
Abstract
A previously healthy 38-year-old female developed vision loss after abdominoplasty and liposuction of the back, flanks, infragluteal region, and thighs. Ophthalmic exam revealed bilateral optic nerve edema consistent with postoperative ischemic optic neuropathy. Laboratory workup revealed severe anemia. Despite correction of anemia, the patient suffered permanent visual loss in the left eye. Here, we review the previous reports on ischemic optic neuropathy after liposuction and the 2012 American Society of Anesthesiology Practice Advisory for perioperative vision loss.
Keywords
Introduction
Perioperative ischemic optic neuropathy (ION) is a rare but devastating complication following nonocular surgery. The incidence of perioperative vision loss has been reported to be most common in cardiothoracic surgery, spinal surgery, head and neck surgery, and nose and sinus surgery. 1 Here, we present a patient with perioperative vision loss associated with abdominoplasty and tumescent liposuction of the back, flanks, infragluteal region, and outer/inner thighs, and we review the previous reports on ION after liposuction. We also review the 2012 American Society of Anesthesiology (ASA) Practice Advisory for perioperative vision loss.
Case
A previously healthy 38-year-old female presented to the emergency department with complaints of left-sided vision loss for 4 days. She was 5 days postoperative from lipoabdominoplasty and tumescent liposuction of the back, flanks, infragluteal region, and outer/inner thighs. The patient reported 2 syncopal episodes in the recovery room after surgery and severe skin pallor. The morning after surgery, the patient awoke with blurry vision in both eyes. The visual changes in her right eye cleared. In her left eye, she reported inability to see anything in the inferior visual field. She denied pain, flashing lights, or floaters in her vision. She had no prior ocular history and was healthy without chronic medical illness, diabetes, or hypertension. Her review of symptoms was positive for menorrhagia the week prior to surgery, as well as tinnitus and headache for 4 days coinciding with the vision loss.
During her liposuction, a total of 3450 mL of fluid including fat, blood, and tumescent liposuction fluid was aspirated. The patient was prone during liposuction of the back, buttock, and thighs. The duration of prone positioning is unknown.
The patient’s initial evaluation by the ophthalmology service was performed in the emergency department. On exam, her central visual acuity was 20/20 in both eyes at near and intraocular pressures were normal. Pupillary exam was notable for a 2+ left afferent pupillary defect. Extraocular movements were full. On confrontational visual fields, there was complete loss of the inferior visual field in the left eye. Anterior segment exam was within normal limits. Dilated fundus exam revealed trace right eye optic disc edema and diffuse left eye optic disc edema with one region of nerve fiber layer hemorrhage superior to the optic nerve.
Magnetic resonance imaging (MRI) and magnetic resonance venogram (MRV) of the brain and orbits were within normal limits. Laboratory studies were notable for severe anemia with hemoglobin of 5.6 g/dL and hematocrit of 16.8%. Lumbar puncture revealed a normal opening pressure and normal cell counts. Focused assessment with sonography for trauma (FAST) was negative for acute abdominal or pelvic hemorrhage. Fecal occult blood testing returned negative. The patient was subsequently admitted due to her severe anemia and received 2 units of packed red blood cells. Follow-up hemoglobin and hematocrit after blood transfusion was 9.1 g/dL and 27.3%, respectively.
The patient subsequently followed up with neuro-ophthalmology as an outpatient 1 week after hospital discharge. Central visual acuity was 20/20 right eye and 20/25 left eye at distance. Intraocular pressures were normal. A 2+ left afferent pupillary defect was noted. Optic nerve exam showed persistent, trace edema on the right and diffuse edema with superior pallor on the left with no hemorrhages. Cirrus optical coherence tomography (OCT) of the retinal nerve fiber layer showed inferior nerve fiber layer thickening on the right and diffuse thickening on the left, consistent with edema (Figure 1). Humphrey visual field 30-2 testing revealed mild visual field constriction on the right and an inferior altitudinal visual field defect on the left (Figure 2). For putative neuroprotection effects, she was started on brimonidine 0.15% ophthalmic drops to both eyes 3 times a day.
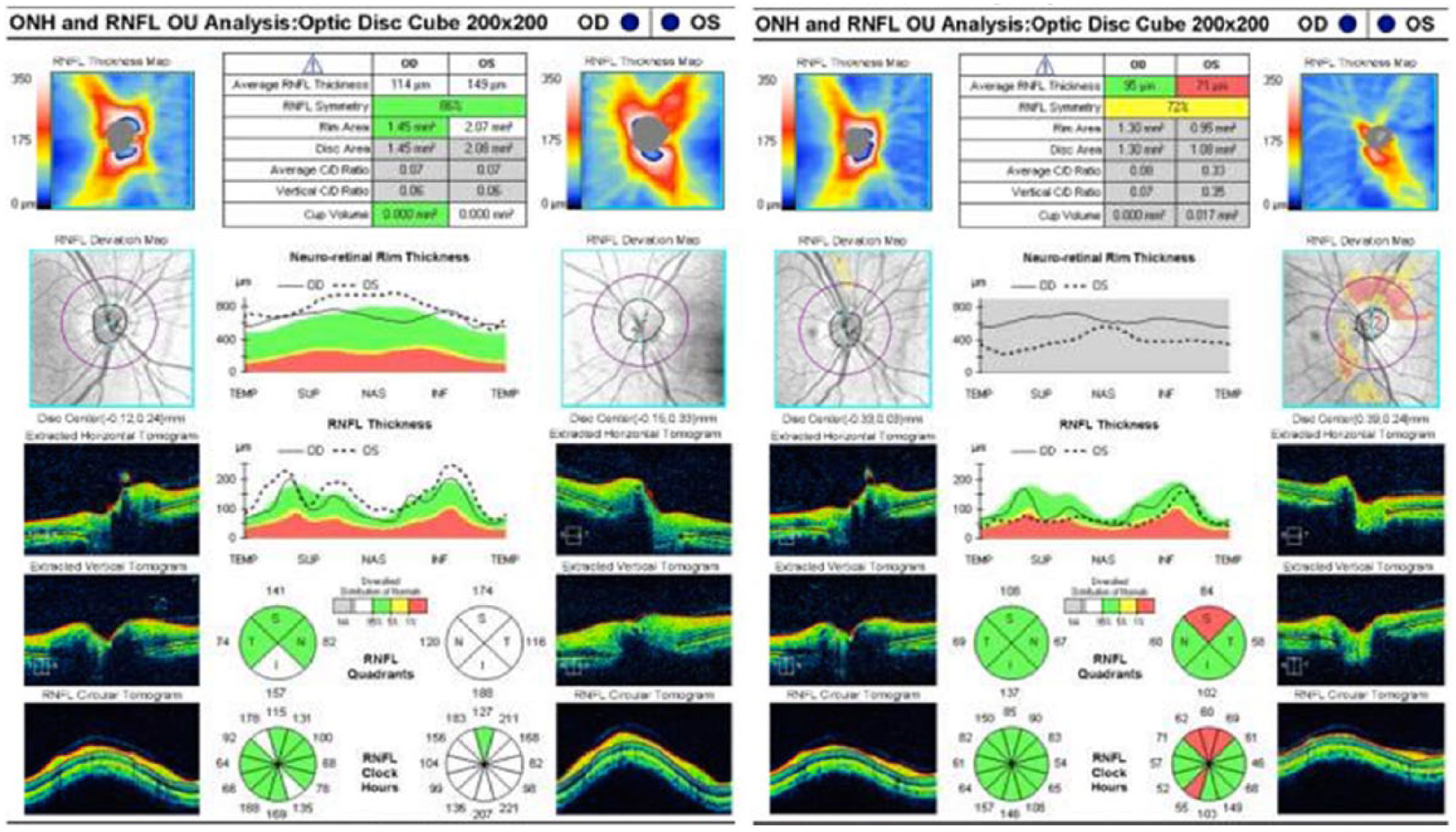
Optical coherence tomography (OCT) of the retinal nerve fiber layer 2 weeks postoperatively (left) shows inferior optic nerve thickening in the right eye and diffuse optic nerve thickening in the left eye, consistent with bilateral optic nerve edema, left worse than right. Repeat OCT 1 month postoperatively (right) shows normal retinal nerve fiber layer thickness in the right eye and superior optic nerve thinning on the left eye, indicating damage to the nerve fiber layer in the left eye. ONH = Optic nerve head; RNFL = Retinal nerve fibre layer; OU = Both eyes; OD = Right eye; OS = Left eye; SUP = Superior; NAS = Nasal; INF = Inferior; TEMP = Temporal.
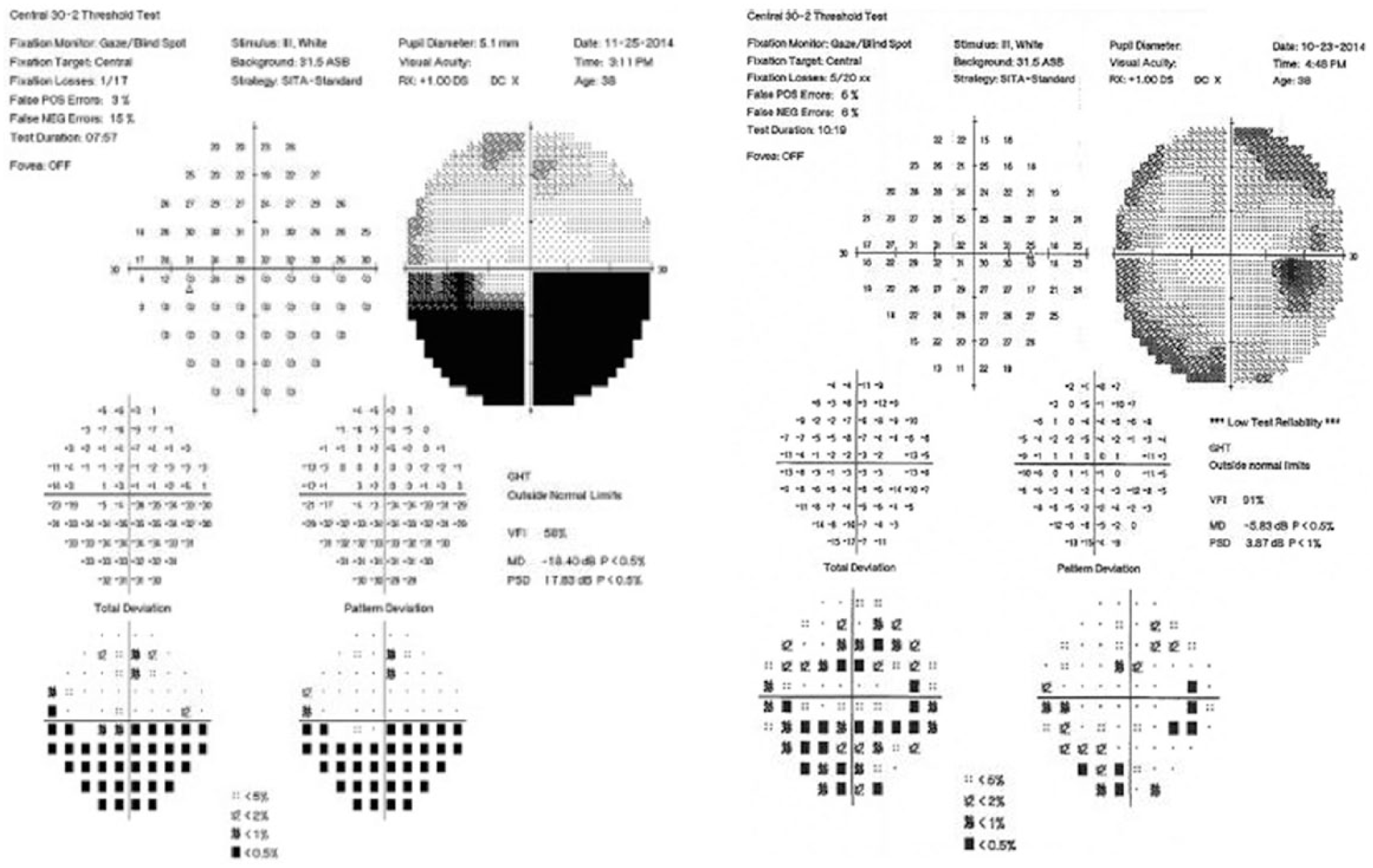
Automated 30-2 threshold Humphrey visual field showing peripheral field constriction in the right eye (right image) and an inferior altitudinal defect in the left eye (left image) after acute vision loss in a 32-year-old female who underwent abdominoplasty and liposuction of the back, flanks, infragluteal region, and thighs.
At the 3-month follow-up visit, central visual acuity and pupillary exam were unchanged. There was persistent inferior visual field loss in the left eye on confrontational visual field testing. Optic nerve exam showed bilateral resolution of edema, and superior left eye optic nerve pallor as noted previously was present (Figure 3). Cirrus OCT of the retinal nerve fiber layer showed superior nerve fiber layer thinning on the left (Figure 1). Brimonidine was discontinued.
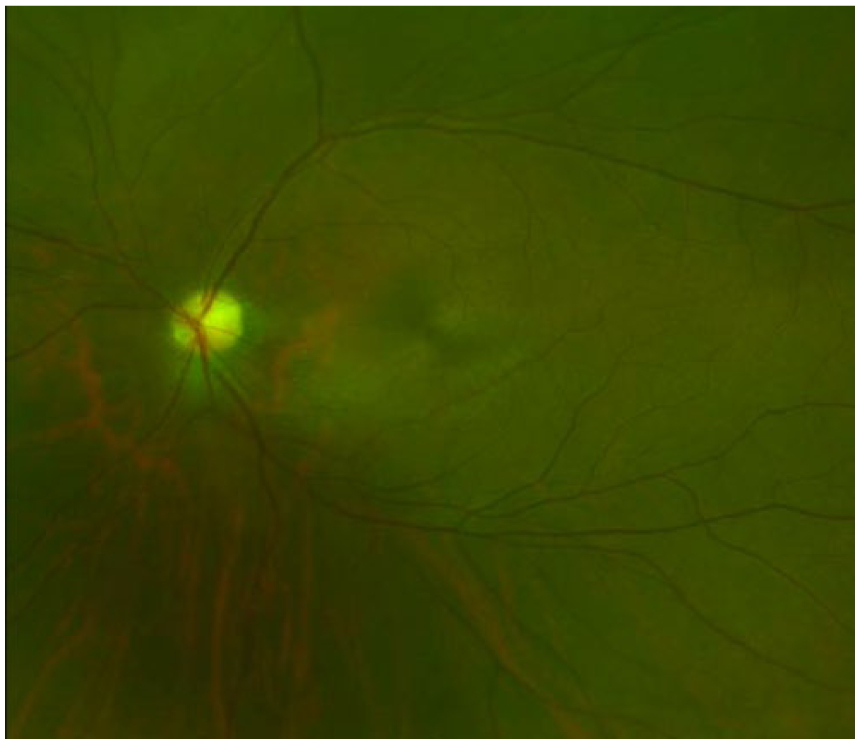
Fundus photograph of the left eye showing superior optic nerve pallor.
Discussion
Perioperative ION presents as painless vision loss within 48 hours of surgery. Visual changes can range from no light perception vision to various degrees of visual field deficits. An afferent pupillary defect and reduced color vision are usually present. Perioperative ION can be either anterior or posterior, with anterior ION initially presenting with optic disc edema and hemorrhages. Optic nerve exam in posterior ION appears normal initially, and then optic nerve atrophy with pale appearance to the nerve becomes apparent with time. The specific mechanism of perioperative ION is unclear, but there are certain perioperative factors including prone positioning, blood loss, anemia, hemodilution, hypotension, and the use of vasopressors that place a patient at risk. Patient characteristics such as small cup-to-disc ratio or a history of diabetes, hypertension, or cardiovascular disease may also increase a patient’s risk. Unfortunately, there is no proven treatment that alters the course of perioperative ION, and prevention is the key to decrease morbidity related to surgery. Correction of hypotension and anemia, though prudent, has an unclear influence on visual prognosis once vision loss has occurred. Putative neuroprotective agents, such as brimonidine, or drugs to lower intraocular pressure have not been studied in perioperative vision loss or other causes of ION. 1
Liposuction is the third most commonly performed aesthetic procedure in the United States. 2 Tumescent liposuction is considered a generally safe procedure, designed to remove 1500 mL of localized fat for cosmesis in nonobese patients. Complications arise with increasing volumes of total aspirate, which are associated with high morbidity due to hemodynamic complications secondary to third-spacing and fluid shifts.3,4 Advancement in liposuction techniques has reduced the amount of estimated blood loss per liter of aspirate and improved morbidity.5-7
There are currently 6 previous reported patients with postliposuction ION in the literature.8-13 Table 1, adapted from a review by Agostini et al, 14 summarizes the previous 6 reported cases and includes the case presented here. The range of aspirate volume among these cases is 2800 to 22 000 mL with a median value of 3575 mL. Five cases, including ours, had bilateral ION,8,10,12,13 and 2 cases were unilateral.9,11 Out of 11 eyes, 2 eyes had suspected posterior ION11,13 and 9 were diagnosed with anterior ION.8-10,12,13 Five out of the 7 cases were reported to have some degree of anemia or hypotension,8-10,13 which was likely present in the immediate postoperative period and before the vision loss in our patient given that she noted severe skin pallor in the recovery room. The reported treatment after onset of vision loss includes systemic corticosteroids, acetazolamide, blood transfusion, and topical brimonidine. Overall, treatment measures initiated after symptoms developed did not appear to have an influence on visual outcome in these patients, as with our patient.8-14
Reported cases of ischemic optic neuropathy associated with liposuction N/A = Not available.
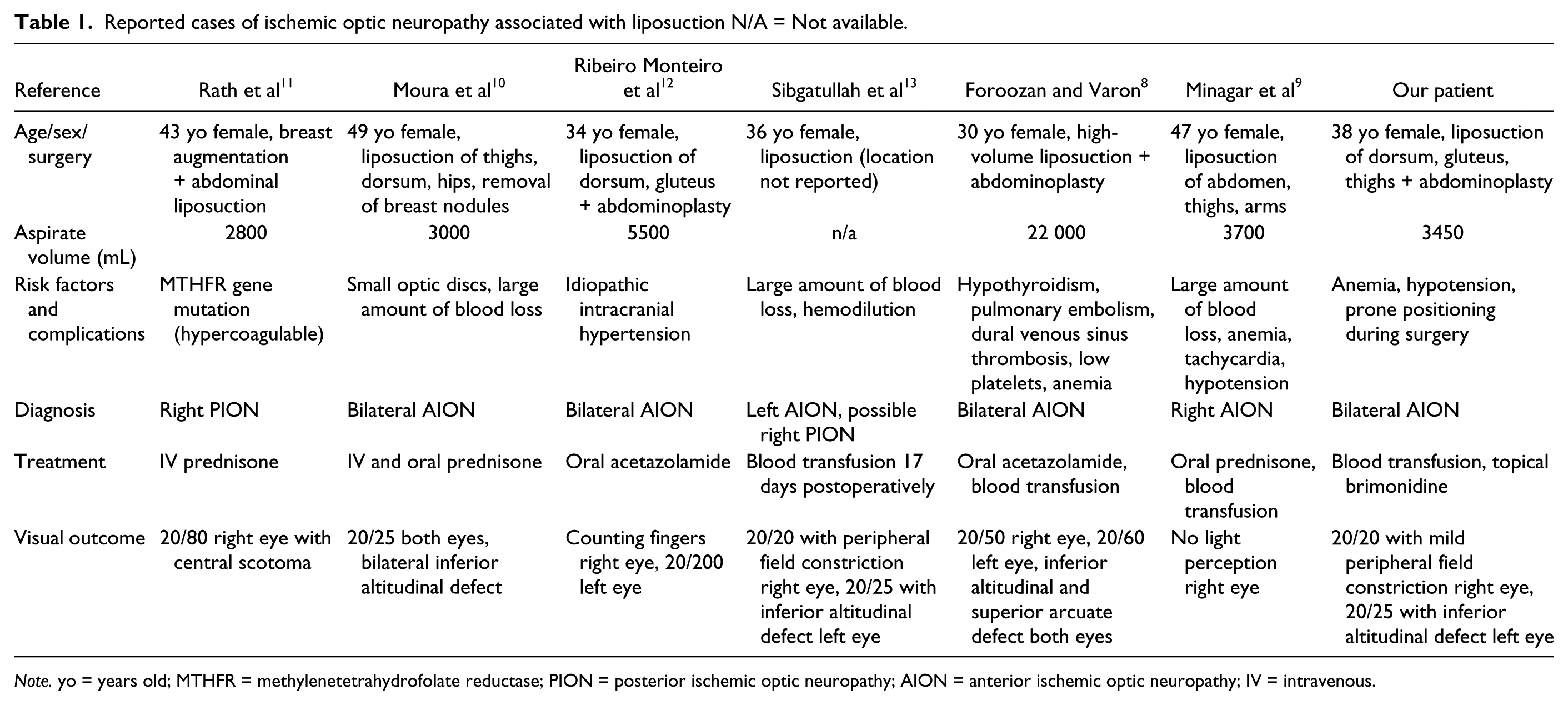
Note. yo = years old; MTHFR = methylenetetrahydrofolate reductase; PION = posterior ischemic optic neuropathy; AION = anterior ischemic optic neuropathy; IV = intravenous.
The ASA released an updated practice advisory in 2012 for perioperative visual loss associated with spine surgery, 15 which warrants consideration in liposuction patients with similar risk factors. In the advisory, vascular risk factors (ie, hypertension, diabetes, coronary artery disease, peripheral vascular disease), preoperative anemia, prolonged procedures, and substantial perioperative blood loss all increase the risk of perioperative visual loss in patients undergoing spinal surgery in the prone position under general anesthesia. 15
The significant risk factors seen in our case include severe perioperative anemia and prone positioning during surgery. Thus, we will focus on the ASA recommendations for these risk factors. The patient’s hemoglobin and hematocrit were not obtained preoperatively. However, given her known history of menorrhagia, it is possible that the patient was anemic prior to her surgery.
The ASA recommends that hemoglobin and hematocrit values should be monitored periodically during surgery. 15 There is, however, no documented lower limit of hemoglobin and hematocrit that has been associated with perioperative vision loss. Thus, a threshold to eliminate the risk of perioperative vision loss has not been established. However, the task force members agree that intraoperative hemoglobin and hematocrit should be maintained at a minimum average of 9.4 g/dL (range = 6-13 g/dL) and 28% (18%-37%), respectively. 15 These recommendations are specific for high-risk patients undergoing prone spine surgery. Given that many otherwise healthy individuals at baseline have hemoglobin and hematocrit values below the above-noted averages, these recommendations may not be reasonably applied to all cosmetic surgery patients.
In regard to prone positioning in patients undergoing spinal surgery, the risk of perioperative visual loss is thought to be associated with direct pressure on the eye or facial edema. Direct pressure in the eye has been associated with perioperative central retinal artery occlusion (CRAO) rather than ION. Direct pressure should be avoided to reduce the risk of CRAO. Prone positioning with face down without direct pressure could lead to poor venous outflow from the eye and predispose to perioperative vision loss, but there is not adequate evidence to support this mechanism with certainty. 15 Given this, it is unclear whether prone positioning contributed to development of ION in our patient. The ASA Task Force recommends that high-risk patients should be positioned so that the head is level with or higher than the heart and that the head should be maintained in a neutral forward position when possible. 15
Additional ASA recommendations include assessment of visual acuity in high-risk patients once they are awake and alert, and obtaining an urgent ophthalmology consult if there is concern for vision loss. 15 Prompt ophthalmic examination is prudent, as early diagnosis and intervention of particular causes of vision loss, specifically retinal artery occlusion, may improve visual outcomes. Optimization of hemoglobin and hematocrit, hemodynamic status, and arterial oxygenation in the immediate postoperative period is recommended. MRI should be considered if vision loss occurs to rule out other intracranial causes of vision loss. Currently, there is no recommendation for antiplatelet agents, steroids, or intraocular pressure lowering agents in the treatment of perioperative vision loss. 15
Conclusion
Postoperative ION is a rare but devastating complication that can occur after liposuction with fluid volumes noted 2800 mL or greater in previously reported cases. It is vital to discuss the possibility of postoperative visual loss with liposuction candidates prior to surgery and to ensure that fluid loss and anemia are treated immediately and continuously given that complications can occur after surgery, as in our patient. Based on our patient’s reports of skin pallor and syncope in the postoperative recovery room and her severe anemia with laboratory testing, her symptoms likely reflected initial postoperative anemia with hypotension. Preventing and treating perioperative blood loss and hypotension with attention to and modifications to prone positioning may be important steps in avoiding this outcome in these patients, as treatment once symptoms develop seems to be of little benefit and even young patients without vascular risk factors can be affected, which is highlighted by our patient’s event.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.