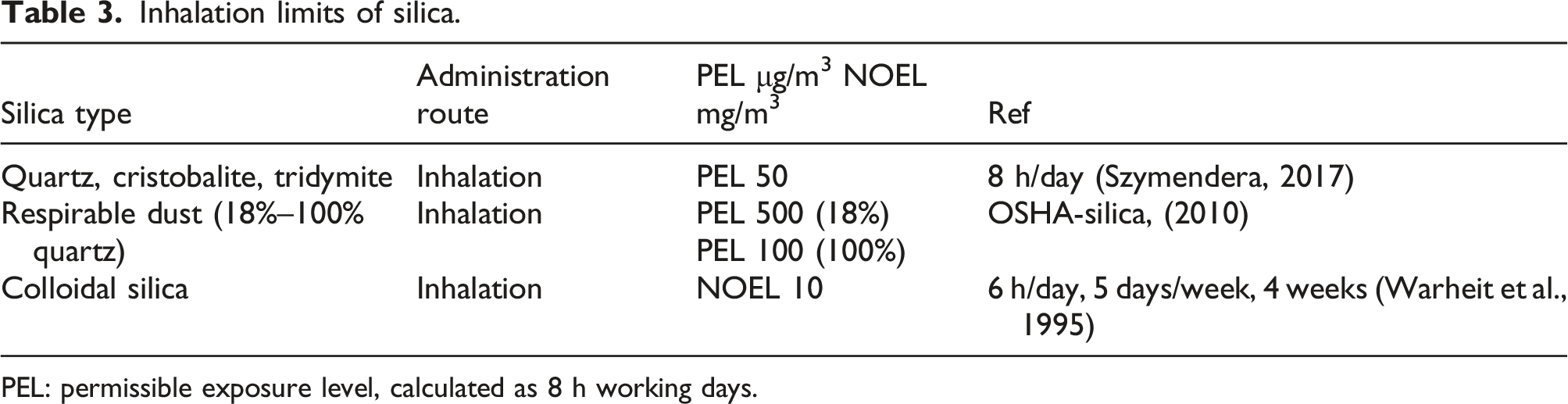
PEL: permissible exposure level, calculated as 8 h working days.
Parenteral route of administration
Intravenous injection of silica sol causes acute toxicity while silica gel leads to no effect within 12 h. Silica sol intravenous (IV) administration leads to blood clots in the blood vessels and heart, and death. Meanwhile, it causes the necrosis of the kidney tubules. The LD of the IP route of administration is equivalent to that of IV with no clear cause of death. The toxicity endpoint of silica sol is the destruction of vascular epidermal cells. Gye’s anatomy and microscopic examination revealed that the vascular wall cells in the liver had varying degrees of destruction, from swelling caused by cell fluid vacuolation to complete exfoliation. Many vascular endothelial cells circulate with the blood after peeling and can be observed in the blood vessel section (Gye and Purdy, 1922). At the same time, liver and kidneys showed visible damage, which was likely caused by failure of elimination of silica sol. Most of the liver necrosis was focally distributed and sometimes half of the hepatocytes were dead. Kidney damage was mainly located in the glomerulus, manifested in the extreme expansion of the capillaries in the glomeruli, the serum penetration into the glomerular cavity, and the complete necrosis of the capillaries in the glomeruli (Gye and Purdy, 1922). Gye also reported that as the storage time of silica sol increased, the sol became a gel with lower toxicity and delayed initiation time of toxicity. A LD of the sol caused death within a few minutes, while the gel had no effect within 12 h. This was probably due to the decrease in toxicity by a further increase in the degree of polymerization.
Acute toxicity of silica by injection route.
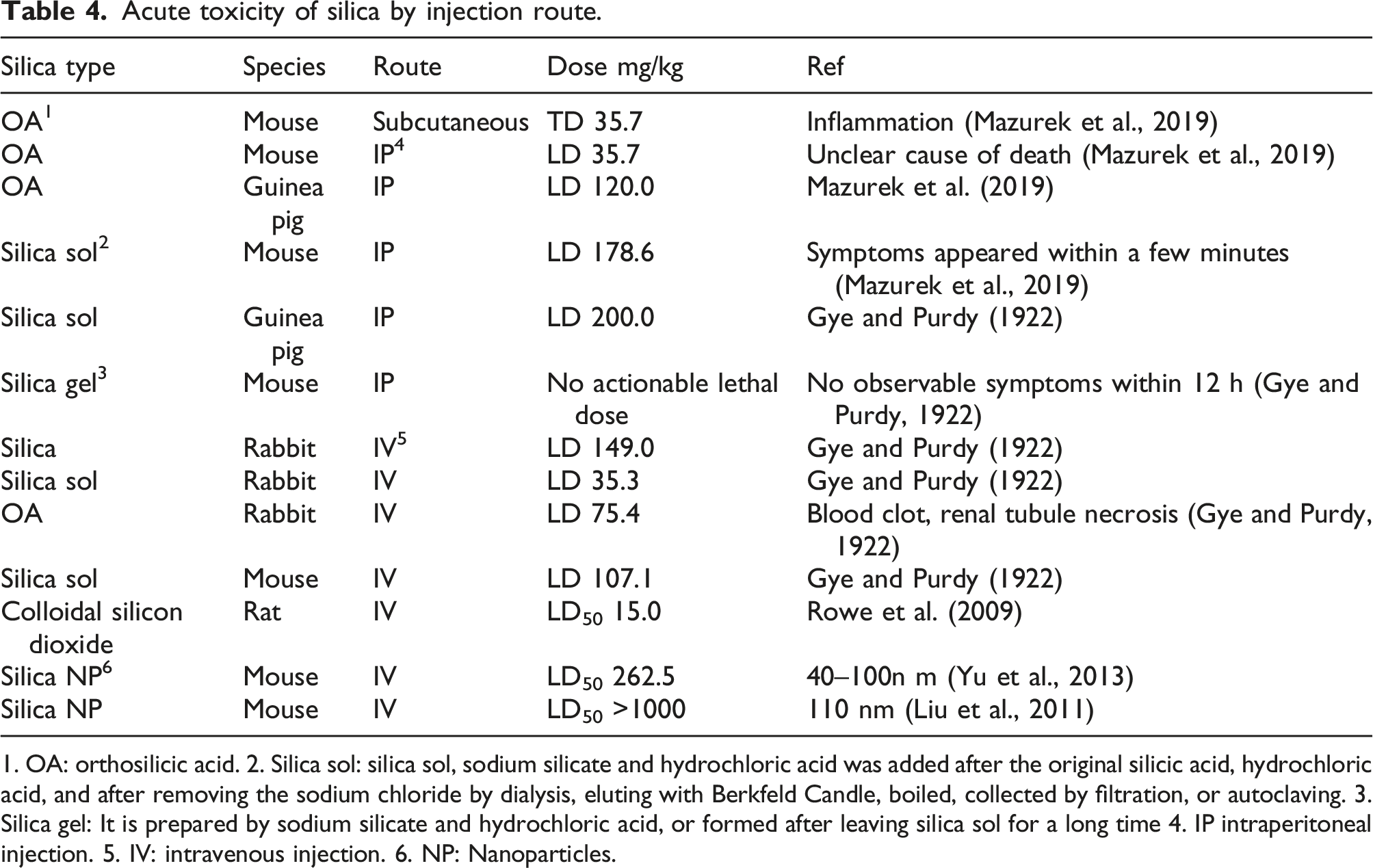
1. OA: orthosilicic acid. 2. Silica sol: silica sol, sodium silicate and hydrochloric acid was added after the original silicic acid, hydrochloric acid, and after removing the sodium chloride by dialysis, eluting with Berkfeld Candle, boiled, collected by filtration, or autoclaving. 3. Silica gel: It is prepared by sodium silicate and hydrochloric acid, or formed after leaving silica sol for a long time 4. IP intraperitoneal injection. 5. IV: intravenous injection. 6. NP: Nanoparticles.
Permitted daily exposure values of inorganic silicon element
NOAEL values of different administration routes of silica.
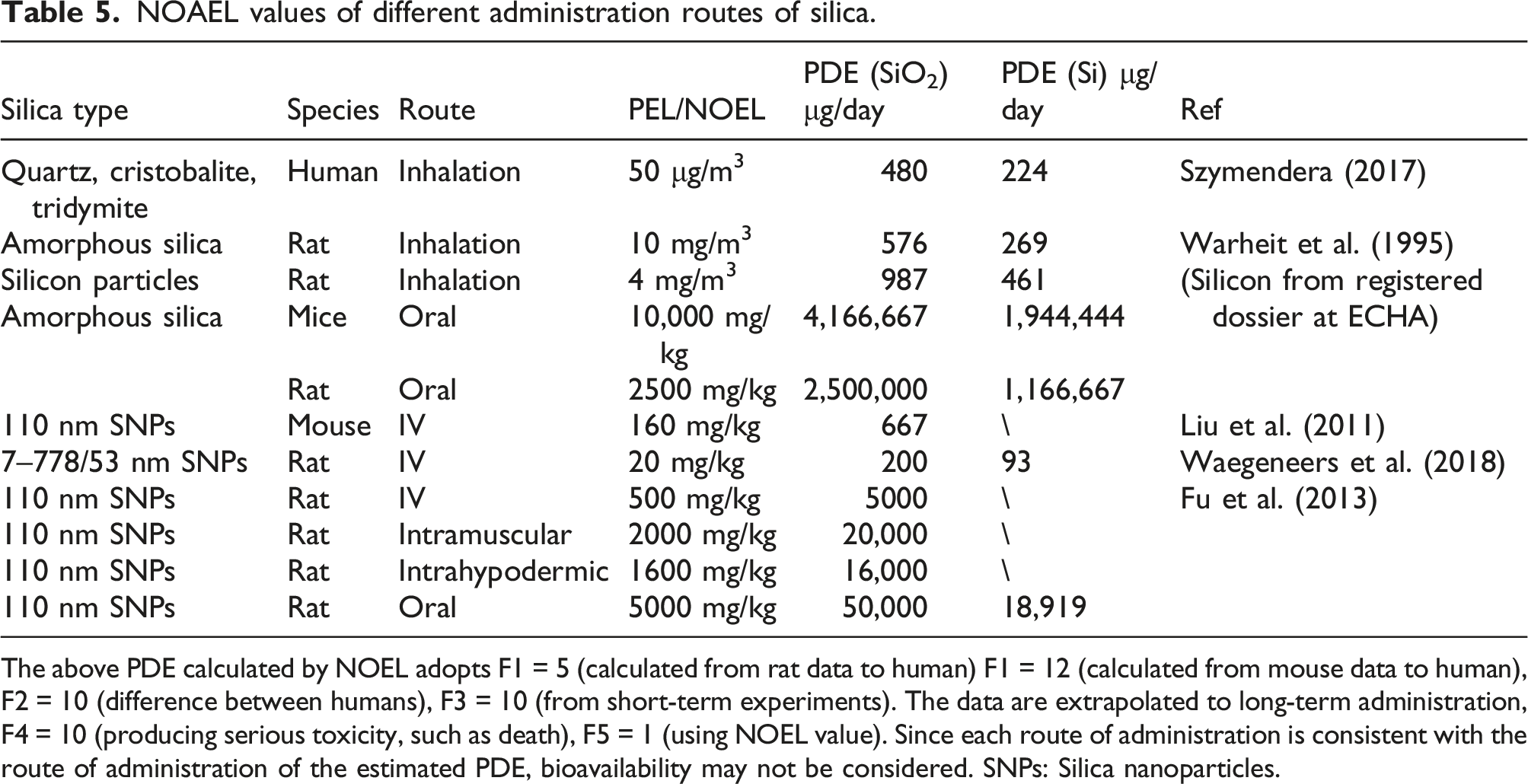
The above PDE calculated by NOEL adopts F1 = 5 (calculated from rat data to human) F1 = 12 (calculated from mouse data to human), F2 = 10 (difference between humans), F3 = 10 (from short-term experiments). The data are extrapolated to long-term administration, F4 = 10 (producing serious toxicity, such as death), F5 = 1 (using NOEL value). Since each route of administration is consistent with the route of administration of the estimated PDE, bioavailability may not be considered. SNPs: Silica nanoparticles.
Exposure of organic silicon compounds in pharmaceutical packaging and process components
Silicone tubes
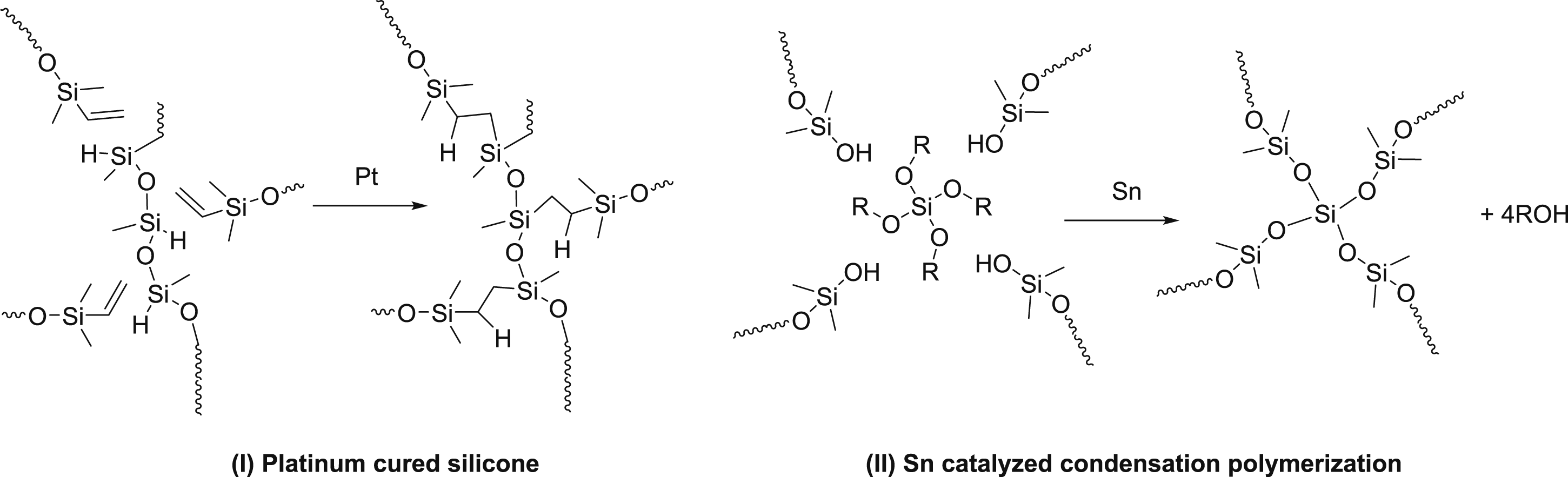
Silicone tubes are made of silicone elastomer, which is mainly composed of PDMS polymer formed by the hydrolysis and polymerization of dichlorodimethylsilane. As in Figure 4, dihydroxydimethylsilane is generated by the hydrolysis of dichlorodimethylsilane, and can be further dehydrated through polymerization process into linear polydimethylsiloxanes and cyclic polydimethylsiloxanes, such as low molecular weight based D3, D4, and D5 (Colas, 2005). Dimethylsiloxane elastomeric polymer is manufactured by the vulcanization process of PDMS, and there are two common curing processes as shown in Figure 5, including (I) platinum cured silicone tube and (II) tin (Sn) catalyzed condensation polymerization (Mazurek et al., 2019). Platinum vulcanized silicone tube utilizes the addition reaction of vinyl and silicon hydride to cross-link multiple linear siloxane polymers into a network. The tin-catalyzed condensation reaction utilizes a siloxane linear polymer with terminal hydroxyl groups and a cross-linking agent (tetraalkoxysilane) to polymerize into a network polymer. Synthesis process of silicone elastomer by silicone polymers (Colas, 2005). Two common silicone elastomers (Mazurek et al., 2019). The curve represents the polymer chain, and R represents the alkyl group.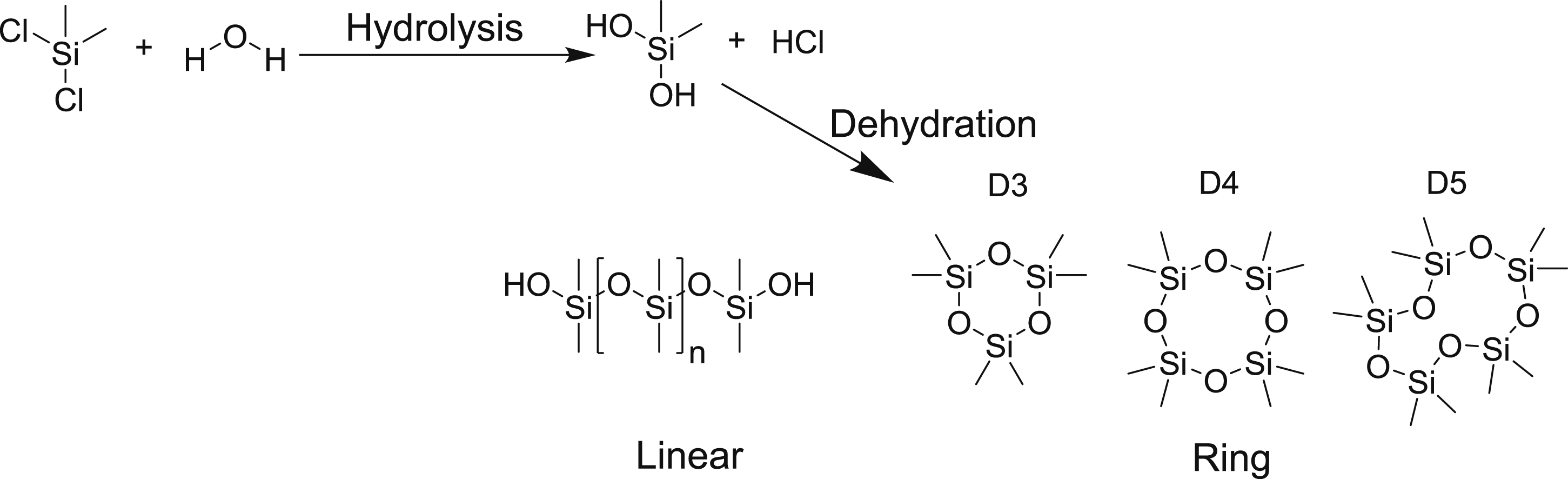
Silicone oil-lubricants
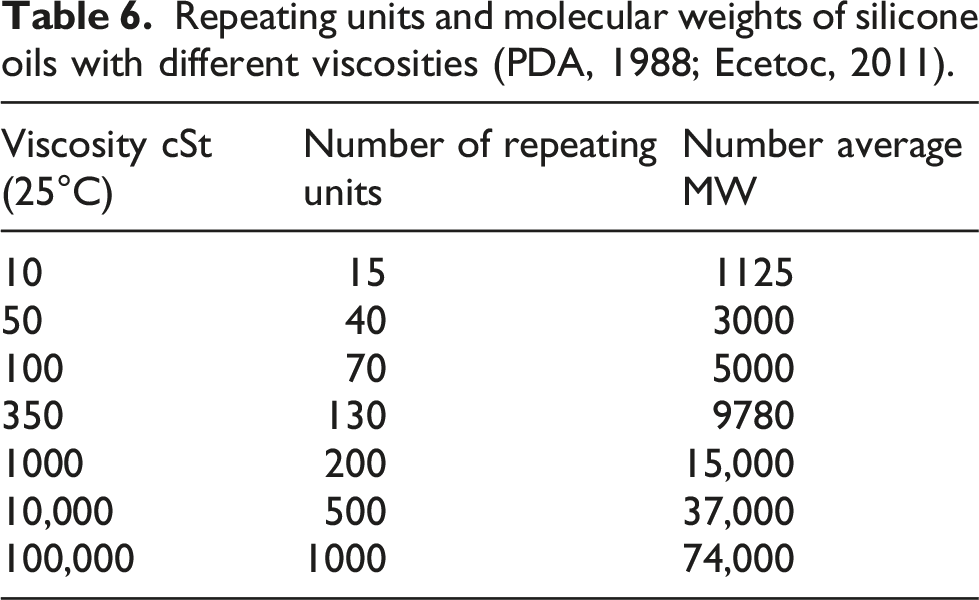
The chemical structure of silicone oil is shown in Figure 6, and the degree of polymerization typically ranges from 400 to 1200 (Eur, 2005), while others reported a common degree of polymerization of two to several thousand, with a viscosity ranging from 0.65 to 1, 000,000 centistokes (CSt) (PDA, 1988). The relationship between molecular weight and degree of polymerization can be found in Table 6 (Ecetoc, 2011). An example of the chemical composition structure of silicone oil. Repeating units and molecular weights of silicone oils with different viscosities (PDA, 1988; Ecetoc, 2011).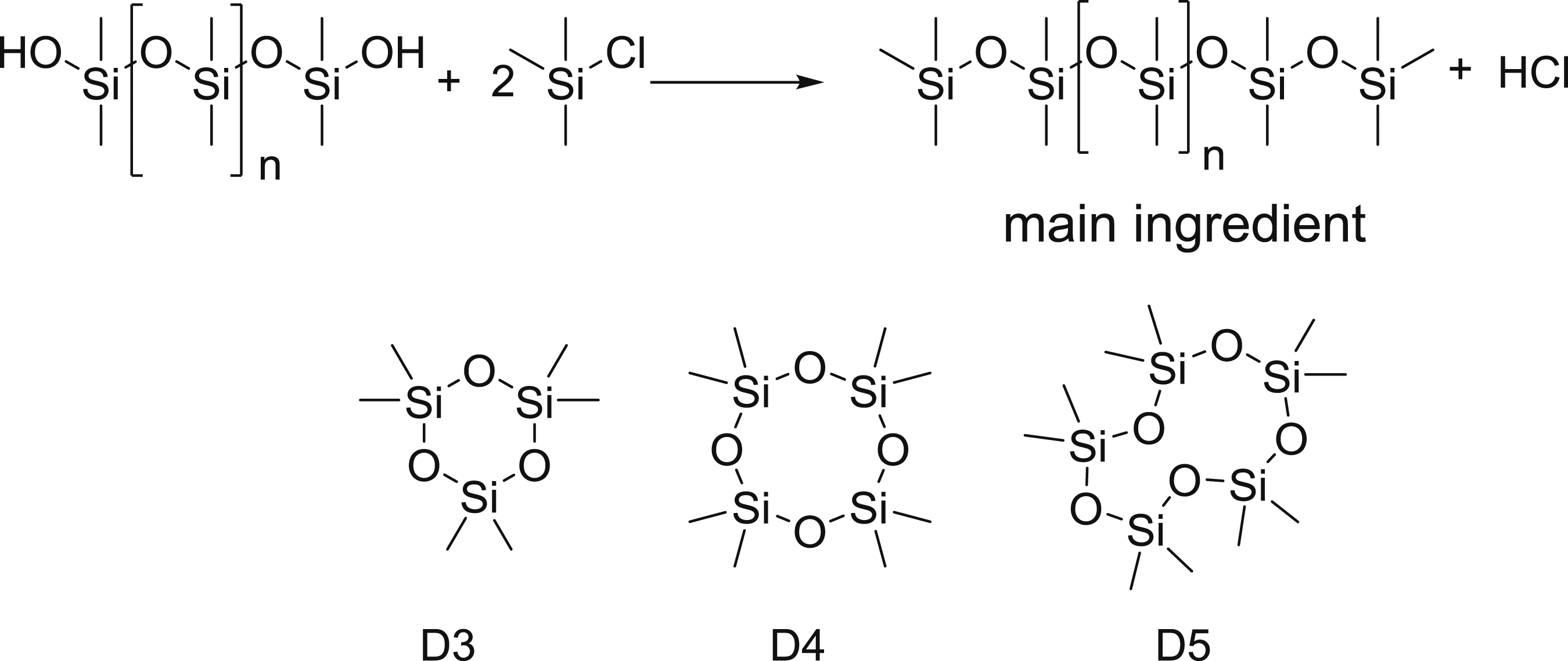
In order to reduce the hydrogen bond between the polymer chains to reduce the viscosity, the two ends of the polydimethylsiloxane polymer chain are often protected with trimethylsilyl groups for lubrication purpose of the application. There is no need to vulcanize the polymer to form cross-linking network for lubrication. Similar to silicone tube, cyclic D3, D4, D5 to D14 dimethylsiloxanes are also present in silicone oil (PDA, 1988).
Toxicity of organosilicon compounds
ADME for linear polydimethylsiloxane
Kow value of linear polydimethylsiloxane.
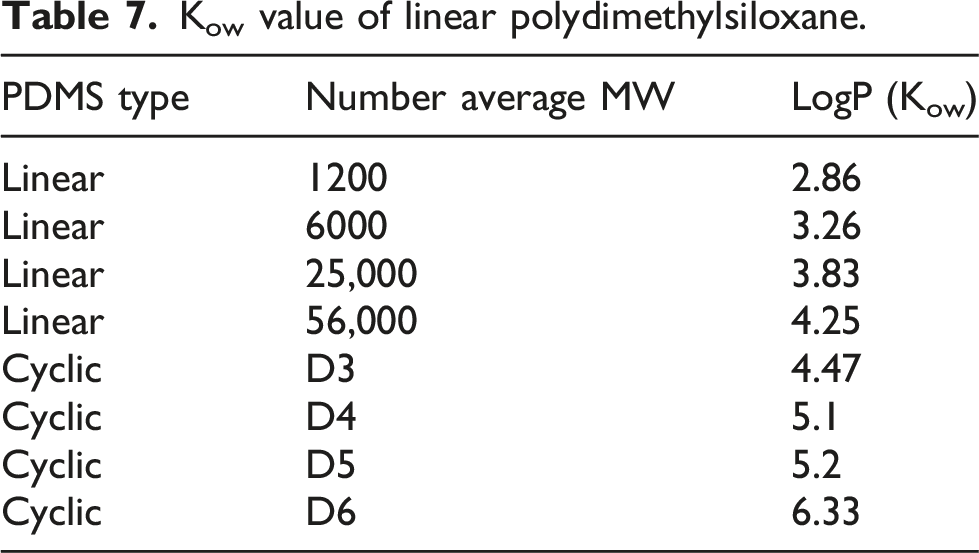
The absorption of PDMS also highly depends upon its volatility. For example, a small MW-based cyclic or linear PDMS is volatile and could be absorbed rapidly, while PDMS polymers with polymerization degrees >15 are non-volatile, limiting exposure via the inhalational route or topical dermal absorption. PDMS administered orally do not degrade and can be eliminated directly through feces; Specifically PDMS of 10 cSt and 350 cSt taken orally cannot be absorbed by rats and are excreted unchanged through feces (Ecetoc, 2011).
Polydimethylsiloxane by IP injection in rats seemed to have difficulty being eliminated in urine, feces, and lung. Specifically, IP injection of PDMS from Dow-Corning MF360 with a viscosity of 12,500 cSt labeled with 14C to rats showed that 100% of the PDMS was detected in rats after 25 days, among which 50% of the PDMS was detected in adipose tissues, followed by gastrointestinal tract and liver, and no PDMS was found in blood and heart (Hine et al., 1969) In comparison, PDMS was distributed into the brain and spine after PDMS was injected into the brain cavity with no migration to the gastrointestinal tract (Hine et al., 1969).
ADME for cyclic polydimethylsiloxane
Cyclic polydimethylsiloxane (cPDMS) has good volatility and high lipophilicity, and the lipophilicity increases with increased degrees of polymerization and MW (Table 7). cPDMS can enter organs through inhalation, oral administration, injection, and transdermal absorption (Greve et al., 2014) After entering the blood circulation, cPDMS can be metabolized in the liver, expelled through the lungs, excreted through kidneys into urine, and eliminated by feces. According to the study from Franzen et al., the oral bioavailability of D5 is about 20%, in which 50% of D5 is removed through exhalation (Franzen et al., 2016). In comparison, D5 is poorly absorbed through the skin (<0.04%) and most of the D5 on the skin evaporated. Even if D5 had entered into the blood circulation, 90% of D5 can be removed via the respiratory tract (Dekant and Klaunig, 2016).
Cyclic polydimethylsiloxane can be metabolized by enzymes, probably CYP450, via oxidation to form silyl alcohols as shown in Figure 7, and further oxidation can produce aldehydes, followed by hydrolysis to generate silanols with smaller degrees of polymerization. Metabolic mechanism of cyclic cPDMS.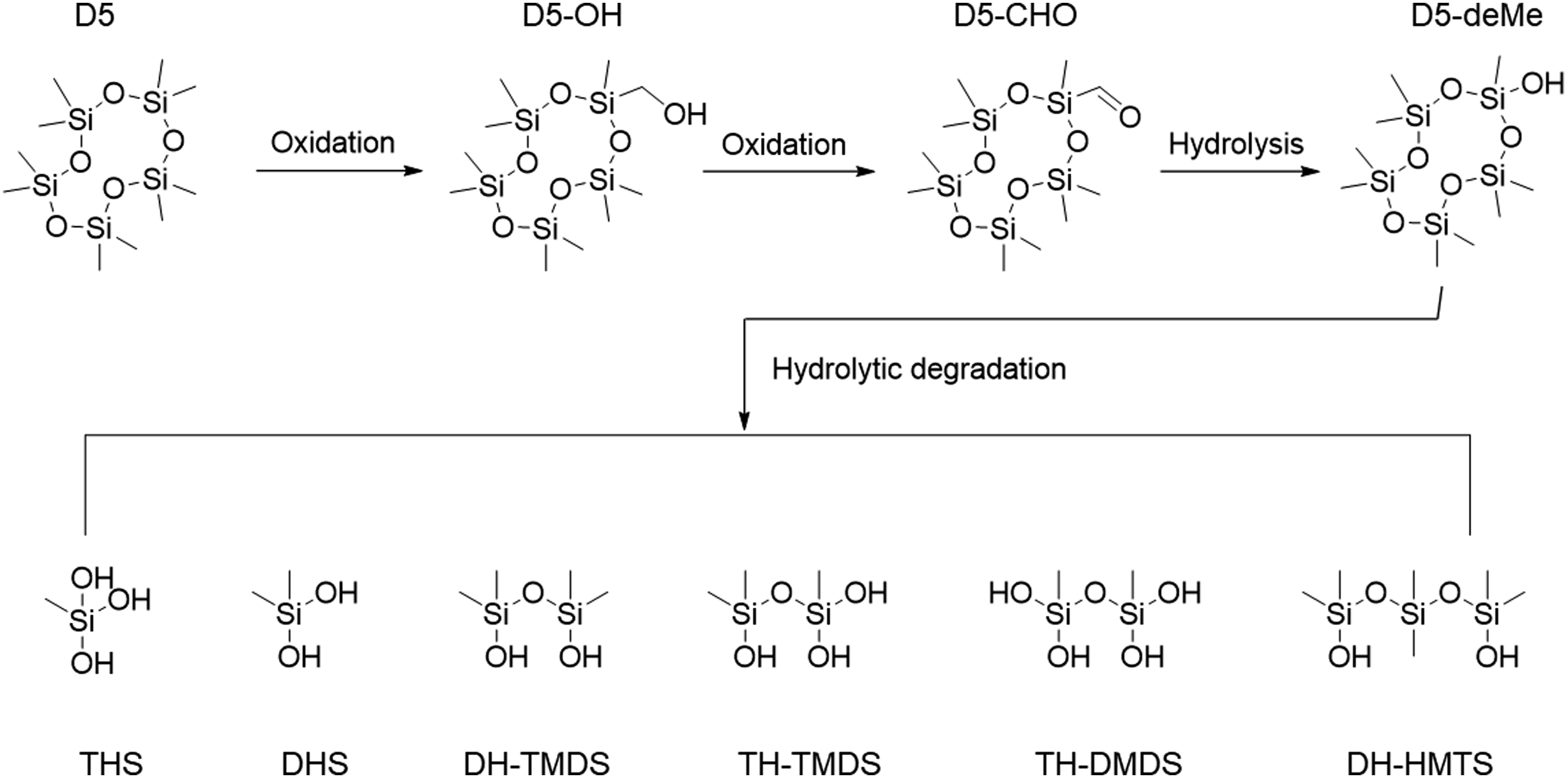
Oral route
The oral toxicity of the macromolecule PDMS is negligible, and it is probably related to its lack of absorption. In a long-term 24-month oral rat study of 0, 100, 300, 1000 mg/kg of 10 cSt PDMS, the NOEL value was the highest dose of 1000 mg/kg and no toxic reaction was found, so the actual NOEL could be >1000 mg/kg.
Parenteral route
The non-intravenous parenteral administration route includes IP, intramuscular, and subcutaneous injection. PDMS has a low non-IV toxicity. When injected intraperitoneally at 1000 mg/kg of 60 cSt PDMS or 140 cSt PDMS to rats, and no animals were found to be dead one year after the injection rats (Ecetoc, 2011). Another study conducted under Good Laboratory Practice (GLP) per OECD Guidelines reported that when intraperitoneally administered to rats, 0, 200, and 2000 mg/kg of 350 cSt PDMS to rats, no clinical signs and no pathology findings in biopsy were found after a 14-day observation period (Greve et al., 2014). Additionally, McGregor et al. from Dow Corning concluded that except for small molecule silicone oil components, PDMS had almost no adverse effects when administrated subcutaneously, intramuscularly, and intraperitoneally (McGregor, 1961) Moreover, Ashely et al. reported that administrated total doses of 1–500 mL of PDMS did not lead to local and systemic toxicity with only minor reactions in more than 1000 animals including rabbits, monkeys, Japanese macaques, guinea pigs, rats, and mice when it was administrated subcutaneously, intramuscularly, intraperitonially, and topically (Ashley et al., 1967).
Although non-IV parenteral administration of PDMS has low toxicity in humans and can be applied to breast implants, IV administration of PDMS leads to visible toxicity in a dose-dependent fashion. It was noted that the intravenous LD50 for rabbits is 500 mg/kg, while a smaller dose of 100 mg/kg for 25 consecutive days showed no apparent adverse effects (Ashley et al., 1967). Although the study duration was relatively short, it may be feasible to derive a chronic exposure PDE at 20 mg/day, which was estimated per ICH Q3C by using a 50-kg human body weight and an uncertainty factor (F1 = 2.5, F2 = 10, F3 = 10, F4 = 1, F5 = 1) of 250. Considering that PDMS cannot be removed from the human body due to the lack for metabolism (Hine CH E H, Wright RR, Cavalli RD, Porter CD., 1969; Hine C E, HW; Wright, RR; Cavalli, RD; Porter, CD, 1969), the strong bioaccumulation effect argues for an extra factor of F6 = 10 applied to derive a reasonable limit of 2 mg/day, though more conservative care should be taken in a case-by-case fashion when applied.
It has been reported that the toxicity of silicon oil is related to its viscosity. The Badura study showed that when dogs were injected IV with 1000 cSt silicone oil, no obvious reaction was observed (McCurdy and Solomons, 1977). However, silicon oil accumulated in the lung and liver leading to blockage of the reticule-endothelial system. In contrast, 350 cSt silicone oil produced emboli in the lungs and death when intravenously injected (Horton and Solomons, 1977).
Inhalation route
Small molecule volatile hexamethyl disiloxane (HMDS) and cPDMS are relatively volatile and lipophilic, and they are more toxic compared with macromolecular PDMS. Death of animals occured when they were administrated percutaneously, orally, intravenously, and by inhalation. Some literature points out that D4 has weak estrogenic or estrogen antagonistic effects, which delays the peaking of mouse luteinizing hormone and ovulation for 24 h, reducing the fertility rate of mice. However, this toxicity endpoint is unlikely to affect humans because of the longer ovulatory cycle of 1 month, which is much longer than that of mice (Greve et al., 2014; Franzen et al., 2017). The above Greve's (2014) study was conducted per OECD TG413 guidance to expose rats intra-nasally with 0, 140, 730, 3420, and 13,640 mg/m3 of HMDS for 6 h/day, 5 days/week for 3 months followed by a 1 month recovery period. The lowest dose group (140 mg/m3) showed intestinal inflammation and accumulations of macrophages in alveoli during the recovery period. Thus, the LOEL of HDMS was determined to be 140 mg/m3. Considering the human respiratory volume of 28.8 m3, we applied the adjusting uncertainty factor of inter-species F1 = 5, intra-human F2 = 10, subchronic to chronic adjustment of F3 = 5, LOEL F5 = 10, and calculated a 24 h/day PDE of 288 μg/day. Since the molecular adjustment factor for silicon in HMDS is 28 × 2÷162 = 0.346, the final inhalational PDE for silicon element is considered 100 μg/day.
Permitted daily exposure values of organosilicon
Summary of toxicology studies of organosilicon compounds.
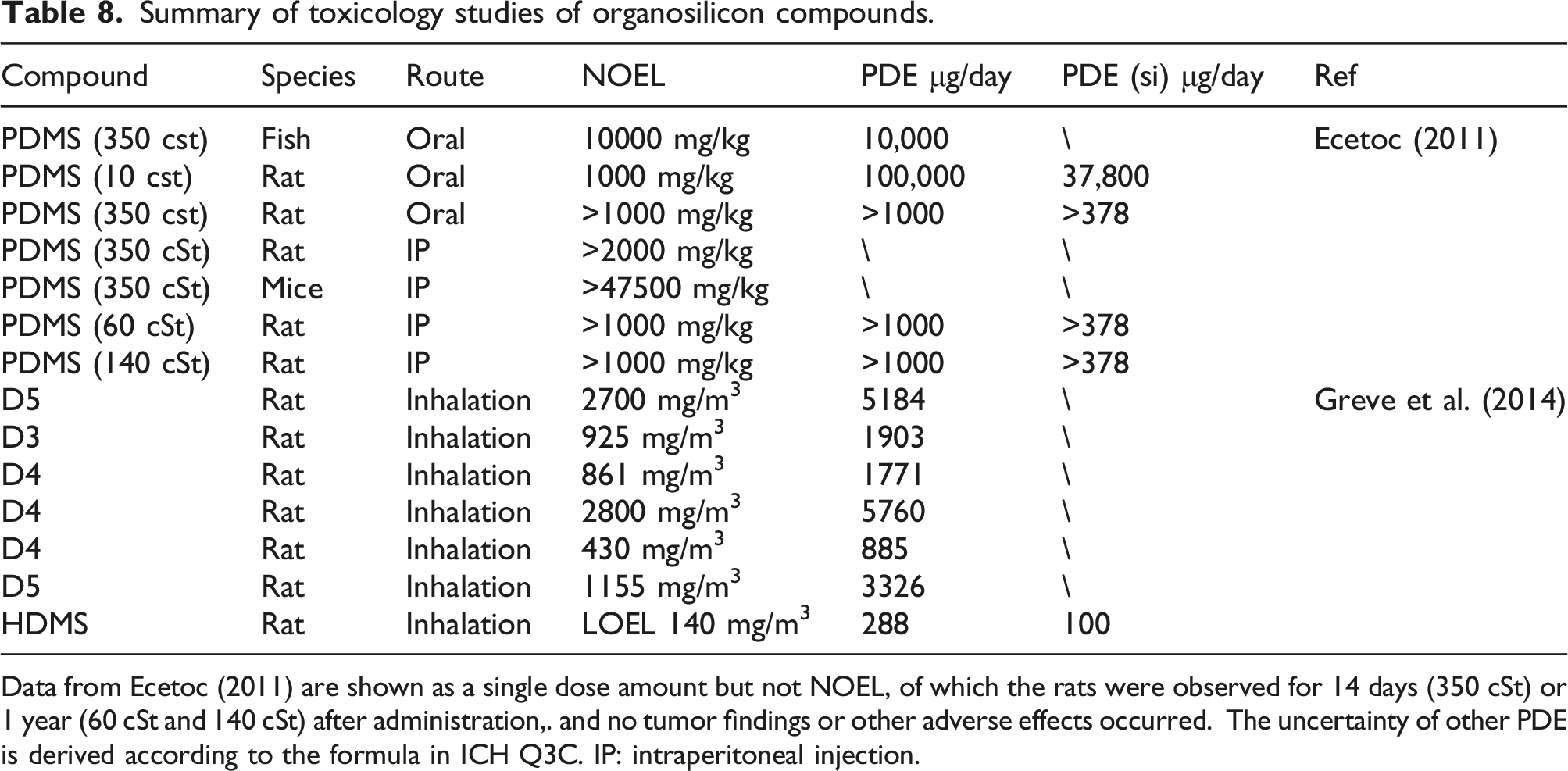
Data from Ecetoc (2011) are shown as a single dose amount but not NOEL, of which the rats were observed for 14 days (350 cSt) or 1 year (60 cSt and 140 cSt) after administration,. and no tumor findings or other adverse effects occurred. The uncertainty of other PDE is derived according to the formula in ICH Q3C. IP: intraperitoneal injection.
Discussions
Toxicology threshold of silicon.
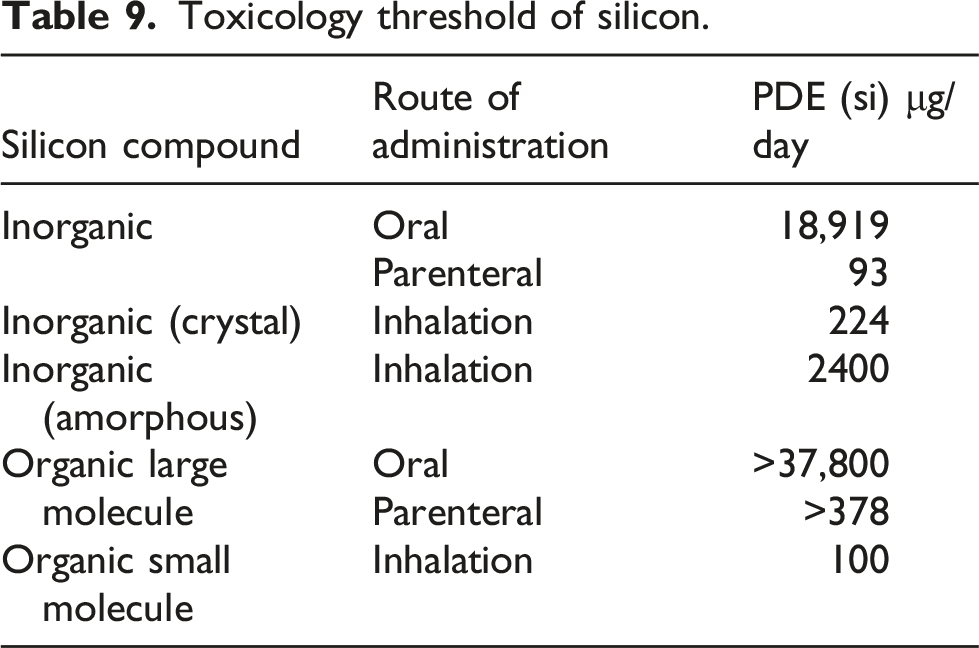
It should be noted that the parenteral PDE (2000 μg/day) of organic silicone-large molecule is derived from a 25-day repeated-dose experiment as discussed in Section 5.4, and the study endpoint was death, which is not suitable for PDE derivations. Since no other repeated-dose toxicological data were available, the parenteral PDE for silicone (large molecule) had to be derived from the oral data for which the additional F6 for bioavailability may be applied. Since the molecular weight of PDMS is large and its bioavailability is very low, 100 was selected per ICH Q3D (ICH Q3D (2019) to derive a PDE of 378 μg/day.
Crystalline inorganic silicon (quartz, cristobalite, tridymite) can cause silicosis and lung cancer by the inhalation route. Lung tissue fibrosis is mainly caused by physical stimulation chronically. It belongs to a non-genotoxic carcinogen and has a threshold. Therefore, it is acceptable to calculate the PDE value by a NOEL or LOEL. Toxicity between amorphous and crystalline silica differs significantly, and the inhalable silicon into lungs on occasion of pharmaceutical exposure condition is usually in its non-crystalline state, thus it is suggested to use an inhalational PDE of amorphous silicon, 2400 μg/day. If crystalline silica exposure data are available for an inhalation drug, the PDE for silicon should be adjusted to 224 μg/day.
The toxicity of the intravenous exposure of inorganic silicon is very common. Toxicity endpoints are blood clots and blockage of blood vessels that leads to damage of liver, kidney, and lung, and acute death. In contrast, a large molecular organic silicon compound such as PDMS is less toxic, but the toxicity from intravenous administration is more obvious than with other parenteral routes such as intraperitoneal and subcutaneous routes, where in case of intravenous injection, a LD can be found. The intravenous PDE derived from non-lethal dose rabbit experiments is equivalent to 2000 μg/day of siloxane and 757 μg/day for elemental silicon. Nevertheless, since these values are much larger than the 378 μg/day in Table 8, it is suggested to use 378 μg/day for the PDE of IV administration of silicon.
The oral toxicity of silica is very low. There is no difference in the toxicity of crystalline and non-crystalline silica reported. Therefore, the PDE value of oral inorganic Si is 18,919 μg/day, suitable for inorganic silicon exposure, mostly amorphous silica, in pharmaceutical packaging, and process components.
The selection of pharmaceutical packaging materials and process component materials should be carried out in accordance with the concept of Product Quality by Design (QbD) recommended by ICH Q8, in addition to the compliance testing of materials with pharmacopoeia or other standards, such as USP <381> for elastomer, <660> for glass, and <661> for plastic, prior knowledge should be considered in the initial selection of materials, based on the clinical use of finished drug products and based on the extractable amount of inorganic and organic silicon that can be obtained under the worst conditions of use or under the conditions of severe acceleration and aggravation (simulation tests can be carried out with the drug product solution to obtain the total amount of silicon leached into the drug product), and the packaging materials and process components can be obtained. A safety risk assessment can be conducted to determine suitable materials for product use.
If the content of silicon in the extract or simulated drug product solution can meet the most stringent PDE requirements for both organic and inorganic silicon in Table 9, no further research on the source of silicon is required, and 93 μg/day is directly used to carry out toxicological risk assessment, combined with other aspects of information (functionality, protection, compatibility of materials and liquids, biological safety evaluation) to comprehensively evaluate the applicability of materials.
On the contrary, it is necessary to use plasma technology (Inductively Coupled Plasma—Mass Spectrometry or Inductively Coupled Plasma—Optical Emission Spectrometry) and gas/liquid chromatography mass spectrometry technology for the analysis of extraction solutions or simulated drug product solutions prepared under suitable conditions to conduct the quantification analysis of inorganic silicon or organic silicon. For identification, qualitative and quantitative research, specific research ideas and methods can be carried out with reference to USP <1663> or <1665>. The content of inorganic silicon is evaluated according to the specific route of administration according to Table 9; among them, for inhalants, after excluding the possibility of the crystalline state of inorganic silicon (unlikely in exposure of glass), a more appropriate PDE of 2400 μg/day can be selected. For organosilicon compounds, after qualitative and quantitative research on the compound, the appropriate PDE value should be selected for preliminary evaluation according to the different administration routes of organosilicon in Table 9. It is worth noting that in the case that relevant toxicological data of a specific organic compound is available, the toxicological data of the compound should be used to calculate its specific PDE for safety assessment. In the case of simultaneous detection of the same type of organosilicon compounds, the respective toxicity mechanisms of multiple compounds should be assessed, and any additive/synergistic toxicological effects should be considered.
Conclusions
Pharmaceutical packaging and process components can contaminate drug product with inorganic silicon such as glass particles from ampoule opening or by erosion followed by freezing, and organic silicon such as silicone oil and silicone tube leachables. The final conclusion is: (1) The oral toxicity of inorganic silicon and silicon organic polymers is negligible, and the oral PDE is 18,919 μg/day and 37,800 μg/day, respectively. (2) The risk for parenteral and inhalational exposure of inorganic silicon is high, which mainly cause lesions to blood vessel endothelia, promote blood clots in blood vessels and heart, and silicosis, for example. The corresponding PDEs are 93 μg/day and 224 μg/day, respectively. (3) Toxicity differs significantly for organic silicon compounds that depend upon molecular weight. Small molecular siloxane is volatile and toxic, and its inhalational PDE is 100 μg/day, similar to that of inorganic silicon. In comparison, large molecular organic silicon compounds are less toxic. PDMS is non-toxic based on repeated-dose oral animal exposures as high as 10 g/kg via the intraperitoneal route. Therefore, it is not practical to derive a PDE for both scenarios. The intravenous route showed clear toxicity, and considering that PDMS is not degradable in vivo and not excretable via feces or urine, a conservative PDE of 378 μg/day was calculated for parenteral organic silicon.
Although inorganic and organic silicon differ significantly structurally, this review shows that the PDE for parenteral and inhalational routes for both types of silicon are around the hundred microgram range, and this review can be a good scientific reference for regulatory authorities to evaluate the safety of silicon compounds by different routes of administration for the pharmaceutical industry.
Footnotes
Acknowledgements
The authors would like to thanks for the support from the program of leading talents in science and technology for Suzhou Jinji Lake.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (31971319; 32171403).