
Abstract
Pterygium is a frequent conjunctival abnormality in outdoor workers. Genetic background factors are involved. In this study, the authors report their experience in utilizing a rotatory conjunctival flap (RCF) under local anesthesia. A retrospective analysis was conducted of all patients undergoing the proposed technique by one surgeon from 2010 to 2016. Preoperative and postoperative photographs at the longest follow-up visit were used for analysis. A total of 76 patients underwent RCF in an office setting. The average follow-up time was 9 months (range, 6 months to 4 years). All patients were satisfied with the result. One patient required a conjunctival granuloma excision. Additional advantages include the ease of operation, cost, conjunctival preservation for glaucoma filtering surgery, and a short execution time.
Pterygium is a wing-shaped conjunctival encroachment onto the cornea generally situated on the nasal side. It sometimes occurs both nasally and temporally, and rarely only on the temporal side. Pterygium is more frequent in areas with more ultraviolet radiation, 1 in hot, dry, windy, dusty, and smoky environments.2,3 There is also a hereditary factor. 4
The incidence of sunlight in the medial angle of the eye globe, plus reflection and refraction of the cornea in that area contribute to its appearance. The external angle is protected from sun exposure by the nasal root. Pterygium provokes ophthalmic discomforts such as photophobia, itching, tearing, burning, foreign body sensation, red eye, and induced astigmatism; but sometimes the patient requests for its removal for cosmetic purposes.
Various pterygium removal techniques have been described.5-9 Today, a wide variety of techniques are in use, from the bare sclera procedure without using a microscope to very complex approaches like amniotic membrane transplantation 10 and lamellar keratoplasty. 11 The aim is to excise the pterygium and prevent its recurrence. An extensive Tenon capsule removal is mandatory. Autologous conjunctival grafting seems to be the best method, giving both low recurrence rate and high safety. However, there is consensus that a flap is better than a graft for reconstructive surgery.12,13 The most reliable techniques consider a conjunctival autograft transplant obtained from the same eye globe and fixed with sutures, biological glue, or autoblood as tissue adhesive.14-16 The controversies appear if sutures or glue are used.17-19 Autoblood has been advocated as a tissue adhesive that minimizes the cost. 20 If a conjunctival autograft, which prolongs the time of surgery, is taken from the upper quadrants of the eye globe, it disables a filtering glaucoma surgery in the future. The donor site of the autograft usually is left bare and heals by granulation. One of the advantages of our proposed technique is that it preserves the conjunctiva. In this study, the authors report their experience in utilizing a rotatory conjunctival flap (RCF).
Methods
This was a retrospective analysis of 76 patients (81 eyes) undergoing the proposed technique, performed by one surgeon (J.S.) starting from 2010 to 2016. Informed consent was obtained for each procedure, and the review adhered to the standards of the Declaration of Helsinki. All patients were from the private practice of the senior author (J.S.), and all surgeries were performed at the office under local anesthesia plus mild sedation. Surgery time was noted from the first incision until the lid speculum was removed. An eye patch was used for 1 day. Topical antibiotic and steroid eye drops were instilled for 1 month in decreasing doses. The follow-up visits were scheduled at 10 days; 1, 3, and 6 months after the operation.
Surgical candidate included any person with pterygium without any other ocular disturbances. Five patients were bilateral; only one of them was operated on simultaneously. Three patients had recurrent pterygium operated on elsewhere. Preoperative and postoperative photographs at the longest follow-up visit were analyzed. Complications were recorded.
Surgical Technique
The operation was performed under local anesthesia (with light oral sedation using 5-10 mg Valium) in the office setting using a surgical microscope. Topical proparacaine hydrochloride 0.5% eye drops were instilled first. The pterygium area was infiltrated with lidocaine 2% with epinephrine 1:100.000. The resection of the lesion involved only the area over the cornea (Figure 1A). Atraumatic tissue forceps tented the conjunctiva and tooth forceps grasped the Tenon capsule to excise it widely with Westcott scissors (Figure 1B). Bipolar hemostasis was performed as follows. A sterile cotton tip applicator soaked in Mitomycin 0.02% was applied to the bare sclera for 30 seconds. A profuse wash was done with saline solution. A thin conjunctival flap 1 mm wide was obtained from the superior edge of the excised triangle with its base in the limbal area (Figure 1C). The free extreme of the flap was anchored in the episclera with a 10-0 nylon suture with buried knots in the lower limbal area. One or two sutures of the same material, carried out in the same way, drew together the edges of the excised triangle, leaving the less denuded area of sclera to heal by granulation (Figure 1D).
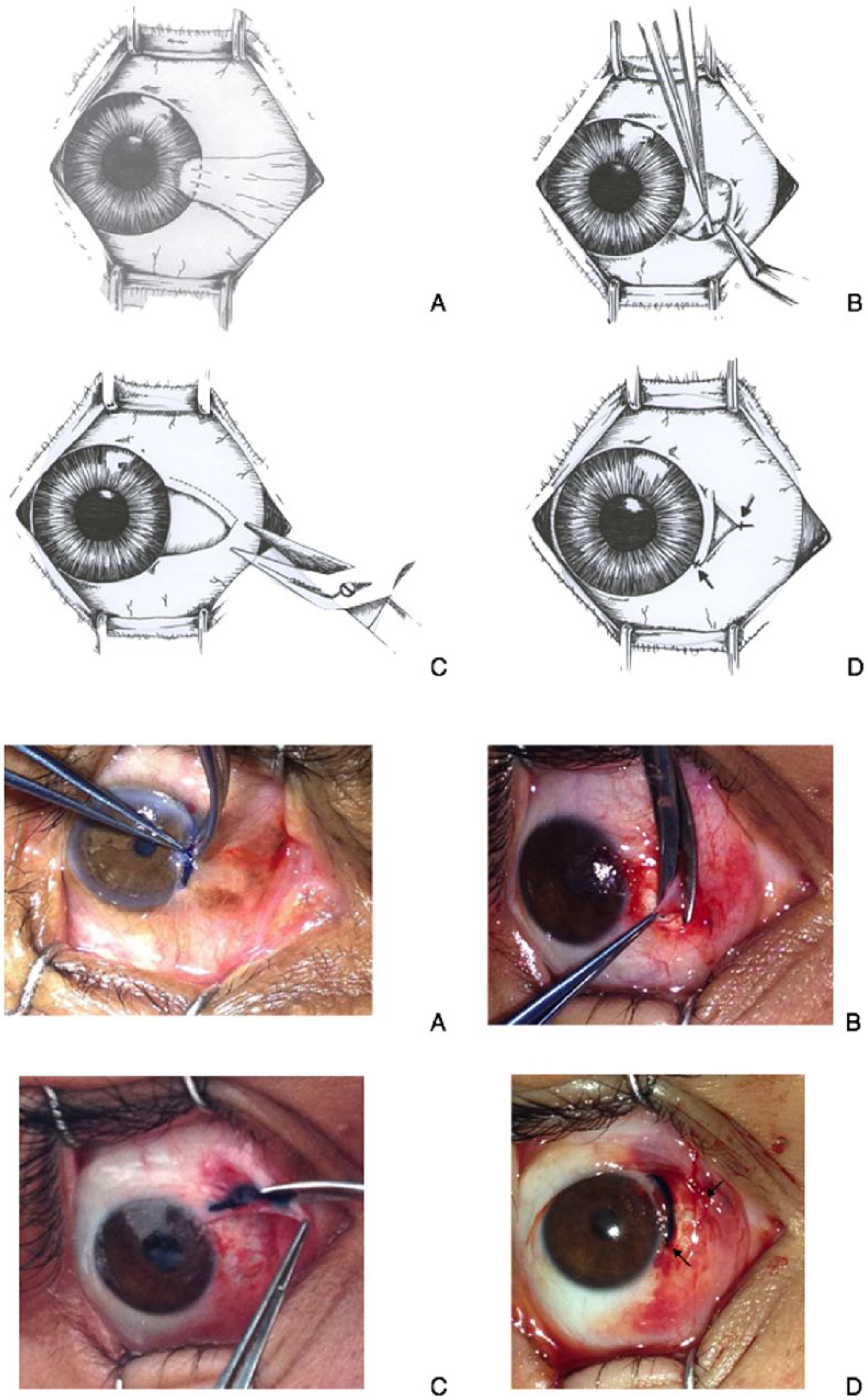
Surgical technique. A, Minimal conjunctival resection following the limbal line, outlined with methylene blue as seen in the photograph. B, The grasping of the Tenon capsule with a tooth forceps helps pull it and excise it thoroughly. C, The conjunctival flap has its base at the limbal area (outlined with methylene blue); this could be performed on the superior or inferior edge of the triangle. D, Usually 2 sutures of nylon 10-0 are sufficient to coapt the edges, as shown by the arrows. In the photograph, the flap is depicted with the dye.
Results
A total of 76 patients (41 males, 35 females; mean age, 52 years; range, 29-64 years) underwent the described technique of RCF. The procedure was done on both eyes simultaneously in one of the 5 bilateral cases due to the fact that the patient was a foreigner. One patient required a conjunctival granuloma excision. The average follow-up time was 9 months (range, 6 months to 4 years).
Representative clinical photographs from one patient in this cohort can be seen in Figure 2.
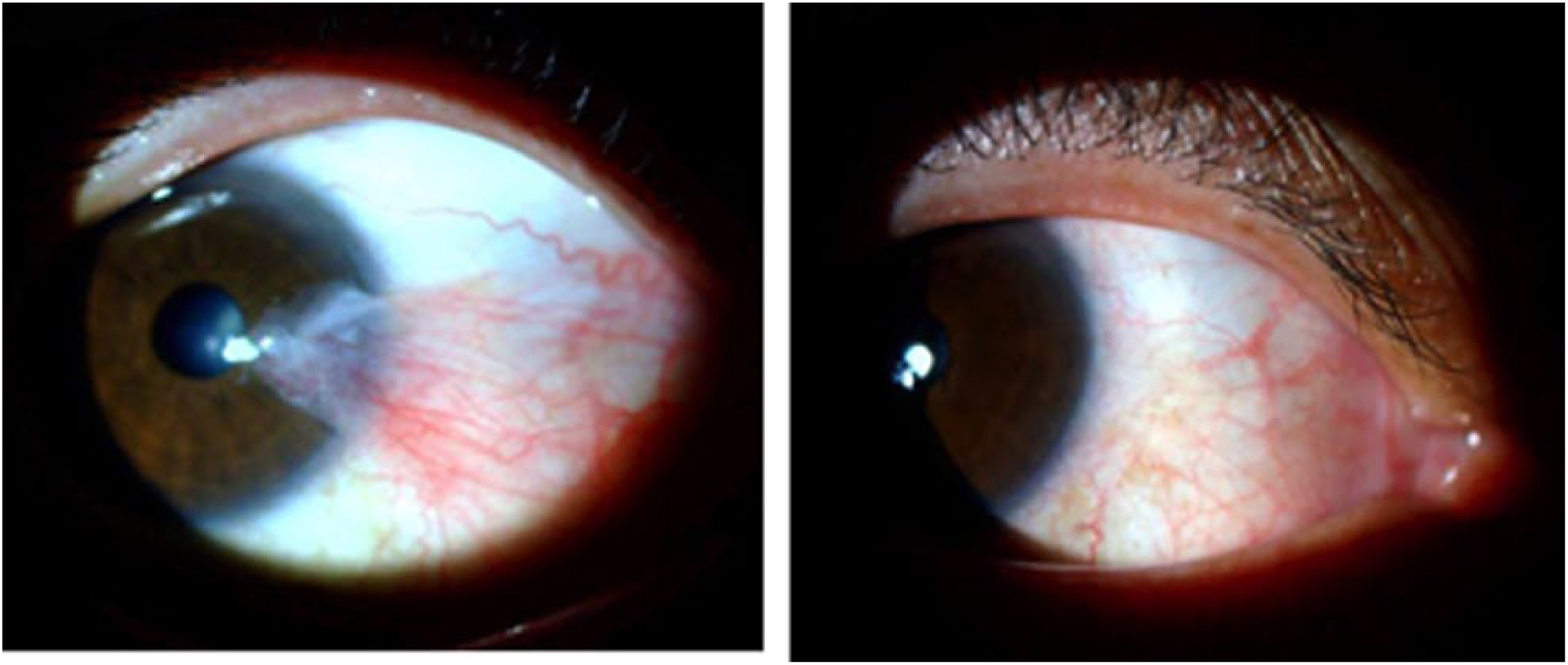
Representative clinical photographs. Preoperative and 1.5-year postoperative photographs of a pterygium removal surgery using the rotatory conjunctival flap technique.
Discussion
RCF for pterygium removal is an effective and safe technique. It has high patient satisfaction, in that all patients were content with the result at the 6-month postoperative visit, as assessed by a short questionnaire at that time. It is an efficient surgery taking an average of 16 minutes to complete, much less than the other techniques. RCF is also an inexpensive technique, due to the fact it does not require the use of adhesives. Finally, it is a reliable method since recurrence of pterygium in most cases is seen within 6 months, 21 and all of the patients who underwent RCF surgery at the 6-month checkup are without recurrences. One of the reasons for this, as it is believed by the authors, is that the RCF acts as a barrier to neovascularization of the limbal area.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.