
Abstract
Rhinoplasty, the third most common cosmetic surgical procedure in the United States, represents the second most litigated facial plastic surgery procedure. Previous examinations of litigation specific to rhinoplasty are limited. The objective of this study was to comprehensively evaluate rhinoplasty malpractice litigation over the past 30 years and to investigate the financial burden of medical malpractice litigation associated with rhinoplasty, as well as factors that contribute to litigation and negative defendant outcomes. Jury verdict and payment reports related to rhinoplasty malpractice litigations over the past 30 years (1988-2018) were obtained using the WestlawNext and Nexis Uni subscription-based legal databases. The term “malpractice” was searched in combination with “rhinoplasty” and various names associated with the procedure. Cases included in the analysis were reviewed for outcomes, verdict payments, defendant specialty, and allegations raised in proceedings. Of the 46 cases identified, 12 (26%) were resolved with a plaintiff verdict payment. The median payment awarded was $127 500 (standard deviation, $96 590.63). The surgeon specialties found for 35 cases included otolaryngology (17 [49%]), plastic surgery (13 [37%]), facial plastic surgery (3 [9%]), and oral/maxillofacial surgery (OMFS; 2 [6%]). A greater proportion of cases involving otolaryngologists were resolved with payment compared with cases involving plastic surgeons (4 [24%] vs 1 [8%]), though this difference did not reach statistical significance (P = .26). The most common allegations raised among the 46 cases were poor cosmesis (20 [43%]), intraoperative negligence (18 [39%]), inadequate informed consent (13 [28%]), and nasal function deficits (13 [28%]). Cases had a higher likelihood of being resolved in payment when allegations of cosmetic deformity (7%, 95% confidence interval [CI], −17.55 to 31.91) and nasal function deficit (17%, 95% CI, −9.29 to 45.32) were present, nevertheless these findings did not reach statistical significance (P = .60 and P = .24, respectively). Rhinoplasty malpractice litigation resulting in payments can create substantial financial burden for the defendant. Common factors cited by plaintiffs for pursuing rhinoplasty malpractice litigation included cosmetic deformity, intraoperative negligence, lack of informed consent, and nasal function deficit. Cosmetic deformity and nasal function deficit allegations tended to result in negative defendant outcomes, though these findings are inconclusive. Our findings reinforce the importance of physician-patient communication, including conducting a comprehensive informed consent process, to limit or avoid postsurgical allegations.
Introduction
Cosmetic surgery continues to grow in popularity. According to the National Clearinghouse of Plastic Surgery Procedural Statistics, there were 1.8 million cosmetic surgical procedures performed in the United States in 2017, representing a 1% increase over 2016. 1 While the overall rate of malpractice claims remains stable, 2 the compensation claims against plastic surgeons are increasing. 3 In addition, plastic surgeons inherently have a higher than average lifetime risk of malpractice litigation compared with other specialties and face nearly twice as many malpractice claims annually. 4 Most claims in plastic surgery (PS) result from lack of informed consent, poor cosmesis, or lack of expertise in performing a procedure. 5
Rhinoplasty represents the third most common cosmetic surgical procedure in the united states (215 000 procedures annually) 1 and constitutes the second most litigated facial PS procedure behind blepharoplasty. 6 Once performed primarily by plastic surgeons, rhinoplasty is now an established procedure within the otolaryngological subspecialty of facial PS. 7 With that in mind, and given today’s litigious environment, it behooves the facial plastic surgeon to understand the factors affecting judicial outcomes for rhinoplasty malpractice claims.
Previous examinations of litigation in otolaryngology8-14 and facial PS 6,15,16 have been performed; however, the data specific to rhinoplasty are limited.7,17 The objective of this study was to perform the first comprehensive analysis of the legal allegations, verdicts, and indemnities associated with rhinoplasty medical malpractice litigation cases.
Methods
Data Sources
Jury verdict and settlement reports were obtained from WestlawNext (Thomson Reuters, New York, NY) and Nexis Uni (RELX Group, New York, NY). WestlawNext is a subscription-based legal database containing publicly available state and federal case laws, public records, and other related information from over 40 000 databases. Westlaw and WestlawNext have been used repeatedly to analyze medical malpractice litigation.6,15,16,18-20 Nexis Uni (formerly LexisNexis Academic) is a subscription-based database which provides access to more than 17 000 business and legal sources from LexisNexis. Nexis Uni has 3 primary collections, 1 of which contains full-text legal documents, including US Federal and State court cases, and law reviews from the late 18th century to present.
Search Strategy
We searched both databases for the term malpractice in conjunction with several search terms related to rhinoplasty, including rhinoplasty, septoplasty, septorhinoplasty, nose job, nose surgery, nasal surgery, and nasalplasty to account for the various procedure names associated with rhinoplasty. The most recent search was performed in June 2018. This search yielded 309 court cases between the 2 databases (WestlawNext, n = 146; Nexis Uni, n = 163) over the last 30 years (1988-2018). Duplicate (n = 135) and unrelated cases (n = 128) were removed, and 46 cases were included in the analysis (WestlawNext, n = 41 and Nexis Uni, n = 5).
Data Collection
For each of the 46 cases, we recorded the procedure, alleged cause of malpractice, case outcome, award value (if applicable), defendant characteristics (sex and surgical specialty), plaintiff characteristics (age and sex), and other allegations raised in proceedings. Information about the surgeon’s training was often unavailable in the database; however, for 35 of the 46 cases, we confirmed the specialty information from individual practice Web sites and physician biographies on the Internet. These specialties included general otolaryngology (OTO), otolaryngology with a fellowship in facial PS (FPS), PS, and OMFS.
Statistical Analysis
We conducted statistical analysis using Fisher exact test for categorical variables (specifically, to compare the presence of legal allegation against a physician with the outcome favorability for that physician). Comparison of means and comparison of proportions were calculated for effect sizes using 2-sided t test. A P value less than .05 was considered statistically significant (MedCalc Software, Mariakerke, Belgium). Data analysis took place from June 18, 2018, to July 12, 2018.
Because the information used in the study was obtained from publicly available court records, no confidential health records were encountered. Consequently, this analysis required no institutional review board approval.
Results
Case Characteristics
A total of 46 cases met our inclusion criteria. Cases were distributed evenly over the last 3 decades: 1988-1997 (14 [34%]), 1998-2007 (15 [37%]), 2008-2018 (12 [29%]). New York represented the state with the most identified cases (12 of 31 with known state [29%]; Figure 1). Thirty-two plaintiffs (70%) were female, and plaintiff age ranged from 16 to 60 years (median age, 33.5 years). Most cases (34 [74%]) were resolved in the defendant’s favor, while the remaining 12 (26%) were resolved with a plaintiff verdict and payment. The mean and median payment awarded was $1 363 458.33 and $127 500.00, respectively (standard deviation, $96 590.63). The characteristics of the cases resolved with payment (n = 12) are presented (Table 1).
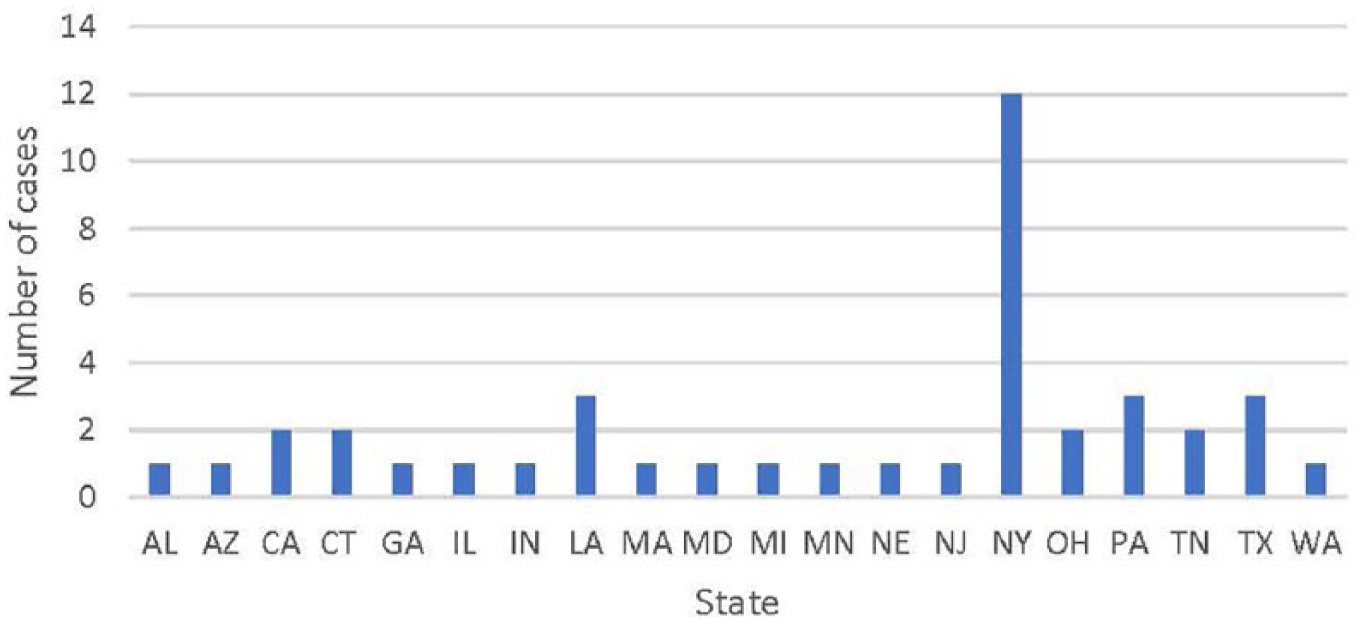
Location (by state) of malpractice litigation related to rhinoplasty.
Characteristics of Cases Resolved With Payment (n = 12).
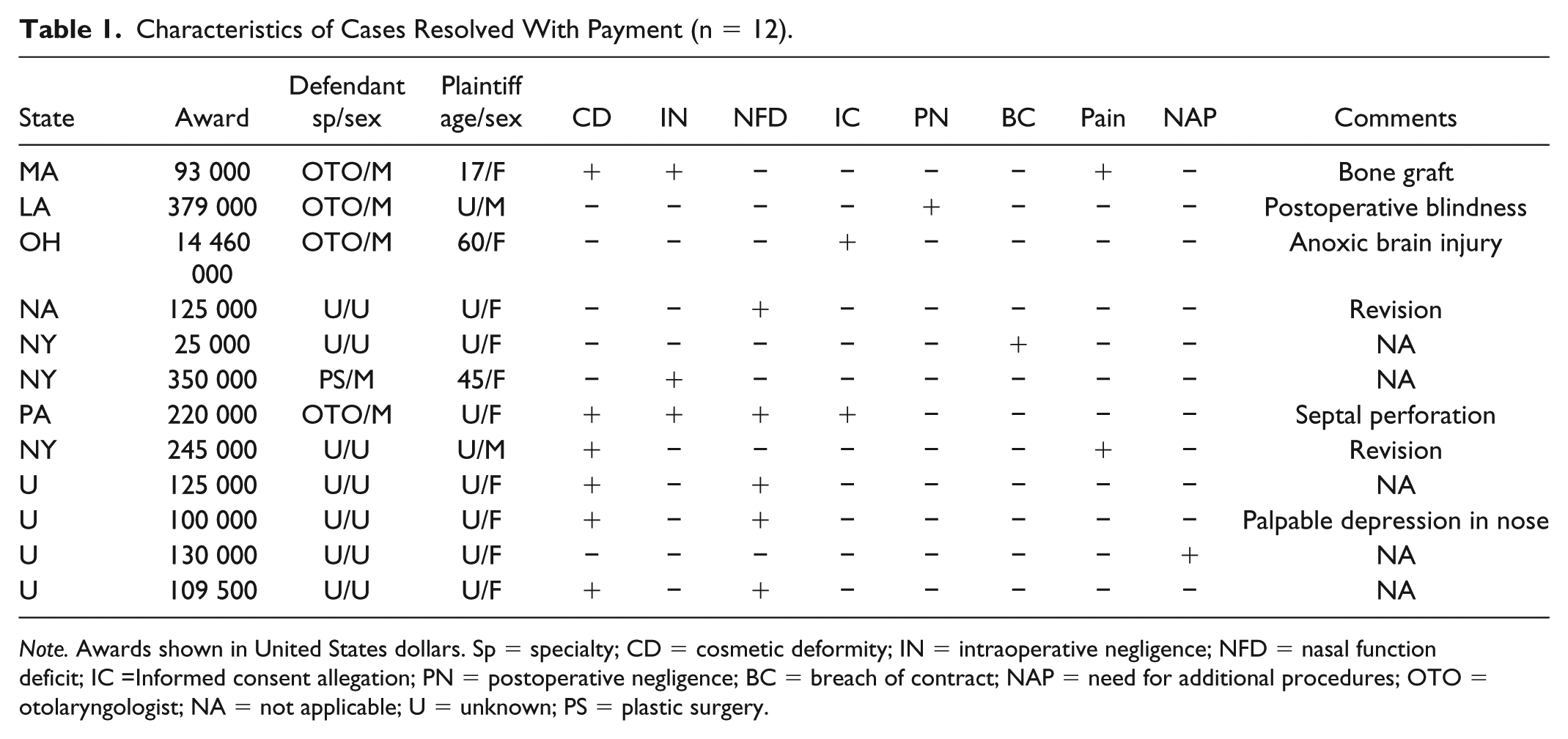
Note. Awards shown in United States dollars. Sp = specialty; CD = cosmetic deformity; IN = intraoperative negligence; NFD = nasal function deficit; IC =Informed consent allegation; PN = postoperative negligence; BC = breach of contract; NAP = need for additional procedures; OTO = otolaryngologist; NA = not applicable; U = unknown; PS = plastic surgery.
Characteristics of Defendants and Cases Resolved With Payments
Most defendants were male (31 of 34 with known sex [91%]). The defendant’s surgical specialty was found for 35 cases and included OTO (17 cases [49%]), PS (13 [37%]), FPS (3 [9%]), and OMFS (2 [6%]) (Figure 2). Of these 35 cases with known physician specialty, 5 (14%) were ruled in favor of the plaintiff and resulted in a mean and median payment of $3 100 400 and $350 000, respectively (standard deviation, $6 351 228.02). The payment frequency and payment amount for these 5 cases varied by specialty: for OTO, 4 of 17 cases (24%) ended in payment with a median reward of $299 500.00 (standard deviation, 7 115 628.67); for PS, 1 of 13 cases (8%) ended in payment with a single reward of $350 000.00. Cases involving OTO defendants were more often resolved with payment compared with cases involving PS defendants (difference of proportions 16%, 95% CI, −13.34 to 40.40), though this difference of 16% is not statistically significant (P = 0.26). No payments were awarded for litigation against FPS and OMFS defendants.
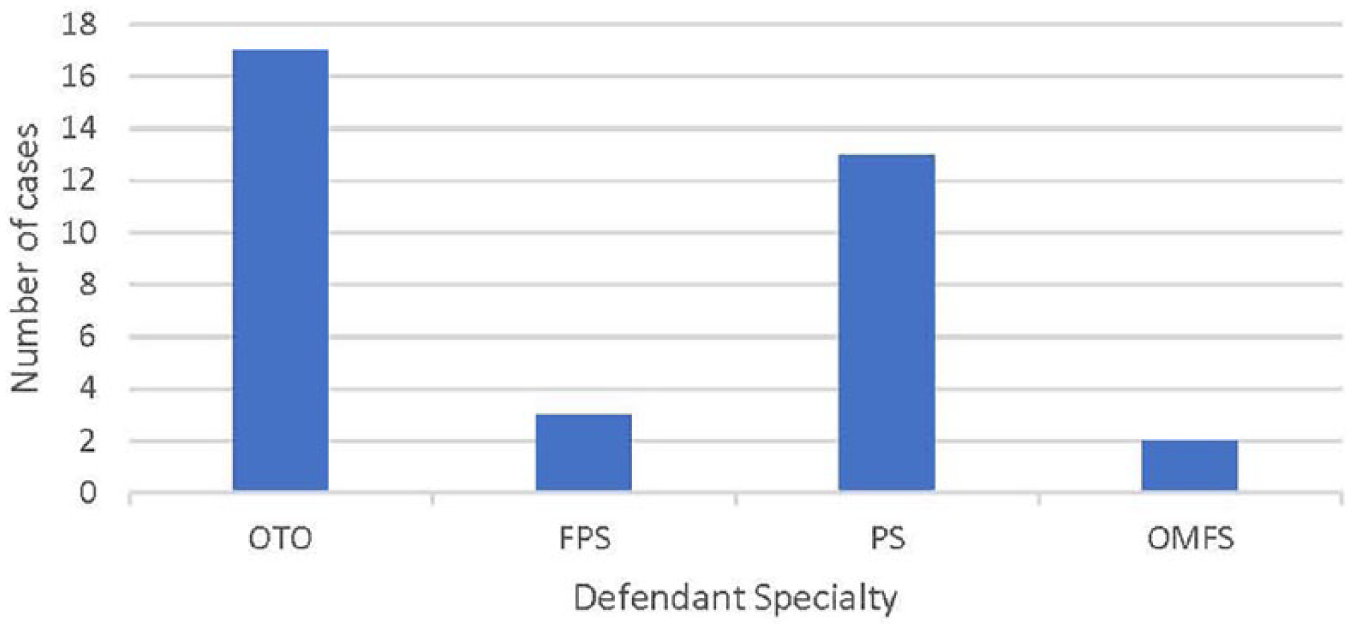
Defendant specialty in malpractice litigation related to rhinoplasty.
Case Allegations and Associated Outcomes
The most common allegations raised in litigation were poor cosmesis (20 [44%]), intraoperative negligence (18 [39%]), inadequate informed consent (13 [28%]), nasal function deficit (13 [28%]), and postoperative negligence (9 [20%]). Other cited factors in pursuing litigation were breach of contract (4 [9%]), pain (4 [9%]), death (2 [4%]), preoperative negligence (2 [4%]), infection (1 [2%]), breach of standard of care (1 [2%]), fraudulent misrepresentation (1 [2%]), fraudulent concealment (1 [2%]), and additional procedures required (1 [2%]) (Figure 3). The presence or absence of certain allegations led to changes in defendant outcomes. Specifically, cases with allegations of cosmetic deformity resulted in a 7% lower rate (95% CI, −17.55 to 31.91) of positive defendant outcomes compared to cases without them; however, this difference of 7% is not statistically significant (p = 0.60). Cases with allegations of nasal function deficits resulted in a 17% lower rate (95% CI −9.29 to 45.32) of positive defendant outcomes compared to cases without them; however, this difference of 17% is not statistically significant (p = 0.24) (Table 2).
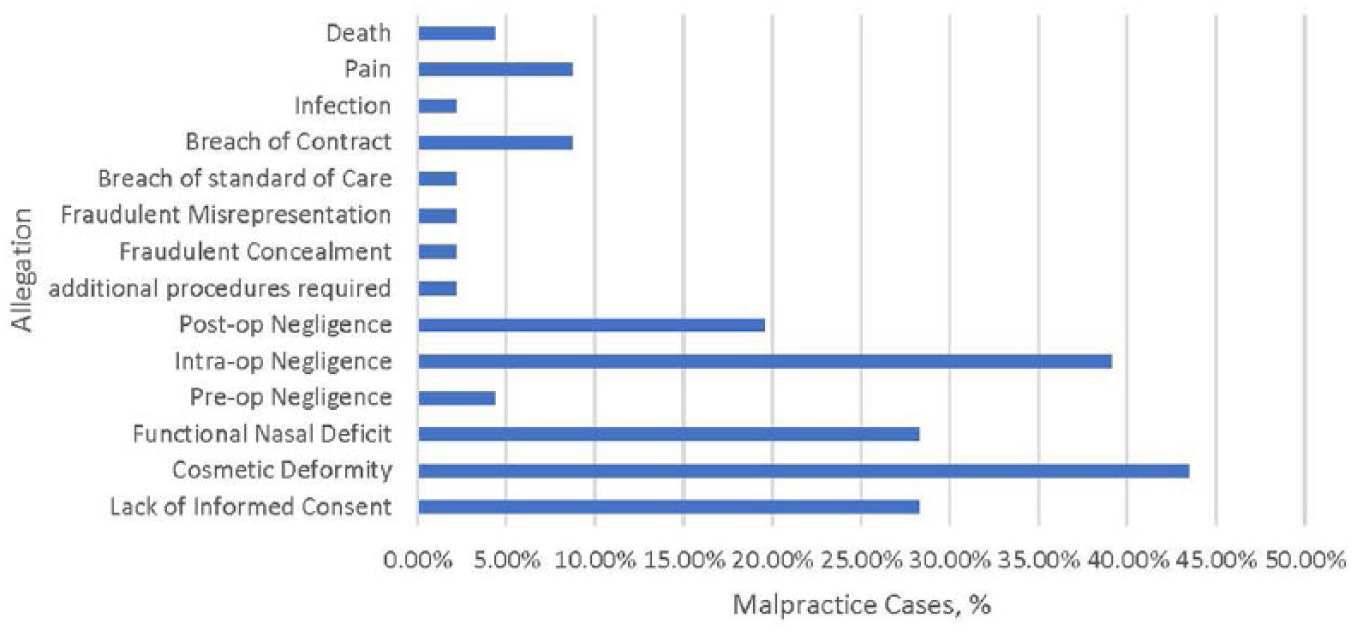
Allegations raised in malpractice litigation related to rhinoplasty.
Allegation Prevalence and Outcomes.
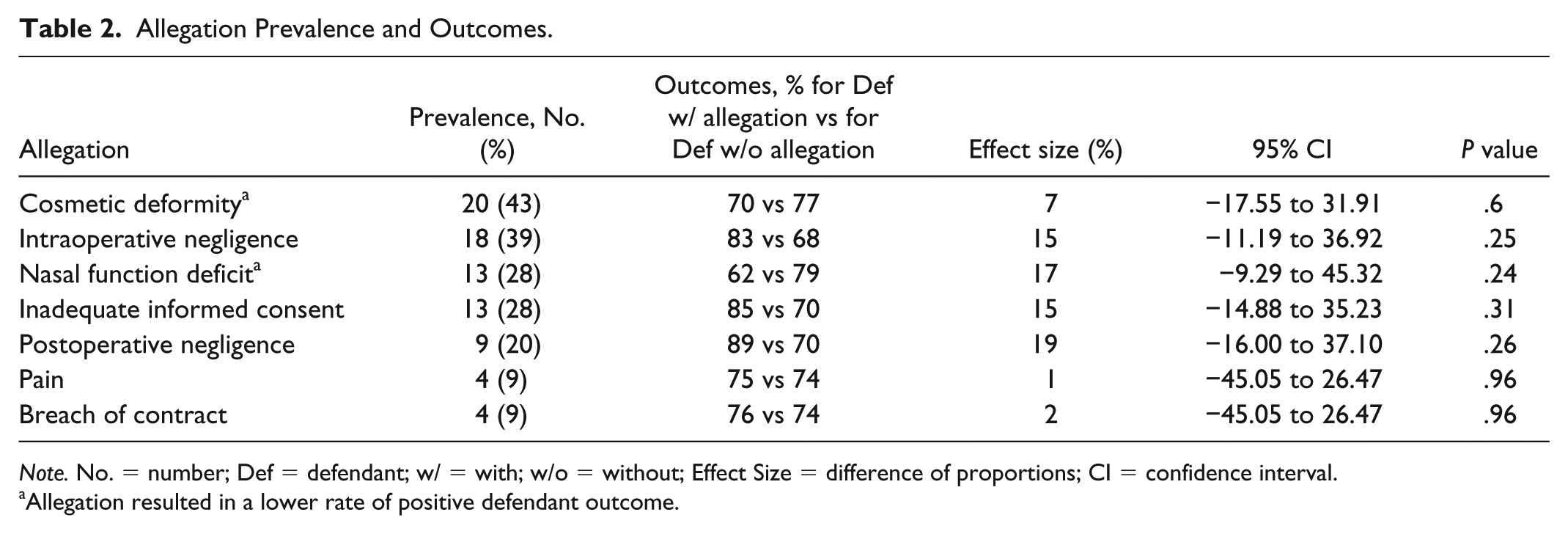
Note. No. = number; Def = defendant; w/ = with; w/o = without; Effect Size = difference of proportions; CI = confidence interval.
Allegation resulted in a lower rate of positive defendant outcome.
Discussion
Rhinoplasty constitutes the third most common cosmetic surgical procedure in the United States 1 and represents the second most litigated FPS procedure. 6 Therefore, understanding factors associated with rhinoplasty medical malpractice litigation takes on special importance, especially in today’s litigious environment. Unfortunately, there is a paucity of well-designed studies analyzing malpractice litigation specific to rhinoplasty.6-8,15,17 The most complete of these studies, published in the Laryngoscope in 2013, reports an analysis of court records pertaining to several different FPS procedures. 6 In their analysis of rhinoplasty-specific claims, the authors used medical malpractice and rhinoplasty as their sole search terms and identified 24 cases related to rhinoplasty. This previous analysis, while useful, is now 5 years old, used only one database (Westlaw), and had narrow search terms. The present study, though similar in methodology, represents a more comprehensive analysis with additional search terms and database sources (addition of Nexis Uni), capturing a greater number of cases (24 vs 46) and more recent cases (2013 vs 2018). In addition, we examined considerations specific to rhinoplasty including allegations of nasal function deficit and the rhinoplasty surgeon’s specialty (ie, PS, general OTO, FPS).
Defendant Outcomes
Previous studies report FPS malpractice litigation cases are often resolved in the physician’s favor. 6 Similarly, the majority (74%) of rhinoplasty litigation cases identified in this study ended in favor of the defendant. This pattern of positive defendant outcomes likely stems from the strict requirement that 4 certain conditions (duty, breach of duty [standard of care], harm, and direct causation) be present for plaintiffs to be awarded damages in medical malpractice cases. 21 Moreover, when trials present mistakes that are either acknowledged by physicians or apparent to juries, most of these cases are ruled in the defendant’s favor because the elements required for negligence are often not all met. 6
Financial Burden
Plaintiff verdict payments had the potential to present devastating financial distress to the defendant physician. In our study, rhinoplasty malpractice litigation cases ending in indemnity payments resulted in a median payment award of $127 500. This reward amount, while comparable to the median indemnity payment seen in malpractice litigation amongst all physicians ($111 749), 4 is significantly less than the previously reported jury awards of $200 000 for PS claims 4 and $500 000 for rhinoplasty-specific claims 6 resulting in indemnity payments.
Defendant Specialty
The surgeon specialties found for 35 identified cases included OTO (49%), PS (37%), FPS (9%), and OMFS (6%). These results suggest that more than half (58%) of rhinoplasty malpractice litigation claims involve otolaryngology-trained physicians (OTO and FPS). Though no definitive conclusions regarding prevalence can be made given the limitations of the databases used (see Limitations below), the larger number of otolaryngologists facing litigation may be best explained by the fact that otolaryngologists now perform almost triple the number of rhinoplasty procedures in comparison to plastic surgeons. 7 In addition, cases involving OTO defendants were more often resolved with payment (24%) compared with cases involving PS defendants (8%). This absolute difference of 16% is not statistically significant (P = .26), but the upper bound result of the 95% CI (40.40%) suggests there is a clinically meaningful difference; therefore, this is an inconclusive finding and warrants further investigation. Interestingly, no payments were awarded for litigation against FPS and OMFS defendants.
Cosmetic Deformity
Dissatisfaction with postoperative appearance plays a significant role in FPS 6 and rhinoplasty litigation.7,17 In our study, cosmetic deformity was the most common allegation (43%) raised in rhinoplasty malpractice litigation and is particularly relevant because of its potential association to poor defendant outcomes. Our study identified a 7% lower rate of a positive defendant outcome with cases involving allegations of cosmetic deformity. The absolute difference of 7% is not statistically significant (P = .6), but the upper bound result of the 95% CI (31.91%) suggests this is a clinically meaningful difference; therefore, this is an inconclusive finding and warrants further investigation.
Nasal Function Deficit
Functional complaints play a significant role in FPS malpractice litigation 6 and may be present in up to 50% of rhinoplasty malpractice claims. 17 In our study, allegations of nasal function deficit existed in nearly a third (28%) of identified cases, reiterating the importance of preserving or improving the nasal airway when performing rhinoplasty. This is particularly relevant because allegations of nasal function deficit may contribute to poor defendant outcomes, as our study identified a 17% lower rate of a positive defendant outcome with cases involving allegations of nasal function deficit. This absolute difference of 17% is not statistically significant (P = .24), but the upper bound result of the 95% CI (45.32%) suggests there exists a clinically meaningful difference; therefore, this is an inconclusive finding and warrants further investigation.
Intraoperative Negligence
Intraoperative negligence, which results when a physician deviates from the accepted medical standard of care, 21 constituted the second most common allegation (39%) in our analysis. The high prevalence of such allegations likely stems from the plaintiff’s attempt to establish a strong case for medical malpractice, since clear causation between negligent treatment and patient harm represent essential factors in determining a plaintiff’s eligibility for recovery of damages in medical malpractice. 21 Moreover, previous studies suggest that complaints directly related to mistakes made in the operating room tend to result in poor defendant outcomes compared with other complaints. 15
All things considered, the dominance of the aforementioned allegations (cosmetic deformity, nasal function deficit, and intraoperative negligence) emphasize that surgical techniques represent significant modifiable factors in avoiding rhinoplasty malpractice litigation.
Informed Consent
The lack or presence of informed consent—the disclosure of any information significant to a patient’s decision to undergo a procedure 21 —strongly impacts judicial outcomes in PS. 22 In an analysis of malpractice litigation involving FPS, a perceived lack of informed consent represented the single most common allegation reported (38% of cases). 6 In our study, allegations related to informed consent occurred in 28% of claims. Such disagreements over informed consent in PS arise from undisclosed risks and unexplained potential lack of benefit.21,23,24 With that being said, avoiding informed consent allegations in rhinoplasty requires the physician to undertake truthful preoperative discussions where he or she appropriately manages expectations and emphasizes the risks and limitations of the procedure, including the real potential for functional and/or cosmetic outcomes. Other factors that may strengthen informed decision making include allowing adequate time to pass (several days) before discussing the procedure in detail and its associated risks. 24 Last, obtaining informed consent with the use of supplemental materials, such as written information, audio-visual recordings and other decision aids enhances postoperative satisfaction25-27 and thus may further limit litigation.
Limitations
Limitations to this study relate primarily to the databases used. First, WestlawNext and Lexis Uni only contain cases that advance far enough to be included in public records, the criteria for which not only varies by jurisdiction but also excludes those cases resolved with out-of-court settlements. Consequently, these databases’ role in accurately analyzing incidence and/or prevalence of malpractice litigation is limited, meaning we most likely underestimated the number of rhinoplasty litigation cases present over the last 30 years. Second, significant heterogeneity exists in the court records available in these databases. Some records included significant detail about the cases presented, while others only offered basic summaries. This heterogeneity resulted in inconsistencies in the available data including defendant specialty and plaintiff age. Nevertheless, the databases used remain useful tools and have shown their value in prior litigation analyses with similar methodology.6,15,16,18-20
To the best of our knowledge, this is the first comprehensive review of malpractice litigation specifically focusing on rhinoplasty. The findings presented herein should serve to educate and benefit those performing such procedures in the future
Conclusion
We present the first comprehensive review of malpractice litigation specific to rhinoplasty. Our findings suggest that rhinoplasty malpractice litigation resulting in payments creates substantial financial burden for the defendant. Common factors cited by plaintiffs for pursuing litigation included cosmetic deformity, nasal function deficit, intraoperative negligence, and lack of informed consent. Cases with allegations of cosmetic or functional deformity tended to result in negative defendant outcomes, though these findings are inconclusive. These findings reinforce the importance of physician-patient communication, including conducting a comprehensive informed consent process, to mitigate post-rhinoplasty allegations.
Footnotes
Acknowledgements
The authors thank Tulane Law Librarian, Megan Garton, JD, MLIS, for her assistance in creating a comprehensive search strategy.
Authors’ Note
The findings of this study were submitted as a podium presentation to the 2019 Advances in Rhinoplasty meeting on April 4-7, 2019, in Orlando, FL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.