
Abstract
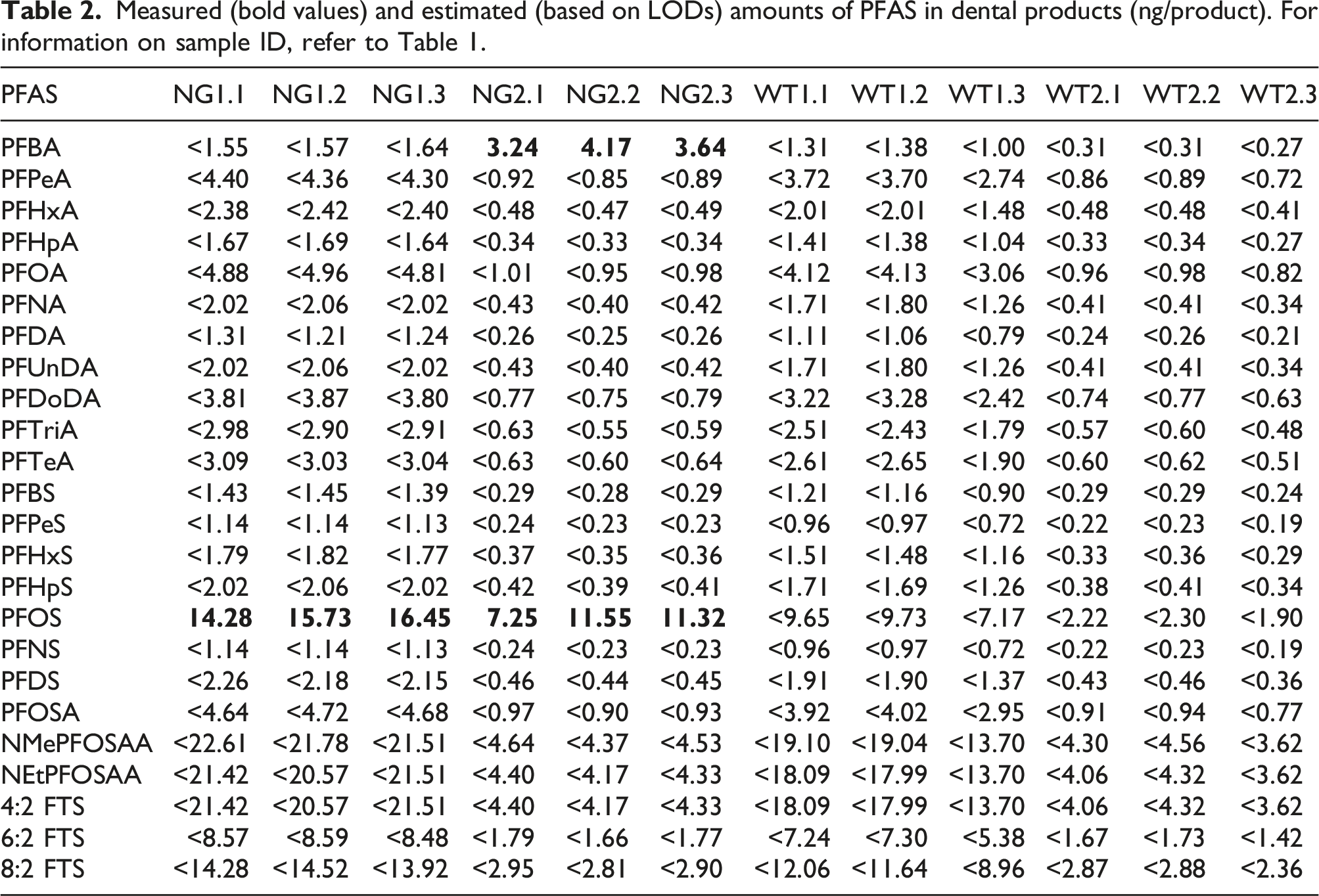
Contaminated water and food are the main sources of documented per- and polyfluoroalkyl substances (PFAS) exposure in humans. However, other sources may contribute to the overall PFAS intake. While several studies documented the presence of PFAS in consumer products, PFAS evaluation in dental products has been limited to floss and tape to date. This study estimated PFAS exposures from a convenience sample of leave-in dental products (night guards and whitening trays), which remain in contact with the mouth for longer durations than previously evaluated dental products. This analysis evaluated whether consumer usage of these dental products meaningfully contributes to oral exposure of PFAS. Leaching of PFAS upon disposal of products was also considered. Out of 24 PFAS measured, perfluorobutanoic acid (PFBA; 3.24–4.17 ng/product or 0.67–0.83 ng/g) and perfluorooctanesulfonic acid (PFOS; 7.25–16.45 ng/product or 1.2–2.3 ng/g) were detected in night guards, and no PFAS were detected in whitening trays. Non-targeted analysis showed additional possible PFAS, which could not be characterized. The findings showed that PFOS and/or PFBA present in night guards were unlikely to pose a health concern. From an ecological perspective, the dental products examined were shown to constitute a negligible contribution to environmental PFAS. In conclusion, the examined dental products do not represent a significant source of exposure to PFAS for humans or the environment. The study demonstrates how risk assessment can be integrated by the industry into product stewardship programs to evaluate the potential health and environmental impacts of chemicals in consumer products.
Keywords
Introduction
Ingestion of contaminated drinking water is a major route of exposure to per- and polyfluoroalkyl substances (PFAS) among the general population [e.g., Garnick et al. (2021)]. Oral exposure can also occur from ingestion of food, ingestion of materials that have come into contact with PFAS-containing packaging or products, and via hand-to-mouth exposure after handling PFAS-containing products [e.g., Trudel et al. (2008)]. Importantly, PFAS have been measured in numerous consumer products (e.g., fluoropolymer-coated cookware, sports clothing, food handling equipment, and medical equipment) (Posner, 2012; Washburn et al., 2005; Yuan et al., 2016).
There is evidence to suggest that PFAS are present in dental products; however, evaluations to date have been limited to dental floss and dental tape made from polytetrafluoroethylene. Begley et al. (2005) reported that these products contained 3–4 ng perfluorooctanoic acid (PFOA)/g, whereas Guo et al. (2009) reported a range of <1.5 to 96.7 ng PFOA/g. Boronow et al. (2019) considered the presence of fluorine in dental floss as an indicator of PFAS. Mamavation® reported that PFAS were suspected to be present in 13 of 39 brands of dental floss based on fluorine measurements (Segedie, 2022). Thus, only a few studies assessed the potential presence of PFAS in dental products (i.e., dental floss/tape). Importantly, specific PFAS were either not assessed (i.e., fluorine was used as a marker of PFAS) or limited to PFOA. Further, none of the aforementioned studies included a risk assessment of PFAS in these products.
Dental floss/tape is a commonly used consumer product; however, leave-in dental products (e.g., night guards, whitening trays) are used for longer periods of time and therefore offer a greater potential exposure to PFAS. Night guards are worn overnight to prevent damage due to teeth grinding while sleeping (i.e., bruxism), which is estimated to occur in adolescents (15%), middle-aged adults (8%), and older adults (3%) (Suni, 2021). Whitening trays are designed to be worn for 5–60 min, depending on the brand. Both the sleeping bruxism and whitening treatment markets represent relatively large consumer segments. According to a report by Market Research Future, the global sleeping bruxism treatment market was set to accrue $638.22 million between 2018 and 2023 (Market Research, 2018). The global teeth whitening market was estimated to reach a revenue of $8,207.20 million in 2026; however, the contribution of whitening trays to the whitening market, relative to other whitening products, was unclear (Mordor Intelligence, 2021).
On the aforementioned study by Mamavation®, Fischer (2022) noted that chemical evaluation is important to ensure consumer safety, but a mere presence of a potentially hazardous chemical may not translate into a health risk when considering its concentration, usage, and exposure. This study demonstrates how risk assessment can be integrated by the industry into product stewardship programs.
This study aimed to characterize the presence of 24 PFAS in two common brands of night guards and whitening trays and to conduct a screening-level risk assessment to evaluate whether consumer usage of these dental products poses a potential health risk. The current study also considered potential for ecological impacts due to PFAS leaching from dental products upon disposal. The ecological aspect was included based on documented PFAS discharge to and accumulation in the environment [e.g., Ahrens and Bundschuh (2014); Casal et al. (2017); Gonzalez-Gaya et al. (2019); Murray and Salim (2019)]. Specifically, the annual mass of measured PFAS from landfill leachate to wastewater treatment plants in the United Stated (U.S.) in 2013 was estimated to range from 563 to 638 kg (Lang et al., 2017). To our knowledge, our study is the first to identify, quantify, and describe the potential for human health and ecological implications due to PFAS from leave-in dental products.
Materials and methods
Dental products
Information on samples tested.
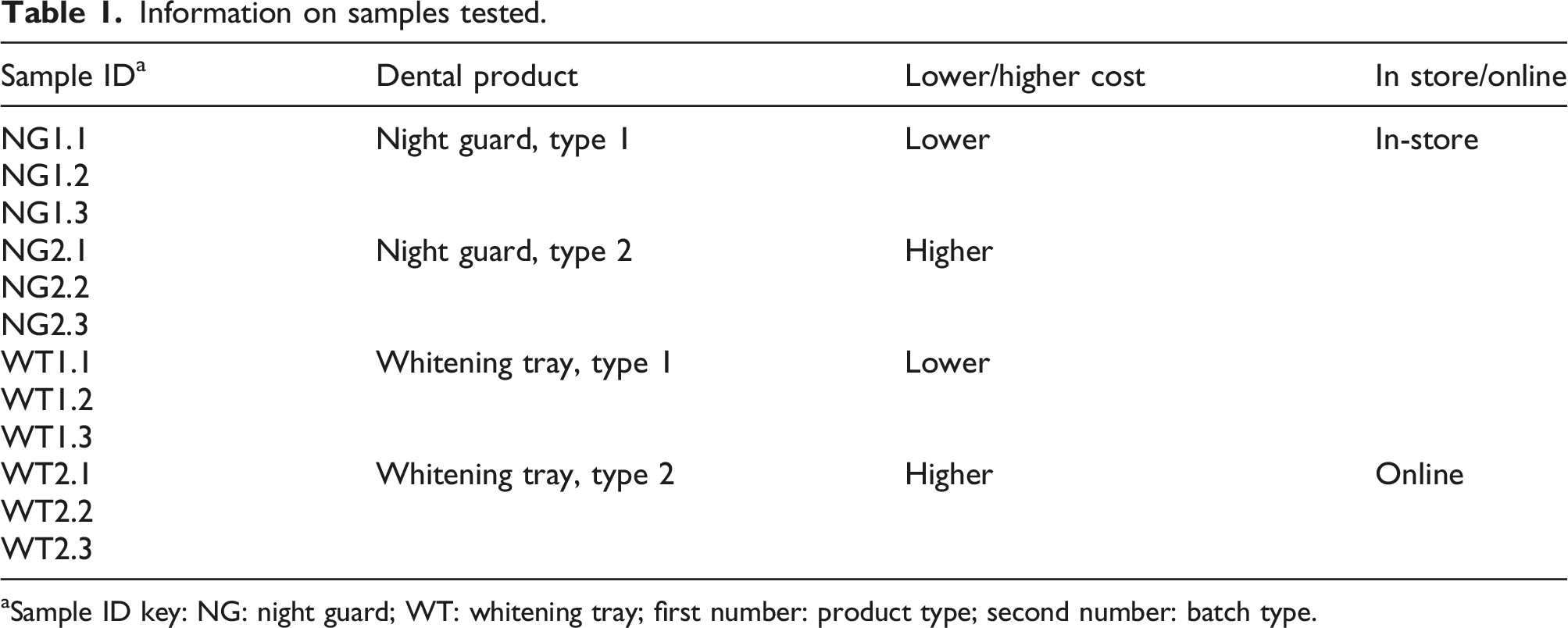
aSample ID key: NG: night guard; WT: whitening tray; first number: product type; second number: batch type.
PFAS analyses
According to Boronow et al. (2019), 11 PFAS were detected in serum of middle-aged women in the Child Health and Developmental Studies from 2010 to 2013 (Table S1). These 11 PFAS were included in our analysis. Additionally, 13 other PFAS were selected for evaluation to increase the comprehensiveness. Thus, a total of 24 PFAS were analyzed (Table S2).
PFAS were analyzed by Eurofins Environmental Testing Northern California, LLC, which holds certification with the Department of Defense (DoD) Environmental Laboratory Accreditation Program (ELAP) and state accreditations for per- and polyfluorinated chemical analysis. Sample preparation and analysis details are provided in Supplemental Materials. Briefly, unopened night guards and whitening trays were shipped in original packaging to the laboratory. The products were opened by laboratory personnel, weighed, ground into small particulates, and serially extracted with basic methanol (0.4% KOH). The extracts were dried with nitrogen and reconstituted in 96% methanol/water. It is noteworthy that PFAS are not addressed in ISO 10993-18: 2020; thus, the current protocol involved use of basic methanolic solutions to extract PFAS. Since PFAS are both hydrophobic and hydrophilic, neither the individual heptane, isopropyl alcohol nor water solutions described in the ISO method are appropriate PFAS extraction solvents. It is also noteworthy that the grinding of the products to particulates exceeds the ISO 10993-18: 2020 guidance for medical device extraction conditions; thus, the extraction method used is likely a worst-case evaluation of the potential exposure.
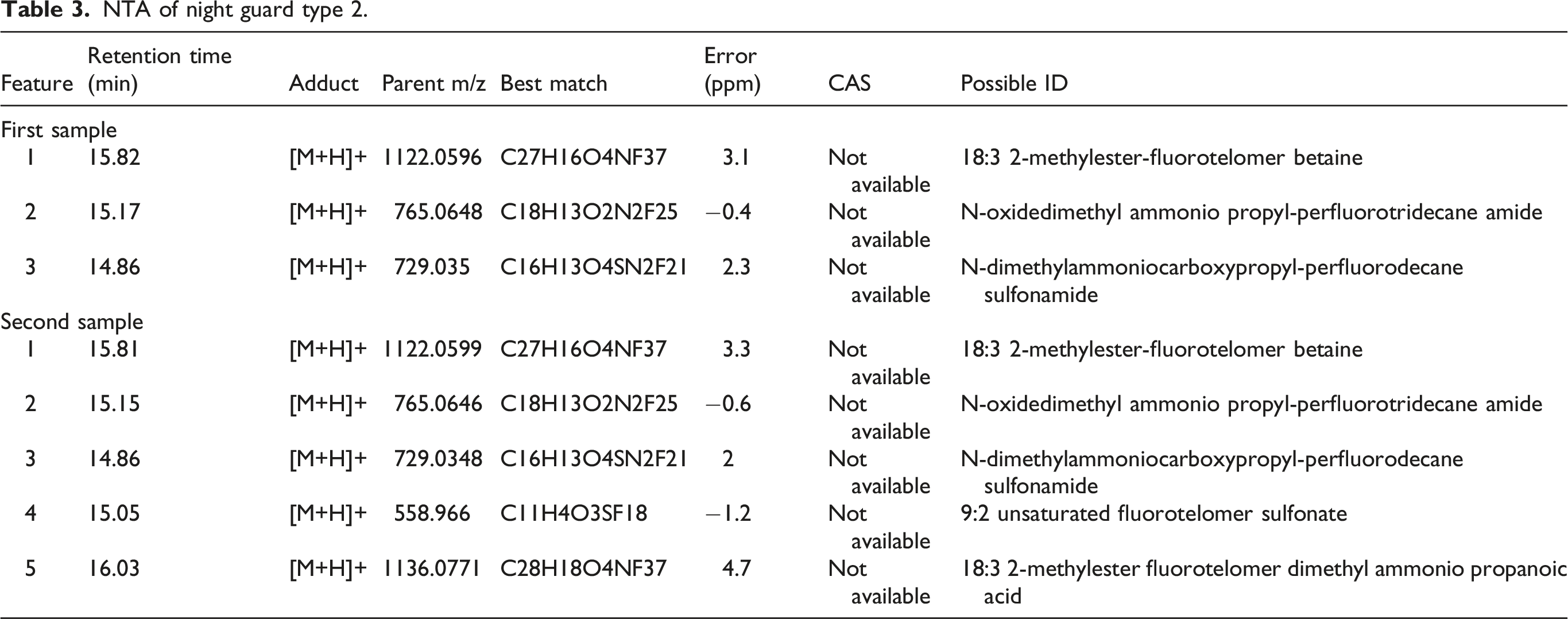
In addition to measuring the 24 specific PFAS in all products, an exploratory non-targeted analysis (NTA) was performed in duplicate on select products in which PFAS were detected to qualitatively assess the potential presence of additional fluorinated or perfluorinated compounds. This analysis was conducted by Eurofins as detailed in Supplemental Materials.
Screening-level exposure assessment and risk characterization
The measured or estimated concentrations of PFAS from each dental product were used to conduct a screening-level risk assessment, which involved comparing daily exposure estimates to available health guidance values (HGVs). The daily exposures (mg/kg/d) to PFAS from night guards and whitening trays were estimated by assuming that the entire mass of the individual PFAS (measured or estimated) leached out of the product during the first use, representing the worst-case scenario. Adult body weight was assumed to be 70 kg. While the Exposure Factors Handbook recommends a body weight of 80 kg, 70 kg is commonly used in risk assessments by the U.S. Environmental Protection Agency (EPA) and was selected as a more conservative option in this risk assessment (U.S. EPA, 2011).
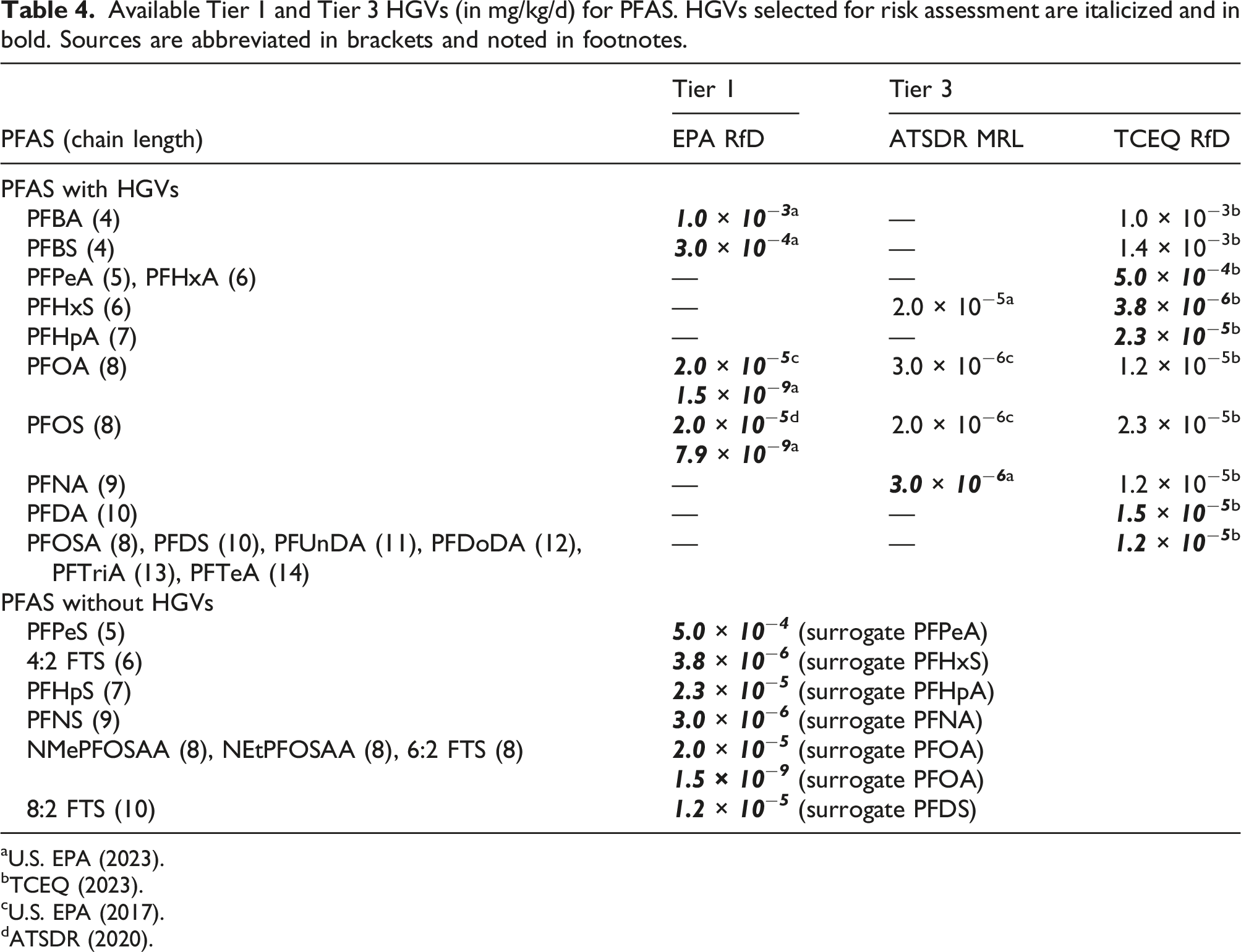
The estimated exposures were compared to HGVs. The selection of HGVs was conducted according to the tiered approach in line with EPA recommendations (U.S. EPA, 2003). For PFAS without HGVs, surrogate HGVs were used based on structural similarity to PFAS with available HGVs (i.e., chain length). Hazard quotients (HQs) were calculated by dividing the daily PFAS exposure from the dental product by the HGV (HQ > 1.0 represents the potential for increased risk of adverse health effects).
Ecological implications
The potential for ecological implications associated with PFAS from the leave-in dental products was assessed using a conservative scenario. It was assumed that dental products were disposed at a landfill site and that the entire mass of the individual PFAS (measured or estimated) leached into the landfill leachate. For night guards, it was assumed that 37% of the U.S. population (i.e., 332,915,073 people) used these products [according to Clark (2020), 5%–37% of the population has bruxism]. For whitening trays, it was assumed that 11% of the U.S. population used these products [according to Statista (2020), 37 million of Americans used tooth whiteners in 2020]. Further, it was assumed that two dental products of each type are used per year by each person (note: currently, there are no data on the frequency of use). Thus, the total amount of PFAS from dental products was characterized using equation (1). The estimated amount of PFAS was then compared to the estimated PFAS release to U.S. municipal landfill leachate as per Lang et al. (2017) PFASleach: maximum amount of PFAS that can leach from two dental products (mg) Usage: 37% U.S. population (night guards) and 11% (whitening trays) (assumptions) Products: two dental products were used by an individual per year (assumption) PFASproduct: total amount of PFAS in dental products (ng/product; Table S3) 10−9: factor to account for unit conversion from “ng” to “kg”
Results
PFAS analyses
Measured (bold values) and estimated (based on LODs) amounts of PFAS in dental products (ng/product). For information on sample ID, refer to Table 1.
NTA of night guard type 2.
Screening-level exposure assessment and risk characterization
Available Tier 1 and Tier 3 HGVs (in mg/kg/d) for PFAS. HGVs selected for risk assessment are italicized and in bold. Sources are abbreviated in brackets and noted in footnotes.
The average exposure estimates for all PFAS in both product types were well below the current HGVs, assuming leaching of available mass over a single day of usage (Figure 1; Table S4). However, when considering the draft RfDs for PFOA and PFOS, the exposure estimates for PFOA and PFOS exceeded HGVs; exposure estimates for N-methylperfluorooctanesulfonamidoacetic acid (NMePFOSAA), N-ethylperfluorooctanesulfonamidoacetic acid (NEtPFOSAA), and 6:2 fluorotelomer sulfonic acid (FTS) were also above the HGV when using the PFOA draft RfD as a surrogate. Notably, PFOA, NMePFOSAA, NEtPFOSAA, and 6:2 FTS were not detected in any sample; thus, the estimated exposures were based on the LOD and may be overestimates of actual exposure. Average exposure estimates for PFAS in leave-in dental products. The HGVs are denoted with vertical lines and numbered text bubbles.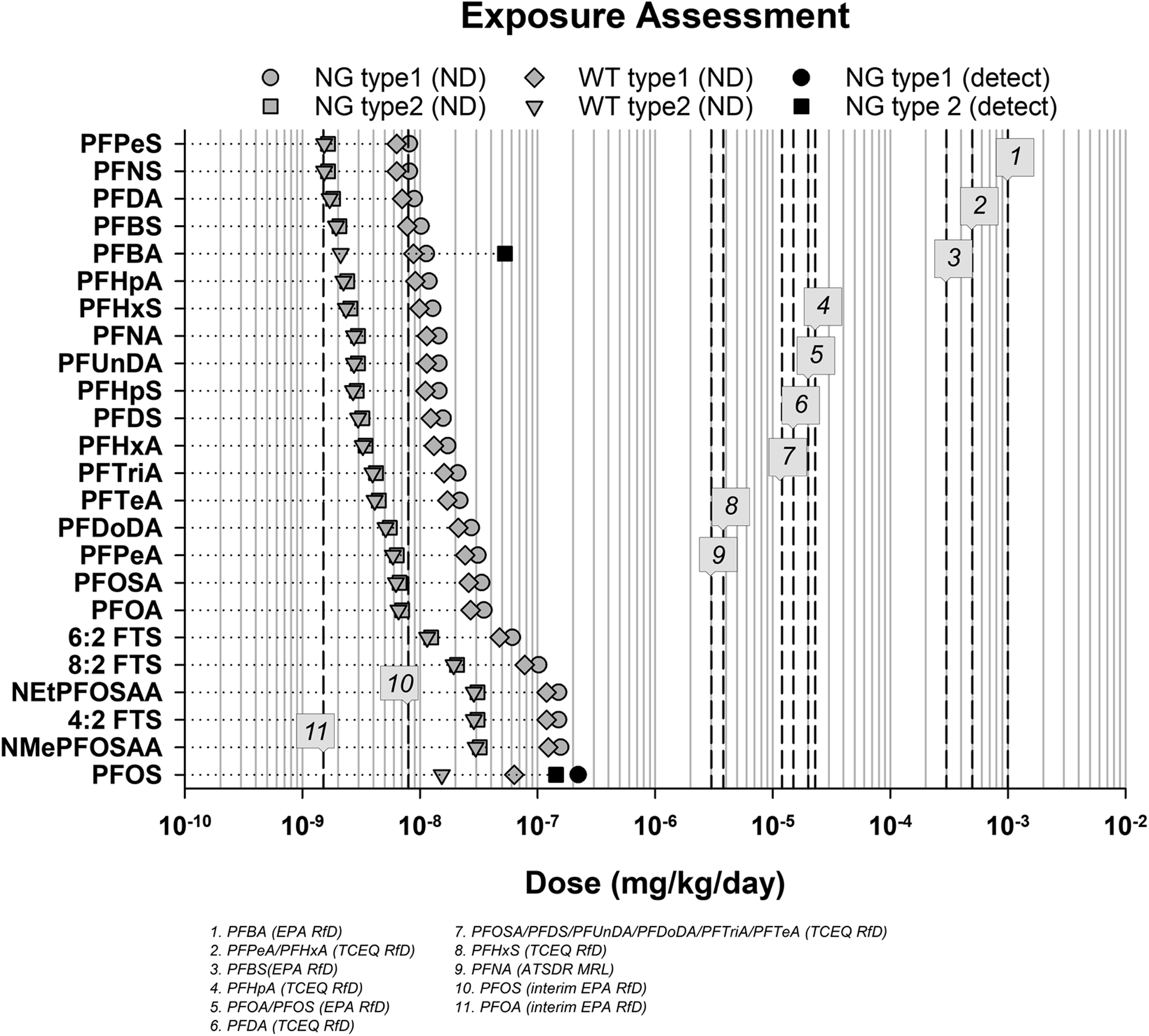
The HQs for all PFAS in both product types were <1.0 when using current HGVs (Figure 2(a); Table S5). Thus, based on the current HGVs, the risk potential is low. However, when considering the draft RfDs for PFOA and PFOS, the HQs for PFOA and PFOS exceeded 1.0; HQs for NMePFOSAA, NEtPFOSAA, and 6:2 FTS were also >1.0 when using the PFOA draft RfD as a surrogate (Figure 2(b); Table S6). Average HQs for PFAS in leave-in dental products relative to HQ of 1.0 when using current HGVs (a) and interim HGVs (b).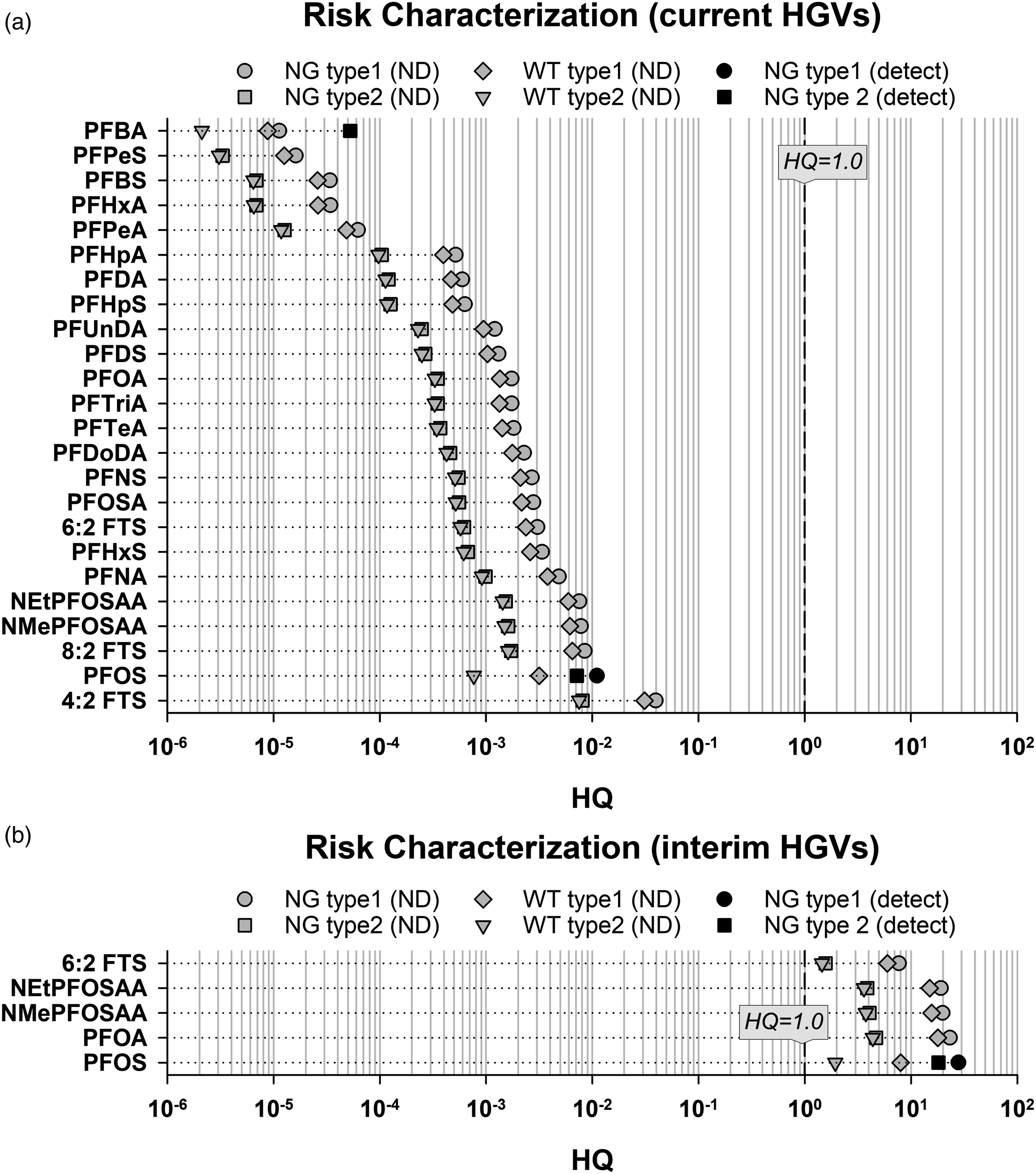
Given the exceedances when using draft RfDs, sensitivity analyses were conducted to provide additional insights on risk potential of PFOS, PFOA, NMePFOSAA, NEtPFOSAA, and 6:2 FTS. Because this assessment assumed that 100% of the available PFAS leaches following a single exposure event (i.e., in 1 day), the sensitivity analyses considered potential for leaching over time, assuming some fraction of the available PFAS leaches per day. The first analysis (HQs were re-calculated by assuming daily leaching percentages of 1%, 10%, 25%, 50%, and 100%) showed that the HQs decreased with decreased leaching, such that the HQs were <1.0 for all products and all PFAS when leaching was set to 1% (Figure 3(a); Table S7). The second analysis [HQs were re-calculated by assuming that leaching of all PFAS content occurred (linearly) over 1, 7, 14, 28, or 56 days to consider the more likely use patterns of the product (i.e., a night guard is likely used over several weeks or months and not replaced daily; whitening trays are unlikely to be used daily)] showed that the HQs were below 1.0 for all PFAS in both product types when leaching occurred over 56 days, whereas leaching over a 28-day period resulted in HQs < 1.0 except for a single substance (PFOS) for which the HQ was equal to 1.0 (Figure 3(b); Table S8). The sensitivity analyses demonstrated that, when considering more realistic exposure conditions (i.e., leaching is not 100% and occurs over multiple days), the risk potential is likely low even when using the more conservative draft RfDs. Average HQs for PFOS, PFOA, NMePFOSAA, NEtPFOSAA, and 6:2 FTS in leave-in dental products relative to HQ of 1.0 when using different leaching percentage (a) and duration (b) scenarios.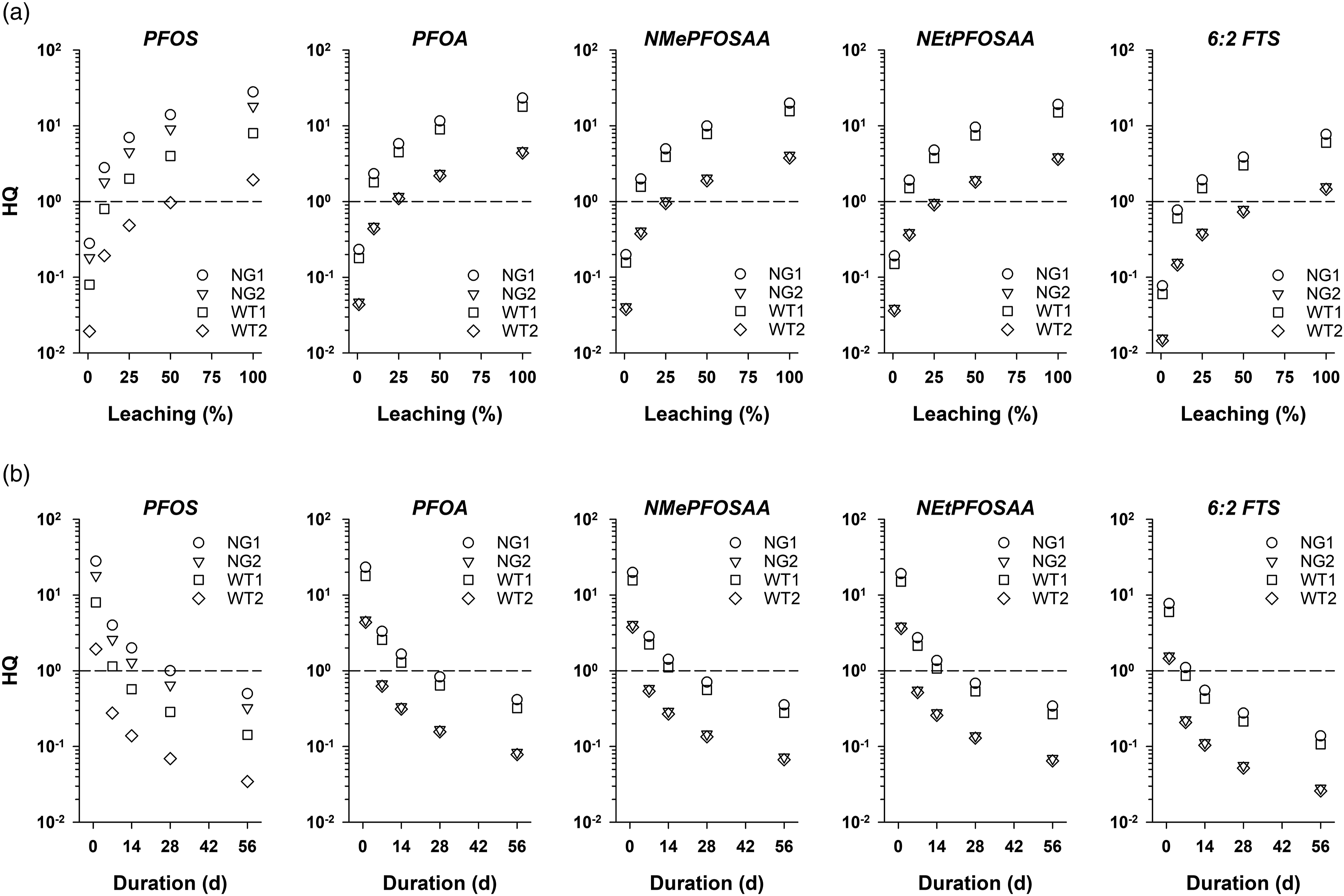
Ecological implications
It was estimated that the hypothetical disposal of night guards and whitening trays near waste sites across the U.S. would contribute to a total of 20.01 and 4.07 g PFAS annually, respectively. These cumulative estimates include all PFAS tested herein, a majority of which were below the LOD. As aforementioned, the mass of measured PFAS from U.S. landfill leachate to wastewater treatment plants was estimated to be between 563 and 638 kg. Thus, the amount of PFAS leached from night guards and whitening trays (under the usage parameters assumed herein and using censored data) into the environment would represent approximately 0.004% of total PFAS in leachate. Notably, the approach is conservative given the use of censored data as well as the assumptions that (i) no PFAS leached during consumer use and (ii) all PFAS leached from the products within 1 year when disposed at the waste sites.
Discussion
This study measured PFAS in night guards and whitening trays and evaluated the potential for human health and ecological implications. With limited exceptions, the 24 measured PFAS were generally not detected across the products evaluated, suggesting that these PFAS are not likely to be found in these products or are present in only trace levels. Both PFOS (7.25 to 16.45 ng/product) and PFBA (3.24 to 4.17 ng/product) were detected in night guards tested. Though different products, the range of measured PFAS concentrations in night guards are similar to those reported for dental floss and tape (Begley et al., 2005; Guo et al., 2009). However, Begley et al. (2005) and Guo et al. (2009) both reported the presence of PFOA (possibly as an impurity in PTFE); PFOA was not detected in any dental product sampled in this study. At this time, the origin of the PFAS detected in these dental products is unknown, but could result from various sources, including precursors, degradation products, or contamination.
A screening-level risk assessment conducted based on the measured/estimated concentrations of PFAS in this study showed that no health risks are anticipated from the use of these products. Using the current HGV and worst-case assumptions for release of PFAS (i.e., leaching occurs at 100% over a single day), the HQs for all PFAS were <1.0 in both product types. When considering the draft RfDs for PFOA and PFOS, the HQs exceeded 1.0; however, sensitivity analyses showed that, under more realistic leaching scenarios, the HQs were likely to be below 1.0.
In addition to having a low likelihood of risk, leave-in dental products contribute very little to overall consumer exposure to PFAS. In the general population, food and contaminated drinking water are expected to be the largest contributors to human PFAS exposure (Trudel et al., 2008). The presence of PFAS in food can result from contact with food-contact materials containing PFAS or uptake into foodstuffs (vegetables and animal) from environmental media such as soil, water, and biosolids (Dalahmeh et al., 2018; Gobelius, 2016; Lee et al., 2014; Trier et al., 2011; Yoo et al., 2011). Though studies on PFAS contamination of food products are limited in the U.S., the European Food Safety Authority conducted a survey of foods in the European Union from 2006 to 2012, detecting PFAS in most of the 7,560 food samples tested (EFSA, 2012). With respect to drinking water, PFAS are detected ubiquitously in samples globally (Domingo and Nadal, 2019). Sampling in the U.S. has also indicated high frequencies of detection of various PFAS in drinking water (Boone et al., 2019; Crone et al., 2019; Kaboré et al., 2018).
Daily doses from leave-in dental products are expected to fall well below those from food or contaminated drinking water. Poothong et al. (2020) estimated daily intake of 10 PFAS from food (mean total PFAS daily dose = 743.4 pg/kg/d); collectively, these represent 74% of average total daily intake of these 10 PFAS from diet, dermal absorption, house dust, and indoor air. For the same 10 PFAS, total daily doses from leave-in dental products (based on 100% leaching over a single day) were expected to be 198.1 pg/kg/d, representing approximately 20% of total daily intake of these 10 PFAS from diet, dermal absorption, house dust, and indoor air.
Daily exposures from contaminated drinking water are highly contingent on the level of contamination. However, as a point of comparison, the lowest and highest measured PFOS concentrations in drinking water (excluding bottled water) were reported to range from 0.071 to 97.5 pg/mL (Jian et al., 2017). Thus, assuming a daily water intake of 1,043 mL/d (U.S. EPA, 2019) and body weight of 70 kg, these concentrations correspond to daily PFOS intakes of 1.06 and 1,452.8 pg/kg/d, respectively. Across the products from this study, the average daily intake of PFOS from leave-in dental products under worst-case conditions was 110 pg/kg/d. Therefore, while leave-in dental products may contain trace concentrations of certain PFAS, such exposures are unlikely to contribute substantively to daily body burden of PFAS when compared to other sources.
Our conclusions are based on assumptions made in this risk assessment and are therefore subject to uncertainties and limitations in the analysis. Uncertainties and limitations in this analysis involve assumptions regarding (1) hazard and dose response associated with both single and cumulative PFAS exposures, (2) temporality of leaching of PFAS from dental products, and (3) concentrations of PFAS when concentrations did not exceed analytical detection limits. These assumptions may over- or under-estimate risk, depending on the specific assumption.
In this assessment, HGVs were selected using a hierarchical approach recommended by the U.S. EPA for selecting appropriate values for use in risk assessment, and included U.S. EPA RfDs, ATSDR MRLs, and TCEQ RfDs. For some chemicals, publicly available HGVs were unavailable. In these instances, the most conservative HGV was selected as a surrogate relying on chain length information. It is acknowledged that, even if PFAS may exhibit similar effects, the potency can vary substantially by chain length and by form. For example, vastly different HGVs are presented for perfluorobutanesulfonic acid (PFBS) and PFOS, which are similar in form but have different chain lengths. Therefore, this default approach may overestimate risk for PFAS for which no HGVs exist.
In addition, there are discrepancies in recommended HGVs between and within agencies. In this assessment, RfDs used by the U.S. EPA for the establishment of the initial and draft Provisional Health Advisories for drinking water were selected as HGVs for PFOA and PFOS (U.S. EPA, 2017; U.S. EPA, 2022). However, ATSDR has proposed alternate MRLs for PFOA and PFOS that are 10-fold lower than current U.S. EPA RfDs (ATSDR, 2020). Furthermore, the draft U.S. EPA RfDs for PFOA and PFOS of 1.5 × 10−9 and 7.9 × 10−9 mg/kg, respectively, have come under significant scrutiny since their publication (U.S. EPA, 2022). Both the ATSDR MRLs and the draft EPA RfDs for PFOA and PFOS are the result of selecting alternative critical health endpoints, specifically, potential immune effects as well as using human data rather than animal data. Several epidemiological studies, largely in a cohort of children in the Faroe Islands, observed decreased antibody response to childhood vaccinations in children exposed to PFAS. However, the findings in these studies are inconsistent across antigens (e.g., rubella, mumps, and tetanus), age, and booster status (Grandjean et al., 2012, 2017). Further, the epidemiological studies assessing PFAS exposure and susceptibility to infectious disease (reflecting decreased immune function) demonstrate no clear or consistent associations [e.g., Fei et al. (2010); Impinen et al. (2018); Kvalem et al. (2020); Looker et al. (2014)], suggesting the effects on antibody response may not manifest in adverse health outcomes; thus, screening values developed on this basis could be considered overly conservative.
To account for the uncertainties with respect to potency of effects of PFAS, we also considered potential risks associated with leave-in dental products using the new proposed U.S. EPA RfD and the ATSDR MRL for PFOS based on the detection of this specific PFAS in two products. Under the assumptions used in this risk assessment, daily exposures to PFOS would exceed the draft proposed U.S. EPA RfD of 1.5 × 10−9 mg/kg/d (HQ = 9.1 to 156.6, depending on product), but not the ATSDR MRL of 2.0 × 10−6 mg/kg/d. However, this initial assessment assumed all PFAS leached within the first use, a scenario that is highly unlikely. Predicted exposures to PFOS would fall below the draft U.S. EPA RfD for all products tested if complete release of PFOS took at least 28 days. Furthermore, leaching of less than 100% of the total available PFOS would also reduce daily exposure to PFOS. Incomplete leaching combined with leaching over time is a more probable scenario than the assumptions in our base screening-level assessment, which are intended to represent an upper bound estimate on exposure and risk for the purposes of being conservative.
In addition to uncertainties with respect to hazard and dose response assessment, many of the assumptions in the exposure assessment were intended to overpredict potential health risk. Firstly, it was assumed that 100% of the available PFAS leached from the leave-in dental product on the first day of use, resulting in the maximum possible daily dose. This scenario is highly improbable, though additional data are required to understand what fraction of the PFAS can be leached and over what duration of time this leaching occurs. Notably, even if immediate and complete leaching of PFAS from these dental products could occur, the use pattern of the product could be considered (i.e., a night guard is likely used over several weeks or months and not replaced daily; whitening trays are unlikely to be used daily); therefore, average daily doses would be reduced compared to what was predicted in our screening-level assessment, depending on frequency of use or replacement.
Secondly, most PFAS were not detected in this study; only PFBA and PFOS were detected in select dental products. This finding suggests that PFAS are either not used in abundance in the manufacture of these products, not intentionally added, or used in only select products. To estimate risk, we assumed PFAS were present in all products at either (1) the measured concentration, where appropriate, or (2) one-half the LOD, when not detected. This assumption is consistent with standard practices for treatment of censored data in risk assessment, but includes uncertainty with respect to actual concentrations present. Though the concentrations of these substances could theoretically fall above or below the assumed concentration, given the overall lack of detection of most of the measured PFAS across these products, it is likely conservative to assume the substance is present at all. Furthermore, even if all non-detect PFAS were present in the leave-in dental products at concentrations equivalent to the LOD, the respective HQs for these PFAS would still be <1.0, which indicates that no adverse health effects are expected from the products.
While this study focused on human health, ecological impacts associated with disposal of dental products and subsequent leaching of PFAS were also considered. Our analysis showed that the amount of PFAS in night guards and whitening trays would represent only about 0.004% when compared to the total amount of PFAS of 563–638 kg in landfill leachate estimated by Lang et al. (2017). Thus, our analysis indicates that PFAS in dental products are not likely to be significant sources of environmental PFAS upon disposal, even under conservative leaching assumptions.
Conclusion
This study examined the presence of PFAS in leave-in night guards and whitening trays. Out of 24 PFAS measured, only PFBA and PFOS were detected in the tested night guards, and none of the measured PFAS were detected in the tested whitening trays. Screening-level risk assessment showed that the presence of PFOS and/or PFBA in night guards was unlikely to pose a human health concern or be a significant source of PFAS in comparison to major sources such as drinking water and food. Ecological assessment revealed that disposed night guards and whitening trays would contribute negligible amounts to environmental PFAS. In conclusion, the leave-in dental products examined did not represent a significant source of PFAS for humans or the environment.
Supplemental material
Supplemental Material - Assessing potential human health and ecological implications of polyfluoroalkyl substances from leave-in dental products
Supplemental Material for Assessing potential human health and ecological implications of polyfluoroalkyl substances from leave-in dental products by Andrey Massarsky, Jillian A Parker, Lauren Gloekler, Melinda T Donnell, Natalie R Binczewski, Jordan S Kozal, Taryn McKnight, Andrew Patterson, and Marisa L Kreider in Toxicology and Industrial Health
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employed by (1) consulting firm Stantec ChemRisk that provides scientific advice to the government, corporations, law firms and various scientific/professional organizations, or (2) Eurofins Environment Testing Northern California, LLC, an accredited laboratory for chemical testing. The funding to conduct this research was provided by Stantec ChemRisk and Eurofins.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eurofins Environment Testing; Stantec ChemRisk.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.