
Abstract
Hypertrophic and atrophic scars are typically thought to be at opposite ends of the pathological healing process, and, as a consequence, cosmetic treatments have tended to be varied and disparate. This article, however, presents data from a pilot study that illustrates a coherent and unified approach can be used for the effective treatment of both scar types. This method studies the use of a precision microneedling device using mixed length needles. This is used in conjunction with the application of topical, pharmaceutical-grade creams consisting of retinoic acid, antioxidants, anti-inflammatory agents, and sea sponge collagen. Data and examples are presented that show good skin remodeling for both types of scars.
Introduction
Typically atrophic scar treatments rely on stimulating the body’s own healing processes, and hypertrophic scars are treated by suppressing them. This article shows, however, that stimulating the body’s healing process can also successfully remodel both. The technique described is based on using a microneedling device that delivers controlled punctures at 2 depths in conjunction with the application of topical preparations. The punctures are made to target both the superficial and deeper layers of the dermis. The objective is to simultaneously trigger the body’s scarless and scarring healing processes, respectively, while controlling the evolution of the scar formation with the topical products. The results presented in this article are based on a sample size insufficient for statistical analysis; however, the results are uniformly indicative of overall improvements for both types of scars.
In the following sections, we recapitulate the key factors of both normal and pathological wound healing. This is followed by a description of the study design and a presentation of the findings.
Normal Wound Healing
Normal wound healing is typically described by 4 phases:
Vascular
Inflammatory
Proliferative
Remodeling and maturation
Vascular Healing
The first reaction to skin trauma is hemostasis. An initial vasoconstriction is followed by vasodilatation, and the formation of a hemostatic plug or clot.
Inflammatory Healing
Hemostasis is followed by the inflammation phase. Within 24 hours, proinflammatory cellular responses start, involving neutrophils, monocytes, and macrophages. This phase lasts for approximately 4 to 6 days. Neutrophils are first attracted to the wound, and monocytes follow 48 to 96 hours later. This response is stimulated by interleukin-1 (IL-1), tumor necrosis factor (TNF), and transforming growth factor (TGF). Angiogenesis and fibroblast proliferation and migration are triggered and are mediated by macrophages that produce vascular endothelial growth factor, fibroblast growth factor, TNF, epidermal growth factor (EGF), platelet-derived growth factor (PDGF), and IL-1. 1
Proliferative Healing
The proliferation phase lasts from 4 to 14 days, during which time the scar is formed, 2 but it can start as early as 24 hours from the injury. The early, full epithelization will lead to a less noticeable scar. Cells migrate from edges of the wound and the adnexa. Fibroblasts migrate into the wound site, and start producing collagen type 3, and this promotes keratinocytes migration. Some fibroblasts transform into myofibroblasts, which are then responsible for wound edge contracture 3 and wound shrinkage. This process is regulated by different signals, mainly by PDGF, EGF, and TGF. 1
Remodeling
The remodeling phase starts roughly 8 days after injury and lasts for over a year. During this time, the initially formed excess collagen is digested, and the type III collagen is replaced with type I collagen. The wound tensile strength against dehiscence increases over the first 2 weeks by 10%, at 1 month by 40%, and at 3 to 12 months by approximately 80% from the baseline. 4
Pathological Wound Healing
Aesthetically unsightly scars are the result of abnormal wound healing; are often associated with redness, itching, and pain; and can cause significant patient distress. Deeper injuries and larger wound surfaces are more likely to produce pathological scars. It has been shown that an injury on the thigh with a depth of more than one-third of the total skin thickness results in scarring. 5 Wound width affects the appearance of scars: Narrow linear cuts require very little wound retraction, whereas wider wounds (eg, from burns) require more. Wider wounds result in more tension and rigidity, 6 which subsequently leads to more uneven scarring.
There are 2 types of raised scars: hypertrophic and keloid. The difference between hypertrophic and keloid scars is that the former stays inside the boundaries of the original lesion, 7 and the latter grows outside the margins of the wound. 8 In contrast to raised scars, sunken scars are referred to as atrophic, and these are a result of a reduction of skin and tissue in the wound area.
All types of scars are created by defective collagen creation. Histologically, collagen fibers in scar tissue are abnormally straight with irregular and somewhat random interlocking patterns, whereas normal skin collagen fibers are helicoidal and have a more regular interwoven structure.
Both raised scar types occur more readily in areas of natural skin tension like the upper shoulders, the anterior chest, and over the surfaces of the joints. Additional risk factors can be genetic predisposition and ethnicity (eg, skin types 5-6), repeated trauma on areas of increased skin tension, prolonged active inflammatory processes (cystonodular acne, foreign body reaction), abnormal immune response, abnormal collagen composition (eg, low mature collagen type 1 combined with high soluble collagen type 3), dysfunction of melanocyte-stimulating hormone, and microcirculatory occlusion.
Both hypertrophic and keloid scars result in increased fibroblasts and extracellular matrix (ECM) formation. The ECM is replaced by overexpressed and randomly oriented collagen and proteoglycans. Random cross-linking and continuation of the collagen synthesis lead to increased density and changed viscoelasticity of collagen fibrils. This subsequently blocks cellular signaling and proliferation, and results in scar tissue that has notably different characteristics from the surrounding skin.
Hypertrophic scars normally grow for a period of up to 3 months after injury and then develop higher tensile strength and rigidity during a period of maturation. Keloid scars can continue to grow much longer, continuing for years after the injury. 9 As a result, there are more fibroblasts and randomly oriented collagen fibers and proteoglycans in a keloid scar, and they have distinct histological features. 10 Fibroblast density is increased in both hypertrophic and keloid scars, but the latter typically exhibits increased fibroblast proliferation rates. 11
Atrophic scars result from the loss of underlying supporting tissues. The scars contain less collagen and proteoglycans, resulting in a thinner ECM than in the surrounding normal tissue. The process can take from a few weeks to a few months, and is mainly due to enzymatic activity in the matrix remodeling. Fibroblasts and keratinocytes produce enzymes, including those that determine the architecture of the ECM, and the balance between matrix metalloproteinases (MMPs) and their inhibitors. It is the lack of MMP inhibitors that leads to the atrophy of resulting scar.
Atrophic scars can occur as a result of inflammation (eg, acne), surgical and accidental trauma, iatrogenic factors (eg, from steroids), abnormalities of collagen synthesis and connective tissue disorders (morphea, scleroderma), 12 and genetic disorders (eg, chromosome 10 anomalies, xeroderma). 13 Treatment modalities are normally directed toward stimulating and elevating atrophic scars and suppressing and diminishing hypertrophic scar areas12,14 (see Table 1).
Recognized Therapeutic Options for the Treatment of Scars.
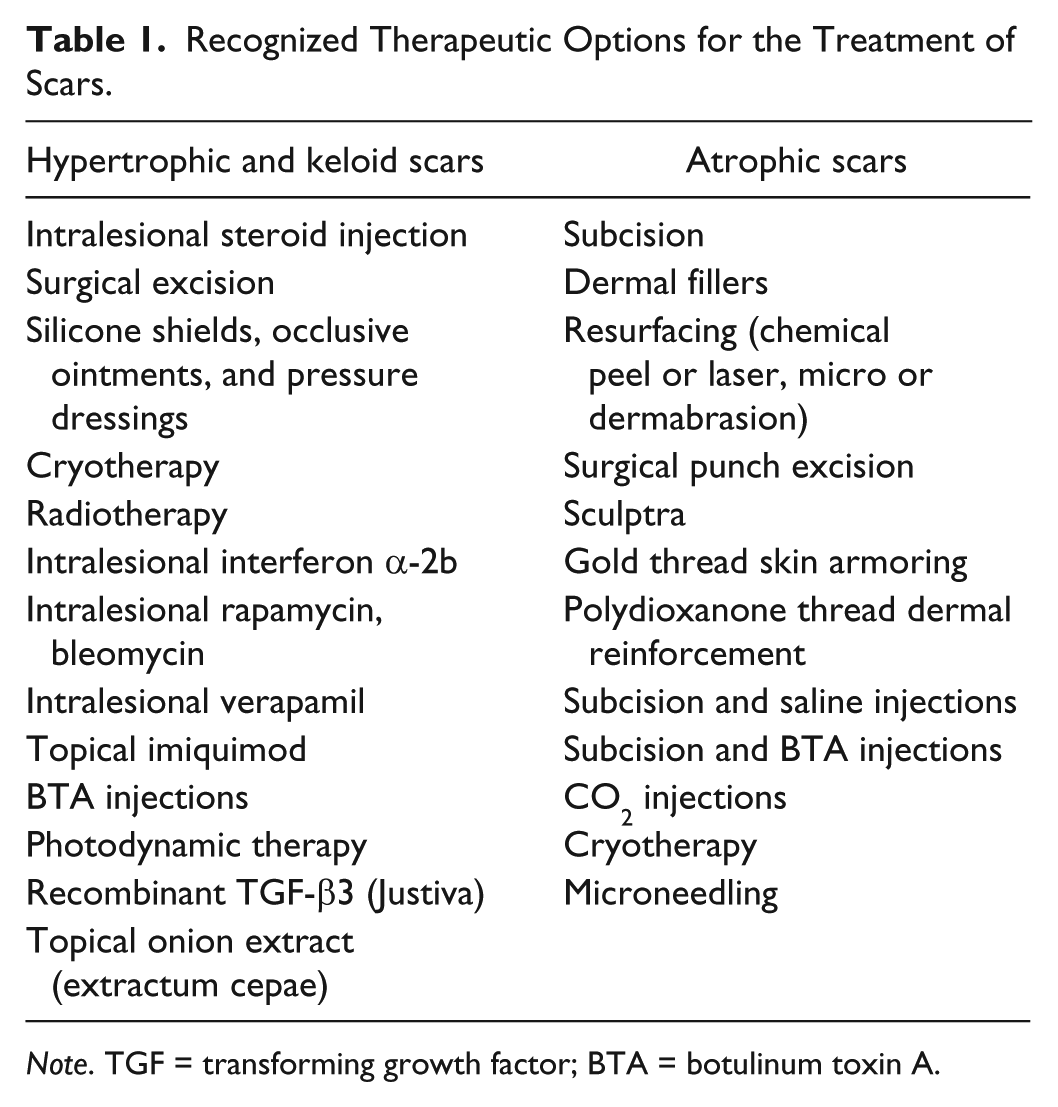
Abbreviations: TGF, transforming growth factor; BTA, botulinum toxin A.
Aim of the Study
The aim of this work was to evaluate a combination therapy for both atrophic and hypertrophic scars. The approach was based on microneedling in conjunction with the use of pharmaceutical-grade topical products. The micropunctures were produced with a spring-loaded derma-stamp, and the topical preparations consisted of retinoic acid, vitamin C, anti-inflammatories, skin lightening agents, and a marine-derived collagen.
Study Design
It was the work of Dunkin et al 5 that motivated this study. Their article showed that an injury on the thigh with a depth of more than one-third of the total skin thickness results in scarring and shallower injuries do not. This suggests that scars are a result of wounds that penetrate the papillary dermal layer, which exists at about this depth.
The motivation of this study was to evaluate a process that combines local skin wounds both above and below the papillary layer to see whether the 2 internal processes of scar formation (scarring and scarless) could successfully diminish existing scars. This was regulated with the use of additional topical products.
This pilot study was based on a small number of patients selected from an existing pool available in an aesthetic clinic. Unfortunately, a small scale of the study did not allow for a proper control group. Treating only a half of a patient’s scar, leaving part untreated was a valid choice. This would have been a good control, but the patients would not have agreed to this and would not have been satisfied.
Patients were not charged fees or offered any inducements. An informed consent was obtained from each participant.
Sample Selection Criteria
The patient sample consisted of 25 participants, aged from 18 to 45 years. The profile of the group included the following:
Nine with hypertrophic scars, and 16 with atrophic scars
Scars were located on various parts of the body
Only patients with mature scars were included (ie, having scars aged at least 12 months)
Scars were caused by trauma, surgery, inflammation, or steroids
None of the patients had had prior treatment for scarring, although most had had other aesthetic treatments
Excluded
Some candidate patients were excluded. These consisted of those with
true keloid scars (ie, hypertrophic scars that had grown beyond the boundaries of the original injury) and
patients with underlying connective tissue disorders and abnormal collagen synthesis.
Equipment and Products Used in the Study
Choice of the equipment and products used for the study was cross-referenced with the existing publications. The review of literature revealed that microneedling is well known to be an effective treatment of atrophic scars. 15 However, there were no studies advocating this for hypertrophic scars. The literature does mention the use of topical retinoids for both types of scars.16-19 Anti-inflammatory agent use is reported for hypertrophic scar treatment.14,20 Most reviews advocate a combined approach using various treatment methods on either atrophic or hypertrophic scars.
The microneedling device used in the study was a spring-loaded derma-stamp. The stamp plate was a unique design consisting of rows of medical-grade stainless steel solid microneedles alternating between 0.8 mm and 2.1 mm in length (see Figures 1 and 2).

Spring-loaded derma-stamp.
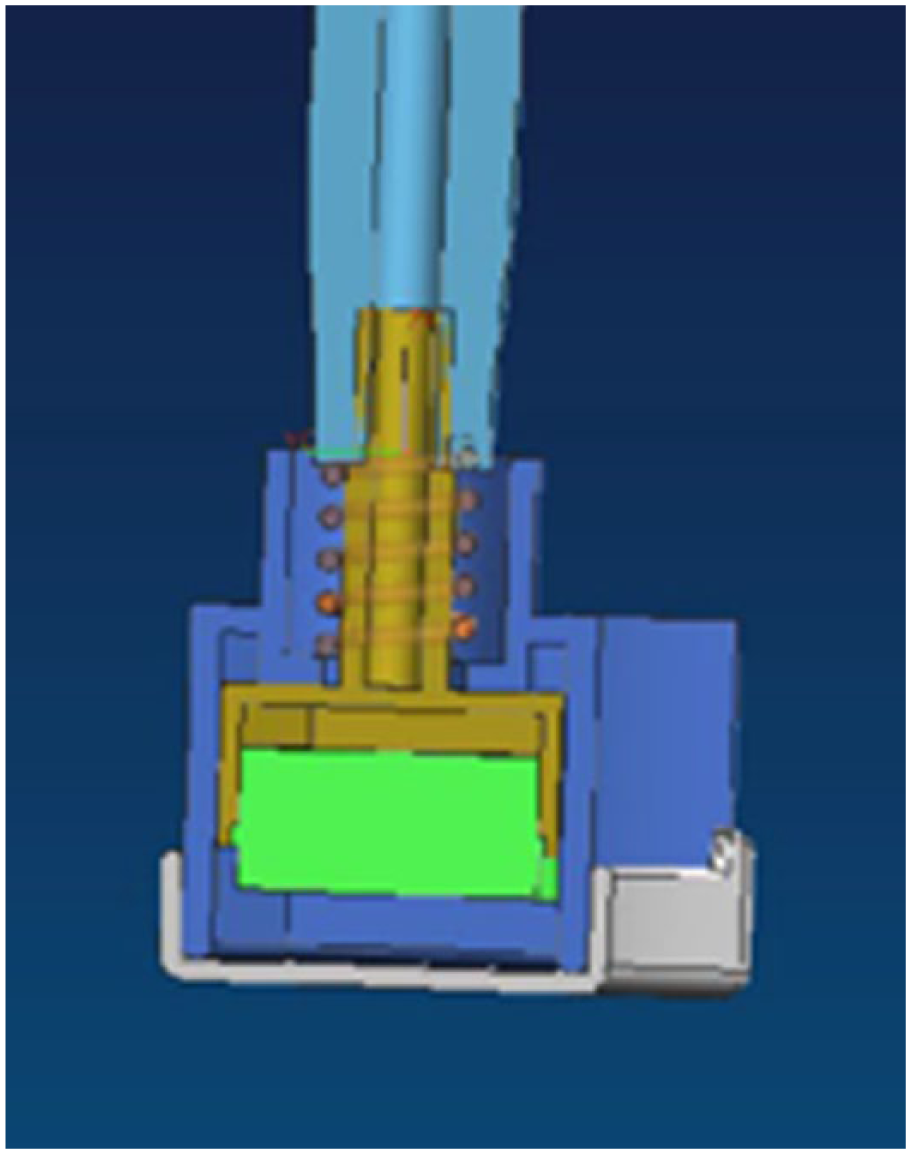
Derma-stamp design.
As discussed before, the stamp was designed to deliver a combined response from the skin. On average, the long needles penetrate below the papillary dermis to stimulate scar healing, whereas the shorter needles remain above the papillary layer and are intended to provoke scarless healing. The spring mechanism helped deliver a more uniform dermal penetration during each application.
The topical preparations used were compounded by a pharmaceutical laboratory, and included the following:
A compounded cream containing retinoic acid, vitamin C, hydroquinone, dexamethasone, alpha hydroxy acid, and acetaminophen
A serum containing nanoparticles of sea sponge collagen in hyaluronic acid base
An antioxidant sunblock containing tea tree and grape seed oils combined with an SPF 85 agent
Treatment Protocol
The microneedling and topical preparations were used in the following way:
Patients applied the cream to the scar area twice a day for 2 weeks before commencing with microneedling.
This was followed by application of the derma-stamp to the scar tissue areas once every 2 weeks for a total of 24 sessions.
Each microneedling session was followed by an application of the serum, which was protected under a Dermatix Silicone dressing, and left for 48 hours.
Between microneedling sessions patients used the cream and sunblock twice a day.
Assessment Methods
The results of the study were assessed both quantitatively and qualitatively:
Quantitative assessment
Physical measurements were made using a cross-sectional ultrasonic technique. The ultrasound device (UF-400AX; Fukuda Denshi, Japan) provided a resolution of 80 microns axially (ie, in the depth axis of the skin) and 250 microns laterally (parallel to the surface). Measurements were made at 4 separate points along the scar using the device’s linear probe. An assessment of each scar was made both before and after completion of the course of treatment.
The same operator made all measurements. The results are compiled in Figures 3 and 4.
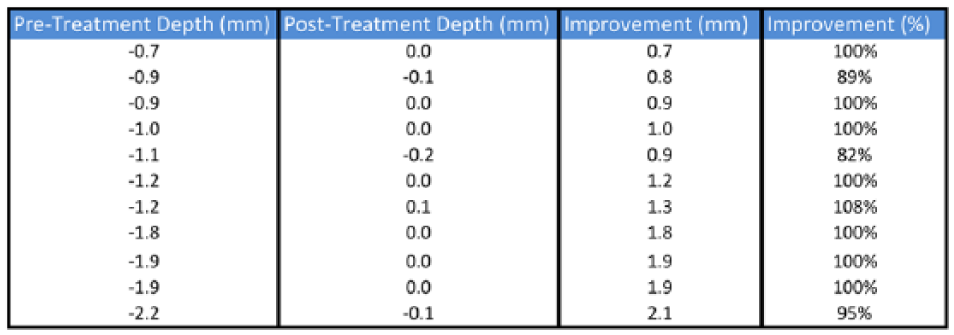
Atrophic scar treatment data.
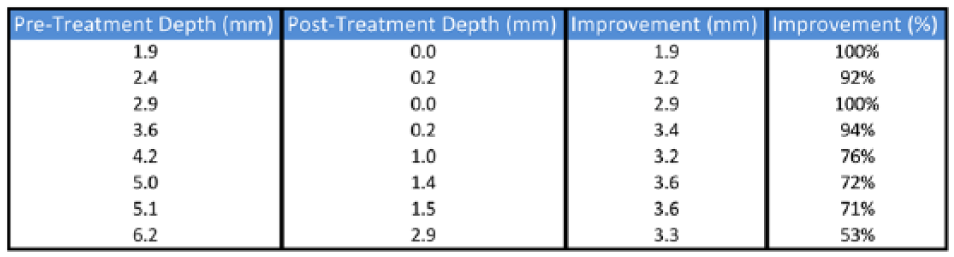
Hypertrophic scar treatment data.
Qualitative assessment
A modified Patient and Observer Scar Assessment Scale (POSAS) was used both before and after using the treatment. The modified scale consists of the traditional one with 2 added criteria: “Aesthetic Appearance” and “Aesthetically Upsetting.” These have been included to capture the psychological aspect related to cosmetic perception. The results are compiled in Figures 5 and 6. Before and after photos were taken by the same operator from anteroposterior, lateral, and oblique views. Scoring was made both from in vivo assessment and the photos. The patients and the physician independently scored the scar characteristics. Scores ranged from 1 to 10 with the latter being a more negative assessment. The scores were accumulated to produce a total.
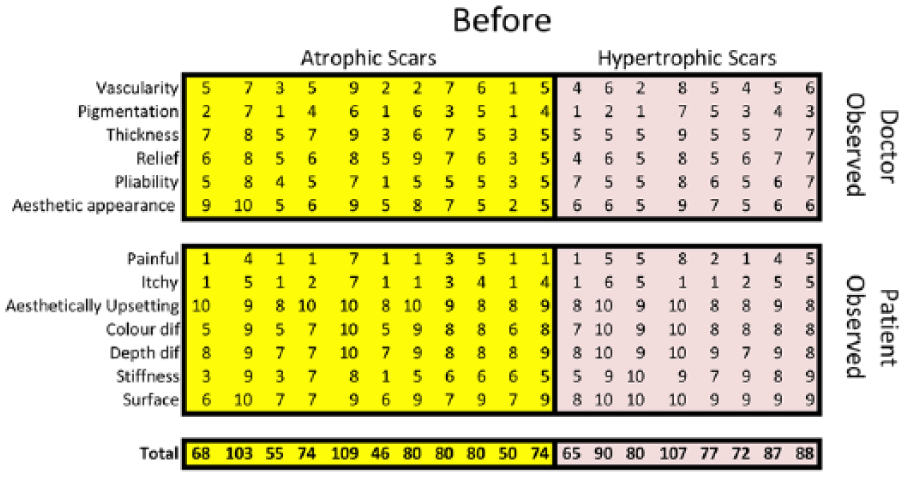
Patient and Observer Scar Assessment Scale score before treatment.
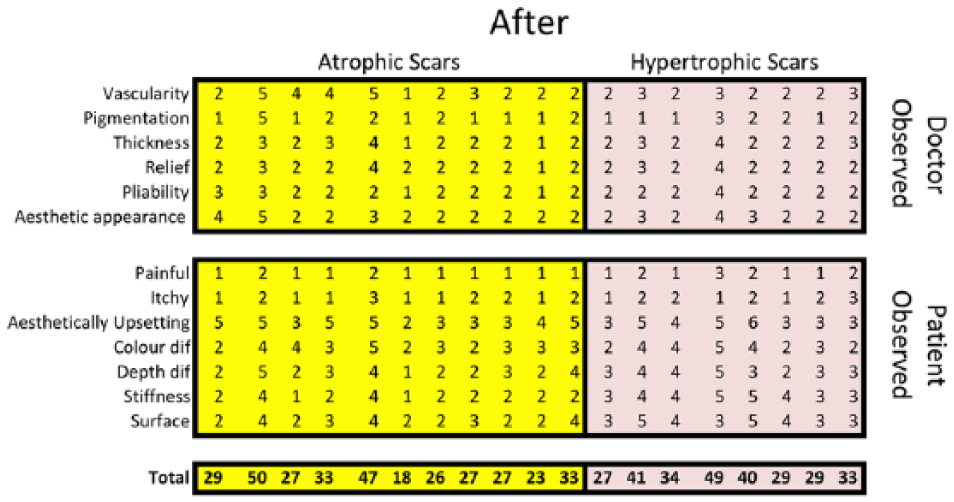
Patient and Observer Scar Assessment Scale score after treatment.
Results
Of the 25 patients that originally enrolled in the study, 19 completed it and 6 dropped out. Of those who did not complete the study, 2 moved away, 1 became pregnant, 1 left for unknown reasons, and 1 stopped due to excessive irritation from topical retinoic acid. Among the 19 participants who completed the study, 11 had atrophic scars and 8 had hypertrophic scars. The distribution of scar types is detailed in Table 2.
Distribution of Scar Types.

Normal skin typically has a modified POSAS score of 13. The tables in Figures 5 and 6 show that the average POSAS score for atrophic scars before treatment was 74 and decreased to 30 after treatment. This is a reduction by 44 points or a 72% improvement with respect to the baseline. The tables also show that for hypertrophic scars the average POSAS score before treatment was 83 and decreased to 35 after treatment. This is a reduction by 48 points or a 69% improvement. On average, patient’s perception of scars before treatment was more negative than the doctor’s, and the patient’s perception after treatment was more positive than the doctor’s.
All of the atrophic scars decreased their depths significantly, and the majority by 100% (that is to say, level with the surface of the normal skin). The average atrophic scar depth was 1.345 mm below normal skin level and improved by 1.318 mm, a quantitative improvement of 98%. The graphs shown in Figures 7 and 8 illustrate the types of improvements achieved over the cohort. It can be seen from the figures that atrophic scars can be uniformly reduced by 100%, at least for the severity of scars seen in this study.
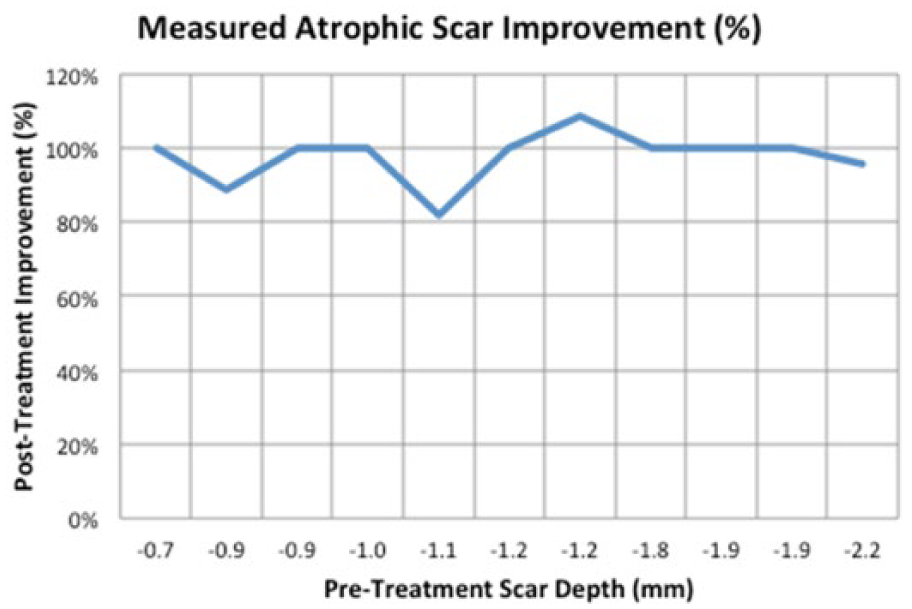
Atrophic scar improvement in percentage.
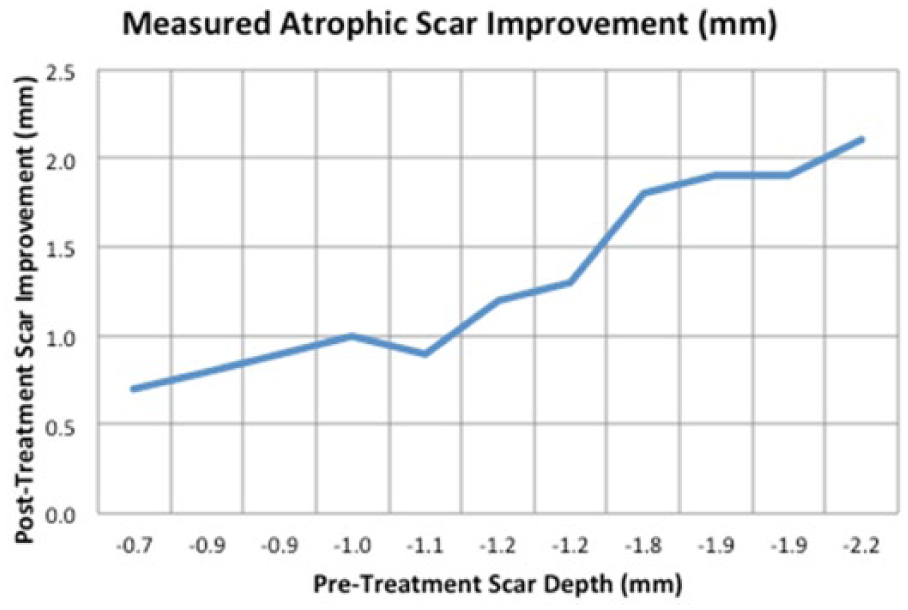
Atrophic scar improvement in millimeters.
The average height of the hypertrophic scars was 3.913 mm. Following treatment, the average height reduction was by 3.013 mm. The graphs in Figures 9 and 10 show the improvements made for the cohort. As can be seen from the figures, there seems to be a cap in the amount of reduction that can be achieved for hypertrophic scars. In this study, the limit was determined to be about 3.5 mm (see Figure 10).
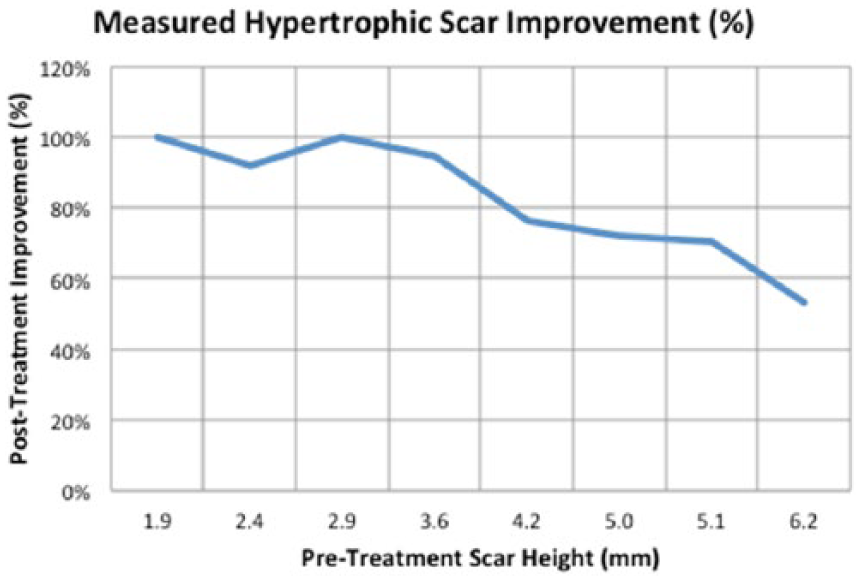
Hypertrophic scar improvement in percentage.
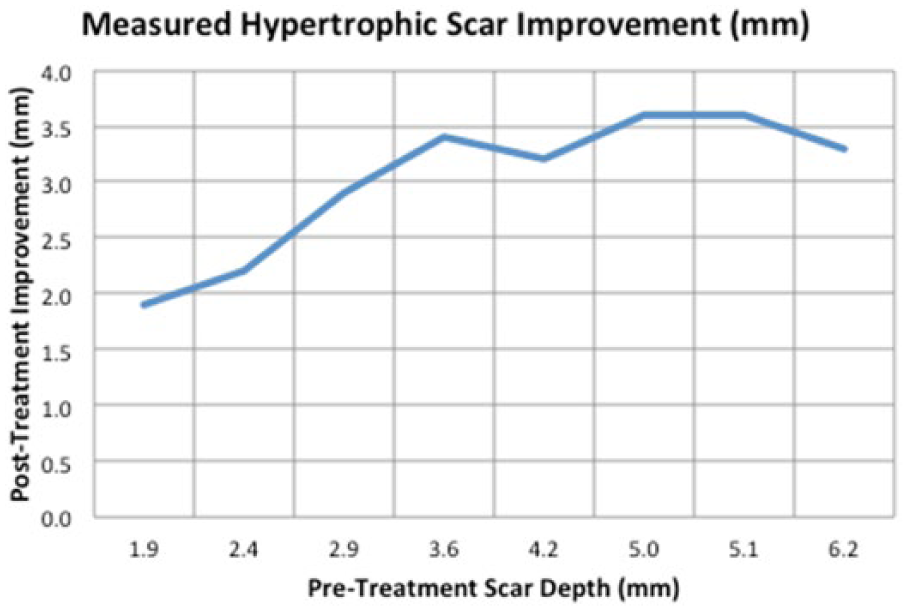
Hypertrophic scar improvement in millimeters.
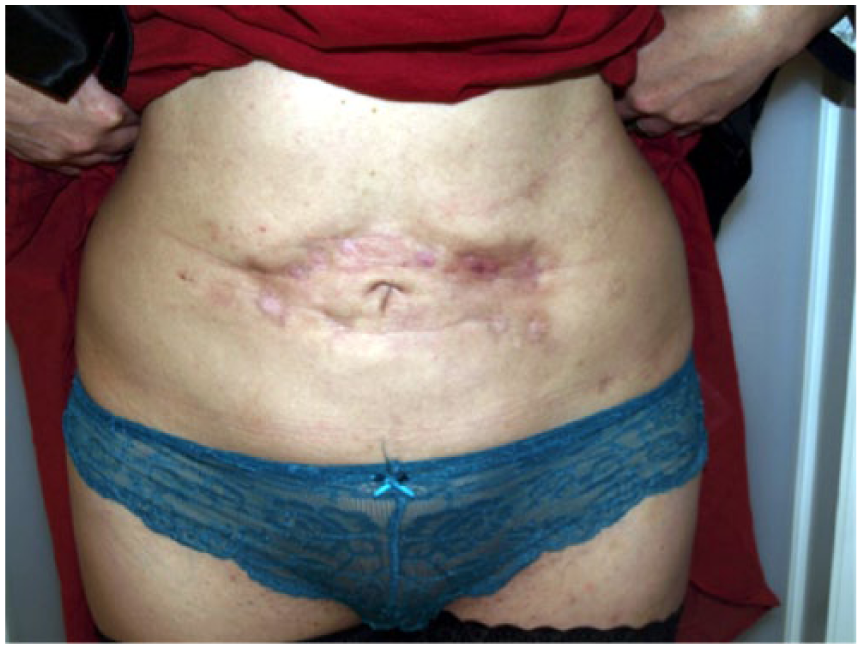
Figures 11 and 12 illustrate the before and after results for a typical example of treating atrophic scars with this method. Figures 13 and 14 illustrate typical before and after results for hypertrophic scars using the method.
Atrophic scar before treatment.

Atrophic scar after treatment.

Hypertrophic scar before treatment.

Hypertrophic scar after treatment.
Conclusions
During the healing process, tissue remodeling involves specific mechanisms that can give rise to either atrophic or hypertrophic scars. The balance between MMPs and their inhibitors controls this process and most of the time results in normal scarring. However, when there is inadequate inhibitor response, this results in a diminished deposition of collagen factors and subsequently forms an atrophic scar. In contrast, if the inhibitor response overly suppresses the MMPs, a raised nodule of fibrotic tissue forms, producing a hypertrophic scar.
This article presents a study of scar treatments using a microneedling stamp device to provide controlled punctures at 2 depths in conjunction with the use of topical preparations. The logic of the approach is to leverage the body’s natural scarless response conjointly with the scarring one and to control these through the local application of regulating ingredients.
The data from the study (as presented in the tables and graphs) illustrate the results of a treatment protocol that combines 2 dermal puncture depths in conjunction with the use of regulating agents. The conclusion is that from both the perspective of quantitative analysis as well as that from subjective perception, significant benefits were obtained. Measured depth or height of scars was significantly improved.
In all the cases, atrophic scars were reduced by 98%, with the average being 1.3 mm. In most of the cases, the improvement was as much as 100%.Hypertrophic scars were reduced more than 60%, with an average of 3 mm of shrinkage. In most of the cases, the improvement was about 75%.
Hypertrophic scars can improve over time even without any treatment 21 ; however, this can take years, causing a significant distress to the sufferer. The study showed a definite benefit from the intervention for decreasing hypertrophic scars. However, the data show that for consequential hypertrophic scars, there seems to be a limitation on the percentage of improvement that can be achieved, with the maximum being about 3.5 mm.
More important is the data on patient perception of the treatments. The modified POSAS scores demonstrated significant benefits. On average, atrophic scars achieved a reduction in score from 74 to 30, and hypertrophic scars from 83 to 35. When compared with the POSAS score for normal skin (13), these are notable improvements.
Although this work is based on a patient sample size too small for meaningful statistical analysis, it does provide indicative data sufficiently compelling to merit further study, and which may also be useful for other practitioners. We conclude that micropunctures in conjunction with the use of topical products acting as regulators seem to retrigger the body’s scar remodeling process. Although it is not understood how this works biochemically, the practical outcome is that it seems to provide an opportunity to adjust the scar expression to a point that is both measurably and subjectively better, and this is true regardless of scar type.
As a final note, an important advantage of this treatment protocol is that it evidently has a much lower cost (of more than a factor of 10) to the patient than methods such as laser, chemical peel, and injectable and immunomodulating therapies currently employed for treatment of scars. Furthermore, the administration of the therapy is much simpler and well tolerated by patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.