
Abstract
Fat grafting has become a popular procedure due to its wide range of clinical applications. Several fat grafting techniques have been described to increase the survival rate of the grafted fat. This article presents carbon dioxide (CO2) pneumodissection to improve the biological microenvironment of the recipient site. A total of 40 patients were treated with CO2 pneumodissection for aesthetic and reconstructive indications. The known effects of carboxitherapy such as vasodilation, enhanced Bohr effect, and neoangiogenesis are applied to facilitate the grafting procedure and in the search for higher rate of graft uptake. Tissue pneumodissection has demonstrated reduced pain due to the fat injection process, and reduces the sedation requirements and local anesthesia infiltration requirements.
Keywords
Introduction
The introduction of grafts and/or fillers within the subcutaneous tissues implies the creation of planes of dissection within these tissues. However, this maneuver is not without some degree of trauma to the cellular structure and the neurovascular structure of the hypodermis.
The resistance of the instrument against cellular tissues produces pain by transecting nerve endings or compression of the pressure sensors and/or direct distension of these fragile receptors within the skin.
Until now, the only possible solution to reduce these effects was the application of local anesthesia of different modalities, that is, blockades, infiltration, or tumescent anesthesia. This implies the introduction of a set volume of liquid and chemicals, which modifies the tissue composition both physically and chemically. This alteration to the bio-physical integrity of the receptor area and the direct limitation of surrounding tissue elasticity and expandability creates a suboptimal graft-recipient environment. We propose a new innovation of utilizing pneumodissection with carbon dioxide (CO2) gas to expand and dissect tissue planes while preserving delicate microcirculation at the site and decreasing pain to the patient prior to augmentation with adipocytes and stroma.
Physiological Effects of CO2
Stimulation in the Blood Circulation
CO2 influences the microcirculation within the connective tissue, promotes vasodilation, and increases the venous and lymphatic drainage.1-3
The persistence of clinical improvement in the treated area after carboxitherapy is explained by the neoangiogenic development, due to the hypercapnia-induced secretion of angiogenic factors, such as vascular endothelial growth factor and fibroblast growth factor. 4
Bohr Effect
There is a consensus about a significant increase in oxygen (O2) concentration after subcutaneous infusion of CO2 demonstrating an increase in the partial pressure of O2. 5 A decrease in affinity of hemoglobin for O2 in the presence of CO2 gas leads to increased O2 delivery to the cells, which would boost the metabolism of tissues (potentiation of the Bohr effect). 6
Role of CO2 in Connective Tissue
Carboxitherapy produces a direct “mechanical trauma” by the insertion of the cannula and the CO2 insufflation gas insufflating between tissue planes. This pneumodissection produces an inflammatory process and the consequent migration and proliferation of fibroblasts to the region of insufflations. 7 Collagen is induced with the activation of other extracellular matrix proteins such as fibronectin and glycoprotein.
Histological studies (of the tissues treated with carboxitherapy) have shown an increase in the dermal thickness, with an increased stimulus of neo-collagenases. 8 There is total preservation of the connective tissue layers, including its neurovascular structures.
CO2 Gas as a Pneumodissector of Tissues: Carboxitherapy
Due to CO2’s high degree of diffusion, this gas is rapidly absorbed and eliminated, leaving only the vasodilator effect in the tissues, without the increased risk of a fatal air embolism. 9
The subcutaneous infiltration of CO2 began to be used for aesthetic purposes in the 1970s in France, to treat cellulitis and localized areas of subcutaneous adiposities. Brandi et al 10 showed reductions in the maximum circumference of abdomen, thigh, and knee regions with the transcutaneous administration of CO2 with an improved skin irregularity after repeated sessions of carboxitherapy.
Theory for Use of Carboxitherapy for Fat Graft
The ideal conditions for adipose (fat) grafting within tissue include (1) ease of dissection of tissue planes with the advancement of the injection cannula, (2) the ability to perform serial injections of fat to maximize contact with the surrounding tissues, (3) good vascularization and oxygenation of recipient site, (4) minimal trauma to reduce the risk of bruising, (5) minimal vasoconstriction, (6) absence of toxic chemicals and by-products in the recipient tissue, and (7) good elasticity and compliance of the recipient area.
We believe that the use of CO2 gas as a pneumodissector of the tissue planes may be one way to achieve these ideal conditions in the host tissue.
The resistance of the tissues to the advancement of a needle or cannula is predetermined by the density of cell structures and fibrotic characteristics of the tissue area. Some of the issues of pain during the introduction of fluids and grafts into tissues are due to the compression of pressure receptors (baroreceptors) and by the stretching of the nerves endings by direct mechanical pressure from the advancing cannula or needle. Also, the pH of the solutions being injected produces pain and burning.
The slow insufflation of the CO2 in its gaseous state, by percutaneous injection, produces tissue plane dissection that subsequently decreases the tissue’s overall resistance while increasing its 3-dimensional space and preserving the neurovascular structures by pneumodissecting these structures away with the advancement of the needle/cannula.
Clinical Experience
In carboxitherapy, the pneumodissection flow and the total volume of gas infiltrated in the subcutaneous are controlled with CARBOTECH F650 from Axt Medical Systems® (Buenos Aires, Argentina), a device with complete control over the speed and volume of CO2 gas infiltrated (Figure 1).
Pneumodissector console.
CARBOTECH F650 is connected to the pure CO2 gas, which is kept within an iron tank and regulated via pressure regulators. The CO2 is injected with a dose-controlled speed of flow through a disposable tubing with 25G needle (attached to luer lock). This needle is inserted directly under the skin within the designated site.
The flow of CO2 is fixed at 80 mL per minute. Insufflation volume is between 40 and 1000 mL per area depending on the procedure to be carried out and the anatomical site (Figure 2).
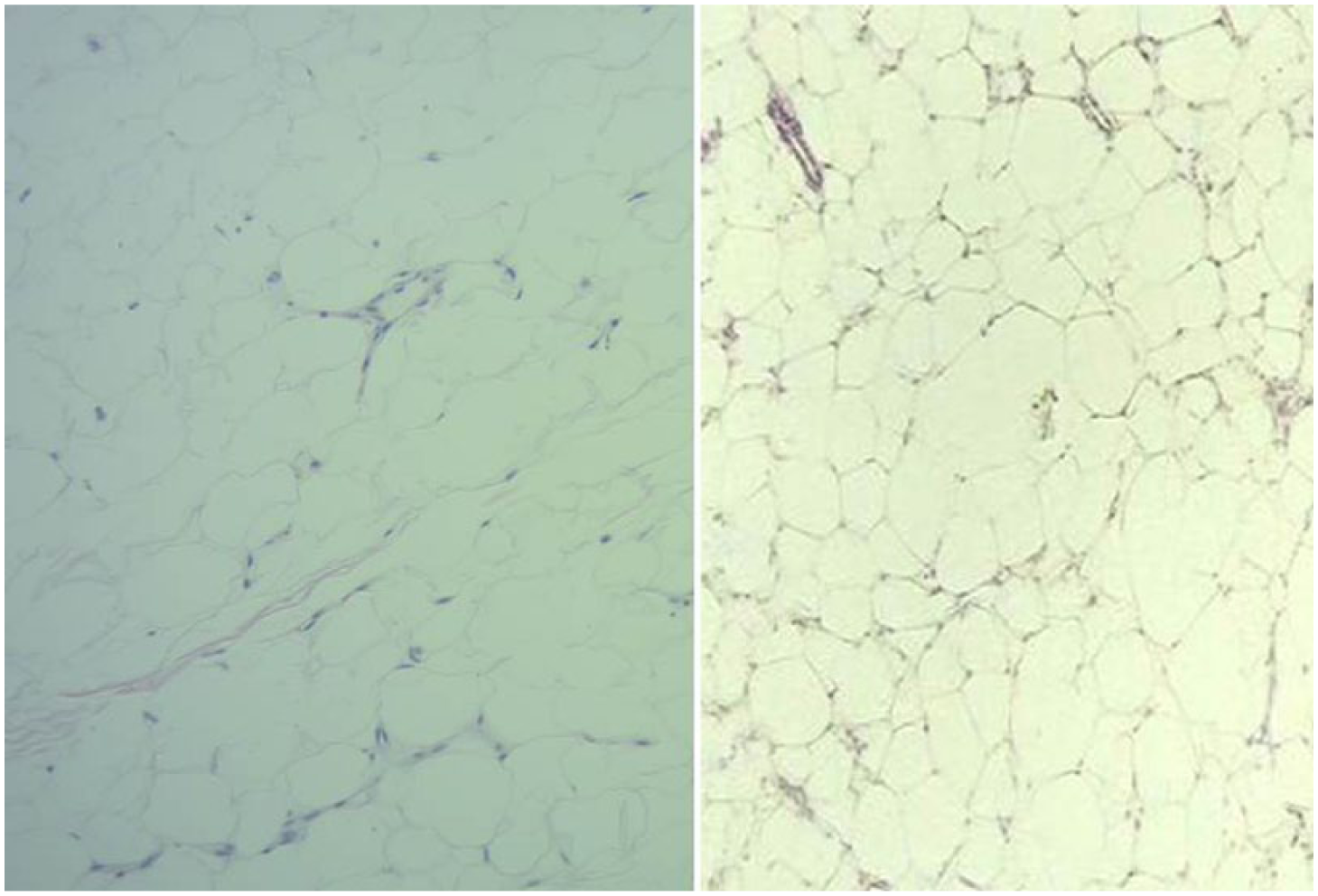
Histology shows the microstructure of the subcutaneous tissue expanding with the preservation of neurovascular structure.
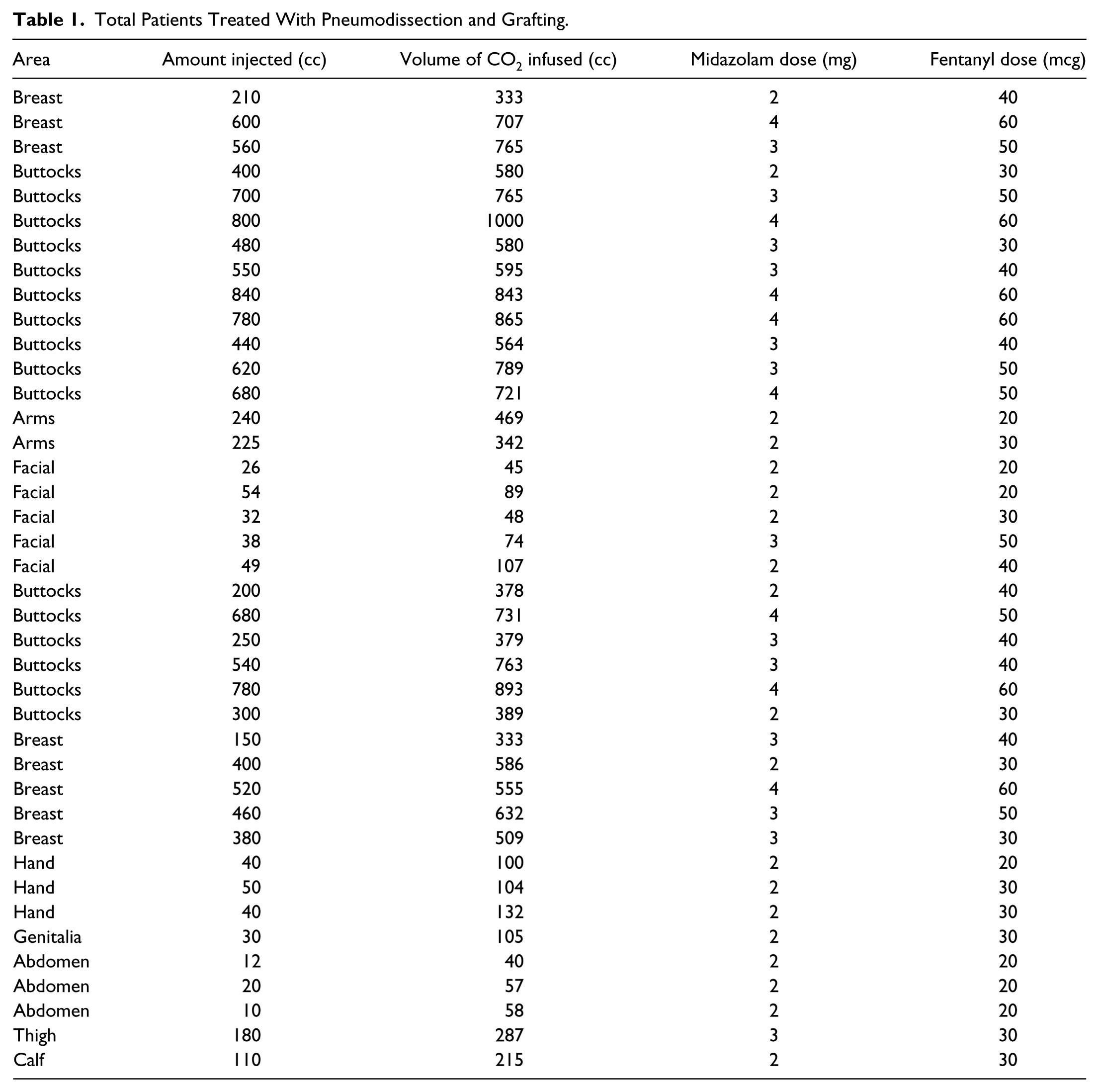
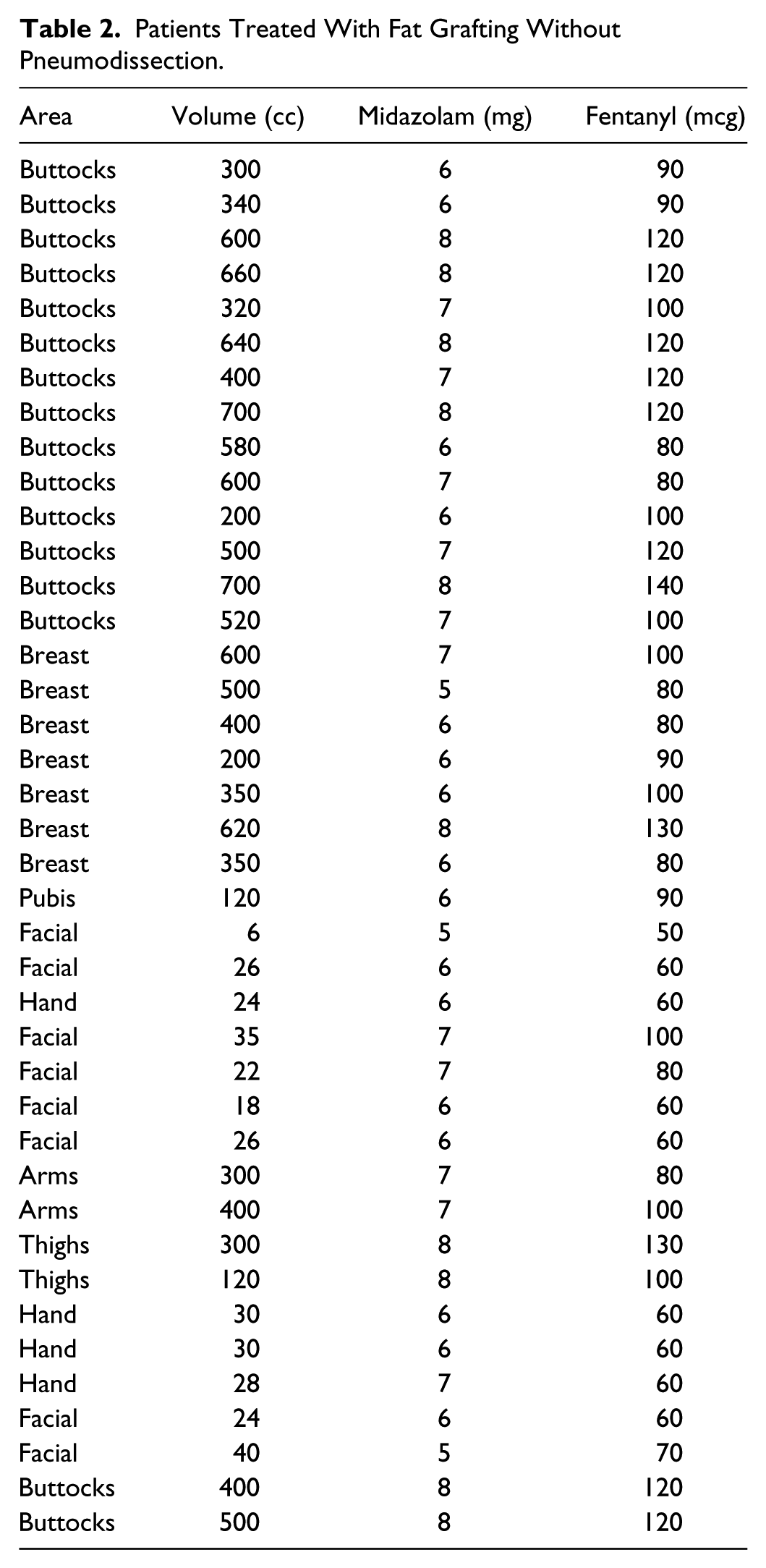
During the past 12 months, we have used the pneumodissection technique prior to the grafting procedure in 40 patients with mild sedation (Table 1). Areas of both the body (abdomen, buttocks, arms, breast, genitalia, and legs) and face have been successfully pneumodissected prior to fat grafting (Figures 3-24). Pneumodissecting the tissue planes facilitates the introduction and advancement of the infiltrating cannula, allowing a higher volume and improved distribution of grafts (adipocytes). The reduced resistance of normal tissues decreases the intraoperative discomfort of the patient. The sedation requirements were compared with patients with fat grafting without pneumodissection (Table 2). Midazolam mean dose in patients with pneumodissection was 2.72 mg (SD = 0.78) whereas in patients without pneumodissection, it was 6.7 mg (SD = 0.94). Fentanyl mean dose in patients with pneumodissection was 38.5 mcg (SD = 13.38) whereas in patients without pneumodissection, it was 92 mcg (SD = 24.52).
Total Patients Treated With Pneumodissection and Grafting.

Patient with mastectomy and radiotherapy, skin adherent to thoracic wall (before pneumodissection and fat grafting).

Patient with mastectomy and radiotherapy, skin adherent to thoracic wall (after 3 months of pneumodissection and fat grafting).

Intraoperative view of fat transferred into the depressed scar in opportunity of implant placement in the mastectomy patient.

Patient after breast silicone implant extrusion, skin adherent to thoracic wall (before neumodissection and grafting).

Patient after breast silicone implant extrusion (after 3 months of first session of pneumodissection and fat grafting).

Patient after breast silicone implant extrusion (after 3 months of second session of pneumodissection and fat grafting).
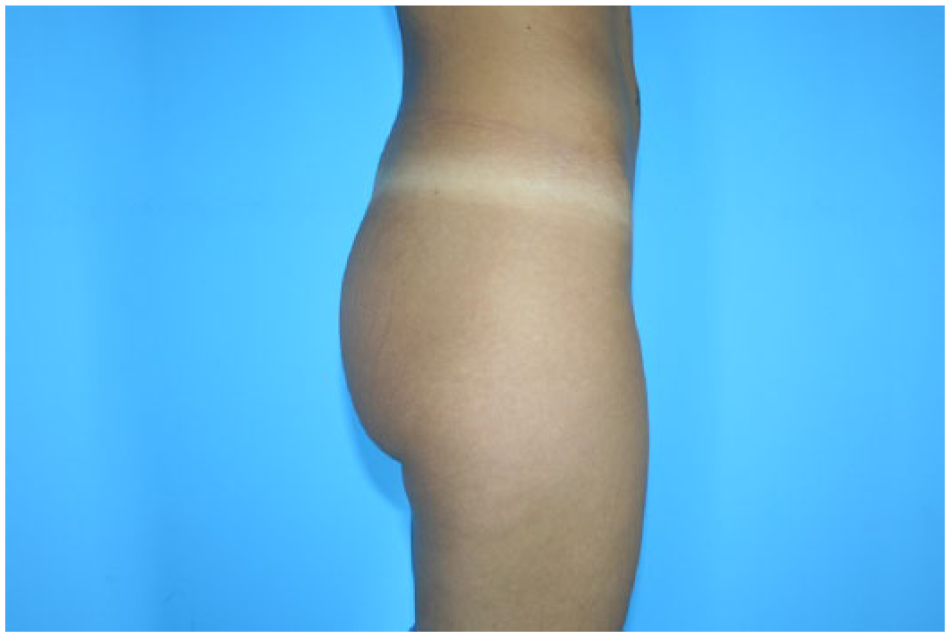
Patient with gluteal hypotrophy (preoperative).
Patient with gluteal hypotrophy (after 5 months of pneumodissection and fat grafting).
Patient with gluteal hypotrophy (preoperative).

Patient with gluteal hypotrophy (after 2 months of pneumodissection and fat grafting).

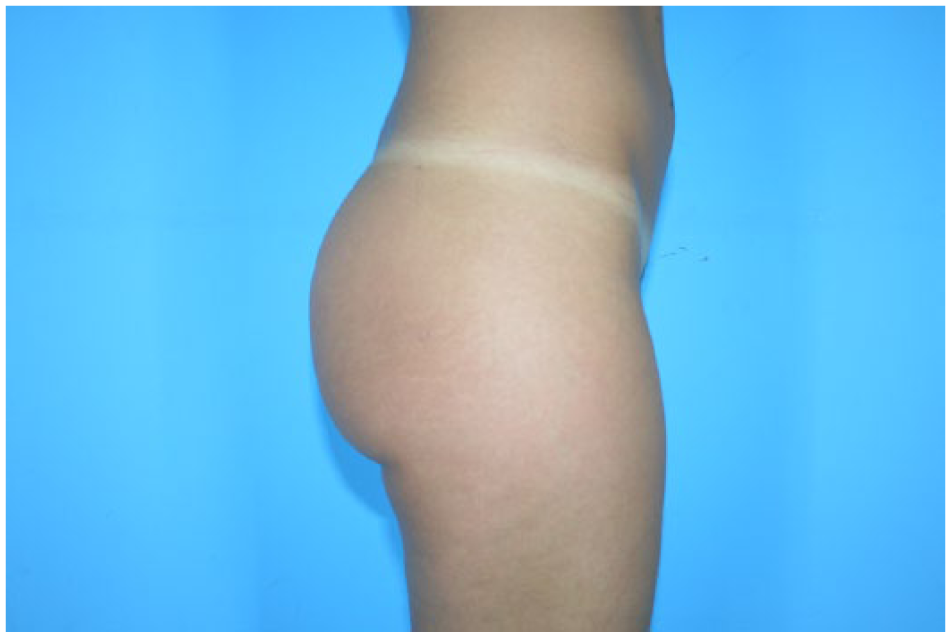
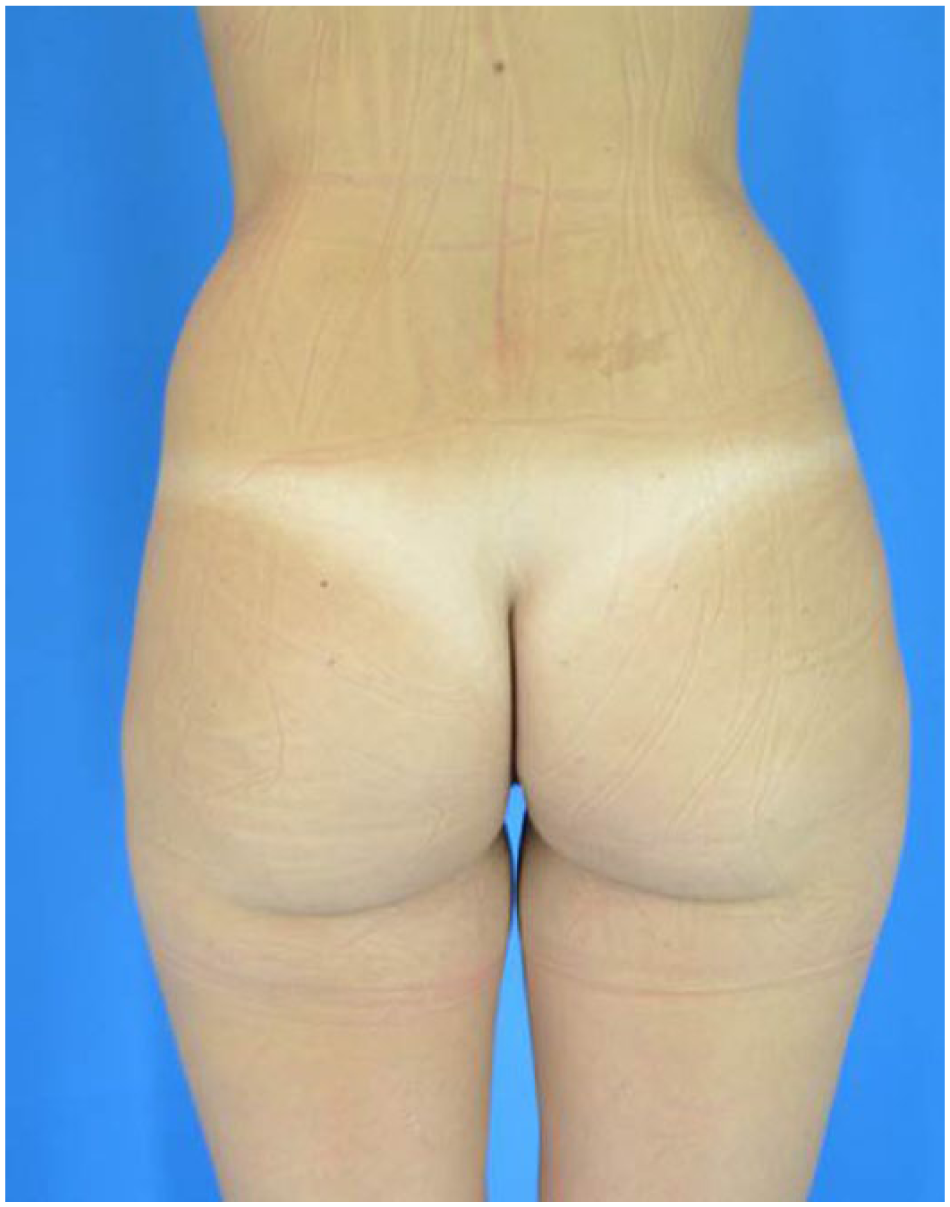
Patient with gluteal hypotrophy (preoperative).

Patient with gluteal hypotrophy (after 2 months of pneumodissection and fat grafting).

Patient with sex reassignment surgery (1 year postoperative).

Patient with sex reassignment surgery (3 months after pneumodissection and fat grafting).
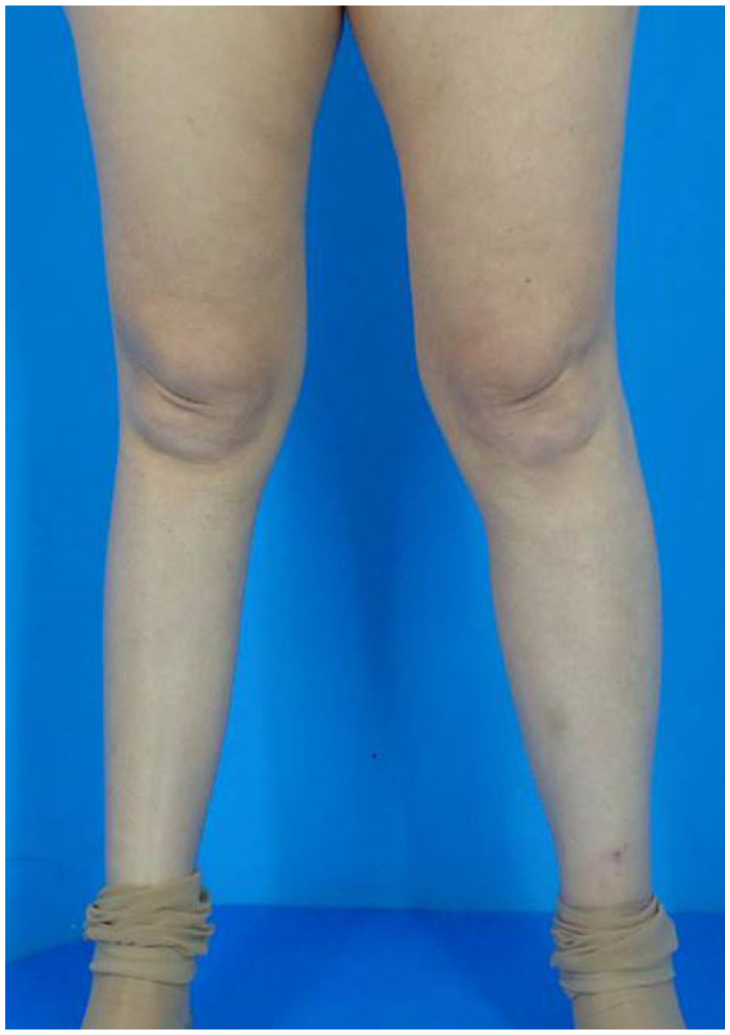
Patient with poliomyelitis sequela in the right leg.

Patient with poliomyelitis sequela in the right leg (after 3 months of pneumodissection and fat grafting).

Patient with gluteal hypotrophy (preoperative).
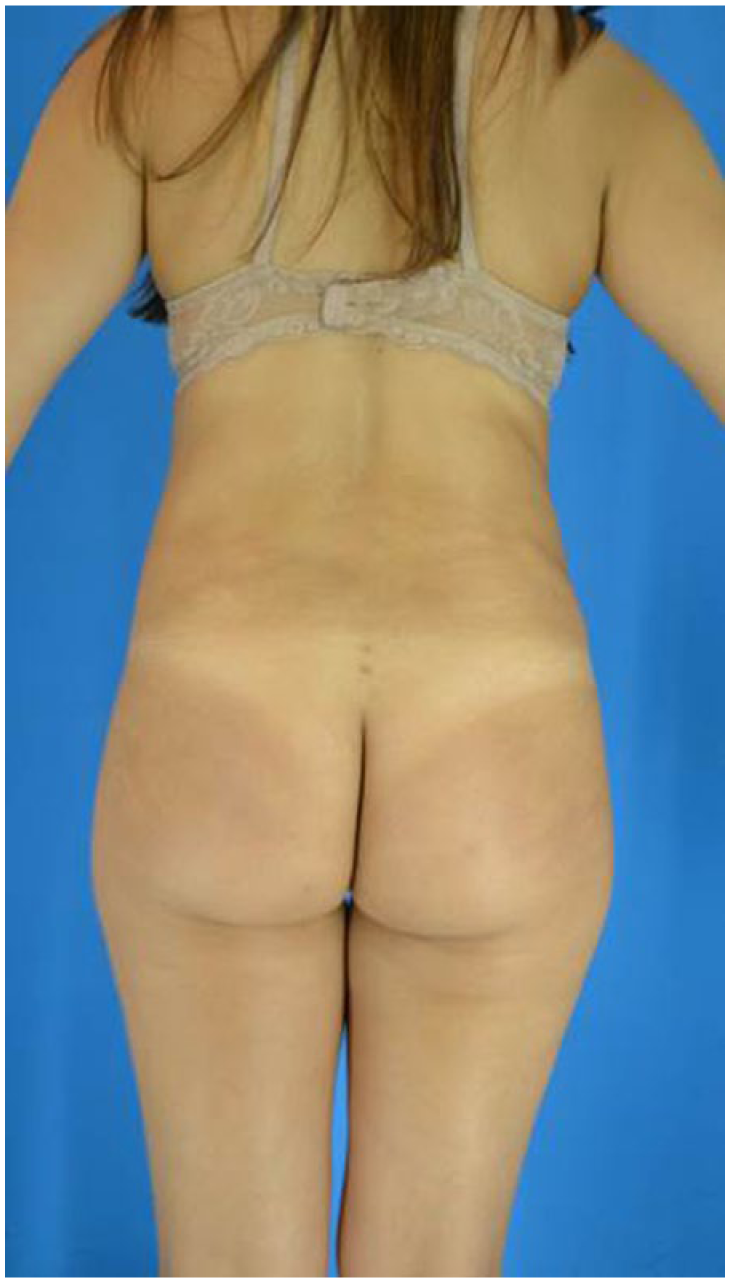
Patient with gluteal hypotrophy (after 3 months of pneumodissection and fat grafting).

Patient with gluteal hypotrophy (preoperative).

Patient with gluteal hypotrophy (after 3 months of pneumodissection and fat grafting).
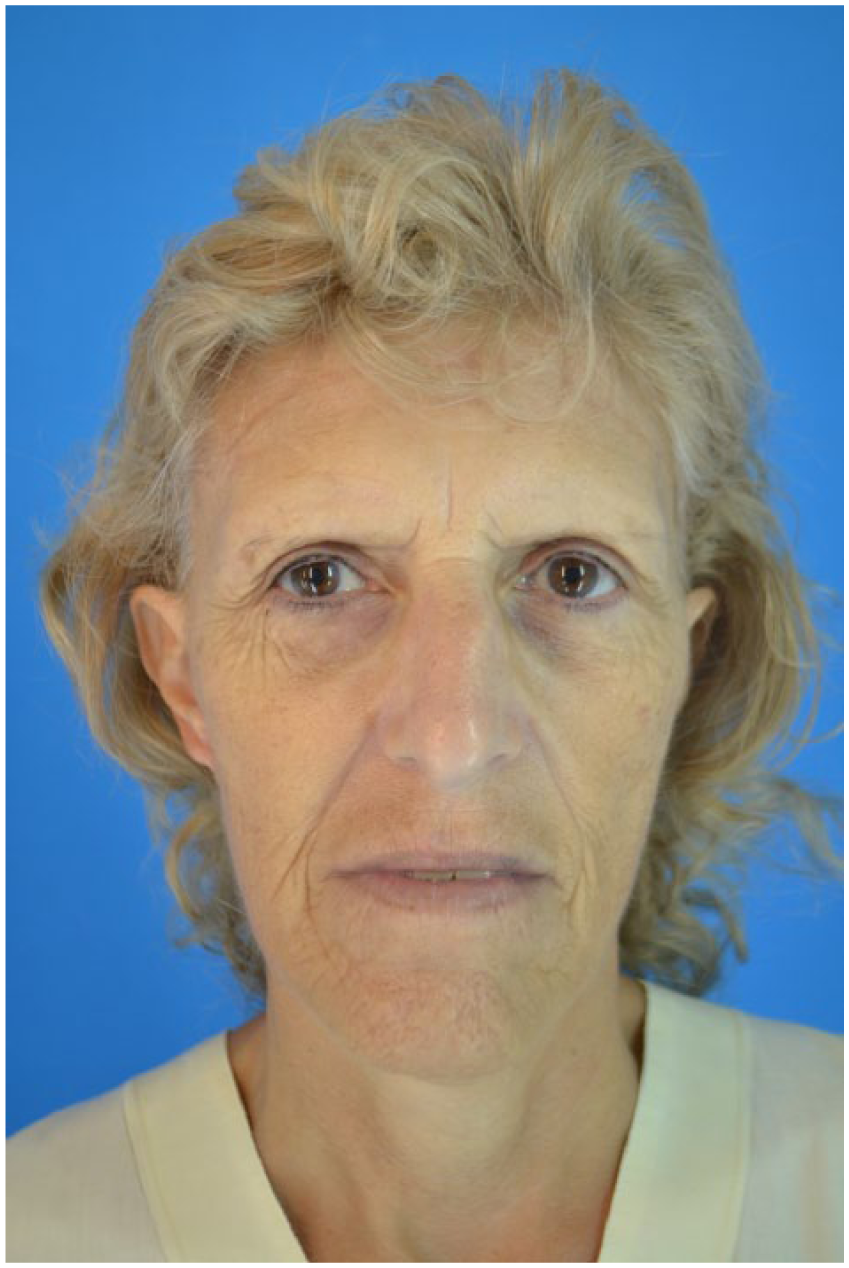
A 55-year-old patient with volumetric loss in the face (preoperative).
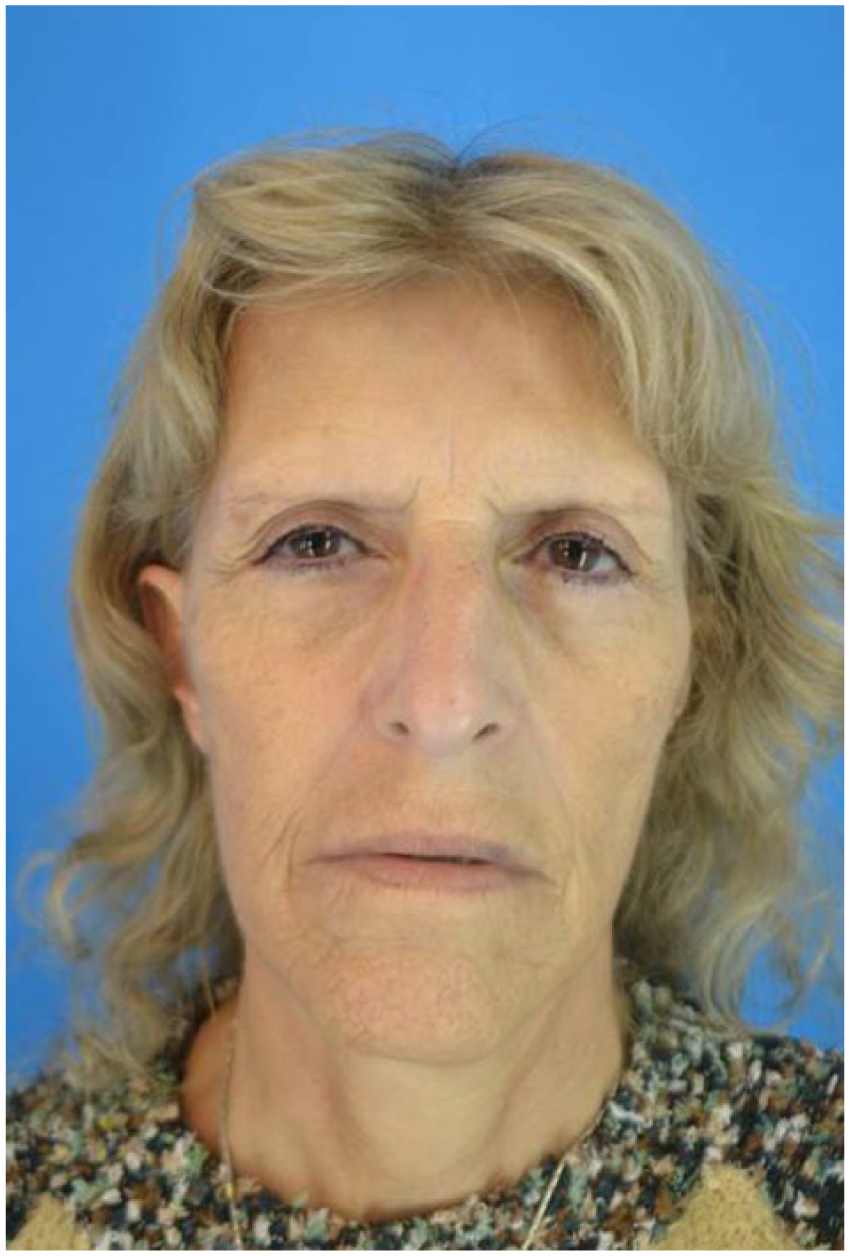
A 55-year-old patient with volumetric loss in the face (after pneumodissection and fat grafting in malar, brow, periorbital, perioral, and nasolabial surcus).
Patients Treated With Fat Grafting Without Pneumodissection.
There are no experimental studies to date, which can confirm our clinical observations and experience with this technique. However, we believe that this technique has demonstrated consistent clinical outcomes and has made the grafting process more comfortable. Further experimental studies need to be conducted to clarify the graft survival rate and the comparative results with standard grafting techniques.
Complications and Adverse Events of Carboxitherapy
The amount of gas injected during a therapeutic dose of carboxitherapy is below the volume produced by the body itself. 11 Our body produces 200 cc of CO2 when at rest and during vigorous exercise this amount may rise to 10 times that value. 12 There are reports of gas embolism during pneumoperitoneum for laparoscopic surgery. 13 There are no reports in the literature of gas embolism during CO2 insufflations in the subcutaneous tissue.
Complications were limited to (1) local pain at the injection site of the 25G needle, (2) small bruising and ecchymosis from the needle entering the dermis, and (3) a “cracking sensation” experienced by patients due to the formation of local emphysema that disappears within 30 minutes of the procedure.
Conclusion
CO2 is an abundant gas found in every living species on Earth. Its role in many industries, including medicine, has stemmed from its early discovery in 1648. With respect to its effect on both the skin and subdermal layers, CO2 has sound physiological principles confirmed via histological studies.
Our technique of pneumodissection prior to adipocyte grafting has worked with these principles in mind: using CO2 to establish volume within given tissue planes, enhancing the recipient area microenvironment in the search for greater graft uptake, and reducing sedation requirements.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.