
Abstract
Nasal bone osteotomies are commonly performed in rhinoplasty to manipulate the upper third of the nose. In patients with a dorsal hump, reduction is often performed, followed by lateral osteotomies to medialize the nasal bone complex. However, fracture patterns are often unknown in vivo. We intend to map nasal bone osteotomies and describe a novel and minimally invasive method of performing medial scoring osteotomies to improve fracture patterns and surgical speed, and decrease complications. In total, 19 formalin-fixed cadavers were dissected to reveal nasal bone architecture. The nasal dorsum (bony and cartilaginous) was reduced to form an open roof deformity. Osteotomies were then performed on all 19 specimens, followed by digital infracture. Medial scoring osteotomies were performed unilaterally, along with a lateral osteotomy. On the contralateral side, only lateral osteotomies were performed. Fracture patterns were mapped and compared. Of 19 cadaver specimens, 38 sides were examined in total: 19 sides underwent medial scoring and 19 sides served as controls. Fracture patterns were linear with less comminution on sides with medial scoring osteotomies. Sides with medial scoring osteotomies also achieved uniform closure of the open roof deformity, compared with 73% in sides without. Rocker deformity was not seen in either group. Osteotomies are integral to nasal dorsum reduction and modification of the upper third of the nose in rhinoplasty. Scoring of the medial nasal bone prior to lateral osteotomy and digital infracture allows for an increased rate of open roof closure. Furthermore, medial scoring osteotomies create smooth, linear fracture patterns that prevent bony spicules, comminution, and irregularities that may be evident in patients with thin nasal skin. Performing the medial scoring osteotomy is a fast, safe method of achieving consistent nasal bone infracture during rhinoplasty.
Introduction
Rhinoplasty is an essential technique used by facial plastic surgeons to restore cosmetic harmony to the face and improve nasal obstruction. Nasal bone osteotomies are frequently performed and allow the surgeon to carefully manipulate the upper third of the nose and manage bone morphology. Osteotomies in the head and neck can be performed under direct visualization in traumatic or orthognathic procedures. Unfortunately, during aesthetic and functional rhinoplasty, the soft-tissue envelope prevents direct view of the nasal bones during osteotomies. For this reason, analysis of the nasal bone osteotomy is difficult and multiple techniques have emerged as a result.
When addressing the dorsal hump, osteotomies are particularly important. Reduction of the dorsal hump is one of the most common indications for aesthetic rhinoplasty. 1 After dorsal hump reduction, many patients require further manipulation of the nasal bone architecture to achieve balance in all views. 2 Typically, after bony and cartilaginous hump reduction, only lateral osteotomies are performed, with the assumption that the hump reduction and open roof deformity create bilateral medial osteotomies. However, objective evaluation of the nasal bone structure has not been performed to determine whether lateral osteotomies alone after dorsal hump reduction adequately mobilize the nasal bone fragment.
In the senior author’s practice, a new technique has been developed to improve the contour and consistency of the fractured nasal bone segment after hump reduction. Similar to scoring of tile to create a clean break, the senior author uses a 2-mm osteotome to create a medial notch in the nasal bone, oriented at a 15-degree angle from the midline, to provide a line of fracture that would otherwise not exist. The purpose of this study is to examine nasal bone architecture in cadavers who have had a nasal dorsal hump reduction and who have undergone medial scoring osteotomy followed by lateral osteotomy with digital infracture of the nasal bones.
Materials and Methods
This study was performed using 19 cadaveric temporal bone specimens from the Emory University School of Medicine. These cadavers were fixed in formalin and all were older than 60 years of age. This study did not require IRB (Institutional Review Board) approval from the Emory University School of Medicine as it did not involve live human subjects or patient documentation. The senior author performed all nasal bone osteotomies to ensure surgical consistency.
The cadavers were initially examined for nasal soft-tissue envelope and nasal bone integrity. All cadavers had intact nasal soft-tissue envelopes and no evidence of nasal bony trauma. Next, each cadaver underwent bony and cartilaginous nasal dorsum takedown to create a straight dorsum with an open roof deformity. Two groups were formed—an experimental group and a control group. The experimental group underwent medial scoring osteotomies followed by an ipsilateral high-low-high lateral nasal bone osteotomy. 3 The medial scoring osteotomy is shown in Figure 1 and diagrammed in Figures 2 and 3. The contralateral side of each cadaver served as the control group, where a medial scoring osteotomy was not performed and only a high-low-high lateral osteotomy was performed. The experimental group consisted of 10 right-sided nasal bones and 9 left-sided nasal bones. The control group consisted of 9 right-sided nasal bones and 10 left-sided nasal bones. Firm digital pressure was used to fracture both nasal bones medially to create a symmetric upper nasal third, narrow the widened bony dorsum, and close the open roof deformity. Next, the nasal soft-tissue envelope of each cadaver was carefully and entirely removed to expose the nasal bone superstructure without manipulating the nasal bone architecture post-osteotomy.
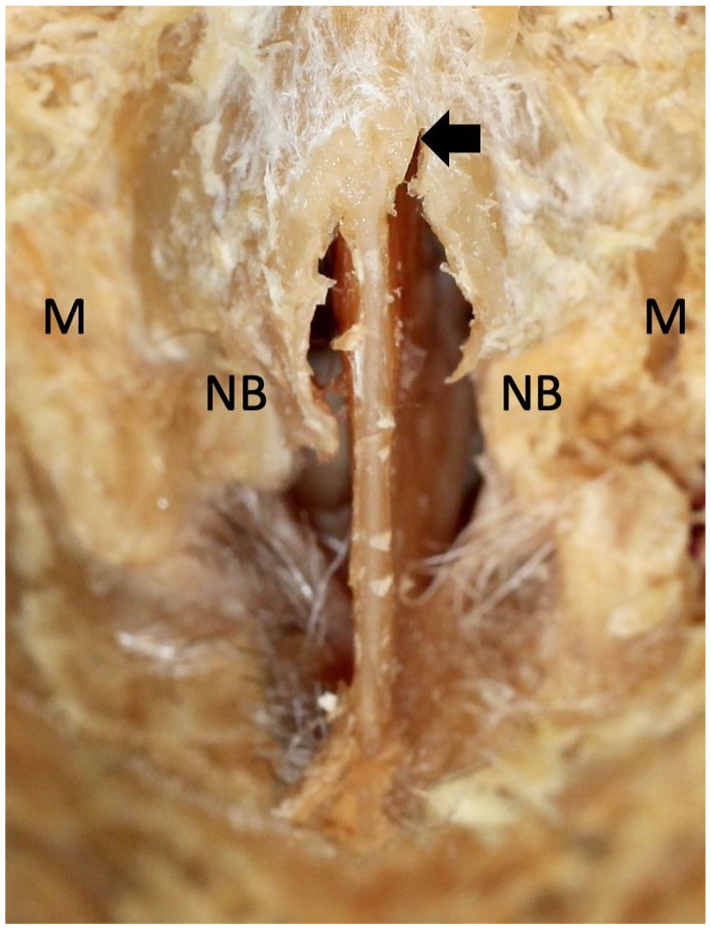
Cadaver photo of open roof deformity and left-sided medial scoring osteotomy.
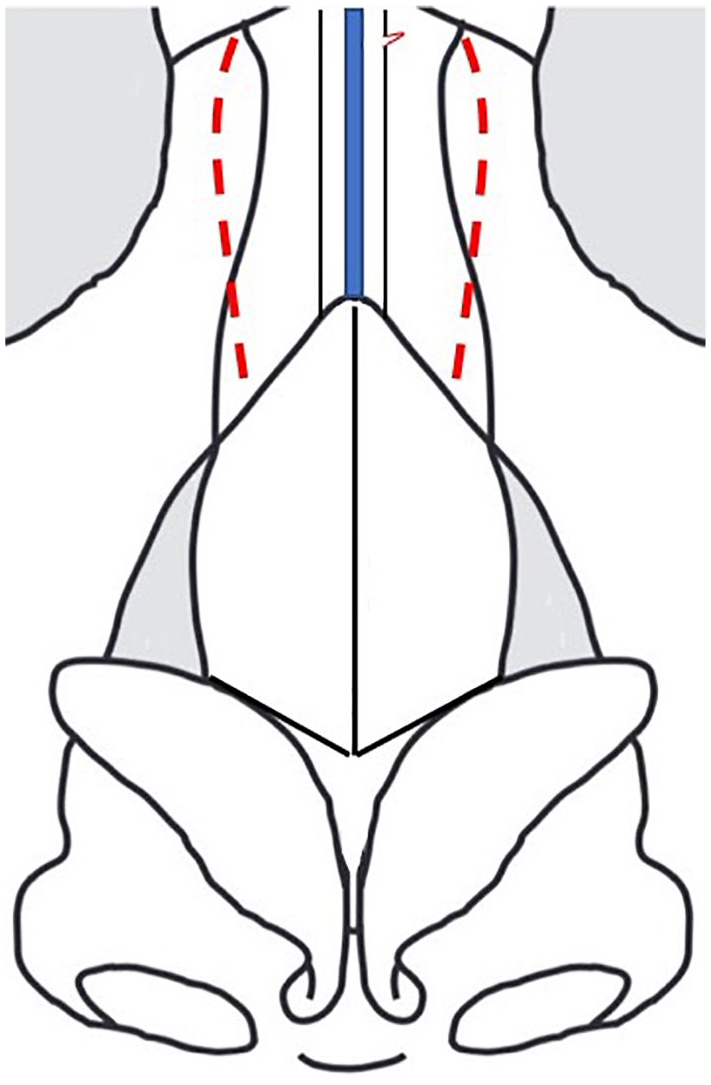
Schematic depiction of technique.
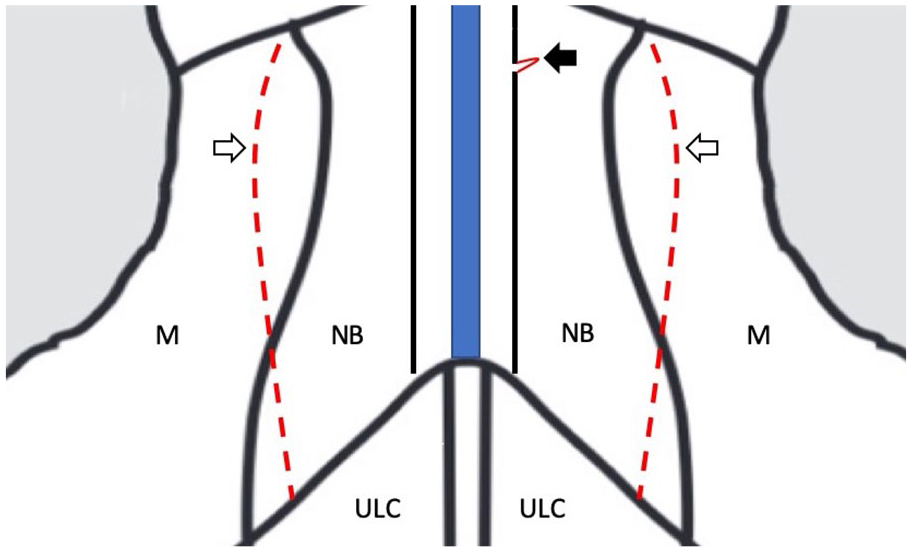
Magnified schematic depiction of technique.
Once the nasal bone superstructure was skeletonized and exposed, detailed photographs were taken with a dSLR Cannon EOS Rebel T4i Camera with an 18-135-mm lens (Ota, Tokyo, Japan). Frontal, side, and three-quarter view photos were taken for each side. The photos were de-identified and stored on a password-secured server for analysis.
The post-osteotomy nasal bone photos were examined, and each nasal bone fragment was outlined carefully (Figure 4). Five parameters were identified: (1) number of fragments, (2) bony irregularities and spicules, (3) presence of a Rocker deformity, (4) closure of the open roof deformity in relation to the ipsilateral cartilaginous septum and perpendicular plate of the ethmoid, and (5) whether the medial osteotomy fracture line was irregular.
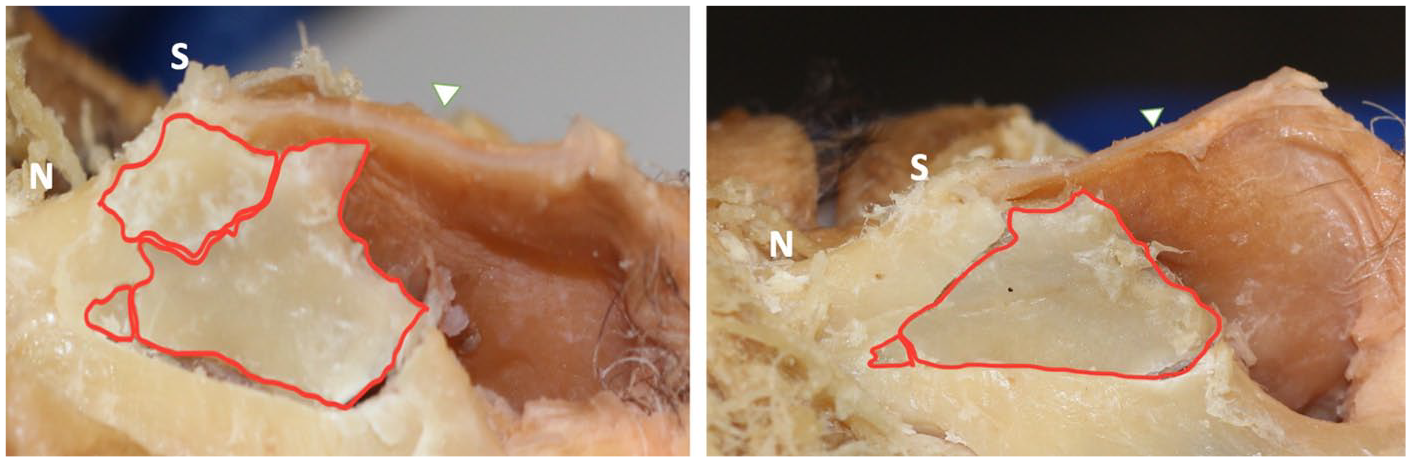
Cadaver dissection after osteotomies and digital infracture with soft-tissue envelope removed: left photo is control group with lateral osteotomy only, and right photo is experimental group with medial scoring osteotomy and lateral osteotomy.
Statistical analysis was performed using a paired t test when comparing the number of fragments in the experimental versus control side. For bony irregularities and spicules, presence of a Rocker deformity, closure of the open roof deformity, and whether the medial osteotomy fracture line was irregular, chi-square categorical analysis was performed. Post hoc power analysis was performed using group means, standard deviations, and an alpha of .05.
Results
In total, 38 cadaver sides were dissected in total (19 cadavers). Two groups were created for analysis: experimental side where medial scoring osteotomy was performed and control side where medial scoring osteotomy was not performed.
Of the dissected cadavers, none had previous palpable bony irregularities or mobile nasal bones. None had a history of head trauma, craniofacial malformations, or craniomaxillofacial fractures. After dissection of the nasal bones, midface, and frontal bones, this was confirmed visually by our team.
Of the 19 dissected cadavers, the average number of fragments in the experimental group was 1.79, compared with 2.26 in the control group (P = .18). There were no cadavers in the experimental group with a persistent open roof deformity after the lateral osteotomy was performed with digital infracture of the nasal bone complex. In the control group, 5 (26.3%) cadaver sides had a persistent open roof deformity (P = .046). There were no Rocker deformities noted in either group. Of the cadavers dissected, all of the nasal bone fractures in the experimental group fractured along the intended medial scoring osteotomy line, at 15 degrees from midline. In the control group, only 8 (42.1%) sides fractured along the intended 15-degrees line (P = .003). In the experimental cadaver sides, 7 (36.8%) sides developed irregular bony edges and spicules, compared with 14 (73.7%) in the control group (P = .049).
Discussion
Creating an aesthetically pleasing result and improving nasal harmony in rhinoplasty can be achieved with appropriate knowledge of nasal anatomy and surgical maneuvers. Medial scoring of the nasal bones after dorsal hump reduction is a safe adjunct after dorsal hump reduction to create predictable fracture patterns. There are various osteotomy techniques available to the facial plastic surgeon to manipulate the nasal bone architecture, 4 , 5 but many are not without risk. In an effort to decrease the number of bony fragments, decrease open roof deformity rates, and improve overall cosmesis, the surgeon can score the medial nasal bone to control the fracture trajectory and pattern.
Multiple studies have examined medial and lateral nasal bone osteotomies and established technical changes to improve immediate and long-term outcomes. Erişir and Tahamiler 6 described a lateral micro-osteotomy technique using a 2-mm, V-shaped osteotome without raising the periosteum, leading to less ecchymosis and edema in the immediate postoperative stage. To examine the medial osteotomy, Harshbarger and Sullivan 7 dissected cadavers and performed 0- or 15-degree medial osteotomies, demonstrating that 0-degree medial osteotomies cut into much thicker bone and created contour irregularities. An early descriptive study by Thomas et al 8 examined surgical technique and suggested that preservation of the nasal bone periosteum with minimal undermining with a micro-osteotome and a medial, oblique fading osteotomy may improve cosmetic outcomes and decrease postoperative edema and ecchymosis.
After nasal dorsum reduction, the subsequent open roof deformity is considered a bilateral medial osteotomy. However, these osteotomies are oriented at 0 degrees from the midline, which can create irregular contour of the nasal bone fragments after fracture. 2 Nasal bones become thin cephalically prior to the transition to the frontal process, predisposing to multiple fractures in an irregular pattern. Medial scoring at a 15-degree angle will begin the fracture line in the natural cleavage plane described by Harshbarger to create a smooth fracture without bony edges, which may correlate to improved cosmesis. Our data show a lower number of bony fragments after medial scoring osteotomy when compared with the control group. Although not statistically significant, a lower number of fragments would suggest fewer bony edges in the fractured nasal bone. This, in addition to the fewer bony spicules and irregular edges demonstrated in the experimental group, allows for fewer irregularities projected onto the overlying soft-tissue envelope.
In addition to cosmetic and functional manipulation of nasal bones, osteotomies allow for mobilization of the nasal bone segment to close the open roof deformity created by dorsal hump reduction. However, it is difficult to determine whether the open roof deformity is fully closed clinically, particularly in a patient with a thick soft-tissue envelope. Our data set demonstrated closure of the open roof deformity in all nasal bones who underwent medial scoring osteotomy, compared with only 73.6% of control sides. Review of the cadavers with persistent open roof deformity demonstrated irregular bony fractures that prevented medialization of the nasal bone subunit to the septum. This raises the question of whether open roof deformities are truly closed after lateral osteotomy alone and whether long-term aesthetic complications can be avoided using the medial scoring osteotomy technique.
There were limitations to this study, the most challenging of which was clinical correlation in our cadaveric study. Unfortunately, the examination of nasal bone architecture with the naked eye before and after experimental techniques is impossible in the clinical setting, and our cadaver study serves as a surrogate. In addition, the comparison of bony fragments between the two groups was underpowered. Although there were fewer bony fragments in the experimental group, the difference compared with the control group did not meet statistical significance. This was limited by the number of cadavers available for dissection at our institution. Finally, the quality of bone can affect fracture patterns. Quality of bone can depend on many patient-specific demographics, including age and sex. Unfortunately, as these data were not available to us during this study, further comments cannot be made. Further studies should be directed at age- and sex-related changes in nasal bone quality and effect on osteotomies.
Conclusion
Controlled fracture of the bony vault is a critical aspect of successful aesthetic and functional rhinoplasty. Scoring of the medial nasal bone can be performed quickly, with minimal instrumentation of the nasal bones and periosteum. This will allow the surgeon to reproducibly manipulate fracture patterns while preventing complications such as open roof deformities and rocker deformities, or aesthetic irregularities due to bony spicules. Medial scoring osteotomy is a useful adjunct in the surgical armamentarium of the cosmetic and reconstructive surgeon, allowing the surgeon reproducible control of the nasal bone suprastructure for more consistent cosmetic results.
Footnotes
Authors’ Note
Paul Daraei, Hardik Doshi, and Louis DeJoseph had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author Contributions
Paul Daraei helped in study design and execution, data collection, data analysis, manuscript drafting, editing, and submission. Hardik Doshi and Louis DeJoseph were involved in study execution, data analysis, manuscript drafting, and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.