
Abstract
Restless legs syndrome (RLS) is characterized by an urge to move that occurs in the evening or night time, suggesting circadian involvement. However, objective evidence regarding the circadian phase in RLS remains limited, particularly in real-world settings. We conducted an exploratory pilot study to investigate circadian rhythm timing in patients with RLS using actigraphy-based dim light melatonin onset (DLMO) estimation and to explore its potential association with symptom severity. Patients with idiopathic RLS (n = 21) and age- and sex-matched chronic insomnia controls (n = 21) underwent 14 days of wrist actigraphy to assess rest-activity rhythms and obtain estimated DLMO (eDLMO) from an actigraphy-based mathematical model. Symptom severity was evaluated with the International RLS Study Group rating scale (IRLS). Group comparisons and correlation analyses were conducted in an exploratory manner given the sample size. Patients with RLS (mean age 61.2 ± 7.7 years, 90% female) demonstrated a non-significant trend toward delayed eDLMO compared with insomnia controls (mean age 61.7 ± 7.1 years, 90% female; 10:01 PM ± 47 min vs 9:33 PM ± 49 min, p = 0.069, Cohen’s d = 0.58). Within the RLS group, higher IRLS scores were modestly associated with later eDLMO (β = 0.0726, p = 0.038), after adjusting for age and depressive symptoms. In contrast, eDLMO was not significantly associated with Insomnia Severity Index (ISI) or Pittsburgh Sleep Quality Index (PSQI) scores in the insomnia control group. In this exploratory pilot study, patients with RLS showed a tendency toward delayed estimated circadian phase compared with insomnia controls, and later estimated circadian phase was modestly associated with greater RLS symptom severity. These findings support a possible link between circadian phase delay and clinical burden in RLS but require confirmation in larger studies.
Keywords
Restless legs syndrome (RLS) is a common neurological sensorimotor disorder characterized by an irresistible urge to move the legs, often accompanied by uncomfortable or unpleasant sensations in the lower limbs (Wijemanne and Jankovic, 2015). These symptoms stereotypically emerge or worsen in the evening and at night and subside in the morning, reflecting a robust circadian pattern that has been confirmed by several studies (Hening et al., 1999; Trenkwalder et al., 1999).
Although the mechanisms underlying the circadian rhythmicity of RLS symptoms remain incompletely understood, several lines of evidence suggest contributions from iron metabolism, dopaminergic neurotransmission, and circadian clock genes. Cerebrospinal fluid ferritin concentrations, reflecting brain iron status, are lower in the morning than in the evening hours; notably, morning ferritin levels are considered to reflect night-time brain iron status, and brain iron deficiency is known to impair dopaminergic function (Earley et al., 2005). Dopamine levels in plasma also follow a circadian pattern, peaking in the morning and reaching their nadir at approximately 3 AM (Sowers and Vlachakis, 1984). Genetic studies have implicated the CLOCK gene, a key regulator of circadian rhythm, with certain CLOCK gene variants associated with decreased susceptibility to RLS in the Korean population (Jung et al., 2014).
Although several studies have examined the circadian rhythmicity of RLS symptoms, few have directly investigated whether patients with RLS exhibit alterations in the timing of the underlying circadian phase and which clinical variables may be associated with such alterations. The primary question of this study was whether patients with idiopathic RLS exhibit differences in circadian phase timing compared with a clinically relevant comparison group, and whether such differences are associated with symptom severity.
Thus, the aims of this exploratory pilot study were (1) to compare estimated circadian phase timing between patients with idiopathic RLS and chronic insomnia controls using actigraphy-based eDLMO and (2) to examine whether later estimated phase timing is associated with greater symptom severity and related clinical features within each group. We hypothesized that the RLS group would show later estimated circadian phase timing than insomnia controls, and that greater RLS symptom severity would be associated with later phase timing within the RLS group.
Methods
Patient Selection and Clinical Data Collection
This retrospective study was conducted at the Department of Neurology, Seoul National University Hospital. We reviewed patients who underwent actigraphy testing between 1 January 2014, and 1 May 2025 and had a diagnosis of either RLS or chronic insomnia disorder. Although age- and sex-matched healthy controls would have been preferable, such controls with comparable actigraphy data were not available in this retrospective real-world dataset. Accordingly, patients with chronic insomnia disorder were used as a pragmatic, clinically relevant comparison group because both groups underwent actigraphy under similar clinical conditions using the same measurement approach. Prior studies have also suggested that circadian phase differences between insomnia patients and healthy controls are often minimal or inconsistent, particularly in sleep-maintenance insomnia (Kim et al., 2020).
The RLS cohort comprised individuals meeting the 2014 revised International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria (Allen et al., 2014). Specifically, all patients were required to meet the five essential diagnostic features. Patients were excluded if they had (1) secondary RLS due to chronic kidney disease, iron-deficiency anemia, or pregnancy; (2) obstructive sleep apnea (OSA) defined as patients meeting the International Classification of Sleep Disorders, Third Edition (ICSD-3) diagnostic criteria with apnea-hypopnea index (AHI) > 15 events/h on attended overnight, with in-laboratory polysomnography scored according to American Academy of Sleep Medicine rules; (3) dopaminergic augmentation present at the time of actigraphy; or (4) a current depressive disorder. These exclusions were applied to reduce potential confounding effects on sleep-wake timing.
The chronic insomnia disorder cohort included individuals diagnosed according to ICSD-3 criteria. To assemble a relatively homogeneous insomnia comparison group, we excluded any concurrent sleep disorder based on ICSD-3 criteria, including circadian rhythm sleep-wake disorders – specifically delayed sleep-wake phase disorder (DSWPD) – OSA, REM sleep behavior disorder (RBD), shift work sleep-wake disorder, and clinically significant sleep-related movement disorders such as periodic limb movement disorder. We also excluded patients with psychiatric or medical conditions judged likely to affect sleep or behavioral sleep-waking timing (e.g. major depressive disorder, generalized anxiety disorder, migraine, nocturia, hyperthyroidism/hypothyroidism, or active cancer).
After applying these eligibility criteria, we selected an equal number of patients with RLS and chronic insomnia disorder. To minimize demographic confounding, patients in the two cohorts were matched 1:1 for age and sex using nearest-neighbor matching without replacement. This approach ensured comparable baseline characteristics between the groups and allowed more reliable comparisons of the estimated circadian phase derived from actigraphy-based modeling.
The following clinical variables were collected for each group. For the RLS group, demographic data included sex, body mass index (BMI), age at symptom onset, and age at the time of actigraphy. Clinical history variables included the presence of a family history of RLS, the time of day when leg symptoms typically occurred, and the presence of pain. Sleep and psychiatric assessments were obtained using standardized questionnaires, including the International RLS Study Group rating scale (IRLS) (Walters et al., 2003), Insomnia Severity Index (ISI) (Bastien et al., 2001), Pittsburgh Sleep Quality Index (PSQI) (Buysse et al., 1989), Epworth Sleepiness Scale (ESS) (Johns, 1991), and Beck Depression Inventory (BDI) (Beck et al., 1961). Laboratory values such as serum ferritin, transferrin saturation, and hemoglobin levels were also recorded. Information on medications taken at the time of actigraphy was collected, including whether the patient was taking any medication and, if so, whether the prescribed drug was a dopamine agonist or an α2δ ligand.
For the chronic insomnia disorder group, collected variables included sex, BMI, age at symptom onset, and age at the time of actigraphy. Standardized sleep and psychiatric questionnaires were administered, including the PSQI, ISI, ESS, and BDI.
This study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Hospital (IRB no. 2507-032-1655), and all analyses were conducted in accordance with institutional and ethical guidelines.
Estimation of Circadian Phase (DLMO) Using Actigraphy
Participants wore a wrist-worn actigraphy device (Actiwatch Spectrum PRO; Philips Respironics, Murrysville, PA, USA) on the non-dominant hand continuously for 2 weeks. The device collected both motor activity and ambient light exposure at 32 Hz, and the raw signals were averaged into 30-second epochs. Activity counts were calculated as a relative measure of movement intensity based on the summed peak accelerations within each epoch. Initial estimates of bed and wake times were generated using Actiware software (version 6.0.9; Philips Respironics). These estimates were then visually reviewed, and sleep diary entries were consulted only when the automated estimates appeared implausible, particularly for bedtime, sleep latency, final awakening, or getting-out-of-bed time. In ambiguous cases, actigraphy-derived light-sensor data were reviewed qualitatively as an ancillary aid but were not used as a formal scoring input.
Circadian phase was estimated as the dim light melatonin onset proxy (eDLMO) using a validated mathematical model of the human circadian system that simulates the human circadian rhythm of core body temperature (CBT) modulated by the light exposures (Forger et al., 1999) and is considered one of the most effective computational methods for estimating circadian phase in field settings (Stone et al., 2020). Although the most ideal input for this mathematical model is direct light exposure data from actigraphy data, raw light data from wearable actigraphy devices were not used in this study due to concerns regarding measurement reliability, as wearable light sensors are often obstructed by clothing or body posture. Previous studies have shown that estimating light exposure from activity data yields more accurate circadian phase predictions than using raw light data (Huang et al., 2021). Following this evidence, we generated individualized light profiles from actigraphy-based sleep-wake patterns, assigning 0 lux light intensity during sleep intervals and 250 lux during wake intervals. To assess the impact of this assumption, a sensitivity analysis was performed in which wake after sleep onset (WASO) periods were assigned 250 lux using an approximate midsleep-centered placement, and eDLMO was re-estimated, yielding a consistent shift in absolute values without altering the between-group differences (Suppl. Fig. S2). The choice of 250 lux has been validated as a reasonable approximation of typical indoor light exposure and has been shown to provide accurate circadian phase predictions despite its simplicity (Lim et al., 2025). These light profiles were utilized as an input for a mathematical model (Forger et al., 1999), which simulated the rhythm of CBT. The minimum point of the simulated CBT was identified for each participant, each day, and eDLMO was estimated by subtracting 7 h from this daily CBT minimum (Figure 1). Thus, in this study, eDLMO represents a model-derived proxy of circadian phase rather than a direct melatonin measurement. This approach has been validated and widely used in prior studies to estimate circadian phase in field settings, including in individuals with irregular sleep-wake schedules such as shift workers (Cheng et al., 2021; Huang et al., 2021; Knock et al., 2021; Lim et al., 2025, 2026; Postnova et al., 2014; Stone et al., 2020; Weed et al., 2026; Woelders et al., 2017). Participant-level actigraphy raster plots are provided in Supplementary Figure S1A-B to illustrate sleep-wake patterns across the recording period.
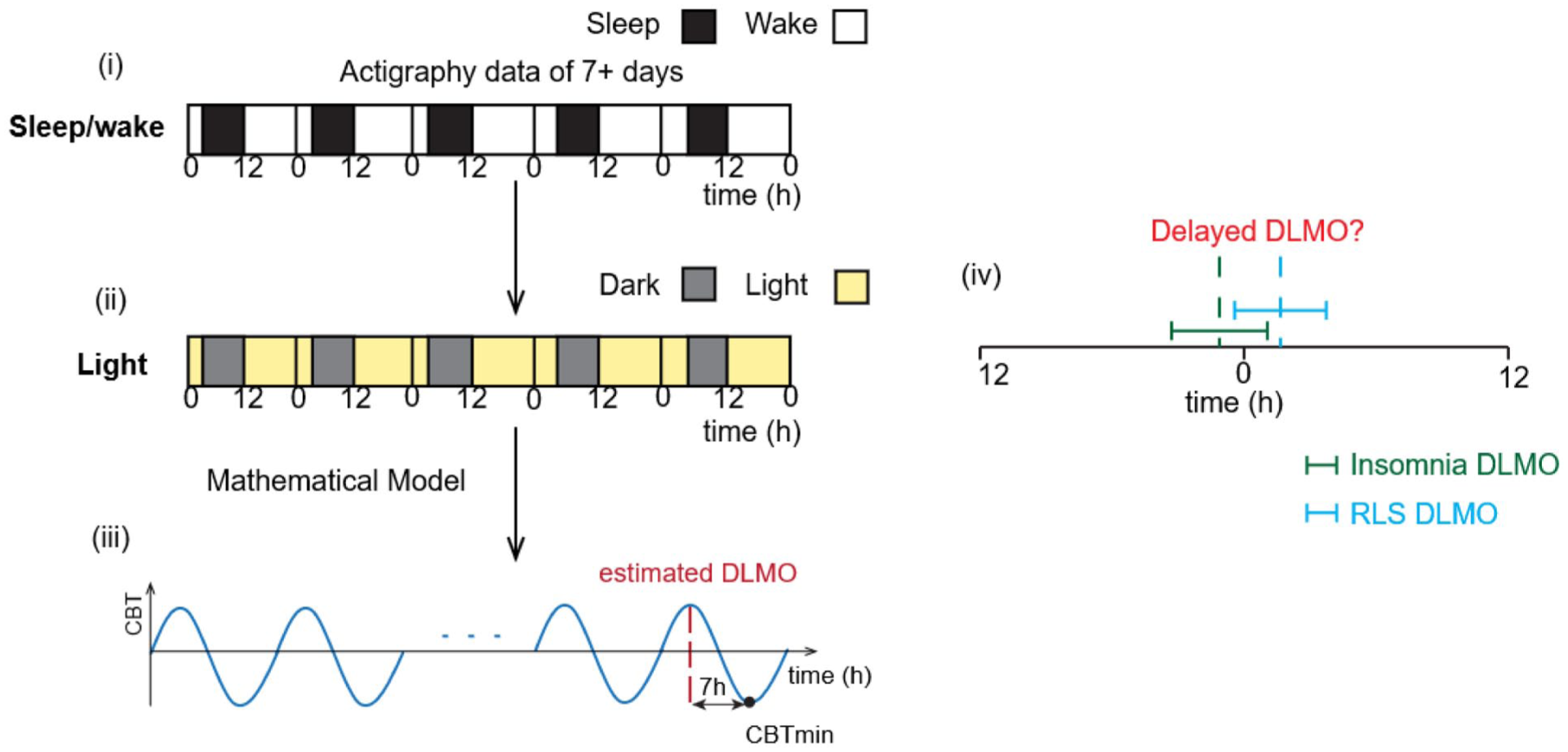
Estimation of DLMO using actigraphy and mathematical modeling. (a) To estimate the DLMO, (1) actigraphy data of more than 7 days were used, focusing on individual sleep-wake patterns. From these patterns, (2) a light profile was derived by assuming light during wake and dark during sleep. This profile was used as input for a mathematical model that (3) simulates the core body temperature (CBT) rhythm (blue curve). From the simulated CBT rhythm, the minimum time point of the core body temperature (CBTmin) was identified, and DLMO (red dotted line) was predicted by subtracting 7 h from this CBTmin. (4) Estimated DLMO values were then compared between groups to examine whether patients with RLS exhibited a delayed circadian phase relative to insomnia controls.
Circadian phase estimation using ordinary differential equation-based models requires specification of initial conditions (ICs), which define the state of the circadian system at the beginning of the simulation. In actigraphy-based field studies, however, the true IC is typically unknown because it depends on prior sleep-wake and light exposure history preceding the recording period, which is not observed. Consistent with established practice, the model was initialized by simulating the 50 consecutive repetitions of an 8-hsleep episode centered on each individual’s average midsleep, following previous studies (Stone et al., 2019). To mitigate the influence of those imposed assumptions, a transient convergence period was applied. Since circadian phase estimates during this early period are driven primarily by the assumed ICs rather than the sleep-wake behavior, eDLMO values for the first 3 days were excluded from all subsequent analyses.
Statistical Analyses
All statistical analyses were performed using R software (version 4.4.2). The primary outcome was the eDLMO, defined as an actigraphy-derived, model-based estimation of DLMO. For each participant, an eDLMO was calculated, and group-level differences in mean eDLMO between the RLS and insomnia control groups were assessed using an independent 2-sample t test. As the groups were matched for age and sex, no additional covariate adjustment was applied.
In addition to the primary outcome comparison, baseline characteristics between the RLS and insomnia groups – including age at the time of actigraphy, age at symptom onset, sex, BMI, medication use, PSQI, ISI, ESS, and BDI scores – were also compared. Depending on the distributional properties of each variable, either an independent 2-sample t test or the Mann-Whitney U test was applied for continuous variables. For categorical variables such as sex and medication use, Fisher’s exact test was used to compare proportions.
Associations between eDLMO and continuous clinical variables were assessed within each group using either Pearson’s or Spearman’s correlation coefficients, depending on the distributional properties of the data. Normality was evaluated using the Shapiro-Wilk test. When the assumption of normality was satisfied, Pearson’s correlation was applied; otherwise, Spearman’s rank correlation was used. In addition, based on prior evidence that DLMO tends to advance with increasing age (Kennaway, 2023), partial correlation analyses were conducted with adjustment for age at the time of actigraphy as a covariate. Associations between eDLMO and categorical clinical variables were assessed separately within each group using either the independent t test or the Mann-Whitney U test, depending on the results of the Shapiro-Wilk test (normality) and Levene’s test (homogeneity of variance).
To further explore the relationship between eDLMO and key clinical predictors, a multiple linear regression analysis was conducted with eDLMO as the dependent variable. Independent variables included age at the time of actigraphy, IRLS, ESS, ISI, PSQI, and BDI scores. These variables were selected based on preliminary correlation analyses within the RLS group (Suppl. Table 1) and clinical relevance and were included in an exploratory modeling framework given the sample size. Missing data were handled using multiple imputation via the MICE package in R. Multicollinearity was assessed using variance inflation factors (VIF). Model diagnostics included evaluation of residual plots for linearity and homoscedasticity, Q-Q plots for normality, and assessment of leverage and Cook’s distance for influential outliers.
Results
Study Population and Baseline Characteristics
A total of 24 patients with RLS were initially identified. Among these, 2 were excluded due to comorbid OSA, and 1 due to missing actigraphy data. Consequently, 21 patients with idiopathic RLS were included in the final analysis. In the chronic insomnia disorder cohort, 136 patients were initially screened. Of these, 98 patients met one or more exclusion criteria, leaving 38 patients with isolated chronic insomnia disorder. From this group, 21 patients were selected as a matched comparison group based on age at the time of actigraphy and sex with the RLS cohort.
The demographic and clinical characteristics of the idiopathic RLS group and the insomnia control group are summarized in Table 1. The two groups were comparable in terms of age at the time of actigraphy and sex, consistent with the matching procedure. There were no significant between-group differences in BMI, PSQI, ISI, ESS, BDI, or medication usage. Although the mean age at symptom onset was lower in the RLS group (41.7 ± 18.0 years) than that in the control group (51.8 ± 13.9 years), this difference did not reach statistical significance (p = 0.081). It should be noted that symptom onset in RLS refers to the first occurrence of sensorimotor symptoms, whereas in insomnia controls, it denotes the onset of persistent sleep-related complaints; therefore, this variable represents different clinical symptoms across the two groups and is not directly comparable as a baseline characteristic.
Demographic and clinical characteristics of the idiopathic RLS group and insomnia control group.
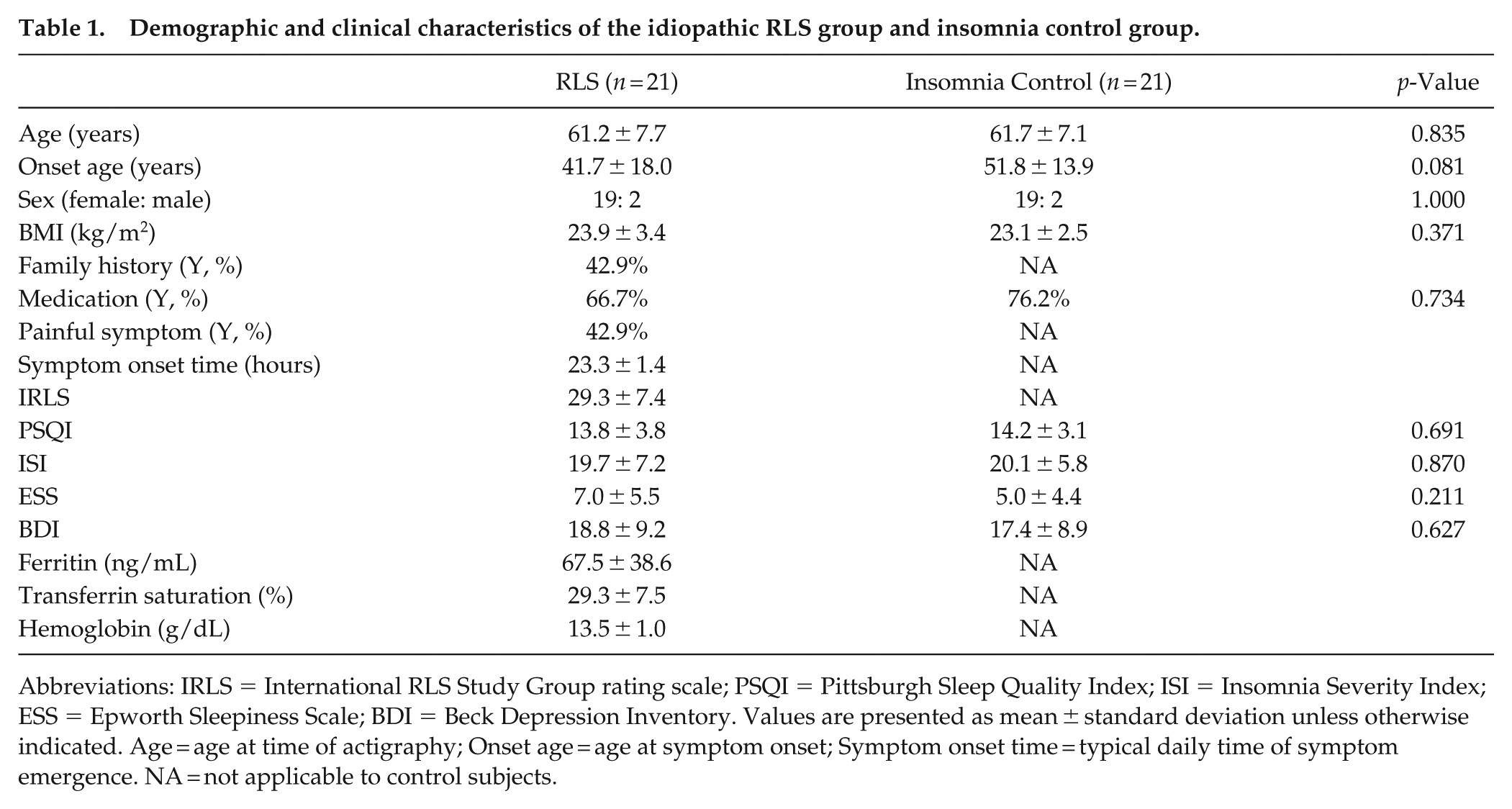
Abbreviations: IRLS = International RLS Study Group rating scale; PSQI = Pittsburgh Sleep Quality Index; ISI = Insomnia Severity Index; ESS = Epworth Sleepiness Scale; BDI = Beck Depression Inventory. Values are presented as mean ± standard deviation unless otherwise indicated. Age = age at time of actigraphy; Onset age = age at symptom onset; Symptom onset time = typical daily time of symptom emergence. NA = not applicable to control subjects.
With respect to medication profiles, specific details including medication class and drug name during the actigraphy recording period are summarized in Supplementary Table 2. Most RLS patients were prescribed dopamine agonists (n = 12), while 2 patients received α2δ ligands and 7 were drug-naïve. Given the small number of α2δ ligand users, exploratory subgroup analyses were conducted within the RLS group: (1) medication users versus non-users, and (2) dopamine agonist users versus non-users, with the latter group combining α2δ ligand users and drug-naïve individuals. In the insomnia control group, 5 patients were treated with benzodiazepines, and 4 with zolpidem. Seven patients used other types of hypnotics, and 5 were drug-naïve. Accordingly, exploratory subgroup analyses were conducted based on overall hypnotic use – comparing users (including those with incomplete medication data) versus non-users.
Comparison of eDLMO Between RLS and Insomnia Controls
All participants underwent wrist actigraphy for a period of 14 consecutive days. The mean eDLMO was later in the RLS group compared with that in the insomnia control group (10:01 PM ± 47 min vs 9:33 PM ± 49 min) (Figure 2). The mean difference corresponded to an average delay of approximately 28 min in the RLS group. Notably, the calculated Cohen’s d for this difference was 0.58, suggesting a moderate effect size, although this should be interpreted cautiously given the small sample size. Although this difference did not reach statistical significance (p = 0.069), the findings suggest a non-significant trend toward later estimated phase timing in patients with RLS relative to insomnia controls.
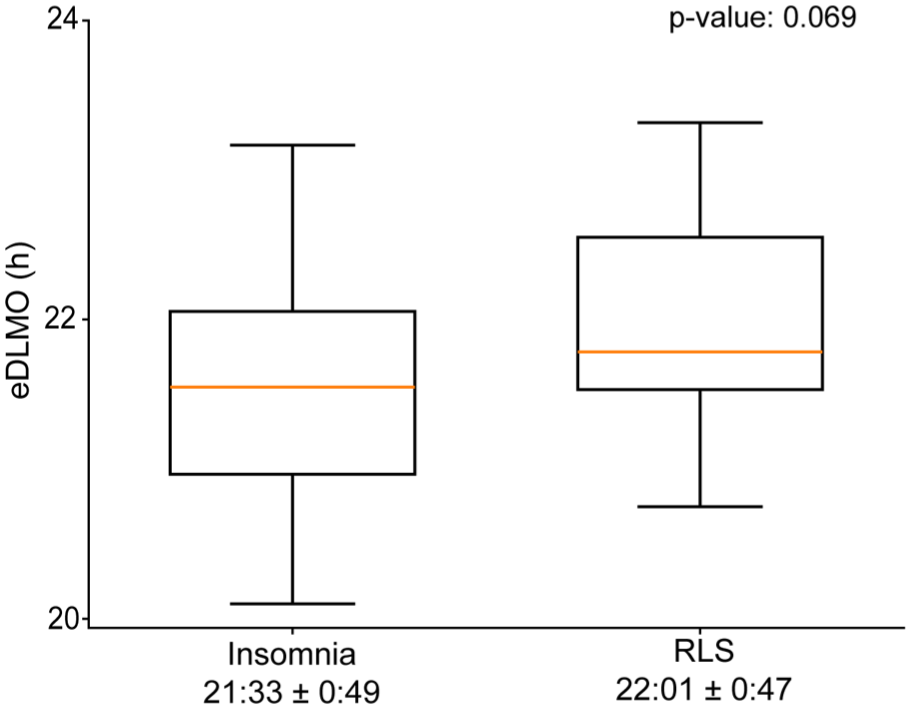
Comparison of eDLMO in both groups. The mean estimated DLMO (eDLMO) was delayed in RLS patients (n = 21; 22:01 ± 47 min) compared to insomnia controls (n = 21; 21:33 ± 49 min), with an average delay of about 28 min. Statistical comparison using an independent 2-sample t test indicated that this difference was marginally significant (p = 0.069), suggesting a tendency toward circadian phase delay in RLS patients. Time units on the axis are presented in decimal hours.
Associations Between Clinical Variables and eDLMO Within the RLS Group
To identify clinical correlates of estimated circadian phase in patients with idiopathic RLS, we examined the associations between eDLMO and a range of clinical characteristics, including both categorical and continuous variables. As summarized in Table 2, eDLMO did not significantly differ according to any of the categorical clinical variables. For instance, when stratified by onset age (cutoff: 45 years), the early-onset group (n = 8) exhibited a slightly later eDLMO (22.1 ± 0.8 h) than the late-onset group (n = 11; 21.9 ± 0.6 h), although this difference was not statistically significant (p = 0.524). No significant differences in eDLMO were observed based on the presence of a family history of RLS, painful sensory symptoms, or medication use. Likewise, no significant differences were found when comparing dopamine agonist users with non-users (including α2δ ligand users and drug-naïve individuals).
eDLMO according to categorical clinical variables in patients with idiopathic RLS.
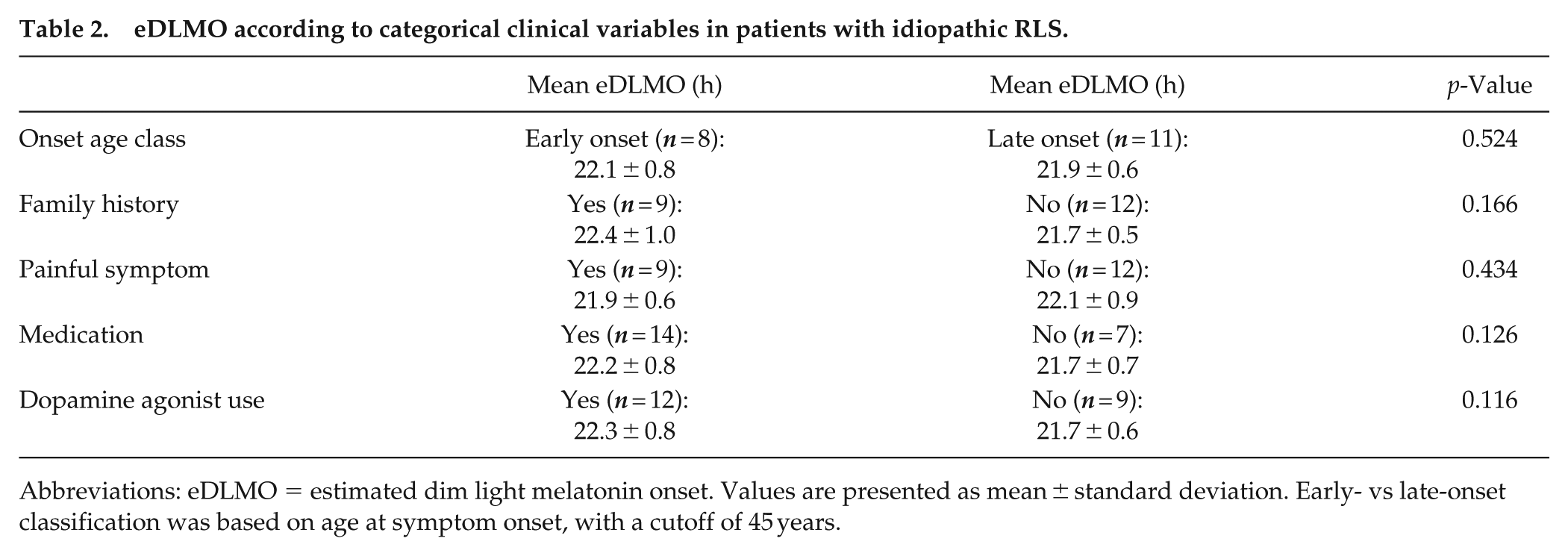
Abbreviations: eDLMO = estimated dim light melatonin onset. Values are presented as mean ± standard deviation. Early- vs late-onset classification was based on age at symptom onset, with a cutoff of 45 years.
Figure 3 presents partial correlations between continuous clinical variables and eDLMO, adjusted for age at the time of actigraphy. Among the examined variables, higher IRLS scores (r = 0.537, p = 0.021) and higher BDI scores (r = 0.587, p = 0.027) were significantly correlated with a later eDLMO, suggesting that greater RLS symptom severity and depressive symptoms may be associated with later estimated phase timing. By contrast, no significant associations were observed for age at the time of actigraphy, age at symptom onset, BMI, ISI, ESS, and iron-related measures. In addition, symptom onset time was not correlated with eDLMO (r = 0.120, p = 0.683), nor was it associated with IRLS score (r = −0.224, p = 0.421), suggesting a potential dissociation between the timing of symptom onset and both estimated phase timing and symptom severity.
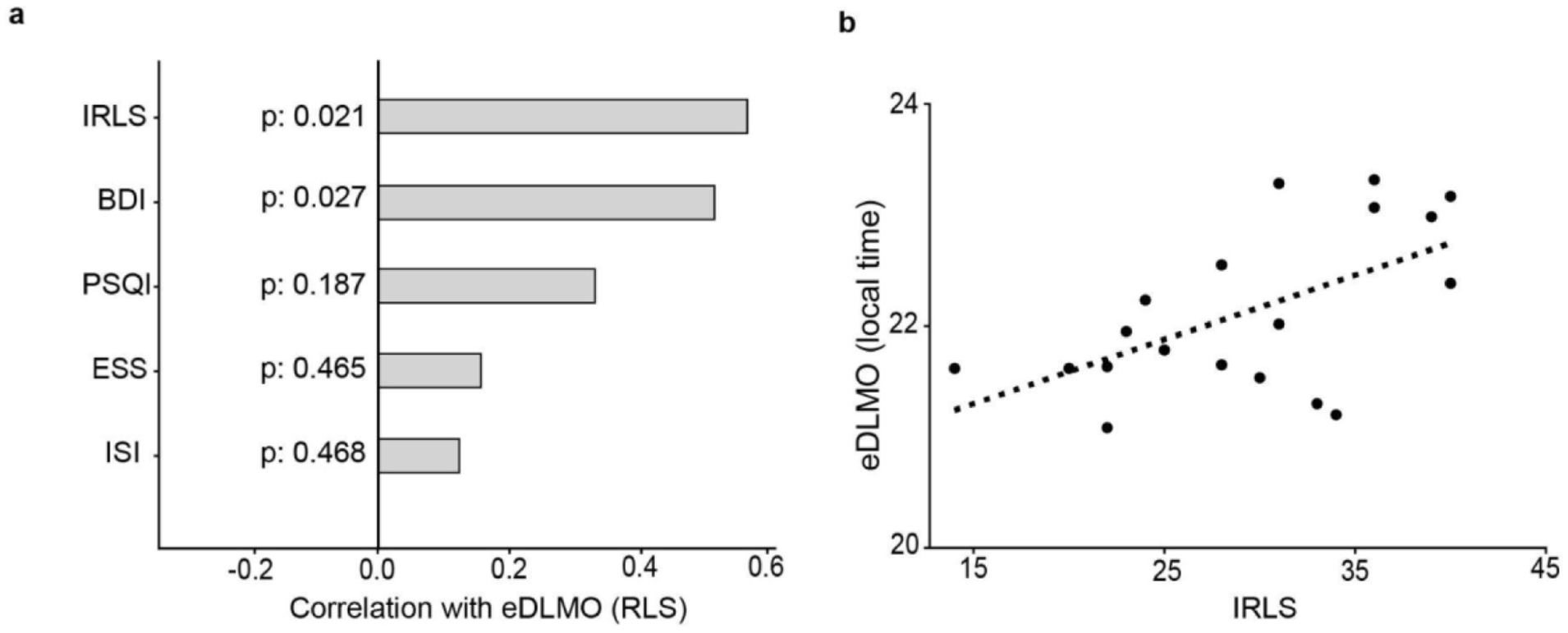
Correlations between eDLMO and clinical/sleep measures in RLS patients (n = 21). (a) Partial correlation coefficients (adjusted for age) showed significant associations of eDLMO with IRLS (p = 0.021) and BDI (p = 0.027), while PSQI, ISI, and ESS were not significantly correlated. (b) The association between IRLS scores and eDLMO (expressed in decimal hours) indicates that greater RLS symptom severity was linked to a later circadian phase.
Because both IRLS and BDI scores were associated with eDLMO in our correlation analysis, we further examined the interrelationships among subjective sleep questionnaires scales (ISI, ESS, PSQI, IRLS, and BDI) using bivariate correlations (Suppl. Table 1). Significant moderate correlations were observed among measures of sleep quality, insomnia severity, daytime sleepiness, and RLS symptom burden, with partial overlap also noted with depressive symptoms. These findings suggest that subjective sleep disturbances and mood are closely interrelated in patients with RLS.
To explore the influence of potential confounders and multicollinearity, we performed a multiple linear regression analysis with eDLMO as the dependent variable and age at the time of actigraphy, IRLS, ISI, ESS, PSQI, and BDI as independent variables (Table 3). Missing values for IRLS (n = 2) and BDI (n = 4) were handled using multiple imputation by chained equations (MICE), generating 5 imputed datasets, and pooled regression coefficients were obtained across these datasets. Multicollinearity was assessed using VIF, all of which were below 4, suggesting no substantial collinearity among predictors. Model diagnostics suggested that the assumptions of linear regression were adequately met: residual plots demonstrated approximate linearity and homoscedasticity, Q-Q plots suggested normality of residuals, and no influential outliers were identified based on leverage and Cook’s distance.
Multiple linear regression predicting eDLMO in patients with idiopathic RLS.
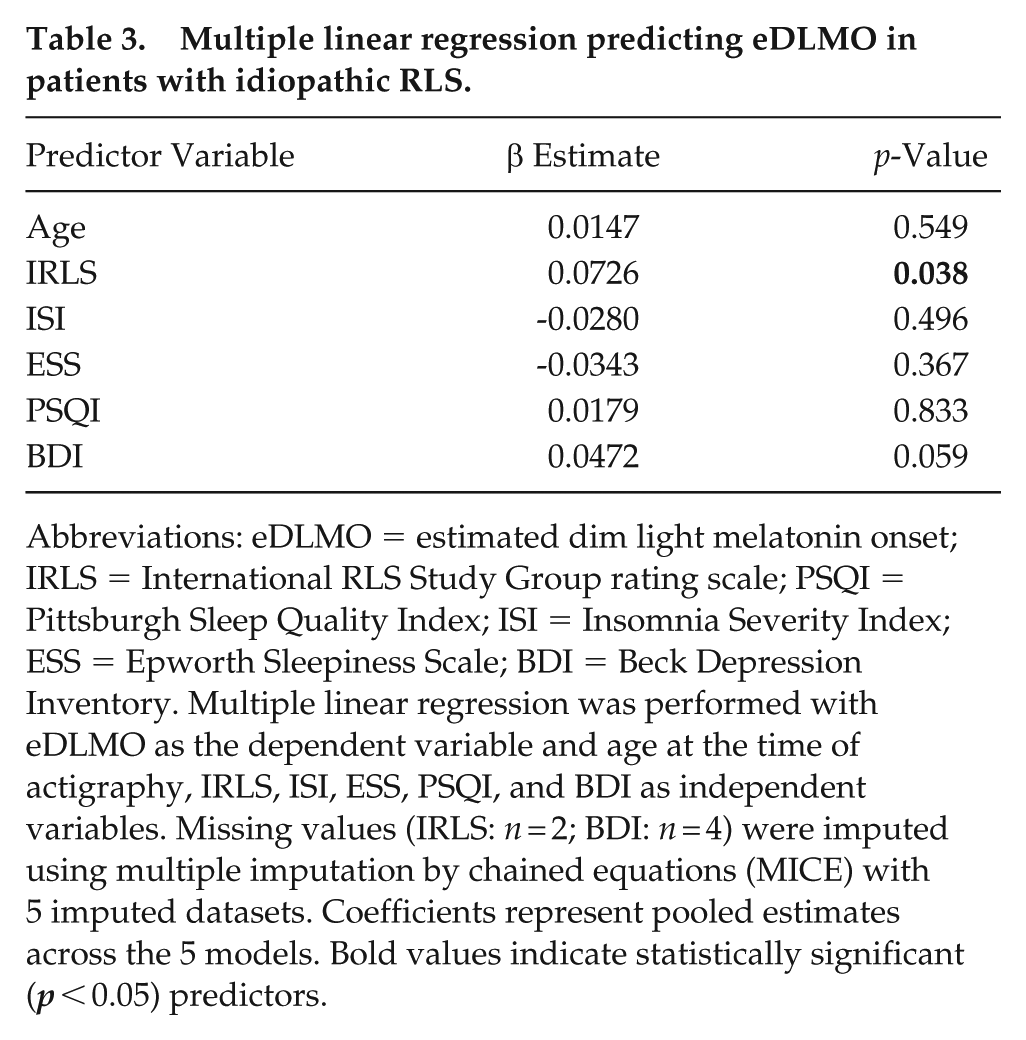
Abbreviations: eDLMO = estimated dim light melatonin onset; IRLS = International RLS Study Group rating scale; PSQI = Pittsburgh Sleep Quality Index; ISI = Insomnia Severity Index; ESS = Epworth Sleepiness Scale; BDI = Beck Depression Inventory. Multiple linear regression was performed with eDLMO as the dependent variable and age at the time of actigraphy, IRLS, ISI, ESS, PSQI, and BDI as independent variables. Missing values (IRLS: n = 2; BDI: n = 4) were imputed using multiple imputation by chained equations (MICE) with 5 imputed datasets. Coefficients represent pooled estimates across the 5 models. Bold values indicate statistically significant (p < 0.05) predictors.
In the multiple linear regression model, IRLS was associated with eDLMO in this exploratory analysis (β = 0.0726, p = 0.038). The estimated effect size suggests that higher IRLS scores may be related to later eDLMO; however, this relationship should be interpreted cautiously given the small sample size. BDI showed a marginal association (β = 0.0472, p = 0.059), while other variables did not show significant associations with eDLMO.
Associations Between Clinical Variables and eDLMO Within the Insomnia Control Group
We also examined the associations between eDLMO and clinical parameters in the insomnia control group to identify potential correlates of estimated circadian phase. Prior studies, including Morris et al. (1990), have suggested that patients with sleep-onset insomnia may exhibit later circadian phase timing. Based on this evidence, we compared eDLMO between patients with sleep-onset insomnia (n = 5) and those with either sleep-maintenance or mixed insomnia (n = 16), combining the latter two categories due to the limited number of pure sleep-maintenance cases (n = 2). As summarized in Supplementary Table 3, the average eDLMO was slightly later in the sleep-onset insomnia group (21.7 ± 0.9 h) compared with the other subtypes (21.5 ± 0.8 h), but this difference was not statistically significant (p = 0.604). Similarly, we investigated whether the use of sleep-related medications influenced eDLMO. As shown in Supplementary Table 3, patients taking medications demonstrated a numerically later eDLMO (21.7 ± 0.7 h) compared with medication-free individuals (21.1 ± 1.0 h); however, this difference also did not reach statistical significance (p = 0.189).
Furthermore, Table 4 presents the partial correlations between continuous clinical variables and eDLMO, adjusted for age at the time of actigraphy. None of the associations reached statistical significance; however, PSQI (r = 0.409, p = 0.073) and ISI (r = 0.408, p = 0.074) showed non-significant trends toward positive correlations with eDLMO, suggesting that poorer subjective sleep quality and greater insomnia severity may be associated with later estimated phase timing in the insomnia control group (Figure 4). As no partial correlations reached statistical significance, additional multivariate regression analyses were not conducted.
Partial correlation between clinical variables and eDLMO in the insomnia control group.
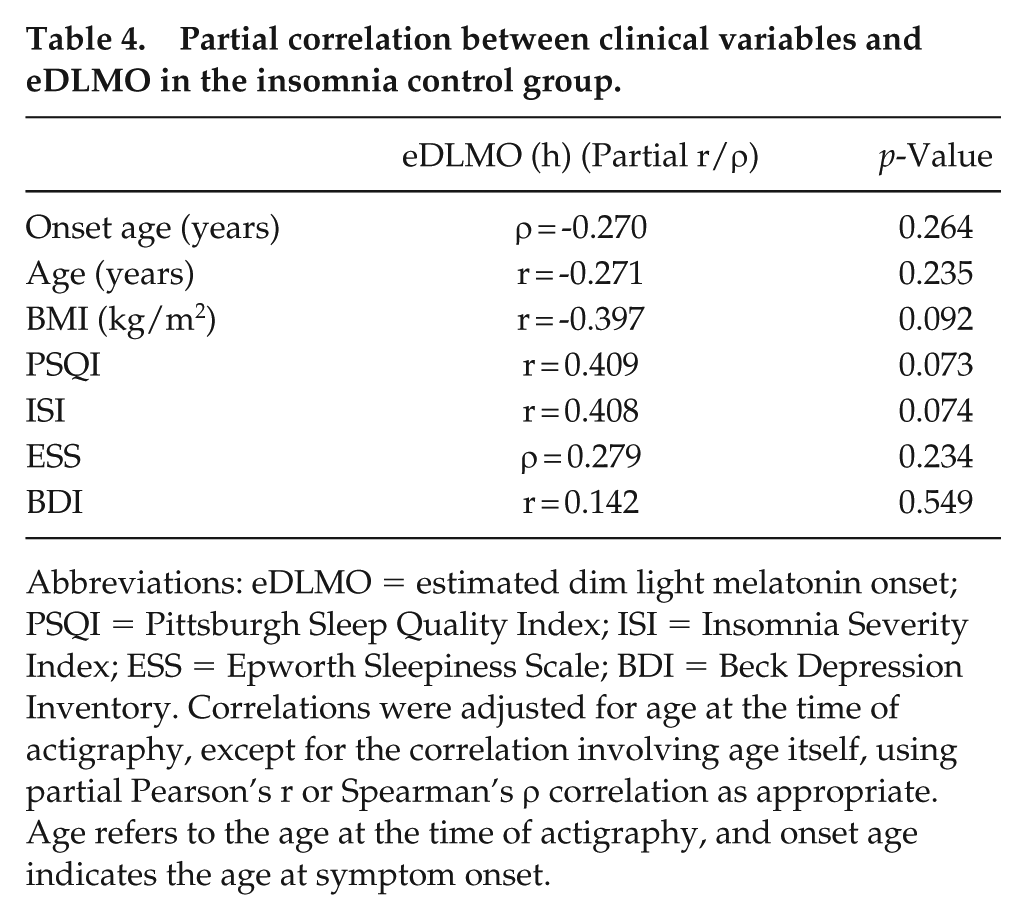
Abbreviations: eDLMO = estimated dim light melatonin onset; PSQI = Pittsburgh Sleep Quality Index; ISI = Insomnia Severity Index; ESS = Epworth Sleepiness Scale; BDI = Beck Depression Inventory. Correlations were adjusted for age at the time of actigraphy, except for the correlation involving age itself, using partial Pearson’s r or Spearman’s ρ correlation as appropriate. Age refers to the age at the time of actigraphy, and onset age indicates the age at symptom onset.
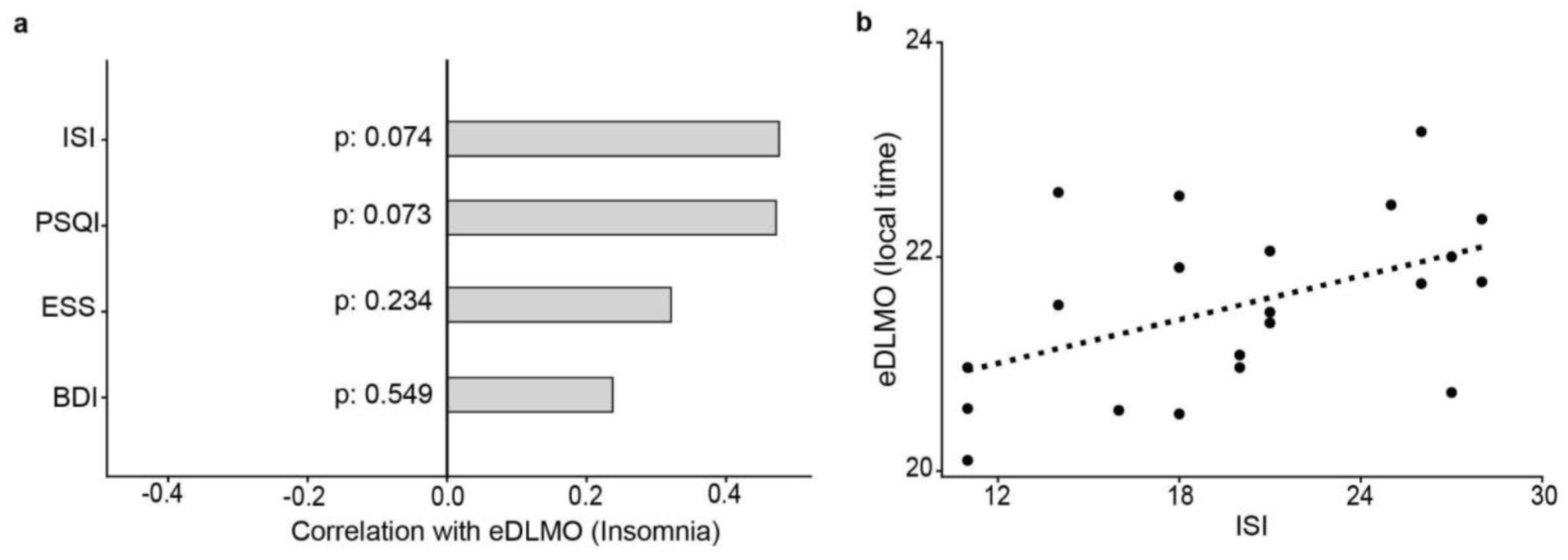
Correlations between eDLMO and clinical/sleep measures in insomnia controls (n = 21). (a) Partial correlation coefficients (adjusted for age) showed marginal positive associations of eDLMO with ISI (p = 0.074) and PSQI (p = 0.073). No significant correlations were observed for ESS and BDI. (b) The association between ISI and eDLMO (expressed in decimal hours) suggests that greater insomnia severity may be linked to a trend toward a later circadian phase, although this did not reach statistical significance.
Discussion
Our study showed that idiopathic RLS patients without augmentation tended to exhibit a later eDLMO compared with chronic insomnia controls, although this difference did not reach statistical significance, suggesting a possible delay in estimated circadian phase based on a model-derived proxy measure. Within the RLS group, greater disease severity was associated with later eDLMO in this exploratory analysis. Notably, the timing of symptom onset did not correlate significantly with eDLMO, nor was it associated with IRLS scores. By examining disorder-specific associations between eDLMO and clinical characteristics, we also found that the patterns of association differed between RLS and chronic insomnia controls, although these findings require confirmation in larger, well-characterized cohorts.
In this study, we estimated DLMO from actigraphy rather than direct measurement. DLMO is considered the gold standard for assessing circadian phase; however, its determination is burdensome for participants and, being limited to a single day, cannot capture circadian rhythms that require multi-day assessment. To address this limitation, computational methods have been developed to estimate circadian phase indirectly from behavioral and environmental data (Forger et al., 1999; Reiter et al., 2020); among these, a mathematical model-based method is known to be the most accurate method (Stone et al., 2020). This modeling approach has been successfully applied to predict alertness in shift workers (Knock et al., 2021; Song et al., 2023) and mood episodes in mood disorder patients (Lim et al., 2024; Song et al., 2024), showing that model-derived circadian phase estimates can serve as a practical alternative to direct DLMO measurement and as reliable markers of clinically relevant outcomes (Cheng et al., 2021; Postnova et al., 2014; Woelders et al., 2017). Therefore, this modeling framework provides an ideal method to investigate whether patients with RLS exhibit a delayed circadian phase compared with insomnia controls, a question that cannot be feasibly addressed using direct DLMO measurement.
However, the current modeling framework relies on fixed parameter values across individuals, implicitly assuming that key circadian and sleep-wake characteristics, such as intrinsic circadian period and light sensitivity, are the same across individuals. This assumption may not hold in clinical populations such as RLS patients, where these characteristics can differ systematically from those of the healthy individuals due to underlying physiological differences. Incorporating subject-specific parameterization into circadian models therefore represents an important direction for future research.
The eDLMO time was positively associated with IRLS scores, suggesting that greater symptom severity may be related to later estimated phase timing. Two non-exclusive pathways may underlie this association, although correlation alone cannot establish causality. First, worsening RLS symptoms may contribute to delayed sleep-wake timing. Sleep disturbance in RLS is frequently characterized by difficulty initiating sleep (Winkelman et al., 2009), as symptoms typically emerge or intensify in the evening hours. Chronic difficulty in falling asleep may gradually delay sleep-wake timing, thereby influencing behavioral phase patterns. Anecdotally, RLS patients often describe that their best sleep occurs in the mid-morning hours, while they may also, by necessity, walk at night to relieve RLS symptoms, thereby delaying sleep. Alternatively, later phase timing itself may be associated with more severe RLS symptoms. In a population-based study of Korean adolescents, RLS was associated with evening chronotype, shorter sleep duration, and higher rates of depression (Kim et al., 2016). Genome-wide causal inference analyses further support potential bidirectional relationships between RLS liability and sleep disturbance, with morning chronotype showing a protective association with RLS (Schormair et al., 2024). Together, these findings suggest a possible interaction between behavioral sleep-wake patterns and RLS symptoms, although the underlying mechanisms remain to be clarified.
Physiological studies also implicate a potential role of endogenous circadian drivers. Michaud et al. demonstrated that RLS symptom intensity peaks approximately 2 h after the melatonin acrophase, suggesting that the evening rise in melatonin may be temporally associated with symptom worsening (Michaud et al., 2004). Indeed, exogenous melatonin has been reported to exacerbate RLS symptoms (Whittom et al., 2010), possibly related to the structural similarity between melatonin and serotonin. Similarly, forced desynchrony protocols have shown that periodic limb movements in sleep (PLMS) exhibit a circadian pattern, with maximal expression in the late evening/early night (Duffy et al., 2011). However, our data did not show a correlation between symptom onset time and eDLMO, which does not support a clear temporal coupling between estimated phase timing and reported symptom onset in this cohort.
At the molecular level, converging evidence suggests disrupted circadian regulation in RLS. Variants in CLOCK and other circadian genes have been associated with altered susceptibility to RLS. Transcriptomic profiling has revealed downregulation of core circadian genes, coupled with upregulation of ferroptosis and dopaminergic pathways, raising the possibility that circadian disruption may promote oxidative stress and neuronal vulnerability (Mogavero et al., 2025). Circadian variation of iron and dopaminergic measures in Cerebrospinal fluid (CSF) has also been reported to parallel symptom severity, with nadirs in brain iron and dopamine occurring at night (Mogavero et al., 2025).
Overall, our findings suggest a potential relationship between estimated circadian phase and RLS symptoms, although the directionality of this association remains unclear. Later phase timing may be associated with greater symptom severity through neurochemical and molecular mechanisms, while symptom-related sleep-initiation difficulties may contribute to delayed sleep-wake patterns. Longitudinal studies with repeated circadian phase assessments, integrated with genetic, transcriptomic, and neurochemical biomarkers, are needed to disentangle these pathways. Importantly, approaches targeting sleep-wake timing, such as timed light exposure, melatonin modulation, or chronotherapeutic adjustment of dopaminergic therapy may hold promise as novel therapeutic avenues for RLS.
In our RLS cohort, the timing of symptom onset did not show meaningful associations with either eDLMO or IRLS scores, suggesting that self-reported onset time may be an imprecise surrogate for underlying circadian or behavioral phase timing. By contrast, eDLMO was associated with disease severity in this exploratory analysis, although it represents a model-based estimate rather than a direct physiological measure of circadian phase. Accordingly, objective circadian markers such as eDLMO may provide complementary information for characterizing phase-related patterns in idiopathic RLS, and their potential clinical utility warrants further investigation.
Augmentation is treatment-emergent worsening of RLS, characterized by an earlier onset of symptoms, increased intensity, or spread to previously unaffected body regions compared with the pre-treatment state. It is considered a serious and potentially disabling complication, and patients frequently report symptoms that exceed those experienced before starting therapy (Wijemanne and Jankovic, 2015). Prior studies have shown that RLS patients who develop augmentation may exhibit a relative advance in circadian phase timing, a finding that appears to contrast with our observation of a delayed eDLMO in idiopathic RLS. In a pivotal study by Garcia-Borreguero et al., patients who later developed augmentation displayed a pronounced advance in DLMO following levodopa (L-DOPA) administration, whereas no such shift was observed in those who remained augmentation-free (Garcia-Borreguero et al., 2004). In our augmentation-free idiopathic RLS cohort, eDLMO was associated with later phase timing and greater symptom severity, raising the possibility that circadian phase delay is a characteristic feature of non-augmented idiopathic RLS.
In the RLS group of our study, higher depressive symptom scores on the BDI were associated with a later eDLMO (r = 0.587, p = 0.027), with a similar trend observed after adjusting for covariates (β = 0.0472, p = 0.059). This suggests that depressive symptom burden may be associated with later estimated phase timing in RLS. Prior studies have consistently reported elevated depression prevalence in RLS (Kim et al., 2016; Sevim et al., 2004), and longitudinal evidence indicates that depressive symptoms can precede the onset of leg discomfort in RLS patients (Gorman et al., 1965), suggesting that depression is not invariably a secondary consequence of chronic sensory symptoms. Our findings extend this literature by suggesting a potential association between depressive symptoms and estimated phase timing in RLS, as measured by a physiological marker rather than secondary to RLS symptoms and its impact on sleep. This raises the possibility that mood disturbances in RLS may be related to alterations in phase-related patterns, rather than being solely secondary to RLS symptoms and their impact on sleep. From a clinical perspective, these results underscore the importance of considering both psychiatric symptoms and sleep-wake timing in the comprehensive assessment of RLS.
In the insomnia control group of our study, eDLMO showed only marginal associations with ISI (insomnia severity) and PSQI (perceived sleep quality), and these did not reach statistical significance. The direction of these trends, however, was generally in line with prior findings suggesting that greater insomnia severity may be associated with later phase timing, as assessed by actigraphy or DLMO (Dermanowski et al., 2023; Roh et al., 2022). Given that our insomnia control group included only 21 participants, the lack of statistical significance may in part reflect limited statistical power rather than the absence of a true association. By contrast, no significant relationship was observed between BDI scores and eDLMO, a finding that is consistent with previous studies reporting no clear linear association between DLMO and depression severity. For example, the correlation between DLMO timing and depressive symptom severity in patients with major depressive disorder was not significant (Swanson et al., 2017), and subjective chronotype measures, such as eveningness preference, rather than physiological markers like DLMO, are more consistently associated with depression in insomnia (Comas et al., 2023).
Collectively, our results suggest that later estimated phase timing in RLS may be associated with symptom severity and mood-related measures, whereas in chronic insomnia, it may be more closely related to subjective perceptions of sleep disturbance and quality. These divergent patterns may indicate potential differences in underlying mechanisms – such as dopaminergic-circadian interactions in RLS versus hyperarousal-related pathways in insomnia – and have implications for personalized therapeutic approaches.
This study has several limitations. First, the sample size was modest, which limits statistical power and the precision of effect estimates; replication in larger, multi-center cohorts is warranted. Second, our control group comprised patients with chronic insomnia rather than healthy individuals. Although we found no significant eDLMO differences across insomnia subtypes in this sample, prior work has reported delayed circadian rhythm in sleep-onset insomnia (Morris et al., 1990); therefore, a comparison with rigorously screened healthy controls will be important to delineate disorder-specific phase characteristics. Third, the cross-sectional, correlational design precludes causal inference regarding the relationship between eDLMO and IRLS severity. Therefore, longitudinal observational study is required to clarify the causal relationship between circadian phase and RLS severity.
Another limitation lies on the use of eDLMO. While eDLMO provides a practical and scalable alternative to direct melatonin sampling, it remains an indirect estimate and cannot fully replace laboratory-based DLMO measurement. Because eDLMO is derived from sleep-wake timing and light exposure, it is not a purely endogenous circadian marker, and in RLS patients, symptom-driven evening activity may prolong nocturnal light exposure and thereby contribute to apparent phase delays. This concern is valid and has been raised in prior work (Stone et al., 2020); however, our study deliberately aimed to capture phase-related patterns as they occur in naturalistic settings rather than under idealized laboratory conditions. From this perspective, the influence of behavioral and environmental factors does not simply represent confounding, but rather clinically relevant features, as circadian misalignment in RLS often emerges from the interplay between endogenous physiology and symptom-related behaviors. Importantly, we applied the same computational approach to both RLS and insomnia controls. Despite comparable analytical conditions, associations with symptom severity were observed only in the RLS group, suggesting a potential disorder-specific relationship between symptom burden and estimated phase timing. Nonetheless, future studies employing direct melatonin-based assessments under controlled conditions will be required to disentangle endogenous circadian shifts from secondary behavioral effects and to validate the present findings more robustly.
A further limitation of this study is the simplified representation of light input in the circadian model. Specifically, wake periods outside the defined sleep interval were assigned a fixed light level of 250 lux, whereas sleep periods were assigned 0 lux. Although this approach provides a pragmatic approximation of light-dark exposure in the absence of reliable continuous light measurements, it may not fully reflect real-world nocturnal light exposure, particularly in patients with RLS or insomnia, for whom the sleep-wake state may not correspond directly to the actual light environment. Future studies incorporating objectively measured or more physiologically realistic nocturnal light exposure assumptions would further improve the validity and interpretability of the model-based circadian estimates.
In conclusion, this exploratory real-world pilot study suggests a possible trend toward later estimated circadian phase timing in idiopathic RLS without augmentation, with greater delay potentially associated with greater symptom severity. Because the primary between-group difference did not reach statistical significance, these findings should be interpreted as preliminary and hypothesis-generating. While eDLMO may offer a useful model-based estimate of circadian phase timing beyond self-reported symptom onset, larger and more clinically differentiated studies are needed to determine whether circadian phase alteration is a reproducible and clinically meaningful feature of RLS.
Supplemental Material
sj-docx-1-jbr-10.1177_07487304261456963 – Supplemental material for Circadian Rhythm in Restless Legs Syndrome and Its Association With Symptom Severity: An Actigraphy-Based Study
Supplemental material, sj-docx-1-jbr-10.1177_07487304261456963 for Circadian Rhythm in Restless Legs Syndrome and Its Association With Symptom Severity: An Actigraphy-Based Study by Se Young Bang, Aqsa Awan, Dongju Lim, Sungeun Hwang, Brian B Koo, Jae Kyoung Kim and Ki-Young Jung in Journal of Biological Rhythms
Supplemental Material
sj-docx-2-jbr-10.1177_07487304261456963 – Supplemental material for Circadian Rhythm in Restless Legs Syndrome and Its Association With Symptom Severity: An Actigraphy-Based Study
Supplemental material, sj-docx-2-jbr-10.1177_07487304261456963 for Circadian Rhythm in Restless Legs Syndrome and Its Association With Symptom Severity: An Actigraphy-Based Study by Se Young Bang, Aqsa Awan, Dongju Lim, Sungeun Hwang, Brian B Koo, Jae Kyoung Kim and Ki-Young Jung in Journal of Biological Rhythms
Footnotes
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF) (RS-2022-NR068758, J.K.K.), the Institute for Basic Science (grant no. IBS-R029C3, J.K.K.), and the Samsung Science and Technology Foundation (grant no. SSTF-BA1902-01, J.K.K.).
Conflict of Interest Statement
Jae Kyoung Kim is a member of the Editorial Board of the Journal of Biological Rhythms. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Data Availability Statement
Access to the data underlying this study may be provided by the corresponding author upon reasonable inquiry.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.