
Abstract
The aim of this study is to introduce a sophisticated method for malar reduction or augmentation through an additive manufacturing technology. Using the results of data analysis in KAVEH software, a surgical guide will be developed for both sides, which will be used in a zygomatic sandwich osteotomy. Both reduction and augmentation malarplasty could be done after osteotomy with outward or inward rotation of the zygomatic complex around the zygomatic arch based on pre-surgical analysis. We recommend usage of additive manufacturing technology in malar augmentation to obtain more precise and predictable outcomes.
Introduction
The malar prominence plays a key role in total beauty and normal proportions of the facial area. Flat and hypoplastic malar region is related to an unappealing, fatigued, and elderly appearance.1-3
Since the development of malar augmentation techniques in 1970s, different methods have been introduced including onlay grafts, alloplastic implants, and malar osteotomies. 4 However, with these techniques, it is not easy to deliver a symmetric and pleasing outcome especially for novice surgeons. 1
Nowadays, 3-dimensional (3D) reconstructive techniques based on rapid prototyping technology showed to be beneficial in various fields of oral and maxillofacial surgery.5-7 The aim of this study is to introduce a simple method to execute malar augmentation by zygomatic sandwich osteotomy using additive manufacturing technology to perform this operation with more predictable and efficient results.
Methods
At first step, 3D computed tomography of the facial region with axial and coronal views (1 mm Incremental slices, Gantry zero, Bone Plus Protocol, HiSpeed QXi, GE Healthcare) was obtained. The raw data were input into KAVEH Software (KAVEH Package, special software package for Cranial and Maxillofacial Implantology/Surgery Tehran, Iran) for virtual malar osteotomy. The software package uses an individualized and dedicated module, specially designed for treating planning of the patient face (Called Omid). Zygomatic Sandwich Osteotomy introduced by Mommaerts et al 8 was chosen to perform in this study due to its better anterolateral projection, easiness, and satisfactory outcomes. To determine the amount of required malar augmentation and optimal soft tissue reposition, the “beauty arch” analysis by Marianetti et al 2 was used in 3 dimensions. For better usage, the software has been modified by special module to reproduce the beauty arch analysis with 3D view for both arches (Figure 1).
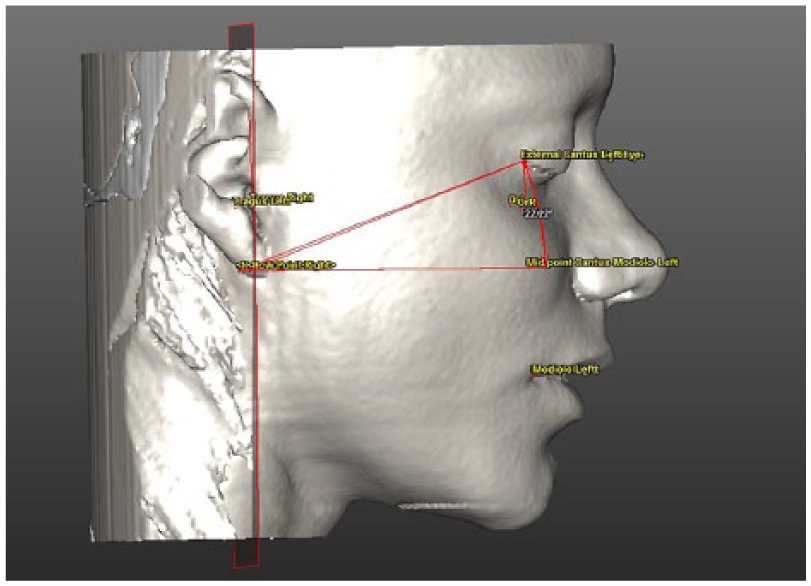
Three-dimensional analysis of the “beauty arch.”
Afterward, planned osteotomy lines were marked on the virtual 3D model existing in the KAVEH software. Finally, 2 surgical guides (left and right) were designed clearly and fabricated through principle of Rapid Prototyping Technology (SLA technology-RUNA CO. Tehran-Iran) to exactly adapt the areas of the osteotomy lines using special resin (Figure 2). The guides, one for the right one for the left, are then fitted on the respective malar areas and fixed. The osteotomy was then achieved by aid of the borders of the guides (Figure 3).
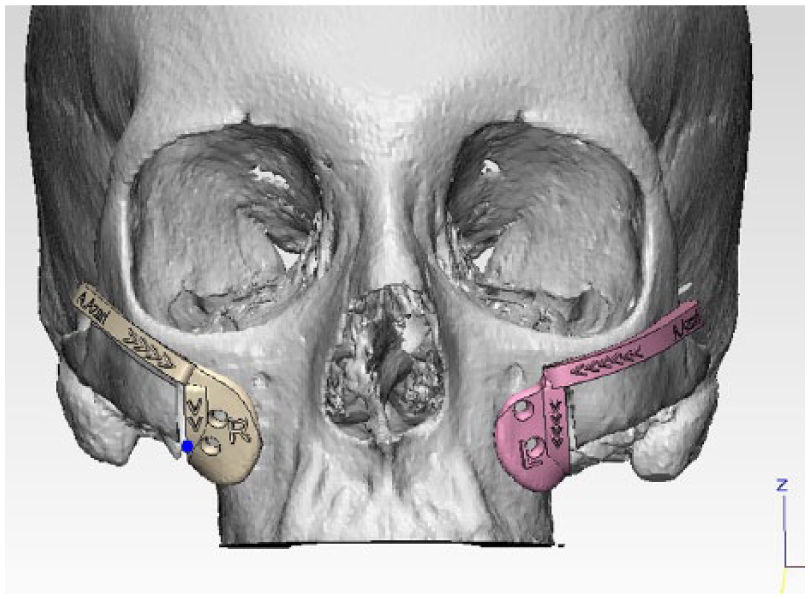
Malar osteotomy surgical guide design and fabrication.
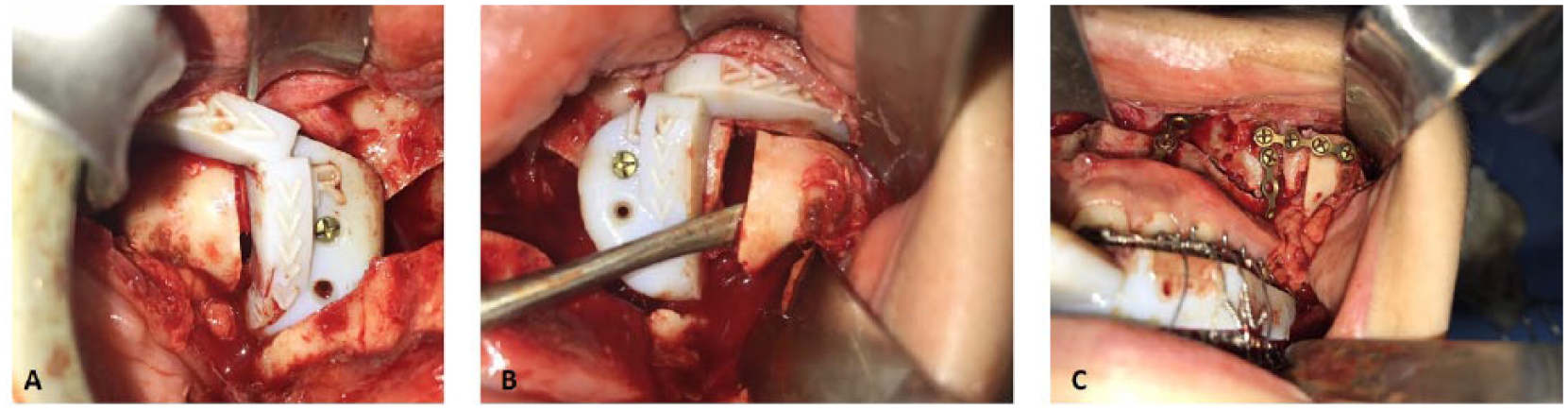
Application of malar osteotomy surgical guide in the patient’s operation.
A horizontal incision, parallel to and at least 5 mm cranial to the mucogingival margin, is made. A vertical subperiosteal tunnel is made over the zygomaticomaxillary suture line. Another subperiosteal tunnel (approximately 20 mm in length) is made over the posterior aspect of the maxillary process of the zygoma. The vertical osteotomy is then made using a thin reciprocating saw blade. This vertical osteotomy transects both the anterior and posterior maxillary sinus walls. The bony cut stops at the semihorizontal groove, approximately 4 mm below the infraorbital rim. While the oblique horizontal osteotomy is performed, the osteotomy starts at this junction and proceeds in an anterior, medial, and slightly inferior direction, traveling through the semi horizontal groove 4 mm under the orbital rim to meet the cranial end of the vertical osteotomy. The reciprocating saw is angulated so that the anterior and posterior sinus walls are transected while leaving the orbital floor intact. The osteotomy lines are completed with chisels. It is important that the osteotomies are complete and that the fulcrum is at the inferior part of the vertical bone cut, where the bone is thick and dense (lateral maxillary buttress). If the lateral maxillary buttress is cut (eg, when a Le Fort I osteotomy is performed), it is advisable to pull laterally with the osteotome without applying pressure on the bone of the canine fossa. In some patients, the zygomatic arch will bend elastically, whereas in others a greenstick fracture occurs at the temporozygomatic suture. A wedge of hydroxyapatite or other material is carved to the exact width and wedged in the vertical osteotomy space.
Results
Both reduction and augmentation malarplasty could be done after osteotomy with outward or inward rotation of the zygomatic complex around the zygomatic arch based on pre-surgical analysis. The advantages of this technique in comparison to the conventional technique include a more precise and finer cutting, and more precise localization of adjacent structures, such as the orbital floor, nerves, etc which reduces the possibility of potential damages. Reported complications with other techniques, such as transient sensory weakness, drooping, nonunion, asymmetry, mouth opening restriction, uncontrolled bleeding, and facial nerve injury, 9 were not noted with our technique, probably because of improved visibility and control during the surgical procedure due to precise cutting. Preoperative and postoperative views of 2 patients who underwent surgery using the malarplasty technique are shown in Figures 4-7. Also, the preoperative and postoperative radiographic views of the first case are shown in Figures 8 and 9.

Preoperative lateral view of the first case.
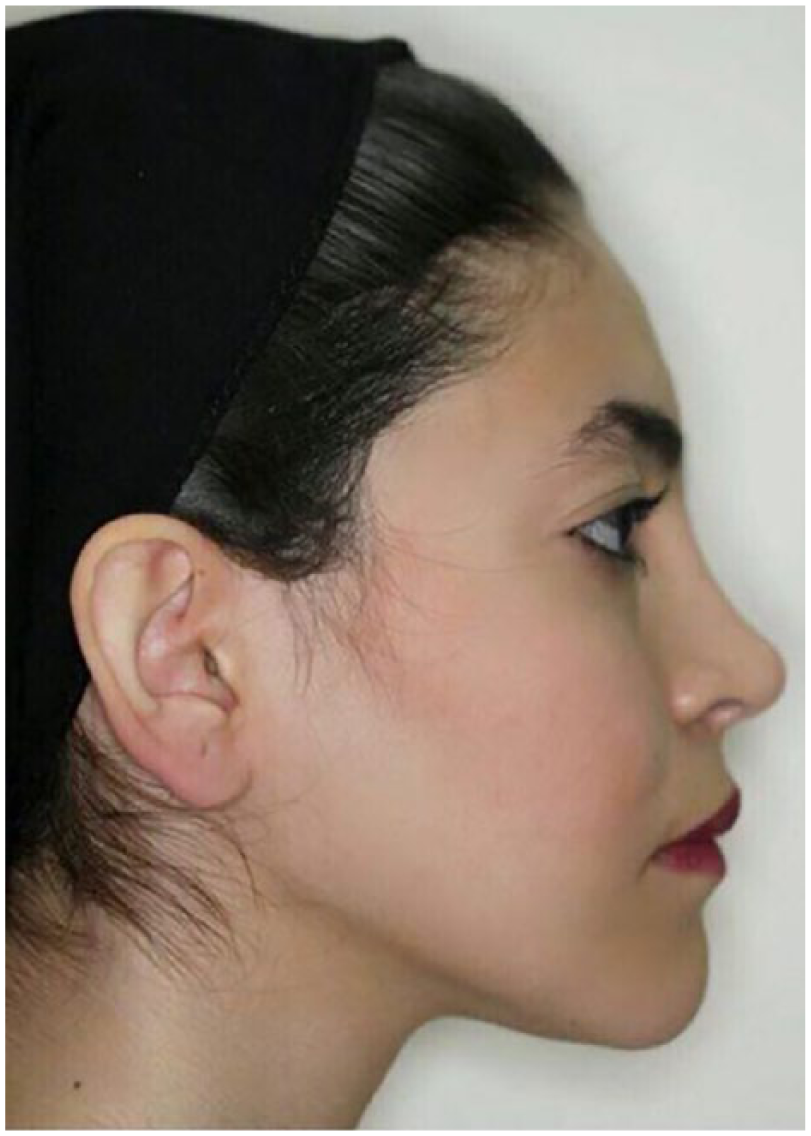
Postoperative lateral view of the first case.
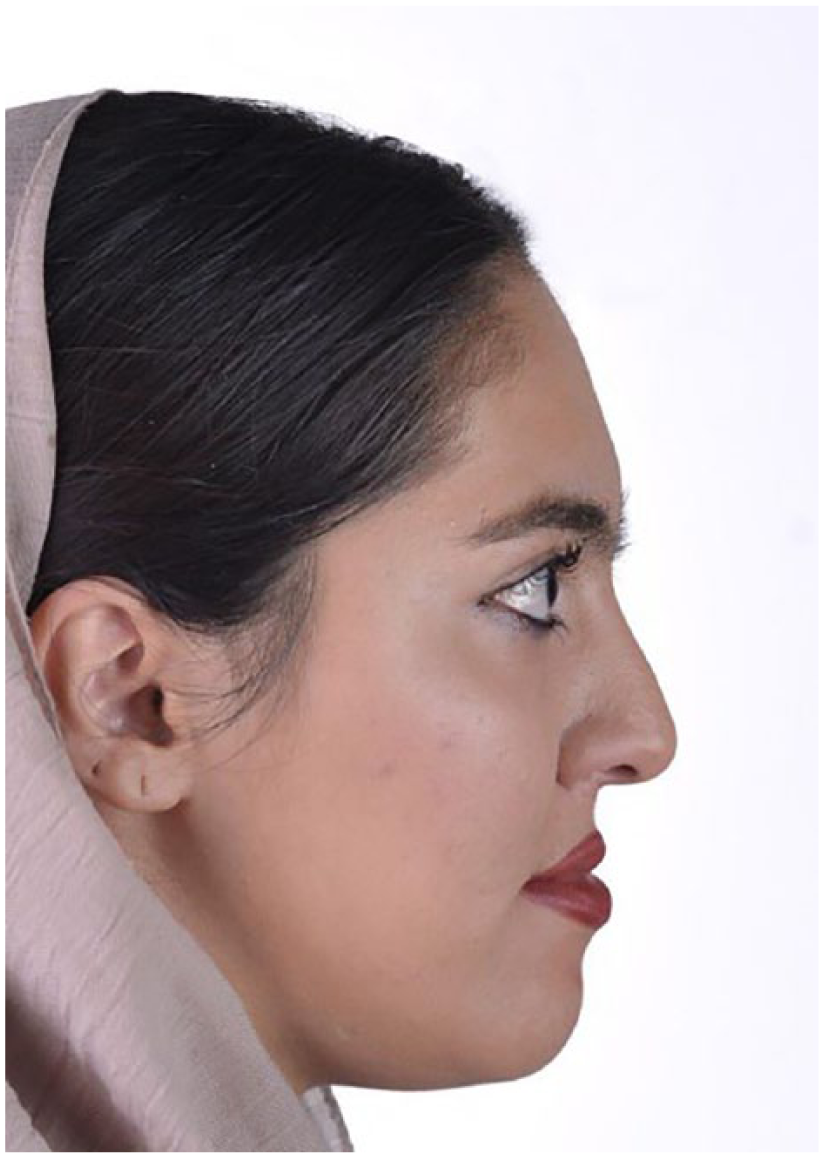
Preoperative lateral view of the second case.

Postoperative lateral view of the second case.

Preoperative lateral cephalometric x-ray of a sample patient.

Postoperative lateral cephalometric x-ray of a sample patient 18 months after surgery.
Discussion
The malar area is a crucial determinant of overall facial beauty. A full malar prominence can provide a young and joyful appearance. 10 Alloplastic implant placement is the most common method for malar augmentation. However, these implants can be possibly accompanied by complications such as improper size selection, infection, malposition, and tissue reaction. 11
To overcome these complications, malar osteotomies were introduced. Zygomatic malar osteotomy, initially introduced by Mommaerts et al, 8 is a quick and easy procedure with predictable and symmetrical outcomes. 1
Three-dimensional printing is cited as a novel fascinating future builder technology in many papers and articles. Application of this technology in medicine is expanding and especially in the field of oral and maxillofacial surgery. This technology is beneficial in decreasing operation time, better treatment planning, and achieving more predictable and efficient results.12,13
Nerve injury, orbital floor fracture, and damage to the components of the oral cavity are recorded among complications of malar augmentation technique, which can be avoided using accurate 3D printed surgical guides. 14 The second advantage of the presence of surgical splints is preventing lateral walls of maxillary sinuses from unwanted fractures caused by rotational forces of osteotomes. Furthermore, application of the KAVEH software enables 3D analysis of the beauty arch and determination of the amount of hard tissue augmentation considering the ratio of soft tissue adaptation to bone in the malar region.
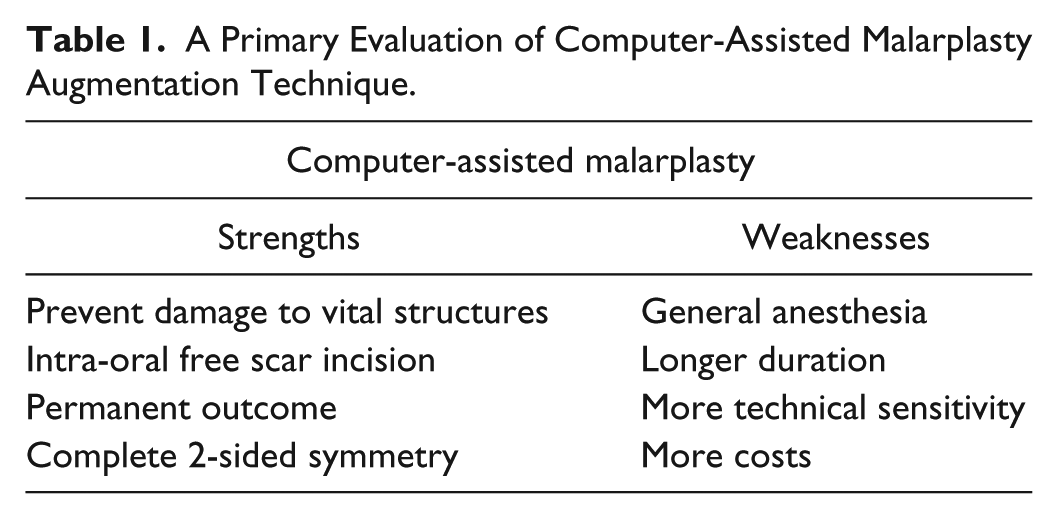
In addition to our technique, other methods, including the use of implants, 15 prosthesis, 16 and fillers,17,18 may also be used in cheek augmentation, each with its own advantages and disadvantages. It can be argued that due to the precise application of 3D design and the use of elegant surgical guides, the malarplasty technique has more predictable results in the long term and significant advantages over other methods. Unlike using fillers,19,20 this technique is a permanent treatment and does not require periodic renewal. In this technique, as augmentation is carried out by the bones itself, and the structures are fixed in a precise and durable manner using the screws, the probability of deformity, displacement, 21 and asymmetry22-24 is less than the use of fillers. This method has a great deal of accuracy and elegance, so its results are more predictable than other methods. Unlike the use of prosthesis, because of lesser use of the external irritating material, probably there is less possibility of bone defects and bone resorption 25 and infection 26 in this method. A definitive judgment about the effects of this technique on adjacent bones requires long-term evaluations in future studies, but in the cases for which this technique was used, there was no indication of bone defects or infection until the last examination of each. All patients were operated by a single surgeon and according to (1) the time required for this surgery, (2) the ability to prevent damage to vital structures through software analysis and surgical guide, (3) the ability to carry out the procedure with intra-oral free scar incision, (4) permanent outcome, and (5) possibility of complete 2-sided symmetry, this method can be used as an alternative method for malar augmentation. By examining and comparing the appearance of person’s faces after applying various techniques, it seems that the changes resulting from the use of the technique described in this study will create a more natural appearance than the other methods, which results, obviously, in the satisfaction of most patients in terms of shape, size, and volume. The use of other techniques, such as removing or lift of buccal fat pad,27,28 can also help the cheeks to look more prominent, but the results are not as satisfactory and predictable as the use of this technique. It should be noted that this article is a preliminary study with limitations such as small group of samples, lack of statistical analyses, and failure to perform long-term follow-up in terms of the quality of the technique results and the degree of satisfaction of patients and surgeons. Therefore, it will be necessary to carry out wider studies in the future that will accurately compare the strengths and weaknesses of this technique with other methods and ensure the validity of this technique through statistical analyses (Table 1).
A Primary Evaluation of Computer-Assisted Malarplasty Augmentation Technique.
It should be noted that in this article, the purpose is merely to report the results of using an innovative surgical procedure on a number of cases; therefore, in the future, it seems necessary to conduct a clinical trial with a larger sample size and statistical analysis to measure the significance of the results.
Conclusions
As a conclusion, we suggest that this additive manufacturing technology can be used both for reduction and for augmentation during the zygomatic sandwich osteotomy technique, to obtain more precise and predictable outcomes.
Footnotes
Acknowledgements
This study was conducted by personal investment of researchers and no institution or organization was involved.
Authors’ Note
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Information contained herein is not intended to be a source of advice or credit analysis with respect to the content presented, and the information and/or documents contained in this paper do not constitute investment advice.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
As this surgical technique is a variation of normal procedure, ethics approval did not seem to be necessary. All patients gave written consent for their image to be published in scientific publications in compliance with current personal data protection regulations.